Embed Size (px)
Citation preview

EPIDEMIOLOGY, INFECTIOUS DISEASE, INTRAPARTUM FETALASSESSMENT, OPERATIVE OBSTETRICS, OBSTETRIC QUALITY& SAFETY, PUBLIC HEALTH-GLOBAL HEALTH
Abstracts 537 – 686537 The risk of fetal death in undelivered patientsin the U.S. between 2003-2005: a comparisonof high-risk and low-risk cohortsAlicia Mandujano1, Thaddeus P. Waters1, Stephen A. Myers1
1MetroHealth Medical Center–Case Western Reserve University,Division of Maternal Fetal Medicine, Departmentof Obstetrics and Gynecology, Cleveland, OHOBJECTIVE: To describe the risk of stillbirth (SB) for undelivered pa-tients stratified by high-risk (HR) and low-risk (LR) status.STUDY DESIGN: This is a retrospective cohort analysis of birth and fetaldeath data between 2003-2005 from the U.S. National Center forHealth Statistics. We selected singletons between 34-42 wks gestationwith no fetal anomalies (N � 8,847,301). HR pregnancies includedmaternal anemia, cardiac, lung disease, diabetes, hemoglobinopathy,chronic hypertension, renal disease, or Rh sensitization. Correctionfor birth weight inconsistent with gestational age was included. Therisk of SB was calculated at each gestational age (GA) as: #SB thatoccurred at a given GA / (total deliveries at a GA � remaining unde-livered pregnancies). Data analyzed with SPSS.RESULTS: Our data included 8,847,301 subjects with 715,266 HR &8,083,325 LR. The number of fetuses beginning each week of gesta-tion, the number of live births, and the number of fetal deaths for theentire cohort are presented in the table. As gestational age increases,risk of SB increases. This trend was also noted in the HR and LRcohorts (data not shown). The graph depicts the risk of SB for eachgroup as gestational age increases. The risk of SB increases exponen-tially for each group, with greater SB risk in the HR cohort. The risk ofSB at 39 weeks was 1.9 times & 1.8 times higher in HR patients whencompared to LR & the cohort respectively.CONCLUSION: The risk of SB increases exponentially beyond 34 weeks;not only in LR patients, but up to 2 times more in HR patients. Deci-sions regarding timing of delivery should include data related to therisk of SB by remaining undelivered.
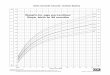
538 A comparison of the risk of stillbirth bybirth weight percentiles in a cohort of low-riskpatients in the U.S. between 2003-2005Alicia Mandujano1, Stephen A. Myers1, Thaddeus P. Waters1
1MetroHealth Medical Center–Case Western Reserve University,Division of Maternal Fetal Medicine, Departmentof Obstetrics and Gynecology, Cleveland, OHOBJECTIVE: To describe the risk of stillbirth (SB) for undelivered preg-nancies stratified by birth weight (BW) percentiles in women withoutknown medical conditions.STUDY DESIGN: This is a retrospective cohort analysis of birth and fetaldeath data between 2003-2005 from the U.S. National Center forHealth Statistics. We selected singletons between 34-42 wks gestationwith no fetal anomalies (N � 8,083,325). Data excluded maternalanemia, cardiac, lung disease, diabetes, hemoglobinopathy, chronichypertension, renal disease, or Rh sensitization. Correction for birthweight inconsistent with gestational age was included. The median�/� 100g at each GA served as the reference group. The 5%-tile and10%-tile were determined based upon the BW distribution at eachweek of gestation. The risk of SB was calculated at each gestational age(GA) as: #SB that occurred at a given GA / (total deliveries at a GA �remaining undelivered pregnancies). Data analyzed with SPSS.RESULTS: Our data included 8,083,325 low-risk (LR) pregnancies. Thenumber of fetuses beginning at each week of gestation, the number oflive births, and the number of fetal deaths for the median BW at eachGA are presented in the table. As gestational age increased, the risk ofSB increased further at the median BW. This trend was also noted forthe 10%-tile and 5%-tile (Figure 1), with the greatest risk of SB at the5%-tile. The risk of SB at 39 weeks was 3 times the risk at the 10%-tileand 5 times the risk at the 5%-tile when compared to the median.CONCLUSION: For women with no known medical conditions, the riskof being undelivered increases as GA increases and as BW percentiledecreases. These data support that for LR pregnancies, altered fetalgrowth is a significant risk that should be considered when timingdelivery.
Poster Session IV www.AJOG.orgFriday, February 10, 2012 • 3:30 pm – 5:30 pm • Marsalis Hall, Dallas Hyatt Regency
S244 American Journal of Obstetrics & Gynecology Supplement to JANUARY 2012

539 The effect of natural disasters on maternal morbidityAlissa Carver1, Marlo Cochran1, GayleOlson1, Mary Munn1, Gary Hankins2
1University of Texas Medical Branch, Ob/Gyn Maternal-FetalMedicine, Galveston, TX, 2The University of Texas MedicalBranch, Obsterics & Gynecology, Galveston, TXOBJECTIVE: Exposure to natural disasters may affect pregnancy out-comes. The objective of this study was to compare maternal morbidityin pregnancies prior to and following Hurricane Ike in September of2008.STUDY DESIGN: Retrospective case-control study examining triage vis-its to our institution over an 18-month period after Hurricane Ike(1/2009-6/2010) in comparison to pre-hurricane controls (3/2007-9/2008). 10/2008-12/2008 was excluded due to interruption of hospitalservices from storm damage. Antepartum complications were evalu-ated as follows: chronic hypertension (CHTN), pregnancy-inducedhypertension (PIH), diabetes (DM), vaginal bleeding (VB), pyelone-phritis, pancreatitis, cholecystitis, hyperemesis gravidarum/nauseaand vomiting (HEG/NV), oligohydramnios, preterm premature rup-ture of membranes (PPROM), threatened preterm labor (PTL), in-trauterine growth restriction (IUGR), decreased fetal movement (DecFM), and abnormal fetal testing. Comparison of demographic infor-mation, individual and composite maternal morbidity were calcu-lated using chi-squared and t-test analyses.RESULTS: Out of 21,202 triage visits, 11,280 (53%) occurred prior tothe storm and 9,922 (47%) after. Only 8 % of patients resided onGalveston Island while the remainder resided on the Texas mainlandwhere any impact from this natural disaster would be expected to beminimal. Composite maternal morbidity increased significantly fol-lowing Hurricane Ike (OR 1.53, 95% CI 1.44-1.63, p�0.0001). Whenexamined separately, this shift remained true for the following vari-ables: CHTN, DM, pyelonephritis, oligohydramnios, PPROM, DecFM, and abnormal fetal testing. Episodes of pancreatitis fell signifi-
cantly (Table 1). Despite a small proportion of patients originatingfrom Galveston proper, this effect was seen in our entire patient pop-ulation.CONCLUSION: Evidence suggests an overall increase in maternal com-plications based upon demand for care in a triage setting followingHurricane Ike. Clinicians should be prepared for increased morbidityand associated obstetric care requirements in pregnant women ex-posed to natural disasters.
540 Short interpregnancy intervals and maternalwell-being: the association with placental abruptionAllison Bryant1, Erin Madden2
1Massachusetts General Hospital, Vincent Obstetrics & Gynecology,Maternal Fetal Medicine, Boston, MA, 2Veteran’s HealthResearch Institute, NCIRE, San Francisco, CAOBJECTIVE: Short interpregnancy intervals (IPI) are associated withseveral adverse pregnancy outcomes such as preterm birth and fetaldeath. The risk of maternal complications is not clear. We sought todetermine whether short IPIs are associated with abnormal placenta-tion or bleeding complications of pregnancy.STUDY DESIGN: Data from vital statistics records for all births in Cali-fornia between 1999 and 2004 were linked with hospital dischargedata. For women with a first birth in 1999-2000 and a second birthbefore the end of 2004, multivariable modeling was used to determineassociations with placental abruption and placenta previa with IPI �6 months as the main risk factor of interest.RESULTS: 191,501 women met study inclusion criteria. Of these 1,538(0.8%) carried a diagnosis of placental abruption and 1,009 (0.5%)carried a diagnosis of placenta previa. After adjustment for potentialconfounders, IPI � 18 months. Adjustment for preexisting and preg-nancy-related hypertensive diagnoses did not change the point esti-mate for the effect of IPI on abruption risk. Placental abruption wasalso associated with having had no prenatal care during pregnancy,with operative delivery and with low birth weight and preterm birth.There was no association between IPI and placenta previa or antepar-tum hemorrhage.CONCLUSION: An interval of less than 6 months between a first andsecond pregnancy is associated with the diagnosis of placental abrup-tion in the second pregnancy, irrespective of hypertensive disorders.Placental dysfunction may be one mechanism by which a short IPIincreases the risk of preterm birth.
www.AJOG.org Epidemiology, Infectious Disease, Intrapartum Fetal Assessment, Operative Obstetrics, Obstetric Quality & Safety, Public Health-Global Health PosterSessionIV
Supplement to JANUARY 2012 American Journal of Obstetrics & Gynecology S245