-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
1/19
333
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
Copyright 2015 Undersea & Hyperbaric Medical Society,
Inc.
Clinical results in brain injury trials using HBO2therapy:
Another perspective
Xavier A. Figueroa, Ph.D.1, James K. Wright, M.D.2
1 The Brain Health & Healing Foundation, Seattle, Washington
U.S.
2 Swedish Medical Center-Edmonds, Wound Healing &
Hyperbarics, Edmonds, Washington U.S.
CORRESPONDINGAUTHOR: Xavier Figueroa [email protected]
______________________________________________________________________________________________________________________________________________________
ABSTRACT
______________________________________________________________________________________________________________________________________________________
The current debate surrounding the use of hyperbaric oxy-
gen (HBO2) for neurological indications, specically mild
to moderate chronic traumatic brain injury (mTBI) and
post-concussion syndrome (PCS), is mired in confusion
due to the use of non-validated controls and an unfamil-
iarity by many practitioners of HBO2 therapy with the
experimental literature. In the past 40 years, the use of
an air sham (21% oxygen, 1.14-1.5 atmospheres absolute/
atm abs) in clinical and animal studies, instead of obser-
vational or crossover controls, has led to false acceptance
of the null hypothesis (declaring no effect when one is
present), due to the biological activity of these sham
controls. The recent Department of Defense/Veterans
Administration (DoD/VA) sponsored trials, previous
published reports on the use of HBO2therapy on stroke
and mTBI and preliminary reports from the HOPPS
Army trial, have helped to highlight the biological ac-
tivity of pressurized air, validate the development of a
convincing control for future studies and demonstrate
the effectiveness of a hyperbaric intervention for mTBI/
PCS. Approval of HBO2 for neurological indications,
especially for mTBI/PCS, should be granted at the federal,
state and certifying body levels as a safe and viable
treatment for recovery in the post-acute phase.
_______________________________________________________________________________________________________________________
KEYWORDS: traumatic brain injury, hyperbaric oxygen, cognitive
function, TBI, HBO, HBO2,
_______________________________________________________________________________________________________________________
ABBREVIATIONS: amyloid precursor protein (APP); tissue
plasminogen activator (tPA); traumatic brain injury (TBI); mild to
mod-
erate traumatic brain injury (mTBI); acquired brain injury
(ABI); post-traumatic stress disorder (PTSD); post-concussion
syndrome
(PCS); single photon emission computed tomography (SPECT);
diffusion tensor imaging (DTI); regional cerebral blood flow
(rCBF); Rivermead Post-Concussion Symptom Questionnaire (RPQ);
PTSD Checklist Military Version (PCL-M); Department of
Defense (DoD); Veterans Administration (VA); standard of care
(SoC); hyperbaric oxygen (HBO2); Hyperbaric Oxygen Therapy for
Persistent Post-Concussive Symptoms (HOPPS). National Institutes
of Health Stroke Scale (NIHSS); activities of daily living
(ADL);
evaluation of quality of life (EQ); evaluation by the EQ-5D
descriptive system (EQ-5D); EQ visual analogue scale (EQ-VAS).
INTRODUCTION
The conclusions of the DoD/VA sponsored studies [1-
4] on the benets of hyperbaric oxygen (HBO2) therapy
for service members diagnosed with post-concussion
syndrome have recommended ceasing the development
of a promising therapy. The published conclusions of
the DoD/VA sponsored studies recommend the view
that there is no benet of HBO2for mild to moderate
traumatic brain injury (mTBI) and post-concussion
syndrome (PCS). The DoD/VA studies have added con-
fusion to the debate on controls for HBO2trials and have
failed to account for within-group pre- and post-treat-
ment outcomes, biasing analysis and reporting towardthe
conclusion that hyperbaric oxygen is ineffective
for the treatment of symptoms of mTBI and PCS. The
assumption that pressurized air is a sham intervention
has led to erroneous conclusions of non-activity, spe-
cically when the conclusions are due to comparison
between sham and HBO2 treatment as the terminal
decision point [5]. A review of the past literature will
show that this has been a recurring problem and has
led to incorrect conclusions of non-efcacy for HBO2.
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
2/19
X.A. Figueroa, J.K. Wright
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
334
The varied biological effects of both low- and high-
pressure delivery of pure and mixed gases are substan-
tial, with a large literature in experimental and applied
therapies. The current evidence from cell culture,
animal studies, case reports and clinical trials for stroke
and mTBI treatment is consistent with a reparative
effect of HBO2on the nervous system, including low-
pressure air treatments. Furthermore, the overall safety
of this intervention is not called into doubt. The use
of HBO2 for mTBI or PCS should be sanctioned and
given provisional approval under Centers for Medi-
care and Medicaid Services (CMS) coverage with evi-
dence guidelines, as well as for the VA and TRICARE.
Biological effects of hyperbaric oxygen
The human body is sensitive to both decreases and
increases in oxygen levels, brought about by changesin total
oxygen concentration and changes in absolute
pressure. Any change in cellular oxygen concentration
will have potential effects on cellular function. Indeed,
both hypobaric and hyperbaric oxygen can induce pre-
conditioning effects that can protect myocardial and
neural tissue from damaging changes in oxygen tension
[6-11]. HBO2 preconditioning has been used in coro-
nary artery bypass graft surgery and for post-operative
recovery [12-14], reducing cognitive impairments and
neurological sequelae. The application of oxygen under
pressure has been shown to induce reparative mechan-isms in a
number of injury and disease induced con-
ditions.
Understanding the mechanisms that are activated
by HBO2 is essential for applying this clinical tool
correctly. In the last 30 years numerous physiological
and cellular effects of HBO2 have been identied
and elucidated. The effects are varied, occurring
simultaneously, in many cases long-lasting and extensive
in the responses that they elicit.
Stem cell upregulation
In the past 10 years, reports of increased circulating
endothelial progenitor cells in mouse [21] and humans
[22] have shed light on mechanisms stimulated by
HBO2 for wound healing and angiogenesis [23]. In
humans and mice, the process of increased stem cell
release is a nitric oxide (NO) mediated process that
is triggered by HBO2. Animal models of TBI have
effectively shown that angiogenesis and neurogenesis
are increased with HBO2in the injured hemisphere and
are correlated with improvements in performance and
recovery vs. the non-HBO2-treated [24,25]. In adult
cerebral stroke models in rats, neurogenesis via stem
cell migration was seen in the cortex, and the duration
of HBO2 treatment was correlated with recovery of
function [26]. Stem cell migration has been observed
in wound healing clinical studies, ranging from diabetic
foot ulcers [27] to skin wounds [28] that are treated by
HBO2. When the injured brain of those suffering from
PCS, TBI or stroke is considered as a type of wound,
the data supporting a model of stem cell recruitment to
damaged areas of the brain [29] becomes better under-
stood.
SummaryHow stem cell migration aids in the restoration of
func-
tion and symptom alleviation in mTBI is not fully un-
derstood, as there are no direct studies linking these
phenomena together in humans. Possible mechanisms
are a restoration of the vascular network in damaged
or low-ow areas of the brain and repair of dam-
ages axons. Stem cell upregulation is a direct effect
of HBO2 treatment and should be considered as a re-
parative function for acquired brain injuries. HBO2
has the untapped potential as a ready and accessible
source for stem cell recruitment in future therapies.The
mechanism of action remains to be elucidated,
and further work should be done, including studies of
the effect of varied pressures or oxygen concentrations
on stem cell numbers in peripheral blood and tissues.
Modulation of inammatory responses by HBO2
One of the initial responses to a TBI is an increase in
inammation to the brain (in animal models and in
humans). HBO2 has been shown to effectively re-
duce inammatory markers in blast- and blunt force
trauma-induced TBI [30-33]. Mouse models of TBI
have shown that head injuries induce widespread in-
ammatory responses; HBO2 exposure can decrease
apoptosis, reactive neuroinammation [33] and inhib-
its microglial activation and production of pro-inam-
matory cytokines [31]. New evidence suggests that
mild to moderate TBI has a strong inammatory com-
ponent that mediates acute and long-term injury [34].
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
3/19
X.A. Figueroa, J.K. Wright
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
335
The role of HBO2induced vasoconstriction is a well-
known effect in reducing cerebral edema [35,36]. In
clinical research with severe TBI study subjects, HBO2
reduces swelling and intracranial pressure [37,38]
as well as increasing survival. More recent work has
shown that HBO2 reduces the rate and the number
of inltrating neutrophils into injury areas [39-46].
Another effect of HBO2 is its ability to modulate the
sensation of pain. In rat models of neuropathic pain
[47-49], HBO2was able to reduce the pain sensation;
it appears to be a NO-mediated process in mice [48].
In the case of severe traumatic brain injury, inam-
matory markers have been detected months to years
after the TBI incident in humans [50]. A lower level
of inammation may be present in mTBI and PCS
sufferers [34]. The recent discovery of -amyloid
(1-42) and APP increasing after blast-induced braininjury in
animal models [51], and severe brain injury
in humans [52] and the increased risk of Alzheimers
disease and cumulative traumatic encephalopathy with
a history of head trauma [53-56], point to the role of a
chronic inammatory response in mediating long-term
damage in TBI and dementia of the Alzheimers type.
Summary
Inammation is a recognized component of TBIs of all
types. HBO2 has well-established anti-inammatory
capabilities in neuroinammation, suggesting that therole of
HBO2in mTBI and PCS treatment extend much
further than oxygenating tissues. Mixed approaches in
controlling inammation, such as Omega-3 polyunsatu-
rated fatty acid supplementation [57-63] may enhance
recovery and alleviate symptoms of mTBI and PCS,
with adjunct HBO2. Chronic administration of NSAIDs,
specically ibuprofen, have negative correlations with
TBI recovery in animal models [64], but inhibition of
specic inammatory mediators have reparative effects
[65-67].
Cellular repair and protection
Over 8000 known biochemical processes are dependent
on oxygen in the atmosphere to carry out metabolic
processes [68]. Changes in the concentration of oxygen
in the ambient environment, hypoxic or hyperoxic, an
increase due to an elevation in air pressure, supple-
mental oxygen administration or hyperbaric oxygen
will more than likely result in changes in cellular pro-
cesses, some of which may be profound and long lasting.
In the past few years there has been a signicant in-
crease in the scientic understanding of how oxygen
works on a cellular level. Many of these cellular pro-
cesses are signaled by reactive oxygen species (ROS)
[69-72] and others are signaled by oxygen itself [73-76].
Initial exposures to HBO2can induce DNA strand breaks
[77] and increased lipid peroxidation of cell mem-
branes [78], but cellular defenses are activated that
repair and protect from further damage [77]. Although
concerns of overproduction are warranted, most organ-
isms have a wide array of defenses to limit the over-
production of oxygen radical species [79]. Cellular
ROS activity is under tight control and is involved in
cell signaling, protein trafcking and regulation of en-
zyme, receptor, transporter and transcription factors[69]. ROS
produced by HBO2 induce mitochondrial
biogenesis [80] and may play a role in cell repair
and protection from neurological injuries [81].
Additionally each organelle within the cell, including
mitochondria, has different ROS regulation character-
istics that govern the function of each organelle.
Mechanisms associated with repair processes, such as
-integrin b1 receptors mediating collagen synthesis
[69] and DNA methylation (which alters the expression
of genes in cells as they divide and differentiate) affects
gene transcription and are signaled by ROS [69]. ROShave a role
in signaling histone acetylation and deacety-
lation which are also key processes of gene expression
[69] and repair processes. Hyperbaric oxygen adminis-
tration alters the ROS in the cellular environment and
its known mechanisms of action in cellular inamma-
tion, repair and apoptosis regulation are activated [82].
Derangements in ROS regulation and oxidative stress
have been implicated in a variety of neurologic diseases,
including TBI [69]. In TBI, oxidative stress plays a role
in the pathology of neuronal dysfunction, while HBO2
upregulates the neuronal repair processes required to
restore function [83,84]. Furthermore, HBO2 upregu-
lates anti-apoptotic mechanisms (such as the Bcl-2
family of proteins) that protect neuronal cells from
dying [85,86] and help maintain mitochondrial function
[85,87,88]. While it is not known precisely how Bcl-2
signals cellular repair via ROS, while hypoxia-induced
ROS cause inammation and cellular degeneration and
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
4/19
336
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
X.A. Figueroa, J.K. Wright
apoptosis, it is theorized that the changes in cellular
oxygen levels, and hence ROS (termed oxygen cy-
cling) cause a perceived hypoxia by the cell which
in turn signals repair processes in the presence of ade-
quate oxygen levels for the repair to proceed [84].
It appears that it is not the actual level of oxygen
present, but the difference in the homeostatic equilib-
rium of oxygen that is sensed and the same ROS that
are produced when the equilibrium swings too far from
the set-point. The ROS act as signaling agents, inde-
pendent of hypoxic, normoxic or hyperoxic states, but
the context of the signaling (the actual level of oxygen)
may mediate the activation of context specic mech-
anisms that interpret the ROS signaling.
Summary
HBO2-produced ROS are mitigated by the cells abilityto quench
ROS overproduction. HBO2activates numer-
ous cellular mechanisms of action which are neuro-
protective and assist the injured brain to heal. The
effects are broad and protective at the cellular level,
including protection of mitochondrial potential [85,87,
88]. Furthermore, the anti-apoptotic proteins, Bcl-2 and
Bcl-xL, are upregulated in neurons in contusion models
of rats after HBO2exposure and the downstream effects
that these proteins exert to inhibit apoptosis [89].
Cellular oxygen utilization: mitochondrialregulation and idling
neurons
Disruption or reduction of mitochondrial activity in
nervous tissue is a reported effect of stroke [90-92] and
TBI [93]. In the case of TBI, the deregulation of mito-
chondrial activity is complex and can lead to changes
in metabolic function [37,93-96] and changes in blood
ow [97]. HBO2 has shown the ability to restore
mitochondrial activity in animal models of TBI [80,
85,87,88,96,98,99]. In the case of blast-induced TBI,
cerebral blood ow and metabolic function were
shown to improve after HBO2in a rabbit model [30].
The hypothesis of hypometabolic neural tissue in a
penumbra or an area of idling neurons in brain in-
jury was promulgated by Dr. Neubauer [100-102], but
was considered untested, mostly due to a lack of an es-
tablished mechanism for neural tissue entering into a
state of hibernation. The evidence of neural tissue that
can be rescued is supported by recovery of function
(neurological testing, EEG or SPECT) in stroke studies
that used HBO2 to detect brain tissue that was viable
in post-acute stroke with 10-15 HBO2 treatments [103]
or even a single HBO2 treatment [104]. Another case
report of post-acute stroke patients treated with HBO2
and imaged with single photon emission computer
tomography (SPECT), reported improved neurological
function [105] and increased regional cerebral blood
ow (rCBF) in the penumbra of the affected region.
The development of diffusion tensor imaging of the
brain in concussion patients appears to validate the
presence of a penumbra of non-functional damaged
axons after injury [106]. These studies help to further
validate the improved outcomes (National Institutes
of Health Stroke Scale, NIHSS; activities of daily
living, ADL; evaluation of quality of life, EQ) of
the recent post-acute stroke recovery study usingHBO2 by Efrati,
et al. [107] and buttress the case
for reactivation of hypometabolic neural tissue.
The landmark studies of Blackstone, et al. [108,109]
were the rst to provide a plausible mechanism for
idling neurons. Blackstone, et al. demonstrated the
ability to downregulate mitochondrial respiration by
simultaneously exposing mice to gaseous H2S and re-
ducing oxygen levels. Not only did the mice survive
periods of reduced oxygen tension of > 6 hour at 5%
oxygen, there was no measurable neurological or myo-
cardial damage when they were restored to normal oxy-gen levels
and metabolic function [108, 109]. The exact
mechanism of neural tissue protection remains unestab-
lished, but the principle is present for future investiga-
tion. Furthermore, the discovery of a hydrogen sulde
(H2S) mechanism modulating long-term potentiation
(LTP) in neurons [110] suggests that this signaling gas
is an integral and conserved mechanism in mammals
[111-115]. From a mechanism perspective, enzymatic
systems in mammalian neural tissues produce H2S
locally and could induce a local hypometabolic state by
direct regulation of mitochondrial activity [116-120].
Summary
The hypothesis that neurons can remain viable but not
electrically active after a traumatic brain injury is sup-
ported by SPECT imaging of TBI patients in the post-
acute phase. Individuals diagnosed with a TBI pres-
ent with reduced rCBF [121,122] when compared to a
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
5/19
337
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
X.A. Figueroa, J.K. Wright
healthy, non-injured population. Diffusion tensor im-
aging in traumatic brain injury provides an anatomic
picture of idling neurons with loss of axonal integrity
demonstrable for years after injury [123]. The effects
of axonal remyelination after chronic TBI using HBO2
saw a signicant restoration of axonal tracts and motor
improvements in rats [124]. Restoration or elevation of
rCBF is seen with HBO2 treatment of TBI study par-
ticipants [125,126] with a concomitant improvement
in cognitive function and symptom improvement in
bomb-blast-induced and study subjects (civilian and
veterans). The existence of hypometabolic neural
tissue provides a plausible mechanism for the recovery
of function seen in both clinical TBI and stroke studies
that tested HBO2 as a treatment. Although the exact
mechanisms for reactivation are not elucidated, it appears
that increases from the 5% to 21% oxygen concentrationcan have
an effect on the mitochondria of hypometabolic
neural tissue, restoring them to baseline function [108,
109].
The unintended oxygen dosing trials
In the literature, a sham in HBO2 (room air at 1.1-1.4
atmospheres absolute/atm abs) has been commonly
used as a comparator against a treatment dose ( 1.5 atm
abs, 100% oxygen). Yet, the sham remains a point of
contention within the hyperbaric medical research
eld. By denition HBO2is a two component therapy:increased
pressure and increased oxygen concentration.
A sham, as established for all clinical trial interven-
tions, is a treatment or procedure that is performed as
a control and which is similar to but omits a key thera-
peutic element of the treatment or procedure under
investigation. Therefore, controlling the oxygen con-
centration (keeping oxygen at a level equivalent to 21%
at sea level) is essential to developing a sham that
controls for oxygen. To effectively create a sham for
a treatment of 100% oxygen at 1.5 atm abs would
require a breathing mixture of 14% oxygen (and the
remainder presumably nitrogen) delivered at 1.5 atm
abs. This would deliver an oxygen equivalent dose to
21% oxygen breathed at sea level (1.0 atm abs) but
would also deliver an increased dose of nitrogen which
could have biological effects. Use of pressurized air at
1.2 to 1.3 atm abs would not be a true sham treatment
for oxygen, as the subjects would be breathing a 20%-
30% increase in oxygen than that breathed at sea level.
This increase in oxygen (and also possibly the nitrogen
increase) would be expected to have cellular effects.
Pressurized air shams are not inactive. In actuality the
use of pressurized air in studies of hyperbaric oxygen
treatments constitutes a dosing trial rather than a sham.
The issue facing hyperbaric medical research boils
down to dening what constitutes a medically relevant
dose of oxygen and fully understanding the biology of
oxygen. Changes in air pressure smaller than 0.1 atm abs
have induced growth factor production and an increase
in cell division [129] in epithelial cell cultures when
compared to the control cultures. Studies of smooth
muscle cells derived from the human aorta reported
that 1.1 atm abs of room air (an increase of 0.1 atm
abs) was sufcient to increase growth rates [130,131].
Cells (as demonstrated in vitro) detect minute change inoxygen
concentration (up or down) and the 20%-30%
increase in dissolved oxygen concentration in reported
shams as comparators in HBO2 trials represent a
therapeutic dose.
The cell culture data is supported by evidence from
studies of lung function and oxygenation with chronic
obstructive pulmonary disease, cystic brosis, pulmo-
nary brosis and pulmonary hypertension (thromboem-
bolic). Moving patients from cities located 800 meters
above sea level (0.91 atm abs, ~21% oxygen) to loca-
tions 400 meters below sea-level (1.05 atm abs, ~21%oxygen)
improved oxygenation and lung function
[132,133]. In a presentation of pilot study data looking
at the effects of scuba diving on veterans diagnosed with
post-traumatic stress disorder (PTSD), a large reduction
(~80%) in PTSD symptoms (PCL-M) was observed
[134], with pressure ranges from 1.3 to 1.5 atm abs
with nitrox (32%-36% oxygen/68%-64% nitrogen) sus-
tained while diving. The sham in the Wolf, et al. [4]
report dissolved ~30% more oxygen into the plasma
than just breathing room air at 1.0 atm abs, inducing
a signicant change in symptoms scores (IMPACT
symptoms score and the PCL-M), which are in agree-
ment with Kaplin, et al. [134], and the HOPPS trial
[135] results, both of which reported a therapeutic
effect of breathing pressurized air.
Illustrative of the sham issues are two published
studies by Anderson, et al. [5] and Nighoghossian, et al.
[136]. Both papers were designed as double-blind
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
6/19
338
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
X.A. Figueroa, J.K. Wright
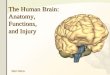
HBO2 (1.5 atm abs, 100% oxygen) vs. air sham cere-bral stroke
studies. The air sham showed an equivalent
effect when compared to HBO2 in the Anderson, et al.
study (Figure 1, left graph: Air: Nstart=19, Nend=11;
HBO2: Nstart=20, Nend=14), while Nighoghossian, et al.
reported statistically signicant results between the
sham and the HBO2 treatment, with the sham show-
ing superior improvement in two out of three measures
(Figure 1, right graph). Lower scores on the Orgogozo
and Rankin scales and higher scores on the Trouillas
scale are measures of better outcomes (N=17; both
groups; Figure 1, left graphs). In both studies it wasassumed
that the shams would not be biologically
active. The authors compared HBO2 treatment to the
supposed inactive sham, resulting in an invalid
analysis. Re-examination of the pre- and post-neuro-
logical scores revealed statistically signicant differ-
ences in both groups (before vs. after treatment)
using a two-tailed T-test (=0.05, Figure 1). Had a
third comparator been included, such as a standard
of care group, the analysis and conclusions would
likely have been markedly different.
The use of an air sham requires the assumption of
inactivity of the sham [137], but with sham treatments
consistently showing better results than higher treat-
ment pressures (100% oxygen, 1.14 atm abs vs. 2.5 atm
abs; Figure 2 [left side]) the sham treatment shows
biological activity. Outcomes at 90 days involved four
stroke scales with good outcomes dened as follows:
Reanalysis of pre- and post-HBO2therapy measures of sham vs.
HBO2treatment in stroke study participants. Left box:
Anderson, et al. study. Right box: Nighoghossian, et al. Columns
are final mean values. Error bars are standard deviations.
__________________________________________________________________________________________________________________________________________________________
Figure 1
Pre-HBO2Post-HBO2
1.5 atm abs 1.5 atm abs
1.2 atm abs 1.5 atm abs 1.2 atm abs 1.5 atm abs 1.2 atm abs 1.5
atm abs
an NIHSS score 1; a Barthel Index score of 95 or 100;
a modied Rankin Scale score 1; and
a Glasgow Outcome Scale score of 5
(Nsham=11; NHBO2=16).
Lacking in the Rusyniak, et al. study [137] was a com-
parator for standard of care (SoC). As can be compared
in Figure 2 (right side), published results [138,139]
of non-related studies (using the same post-stroke
outcome denition criteria as Rusyniak, et al.) give
a clear indication that air shams are not inactive, and
higher pressures of oxygen are not necessarily betterfor
treatment in post-acute stroke. Some of the problems
in selecting an appropriate sham or control in a hyper-
baric oxygen trial are illustrated in Table 1.
Summary
Pressurized air is not inactive, and comparison between
different pressure regimes suggest that a dose response
to neuronal healing is present with different levels of
oxygen concentration and pressure. The 2.5-atm abs
(at 100% oxygen) treatments appear to have very little
effect when compared to standard of care (Figure 2),
but mild pressurization (1.14 atm abs, 100% oxygen)
appears to have an equivalent clinical response as tPA
therapy for stroke and a superior response than 2.5 atm
abs It is no surprise that subsequent DoD/VA spon-
sored reports [1,2] used a different control group: An
oxygen sham that controlled for oxygen concentration
(10.5% O2 at 2.0 atm abs=21% oxygen equivalent).
neurologic
score
Anderson, et al. Orgogozo RankinTrouillas
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
7/19
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
339X.A. Figueroa, J.K. Wright
Graph of pre- and post-HBO2therapy measures of sham (1.14 atm
abs, 100% oxygen) vs. 2.5 atm abs in stroke study
participants (left graph) Columns are the end mean values.
Standard of care for stroke and of tPA intervention (right
graph).
__________________________________________________________________________________________________________________________________________________________
Figure 2
1.14 atm abs
2.5 atm abs
___________________________________________________________________________________________________________________________________________________________
Table 1
type of control purported effect advantage(s) disadvantage(s)
potential error as
control___________________________________________________________________________________________________________________________________________________________
pressurized air at no oxygen effect allows for pressure effect
increased concentration ignores cellular effects of
1.2-1.5 atm abs in experimental subjects of oxygen and nitrogen
increased oxygen and nitrogen
have biological effects
concentration___________________________________________________________________________________________________________________________________________________________
no treatment none allows for monitoring subjects may experience
enrolling in a study may have
observation at rare subjects with minimal Hawthorne effect a
treatment effect intervals placebo or Hawthorne
effect___________________________________________________________________________________________________________________________________________________________
pressurization with mixed none for oxygen control oxygen
concentration pressure effects, regular participation in study
gas to give room air at room air (1 atm abs) increased nitrogen
protocol, increased nitrogen
(1 atm abs) equivalent equivalent effects, placebo and
concentration may have an
oxygen concentration Hawthorne effects
effect___________________________________________________________________________________________________________________________________________________________
delay in treatment/ none during delay all participants can be
subjects may improve subjects may change for
crossover study offered HBO2therapy or deteriorate during better
or worse during delay
delay, placebo and and differ from treatment
Hawthorne effects may group
be operational during
delay___________________________________________________________________________________________________________________________________________________________
historical controls none allows for monitoring the data may be
insufficient
untreated course of the and too varied for
disease adequate comparison,
no possibility of measuring
placebo or Hawthorne
effects___________________________________________________________________________________________________________________________________________________________
standard of care healing through allows comparison with standard
of care may not excludes intervention, placebo
supportive therapy historical data and comparison actually be
therapeutic and Hawthorne effects
or accepted standard with new treatments
therapy___________________________________________________________________________________________________________________________________________________________
Comparison of different controls used in HBO2clinical trials for
TBI/PCS and PTSD.
p=0.11 p=0.02 p=0.01 p=0.04
percentagepfparticipants
with
goodoutcomemeasures
Barthel Modified Glasgow NIHHS Barthel Modified NIHHS
Index Rankin Outcome Index Rankin
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
8/19
340
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
X.A. Figueroa, J.K. Wright
Reinterpreting the DoD/VA results
The single DoD/VA sponsored clinical trial by Cifu,
et al. was a three-arm design [1,2] and reported on
one group of Marines (N=61). Study participant were
randomized into three different treatments groups
(2.0 atm abs: 10.5% oxygen, 75% oxygen and 100%
oxygen), with participants and researchers blinded to
treatment. The participants were given the exact same
pressure (2.0 atm abs) but given different oxygen mix-
tures to simulate different treatments: 21% oxygen;
1.5 atm abs at 100% oxygen; 2.0 atm abs at 100% oxy-
gen. The two primary measures they looked at were
the Rivermead Post-Concussion Questionnaire (RPQ)
and the PTSD Checklist Military Version (PCL-M).
In each of the articles by Cifu, et al. [1,2], the con-
clusions were that there was no effect from HBO2,
partially contradicting the reported results from the
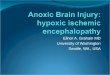
Wolf, et al. study [4]. The Wolf, et al. study reports a
statistically signicant effect with hyperbaric air (1.3
atm abs, 21% oxygen). The effects were large in the
Wolf, et al. publication (41% difference between pre-
and post-testing on the RPQ, Figure 3), but they were
not reported as signicant in the aggregate scores,
although nine symptoms showed signicant differenc-
es in the sham treatment group (Figure 3). The PCL-
M scores are also very close in overall effect between
pre- and post-treatment: 16% improvement in the Wolf
__________________________________________________________________________________________________________________________________________________________
Figure 3
Pre-HBO2Post-HBO2
Wolf, et al.
Meansymptoms
core
Cifu, et al. Harch, et al.
sham
2.4atm
sham
2.4atm
10.5
%
75%
100%
10.5
%
75%
100%
1.4atm
1.5atm
RPQ PTSD RPQ PTSD RPQ PTSD
Cross-study analysis of results from the Rivermead
Post-Concussion Questionnaire (RPQ) and the PTSD Checklist-Military
Version
(PCL-M). Wolf: Nsham=24, NHBO2=24; Cifu: N10.5%= 21, N75%= 18,
N100%=21; Harch: N=16. *= p 0.05; ?=unreported value of P.
study and 14% in the Cifu study. The Cifu, et al. studies
conclude that the results were clinically non-signicant,
but the aggregate PCL-M scores were statistically sig-
nicant, just like in the Wolf, et al. study (see Figure 3).
The lack of change in the RPQ and PCL-M scores
in the sham and 1.5 atm abs equivalent groups for
the Cifu study could be due to insufcient number
of study participants, the use of paper and pencil vs.
computerized testing (time variations in response times
are subject to analysis in computer tests), subject
selection (all Marines were in a Warrior Transition
Unit) or other external factors associated with study
location. The Wolf, et al. study had six and three more
study participants per group, respectively (N=24 for
both the sham and 2.4 atm abs groups) than the Cifu
study (N=18 for the 75% oxygen and N=21 for the
100% group). Given how close the results were be-
tween both studies, the addition of six and three more
study participants by the Wolf, et al. study could ex-
plain the difference seen between both articles. The Cifu
et al. studies [1,2] also appears to have been under-
powered, a point they acknowledge in their publication.
Another factor at play is the relatively high pressures
used by the DoD/VA sponsored studies [1,2,4]. Global-
ly, a consensus is building for the use of lower pressure
treatments, ideally 1.5 atm abs or lower, for central
nervous system injuries. For the DoD/VA sponsored
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
9/19
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
341X.A. Figueroa, J.K. Wright
studies [1,2,4], the HBO2 intervention doses were
at or above 2.0 atm abs in pressure. The lower sham
treatment [4] was much closer to the ideal pressure
that proponents of HBO2normally use for neurological
treatments [125,126,140,141].
The improvements measured for RPQ and PCL-M
outcomes in the Wolf and Cifu studies are in agreement
with another published report by Harch, et al. [126].
Harch, et al. reported on the treatment of 16 Marines
with bomb-blast-induced mild TBIs (mTBI) and pro-
duced results that were in agreement with the DoD/VA
sponsored study results [1,2,4], if not their conclusions
(Figure 3). The conclusion of Cifu, et al. that HBO2 is
ineffective on mTBI is not supported by the data they
acquired. All three studies measured statistically signi-
cant improvements in the PCL-M scores [1,3,126] and
are in agreement with previously published outcomes
[142] in case reports of HBO2 reducing PTSD symp-
toms. The overall trend between the published studies
using HBO2 as an intervention on chronic mTBI/PCS
favors a clinically positive outcome with HBO2 treat-
ment across a variety of measures. Adding to this dis-
cussion is a presentation of an Army study, HOPPS
[135] (Clinicaltrials.gov, NCT01306968). The HOPPS
study (Hyperbaric Oxygen Therapy for Persistent Post-
Concussive Symptoms) saw a statistically and clinically
__________________________________________________________________________________________________________________________________________________________
Figure 4
SoC N = 23
1.5 atm N = 24
sham N = 25
SoC
1.5atm
sham
SoC
1.5atm
sham
SoC 1.5 atm sham
Result of HOPPS study. (Left side) RPQ and PCL-M (PTSD) results
compared to standard of care (SoC), 1.5 atm abs
(100% oxygen) and sham (1.3 atm abs, 21% oxygen). PTSD scores
that exceed 8 points (*C) are considered clinically
significant.
(Right side) The results of the health survey (SF36) of HOPPS
study.
RPQ PTSD
signicant improvement six months post-treatment
in the Rivermead Symptoms Questionnaire (RPQ;
p< 0.05) and PCL-M scores (*C; >8 point improvement;
Figure 4). Six-month post treatment measures (using
the Short Form Health Survey [143]) revealed that im-
provements were greater than standard of care (SoC),
but it also saw a graded improvement between sham
and HBO2 treatments. The sham produced results
equivalent to or better than the 1.5 atm abs treatments.
HOPPS has a one-year follow-up to perform and other
measures, such as cognitive, neurological and psycho-
motor outcomes remain to be reported, but based on
previous clinical experience with TBI and PCS sufferers
we expect the one-year follow-up results to retain
their signicance.
Relevant to our discussion regarding the use of
HBO2for neurological injuries is the necessity to ensure
that studies use a well-controlled population of study
subjects. The Churchill, et al. study [144] tested a
mixed population of acquired brain injury study subjects
(ABI; stroke, anoxia and trauma) and saw a mix of posi-
tive and inconclusive results. The TBI population was
skewed toward the severe TBI category (21/27), with
six study subjects in the mild-to-moderate TBI category
(Figure 4, top graph). Illustrative of the difculties in
testing a heterogeneous ABI population are the Wechsler
Short Form Health Survey (SF36)HOPPS
pointimprovement
fromb
aseline
unfavorable
favorable
14
12
10
8
6
4
2
0
20
15
10
5
0
-5
-10
-15
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
10/19
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
X.A. Figueroa, J.K. Wright342
Abbreviated Scale of Intelligence (WASI: Figure 5,
bottom graph) scores. Although the WASI reported
signicant improvements in aggregate, when broken
down by groups (TBI, stroke and anoxia), only theTBI and stroke
showed statistically signicant changes
(Figure 4, bottom graphs). The anoxia group saw no
statistically signicant improvements using the WASI.
Further testing via other parameters produced results
that were, at best, difcult to interpret. Although there
is a temptation to conclude that HYBOBI (hyper-
baric oxygen therapy in chronic stable brain injury;
NCT00830453) is another publication pointing to the
failure of HBO2 for treating neurological conditions,
we would agree with the authors concluding remarks:
Many clinical trials incorporate patient reported
outcomes, but future studies should use a standard-
ized brain injury symptom questionnaire that has
been robustly validated in the population of interest
[underline is ours]. Unfortunately, such a measure,
validated across all brain injury etiologies and
severities, was not available for this study.
Dening the population that will be treated and grading
the injury level are important steps in assessing and
validating the effectiveness of a therapy.
Summary
The DoD/VA sponsored studies [1,2,4] reached conclu-
sions that were technically correct, but failed to recog-
nize the clinical relevance in the pre- and post-treatment
values; one study [4] relied on the difference between
treatment groups and a questionable sham intervention
to reach a questionable conclusion. Published case
reports and clinical studies that have utilized HBO2as
an intervention in mild to moderate TBI and PCS have
shown consistent positive results [125,126,141,145,
146]. The conclusions of the DoD/VA sponsored tri-
als received the widest media coverage [147], giv-
ing the impression to the public and general medicine
that HBO2 was ineffective for the treatment of mTBI/
PCS. In reality, the DoD/VA study results provid-
ed a boon to HBO2 clinical research at many levels.
__________________________________________________________________________________________________________________________________________________________
Figure 5
Graphical representation of HYBOBI results. Top graph,
distribution of acquired brain injuries.
Bottom graphs, WASI intelligence scores divided by injury type.
P-values are pre- and post-HBO 2analysis at six months.
WechslerAbbreviated
Scale
ofIntelligence
numberofstudy
participants
Pre-HBO2
Post-HBO2
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
11/19
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
X.A. Figueroa, J.K. Wright 343
The missing placebo
The placebo effect is a well-recognized component of
medical treatment, sometimes superseding the effects
of the actual treatment [148-152]. Controls are an es-
sential component of clinical trials, but sometimes the
use of specic controls (a sham or placebo) is just not
feasible or too costly to set up (especially with HBO2).
Placebos are not always used (cancer studies compare
new drugs or procedures against standard of care) and
comparing pre- and post-treatment measures (including
crossover designs), although not deemed the most
stringent, are acceptable and valuable in medicine
[153]. As we have discussed above, the use of a non-
validated sham (pressurized air) in many of the previ-
ous HBO2 studies have clouded the debate regarding
HBO2 effects and efcacy for neurological injuries.
The assumption of a placebo effect with studies thatused
pressurized air as a sham control is awed. Using
a comparator that has biological activity equal to the
treatment group is not a sham or a placebo: It is a bad
study design.
Although poorly controlled, some useful results can
be extracted from existing studies. An example is
the magnitude of the placebo effect in HBO2 studies.
Unreported in the discussions of the Cifu, et al. publi-
cations [1,2] was the lack of any measurable placebo
or Hawthorne effect in the 2.0 atm abs, 10.5% oxygen
group (the 21% oxygen equivalent; Figure 3). TheCifu, et al.
study demonstrated that being in the pres-
ence of a hyperbaric chamber and sensing an increase
in pressure did not induce a placebo effect in their
21% oxygen equivalent sham group (Figure 3). The
increased attention by the study technician and doctors
did not produce a Hawthorne effect on the study par-
ticipants. On the contrary:
...we found that the sham and the 1.5 ATA
equivalent groups demonstrated nonsignicant
[underline is ours] ... (worsening) in their raw
total RPQ scores... (P.18) [2]
The 2.0 atm abs, 10.5% oxygen group did not produce
any statistically signicant changes in the RPQ or
PTSD scores (placebo or nocebo) from baseline
measures, as would be expected when simulating a
21% oxygen equivalent.
In lieu of this analysis, a serious reconsideration of
the published literature must occur. Previous studies that
have a crossover design, that compare pre- and post-
treatment measures and have avoided the sham assump-
tion (using compressed air at 1.14-1.5 atm abs) should
be given equal consideration when analyzed side by
side with the sham or placebo controlled studies. The
assumption that pressurized air has negligible or no
biological activity is refuted by cell culture, animal
studies and clinical reports. The requirement for a sham
control is an important component for clinical trials,
but the absolute requirement for a sham should be
tempered by the results of previous trials, the realiza-
tion that pressurized air is biologically active and the
inclusion of other controls (such as standard of care).
Taken as a whole, these results support the idea that we
are witnessing a real and powerful neurological repair/
reactivation mechanism for mTBI with oxygen, even
under low positive-pressure room air.
Summary
The result from the rst DoD/VA study [4] must be
viewed as an early entry in the arena of low-pressure
therapy results, as the sham group is not a true sham.
The results from the other DoD/VA sponsored stud-
ies [1,2], highlight the lack of a measurable placebo/
Hawthorne effect and the ability of HBO2 to improve
PTSD symptoms in blast-induced PCS. The HOPPS
study [135] supports the results of the Wolf, et al. study
[4] and the other published HBO2outcome for
TBI/PCS[125,126,141,145,146]. Pressurized air (1.3 stm abs,
21% oxygen) can produce a treatment response that
improves measured outcomes in TBI/PCS and PTSD
symptoms and is superior to standard of care for
TBI/PCS [135].
The urgency of now
A large fraction of the current epidemic of active duty
U.S. military suicides (22+ service members a day take
their lives, 44 attempt suicide) [154] is possibly due to
misdiagnosing the military TBI population with PTSD
or failing to appropriately diagnose other mental health
conditions [155]. In the civilian population as well, the
issue of misdiagnosis of TBI as PTSD is similar to that
for the U.S. military [156]. The DoD and VA have spent
at least $9.2 billion since 2010 [157] treating PTSD
but have been unable to stem the epidemic of suicide
and mental illness in veterans. Drug interventions are
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
12/19
344
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
X.A. Figueroa, J.K. Wright
inadequate, and studies continue to nd that pharmaco-
logical interventions are not effective in treating the
symptoms of TBI or PTSD [158-160]. Many cases of
veteran suicide have been linked to prescribed medi-
cation [161,162].
Currently, the debate regarding the utility of HBO2for
treating mTBI, PCS or PTSD is mired in controversy. At
the heart of this controversy is a simple question:
Does it work?
Based on information from case reports and phase I
studies HBO2 does work as a therapy for mTBI/PCS
and PTSD as they are currently diagnosed. None of
the prescribed therapies for mTBI or PCS for service
members (or civilians) has undergone a phase III RCT.
Currently, the best that medicine and therapy can offer
is the chance for a new normal, a term that is utilized
in rehabilitation to inform those with a brain injury that
they have to live with lower expectations and abilities.
For individuals who are living with a chronic brain
injury and surviving the symptoms, being told that they
need to adapt to reduced abilities can be a demoralizing
diagnosis. The literature in English for mTBI, PCS and
PTSD case reports and clinical trials has the weight of
evidence in favor of HBO2 having a reparative
effect (Table 2).
Realistically, not all patients will benet from HBO2.
Yet, is it worthwhile to consider HBO2 as a therapy
for mTBI/PCS if it can improve the lives of 10%, 25%
or 50% of affected individuals? Would a new new
normal that is, 25%-50% better than the old new
normal be worth the effort? At what point will the
general medical community draw the line for the
potential treatment of more than 5 million Americans?
The fundamental questions that should be asked by
physicians are the following:
1. Who are the most likely candidates to benet
from HBO2?
2. What are the minimum treatments that can elicit
a clinically relevant improvement?
_____________________________________________________________________________________________________________________________________
Table 2
authors year Dx symptoms neurocog pre-/post- between type of #
of sham HBO2 HBO2 # of time since tests HBO2 tests design arms
press. press. dives subj. injury
A75% O2 100% O2 totalB10.5% O2
C(Med
Air)_____________________________________________________________________________________________________________________________________
Eovaldi, et al. 2005 PTSD yes N/A N/A N/A pre- to post- 1 N/A
2.4 atm 7 1 4
days_____________________________________________________________________________________________________________________________________
Hardy, et al. 2007 mTBI yes yes yes N/A pre- to post- 1 N/A 2 atm
20/60 1 12 mos.
_____________________________________________________________________________________________________________________________________
Lin, et al. 2008 SoCno N/A N/A SoCno yes RCT w/ 2 N/A 1.5 atm
22/22
/yes /yes SoC grp.
(44)_____________________________________________________________________________________________________________________________________
Wright et al. 2009 mTBI yes yes yes N/A pre- to post- 1 N/A 1.5 atm
40 2 8 mos.
_____________________________________________________________________________________________________________________________________
Harch et al. 2009 mTBI yes yes yes N/A pre- to post- 1 N/A 1.5 atm
40 1
_____________________________________________________________________________________________________________________________________
Harch et al. 2009 mTBI yes yes yes N/A pre- to post- 1 N/A 1.5 atm
40 12 ~ 2 yrs.
_____________________________________________________________________________________________________________________________________
Stoller et al. 2011 mTBI yes yes yes N/A pre- to post- 1 N/A 1.5
atm 40 3 3 mos./20 yrs.
_____________________________________________________________________________________________________________________________________
HOPPS 2012 PCS SoCno/ N/A SoCno/ SoCyes/ RCT w/sham 3 C1.5 atm 1.5
atm 40 23/24 ~ 2 yrs.
Ayes/yes Ayes/yes Ano/no /SoC /25
(72)_____________________________________________________________________________________________________________________________________
Wolf et al. 2012 PCS *no *no *no *no RCT w/ 2 C1.3 atm 2.4 atm 30
24/24 3-71 mos.
sham (48)
_____________________________________________________________________________________________________________________________________
Boussi- 2013 mTBI yes/no yes/no yes/no yes//no crossover 2 N.A 1.5
atm 40 32/24 ~34.6 mos./
Gross, et al. //yes //yes //yes //24 (56) ~31.7
mos._____________________________________________________________________________________________________________________________________
Cifu et al.+ 2013 PCS Bno/Ano/ Bno/Ano/ Bno/Ano/ Bno/Ano/ RCT w/ 3
B2 atm/ 2 atm 40 B21/A18 ~8.5 mos.
Walker et al. no* no* no* no sham A2 atm/ /21
(60)_____________________________________________________________________________________________________________________________________
Filled light-grey cells are for reports of positive outcomes
with HBO2. Dark-grey cells are for outcome with no discernible
change.
SoC = standard of care. Starred outcomes (*) for Symptoms,
Neurocog Tests, Pre-/Post-HBO2and Between Groups are for stud-
ies that concluded no significant result, but statistical
analysis contradicts conclusion with results that are statistically
significant
between pre- and post-testing within groups.
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
13/19
345
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
X.A. Figueroa, J.K. Wright
3. What combination of treatments can produce
the maximum improvement?
Ideally, a set of RCTs with true shams and standard of
care comparators will settle this long-standing issue.
But we are far from the ideal. People with an mTBI or
PCS need treatment now. Given the published super-
iority of HBO2over the standard of care (in a military
and civilian population), HBO2 should be covered
or given provisional approval. If, in the future, the
medical community can replicate the presumptive
placebo effect induced by HBO2 chambers and fa-
cilities, this can become the standard of care.
The contradictory outcomes from published HBO2
studies have muddied the waters and added to the con-
fusion of clinically relevant results. Replication of
results remains difcult to accomplish with the ob-
stacles of cost, ill-dened controls and non-standardassessment
scales. HBO2is not a eld known for deep
research pockets, industrial/academic collaboration or
a dedicated budget from the Federal government for
research. Clinical trials in diffuse neurological injuries
are attempts at placing parameters on complex medical
cases with varied history of injury, genetic background,
nutritional variations, socioeconomic factors and previ-
ous attempts at medical intervention. There is no single
standard for testing recovery in a general TBI popula-
tion, the ideal measure of efcacy being the return to a
productive life for the study subjects and the
long-termcessation of brain injury sequelae. For the majority
of
HBO2 studies approximations vs. replications of the
trials are par for the course. Variations are to be
expected with the current low number of subjects
recruited in U.S., Israeli, Taiwanese and Chinese
HBO2studies on TBI recovery.
The Wolf, et al. [4], Cifu, et al. [1,2] and Army [143]
results have added to the growing database of effects
that HBO2 has on neurological injuries. These are ac-
complishments that should be roundly applauded and
commended. We do, however, disagree with the con-
clusions reached by the authors and their interpretation
of their results. We urge the UHMS Committee to grant
preliminary approval for the use of HBO2 in the treat-
ment of chronic mild to moderate TBI/PCS. Given the
history of using non-validated shams and the emerging
data comparing HBO2 to standard of care, HBO2has a
superior outcome in phase I studies. The clinical reality
is stark: currently there are no treatments that can im-
prove symptom and cognitive performance for chronic
mild to moderate TBI or PCS, especially one year or
longer from the time of injury. HBO2 is safe, with few
side effects, has durable treatment outcomes, has avail-ability
in many metropolitan centers and is managed
by both hospital-based and independent clinics. The
evidence for improving long-term symptoms (includ-
ing PTSD symptoms) and cognitive performance is
substantial in this regard. Approval of HBO2 on a
tentative basis would allow for the collection of
results in a large patient population, and we recom-
mend this be done. Even if some of the improvement
seen could be attributed to placebo or Hawthorne
effects, it is still durable and should be considered
treatment. No other intervention can offer these resultsor this
degree of hope for the mTBI/PCS patient. HBO2
should be part of the approved treatment armamen-
tarium, along with other appropriate and proven thera-
pies, for mild to moderate TBI and PCS in civilian,
active-duty and veteran populations.
Conict of interest
The authors report no conict of interest with this
submission. n
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
14/19
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
346 X.A. Figueroa, J.K. Wright
1. Cifu DX, et al. Hyperbaric oxygen for blast-related
postconcussion syndrome: Three-month outcomes. Ann
Neurol, 2014. 75(2): p. 277-286.
2. Cifu DX, et al. The effect of hyperbaric oxygen onpersistent
postconcussion symptoms. J Head Trauma
Rehabil, 2014. 29(1): p. 11-20.
3. Walker WC, et al. Randomized, sham-controlled,
feasibility trial of hyperbaric oxygen for service members
with postconcussion syndrome: cognitive and psychomotor
outcomes 1 week postintervention. Neurorehabil Neural
Repair, 2013.
4. Wolf G, et al. The effect of hyperbaric oxygen on symp-
toms after mild traumatic brain injury. J Neurotrauma, 2012.
29(17): p. 2606-2612.
5. Anderson DC, et al. A pilot study of hyperbaric oxygen
in the treatment of human stroke. Stroke, 1991. 22(9):
p.1137-42.
6. Stetler RA, et al. Preconditioning provides neuro-
protection in models of CNS disease: Paradigms and clinical
signicance. Prog Neurobiol, 2014.
7. Soejima Y, et al. Hyperbaric oxygen preconditioning
attenuates hyperglycemia-enhanced hemorrhagic trans-
formation by inhibiting matrix metalloproteinases in focal
cerebral ischemia in rats. Experimental Neurology, 2013.
247: p. 737-743.
8. Zeng Y, et al. Hyperbaric oxygen preconditioning
protects cortical neurons against oxygen-glucose deprivation
injury: role of peroxisome proliferator-activated receptor-
gamma. Brain Res, 2012. 1452: p. 140-150.
9. Li Z, et al. Mechanism of hyperbaric oxygen precondi-
tioning in neonatal hypoxia-ischemia rat model. Brain Res,
2008. 1196: p. 151-156.
10. Gu GJ, et al., Mechanism of ischemic tolerance induced
by hyperbaric oxygen preconditioning involves upregulation
of hypoxia-inducible factor-1alpha and erythropoietin in
rats.
J Appl Physiol, 2008. 104(4): p. 1185-1191.
11. Freiberger JJ, et al. A comparison of hyperbaric oxygen
versus hypoxic cerebral preconditioning in neonatal rats.
Brain Res, 2006. 1075(1): p. 213-222.
12. Li Y, et al. Preconditioning with repeated hyperbaricoxygen
induces myocardial and cerebral protection in
patients undergoing coronary artery bypass graft surgery:
a prospective, randomized, controlled clinical trial.
J Cardiothorac Vasc Anesth, 2011. 25(6): p. 908-916.
13. Jeysen ZY, et al. Research report: the effects of
hyperbaric oxygen preconditioning on myocardial
biomarkers of cardioprotection in patients having coronary
artery bypass graft surgery. Undersea Hyperb Med, 2011.
38(3): p. 175-185.
14. Yogaratnam JZ, et al.,Hyperbaric oxygen precondition-
ing improves myocardial function, reduces length of
intensive care stay, and limits complications post
coronaryartery bypass graft surgery. Cardiovasc Revasc Med,
2010.
11(1): p. 8-19.
15. Goldstein LJ, Hyperbaric oxygen for chronic wounds.
Dermatol Ther, 2013. 26(3): p. 207-214.
16. Game FL, et al. A systematic review of interventions to
enhance the healing of chronic ulcers of the foot in
diabetes.
Diabetes Metab Res Rev, 2012. 28 Suppl 1: p. 119-141.
17. Thom SR, Hyperbaric oxygen: its mechanisms and
efcacy. Plastic and Reconstructive Surgery, 2011. 127
Suppl 1: p. 131S-141S.
18. Garcia-Lechuz J, Bouza E. Treatment recommendations
and strategies for the management of bone and jointinfections.
Expert Opin Pharmacother, 2009. 10(1): p. 35-55.
19. Cimsit M, Uzun G, Yildiz S. Hyperbaric oxygen therapy
as an anti-infective agent. Expert Rev Anti Infect Ther,
2009.
7(8): p. 1015-1026.
20. Brown RB. Sands M. Infectious disease indications
for hyperbaric oxygen therapy. Compr Ther, 1995. 21(11):
p. 663-667.
21. Goldstein LJ, et al. Endothelial progenitor cell release
into circulation is triggered by hyperoxia-induced increases
in bone marrow nitric oxide. Stem Cells, 2006. 24(10):
p. 2309-2318.
22. Thom SR, et al. Stem cell mobilization by hyperbaricoxygen.
Am J Physiol Heart Circ Physiol, 2006. 290(4): p.
H1378-86.
23. Velazquez OC. Angiogenesis and vasculogenesis:
inducing the growth of new blood vessels and wound healing
by stimulation of bone marrow-derived progenitor cell mobi-
lization and homing. J Vasc Surg, 2007. 45 Suppl A:
p. A39-47.
24. Lin KC, et al. Attenuating inammation but stimulating
both angiogenesis and neurogenesis using hyperbaric oxygen
in rats with traumatic brain injury. J Trauma Acute Care
Surg, 2012. 72(3): p. 650-659.
25. Harch PG, et al. Hyperbaric oxygen therapy improvesspatial
learning and memory in a rat model of chronic
traumatic brain injury. Brain Res, 2007. 1174: p. 120-129.
26. Lee YS, et al. Long course hyperbaric oxygen
stimulates neurogenesis and attenuates inammation after
ischemic stroke. Mediators Inamm, 2013. 2013: p. 512978.
27. Liu ZJ, Velazquez OC. Hyperoxia, endothelial
progenitor cell mobilization, and diabetic wound healing.
Antioxid Redox Signal, 2008. 10(11): p. 1869-1882.
_________________________________________________________________________________________________________________________________________________________
REFERENCES
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
15/19
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
347X.A. Figueroa, J.K. Wright
28. Thom SR, et al. Vasculogenic stem cell mobilization
and wound recruitment in diabetic patients: increased cell
number and intracellular regulatory protein content
associated with hyperbaric oxygen therapy. Wound Repair
Regen, 2011. 19(2): p. 149-161.
29. Zhang K, Zhu L, Fan M. Oxygen, a key factor
regulating cell behavior during neurogenesis and
cerebraldiseases. Front Mol Neurosci, 2011. 4: p. 5.
30. Zhang Y, et al. Hyperbaric oxygen therapy ameliorates
local brain metabolism, brain edema and inammatory
response in a blast-induced traumatic brain injury model
in rabbits. Neurochem Res, 2014. 39(5): p. 950-960.
31. Lim SW, et al. Microglial activation induced by
traumatic brain injury is suppressed by postinjury treatment
with hyperbaric oxygen therapy. J Surg Res, 2013.
32. Wilson HD, et al. Hyperbaric oxygen treatment is
comparable to acetylsalicylic acid treatment in an animal
model of arthritis. J Pain, 2007. 8(12): p. 924-930.
33. Vlodavsky E, Palzur E, Soustiel JF. Hyperbaric oxygentherapy
reduces neuroinammation and expression of matrix
metalloproteinase-9 in the rat model of traumatic brain
injury. Neuropathol Appl Neurobiol, 2006. 32(1): p. 40-50.
34. Roth TL, et al., Transcranial amelioration of inamma-
tion and cell death after brain injury. Nature, 2014. 505
(7482): p. 223-228.
35. Niklas A, et al. Continuous measurements of cerebral
tissue oxygen pressure during hyperbaric oxygenation--HBO
effects on brain edema and necrosis after severe brain
trauma
in rabbits. J Neurol Sci, 2004. 219(1-2): p. 77-782.
36. Rockswold SB, et al. A prospective, randomized phase
II clinical trial to evaluate the effect of combined
hyperbaricand normobaric hyperoxia on cerebral metabolism,
intracranial pressure, oxygen toxicity, and clinical outcome
in severe traumatic brain injury. J Neurosurg, 2013. 118(6):
p. 1317-1328.
37. Rockswold SB, et al. A prospective, randomized
clinical trial to compare the effect of hyperbaric to normo-
baric hyperoxia on cerebral metabolism, intracranial
pressure, and oxygen toxicity in severe traumatic brain
injury. J Neurosurg, 2010. 112(5): p. 1080-1094.
38. Rockswold SB,Rockswold GL, Dello A. Hyperbaric
oxygen in traumatic brain injury. Neurol Res, 2007. 29(2):
p.
162-172.39. Thom SR, et al. Nitric-oxide synthase-2 linkage to
focal
adhesion kinase in neutrophils inuences enzyme activity
and beta2 integrin function. J Biol Chem, 2013. 288(7): p.
4810-4818.
40. Kendall AC, et al. Hyperbaric oxygen treatment reduces
neutrophil-endothelial adhesion in chronic wound conditions
through S-nitrosation. Wound Repair Regen, 2013. 21(6): p.
860-868.
41. Yogaratnam JZ, et al. Pharmacological preconditioning
with hyperbaric oxygen: can this therapy attenuate myo-
cardial ischemic reperfusion injury and induce myocardial
protection via nitric oxide? J Surg Res, 2008. 149(1):
p. 155-164.
42. Khiabani KT, et al. A quantitative method for
determining polarization of neutrophil adhesion
moleculesassociated with ischemia reperfusion. Plastic and
Reconstructive Surgery, 2004. 114(7): p. 1846-1850.
43. Miljkovic-Lolic M, et al. Neuroprotective effects of
hyperbaric oxygen treatment in experimental focal cerebral
ischemia are associated with reduced brain leukocyte
myeloperoxidase activity. Brain Res, 2003. 971(1): p. 90-94.
44. Larson JL, Stephenson LL, Zamboni WA. Effect of
hyperbaric oxygen on neutrophil CD18 expression. Plastic
and Reconstructive Surgery, 2000. 105(4): p. 1375-1381.
45. Buras JA, et al. Hyperbaric oxygen downregulates
ICAM-1 expression induced by hypoxia and hypoglycemia:
the role of NOS. Am J Physiol Cell Physiol, 2000. 278(2):
p. C292-302.
46. Atochin DN, et al. Neutrophil sequestration and the
effect of hyperbaric oxygen in a rat model of temporary
middle cerebral artery occlusion. Undersea Hyperb Med,
2000. 27(4): p. 185-190.
47. Gu N, et al. Hyperbaric oxygen therapy attenuates
neuropathic hyperalgesia in rats and idiopathic trigeminal
neuralgia in patients. Eur J Pain, 2012. 16(8): p.
1094-1105.
48. Quock LP, et al. The acute antinociceptive effect of
HBO is mediated by a NO-cyclic GMP-PKG-KATP channel
pathway in mice. Brain Res, 2011. 1368: p. 102-107.
49. Li F. et al. Hyperbaric oxygenation therapy alleviates
chronic constrictive injury-induced neuropathic pain and
reduces tumor necrosis factor-alpha production. Anesth
Analg, 2011. 113(3): p. 626-633.
50. Smith C. et al. The neuroinammatory response in
humans after traumatic brain injury. Neuropathol Appl
Neurobiol, 2013. 39(6): p. 654-666.
51. Tompkins P. et al. Brain injury: neuro-inammation,
cognitive decit, and magnetic resonance imaging in a
model of blast induced traumatic brain injury. J
Neurotrauma,
2013. 30(22): p. 1888-1897.
52. Olsson A. et al. Marked increase of beta-amyloid (1-42)
and amyloid precursor protein in ventricular cerebrospinal
uid after severe traumatic brain injury. J Neurol, 2004.
251(7): p. 870-876.
53. Dams-OConnor K. et al. Risk for late-life re-injury,
dementia and death among individuals with traumatic brain
injury: a population-based study. J Neurol Neurosurg
Psychiatry, 2013. 84(2): p. 177-182.
54. Moretti L, et al. Cognitive decline in older adults with
a history of traumatic brain injury. Lancet Neurol, 2012.
11(12): p. 1103-12.
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
16/19
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
348 X.A. Figueroa, J.K. Wright
55. Jellinger KA, et al. Effects of closed traumatic brain
injury and genetic factors on the development of Alzheimers
disease. Eur J Neurol, 2001. 8(6): p. 707-710.
56. Jellinger KA, et al. Traumatic brain injury as a risk
factor for Alzheimer disease. Comparison of two retro-
spective autopsy cohorts with evaluation of ApoE genotype.
BMC Neurol, 2001. 1: p. 3.57. Desai A, Kevala K, Kim HY.
Depletion of brain docosa-
hexaenoic Acid impairs recovery from traumatic brain injury.
PLoS One, 2014. 9(1): p. e86472.
58. Pu H, et al. Omega-3 polyunsaturated fatty acid supple-
mentation improves neurologic recovery and attenuates
white matter injury after experimental traumatic brain
injury.
J Cereb Blood Flow Metab, 2013. 33(9): p. 1474-1484.
59. Lewis M, Ghassemi P, Hibbeln J. Therapeutic use of
omega-3 fatty acids in severe head trauma. Am J Emerg
Med, 2013. 31(1): p. 273 e5-8.
60. Hasadsri L, et al. Omega-3 fatty acids as a putative
treatment for traumatic brain injury. J Neurotrauma,
2013.30(11): p. 897-906.
61. Shin SS, Dixon CE. Oral sh oil restores striatal
dopamine release after traumatic brain injury. Neurosci
Lett,
2011. 496(3): p. 168-171.
62. Mills JD, et al. Omega-3 fatty acid supplementation and
reduction of traumatic axonal injury in a rodent head injury
model. J Neurosurg, 2011. 114(1): p. 77-84.
63. Bailes JE, Mills JD. Docosahexaenoic acid reduces
traumatic axonal injury in a rodent head injury model. J
Neurotrauma, 2010. 27(9): p. 1617-1624.
64. Browne KD, et al. Chronic ibuprofen administration
worsens cognitive outcome following traumatic brain injuryin
rats. Experimental Neurology, 2006. 201(2): p. 301-307.
65. Tobinick E, et al. Selective TNF inhibition for chronic
stroke and traumatic brain injury: an observational study
involving 629 consecutive patients treated with perispinal
etanercept. CNS Drugs, 2012. 26(12): p. 1051-70.
66. Tobinick E. Perispinal etanercept: a new therapeutic
paradigm in neurology. Expert Rev Neurother, 2010. 10(6):
p. 985-1002.
67. Gopez JJ, et al. Cyclooxygenase-2-specic inhibitor
improves functional outcomes, provides neuroprotection,
and reduces inammation in a rat model of traumatic brain
injury. Neurosurgery, 2005. 56(3): p. 590-604.68. Godman CA, et
al. Hyperbaric oxygen induces a cyto-
protective and angiogenic response in human microvascular
endothelial cells. Cell Stress Chaperones, 2010. 15(4): p.
431-442.
69. Kaludercic N, Deshwal S, Di Lisa F. Reactive oxygen
species and redox compartmentalization. Front Physiol,
2014. 5: p. 285.
70. Schmeisser S, et al. Neuronal ROS signaling rather than
AMPK/sirtuin-mediated energy sensing links dietary restric-
tion to lifespan extension. Mol Metab, 2013. 2(2): p.
92-102.
71. Wolin MS, Ahmad M, Gupte SA. Oxidant and redox
signaling in vascular oxygen sensing mechanisms: basic
concepts, current controversies, and potential importance
of cytosolic NADPH. Am J Physiol Lung Cell Mol Physiol,2005.
289(2): p. L159-73.
72. Waypa GB, et al. Mitochondrial reactive oxygen species
trigger calcium increases during hypoxia in pulmonary arte-
rial myocytes. Circ Res, 2002. 91(8): p. 719-26.
73. Gilles-Gonzalez MA. Oxygen signal transduction.
IUBMB Life, 2001. 51(3): p. 165-173.
74. Aragones J. et al. Oxygen sensors at the crossroad of
metabolism. Cell Metab, 2009. 9(1): p. 11-22.
75. Chandel NS, Schumacker PT. Cellular oxygen sensing
by mitochondria: old questions, new insight. J Appl Physiol
(1985), 2000. 88(5): p. 1880-1889.
76. Quaegebeur A, Carmeliet P. Oxygen sensing: a commoncrossroad
in cancer and neurodegeneration. Curr Top
Microbiol Immunol, 2010. 345: p. 71-103.
77. Dennog C. et al. Detection of DNA damage after
hyperbaric oxygen (HBO) therapy. Mutagenesis, 1996.
11(6): p. 605-609.
78. Hall ED. Lipid antioxidants in acute central nervous
system injury. Annals of Emergency Medicine, 1993. 22(6):
p. 1022-1027.
79. Benedetti S, et al. Oxidative stress and antioxidant
status in patients undergoing prolonged exposure to hyper-
baric oxygen. Clin Biochem, 2004. 37(4): p. 312-317.
80. Gutsaeva DR, et al. Oxygen-induced mitochondrial
biogenesis in the rat hippocampus. Neuroscience, 2006.
137(2): p. 493-504.
81. Anne Stetler R, et al. The dynamics of the mitochondrial
organelle as a potential therapeutic target. J Cereb Blood
Flow Metab, 2013. 33(1): p. 22-32.
82. Matchett GA, Martin RD, Zhang JH. Hyperbaric
oxygen therapy and cerebral ischemia: neuroprotective
mechanisms. Neurol Res, 2009. 31(2): p. 114-121.
83. Leask A. Integrin 1: a mechanosignaling sensor
essential for connective tissue deposition by broblasts.
Adv Wound Care (New Rochelle), 2013. 2(4): p. 160-166.
84. Kufer DP. The role of hyperbaric oxygen therapy in
enhancing the rate of wound healing with a focus on axon
regeneration. P R Health Sci J, 2011. 30(1): p. 35-42.
85. Palzur E, et al. Neuroprotective effect of hyperbaric
oxygen therapy in brain injury is mediated by preservation
of
mitochondrial membrane properties. Brain Res, 2008. 1221:
p. 126-133.
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
17/19
349
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
X.A. Figueroa, J.K. Wright
86. Wada K, et al. Mn-SOD and Bcl-2 expression after
repeated hyperbaric oxygenation. Acta Neurochir Suppl,
2000. 76: p. 285-90.
87. Soustiel JF, et al. The effect of oxygenation level on
cerebral post-traumatic apoptotsis is modulated by the
18-kDa translocator protein (also known as peripheral-type
benzodiazepine receptor) in a rat model of corticalcontusion.
Neuropathol Appl Neurobiol, 2008. 34(4):
p. 412-423.
88. Zhou Z, et al. Protection of mitochondrial function
and improvement in cognitive recovery in rats treated with
hyperbaric oxygen following lateral uid-percussion injury.
J Neurosurg, 2007. 106(4): p. 687-94.
89. Chen X, et al. Interleukin-10 mediates the neuro-
protection of hyperbaric oxygen therapy against traumatic
brain injury in mice. Neuroscience, 2014. 266: p. 235-243.
90. Ito U, et al. Temporal prole of experimental ischemic
edema after threshold amount of insult to induce infarction-
-ultrastructure, gravimetry and Evans blue extravasation.Acta
Neurochir Suppl, 2003. 86: p. 131-5.
91. Livnat A, Barbiro-Michaely E, Mayevsky A.
Mitochondrial function and cerebral blood ow variable
responses to middle cerebral artery occlusion. J Neurosci
Methods, 2010. 188(1): p. 76-82.
92. Villa RF, et al. Energy metabolism of cerebral mito-
chondria during aging, ischemia and post-ischemic recovery
assessed by functional proteomics of enzymes. Neurochem
Int, 2013. 63(8): p. 765-781.
93. Mazzeo AT, et al. The role of mitochondrial transition
pore, and its modulation, in traumatic brain injury and
delayed neurodegeneration after TBI. ExperimentalNeurology,
2009. 218(2): p. 363-370.
94. Sayeed I, et al. Direct inhibition of the mitochondrial
permeability transition pore: a possible mechanism for
better
neuroprotective effects of allopregnanolone over progester-
one. Brain Res, 2009. 1263: p. 165-173.
95. Robertson CL, et al. The potential role of mitochondria
in pediatric traumatic brain injury. Dev Neurosci, 2006.
28(4-5): p. 432-46.
96. Liu Z, et al. Effect of hyperbaric oxygen on cytochrome
C, Bcl-2 and Bax expression after experimental traumatic
brain injury in rats. Chin J Traumatol, 2006. 9(3): p.
168-174.
97. Busija DW, Katakam PV. Mitochondrial mechanismsin cerebral
vascular control: shared signaling pathways with
preconditioning. J Vasc Res, 2014. 51(3): p. 175-189.
98. Lou M, et al. Involvement of the mitochondrial ATP-
sensitive potassium channel in the neuroprotective effect of
hyperbaric oxygenation after cerebral ischemia. Brain Res
Bull, 2006. 69(2): p. 109-116.
99. Daugherty WP, et al. Effects of hyperbaric oxygen
therapy on cerebral oxygenation and mitochondrial function
following moderate lateral uid-percussion injury in rats.
J Neurosurg, 2004. 101(3): p. 499-504.
100. Neubauer RA, Gottlieb SF, Kagan RL. Enhancing
idling neurons. Lancet, 1990. 335(8688): p. 542.
101. Neubauer, R.A., Idling neurons. Lancet, 1990.335(8699): p.
1217.
102. Neubauer RA, James P. Cerebral oxygenation and the
recoverable brain. Neurol Res, 1998. 20 Suppl 1: p. S33-S36.
103. Holbach KH, et al. Differentiation between reversible
and irreversible post-stroke changes in brain tissue: its
relevance for cerebrovascular surgery. Surg Neurol, 1977.
7(6): p. 325-331.
104. Rossi GF, et al. Neurological improvement in chronic
ischemic stroke following surgical brain revascularization.
Ital J Neurol Sci, 1987. 8(5): p. 465-75.
105. Neubauer RA, Gottlieb SF, Miale A Jr. Identication of
hypometabolic areas in the brain using brain imaging
andhyperbaric oxygen. Clin Nucl Med, 1992. 17(6): p. 477-481.
106. Shin SS, et al. Detection of white matter injury in
concussion using high-denition ber tractography.
Prog Neurol Surg, 2014. 28: p. 86-93.
107. Efrati S, et al. Hyperbaric oxygen induces late neuro-
plasticity in post stroke patients - randomized, prospective
trial. PLoS One, 2013. 8(1): p. e53716.
108. Blackstone E, Morrison M, Roth MB. H2S induces
a suspended animation-like state in mice. Science, 2005.
308(5721): p. 518.
109. Blackstone E, Roth MB. Suspended animation-like
state protects mice from lethal hypoxia. Shock, 2007. 27(4):p.
370-372.
110. Eto K, et al. Hydrogen sulde is produced in response
to neuronal excitation. J Neurosci, 2002. 22(9): p. 3386-91.
111. Chen CQ, Xin H, Zhu YZ. Hydrogen sulde: third gas-
eous transmitter, but with great pharmacological potential.
Acta Pharmacol Sin, 2007. 28(11): p. 1709-1716.
112. Qu K, et al. Hydrogen sulde: neurochemistry and
neurobiology. Neurochem Int, 2008. 52(1-2): p. 155-165.
113. Baumgart K, Radermacher P, Wagner F. Applying gases
for microcirculatory and cellular oxygenation in sepsis:
effects of nitric oxide, carbon monoxide, and hydrogen
sulde. Curr Opin Anaesthesiol, 2009. 22(2): p. 168-176.
114. Wagner F, et al. Bench-to-bedside review: Hydrogen
sulde--the third gaseous transmitter: applications for
critical care. Crit Care, 2009. 13(3): p. 213.
115. Olson KR, Whiteld NL. Hydrogen sulde and oxygen
sensing in the cardiovascular system. Antioxid Redox Signal,
2010. 12(10): p. 1219-1234.
116. Pun PB, et al. Gases in the mitochondria. Mitochon-
drion, 2010. 10(2): p. 83-93.
-
7/26/2019 5 Clinical Results in Brain Injury Trials - Another
Perspective
18/19
UHM 2015, VOL. 42, NO. 4
CLINICALRESULTSINBRAININJURYTRIALS:ANOTHER PERSPECTIVE
350 X.A. Figueroa, J.K. Wright
117. Tay AS, et al . Hydrogen sulde protects neurons against
hypoxic injury via stimulation of ATP-sensitive potassium
channel/protein kinase C/extracellular signal-regulated
kinase/heat shock protein 90 pathway. Neuroscience, 2010.
167(2): p. 277-86.
118. Yong QC, et al. Effect of hydrogen sulde on intra-
cellular calcium homeostasis in neuronal cells. NeurochemInt,
2010. 56(3): p. 508-515.
119. Mikami Y, et al. Hydrogen sulde protects the retina
from light-induced degeneration by the modulation of Ca2+
inux. J Biol Chem, 2011. 286(45): p. 39379-39386.
120. Kimura H, Shibuya N. Kimura T. Hydrogen sulde is
a signaling molecule and a cytoprotectant. Antioxid Redox
Signal, 2012.
121. Morbelli S. Arnaldi D. Brain perfusion SPECT provides
new insight on neurobiological effects of hyperbaric hyper-
oxia. Acta Physiol (Oxf), 2013.
122. Barrett KF, et al. Regional CBF in chronic stable TBI
treated with hyperbaric oxygen. Undersea Hyperb Med,2004. 31(4):
p. 395-406.
123. Kraus MF, et al. White matter integrity and cognition
in chronic traumatic brain injury: a diffusion tensor
imaging
study. Brain, 2007. 130(Pt 10): p. 2508-2519.
124. Kraitsy K, et al. Repetitive long-term hyperbaric
oxygen treatment (HBOT) administered after experimental
traumatic brain injury in rats induces signicant remyelina-
tion and a recovery of sensorimotor function. PLoS One,
2014. 9(5): p. e97750.
125. Boussi-Gross R, et al. Hyperbaric oxygen therapy
can improve post concussion syndrome years after mild
traumatic brain injury - randomized prospective trial.PLoS One,
2013. 8(11): p. e79995.
126. Harch PG, et al. A phase I study of low-pressure hyper-
baric oxygen therapy for blast-induced post-concussion
syndrome and post-traumatic stress disorder. J Neurotrauma,
2012. 29(1): p. 168-85.
127. Gesell LB. Hyperbaric oxygen therapy indications., in
The Hyperbaric Oxygen Therapy Committee report. 2008,
Undersea and Hyperbaric Medical Society: Durham, N.C.
128. Acker T, Acker H. Cellular oxygen sensing need in CNS
function: physiological and pathological implications. J Exp
Biol, 2004. 207(Pt 18): p. 3171-3188.
129. Acevedo AD, et al. Morphological and proliferativeresponses
of endothelial cells to hydrostatic pressure: role
of broblast growth factor. J Cell Physiol, 1993. 157(3):
p. 603-614.
130. Tokunaga O, Fan JL, Watanabe T. Atherosclerosis and
endothelium. Part II. Properties of aortic endothelial and
smooth muscle cells cultured at various ambient pressures.
Acta Pathol Jpn, 1989. 39(6): p. 356-362.
131. Tokunaga O, Watanabe T. Properties of endothelial cell
and smooth muscle cell cultured in ambient pressure. In
Vitro Cell Dev Biol, 1987. 23(8): p. 528-534.
132. Kramer MR, et al. Effect of natural oxygen enrichment
at low altitude on oxygen-dependent patients with end-stage
lung disease. Ann Intern Med, 1994. 121(9): p. 658-662.
133. Kramer MR, et al. Rehabilitation of hypoxemic patientswith
COPD at low altitude at the Dead Sea, the lowest place
on earth. Chest, 1998. 113(3): p. 571-575.
134. Medicine JH. Scuba diving improves function of body,
mind in vets with spinal cord injury. [Current News Release]
2011 September 17, 2011 [cited 2014 August 22]; Johns
Hopkins researchers nd dramatic results in small prelimi-
nary study]. Available from: http://www.hopkinsmedicine.
org/news/media/releases/scuba_diving_improves_function_
of_body_mind_in_vets_with_spinal_cord_injury.
135. Miller S. Primary outcomes from randomized, multi-
center trial of HBOT 1.5 ATA for post concussion syndrome.
2013, US Army Medical Materiel Development Activity:Ft. Detrick.
p. 15.
136. Nighoghossian N, et al. Hyperbaric oxygen in the treat-
ment of acute ischemic stroke. A double-blind pilot study.
Stroke, 1995. 26(8): p. 1369-72.
137. Rusyniak DE, et al. Hyperbaric oxygen therapy in acute
ischemic stroke: results of the hyperbaric oxygen in acute
ischemic stroke trial pilot study. Stroke, 2003. 34(2):
p. 571-574.
138. Wilkinson PR, et al. Longer term quality of life and
outcome in stroke patients: is the Barthel index alone an
adequate measure of outcome? Qual Health Care, 1997. 6(3):
p. 125-130.139. Wasserman S, Bryer A. Early outcomes of
thrombolysis
for acute ischaemic stroke in a South African tertiary care
centre. S Afr Med J, 2012. 102(6): p. 541-544.
140. Stoller KP. Hyperbaric oxygen therapy (1.5 ATA) in
treating sports related TBI/CTE: two case reports. Med Gas
Res, 2011. 1(1): p. 17.
141. Wright JK, et al. Case report: treatment of mild trau-
matic brain injury with hyperbaric oxygen. Undersea Hyperb
Med, 2009. 36(6): p. 391-399.
142. Eovaldi B, Zanetti C. Hyperbaric oxygen ameliorates
worsening signs and symptoms of post-trauma