Embed Size (px)
Citation preview
5/17/2016
1
Hemodynamics in the Cath Lab:
What You Should Know or Have Long
Since Forgotten
Zoltan G Turi MD, FACC, MSCAI
Rutgers Robert Wood Johnson Medical School
Why Johnny Can’t Diagnose – Our Failure
to Educate and Re-Educate the
Cardiologist of Today and Tomorrow
Presenter Disclosure Information
Zoltan G. Turi, M.D.
The following relationships exist that are related to this presentation:
No relationships to disclose
5/17/2016
2
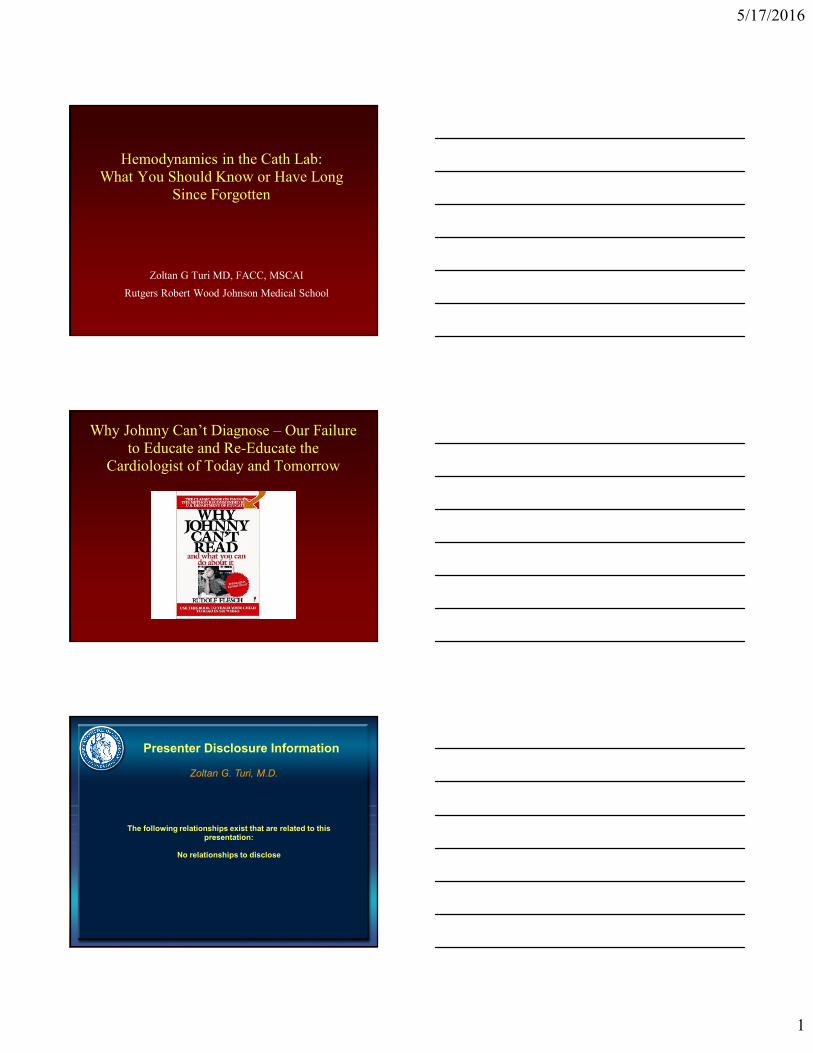
Case 1. Healthy Farmer from Western
Michigan
● Chest pain riding his tractor
● Chest pain at rest
● Electrocardiogram shows EKG changes in seven leads when patient has pain
5/17/2016
3
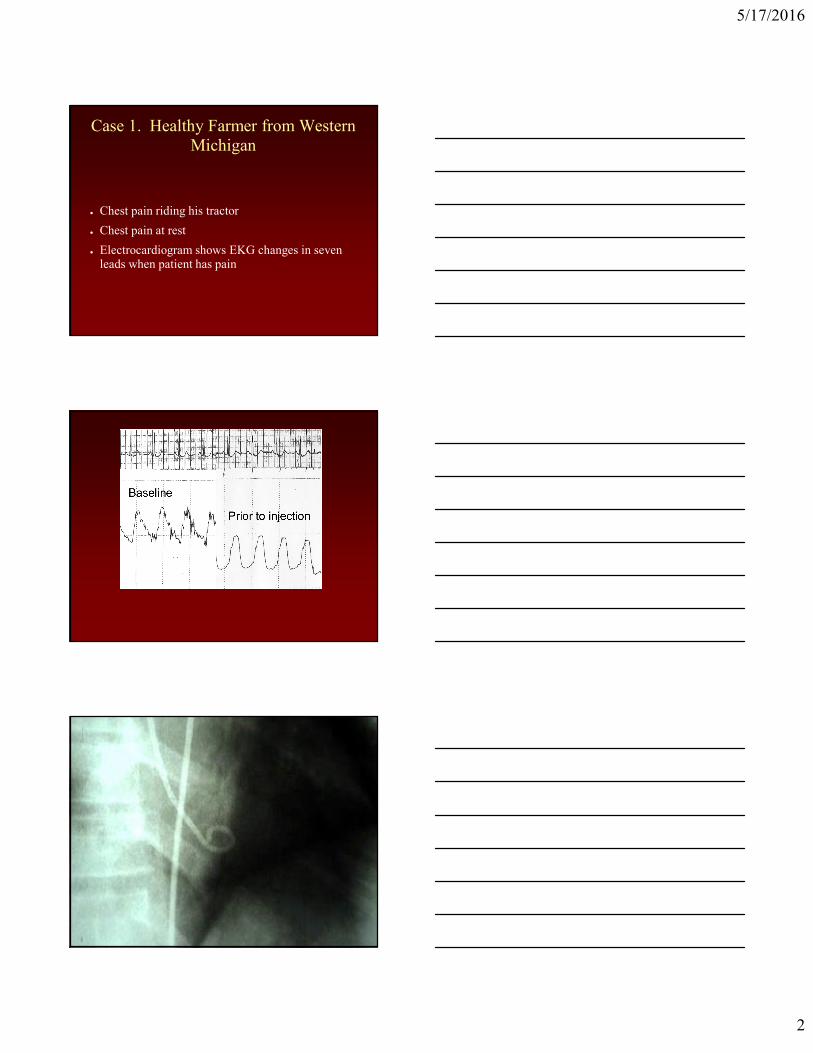
Invasive Cardiology CME US
0
50
100
150
200
250
300
350
400
Interventional Diagnostic
Catheterization and Cardiovascular
Diagnosis:
What Happened to Diagnosis ?
CCD
b. 1975
d. 1995
● 1st year fellowship – 2 months
– Diagnostic cath only – right heart
– Patients admitted Monday
● Research protocol Tuesday morning
● Team meeting with review of history, physical, chest x-
ray Tuesday evening
● Routine right heart cath, left heart cath coronaries 4hours
Wednesday
● Research protocol Thursday
● Discharge Friday
LVEDP
5/17/2016
4
Right Heart Catheterization
● Near 100% in late 1970’s
● Now < 10%
● Used as a marker of inappropriate procedure
selection
● In critical care units – “just get a wedge”
Heart Catheterization 2016
in Most Teaching Hospitals
● Patient admitted and discharged in several hours
● No medical student involvement – slows things
down – and nobody around to teach anyway
● Worked up by physician assistant/nurse
practitioners (“physician extenders”)
● Fellows scrub on case – don’t know patient at all
● Attendings scrub on case – don’t know patient at all
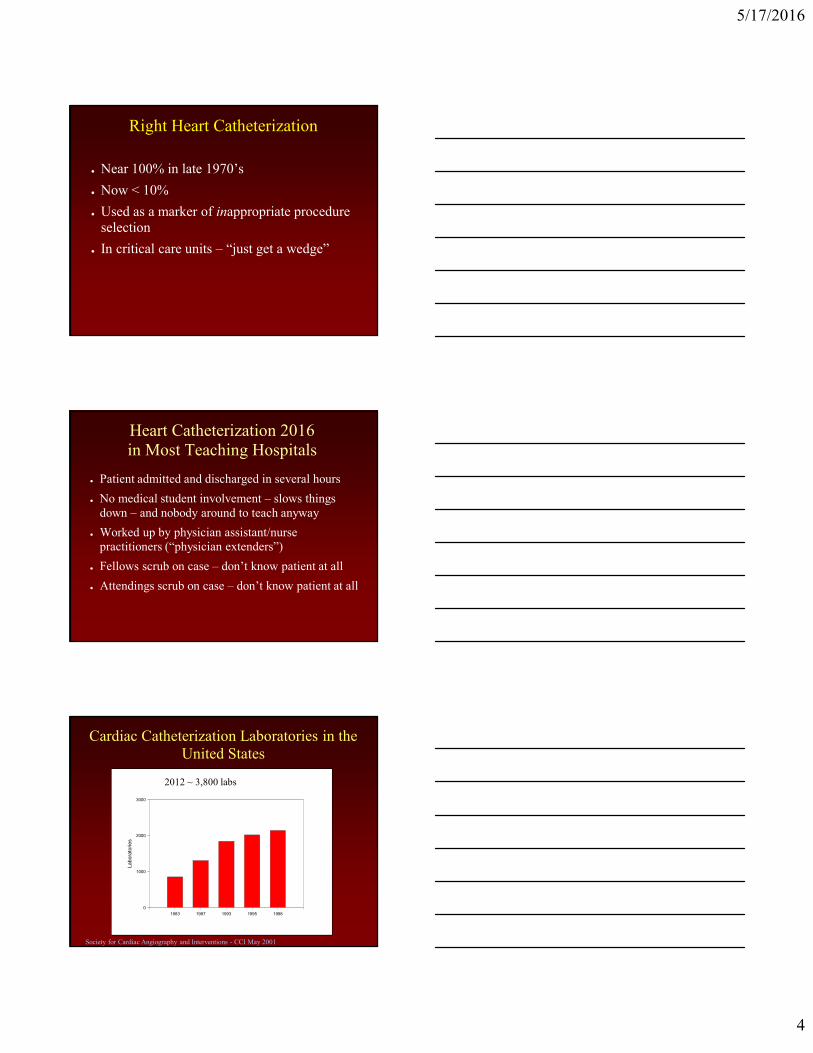
Cardiac Catheterization Laboratories in the
United States
1983 1987 1993 1995 1998
La
bo
rato
rie
s
0
1000
2000
3000
1983 1987 1993 1995 1998
La
bo
rato
rie
s
0
1000
2000
3000
Society for Cardiac Angiography and Interventions - CCI May 2001
2012 ~ 3,800 labs
5/17/2016
5
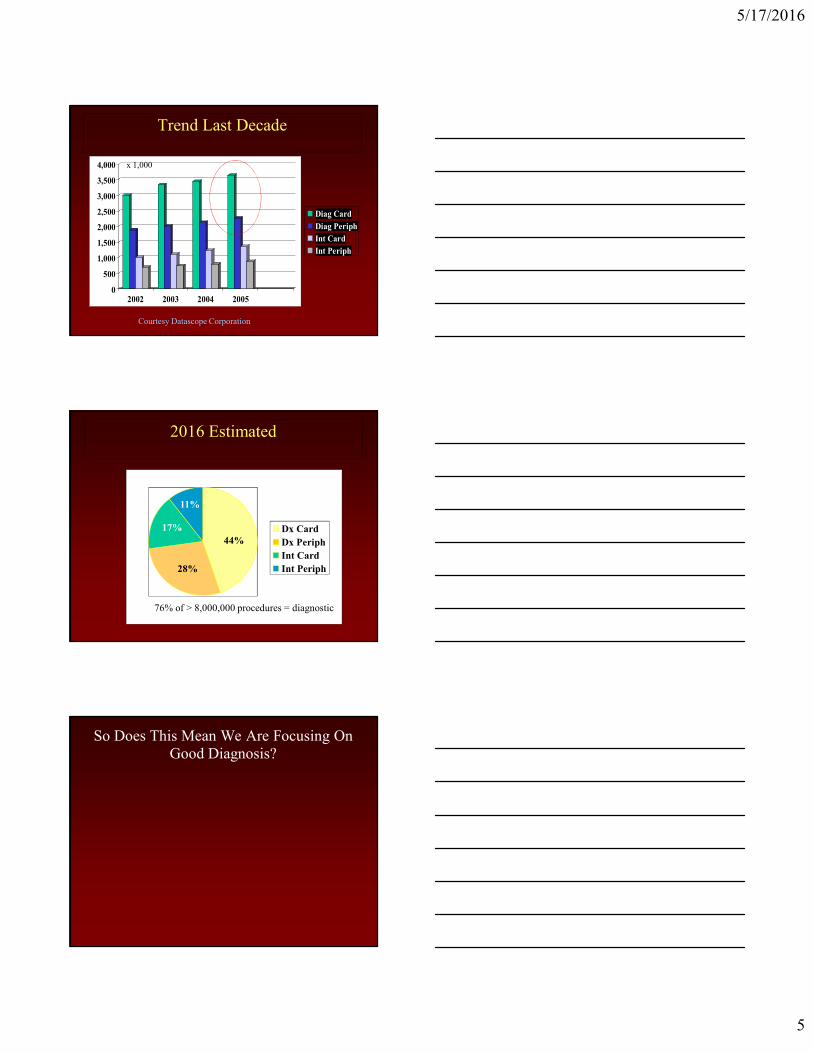
Trend Last Decade
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
2002 2003 2004 2005
Diag Card
Diag Periph
Int Card
Int Periph
Courtesy Datascope Corporation
x 1,000
2016 Estimated
44%
28%
17%
11%
Dx Card
Dx Periph
Int Card
Int Periph
76% of > 8,000,000 procedures = diagnostic
So Does This Mean We Are Focusing On
Good Diagnosis?
5/17/2016
6
The Cardiac Cath Lab 2016
This Should be a Hot Button…
● “Don’t worry about the hemodynamics, I’ll just get an echo…”
● The cath lab has historically been (and should continue to be) the “gold standard” for physiologic diagnosis!
● We have a responsibility to understand hemodynamic recordings and to hold ourselves to a standard of top quality measurements to continue to earn the gold standard title.
– We’re not all doing it well.
Courtesy John Hirshfeld – U Penn
Pitfalls of the “Picture Taking Studio
Cath Lab”
● We use hemodynamic measurement equipment
improperly
● We don’t put information in context
● We fail to differentiate between noise and artifact
● We fail to understand subtleties of findings
● We accept whatever numbers the computer
generates
5/17/2016
7
Case 2. Patient referred for treatment
of aortic stenosis
● 82 year old patient with syncope and systolic ejection murmur, aortic stenosis by echo.
● Inoperable malignancy, thought to have up to 2 years survival.
● Lives independently in relatively good health otherwise. Not frail.
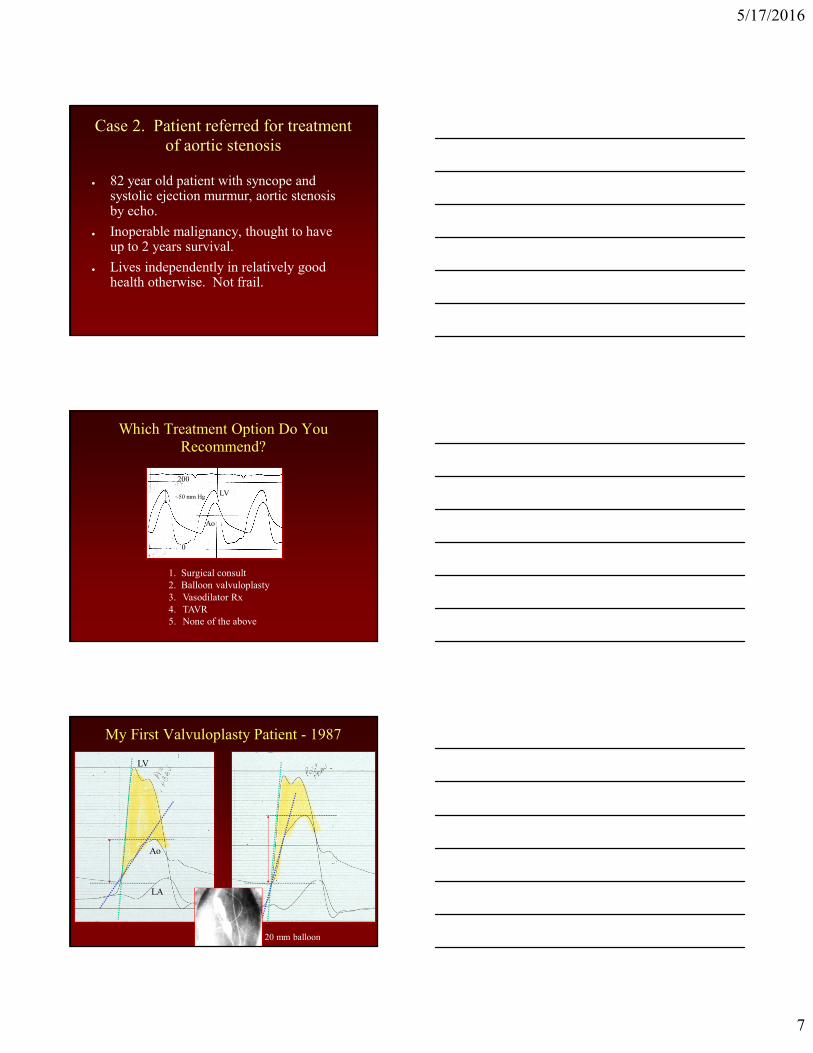
Which Treatment Option Do You
Recommend?
1. Surgical consult
2. Balloon valvuloplasty
3. Vasodilator Rx
4. TAVR
5. None of the above
0
200
LV
Ao
~50 mm Hg
LV
Ao
LA
My First Valvuloplasty Patient - 1987
20 mm balloon
5/17/2016
8
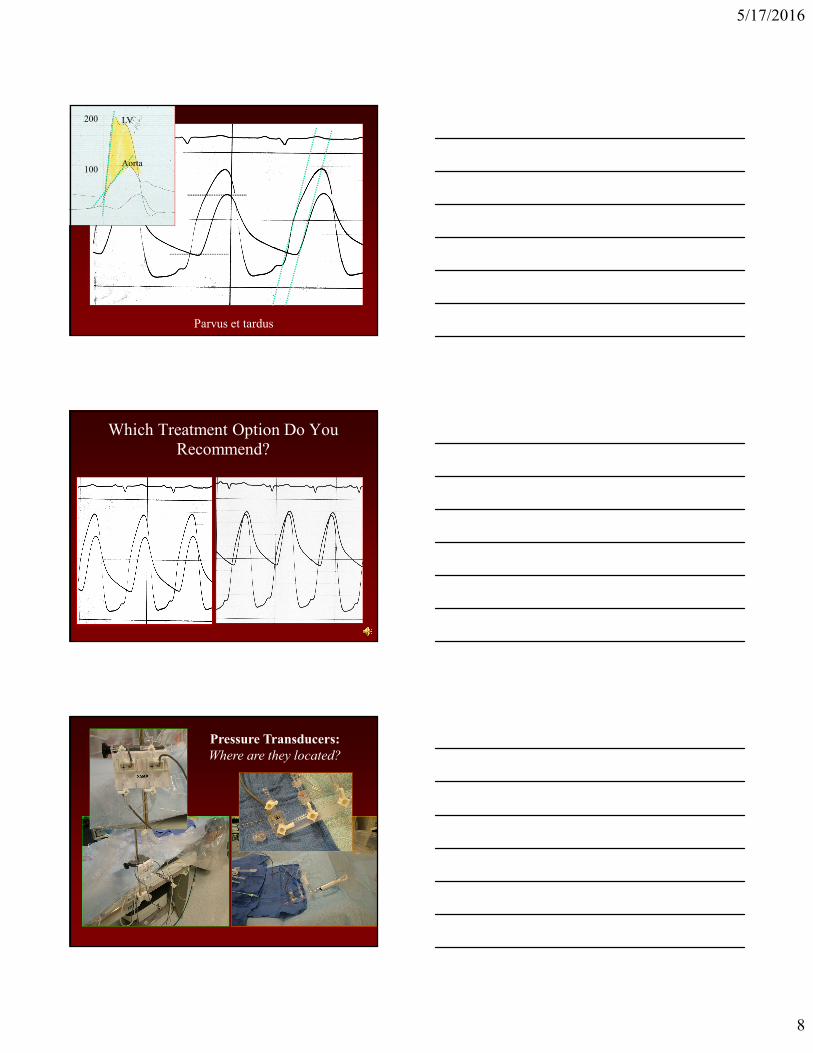
Parvus et tardus
LV
Aorta
200
100
Which Treatment Option Do You
Recommend?
Pressure Transducers:
Where are they located?
5/17/2016
9
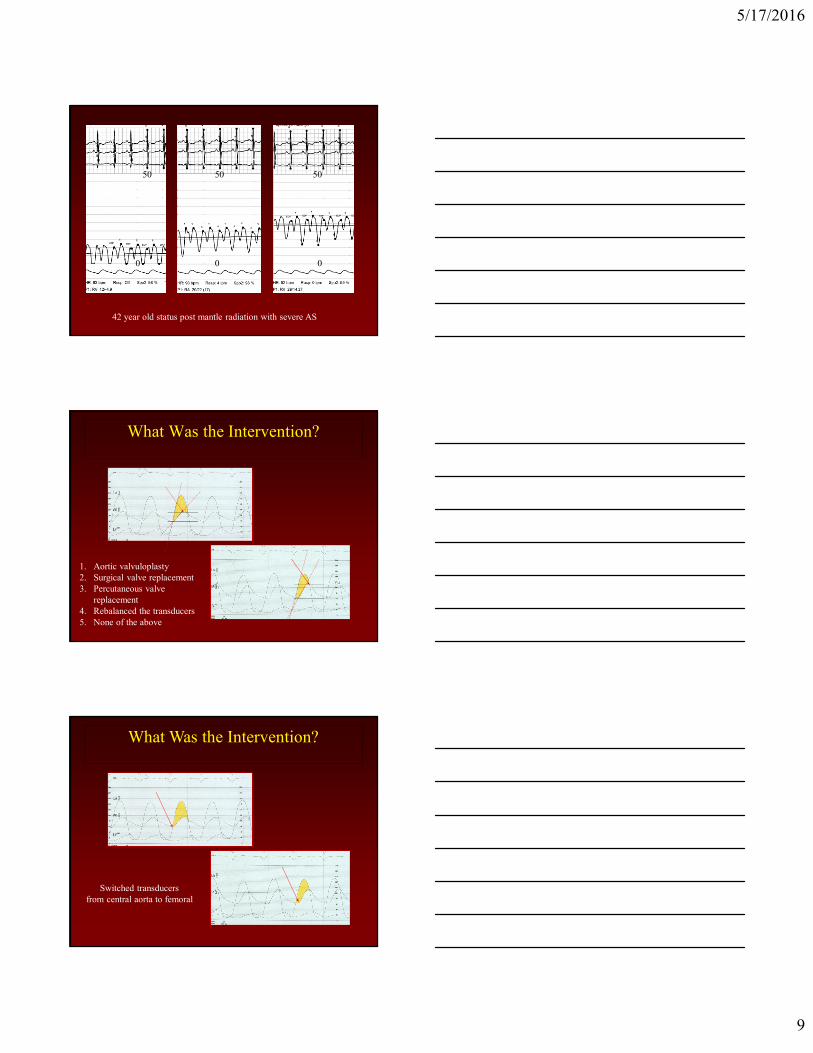
42 year old status post mantle radiation with severe AS
0 0 0
50 50 50
What Was the Intervention?
1. Aortic valvuloplasty
2. Surgical valve replacement
3. Percutaneous valve
replacement
4. Rebalanced the transducers
5. None of the above
What Was the Intervention?
Switched transducers
from central aorta to femoral
5/17/2016
10
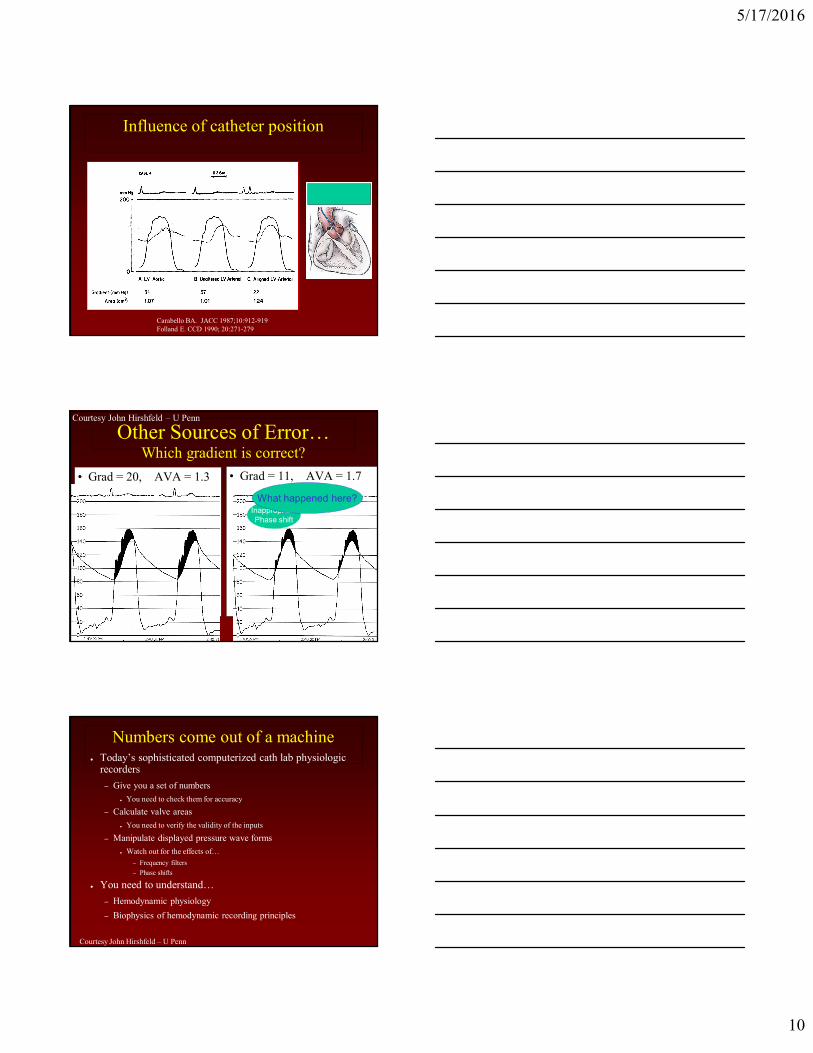
Influence of catheter position
Carabello BA. JACC 1987;10:912-919
Folland E. CCD 1990; 20:271-279
Other Sources of Error…Which gradient is correct?
• Grad = 20, AVA = 1.3 • Grad = 11, AVA = 1.7
Inappropriate
Phase shift
What happened here?
Courtesy John Hirshfeld – U Penn
Numbers come out of a machine● Today’s sophisticated computerized cath lab physiologic
recorders
– Give you a set of numbers
● You need to check them for accuracy
– Calculate valve areas
● You need to verify the validity of the inputs
– Manipulate displayed pressure wave forms
● Watch out for the effects of…
– Frequency filters
– Phase shifts
● You need to understand…
– Hemodynamic physiology
– Biophysics of hemodynamic recording principles
Courtesy John Hirshfeld – U Penn
5/17/2016
11
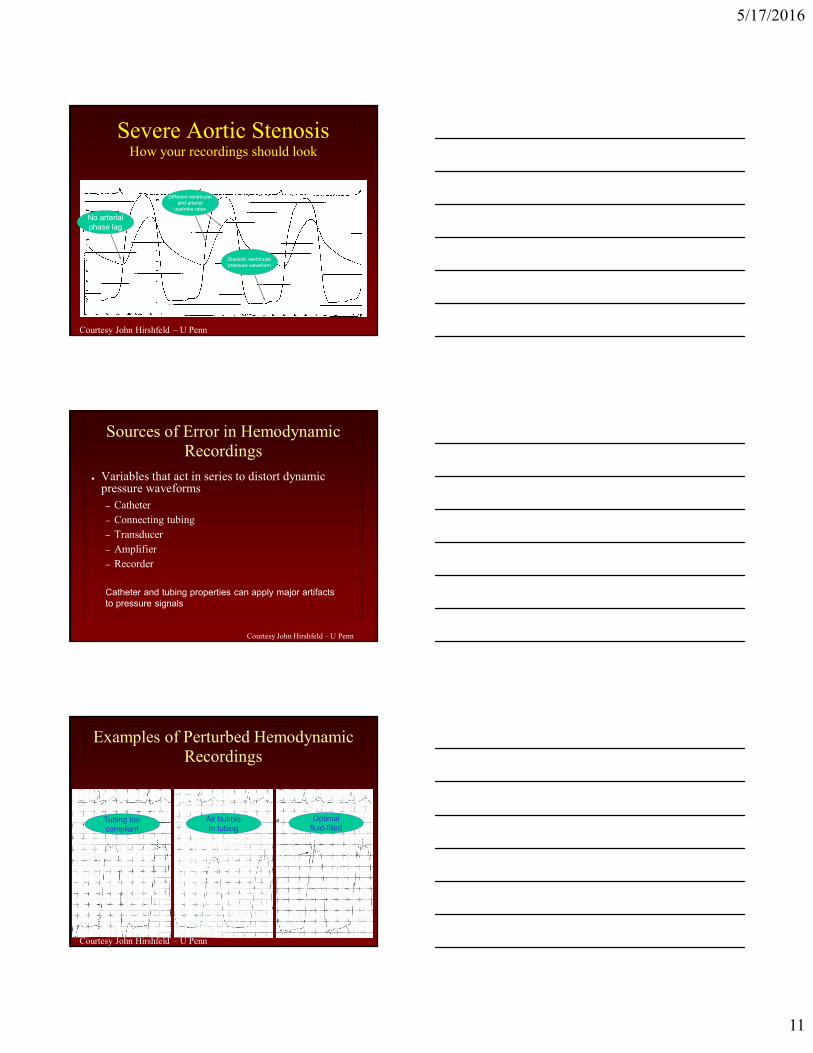
Severe Aortic StenosisHow your recordings should look
No arterial
phase lag
Different ventricular
and arterial
upstroke rates
Diastolic ventricular
pressure waveform
Courtesy John Hirshfeld – U Penn
Sources of Error in Hemodynamic
Recordings
● Variables that act in series to distort dynamic pressure waveforms
– Catheter
– Connecting tubing
– Transducer
– Amplifier
– Recorder
Catheter and tubing properties can apply major artifacts
to pressure signals
Courtesy John Hirshfeld – U Penn
Examples of Perturbed Hemodynamic
Recordings
Tubing too
compliant
Optimal
fluid-filledAir bubble
In tubing
Courtesy John Hirshfeld – U Penn
5/17/2016
12
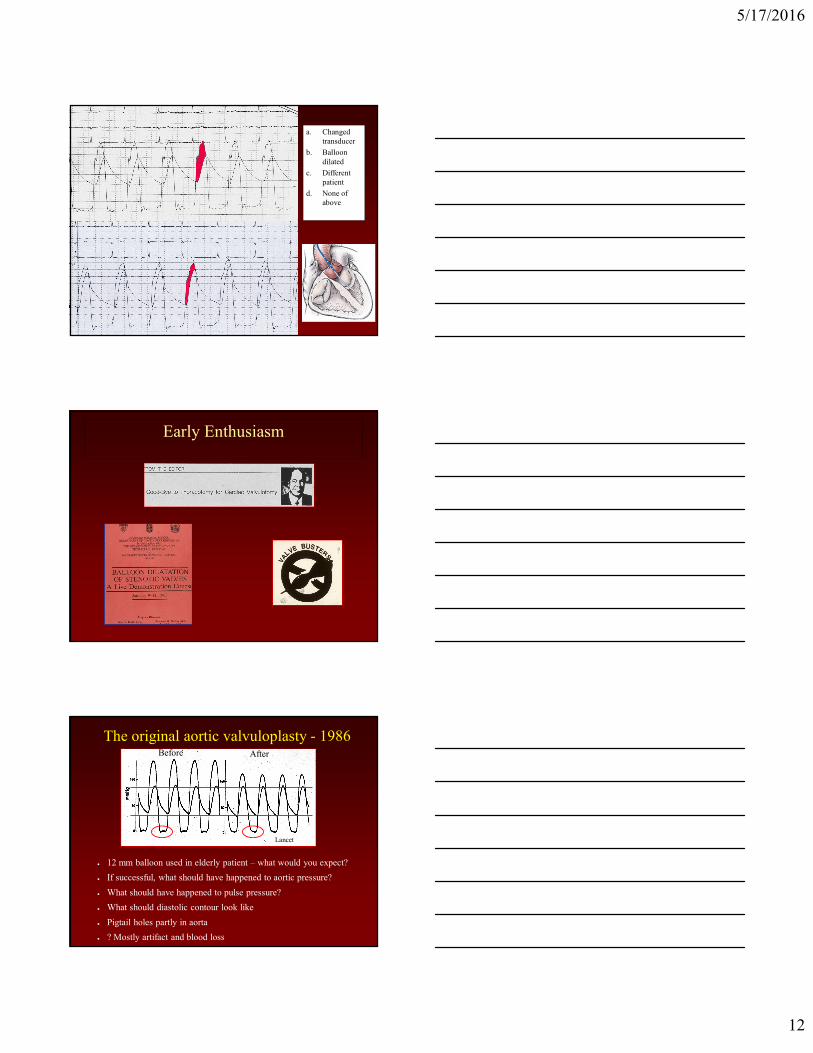
a. Changed
transducer
b. Balloon
dilated
c. Different
patient
d. None of
above
Early Enthusiasm
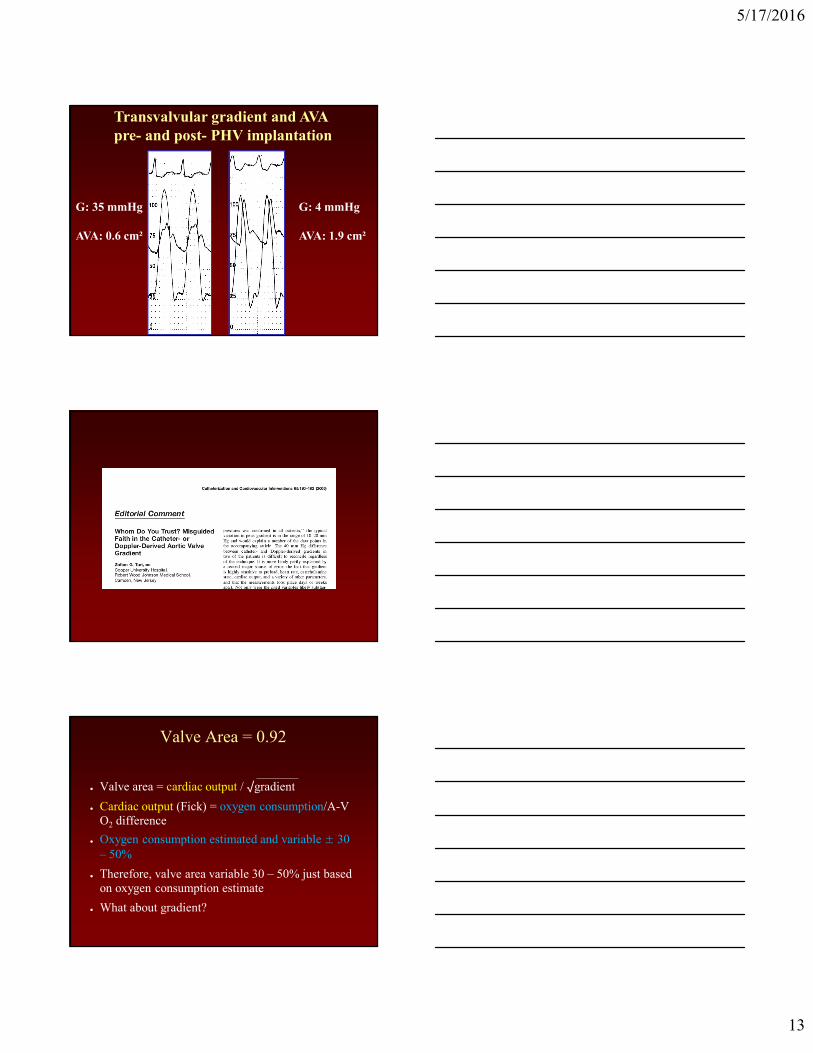
The original aortic valvuloplasty - 1986
● 12 mm balloon used in elderly patient – what would you expect?
● If successful, what should have happened to aortic pressure?
● What should have happened to pulse pressure?
● What should diastolic contour look like
● Pigtail holes partly in aorta
● ? Mostly artifact and blood loss
Before After
Lancet
5/17/2016
13
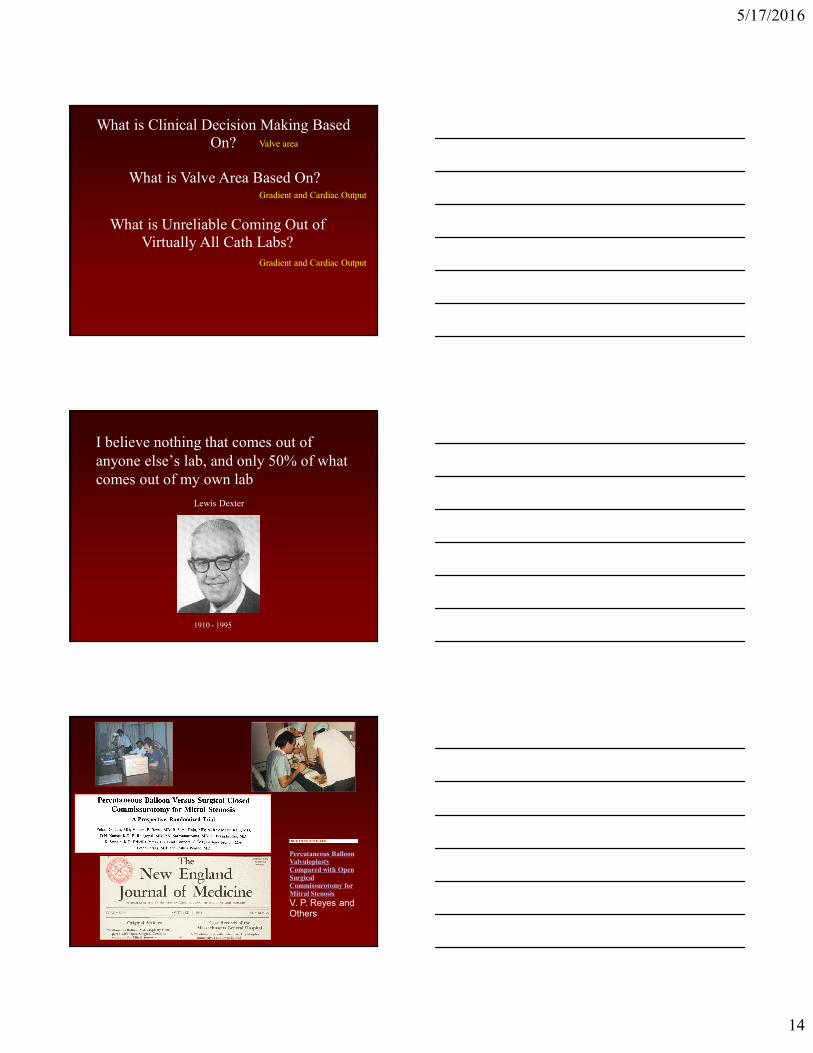
Transvalvular gradient and AVA
pre- and post- PHV implantation
G: 35 mmHg
AVA: 0.6 cm²
G: 4 mmHg
AVA: 1.9 cm²
Valve Area = 0.92
● Valve area = cardiac output / √gradient
● Cardiac output (Fick) = oxygen consumption/A-V
O2 difference
● Oxygen consumption estimated and variable ± 30
– 50%
● Therefore, valve area variable 30 – 50% just based
on oxygen consumption estimate
● What about gradient?
5/17/2016
14
What is Clinical Decision Making Based
On? Valve area
What is Unreliable Coming Out of
Virtually All Cath Labs?
Gradient and Cardiac Output
What is Valve Area Based On?
Gradient and Cardiac Output
I believe nothing that comes out of
anyone else’s lab, and only 50% of what
comes out of my own lab
1910 - 1995
Lewis Dexter
Percutaneous Balloon Valvuloplasty
Compared with Open
Surgical
Commissurotomy for
Mitral Stenosis
V. P. Reyes and Others
5/17/2016
15
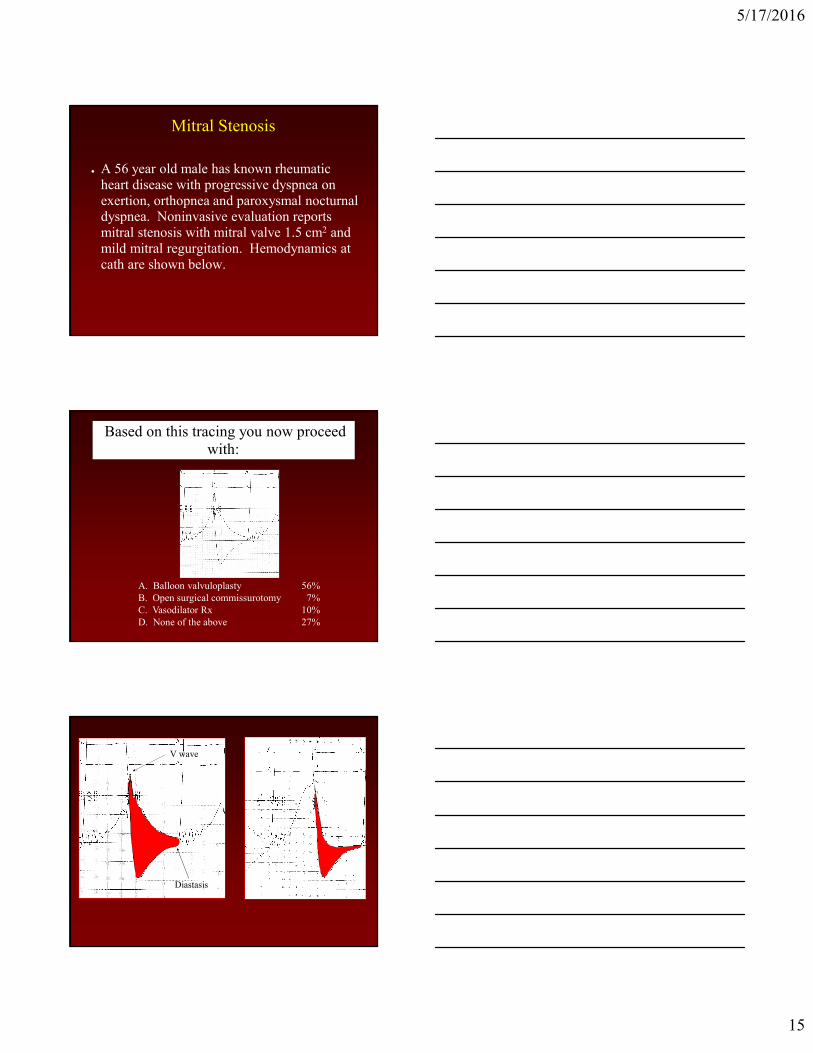
Mitral Stenosis
● A 56 year old male has known rheumatic
heart disease with progressive dyspnea on
exertion, orthopnea and paroxysmal nocturnal dyspnea. Noninvasive evaluation reports
mitral stenosis with mitral valve 1.5 cm2 and
mild mitral regurgitation. Hemodynamics at
cath are shown below.
Based on this tracing you now proceed
with:
A. Balloon valvuloplasty
B. Open surgical commissurotomy
C. Vasodilator Rx
D. None of the above
56%
7%
10%
27%
Diastasis
V wave
5/17/2016
16
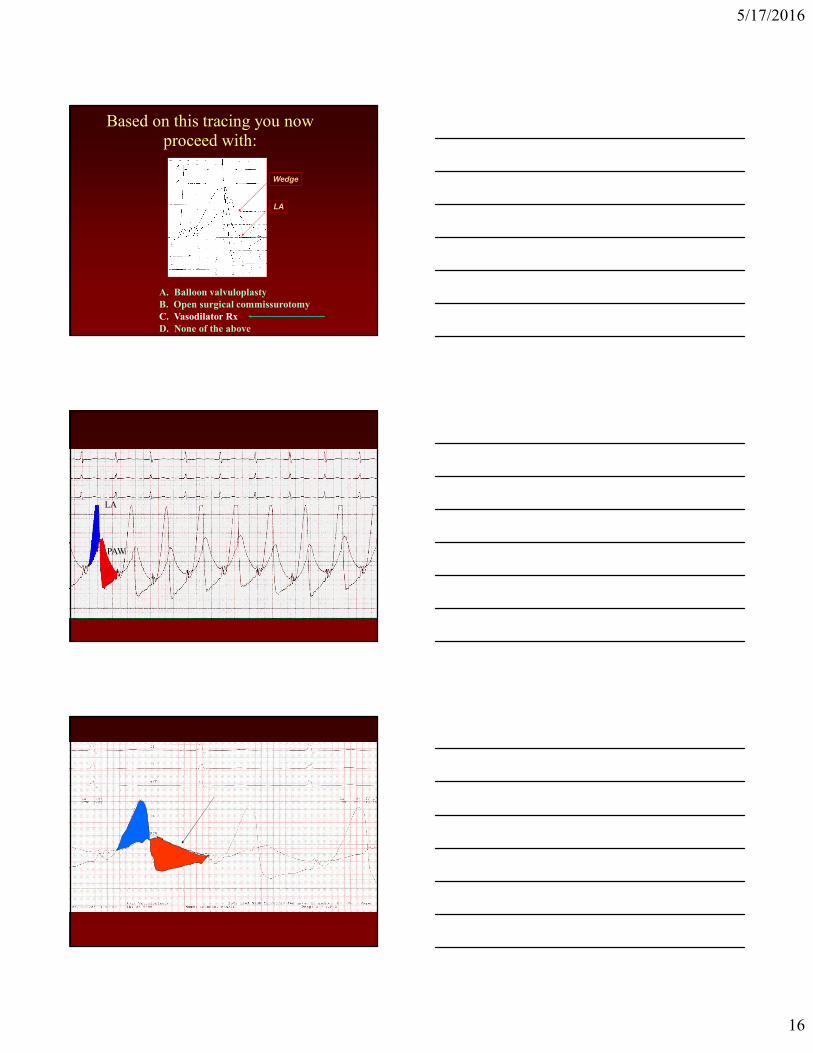
Based on this tracing you now
proceed with:
A. Balloon valvuloplasty
B. Open surgical commissurotomy
C. Vasodilator Rx
D. None of the above
LA
Wedge
LA
PAW
5/17/2016
17
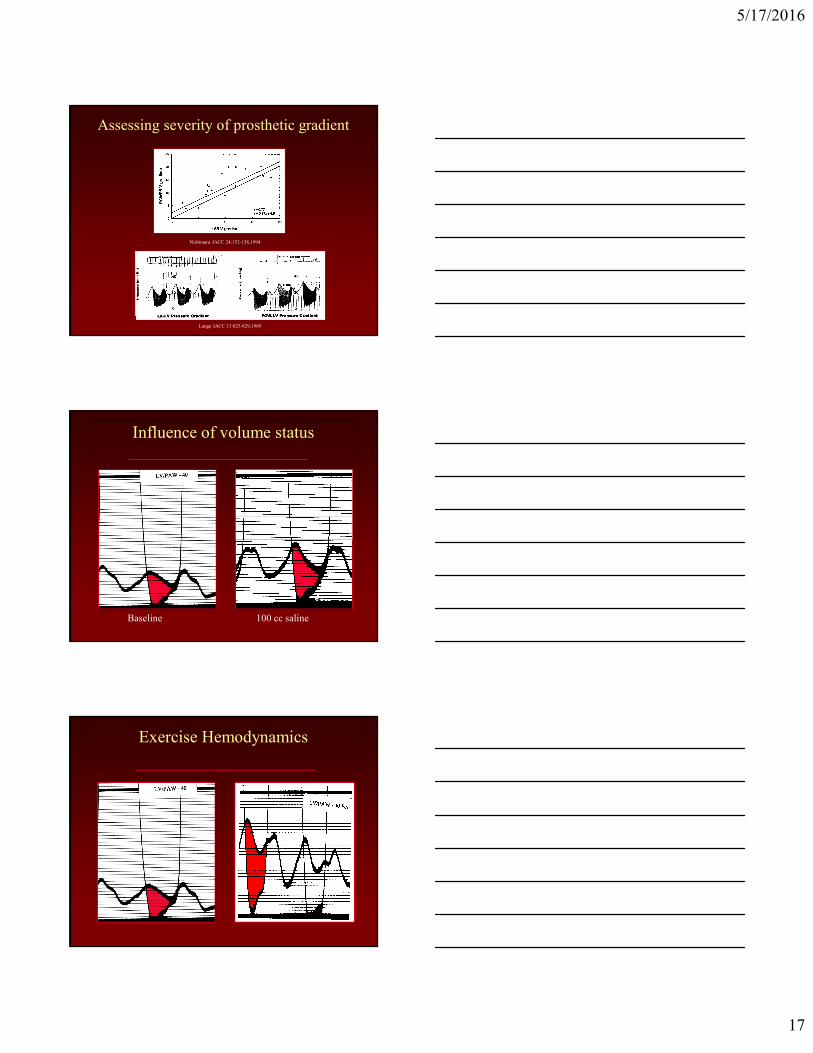
Assessing severity of prosthetic gradient
Lange JACC 13:825-829,1989
Nishimura JACC 24:152-158,1994
Influence of volume status
Baseline 100 cc saline
Exercise Hemodynamics
5/17/2016
18
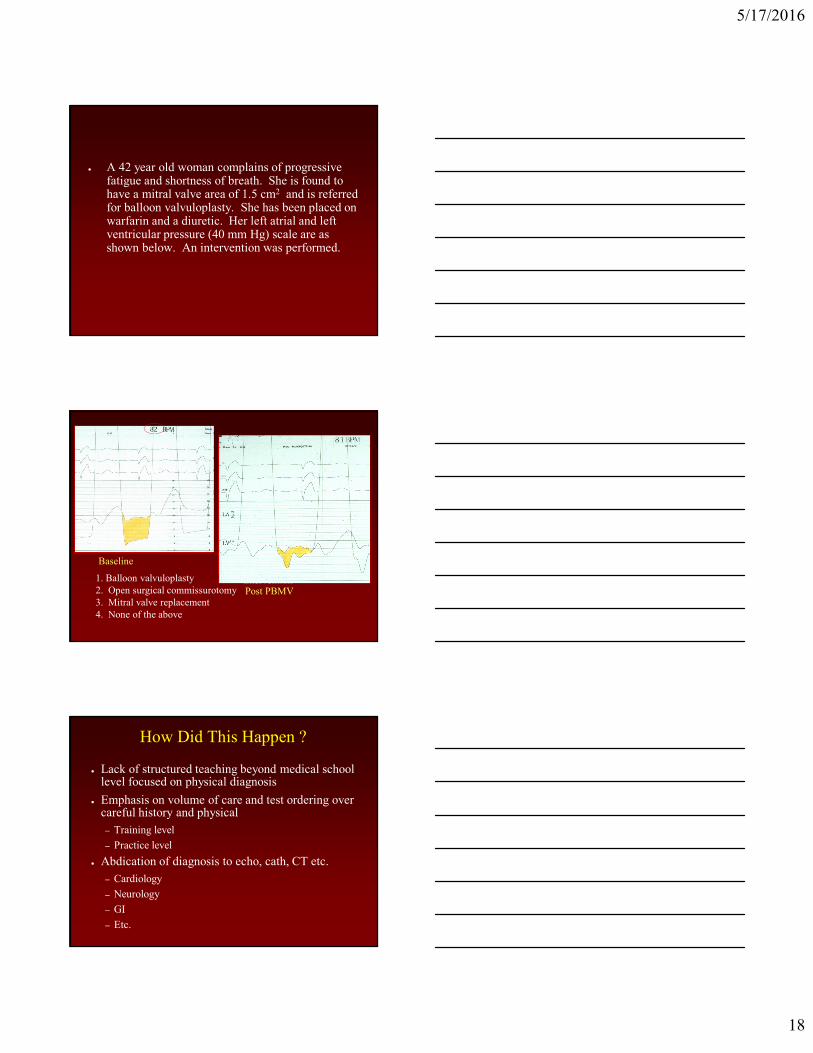
● A 42 year old woman complains of progressive fatigue and shortness of breath. She is found to have a mitral valve area of 1.5 cm2 and is referred for balloon valvuloplasty. She has been placed on warfarin and a diuretic. Her left atrial and left ventricular pressure (40 mm Hg) scale are as shown below. An intervention was performed.
Baseline
Intervention1. Balloon valvuloplasty
2. Open surgical commissurotomy
3. Mitral valve replacement
4. None of the above
Post PBMV
How Did This Happen ?
● Lack of structured teaching beyond medical school level focused on physical diagnosis
● Emphasis on volume of care and test ordering over careful history and physical
– Training level
– Practice level
● Abdication of diagnosis to echo, cath, CT etc.
– Cardiology
– Neurology
– GI
– Etc.

5/17/2016
19
AAIM Keynote Lecture Abraham Verghese
Auscultation
Age of Pericles 460 -
370 BC
Hippocrates succussion
splash
1578 - 1657 1628
“two clacks of a water bellows”
• Theophile Rene
Hyacinthe
Laennec - 1816
• “Could hear the
heart much more
clearly than if I
had applied my
ear directly”
Stethos = chest Skope = examination
5/17/2016
20
• Electrocardiogram –
1901
• Phonocardiogram -
1908
This is a plea for the sane use of every
means that may help in diagnosis,
including the stethoscope and all that it
stands for in the way of physical
diagnosis.
Physical examination should not yet be
regarded as displaced by electro-
cardiography . It still has a legitimate
function.
Herrick JB. In defense of the
stethoscope. Ann Intern Med. 1930
This is a plea for the sane use of every
means that may help in diagnosis,
including the stethoscope and all that it
stands for in the way of physical
diagnosis.
Heart catheterization should not yet be
regarded as displaced by echo-
cardiography. It still has a legitimate
function.
5/17/2016
21
● Only ¼ primary care residencies offer structured
teaching of cardiac auscultation
Mangione S. Academic Medicine 1998
The Era of Bedside Teaching Has
Largely Ended
Ability to Identify Murmurs and Extra
Heart Sounds
● 453 physicians in training -
Mangione S Am J Med 2001
5/17/2016
22
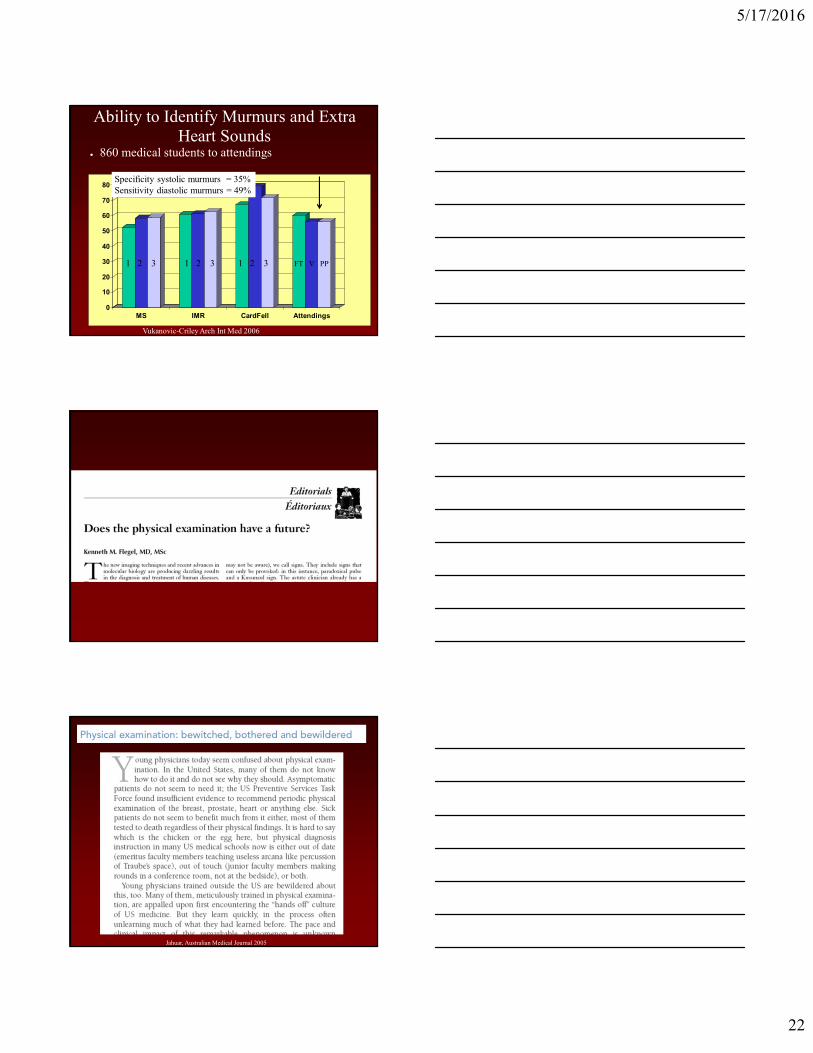
Ability to Identify Murmurs and Extra
Heart Sounds
0
10
20
30
40
50
60
70
80
MS IMR CardFell Attendings
● 860 medical students to attendings
1 2 3 1 2 3 1 2 3 FT V PP
Vukanovic-Criley Arch Int Med 2006
Specificity systolic murmurs = 35%
Sensitivity diastolic murmurs = 49%
Jahuar, Australian Medical Journal 2005
5/17/2016
23

5/17/2016
24
Would you teach auscultation this way ?
What the extraterrestrial might see
if he came to observe teaching rounds:
● Rounds removed from the living patient
● The purpose of admission is to render the live 3D
human into a 2D image
Verghese A, Horwitz R:
In Praise of the Physical Examination
BMJ 2009
5/17/2016
25
AAIM Keynote Lecture Abraham Verghese
Sir William Osler, 1st Baronet
● To learn medicine
without books is to sail
an uncharted sea;
● To learn medicine
without patients, is
never to have sailed at all.
● Time pressures
● Lack of access to “hard
data” while in the room
● Loss of (or never
learned) attending
physical diagnostic skills
● Lack of interest by
trainees
● And it’s just plain more comfortable to sit
in a room
5/17/2016
26
Fildes The Doctor Tate Gallery London
Medicine is an Art - 1880
- 2015
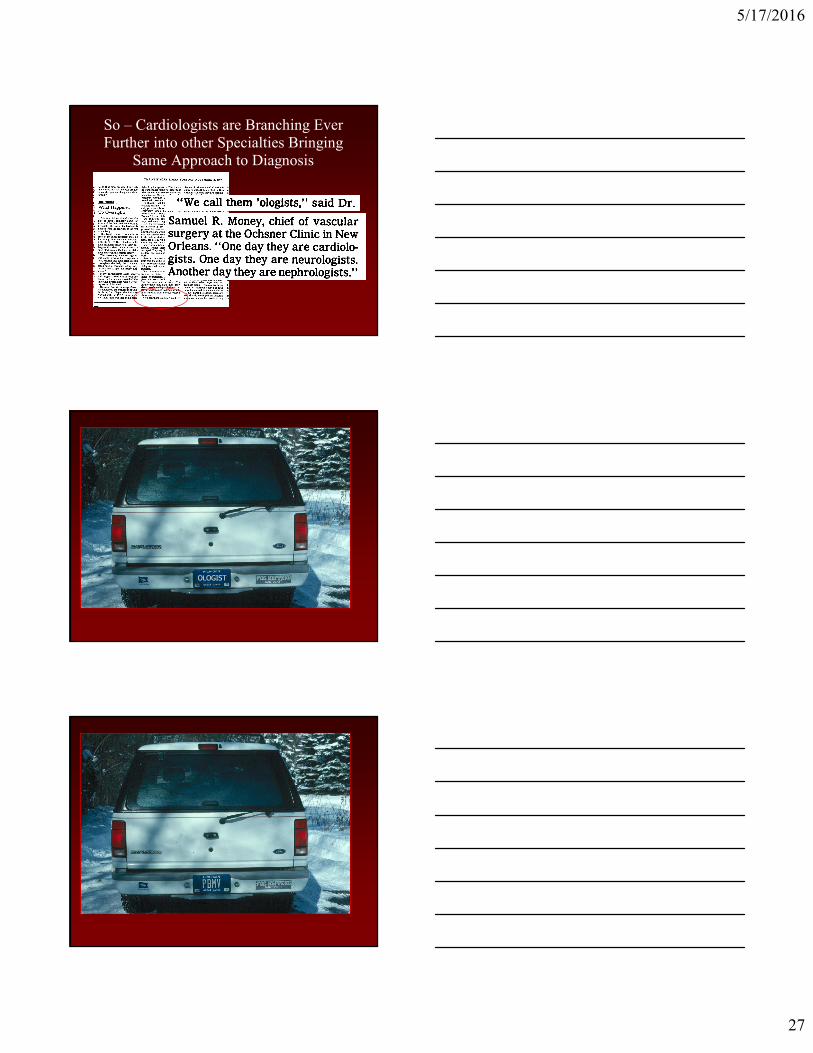
How are Cardiologists Rewarded?
0
50
100
150
200
250
300
350
400
x $
1,0
00
25th Median 75th 90th
Generalist
Echo
Intervention
Academic Benchmark Survery MBMA 2005
No surprise – only 13% of fellows surveyed by ACC
wanted to do general cardiology
5/17/2016
27
So – Cardiologists are Branching Ever
Further into other Specialties Bringing
Same Approach to Diagnosis
OLOGIST

5/17/2016
28
Internal Carotid Artery
Anterior Carotid
Middle Cerebral
• Can you name the
anatomy?
Don’t Be a Hyposkilliac
● Hyposkilliacs are cardiologists who:
– Cannot take an adequate medical history
– Cannot do a reliable physical exam
– Cannot critically assess information they gather
– Cannot create sound management plan
– Cannot reason with sophistication
– Cannot communicate
– Send patients off for “a bunch of tests”
Fred HL Texas Heart Institute Journal 2005
5/17/2016
29
5/17/2016
30
A. Verghese
6