Embed Size (px)
Citation preview
426 SPO Abstracts
557 A NOVEL THERAPEUTIC APPROACH FOR REFRACTORY HYPEREMESIS GRAVIDARUM
W Burrows S Zwickx , MA Krew, L Dierker, PM Catalano, MetroHealth Medical Center, Case Western Reserve University, Cleveland, Ohio
A two year retrospective analysis was done to evaluate the use of nasoalimentary feeding (Dobhoff tubes) in the therapy of severe hyperemesis gravidarum. At our institution, after an initial attempt to treat hyperemesis on an outpatient basis, failures are adm~ted for prolonged intravenous hydration and antiemetic therapy. Severe cases were unresponsive to this treatment or required multiple admissions. The charts of 55 patients w~h an admission diagnosis of hyperemesiS gravidarum were reviewed. Seven (13%) received nasoalimentary tube feedings. These 7 included patients w~h prior pregnancies involving intractable hyperemesis (5), prior elective abortion for hyperemesis (3), mu~iple admissions for hyperemesis in the index pregnancy (5) and prolonged admission over 7 days (7). These 7 patients had a mean of two admissions prior to in~iation of tube feedings. Five cases were considered to be successfully treated for intractable hyperemesis. Two cases were considered treatment failures. In one, the patient was unable to tolerate continued tube feedings, (but had no further hyperemesis). In the other case, symptom relief was transient w~h mu~iple subsequent admissions for hyperemesis. In all but this case, no further admissions were required after nasoalimentary feeding began. Two patients continued nasoalimentary therapy after discharge. One patient receiving nasoalimentry therapy electively aborted for a fetal anomaly (holoprosencephaly). Of the 48 who were treated in the standard fashion, 4 (8%) aborted because of hyperemesis. A prospective randomized study is being implemented to evaluate further this low cost alternative to central hyperalimentation.
558 DEPRESSIVE MOOD AT THE BEGINNING OF PREGNANCY. L.Duperron: J.F.Saucier: H.David: Dept. Ob/Gyn, Psychiatry, Saiote-Justine Hospital, Montreal, Canada.
The goal. of the study was to determine whether there are specific factors which· identify patients at iocreased risk for depression io early pregnancy. Four hundred and twelve primiparous (56.6 %) ·and secundiparous (43.4 %) were ioterviewed io early pregnancy, between the 10th and the 22nd week. They were from all social classes; 55.4% (N: 229) were married, 31.2% (N: 128) were io a stable relationship, 6.1 % (N: 25) were siogle, 1.5% (N: 6) were separated or divorced, 1.5 % (N: 6) were separated or divorced and remarried, and 4.4% (N: 18) were separated or divorced and liviog io a stable relationship. No relationship was found between the social class or the civil status and depressive mood, as measured by the short form of the Beck scale. On the other hand, the followiog situations io these pregnant women were significantly related to the presence of depressive mood: 1- Haviog a male child (among secundiparous subjects). 2- Beiog 35 to 39 of age (as compared with beiog 20 to 34). 3- Haviog a weak support system, especially if one fiods it unsatisfactory. 4- Haviog two disturbiog persons io their social environment who cannot be avoided. In addition, women whose parents were divorced when they were a child or a teenager, were more often ioclioed (p.07) to feel depressed when pregnant. Ongoiog siudies will determine whether these factors identify patients at iocreased risk of post-pactum depression.
January 1992 Am J Obstet Gynecol
559 SARCOIDOSIS IN PREGNANCY ~,Dept. Ob/Gyn,
561
Georgetown University School of Medicine, Washington ,DC Pulmonary sarcoid is a rare complication affecting at most
0.05:1; of pregnancies. Previously it has been suggested that no special management during pregnancy was necessary for patients with sarcoid since clinical status is rarely changed. We report 6 cases of adVanced sarcoidosis occurring between 1985 and 1991 complicating pregnancy. Two patients having undergone pulmonary resections for progressive cavitary disease with one of these patients subsequently developing HIV infection potentially from blood transfusion at the time of surgery. serial pulmonary function testing revealed reduced vital capacity for all patients. Additionally, there frequently was a signiflcant impairment of diffusing capacity. While the use of steroids should not be withheld, 50:1; of steroid users developed carbohydrate intolerance requiring either diet or insulin therapy. There were no maternal deaths but there was 100:1; maternal morbidity from a high frequency of infection with staphylococcus aureus or other pathologiC organisms. There was a 16:1; incidence of perinatal mortal1ty( stillbirth) with a higher than expected frequency of smaller infants. The flnding of secondary pulmonary hypertension in two patients underscores the importance of serial cardiovascular assessment. In both patients the development of pulmonary hypertenSion was not discovered until the middle of the third trimester. While physical examination is often suggestive of pulmonary hypertenSion, the utility of echocardiography and right heart catheterization will be discussed. A clinical management scheme will be presented.
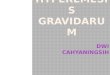
MILD GLUCOSE INTOLERANCE AND PERINATAL OUTCOME s. Colemanx, B. Campbell, P. Roussis, G. Harllisonx, s. Cox University of Kentucky, Lexington, KY
This retrospective review was to determine pregnancy complications associated with mild glucose intolerance defined by an abnonnal 50 gram glucose screen but a normal 3 hour oral glucose tolerance test (OGlT). During a 34 month period, 822 glucose screens were positive (one hour glucose 2140 mg/dl). Of these, 594 (72%) had a normal OGTI, 108 (13%) had one abnormal value, and 120 (15%) were found to have two or more abnormal values (ie. gestational OM). The study consists of 200 normal controls and 100 patients from each group from which delivery data was available. There was no difference in gestational age at delivery, five minute Apgar scores, or shoulder dystocia (Table). Although the incidence of macrosomia in the normal group (10%) was higher than expected, patients with one abnormal value of the OGTI had a significantly higher risk (19%, P<O.Ol) as did those with two abnormal values (16%, P<O.05). The incidence of cesarean section was also significantly higher in these two groups of patients. The results suggest that women with mild glucose intolerance (as evidenced by one abnormal OGTI value) are susceptible to the same pregnancy complications as those with gestational diabetes. These pregnancies have a two-fold increase risk of fetal macrosomia and cesarean section when compared to normal controls. Therefore, it would seem reasonable to incorporate a more aggressive approach to mild glucose intolerance in an attempt to further decrease perinatal morllidity. Patients with an abnormal screen followed by a normal 3 hour OGTI were also noted to have an increase in incidence of macrosomia. This could represent false negative oral glucose tolerance tests and warrants further study to evaluate perinatal morllidity and its prevention in this group. Table I Control NI 3' OGTT 1 Abol. Gest. D.M.
N = 200 N = 100 N = 100 N=I00
Macrosomia 19 (9.5%) 13 19** 16* Cesarean section 24 (12%) 11 20+ 31*** ForcepslV acuum 8 (4%) 11 10 5 Preeclampsia 12 (6%) 7 6 3
• P<0.05 ** P<O.Ol **. P<O.ool +p = 0.09




![[PPT]Hyperemesis Gravidarum - Philadelphia University …philadelphia.edu.jo/academics/aalrazek/uploads... · Web viewHyperemesis Gravidarum Learning objective Identify Hyperemesis](https://img.pdfslide.net/doc/110x75/5af587257f8b9a190c8e7497/ppthyperemesis-gravidarum-philadelphia-university-viewhyperemesis-gravidarum.jpg)