Embed Size (px)
Citation preview

4/4/2010
1
1
Chest CT
Protocols

4/4/2010
2
Educational Objectives
By the end of this lecture you should be able to:
� Explain patient preparation for chest CT examinations
� Explain the CT protocol for :
• Routine chest
• High resolution Chest
� State the common indications for each protocol
� Identify the contrast volume and route of administration for each protocol
� Identify the standard windowing for each protocol
� Explain how to modify the technique according to patient condition
3
4
1. Protocols for Multislice Helical Computed Tomography, The fundamentals.
by Peter Dawson
2. Body CT protocols state of the Art , Rogalla P., Mutze S., Hamm B.
3. Text book of radiographic positioning and related anatomy; by Kenneth
L.Bontrager,6th edition.
Websites
http://www.ctisus.org/
http://www.halls.md/ct/ct.htm
http://www.slaney.org/pct/
References

4/4/2010
3
Advantages of spiral CT chest
� Allows major portions or entire chest to be scanned during
a single breath hold
� Eliminates motion artifacts
� High quality multiplanar, three dimensional image display
� Basis of virtual bronchoscope
5
Advantages of spiral CT chest
6
Virtual bronchoscopy combines multidetector helical CT with
computer-assisted image processing to generate high quality
intra- and extra-luminal views of the airways. The use of novel,
automated reconstruction algorithms can help assess the extent
of an airway abnormality, detect subtle areas of stenosis, and
define complex anatomical relationships prior to bronchoscopy
or surgical intervention. In addition, this technology improves
the ability of radiologists to assess airway disease noninvasively.
Virtual bronchoscopy

4/4/2010
4
Some Indications of Chest CT
1. Evaluation of mediastinal or pleural mass
2. Detection of pulmonary metastasis
3. Emphysema (COPD)
4. Patient with Hemoptysis
5. Abscesses or cysts
6. Lung fibrosis
7. Atelectasis
8. Bronchitis (COPD)
9. Guidance FNA
7
COPD
Emphysema
Chronic
Bronchitis
Asthma
8
Chronic Obstructive Pulmonary Disease

4/4/2010
5
Patient Preparation and contrast
Patient preparation:Fasting for 3-4 Hours before the examination
Contrast:
• The use of contrast media which injected intravenously is important for visualization of structures within the mediastinum.
• Department protocols/radiologist preferences determine the specific type, volume and site of injection. ( Average dose 100ml)
• For children 2 ml per kilogram body weight.
The advantage of contrast media :
1. To detect lesions
2. To distinguish vessels from lesions
3. To demonstrate displacement of vessels by masses
4. To demonstrate the enhancement of pathologies
9
CT Chest -Slice spacing
� Adequate assessment of patient 10 mm interval
� Improved spatial resolution allows better assessment of
normal and abnormal findings
� Pulmonary metastasis requires spiral CT with 5 to 7mm
thick sections
� Trachea and central bronchi 3 to 5mm thick spiral CT
� Pulmonary parenchyma and peripheral bronchi requires
1 to 2 mm sections
10

4/4/2010
6
Image display settings
� Mediastinum ,Hilum
� WW 350 to 500HU
� WL 30 to 50HU
� lungs:
� WW 1000 to 1500HU
� WL -600 to -700HU
11
12
Normal Anatomy
1. Coracoid. 2. Right clavicle. 3. Right common carotid artery. 4. Thyroid. 5. Internal jugular vein. 6. Left clavicle. 7. Left Subclavian vein. 8. Left humeral head. 9. Scapular spine. 10.Spinous process.
Axial cut. Mediastinal Window

4/4/2010
7
13
Normal Anatomy
1. Right humeral head. 2. Esophagus. 3. Trachea. 4. Left Subclavian vein.5. Scapular spine.6. Glena
Axial cut. Mediastinal Window
14
Normal Anatomy
Axial cut. Mediastinal Window
1. Right lung. 2. Rib. 3. Esophagus. 4. Trachea.5. Left brachiocephalic vein . 6. Left common carotid artery. 7. Left Axillary vein. 8. Left Lung.9. Transverse process. 10. Scapula.

4/4/2010
8
15
Normal Anatomy
Axial cut. Mediastinal Window
1. Right lung. 2. Rib.3. Trachea.4. Left brachiocephalic vein . Brachiocephalic artery.
5. Left common carotid artery. 6. Left Subclavian artery. 7. Scapula. 8. Esophagus. 9. Spinous process.
16
Normal Anatomy
Axial cut. Mediastinal Window
1. Right lung. 2. Trachea. 3. Superior vena cava. 4. Aortic arch. 5. Left Lung. 6. Scapula 7. Vertebral body. 8. Rib.

4/4/2010
9
17
Normal Anatomy
Axial cut. Mediastinal Window
1. Right lung. 2. Right pulmonary artery. 3. Superior vena cava. 4. Thoracic ascending aorta. 5. Pulmonary artery root. 6. Left pulmonary vein. 7. Left pulmonary artery. 8. Rib. 9. Thoracic descending aorta
18
Normal Anatomy
Axial cut. Mediastinal Window
1. Right atrium. 2. Aortic root. 3. Right ventricle. 4. Left atrium. 5. Thoracic descending aorta.

4/4/2010
10
19
Normal Anatomy
Axial cut. Mediastinal Window
1. Right lung. 2. Right atrium. 3. Right ventricle. 4. Left ventricle. 5. Left Lung. 6. Thoracic descending aorta.
20
Normal Anatomy
Axial cut. Mediastinal Window
1. Right lung. 2. Inferior vena cava. 3. Right ventricle. 4. Left ventricle. 5. Esophagus. 6. Left Lung. 7. Thoracic descending aorta. 8. Spinal canal.

4/4/2010
11
21
Normal Anatomy
Axial cut. Mediastinal Window
1. Right lung. 2. Liver. 3. Inferior vena cava. 4. Right ventricle. 5. Left ventricle. 6. Esophagus. 7. Left Lung. 8. Thoracic descending aorta. 9. Vertebral body.
22
Normal Anatomy
Axial cut. Mediastinal Window
1, Inferior lobe of right lung. 2, Liver. 3, Inferior vena cava. 4, Esophagus. 5, Left Lung 6, Aorta.

4/4/2010
12
23
Normal Anatomy
Axial cut. Mediastinal Window
1. Inferior lobe of right lung. 2. Liver.3. Inferior vena cava. 4. Inferior lobe of left lung. 5. Aorta.
24
Normal Anatomy
Axial cut. Lung Window
1. Apical segment bronchus upper lobe (Right lung). 2. Division of Trachea. 3. Superior lobe of the left lung. 4. Inferior lobe of left lung. Red arrow, Major fissure.

4/4/2010
13
25
Normal Anatomy
1. Posterior segmental bronchus upper lobe (right lung). 2. Anterior segmental bronchus upper lobe (right lung). 3. Right main bronchus. 4. Left main bronchus. 5. Superior lobe of the left lung.6. Inferior lobe of left lung. Red arrow, Major fissure.
Axial cut. Lung Window
26
Normal Anatomy
1. Right lower lobe bronchus. 2. Inferior lobe of the right lung. 3. Right middle-lobe bronchus. 4. Right middle lobe. 5, Superior lobe of the right lung. 5. Superior lobe of the left lung. 6. Inferior lobe of left lung.
Axial cut. Lung Window

4/4/2010
14
27
Normal Anatomy
1. Trachea.2. Left main bronchus. 3. Right main bronchus. 4. Apical segmental bronchus upper lobe (Right lung).
5. Right lower lobe bronchus. Red arrow, Major fissure.
Coronal Reconstruction Image
28
Protocols
Reminder
� Variables
� Plain or contrast enhanced
� Slice positioning
� Slice thickness
� Slice orientation
� Slice spacing and overlap
� Timing of imaging and contrast administration
� Reconstruction algorithm
� Radiation dosimetry

4/4/2010
15
29
Optimization of the CT examination requires the supervising
physician and Technologist to develop an appropriate CT
protocol based on careful review of relevant patient history and
clinical indications as well as all prior available imaging studies.
Protocols ( Routine/ HRCT)
Note
CHEST ( Lungs and Mediastinum)
Indications General screening of Pathology
Patient Position Supine arms elevated above head
Topogram From lung apices to below diaphragm
Breathing Breath hold in inspiration ( single breath hold)
Contrast � I.V : 100 ml at 3ml/s. Imaging timing about 30-40 s.
Technical Parameters
� Pitch : 1 mm Slice thickness : 7-10mm (3-5 mm for small lesions)
FilmingParameters
� Soft tissue widow and Lung widow ( Refer to slice No.26)
� Bone window if needed
Comments� For the demonstration of lung nodules or inflammation
low dose protocol with out contrast enhancement is
recommended.
30

4/4/2010
16
CHEST ( HRCT)
Indicationslung diseases e.g. :-• Bronchiectasis • Pulmonary Fibrosis• Emphysema
Patient Position Supine arms elevated above head
Topogram From lung apices to below diaphragm
Breathing Breath hold in inspiration ( single breath hold)
Contrast N/A
Technical Parameters
�Pitch : 1 Suggested collimation 64x0,6 mm Slice thickness : 2-3 mm
FilmingParameters
� Lung widow
Comments � Expiration sequence if required
31
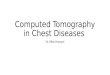
� Thin section and high spatial algorithm makes structures sharper
HRCTHRCT
- bronchial dilatation
Routine CT HRCT

4/4/2010
17
THANK YOU
33