Embed Size (px)
Citation preview

Research Article5G Edge Computing Enabled Directional Data Collection forMedical Community Electronic Health Records
Xiaoqiang Yan 1 and Xiaogang Ren 12
113e Affiliated Changshu Hospital of Soochow University (Changshu No 1 Peoplersquos Hospital) Jiangsu 215500 ChangshuSuzhou China2China University of Mining Technology Jiangsu 221116 Xuzhou China
Correspondence should be addressed to Xiaogang Ren lb20060005cumteducn
Received 2 March 2021 Revised 13 May 2021 Accepted 9 July 2021 Published 23 July 2021
Academic Editor Khin wee Lai
Copyright copy 2021 Xiaoqiang Yan and Xiaogang Ren is is an open access article distributed under the Creative CommonsAttribution License which permits unrestricted use distribution and reproduction in anymedium provided the original work isproperly cited
It is important to promote the development and application of hospital information system community health service system etcHowever it is difficult to realize the intercommunication between various information systems because it is not enough to realizethe in-depth management of health information To address these issues we design the 5G edge computing-assisted architecturefor medical communityen we formulate the directional data collection (DDC) problem to gather the EMRHER data from themedical community to minimize the service error under the deadline constraint of data collection deadline Moreover we designthe data direction prediction algorithm (DDPA) to predict the data collection direction and propose the data collection planningalgorithm (DCPA) tominimize the data collecting time costrough the numerical simulation experiments we demonstrate thatour proposed algorithms can decrease the total time cost by 6248 and improve the data quality by 3647 through the designedsystem respectively
1 Introduction
Recently the core role of smart medicine is the constructionof hospital information platform based on electronicmedical records and regional health information platformwith residentrsquos electronic health records [1] Electronichealth records [2] can improve the phenomenon of infor-mation asymmetry between doctors and patients and satisfythe demand-oriented development of medical service re-form e construction of electronic health records is thefocus of future smart medicine [3] which can not onlysatisfy the diversity requirements of medical and healthreform but also accelerate and strengthen the developmentof information technology in medical and health institu-tions Recently the vigorous development of informationtechnology in Chinarsquos medical and health industry has givenbirth to the vigorous development and application of hos-pital information system (HIS) community health servicesystem (CHSS) and other information systems However it
is difficult to realize the intercommunication between var-ious information systems because it is not enough to realizethe in-depth management of health information
e National Health Commission of the Peoplersquos Re-public of China [4] is committed to promoting the 5G-assisted medical action project On the basis of medical andhealth information it can promote not only the imple-mentation of hierarchical diagnosis and treatment but alsothe reform of public medical institutions and public healthmanagement mode en 5G-assisted medical care aims toimprove the efficiency of medical institutions and integratehigh-quality medical resources such as electronic healthrecords (EHRs) [5] overcoming the shortcoming of tradi-tional medical services and enabling patients and improvingthe upgrading of traditional medical service mode
e scientific and technological application of medicalcommunity [6] electronic health records have beenattracting the attention of many researchers and enterprisesReference [7] compared achievement of and improvement
HindawiJournal of Healthcare EngineeringVolume 2021 Article ID 5598077 12 pageshttpsdoiorg10115520215598077
in quality standards for diabetes at practices using EHRswith those at practices using paper records Reference [7]examined the effects of electronic health records on thesafety of patients in medical facilities Reference [8] analyzedthe costs and benefits of EHRs in six community healthcenters (CHCs) that serve disadvantaged patients
However the above researches do not deeply study therequirements and data characteristics of medical communityplatform for EHR management In terms of credibilityreliability and real-time it is necessary to deeply study thedirectional collection mechanism of archival data such aslarge-scale mobile terminal sensing under 5G diversifiedarchival data collection and archival information sharingunder the medical community
So there are some major challenges as follows
(i) e diversity and complexity of medical communityseriously restrict the classification efficiency andmarking accuracy of medical community electronichealth records data which affects the intelligentmanagement efficiency of EHRs
(ii) e differences of medical level and service objectsbetween different medical institutions in the med-ical community make the sharing of electronicrecords which is an important basis for specialistcollaboration more complex e low efficient andprecision data sharing will seriously restrict themedical communityrsquos ability to solve major diseasesand it is difficult to form a complementary devel-opment mode
(iii) How to accurately and timely collect the data ofmedical community electronic health record man-agement has become a difficult problem because it isdifficult to predict which medical structure willproduce what type of electronic health record dataat what time
Our key contributions can be summarized as follows
(i) We design the 5G edge computing-assisted archi-tecture for medical community
(ii) We formulate the directional data collection (DDC)problem to gather the EMRHER data from themedical community with minimizing the serviceerror under the deadline constraint of datacollection
(iii) We design the data direction prediction algorithm(DDPA) to predict the data collection direction andpropose the data collection planning algorithm(DCPA) to minimize the data collecting time cost
(iv) We conduct extensive simulations for the designedsystem and proposed algorithms e results showthat our proposed algorithms can decrease the totaltime cost by 6248 and improve the data quality by6995 through the designed system respectively
e rest of the paper is organized as follows We reviewthe state-of-the-art research in Section 2 We design the 5G-assisted edge computing system in Section 3 We present the
system model and formulate the DDC problem in Section 4We design the intelligent data collection scheme with theassistance of random forest for solving the DDC problem inSection 5 We conduct the simulations in Section 6 Weconclude this work in Section 7
2 Related Work
e current situation of medical archives management in themedical community is discussed as follows Reference [9]found the significant deficiencies in the practice of warfarinmanagement and suggestive evidence that anticoagulationservices can partially ameliorate these deficiencies Reference[10] described a randomized trial of a program to identifyand treat depression among high utilizers of general medicalcare Reference [11] designed an intelligent archive man-agement system by integrating 5G network and Internet ofings for smart hospitals Reference [12] used the exomesequencing for infants in intensive care units to determinethe diagnostic yield and use of clinical exome sequencing incritically ill infants Reference [13] proposed a novel drugsupply chain management using hyper ledger fabric basedon block-chain technology to handle secure drug supplychain records
About the status of data collection reference [14]extracted security data that plays an important role indetecting security anomaly toward security measurementReference [15] provided a theoretical model of privacy inwhich data collection requires the consent of consumers whoare fully aware of the consequences of consent Reference[16] considered a scenario where an unmanned aerial vehiclecollects data from a set of sensors on a straight line Ref-erence [17] proposed a low redundancy data collectionscheme to reduce the delay as well as energy consumptionfor monitoring network by using matrix completion tech-nique Reference [18] proposed a practical framework calledPrivacy Protector patient privacy-protected data collectionwith the objective of preventing these types of attacks
3 5G-Assisted Edge Computing System
First of all according to the requirements of medicalcommunity e-health records management based on thecomplex environment of regional medical institutions in-formation platform we design the mathematical model ofe-health records management and its 5G application systemframework Secondly by deploying multiple mobile ter-minal nodes we design the medical community electronichealth records management 5G architecture to provide real-time and reliable communication guarantee for large-scalemedical community electronic health records data appli-cation business en in order to ensure the real-time andreliability of data sharing of medical community electronichealth records a massive data collection mechanism basedon edge computing is established Finally based on theabove requirements we combine the large-scale mobilecommunication of 5G with the massive data real-timecollection technology of edge computing to study the ap-
2 Journal of Healthcare Engineering
plication mechanism of data directional collection so as toprovide the reliability credibility and feasibility guaranteefor the data update and sharing application of medicalcommunity electronic health records management
According to the requirements of regional medical in-stitutions information platform construction we analyze theinformation interconnection and regional differences be-tween community health service centers and municipalhospitals en we introduce edge computing into 5Gthrough the organic allocation and deep integration betweenthe mobile terminals and cloud computing server e edgecomputing reasonably allocates the storage computing andnetwork services resources between the computing centerand the mobile terminals so as to achieve the local optimaldivision of labor and cooperation before the network servicequality and user experience quality erefore the intro-duction of edge computing into 5G can satisfy the com-puting and communication needs of mobile terminals withdistributed and random characteristics Hence edge com-puting can well solve the geographical deployment char-acteristics of 5G nodes scattered between community healthservice centers and municipal hospitals Moreover the edgecomputing architecture with 5G is shown in Figure 1 Herethe 5G platform is the center ie the municipal hospital andseveral subnets of edge community service center aredeployede network control ability of these center subnetsis the same as that of the servers in the platform where thearchitecture can effectively reduce the calculation delay andimprove the storage efficiency of medical communityelectronic health record data
e 5G architecture shown in Figure 1 can provideconvenient services health management services traditionalChinese medicine (TCM) health care services and otherservices is architecture can give full play to its advantagesin data sharing and family doctor follow-up continuouslyimprove the accessibility and effectiveness of servicescomprehensively improve service level and satisfaction andprovide medical services and health management services tothe majority of residents conveniently and quickly At thesame time the medical community platform can solve thefollowing problem lack of medical resources shortagedifficulty to see a doctor and realize the integration of healthresources and then improve the level of primary health carethrough the establishment of complete electronic healthrecords for residents en we integrate the sharing ofmedical records and test results medical images medicationrecords and patientsrsquo basic health information betweensecondary and tertiary comprehensive medical institutionsin the community to realize the sharing of high-qualitymedical resources in the region
With the rapid development of 5G edge terminals usedto collect electronic health records data how to reasonablyallocate and effectively recover the diversity resources of 5Ghas become a key problem In 5G environment the dis-tribution and recovery of resources and the reconstructionof network topology are dynamic ere is an unknownmapping and interference relationship between 5G real-timeresource statistics computing task resource allocation and
task scheduling and 5G network edge computing terminaltrusted resource information ese relationships are real-time and random It is the main goal of network resourcemanagement to make 5G system execution efficiency andresource utilization always in the best state It is well knownthat 5G supports a large amount of traffic e resourcerequest queue is very easy to overflow which makes thearrival rate and processing efficiency of resource requestsignaling and computing task control signaling between thenetwork control center and the edge terminal irregular andthe reliability of resource allocation and computing taskunbalanced among different services In order to improvethe instantaneous resource management level of 5G and theutilization rate of global resources and make 5G bettercommunication support for medical community electronichealth records management we design the 5G edge com-puting architecture as shown in Figure 2 where we deployedwith multiple edge terminals multiple autonomous basestations and multiple autonomous control networks
In Figure 2 edge computing terminals share EHR in-formation and exchange unified standard data sourcesthrough regional platform interfaces of medical institutionsAccording to the edge computing architecture shown inFigure 2 medical institutions improve the interconnectionarchitecture of regional health information platform andguide the electronic medical record system and electronichealth record management system of medical institutionsunder their jurisdiction In particular electronic healthrecords need to achieve unified data interface standards ofmedical institutions medical insurance community andother related systems so as to facilitate information sharing
e common data element established in the 5G controlcenter of medical community can efficiently improve thereal-time sharing efficiency of electronic medical record(EMR) and EHR erefore the electronic medical recordsand electronic health records storage system of medicalinstitutions in medical community must follow the stan-dardized description of national public health data elementattributes describe the extracted data element attributesconduct business modeling and realize data sharingMedical institutions at all levels should use the ID number asthe main identification code for the transmission and cir-culation of information in the diagnosis and treatment ofpublic health services in the business system so as to ensurethe effective collection of archival information Each edgecomputing terminal server should ensure the validity andtimeliness of data transmission verification processtracking and traceability so as to ensure that all kinds ofinformation can be uploaded to 5G information platformtimely accurately and comprehensively
erefore how to collect and improve data from thecommunity and medical institutions at all levels in accor-dance with the electronic medical record informationstandards and unified specification of disease coding andother important databases to ensure the quality of data hasbecome the key of medical community archives manage-ment e process of data collection should have the fol-lowing properties
Journal of Healthcare Engineering 3
Control center of 5G
Medical community
Edgecomputing
terminal
Edgecomputingterminal
Information sharingplatform of EHR
EHR
EHR
Figure 2 5G edge computing architecture for medical community
5G
Medicalcommunity
Medicalcommunity
ResidentMedical
community
Medicalcommunity
Figure 1 5G architecture for medical community
4 Journal of Healthcare Engineering
(i) e process of data collection should be based onthe main index of patient identity correctly asso-ciated with the previous diagnosis and treatmentdata and form a complete and standardized medicalrecord file which is convenient for medical staff touse
(ii) e process of data collection should be carried outaccording to the interface specification of regionalinformation platform e diagnosis and treatmentinformation should be uploaded and collected intohealth records in time
(iii) e process of data collection should implement thecodes of clinical symptoms diagnosis surgerydrugs inspection and so on released by the state toensure the standardization and unification of di-agnosis and treatment information uploaded to theplatform
Figure 3 gives a toy example for the Directional DataCollection and application of medical community electronichealth record with the above characteristics In this scenariocloud platform edge computing terminal and 5G platformare effectively integrated into the directional data collectionof medical community electronic health records such ascommunity classification data directional collection anddata storage
e edge computing procedure is illustrated as follows
(1) e communities generate their EMRHER datawhich can be collected by a corresponding oppor-tunistically encountered edge computing terminal
(2) e edge computing terminal analyzes andmines thevalid information from collected EMRHER dataeg the location resident ID and hisher historicalrecords en the dataset is sent to the cloud serversin real time e edge computing terminal predictstheir medical demand according to the historicalrecords by using the algorithm proposed in Section41 and returns the prediction results to the 5G cloudservers
(3) e 5G cloud servers periodically compute the datacollection route via the algorithms in Section 42 fordata collection terminal according to the informa-tion of communities and residents from edgecomputing terminals
(4) e data is collected by the data collection terminalthrough the route calculated in the above step
4 Directional Data Collection forMedical Community
41 SystemModel Suppose that the 5G platform of medicalcommunity includes m medical institutions and n com-munities According to the scope of service and medicallevel the mapping relationship between each communityand different medical institutions is established denoted byC cij1113966 1113967
mn
i1j1 Here the electronic file data is generated bythe medical institutions according to the community it
serves which is used to obtain the medical needs andfeedback of residents Note that each medical institutioninitiates one data collection task in the time dimension SoT ti1113864 1113865
m
i1 denotes the task set For convenience we definethe data collection process as follows
Definition 1 (data collection task) e process of edgecomputing terminal completing data collection task is toselect the corresponding observation values from a series ofcandidate data samples corresponding to the community for5G platform
For each data collection task ti we assume that it has acandidate sample set Ai shown as follows
Ai ai(1) ai(2) ai Ai
111386811138681113868111386811138681113868111386811138681113872 11138731113966 1113967 (1)
en let ai(0) denote the optimal data sample corre-sponding to the task ti erefore the data error caused bytask ti can be calculated by
ei 1Ai
11138681113868111386811138681113868111386811138681113868
1113944
Ai| |
k1ai(k) minus ai(0)⎛⎜⎝ ⎞⎟⎠ (2)
e resident set who provides the EMRHER datasetfrom all communities can be represented as follows
Bi bji1113966 1113967
n
j1 (3)
Here bji represents the data in task ti which is provided
by the j-th community when the i-th task is initiated by i-thmedical institution when there is the mapping relationshipbelonging to C So we can calculate the data matrix cor-responding to data collection tasks from all communitiesthrough the following equation
5G networks
Cloud servers
EHR data collection
EHR data collection
EHR data collection
Medical community
Community
Community
Edge computing terminal
Figure 3 Application of directional data collection with the as-sistance of 5G and edge computing system
Journal of Healthcare Engineering 5
A aij1113966 1113967mn
i1j1
1113945m
i1Ai minus eiBi( 1113857
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus eiBi⎛⎜⎝ ⎞⎟⎠
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus ei 1113944
n
j1b
ji
⎛⎜⎝ ⎞⎟⎠
(4)
Here we redefine the data sample ai(k) in Ai as ai(k)twhich is calculated according to the time dependence of edgecomputing Note that we can update the mapping rela-tionship between each community and different medicalinstitutions through the following equation
cij
0 if 0ltaij
ei
lt cij
1 ifaij
ei
ge cij
⎧⎪⎪⎪⎪⎪⎨
⎪⎪⎪⎪⎪⎩
(5)
Here cij is the tolerance threshold of the data collectionerror which is a given empirical value
In order to analyze the direction accuracy of data col-lection conveniently we give the following definition of datacollection aggregation reliability
Definition 2 (data collection task) For m data collectiontasks and n communities the direction of data collection isaccurate when each task satisfies the following conditions
(1) e i-th task and j-th community have the mappingrelationship ie cij 1
(2) Ai and Bi have the same rank for each task ti(3) All the data samples collected by all the medical
institutions have consistency ie the followingfunction f(A) is valid
f(A) limn⟶infin
limm⟶infinA
1113936iiprime1 riprime + 1113936eisinTi
te
(6)
(4) Let Γ(ti) denote the data collection time cost etime cost of the i-th task is not larger than thedeadline τi
42 Problem Formulation e objective of directional datacollection (DDC) problem is to design a data collectionscheme based on 5G edge computing system to gather theEMRHER data from the medical community to minimizethe service error under the deadline constraint of datacollection xij is a binary variable to indicate whether data of
task ti is collected from j-th community xij 1 if data oftask ti is collected from j-th community xij 0 otherwise
e DDC problem can be formulated as follows
DDCmin xij 1113944
m
i1ei
st
(a) xij isin 0 1 forallti isin T
(b) r Ai( 1113857 r Bi( 1113857 forallti isin T
(c) 1113945m
i11113945
n
j1cij 1
(d) Γ ti( 1113857le τi forallti isin T
(7)
Constraint (a) gives the value range of xij Constraint (b)ensures that the rank of candidate data sample set is equal tothat of data in task ti on the basis of C Constraint (c) ensuresthat each mapping between the task and its correspondingcommunity is valid Constraint (d) ensures that the time costof data collection in each task is not larger than its deadline
We list the frequently used notations in Table 1
5 Intelligent Data Collection Scheme
In this section we propose our 5G edge computing enableddirectional data collection (5EDDC) algorithm en thedetailed description of the proposed algorithm is presentedin two phases data direction prediction and data collectionplanning
51 Data Direction Prediction Algorithm Medical behaviorsand requirements of residents in different communitiesactually reflect the regeneration direction of EMR whichcontains a lot of medical information such as commondiseases and medical habits Based on the implementation ofa variant of algorithms [19] we design Algorithm 1 forsolving the problem of data direction prediction
First we predict the medical behavior of residentsthrough the following steps
Step 1 Feature extraction takes into account the fol-lowing features for each behavior in community gen-erating along the historical records Bi with the last datacollection task ti and candidate sample set Ai of currentmedical community time of day medical behaviorstarting time medical community name and its loca-tion resident ID and medical treatment time of eachlocation e above procedure is denoted as functionFeature Extraction(dataset)Step 2 Random forest-based prediction needs the inputvector nt representing the information of a residentwhich includes the origin community and destinationmedical institute as well as the corresponding extractedfeatures from step 1 en the data generating time ofany community can be predicted based on temporal
6 Journal of Healthcare Engineering
data dependencies and spatial data correlations eabove process is denoted as function RandomForests
Second we can predict the data direction of communityfor collecting data via the Interval-based Historical Average(IHA) [20] as shown in the following equation
IHA E ta1113858 1113859 λ( 1113857 1
2λ + 11113944
λ
pminusλ1113944
days
q1tp minus E ta1113858 1113859 minus q1113872 1113873⎛⎝ ⎞⎠ (8)
Here E[ta] is the expectation of data generating time oftask ta based on historical EMRHER data λ is the meanabsolute error of the random forests [21] for data generatingtime prediction and days is the days of historical EMREHRdataset tp is the first data collection starting time afterE[ta] + q in the p-th day of the dataset where E[ta] + q is thegenerating time of EMRHER data for recording residents ina-th community at the q-th day us tp minus E[ta] minus q is thehistorical data collection time on the q-th day Finally wecalculate the EMREHR data generating time of commu-nities and data collection direction of medical community
In Algorithm 1 the Sink(F B) function is used to find allthe data collection sinks of EMREHR at its medical com-munity In addition Algorithm 1 updates all the datasamples and records between any two communities andcomputes their collecting time through the following steps
(1) Find all ai which can satisfy the tolerance(2) Extract all the features from historical dataset
52 Data Collection Planning Algorithm Based on the di-rection prediction of data collection the DDC problem isequivalent to finding a data route to collect the EMRHERdata for all selected medical communities with minimumtime cost e above data collection planning (DCP)problem can be formulated as follows
DCPmin 1113944C
01Γ to( 1113857 (9)
Moreover we design the data collection planning al-gorithm (DCPA) to solve the DCP probleme basic idea isgiven as follows (see Algorithm 2)
(1) Transform Ai and integrate into 1113957A (line 5)(2) Update 1113957B (line 6)(3) For each element in 1113957B we first divide it into two
separate sets P1 and P2 and then remove half ofelements in 1113957B (lines 8ndash10) and then find the cor-responding subroutes (lines 11ndash14)
(4) Integrate all the subroutes into the final data col-lection planning P (lines 15ndash18) where the symbol ⊎represents the integration of some routes
6 Numerical Experiments
In this section we conduct extensive simulations to verifythe performance of our proposed algorithms with differentnumber of medical institutions number of communitiesdays of month and number of residents of a community
61DataDescription e dataset used in our experiments isfrom the electronic records system of Changshu No 1Peoplersquos Hospital e dataset shows a kind of representativemedical community data It is generated by the medicalcommunity supported by Changshu No 1 Peoplersquos Hospitalwhich covers the period from January 1 2018 to November30 2018 e dataset includes the record data of medicalinstitute and residents and GPS data of medical institutese data record contains various fields such as time of daymedical behavior starting time medical community nameand its location resident ID medical treatment time of each
Table 1 Frequently used notations
Notation Descriptioncij Mapping relationship between i-th community and j-th different medical institutionC Set of mappingsti i-th data collection taskT Set of tasksAi Set of candidate data samples belonging to i-th taskai(k) k-th data sample in Ai
|Ai| Size of data sample in Ai
ai(0) Optimal data sample corresponding to task ti
ei Data error caused by task ti
bji Data in task ti provided by the j-th community when the i-th task is initiated by i-th medical institution
Bi Set of data in task ti on the basis of C
ai(k)t k-th data sample calculated according to the time dependence of edge computingcij Tolerance threshold of the data collection error between the i-th task and j-th communityf(A) Consistence functionτi Deadline of task ti
Journal of Healthcare Engineering 7
location and the number of patients of the correspondingmedical institute etc e GPS data contains latitude lon-gitude and treatment time of medical institute
62 Simulation Setup andBenchmark We assume that thereare 10 medical institutions to provide medical care for 10communities which are supported by Changshu No 1Peoplersquos Hospital e residents receive medical treatmentfrom the above medical institutions In our simulation weevaluate the total time cost of data collection and dataquality calculated by equation (2) All the simulations wererun on a cloud server ECS [23] with 12-core Intel XeonPlatinum 8269CY and 48GB memory e other parametersettings of our simulations are listed in Table 2
We develop the data collection algorithm DCA in [22] asthe benchmark algorithm for comparison which can makean efficient tradeoff between the data collection efficiency
and energy consumption through the combination of theenergy of the emotional device wireless device
63 Performance Evaluation In this subsection we evaluatethe performance of our algorithms and DCA in the scenarioshown in Figure 4 Tables 3 and 4 give the locations ofmedical institutions and communities in the area respec-tively e above information is calculated based on GoogleMaps
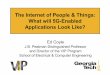
Figure 5 shows the prediction errors on two differentdays ie March 10 2018 and October 20 2018 e pre-diction results demonstrate the effectiveness of our proposedprediction algorithm DDPA e average prediction erroron March 10 2018 and October 20 2018 is 321 and193 respectively
Figures 6 and 7 show the impact of medical institutionson total time cost and data quality of our algorithms and
Input T datasetOutput A B
(1) for i 2 tom do(2) ei⟵ (1|Ai|)(1113936
|Ai |
k1 ai(k) minus ai(0))
(3) Ai⟵ ai|ai lt ei1113864 1113865(4) for j 1 to n do(5) b
ji⟵ ai(j)
(6) for each a isin A do(7) F⟵ Feature Extraction(dataset)(8) B⟵ Sink(F B)(9) for each b isin B do(10) (A B)⟵ RandomForests(F A B)
ALGORITHM 1 Data direction prediction algorithm (DDPA)
Input A B
Output P
(1) count⟵ 0 1113954A⟵A 1113957B⟵empty
(2) while countle log B minus 1 do(3) for i 1 tom do(4) for j 1 to n do(5) 1113957A⟵ 1113957ai(1) 1113957ai(2) 1113957ai(|Ai|)1113864 1113865
(6) 1113957B⟵ 1113957bj
i1113882 1113883cup 1113957B
(7) for each 1113957b isin 1113957B do(8) Take (|1113957B|2) elements to P1(9) Take another (|1113957B|2) elements to P2(10) Remove (|1113957B|2) elements from 1113957B(11) Find subroute pcount
1 of P1(12) Pcount
1 ⟵ Pcount1 cup pcount
11113864 1113865(13) Find subroute pcount
2 of P2(14) Pcount
2 ⟵ Pcount2 cup pcount
21113864 1113865(15) for each p1 isin P1 do(16) P⟵ P ⊎ p11113864 1113865(17) for each p2 isin P2 do(18) P⟵ P ⊎ p21113864 1113865
ALGORITHM 2 Data Collection Planning Algorithm (DCPA)
8 Journal of Healthcare Engineering
DCA respectively e average total time cost of our al-gorithms and DCA is 885 hours and 244 hours respec-tivelye average data quality of our algorithms and DCA is7576 and 9475 respectively e results show that ouralgorithms can reduce 7238 of total time cost of DCA onaverage and improve 2506 of data quality of DCA re-spectively is indicates that the proposed algorithmssignificantly outperform DCA is is because the dataquality of our algorithms is better than the those obtained byDCA respectively
Figures 8 and 9 show the impact of communities on totaltime cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 575 hours and 163 hours respectively eaverage data quality of our algorithms and DCA is 7327and 9759 respectively e results show that our
Table 2 Parameter settings
Parameter Valuen 10m 10|T| 10cij [001 005]τi [1 10] hours|Ai| [100 500]
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Figure 4 Medical community for EMRHER data collection ered nodes represent locations of medical institutions and the greennodes represent locations of communities
Table 3 Locations of medical institutions
i Longitude Latitude1 31629934025445163 120745726947073172 31637070592885376 120744987234992693 31641308857555806 120742605433500614 31644304755694158 1207431204176075 31639559503878488 120739966849915396 3163350810894618 120741081938852527 31634421579375328 120735202536971168 31640051243952147 120743342172446979 3163600474671818 1207442755811459110 31640862982947134 12074781351639375
Table 4 Locations of communities
i Longitude Latitude1 31633639306384033 120736407142357452 31635638094098336 120744138979835573 3164162333734517 120746486600514814 31638983794798012 120748808703562535 31641820359193588 120738421187636156 3163745217402931 120743756215726587 31643893501251643 120747443511151158 3163659402090503 1207420720531559 31634475760812066 1207435393159863510 31634834238968633 12074956147326746
7 8 9 10 11 12 13 14 15 16 170
2
4
6
8
Time
Pred
ictio
n er
ror (
)
March 10 2018
October 20 2018
Figure 5 Prediction errors on March 10 2018 and October 202018
2 4 6 8 10
5
10
15
Number of medical institutions
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 6 Total time cost vs number of medical institutions
Journal of Healthcare Engineering 9
algorithms reduces 7167 of total time cost of DCA onaverage and improves 3320 of data quality of DCArespectively
Figures 10 and 11 show the impact of days of month ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 1615 hours and 999 hours respectively eaverage data quality of our algorithms and DCA is 6331and 9401 respectively e results show that our
algorithms can reduce 3812 of total time cost of DCA onaverage and improve 4849 of data quality of DCArespectively
Figures 12 and 13 show the impact of communities ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 892 hours and 286 hours respectively eaverage data quality of our algorithms and DCA is 6844and 9521 respectively e results show that our
2 4 6 8 1050
60
70
80
90
100
Number of medical institutions
Dat
a qua
lity
()
DCAOurs
Figure 7 Data quality vs number of medical institutions
2 4 6 8 10
2
4
6
8
10
Number of communities
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 8 Total time cost vs number of communities
10 Journal of Healthcare Engineering
algorithms can reduce 6776 of total time cost of DCA onaverage and improve 3911 of data quality of DCArespectively
Overall our algorithms can significantly decrease thetotal time cost and improve the data quality through thedesigned data direction prediction algorithm and datacollection planning algorithm
7 Conclusion
In this article we have designed the 5G edge computingarchitecture for medical community to improve the effec-tiveness and efficiency of EMREHR data collection Firstwe formulate the directional data collection (DDC) problemto gather the EMRHER data from the medical communityfor minimizing the service error under the deadline con-straint of data collection deadline Second we design thedata direction prediction algorithm (DDPA) to predict thedata collection direction and propose the data collection
10 15 2050
60
70
80
90
100
Days of month
Dat
a qua
lity
()
DCAOurs
Figure 11 Data quality vs days of month
20 40 60 80 1000
2
4
6
8
10
12
Number of residents of a community
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 12 Total time cost vs number of residents of a community
20 40 60 80 10060
70
80
90
100
Number of residents of a community
Dat
a qua
lity
()
DCAOurs
Figure 13 Data quality vs number of residents of a community
2 4 6 8 1060
70
80
90
100
Number of communities
Dat
a qua
lity
()
DCAOurs
Figure 9 Data quality vs number of communities
10 15 208
10
12
14
16
18
20
Days of month
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 10 Total time cost vs days of month
Journal of Healthcare Engineering 11
planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering

in quality standards for diabetes at practices using EHRswith those at practices using paper records Reference [7]examined the effects of electronic health records on thesafety of patients in medical facilities Reference [8] analyzedthe costs and benefits of EHRs in six community healthcenters (CHCs) that serve disadvantaged patients
However the above researches do not deeply study therequirements and data characteristics of medical communityplatform for EHR management In terms of credibilityreliability and real-time it is necessary to deeply study thedirectional collection mechanism of archival data such aslarge-scale mobile terminal sensing under 5G diversifiedarchival data collection and archival information sharingunder the medical community
So there are some major challenges as follows
(i) e diversity and complexity of medical communityseriously restrict the classification efficiency andmarking accuracy of medical community electronichealth records data which affects the intelligentmanagement efficiency of EHRs
(ii) e differences of medical level and service objectsbetween different medical institutions in the med-ical community make the sharing of electronicrecords which is an important basis for specialistcollaboration more complex e low efficient andprecision data sharing will seriously restrict themedical communityrsquos ability to solve major diseasesand it is difficult to form a complementary devel-opment mode
(iii) How to accurately and timely collect the data ofmedical community electronic health record man-agement has become a difficult problem because it isdifficult to predict which medical structure willproduce what type of electronic health record dataat what time
Our key contributions can be summarized as follows
(i) We design the 5G edge computing-assisted archi-tecture for medical community
(ii) We formulate the directional data collection (DDC)problem to gather the EMRHER data from themedical community with minimizing the serviceerror under the deadline constraint of datacollection
(iii) We design the data direction prediction algorithm(DDPA) to predict the data collection direction andpropose the data collection planning algorithm(DCPA) to minimize the data collecting time cost
(iv) We conduct extensive simulations for the designedsystem and proposed algorithms e results showthat our proposed algorithms can decrease the totaltime cost by 6248 and improve the data quality by6995 through the designed system respectively
e rest of the paper is organized as follows We reviewthe state-of-the-art research in Section 2 We design the 5G-assisted edge computing system in Section 3 We present the
system model and formulate the DDC problem in Section 4We design the intelligent data collection scheme with theassistance of random forest for solving the DDC problem inSection 5 We conduct the simulations in Section 6 Weconclude this work in Section 7
2 Related Work
e current situation of medical archives management in themedical community is discussed as follows Reference [9]found the significant deficiencies in the practice of warfarinmanagement and suggestive evidence that anticoagulationservices can partially ameliorate these deficiencies Reference[10] described a randomized trial of a program to identifyand treat depression among high utilizers of general medicalcare Reference [11] designed an intelligent archive man-agement system by integrating 5G network and Internet ofings for smart hospitals Reference [12] used the exomesequencing for infants in intensive care units to determinethe diagnostic yield and use of clinical exome sequencing incritically ill infants Reference [13] proposed a novel drugsupply chain management using hyper ledger fabric basedon block-chain technology to handle secure drug supplychain records
About the status of data collection reference [14]extracted security data that plays an important role indetecting security anomaly toward security measurementReference [15] provided a theoretical model of privacy inwhich data collection requires the consent of consumers whoare fully aware of the consequences of consent Reference[16] considered a scenario where an unmanned aerial vehiclecollects data from a set of sensors on a straight line Ref-erence [17] proposed a low redundancy data collectionscheme to reduce the delay as well as energy consumptionfor monitoring network by using matrix completion tech-nique Reference [18] proposed a practical framework calledPrivacy Protector patient privacy-protected data collectionwith the objective of preventing these types of attacks
3 5G-Assisted Edge Computing System
First of all according to the requirements of medicalcommunity e-health records management based on thecomplex environment of regional medical institutions in-formation platform we design the mathematical model ofe-health records management and its 5G application systemframework Secondly by deploying multiple mobile ter-minal nodes we design the medical community electronichealth records management 5G architecture to provide real-time and reliable communication guarantee for large-scalemedical community electronic health records data appli-cation business en in order to ensure the real-time andreliability of data sharing of medical community electronichealth records a massive data collection mechanism basedon edge computing is established Finally based on theabove requirements we combine the large-scale mobilecommunication of 5G with the massive data real-timecollection technology of edge computing to study the ap-
2 Journal of Healthcare Engineering
plication mechanism of data directional collection so as toprovide the reliability credibility and feasibility guaranteefor the data update and sharing application of medicalcommunity electronic health records management
According to the requirements of regional medical in-stitutions information platform construction we analyze theinformation interconnection and regional differences be-tween community health service centers and municipalhospitals en we introduce edge computing into 5Gthrough the organic allocation and deep integration betweenthe mobile terminals and cloud computing server e edgecomputing reasonably allocates the storage computing andnetwork services resources between the computing centerand the mobile terminals so as to achieve the local optimaldivision of labor and cooperation before the network servicequality and user experience quality erefore the intro-duction of edge computing into 5G can satisfy the com-puting and communication needs of mobile terminals withdistributed and random characteristics Hence edge com-puting can well solve the geographical deployment char-acteristics of 5G nodes scattered between community healthservice centers and municipal hospitals Moreover the edgecomputing architecture with 5G is shown in Figure 1 Herethe 5G platform is the center ie the municipal hospital andseveral subnets of edge community service center aredeployede network control ability of these center subnetsis the same as that of the servers in the platform where thearchitecture can effectively reduce the calculation delay andimprove the storage efficiency of medical communityelectronic health record data
e 5G architecture shown in Figure 1 can provideconvenient services health management services traditionalChinese medicine (TCM) health care services and otherservices is architecture can give full play to its advantagesin data sharing and family doctor follow-up continuouslyimprove the accessibility and effectiveness of servicescomprehensively improve service level and satisfaction andprovide medical services and health management services tothe majority of residents conveniently and quickly At thesame time the medical community platform can solve thefollowing problem lack of medical resources shortagedifficulty to see a doctor and realize the integration of healthresources and then improve the level of primary health carethrough the establishment of complete electronic healthrecords for residents en we integrate the sharing ofmedical records and test results medical images medicationrecords and patientsrsquo basic health information betweensecondary and tertiary comprehensive medical institutionsin the community to realize the sharing of high-qualitymedical resources in the region
With the rapid development of 5G edge terminals usedto collect electronic health records data how to reasonablyallocate and effectively recover the diversity resources of 5Ghas become a key problem In 5G environment the dis-tribution and recovery of resources and the reconstructionof network topology are dynamic ere is an unknownmapping and interference relationship between 5G real-timeresource statistics computing task resource allocation and
task scheduling and 5G network edge computing terminaltrusted resource information ese relationships are real-time and random It is the main goal of network resourcemanagement to make 5G system execution efficiency andresource utilization always in the best state It is well knownthat 5G supports a large amount of traffic e resourcerequest queue is very easy to overflow which makes thearrival rate and processing efficiency of resource requestsignaling and computing task control signaling between thenetwork control center and the edge terminal irregular andthe reliability of resource allocation and computing taskunbalanced among different services In order to improvethe instantaneous resource management level of 5G and theutilization rate of global resources and make 5G bettercommunication support for medical community electronichealth records management we design the 5G edge com-puting architecture as shown in Figure 2 where we deployedwith multiple edge terminals multiple autonomous basestations and multiple autonomous control networks
In Figure 2 edge computing terminals share EHR in-formation and exchange unified standard data sourcesthrough regional platform interfaces of medical institutionsAccording to the edge computing architecture shown inFigure 2 medical institutions improve the interconnectionarchitecture of regional health information platform andguide the electronic medical record system and electronichealth record management system of medical institutionsunder their jurisdiction In particular electronic healthrecords need to achieve unified data interface standards ofmedical institutions medical insurance community andother related systems so as to facilitate information sharing
e common data element established in the 5G controlcenter of medical community can efficiently improve thereal-time sharing efficiency of electronic medical record(EMR) and EHR erefore the electronic medical recordsand electronic health records storage system of medicalinstitutions in medical community must follow the stan-dardized description of national public health data elementattributes describe the extracted data element attributesconduct business modeling and realize data sharingMedical institutions at all levels should use the ID number asthe main identification code for the transmission and cir-culation of information in the diagnosis and treatment ofpublic health services in the business system so as to ensurethe effective collection of archival information Each edgecomputing terminal server should ensure the validity andtimeliness of data transmission verification processtracking and traceability so as to ensure that all kinds ofinformation can be uploaded to 5G information platformtimely accurately and comprehensively
erefore how to collect and improve data from thecommunity and medical institutions at all levels in accor-dance with the electronic medical record informationstandards and unified specification of disease coding andother important databases to ensure the quality of data hasbecome the key of medical community archives manage-ment e process of data collection should have the fol-lowing properties
Journal of Healthcare Engineering 3
Control center of 5G
Medical community
Edgecomputing
terminal
Edgecomputingterminal
Information sharingplatform of EHR
EHR
EHR
Figure 2 5G edge computing architecture for medical community
5G
Medicalcommunity
Medicalcommunity
ResidentMedical
community
Medicalcommunity
Figure 1 5G architecture for medical community
4 Journal of Healthcare Engineering
(i) e process of data collection should be based onthe main index of patient identity correctly asso-ciated with the previous diagnosis and treatmentdata and form a complete and standardized medicalrecord file which is convenient for medical staff touse
(ii) e process of data collection should be carried outaccording to the interface specification of regionalinformation platform e diagnosis and treatmentinformation should be uploaded and collected intohealth records in time
(iii) e process of data collection should implement thecodes of clinical symptoms diagnosis surgerydrugs inspection and so on released by the state toensure the standardization and unification of di-agnosis and treatment information uploaded to theplatform
Figure 3 gives a toy example for the Directional DataCollection and application of medical community electronichealth record with the above characteristics In this scenariocloud platform edge computing terminal and 5G platformare effectively integrated into the directional data collectionof medical community electronic health records such ascommunity classification data directional collection anddata storage
e edge computing procedure is illustrated as follows
(1) e communities generate their EMRHER datawhich can be collected by a corresponding oppor-tunistically encountered edge computing terminal
(2) e edge computing terminal analyzes andmines thevalid information from collected EMRHER dataeg the location resident ID and hisher historicalrecords en the dataset is sent to the cloud serversin real time e edge computing terminal predictstheir medical demand according to the historicalrecords by using the algorithm proposed in Section41 and returns the prediction results to the 5G cloudservers
(3) e 5G cloud servers periodically compute the datacollection route via the algorithms in Section 42 fordata collection terminal according to the informa-tion of communities and residents from edgecomputing terminals
(4) e data is collected by the data collection terminalthrough the route calculated in the above step
4 Directional Data Collection forMedical Community
41 SystemModel Suppose that the 5G platform of medicalcommunity includes m medical institutions and n com-munities According to the scope of service and medicallevel the mapping relationship between each communityand different medical institutions is established denoted byC cij1113966 1113967
mn
i1j1 Here the electronic file data is generated bythe medical institutions according to the community it
serves which is used to obtain the medical needs andfeedback of residents Note that each medical institutioninitiates one data collection task in the time dimension SoT ti1113864 1113865
m
i1 denotes the task set For convenience we definethe data collection process as follows
Definition 1 (data collection task) e process of edgecomputing terminal completing data collection task is toselect the corresponding observation values from a series ofcandidate data samples corresponding to the community for5G platform
For each data collection task ti we assume that it has acandidate sample set Ai shown as follows
Ai ai(1) ai(2) ai Ai
111386811138681113868111386811138681113868111386811138681113872 11138731113966 1113967 (1)
en let ai(0) denote the optimal data sample corre-sponding to the task ti erefore the data error caused bytask ti can be calculated by
ei 1Ai
11138681113868111386811138681113868111386811138681113868
1113944
Ai| |
k1ai(k) minus ai(0)⎛⎜⎝ ⎞⎟⎠ (2)
e resident set who provides the EMRHER datasetfrom all communities can be represented as follows
Bi bji1113966 1113967
n
j1 (3)
Here bji represents the data in task ti which is provided
by the j-th community when the i-th task is initiated by i-thmedical institution when there is the mapping relationshipbelonging to C So we can calculate the data matrix cor-responding to data collection tasks from all communitiesthrough the following equation
5G networks
Cloud servers
EHR data collection
EHR data collection
EHR data collection
Medical community
Community
Community
Edge computing terminal
Figure 3 Application of directional data collection with the as-sistance of 5G and edge computing system
Journal of Healthcare Engineering 5
A aij1113966 1113967mn
i1j1
1113945m
i1Ai minus eiBi( 1113857
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus eiBi⎛⎜⎝ ⎞⎟⎠
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus ei 1113944
n
j1b
ji
⎛⎜⎝ ⎞⎟⎠
(4)
Here we redefine the data sample ai(k) in Ai as ai(k)twhich is calculated according to the time dependence of edgecomputing Note that we can update the mapping rela-tionship between each community and different medicalinstitutions through the following equation
cij
0 if 0ltaij
ei
lt cij
1 ifaij
ei
ge cij
⎧⎪⎪⎪⎪⎪⎨
⎪⎪⎪⎪⎪⎩
(5)
Here cij is the tolerance threshold of the data collectionerror which is a given empirical value
In order to analyze the direction accuracy of data col-lection conveniently we give the following definition of datacollection aggregation reliability
Definition 2 (data collection task) For m data collectiontasks and n communities the direction of data collection isaccurate when each task satisfies the following conditions
(1) e i-th task and j-th community have the mappingrelationship ie cij 1
(2) Ai and Bi have the same rank for each task ti(3) All the data samples collected by all the medical
institutions have consistency ie the followingfunction f(A) is valid
f(A) limn⟶infin
limm⟶infinA
1113936iiprime1 riprime + 1113936eisinTi
te
(6)
(4) Let Γ(ti) denote the data collection time cost etime cost of the i-th task is not larger than thedeadline τi
42 Problem Formulation e objective of directional datacollection (DDC) problem is to design a data collectionscheme based on 5G edge computing system to gather theEMRHER data from the medical community to minimizethe service error under the deadline constraint of datacollection xij is a binary variable to indicate whether data of
task ti is collected from j-th community xij 1 if data oftask ti is collected from j-th community xij 0 otherwise
e DDC problem can be formulated as follows
DDCmin xij 1113944
m
i1ei
st
(a) xij isin 0 1 forallti isin T
(b) r Ai( 1113857 r Bi( 1113857 forallti isin T
(c) 1113945m
i11113945
n
j1cij 1
(d) Γ ti( 1113857le τi forallti isin T
(7)
Constraint (a) gives the value range of xij Constraint (b)ensures that the rank of candidate data sample set is equal tothat of data in task ti on the basis of C Constraint (c) ensuresthat each mapping between the task and its correspondingcommunity is valid Constraint (d) ensures that the time costof data collection in each task is not larger than its deadline
We list the frequently used notations in Table 1
5 Intelligent Data Collection Scheme
In this section we propose our 5G edge computing enableddirectional data collection (5EDDC) algorithm en thedetailed description of the proposed algorithm is presentedin two phases data direction prediction and data collectionplanning
51 Data Direction Prediction Algorithm Medical behaviorsand requirements of residents in different communitiesactually reflect the regeneration direction of EMR whichcontains a lot of medical information such as commondiseases and medical habits Based on the implementation ofa variant of algorithms [19] we design Algorithm 1 forsolving the problem of data direction prediction
First we predict the medical behavior of residentsthrough the following steps
Step 1 Feature extraction takes into account the fol-lowing features for each behavior in community gen-erating along the historical records Bi with the last datacollection task ti and candidate sample set Ai of currentmedical community time of day medical behaviorstarting time medical community name and its loca-tion resident ID and medical treatment time of eachlocation e above procedure is denoted as functionFeature Extraction(dataset)Step 2 Random forest-based prediction needs the inputvector nt representing the information of a residentwhich includes the origin community and destinationmedical institute as well as the corresponding extractedfeatures from step 1 en the data generating time ofany community can be predicted based on temporal
6 Journal of Healthcare Engineering
data dependencies and spatial data correlations eabove process is denoted as function RandomForests
Second we can predict the data direction of communityfor collecting data via the Interval-based Historical Average(IHA) [20] as shown in the following equation
IHA E ta1113858 1113859 λ( 1113857 1
2λ + 11113944
λ
pminusλ1113944
days
q1tp minus E ta1113858 1113859 minus q1113872 1113873⎛⎝ ⎞⎠ (8)
Here E[ta] is the expectation of data generating time oftask ta based on historical EMRHER data λ is the meanabsolute error of the random forests [21] for data generatingtime prediction and days is the days of historical EMREHRdataset tp is the first data collection starting time afterE[ta] + q in the p-th day of the dataset where E[ta] + q is thegenerating time of EMRHER data for recording residents ina-th community at the q-th day us tp minus E[ta] minus q is thehistorical data collection time on the q-th day Finally wecalculate the EMREHR data generating time of commu-nities and data collection direction of medical community
In Algorithm 1 the Sink(F B) function is used to find allthe data collection sinks of EMREHR at its medical com-munity In addition Algorithm 1 updates all the datasamples and records between any two communities andcomputes their collecting time through the following steps
(1) Find all ai which can satisfy the tolerance(2) Extract all the features from historical dataset
52 Data Collection Planning Algorithm Based on the di-rection prediction of data collection the DDC problem isequivalent to finding a data route to collect the EMRHERdata for all selected medical communities with minimumtime cost e above data collection planning (DCP)problem can be formulated as follows
DCPmin 1113944C
01Γ to( 1113857 (9)
Moreover we design the data collection planning al-gorithm (DCPA) to solve the DCP probleme basic idea isgiven as follows (see Algorithm 2)
(1) Transform Ai and integrate into 1113957A (line 5)(2) Update 1113957B (line 6)(3) For each element in 1113957B we first divide it into two
separate sets P1 and P2 and then remove half ofelements in 1113957B (lines 8ndash10) and then find the cor-responding subroutes (lines 11ndash14)
(4) Integrate all the subroutes into the final data col-lection planning P (lines 15ndash18) where the symbol ⊎represents the integration of some routes
6 Numerical Experiments
In this section we conduct extensive simulations to verifythe performance of our proposed algorithms with differentnumber of medical institutions number of communitiesdays of month and number of residents of a community
61DataDescription e dataset used in our experiments isfrom the electronic records system of Changshu No 1Peoplersquos Hospital e dataset shows a kind of representativemedical community data It is generated by the medicalcommunity supported by Changshu No 1 Peoplersquos Hospitalwhich covers the period from January 1 2018 to November30 2018 e dataset includes the record data of medicalinstitute and residents and GPS data of medical institutese data record contains various fields such as time of daymedical behavior starting time medical community nameand its location resident ID medical treatment time of each
Table 1 Frequently used notations
Notation Descriptioncij Mapping relationship between i-th community and j-th different medical institutionC Set of mappingsti i-th data collection taskT Set of tasksAi Set of candidate data samples belonging to i-th taskai(k) k-th data sample in Ai
|Ai| Size of data sample in Ai
ai(0) Optimal data sample corresponding to task ti
ei Data error caused by task ti
bji Data in task ti provided by the j-th community when the i-th task is initiated by i-th medical institution
Bi Set of data in task ti on the basis of C
ai(k)t k-th data sample calculated according to the time dependence of edge computingcij Tolerance threshold of the data collection error between the i-th task and j-th communityf(A) Consistence functionτi Deadline of task ti
Journal of Healthcare Engineering 7
location and the number of patients of the correspondingmedical institute etc e GPS data contains latitude lon-gitude and treatment time of medical institute
62 Simulation Setup andBenchmark We assume that thereare 10 medical institutions to provide medical care for 10communities which are supported by Changshu No 1Peoplersquos Hospital e residents receive medical treatmentfrom the above medical institutions In our simulation weevaluate the total time cost of data collection and dataquality calculated by equation (2) All the simulations wererun on a cloud server ECS [23] with 12-core Intel XeonPlatinum 8269CY and 48GB memory e other parametersettings of our simulations are listed in Table 2
We develop the data collection algorithm DCA in [22] asthe benchmark algorithm for comparison which can makean efficient tradeoff between the data collection efficiency
and energy consumption through the combination of theenergy of the emotional device wireless device
63 Performance Evaluation In this subsection we evaluatethe performance of our algorithms and DCA in the scenarioshown in Figure 4 Tables 3 and 4 give the locations ofmedical institutions and communities in the area respec-tively e above information is calculated based on GoogleMaps
Figure 5 shows the prediction errors on two differentdays ie March 10 2018 and October 20 2018 e pre-diction results demonstrate the effectiveness of our proposedprediction algorithm DDPA e average prediction erroron March 10 2018 and October 20 2018 is 321 and193 respectively
Figures 6 and 7 show the impact of medical institutionson total time cost and data quality of our algorithms and
Input T datasetOutput A B
(1) for i 2 tom do(2) ei⟵ (1|Ai|)(1113936
|Ai |
k1 ai(k) minus ai(0))
(3) Ai⟵ ai|ai lt ei1113864 1113865(4) for j 1 to n do(5) b
ji⟵ ai(j)
(6) for each a isin A do(7) F⟵ Feature Extraction(dataset)(8) B⟵ Sink(F B)(9) for each b isin B do(10) (A B)⟵ RandomForests(F A B)
ALGORITHM 1 Data direction prediction algorithm (DDPA)
Input A B
Output P
(1) count⟵ 0 1113954A⟵A 1113957B⟵empty
(2) while countle log B minus 1 do(3) for i 1 tom do(4) for j 1 to n do(5) 1113957A⟵ 1113957ai(1) 1113957ai(2) 1113957ai(|Ai|)1113864 1113865
(6) 1113957B⟵ 1113957bj
i1113882 1113883cup 1113957B
(7) for each 1113957b isin 1113957B do(8) Take (|1113957B|2) elements to P1(9) Take another (|1113957B|2) elements to P2(10) Remove (|1113957B|2) elements from 1113957B(11) Find subroute pcount
1 of P1(12) Pcount
1 ⟵ Pcount1 cup pcount
11113864 1113865(13) Find subroute pcount
2 of P2(14) Pcount
2 ⟵ Pcount2 cup pcount
21113864 1113865(15) for each p1 isin P1 do(16) P⟵ P ⊎ p11113864 1113865(17) for each p2 isin P2 do(18) P⟵ P ⊎ p21113864 1113865
ALGORITHM 2 Data Collection Planning Algorithm (DCPA)
8 Journal of Healthcare Engineering
DCA respectively e average total time cost of our al-gorithms and DCA is 885 hours and 244 hours respec-tivelye average data quality of our algorithms and DCA is7576 and 9475 respectively e results show that ouralgorithms can reduce 7238 of total time cost of DCA onaverage and improve 2506 of data quality of DCA re-spectively is indicates that the proposed algorithmssignificantly outperform DCA is is because the dataquality of our algorithms is better than the those obtained byDCA respectively
Figures 8 and 9 show the impact of communities on totaltime cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 575 hours and 163 hours respectively eaverage data quality of our algorithms and DCA is 7327and 9759 respectively e results show that our
Table 2 Parameter settings
Parameter Valuen 10m 10|T| 10cij [001 005]τi [1 10] hours|Ai| [100 500]
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Figure 4 Medical community for EMRHER data collection ered nodes represent locations of medical institutions and the greennodes represent locations of communities
Table 3 Locations of medical institutions
i Longitude Latitude1 31629934025445163 120745726947073172 31637070592885376 120744987234992693 31641308857555806 120742605433500614 31644304755694158 1207431204176075 31639559503878488 120739966849915396 3163350810894618 120741081938852527 31634421579375328 120735202536971168 31640051243952147 120743342172446979 3163600474671818 1207442755811459110 31640862982947134 12074781351639375
Table 4 Locations of communities
i Longitude Latitude1 31633639306384033 120736407142357452 31635638094098336 120744138979835573 3164162333734517 120746486600514814 31638983794798012 120748808703562535 31641820359193588 120738421187636156 3163745217402931 120743756215726587 31643893501251643 120747443511151158 3163659402090503 1207420720531559 31634475760812066 1207435393159863510 31634834238968633 12074956147326746
7 8 9 10 11 12 13 14 15 16 170
2
4
6
8
Time
Pred
ictio
n er
ror (
)
March 10 2018
October 20 2018
Figure 5 Prediction errors on March 10 2018 and October 202018
2 4 6 8 10
5
10
15
Number of medical institutions
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 6 Total time cost vs number of medical institutions
Journal of Healthcare Engineering 9
algorithms reduces 7167 of total time cost of DCA onaverage and improves 3320 of data quality of DCArespectively
Figures 10 and 11 show the impact of days of month ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 1615 hours and 999 hours respectively eaverage data quality of our algorithms and DCA is 6331and 9401 respectively e results show that our
algorithms can reduce 3812 of total time cost of DCA onaverage and improve 4849 of data quality of DCArespectively
Figures 12 and 13 show the impact of communities ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 892 hours and 286 hours respectively eaverage data quality of our algorithms and DCA is 6844and 9521 respectively e results show that our
2 4 6 8 1050
60
70
80
90
100
Number of medical institutions
Dat
a qua
lity
()
DCAOurs
Figure 7 Data quality vs number of medical institutions
2 4 6 8 10
2
4
6
8
10
Number of communities
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 8 Total time cost vs number of communities
10 Journal of Healthcare Engineering
algorithms can reduce 6776 of total time cost of DCA onaverage and improve 3911 of data quality of DCArespectively
Overall our algorithms can significantly decrease thetotal time cost and improve the data quality through thedesigned data direction prediction algorithm and datacollection planning algorithm
7 Conclusion
In this article we have designed the 5G edge computingarchitecture for medical community to improve the effec-tiveness and efficiency of EMREHR data collection Firstwe formulate the directional data collection (DDC) problemto gather the EMRHER data from the medical communityfor minimizing the service error under the deadline con-straint of data collection deadline Second we design thedata direction prediction algorithm (DDPA) to predict thedata collection direction and propose the data collection
10 15 2050
60
70
80
90
100
Days of month
Dat
a qua
lity
()
DCAOurs
Figure 11 Data quality vs days of month
20 40 60 80 1000
2
4
6
8
10
12
Number of residents of a community
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 12 Total time cost vs number of residents of a community
20 40 60 80 10060
70
80
90
100
Number of residents of a community
Dat
a qua
lity
()
DCAOurs
Figure 13 Data quality vs number of residents of a community
2 4 6 8 1060
70
80
90
100
Number of communities
Dat
a qua
lity
()
DCAOurs
Figure 9 Data quality vs number of communities
10 15 208
10
12
14
16
18
20
Days of month
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 10 Total time cost vs days of month
Journal of Healthcare Engineering 11
planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering

plication mechanism of data directional collection so as toprovide the reliability credibility and feasibility guaranteefor the data update and sharing application of medicalcommunity electronic health records management
According to the requirements of regional medical in-stitutions information platform construction we analyze theinformation interconnection and regional differences be-tween community health service centers and municipalhospitals en we introduce edge computing into 5Gthrough the organic allocation and deep integration betweenthe mobile terminals and cloud computing server e edgecomputing reasonably allocates the storage computing andnetwork services resources between the computing centerand the mobile terminals so as to achieve the local optimaldivision of labor and cooperation before the network servicequality and user experience quality erefore the intro-duction of edge computing into 5G can satisfy the com-puting and communication needs of mobile terminals withdistributed and random characteristics Hence edge com-puting can well solve the geographical deployment char-acteristics of 5G nodes scattered between community healthservice centers and municipal hospitals Moreover the edgecomputing architecture with 5G is shown in Figure 1 Herethe 5G platform is the center ie the municipal hospital andseveral subnets of edge community service center aredeployede network control ability of these center subnetsis the same as that of the servers in the platform where thearchitecture can effectively reduce the calculation delay andimprove the storage efficiency of medical communityelectronic health record data
e 5G architecture shown in Figure 1 can provideconvenient services health management services traditionalChinese medicine (TCM) health care services and otherservices is architecture can give full play to its advantagesin data sharing and family doctor follow-up continuouslyimprove the accessibility and effectiveness of servicescomprehensively improve service level and satisfaction andprovide medical services and health management services tothe majority of residents conveniently and quickly At thesame time the medical community platform can solve thefollowing problem lack of medical resources shortagedifficulty to see a doctor and realize the integration of healthresources and then improve the level of primary health carethrough the establishment of complete electronic healthrecords for residents en we integrate the sharing ofmedical records and test results medical images medicationrecords and patientsrsquo basic health information betweensecondary and tertiary comprehensive medical institutionsin the community to realize the sharing of high-qualitymedical resources in the region
With the rapid development of 5G edge terminals usedto collect electronic health records data how to reasonablyallocate and effectively recover the diversity resources of 5Ghas become a key problem In 5G environment the dis-tribution and recovery of resources and the reconstructionof network topology are dynamic ere is an unknownmapping and interference relationship between 5G real-timeresource statistics computing task resource allocation and
task scheduling and 5G network edge computing terminaltrusted resource information ese relationships are real-time and random It is the main goal of network resourcemanagement to make 5G system execution efficiency andresource utilization always in the best state It is well knownthat 5G supports a large amount of traffic e resourcerequest queue is very easy to overflow which makes thearrival rate and processing efficiency of resource requestsignaling and computing task control signaling between thenetwork control center and the edge terminal irregular andthe reliability of resource allocation and computing taskunbalanced among different services In order to improvethe instantaneous resource management level of 5G and theutilization rate of global resources and make 5G bettercommunication support for medical community electronichealth records management we design the 5G edge com-puting architecture as shown in Figure 2 where we deployedwith multiple edge terminals multiple autonomous basestations and multiple autonomous control networks
In Figure 2 edge computing terminals share EHR in-formation and exchange unified standard data sourcesthrough regional platform interfaces of medical institutionsAccording to the edge computing architecture shown inFigure 2 medical institutions improve the interconnectionarchitecture of regional health information platform andguide the electronic medical record system and electronichealth record management system of medical institutionsunder their jurisdiction In particular electronic healthrecords need to achieve unified data interface standards ofmedical institutions medical insurance community andother related systems so as to facilitate information sharing
e common data element established in the 5G controlcenter of medical community can efficiently improve thereal-time sharing efficiency of electronic medical record(EMR) and EHR erefore the electronic medical recordsand electronic health records storage system of medicalinstitutions in medical community must follow the stan-dardized description of national public health data elementattributes describe the extracted data element attributesconduct business modeling and realize data sharingMedical institutions at all levels should use the ID number asthe main identification code for the transmission and cir-culation of information in the diagnosis and treatment ofpublic health services in the business system so as to ensurethe effective collection of archival information Each edgecomputing terminal server should ensure the validity andtimeliness of data transmission verification processtracking and traceability so as to ensure that all kinds ofinformation can be uploaded to 5G information platformtimely accurately and comprehensively
erefore how to collect and improve data from thecommunity and medical institutions at all levels in accor-dance with the electronic medical record informationstandards and unified specification of disease coding andother important databases to ensure the quality of data hasbecome the key of medical community archives manage-ment e process of data collection should have the fol-lowing properties
Journal of Healthcare Engineering 3
Control center of 5G
Medical community
Edgecomputing
terminal
Edgecomputingterminal
Information sharingplatform of EHR
EHR
EHR
Figure 2 5G edge computing architecture for medical community
5G
Medicalcommunity
Medicalcommunity
ResidentMedical
community
Medicalcommunity
Figure 1 5G architecture for medical community
4 Journal of Healthcare Engineering
(i) e process of data collection should be based onthe main index of patient identity correctly asso-ciated with the previous diagnosis and treatmentdata and form a complete and standardized medicalrecord file which is convenient for medical staff touse
(ii) e process of data collection should be carried outaccording to the interface specification of regionalinformation platform e diagnosis and treatmentinformation should be uploaded and collected intohealth records in time
(iii) e process of data collection should implement thecodes of clinical symptoms diagnosis surgerydrugs inspection and so on released by the state toensure the standardization and unification of di-agnosis and treatment information uploaded to theplatform
Figure 3 gives a toy example for the Directional DataCollection and application of medical community electronichealth record with the above characteristics In this scenariocloud platform edge computing terminal and 5G platformare effectively integrated into the directional data collectionof medical community electronic health records such ascommunity classification data directional collection anddata storage
e edge computing procedure is illustrated as follows
(1) e communities generate their EMRHER datawhich can be collected by a corresponding oppor-tunistically encountered edge computing terminal
(2) e edge computing terminal analyzes andmines thevalid information from collected EMRHER dataeg the location resident ID and hisher historicalrecords en the dataset is sent to the cloud serversin real time e edge computing terminal predictstheir medical demand according to the historicalrecords by using the algorithm proposed in Section41 and returns the prediction results to the 5G cloudservers
(3) e 5G cloud servers periodically compute the datacollection route via the algorithms in Section 42 fordata collection terminal according to the informa-tion of communities and residents from edgecomputing terminals
(4) e data is collected by the data collection terminalthrough the route calculated in the above step
4 Directional Data Collection forMedical Community
41 SystemModel Suppose that the 5G platform of medicalcommunity includes m medical institutions and n com-munities According to the scope of service and medicallevel the mapping relationship between each communityand different medical institutions is established denoted byC cij1113966 1113967
mn
i1j1 Here the electronic file data is generated bythe medical institutions according to the community it
serves which is used to obtain the medical needs andfeedback of residents Note that each medical institutioninitiates one data collection task in the time dimension SoT ti1113864 1113865
m
i1 denotes the task set For convenience we definethe data collection process as follows
Definition 1 (data collection task) e process of edgecomputing terminal completing data collection task is toselect the corresponding observation values from a series ofcandidate data samples corresponding to the community for5G platform
For each data collection task ti we assume that it has acandidate sample set Ai shown as follows
Ai ai(1) ai(2) ai Ai
111386811138681113868111386811138681113868111386811138681113872 11138731113966 1113967 (1)
en let ai(0) denote the optimal data sample corre-sponding to the task ti erefore the data error caused bytask ti can be calculated by
ei 1Ai
11138681113868111386811138681113868111386811138681113868
1113944
Ai| |
k1ai(k) minus ai(0)⎛⎜⎝ ⎞⎟⎠ (2)
e resident set who provides the EMRHER datasetfrom all communities can be represented as follows
Bi bji1113966 1113967
n
j1 (3)
Here bji represents the data in task ti which is provided
by the j-th community when the i-th task is initiated by i-thmedical institution when there is the mapping relationshipbelonging to C So we can calculate the data matrix cor-responding to data collection tasks from all communitiesthrough the following equation
5G networks
Cloud servers
EHR data collection
EHR data collection
EHR data collection
Medical community
Community
Community
Edge computing terminal
Figure 3 Application of directional data collection with the as-sistance of 5G and edge computing system
Journal of Healthcare Engineering 5
A aij1113966 1113967mn
i1j1
1113945m
i1Ai minus eiBi( 1113857
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus eiBi⎛⎜⎝ ⎞⎟⎠
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus ei 1113944
n
j1b
ji
⎛⎜⎝ ⎞⎟⎠
(4)
Here we redefine the data sample ai(k) in Ai as ai(k)twhich is calculated according to the time dependence of edgecomputing Note that we can update the mapping rela-tionship between each community and different medicalinstitutions through the following equation
cij
0 if 0ltaij
ei
lt cij
1 ifaij
ei
ge cij
⎧⎪⎪⎪⎪⎪⎨
⎪⎪⎪⎪⎪⎩
(5)
Here cij is the tolerance threshold of the data collectionerror which is a given empirical value
In order to analyze the direction accuracy of data col-lection conveniently we give the following definition of datacollection aggregation reliability
Definition 2 (data collection task) For m data collectiontasks and n communities the direction of data collection isaccurate when each task satisfies the following conditions
(1) e i-th task and j-th community have the mappingrelationship ie cij 1
(2) Ai and Bi have the same rank for each task ti(3) All the data samples collected by all the medical
institutions have consistency ie the followingfunction f(A) is valid
f(A) limn⟶infin
limm⟶infinA
1113936iiprime1 riprime + 1113936eisinTi
te
(6)
(4) Let Γ(ti) denote the data collection time cost etime cost of the i-th task is not larger than thedeadline τi
42 Problem Formulation e objective of directional datacollection (DDC) problem is to design a data collectionscheme based on 5G edge computing system to gather theEMRHER data from the medical community to minimizethe service error under the deadline constraint of datacollection xij is a binary variable to indicate whether data of
task ti is collected from j-th community xij 1 if data oftask ti is collected from j-th community xij 0 otherwise
e DDC problem can be formulated as follows
DDCmin xij 1113944
m
i1ei
st
(a) xij isin 0 1 forallti isin T
(b) r Ai( 1113857 r Bi( 1113857 forallti isin T
(c) 1113945m
i11113945
n
j1cij 1
(d) Γ ti( 1113857le τi forallti isin T
(7)
Constraint (a) gives the value range of xij Constraint (b)ensures that the rank of candidate data sample set is equal tothat of data in task ti on the basis of C Constraint (c) ensuresthat each mapping between the task and its correspondingcommunity is valid Constraint (d) ensures that the time costof data collection in each task is not larger than its deadline
We list the frequently used notations in Table 1
5 Intelligent Data Collection Scheme
In this section we propose our 5G edge computing enableddirectional data collection (5EDDC) algorithm en thedetailed description of the proposed algorithm is presentedin two phases data direction prediction and data collectionplanning
51 Data Direction Prediction Algorithm Medical behaviorsand requirements of residents in different communitiesactually reflect the regeneration direction of EMR whichcontains a lot of medical information such as commondiseases and medical habits Based on the implementation ofa variant of algorithms [19] we design Algorithm 1 forsolving the problem of data direction prediction
First we predict the medical behavior of residentsthrough the following steps
Step 1 Feature extraction takes into account the fol-lowing features for each behavior in community gen-erating along the historical records Bi with the last datacollection task ti and candidate sample set Ai of currentmedical community time of day medical behaviorstarting time medical community name and its loca-tion resident ID and medical treatment time of eachlocation e above procedure is denoted as functionFeature Extraction(dataset)Step 2 Random forest-based prediction needs the inputvector nt representing the information of a residentwhich includes the origin community and destinationmedical institute as well as the corresponding extractedfeatures from step 1 en the data generating time ofany community can be predicted based on temporal
6 Journal of Healthcare Engineering
data dependencies and spatial data correlations eabove process is denoted as function RandomForests
Second we can predict the data direction of communityfor collecting data via the Interval-based Historical Average(IHA) [20] as shown in the following equation
IHA E ta1113858 1113859 λ( 1113857 1
2λ + 11113944
λ
pminusλ1113944
days
q1tp minus E ta1113858 1113859 minus q1113872 1113873⎛⎝ ⎞⎠ (8)
Here E[ta] is the expectation of data generating time oftask ta based on historical EMRHER data λ is the meanabsolute error of the random forests [21] for data generatingtime prediction and days is the days of historical EMREHRdataset tp is the first data collection starting time afterE[ta] + q in the p-th day of the dataset where E[ta] + q is thegenerating time of EMRHER data for recording residents ina-th community at the q-th day us tp minus E[ta] minus q is thehistorical data collection time on the q-th day Finally wecalculate the EMREHR data generating time of commu-nities and data collection direction of medical community
In Algorithm 1 the Sink(F B) function is used to find allthe data collection sinks of EMREHR at its medical com-munity In addition Algorithm 1 updates all the datasamples and records between any two communities andcomputes their collecting time through the following steps
(1) Find all ai which can satisfy the tolerance(2) Extract all the features from historical dataset
52 Data Collection Planning Algorithm Based on the di-rection prediction of data collection the DDC problem isequivalent to finding a data route to collect the EMRHERdata for all selected medical communities with minimumtime cost e above data collection planning (DCP)problem can be formulated as follows
DCPmin 1113944C
01Γ to( 1113857 (9)
Moreover we design the data collection planning al-gorithm (DCPA) to solve the DCP probleme basic idea isgiven as follows (see Algorithm 2)
(1) Transform Ai and integrate into 1113957A (line 5)(2) Update 1113957B (line 6)(3) For each element in 1113957B we first divide it into two
separate sets P1 and P2 and then remove half ofelements in 1113957B (lines 8ndash10) and then find the cor-responding subroutes (lines 11ndash14)
(4) Integrate all the subroutes into the final data col-lection planning P (lines 15ndash18) where the symbol ⊎represents the integration of some routes
6 Numerical Experiments
In this section we conduct extensive simulations to verifythe performance of our proposed algorithms with differentnumber of medical institutions number of communitiesdays of month and number of residents of a community
61DataDescription e dataset used in our experiments isfrom the electronic records system of Changshu No 1Peoplersquos Hospital e dataset shows a kind of representativemedical community data It is generated by the medicalcommunity supported by Changshu No 1 Peoplersquos Hospitalwhich covers the period from January 1 2018 to November30 2018 e dataset includes the record data of medicalinstitute and residents and GPS data of medical institutese data record contains various fields such as time of daymedical behavior starting time medical community nameand its location resident ID medical treatment time of each
Table 1 Frequently used notations
Notation Descriptioncij Mapping relationship between i-th community and j-th different medical institutionC Set of mappingsti i-th data collection taskT Set of tasksAi Set of candidate data samples belonging to i-th taskai(k) k-th data sample in Ai
|Ai| Size of data sample in Ai
ai(0) Optimal data sample corresponding to task ti
ei Data error caused by task ti
bji Data in task ti provided by the j-th community when the i-th task is initiated by i-th medical institution
Bi Set of data in task ti on the basis of C
ai(k)t k-th data sample calculated according to the time dependence of edge computingcij Tolerance threshold of the data collection error between the i-th task and j-th communityf(A) Consistence functionτi Deadline of task ti
Journal of Healthcare Engineering 7
location and the number of patients of the correspondingmedical institute etc e GPS data contains latitude lon-gitude and treatment time of medical institute
62 Simulation Setup andBenchmark We assume that thereare 10 medical institutions to provide medical care for 10communities which are supported by Changshu No 1Peoplersquos Hospital e residents receive medical treatmentfrom the above medical institutions In our simulation weevaluate the total time cost of data collection and dataquality calculated by equation (2) All the simulations wererun on a cloud server ECS [23] with 12-core Intel XeonPlatinum 8269CY and 48GB memory e other parametersettings of our simulations are listed in Table 2
We develop the data collection algorithm DCA in [22] asthe benchmark algorithm for comparison which can makean efficient tradeoff between the data collection efficiency
and energy consumption through the combination of theenergy of the emotional device wireless device
63 Performance Evaluation In this subsection we evaluatethe performance of our algorithms and DCA in the scenarioshown in Figure 4 Tables 3 and 4 give the locations ofmedical institutions and communities in the area respec-tively e above information is calculated based on GoogleMaps
Figure 5 shows the prediction errors on two differentdays ie March 10 2018 and October 20 2018 e pre-diction results demonstrate the effectiveness of our proposedprediction algorithm DDPA e average prediction erroron March 10 2018 and October 20 2018 is 321 and193 respectively
Figures 6 and 7 show the impact of medical institutionson total time cost and data quality of our algorithms and
Input T datasetOutput A B
(1) for i 2 tom do(2) ei⟵ (1|Ai|)(1113936
|Ai |
k1 ai(k) minus ai(0))
(3) Ai⟵ ai|ai lt ei1113864 1113865(4) for j 1 to n do(5) b
ji⟵ ai(j)
(6) for each a isin A do(7) F⟵ Feature Extraction(dataset)(8) B⟵ Sink(F B)(9) for each b isin B do(10) (A B)⟵ RandomForests(F A B)
ALGORITHM 1 Data direction prediction algorithm (DDPA)
Input A B
Output P
(1) count⟵ 0 1113954A⟵A 1113957B⟵empty
(2) while countle log B minus 1 do(3) for i 1 tom do(4) for j 1 to n do(5) 1113957A⟵ 1113957ai(1) 1113957ai(2) 1113957ai(|Ai|)1113864 1113865
(6) 1113957B⟵ 1113957bj
i1113882 1113883cup 1113957B
(7) for each 1113957b isin 1113957B do(8) Take (|1113957B|2) elements to P1(9) Take another (|1113957B|2) elements to P2(10) Remove (|1113957B|2) elements from 1113957B(11) Find subroute pcount
1 of P1(12) Pcount
1 ⟵ Pcount1 cup pcount
11113864 1113865(13) Find subroute pcount
2 of P2(14) Pcount
2 ⟵ Pcount2 cup pcount
21113864 1113865(15) for each p1 isin P1 do(16) P⟵ P ⊎ p11113864 1113865(17) for each p2 isin P2 do(18) P⟵ P ⊎ p21113864 1113865
ALGORITHM 2 Data Collection Planning Algorithm (DCPA)
8 Journal of Healthcare Engineering
DCA respectively e average total time cost of our al-gorithms and DCA is 885 hours and 244 hours respec-tivelye average data quality of our algorithms and DCA is7576 and 9475 respectively e results show that ouralgorithms can reduce 7238 of total time cost of DCA onaverage and improve 2506 of data quality of DCA re-spectively is indicates that the proposed algorithmssignificantly outperform DCA is is because the dataquality of our algorithms is better than the those obtained byDCA respectively
Figures 8 and 9 show the impact of communities on totaltime cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 575 hours and 163 hours respectively eaverage data quality of our algorithms and DCA is 7327and 9759 respectively e results show that our
Table 2 Parameter settings
Parameter Valuen 10m 10|T| 10cij [001 005]τi [1 10] hours|Ai| [100 500]
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Figure 4 Medical community for EMRHER data collection ered nodes represent locations of medical institutions and the greennodes represent locations of communities
Table 3 Locations of medical institutions
i Longitude Latitude1 31629934025445163 120745726947073172 31637070592885376 120744987234992693 31641308857555806 120742605433500614 31644304755694158 1207431204176075 31639559503878488 120739966849915396 3163350810894618 120741081938852527 31634421579375328 120735202536971168 31640051243952147 120743342172446979 3163600474671818 1207442755811459110 31640862982947134 12074781351639375
Table 4 Locations of communities
i Longitude Latitude1 31633639306384033 120736407142357452 31635638094098336 120744138979835573 3164162333734517 120746486600514814 31638983794798012 120748808703562535 31641820359193588 120738421187636156 3163745217402931 120743756215726587 31643893501251643 120747443511151158 3163659402090503 1207420720531559 31634475760812066 1207435393159863510 31634834238968633 12074956147326746
7 8 9 10 11 12 13 14 15 16 170
2
4
6
8
Time
Pred
ictio
n er
ror (
)
March 10 2018
October 20 2018
Figure 5 Prediction errors on March 10 2018 and October 202018
2 4 6 8 10
5
10
15
Number of medical institutions
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 6 Total time cost vs number of medical institutions
Journal of Healthcare Engineering 9
algorithms reduces 7167 of total time cost of DCA onaverage and improves 3320 of data quality of DCArespectively
Figures 10 and 11 show the impact of days of month ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 1615 hours and 999 hours respectively eaverage data quality of our algorithms and DCA is 6331and 9401 respectively e results show that our
algorithms can reduce 3812 of total time cost of DCA onaverage and improve 4849 of data quality of DCArespectively
Figures 12 and 13 show the impact of communities ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 892 hours and 286 hours respectively eaverage data quality of our algorithms and DCA is 6844and 9521 respectively e results show that our
2 4 6 8 1050
60
70
80
90
100
Number of medical institutions
Dat
a qua
lity
()
DCAOurs
Figure 7 Data quality vs number of medical institutions
2 4 6 8 10
2
4
6
8
10
Number of communities
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 8 Total time cost vs number of communities
10 Journal of Healthcare Engineering
algorithms can reduce 6776 of total time cost of DCA onaverage and improve 3911 of data quality of DCArespectively
Overall our algorithms can significantly decrease thetotal time cost and improve the data quality through thedesigned data direction prediction algorithm and datacollection planning algorithm
7 Conclusion
In this article we have designed the 5G edge computingarchitecture for medical community to improve the effec-tiveness and efficiency of EMREHR data collection Firstwe formulate the directional data collection (DDC) problemto gather the EMRHER data from the medical communityfor minimizing the service error under the deadline con-straint of data collection deadline Second we design thedata direction prediction algorithm (DDPA) to predict thedata collection direction and propose the data collection
10 15 2050
60
70
80
90
100
Days of month
Dat
a qua
lity
()
DCAOurs
Figure 11 Data quality vs days of month
20 40 60 80 1000
2
4
6
8
10
12
Number of residents of a community
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 12 Total time cost vs number of residents of a community
20 40 60 80 10060
70
80
90
100
Number of residents of a community
Dat
a qua
lity
()
DCAOurs
Figure 13 Data quality vs number of residents of a community
2 4 6 8 1060
70
80
90
100
Number of communities
Dat
a qua
lity
()
DCAOurs
Figure 9 Data quality vs number of communities
10 15 208
10
12
14
16
18
20
Days of month
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 10 Total time cost vs days of month
Journal of Healthcare Engineering 11
planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering

Control center of 5G
Medical community
Edgecomputing
terminal
Edgecomputingterminal
Information sharingplatform of EHR
EHR
EHR
Figure 2 5G edge computing architecture for medical community
5G
Medicalcommunity
Medicalcommunity
ResidentMedical
community
Medicalcommunity
Figure 1 5G architecture for medical community
4 Journal of Healthcare Engineering
(i) e process of data collection should be based onthe main index of patient identity correctly asso-ciated with the previous diagnosis and treatmentdata and form a complete and standardized medicalrecord file which is convenient for medical staff touse
(ii) e process of data collection should be carried outaccording to the interface specification of regionalinformation platform e diagnosis and treatmentinformation should be uploaded and collected intohealth records in time
(iii) e process of data collection should implement thecodes of clinical symptoms diagnosis surgerydrugs inspection and so on released by the state toensure the standardization and unification of di-agnosis and treatment information uploaded to theplatform
Figure 3 gives a toy example for the Directional DataCollection and application of medical community electronichealth record with the above characteristics In this scenariocloud platform edge computing terminal and 5G platformare effectively integrated into the directional data collectionof medical community electronic health records such ascommunity classification data directional collection anddata storage
e edge computing procedure is illustrated as follows
(1) e communities generate their EMRHER datawhich can be collected by a corresponding oppor-tunistically encountered edge computing terminal
(2) e edge computing terminal analyzes andmines thevalid information from collected EMRHER dataeg the location resident ID and hisher historicalrecords en the dataset is sent to the cloud serversin real time e edge computing terminal predictstheir medical demand according to the historicalrecords by using the algorithm proposed in Section41 and returns the prediction results to the 5G cloudservers
(3) e 5G cloud servers periodically compute the datacollection route via the algorithms in Section 42 fordata collection terminal according to the informa-tion of communities and residents from edgecomputing terminals
(4) e data is collected by the data collection terminalthrough the route calculated in the above step
4 Directional Data Collection forMedical Community
41 SystemModel Suppose that the 5G platform of medicalcommunity includes m medical institutions and n com-munities According to the scope of service and medicallevel the mapping relationship between each communityand different medical institutions is established denoted byC cij1113966 1113967
mn
i1j1 Here the electronic file data is generated bythe medical institutions according to the community it
serves which is used to obtain the medical needs andfeedback of residents Note that each medical institutioninitiates one data collection task in the time dimension SoT ti1113864 1113865
m
i1 denotes the task set For convenience we definethe data collection process as follows
Definition 1 (data collection task) e process of edgecomputing terminal completing data collection task is toselect the corresponding observation values from a series ofcandidate data samples corresponding to the community for5G platform
For each data collection task ti we assume that it has acandidate sample set Ai shown as follows
Ai ai(1) ai(2) ai Ai
111386811138681113868111386811138681113868111386811138681113872 11138731113966 1113967 (1)
en let ai(0) denote the optimal data sample corre-sponding to the task ti erefore the data error caused bytask ti can be calculated by
ei 1Ai
11138681113868111386811138681113868111386811138681113868
1113944
Ai| |
k1ai(k) minus ai(0)⎛⎜⎝ ⎞⎟⎠ (2)
e resident set who provides the EMRHER datasetfrom all communities can be represented as follows
Bi bji1113966 1113967
n
j1 (3)
Here bji represents the data in task ti which is provided
by the j-th community when the i-th task is initiated by i-thmedical institution when there is the mapping relationshipbelonging to C So we can calculate the data matrix cor-responding to data collection tasks from all communitiesthrough the following equation
5G networks
Cloud servers
EHR data collection
EHR data collection
EHR data collection
Medical community
Community
Community
Edge computing terminal
Figure 3 Application of directional data collection with the as-sistance of 5G and edge computing system
Journal of Healthcare Engineering 5
A aij1113966 1113967mn
i1j1
1113945m
i1Ai minus eiBi( 1113857
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus eiBi⎛⎜⎝ ⎞⎟⎠
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus ei 1113944
n
j1b
ji
⎛⎜⎝ ⎞⎟⎠
(4)
Here we redefine the data sample ai(k) in Ai as ai(k)twhich is calculated according to the time dependence of edgecomputing Note that we can update the mapping rela-tionship between each community and different medicalinstitutions through the following equation
cij
0 if 0ltaij
ei
lt cij
1 ifaij
ei
ge cij
⎧⎪⎪⎪⎪⎪⎨
⎪⎪⎪⎪⎪⎩
(5)
Here cij is the tolerance threshold of the data collectionerror which is a given empirical value
In order to analyze the direction accuracy of data col-lection conveniently we give the following definition of datacollection aggregation reliability
Definition 2 (data collection task) For m data collectiontasks and n communities the direction of data collection isaccurate when each task satisfies the following conditions
(1) e i-th task and j-th community have the mappingrelationship ie cij 1
(2) Ai and Bi have the same rank for each task ti(3) All the data samples collected by all the medical
institutions have consistency ie the followingfunction f(A) is valid
f(A) limn⟶infin
limm⟶infinA
1113936iiprime1 riprime + 1113936eisinTi
te
(6)
(4) Let Γ(ti) denote the data collection time cost etime cost of the i-th task is not larger than thedeadline τi
42 Problem Formulation e objective of directional datacollection (DDC) problem is to design a data collectionscheme based on 5G edge computing system to gather theEMRHER data from the medical community to minimizethe service error under the deadline constraint of datacollection xij is a binary variable to indicate whether data of
task ti is collected from j-th community xij 1 if data oftask ti is collected from j-th community xij 0 otherwise
e DDC problem can be formulated as follows
DDCmin xij 1113944
m
i1ei
st
(a) xij isin 0 1 forallti isin T
(b) r Ai( 1113857 r Bi( 1113857 forallti isin T
(c) 1113945m
i11113945
n
j1cij 1
(d) Γ ti( 1113857le τi forallti isin T
(7)
Constraint (a) gives the value range of xij Constraint (b)ensures that the rank of candidate data sample set is equal tothat of data in task ti on the basis of C Constraint (c) ensuresthat each mapping between the task and its correspondingcommunity is valid Constraint (d) ensures that the time costof data collection in each task is not larger than its deadline
We list the frequently used notations in Table 1
5 Intelligent Data Collection Scheme
In this section we propose our 5G edge computing enableddirectional data collection (5EDDC) algorithm en thedetailed description of the proposed algorithm is presentedin two phases data direction prediction and data collectionplanning
51 Data Direction Prediction Algorithm Medical behaviorsand requirements of residents in different communitiesactually reflect the regeneration direction of EMR whichcontains a lot of medical information such as commondiseases and medical habits Based on the implementation ofa variant of algorithms [19] we design Algorithm 1 forsolving the problem of data direction prediction
First we predict the medical behavior of residentsthrough the following steps
Step 1 Feature extraction takes into account the fol-lowing features for each behavior in community gen-erating along the historical records Bi with the last datacollection task ti and candidate sample set Ai of currentmedical community time of day medical behaviorstarting time medical community name and its loca-tion resident ID and medical treatment time of eachlocation e above procedure is denoted as functionFeature Extraction(dataset)Step 2 Random forest-based prediction needs the inputvector nt representing the information of a residentwhich includes the origin community and destinationmedical institute as well as the corresponding extractedfeatures from step 1 en the data generating time ofany community can be predicted based on temporal
6 Journal of Healthcare Engineering
data dependencies and spatial data correlations eabove process is denoted as function RandomForests
Second we can predict the data direction of communityfor collecting data via the Interval-based Historical Average(IHA) [20] as shown in the following equation
IHA E ta1113858 1113859 λ( 1113857 1
2λ + 11113944
λ
pminusλ1113944
days
q1tp minus E ta1113858 1113859 minus q1113872 1113873⎛⎝ ⎞⎠ (8)
Here E[ta] is the expectation of data generating time oftask ta based on historical EMRHER data λ is the meanabsolute error of the random forests [21] for data generatingtime prediction and days is the days of historical EMREHRdataset tp is the first data collection starting time afterE[ta] + q in the p-th day of the dataset where E[ta] + q is thegenerating time of EMRHER data for recording residents ina-th community at the q-th day us tp minus E[ta] minus q is thehistorical data collection time on the q-th day Finally wecalculate the EMREHR data generating time of commu-nities and data collection direction of medical community
In Algorithm 1 the Sink(F B) function is used to find allthe data collection sinks of EMREHR at its medical com-munity In addition Algorithm 1 updates all the datasamples and records between any two communities andcomputes their collecting time through the following steps
(1) Find all ai which can satisfy the tolerance(2) Extract all the features from historical dataset
52 Data Collection Planning Algorithm Based on the di-rection prediction of data collection the DDC problem isequivalent to finding a data route to collect the EMRHERdata for all selected medical communities with minimumtime cost e above data collection planning (DCP)problem can be formulated as follows
DCPmin 1113944C
01Γ to( 1113857 (9)
Moreover we design the data collection planning al-gorithm (DCPA) to solve the DCP probleme basic idea isgiven as follows (see Algorithm 2)
(1) Transform Ai and integrate into 1113957A (line 5)(2) Update 1113957B (line 6)(3) For each element in 1113957B we first divide it into two
separate sets P1 and P2 and then remove half ofelements in 1113957B (lines 8ndash10) and then find the cor-responding subroutes (lines 11ndash14)
(4) Integrate all the subroutes into the final data col-lection planning P (lines 15ndash18) where the symbol ⊎represents the integration of some routes
6 Numerical Experiments
In this section we conduct extensive simulations to verifythe performance of our proposed algorithms with differentnumber of medical institutions number of communitiesdays of month and number of residents of a community
61DataDescription e dataset used in our experiments isfrom the electronic records system of Changshu No 1Peoplersquos Hospital e dataset shows a kind of representativemedical community data It is generated by the medicalcommunity supported by Changshu No 1 Peoplersquos Hospitalwhich covers the period from January 1 2018 to November30 2018 e dataset includes the record data of medicalinstitute and residents and GPS data of medical institutese data record contains various fields such as time of daymedical behavior starting time medical community nameand its location resident ID medical treatment time of each
Table 1 Frequently used notations
Notation Descriptioncij Mapping relationship between i-th community and j-th different medical institutionC Set of mappingsti i-th data collection taskT Set of tasksAi Set of candidate data samples belonging to i-th taskai(k) k-th data sample in Ai
|Ai| Size of data sample in Ai
ai(0) Optimal data sample corresponding to task ti
ei Data error caused by task ti
bji Data in task ti provided by the j-th community when the i-th task is initiated by i-th medical institution
Bi Set of data in task ti on the basis of C
ai(k)t k-th data sample calculated according to the time dependence of edge computingcij Tolerance threshold of the data collection error between the i-th task and j-th communityf(A) Consistence functionτi Deadline of task ti
Journal of Healthcare Engineering 7
location and the number of patients of the correspondingmedical institute etc e GPS data contains latitude lon-gitude and treatment time of medical institute
62 Simulation Setup andBenchmark We assume that thereare 10 medical institutions to provide medical care for 10communities which are supported by Changshu No 1Peoplersquos Hospital e residents receive medical treatmentfrom the above medical institutions In our simulation weevaluate the total time cost of data collection and dataquality calculated by equation (2) All the simulations wererun on a cloud server ECS [23] with 12-core Intel XeonPlatinum 8269CY and 48GB memory e other parametersettings of our simulations are listed in Table 2
We develop the data collection algorithm DCA in [22] asthe benchmark algorithm for comparison which can makean efficient tradeoff between the data collection efficiency
and energy consumption through the combination of theenergy of the emotional device wireless device
63 Performance Evaluation In this subsection we evaluatethe performance of our algorithms and DCA in the scenarioshown in Figure 4 Tables 3 and 4 give the locations ofmedical institutions and communities in the area respec-tively e above information is calculated based on GoogleMaps
Figure 5 shows the prediction errors on two differentdays ie March 10 2018 and October 20 2018 e pre-diction results demonstrate the effectiveness of our proposedprediction algorithm DDPA e average prediction erroron March 10 2018 and October 20 2018 is 321 and193 respectively
Figures 6 and 7 show the impact of medical institutionson total time cost and data quality of our algorithms and
Input T datasetOutput A B
(1) for i 2 tom do(2) ei⟵ (1|Ai|)(1113936
|Ai |
k1 ai(k) minus ai(0))
(3) Ai⟵ ai|ai lt ei1113864 1113865(4) for j 1 to n do(5) b
ji⟵ ai(j)
(6) for each a isin A do(7) F⟵ Feature Extraction(dataset)(8) B⟵ Sink(F B)(9) for each b isin B do(10) (A B)⟵ RandomForests(F A B)
ALGORITHM 1 Data direction prediction algorithm (DDPA)
Input A B
Output P
(1) count⟵ 0 1113954A⟵A 1113957B⟵empty
(2) while countle log B minus 1 do(3) for i 1 tom do(4) for j 1 to n do(5) 1113957A⟵ 1113957ai(1) 1113957ai(2) 1113957ai(|Ai|)1113864 1113865
(6) 1113957B⟵ 1113957bj
i1113882 1113883cup 1113957B
(7) for each 1113957b isin 1113957B do(8) Take (|1113957B|2) elements to P1(9) Take another (|1113957B|2) elements to P2(10) Remove (|1113957B|2) elements from 1113957B(11) Find subroute pcount
1 of P1(12) Pcount
1 ⟵ Pcount1 cup pcount
11113864 1113865(13) Find subroute pcount
2 of P2(14) Pcount
2 ⟵ Pcount2 cup pcount
21113864 1113865(15) for each p1 isin P1 do(16) P⟵ P ⊎ p11113864 1113865(17) for each p2 isin P2 do(18) P⟵ P ⊎ p21113864 1113865
ALGORITHM 2 Data Collection Planning Algorithm (DCPA)
8 Journal of Healthcare Engineering
DCA respectively e average total time cost of our al-gorithms and DCA is 885 hours and 244 hours respec-tivelye average data quality of our algorithms and DCA is7576 and 9475 respectively e results show that ouralgorithms can reduce 7238 of total time cost of DCA onaverage and improve 2506 of data quality of DCA re-spectively is indicates that the proposed algorithmssignificantly outperform DCA is is because the dataquality of our algorithms is better than the those obtained byDCA respectively
Figures 8 and 9 show the impact of communities on totaltime cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 575 hours and 163 hours respectively eaverage data quality of our algorithms and DCA is 7327and 9759 respectively e results show that our
Table 2 Parameter settings
Parameter Valuen 10m 10|T| 10cij [001 005]τi [1 10] hours|Ai| [100 500]
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Figure 4 Medical community for EMRHER data collection ered nodes represent locations of medical institutions and the greennodes represent locations of communities
Table 3 Locations of medical institutions
i Longitude Latitude1 31629934025445163 120745726947073172 31637070592885376 120744987234992693 31641308857555806 120742605433500614 31644304755694158 1207431204176075 31639559503878488 120739966849915396 3163350810894618 120741081938852527 31634421579375328 120735202536971168 31640051243952147 120743342172446979 3163600474671818 1207442755811459110 31640862982947134 12074781351639375
Table 4 Locations of communities
i Longitude Latitude1 31633639306384033 120736407142357452 31635638094098336 120744138979835573 3164162333734517 120746486600514814 31638983794798012 120748808703562535 31641820359193588 120738421187636156 3163745217402931 120743756215726587 31643893501251643 120747443511151158 3163659402090503 1207420720531559 31634475760812066 1207435393159863510 31634834238968633 12074956147326746
7 8 9 10 11 12 13 14 15 16 170
2
4
6
8
Time
Pred
ictio
n er
ror (
)
March 10 2018
October 20 2018
Figure 5 Prediction errors on March 10 2018 and October 202018
2 4 6 8 10
5
10
15
Number of medical institutions
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 6 Total time cost vs number of medical institutions
Journal of Healthcare Engineering 9
algorithms reduces 7167 of total time cost of DCA onaverage and improves 3320 of data quality of DCArespectively
Figures 10 and 11 show the impact of days of month ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 1615 hours and 999 hours respectively eaverage data quality of our algorithms and DCA is 6331and 9401 respectively e results show that our
algorithms can reduce 3812 of total time cost of DCA onaverage and improve 4849 of data quality of DCArespectively
Figures 12 and 13 show the impact of communities ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 892 hours and 286 hours respectively eaverage data quality of our algorithms and DCA is 6844and 9521 respectively e results show that our
2 4 6 8 1050
60
70
80
90
100
Number of medical institutions
Dat
a qua
lity
()
DCAOurs
Figure 7 Data quality vs number of medical institutions
2 4 6 8 10
2
4
6
8
10
Number of communities
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 8 Total time cost vs number of communities
10 Journal of Healthcare Engineering
algorithms can reduce 6776 of total time cost of DCA onaverage and improve 3911 of data quality of DCArespectively
Overall our algorithms can significantly decrease thetotal time cost and improve the data quality through thedesigned data direction prediction algorithm and datacollection planning algorithm
7 Conclusion
In this article we have designed the 5G edge computingarchitecture for medical community to improve the effec-tiveness and efficiency of EMREHR data collection Firstwe formulate the directional data collection (DDC) problemto gather the EMRHER data from the medical communityfor minimizing the service error under the deadline con-straint of data collection deadline Second we design thedata direction prediction algorithm (DDPA) to predict thedata collection direction and propose the data collection
10 15 2050
60
70
80
90
100
Days of month
Dat
a qua
lity
()
DCAOurs
Figure 11 Data quality vs days of month
20 40 60 80 1000
2
4
6
8
10
12
Number of residents of a community
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 12 Total time cost vs number of residents of a community
20 40 60 80 10060
70
80
90
100
Number of residents of a community
Dat
a qua
lity
()
DCAOurs
Figure 13 Data quality vs number of residents of a community
2 4 6 8 1060
70
80
90
100
Number of communities
Dat
a qua
lity
()
DCAOurs
Figure 9 Data quality vs number of communities
10 15 208
10
12
14
16
18
20
Days of month
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 10 Total time cost vs days of month
Journal of Healthcare Engineering 11
planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering

(i) e process of data collection should be based onthe main index of patient identity correctly asso-ciated with the previous diagnosis and treatmentdata and form a complete and standardized medicalrecord file which is convenient for medical staff touse
(ii) e process of data collection should be carried outaccording to the interface specification of regionalinformation platform e diagnosis and treatmentinformation should be uploaded and collected intohealth records in time
(iii) e process of data collection should implement thecodes of clinical symptoms diagnosis surgerydrugs inspection and so on released by the state toensure the standardization and unification of di-agnosis and treatment information uploaded to theplatform
Figure 3 gives a toy example for the Directional DataCollection and application of medical community electronichealth record with the above characteristics In this scenariocloud platform edge computing terminal and 5G platformare effectively integrated into the directional data collectionof medical community electronic health records such ascommunity classification data directional collection anddata storage
e edge computing procedure is illustrated as follows
(1) e communities generate their EMRHER datawhich can be collected by a corresponding oppor-tunistically encountered edge computing terminal
(2) e edge computing terminal analyzes andmines thevalid information from collected EMRHER dataeg the location resident ID and hisher historicalrecords en the dataset is sent to the cloud serversin real time e edge computing terminal predictstheir medical demand according to the historicalrecords by using the algorithm proposed in Section41 and returns the prediction results to the 5G cloudservers
(3) e 5G cloud servers periodically compute the datacollection route via the algorithms in Section 42 fordata collection terminal according to the informa-tion of communities and residents from edgecomputing terminals
(4) e data is collected by the data collection terminalthrough the route calculated in the above step
4 Directional Data Collection forMedical Community
41 SystemModel Suppose that the 5G platform of medicalcommunity includes m medical institutions and n com-munities According to the scope of service and medicallevel the mapping relationship between each communityand different medical institutions is established denoted byC cij1113966 1113967
mn
i1j1 Here the electronic file data is generated bythe medical institutions according to the community it
serves which is used to obtain the medical needs andfeedback of residents Note that each medical institutioninitiates one data collection task in the time dimension SoT ti1113864 1113865
m
i1 denotes the task set For convenience we definethe data collection process as follows
Definition 1 (data collection task) e process of edgecomputing terminal completing data collection task is toselect the corresponding observation values from a series ofcandidate data samples corresponding to the community for5G platform
For each data collection task ti we assume that it has acandidate sample set Ai shown as follows
Ai ai(1) ai(2) ai Ai
111386811138681113868111386811138681113868111386811138681113872 11138731113966 1113967 (1)
en let ai(0) denote the optimal data sample corre-sponding to the task ti erefore the data error caused bytask ti can be calculated by
ei 1Ai
11138681113868111386811138681113868111386811138681113868
1113944
Ai| |
k1ai(k) minus ai(0)⎛⎜⎝ ⎞⎟⎠ (2)
e resident set who provides the EMRHER datasetfrom all communities can be represented as follows
Bi bji1113966 1113967
n
j1 (3)
Here bji represents the data in task ti which is provided
by the j-th community when the i-th task is initiated by i-thmedical institution when there is the mapping relationshipbelonging to C So we can calculate the data matrix cor-responding to data collection tasks from all communitiesthrough the following equation
5G networks
Cloud servers
EHR data collection
EHR data collection
EHR data collection
Medical community
Community
Community
Edge computing terminal
Figure 3 Application of directional data collection with the as-sistance of 5G and edge computing system
Journal of Healthcare Engineering 5
A aij1113966 1113967mn
i1j1
1113945m
i1Ai minus eiBi( 1113857
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus eiBi⎛⎜⎝ ⎞⎟⎠
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus ei 1113944
n
j1b
ji
⎛⎜⎝ ⎞⎟⎠
(4)
Here we redefine the data sample ai(k) in Ai as ai(k)twhich is calculated according to the time dependence of edgecomputing Note that we can update the mapping rela-tionship between each community and different medicalinstitutions through the following equation
cij
0 if 0ltaij
ei
lt cij
1 ifaij
ei
ge cij
⎧⎪⎪⎪⎪⎪⎨
⎪⎪⎪⎪⎪⎩
(5)
Here cij is the tolerance threshold of the data collectionerror which is a given empirical value
In order to analyze the direction accuracy of data col-lection conveniently we give the following definition of datacollection aggregation reliability
Definition 2 (data collection task) For m data collectiontasks and n communities the direction of data collection isaccurate when each task satisfies the following conditions
(1) e i-th task and j-th community have the mappingrelationship ie cij 1
(2) Ai and Bi have the same rank for each task ti(3) All the data samples collected by all the medical
institutions have consistency ie the followingfunction f(A) is valid
f(A) limn⟶infin
limm⟶infinA
1113936iiprime1 riprime + 1113936eisinTi
te
(6)
(4) Let Γ(ti) denote the data collection time cost etime cost of the i-th task is not larger than thedeadline τi
42 Problem Formulation e objective of directional datacollection (DDC) problem is to design a data collectionscheme based on 5G edge computing system to gather theEMRHER data from the medical community to minimizethe service error under the deadline constraint of datacollection xij is a binary variable to indicate whether data of
task ti is collected from j-th community xij 1 if data oftask ti is collected from j-th community xij 0 otherwise
e DDC problem can be formulated as follows
DDCmin xij 1113944
m
i1ei
st
(a) xij isin 0 1 forallti isin T
(b) r Ai( 1113857 r Bi( 1113857 forallti isin T
(c) 1113945m
i11113945
n
j1cij 1
(d) Γ ti( 1113857le τi forallti isin T
(7)
Constraint (a) gives the value range of xij Constraint (b)ensures that the rank of candidate data sample set is equal tothat of data in task ti on the basis of C Constraint (c) ensuresthat each mapping between the task and its correspondingcommunity is valid Constraint (d) ensures that the time costof data collection in each task is not larger than its deadline
We list the frequently used notations in Table 1
5 Intelligent Data Collection Scheme
In this section we propose our 5G edge computing enableddirectional data collection (5EDDC) algorithm en thedetailed description of the proposed algorithm is presentedin two phases data direction prediction and data collectionplanning
51 Data Direction Prediction Algorithm Medical behaviorsand requirements of residents in different communitiesactually reflect the regeneration direction of EMR whichcontains a lot of medical information such as commondiseases and medical habits Based on the implementation ofa variant of algorithms [19] we design Algorithm 1 forsolving the problem of data direction prediction
First we predict the medical behavior of residentsthrough the following steps
Step 1 Feature extraction takes into account the fol-lowing features for each behavior in community gen-erating along the historical records Bi with the last datacollection task ti and candidate sample set Ai of currentmedical community time of day medical behaviorstarting time medical community name and its loca-tion resident ID and medical treatment time of eachlocation e above procedure is denoted as functionFeature Extraction(dataset)Step 2 Random forest-based prediction needs the inputvector nt representing the information of a residentwhich includes the origin community and destinationmedical institute as well as the corresponding extractedfeatures from step 1 en the data generating time ofany community can be predicted based on temporal
6 Journal of Healthcare Engineering
data dependencies and spatial data correlations eabove process is denoted as function RandomForests
Second we can predict the data direction of communityfor collecting data via the Interval-based Historical Average(IHA) [20] as shown in the following equation
IHA E ta1113858 1113859 λ( 1113857 1
2λ + 11113944
λ
pminusλ1113944
days
q1tp minus E ta1113858 1113859 minus q1113872 1113873⎛⎝ ⎞⎠ (8)
Here E[ta] is the expectation of data generating time oftask ta based on historical EMRHER data λ is the meanabsolute error of the random forests [21] for data generatingtime prediction and days is the days of historical EMREHRdataset tp is the first data collection starting time afterE[ta] + q in the p-th day of the dataset where E[ta] + q is thegenerating time of EMRHER data for recording residents ina-th community at the q-th day us tp minus E[ta] minus q is thehistorical data collection time on the q-th day Finally wecalculate the EMREHR data generating time of commu-nities and data collection direction of medical community
In Algorithm 1 the Sink(F B) function is used to find allthe data collection sinks of EMREHR at its medical com-munity In addition Algorithm 1 updates all the datasamples and records between any two communities andcomputes their collecting time through the following steps
(1) Find all ai which can satisfy the tolerance(2) Extract all the features from historical dataset
52 Data Collection Planning Algorithm Based on the di-rection prediction of data collection the DDC problem isequivalent to finding a data route to collect the EMRHERdata for all selected medical communities with minimumtime cost e above data collection planning (DCP)problem can be formulated as follows
DCPmin 1113944C
01Γ to( 1113857 (9)
Moreover we design the data collection planning al-gorithm (DCPA) to solve the DCP probleme basic idea isgiven as follows (see Algorithm 2)
(1) Transform Ai and integrate into 1113957A (line 5)(2) Update 1113957B (line 6)(3) For each element in 1113957B we first divide it into two
separate sets P1 and P2 and then remove half ofelements in 1113957B (lines 8ndash10) and then find the cor-responding subroutes (lines 11ndash14)
(4) Integrate all the subroutes into the final data col-lection planning P (lines 15ndash18) where the symbol ⊎represents the integration of some routes
6 Numerical Experiments
In this section we conduct extensive simulations to verifythe performance of our proposed algorithms with differentnumber of medical institutions number of communitiesdays of month and number of residents of a community
61DataDescription e dataset used in our experiments isfrom the electronic records system of Changshu No 1Peoplersquos Hospital e dataset shows a kind of representativemedical community data It is generated by the medicalcommunity supported by Changshu No 1 Peoplersquos Hospitalwhich covers the period from January 1 2018 to November30 2018 e dataset includes the record data of medicalinstitute and residents and GPS data of medical institutese data record contains various fields such as time of daymedical behavior starting time medical community nameand its location resident ID medical treatment time of each
Table 1 Frequently used notations
Notation Descriptioncij Mapping relationship between i-th community and j-th different medical institutionC Set of mappingsti i-th data collection taskT Set of tasksAi Set of candidate data samples belonging to i-th taskai(k) k-th data sample in Ai
|Ai| Size of data sample in Ai
ai(0) Optimal data sample corresponding to task ti
ei Data error caused by task ti
bji Data in task ti provided by the j-th community when the i-th task is initiated by i-th medical institution
Bi Set of data in task ti on the basis of C
ai(k)t k-th data sample calculated according to the time dependence of edge computingcij Tolerance threshold of the data collection error between the i-th task and j-th communityf(A) Consistence functionτi Deadline of task ti
Journal of Healthcare Engineering 7
location and the number of patients of the correspondingmedical institute etc e GPS data contains latitude lon-gitude and treatment time of medical institute
62 Simulation Setup andBenchmark We assume that thereare 10 medical institutions to provide medical care for 10communities which are supported by Changshu No 1Peoplersquos Hospital e residents receive medical treatmentfrom the above medical institutions In our simulation weevaluate the total time cost of data collection and dataquality calculated by equation (2) All the simulations wererun on a cloud server ECS [23] with 12-core Intel XeonPlatinum 8269CY and 48GB memory e other parametersettings of our simulations are listed in Table 2
We develop the data collection algorithm DCA in [22] asthe benchmark algorithm for comparison which can makean efficient tradeoff between the data collection efficiency
and energy consumption through the combination of theenergy of the emotional device wireless device
63 Performance Evaluation In this subsection we evaluatethe performance of our algorithms and DCA in the scenarioshown in Figure 4 Tables 3 and 4 give the locations ofmedical institutions and communities in the area respec-tively e above information is calculated based on GoogleMaps
Figure 5 shows the prediction errors on two differentdays ie March 10 2018 and October 20 2018 e pre-diction results demonstrate the effectiveness of our proposedprediction algorithm DDPA e average prediction erroron March 10 2018 and October 20 2018 is 321 and193 respectively
Figures 6 and 7 show the impact of medical institutionson total time cost and data quality of our algorithms and
Input T datasetOutput A B
(1) for i 2 tom do(2) ei⟵ (1|Ai|)(1113936
|Ai |
k1 ai(k) minus ai(0))
(3) Ai⟵ ai|ai lt ei1113864 1113865(4) for j 1 to n do(5) b
ji⟵ ai(j)
(6) for each a isin A do(7) F⟵ Feature Extraction(dataset)(8) B⟵ Sink(F B)(9) for each b isin B do(10) (A B)⟵ RandomForests(F A B)
ALGORITHM 1 Data direction prediction algorithm (DDPA)
Input A B
Output P
(1) count⟵ 0 1113954A⟵A 1113957B⟵empty
(2) while countle log B minus 1 do(3) for i 1 tom do(4) for j 1 to n do(5) 1113957A⟵ 1113957ai(1) 1113957ai(2) 1113957ai(|Ai|)1113864 1113865
(6) 1113957B⟵ 1113957bj
i1113882 1113883cup 1113957B
(7) for each 1113957b isin 1113957B do(8) Take (|1113957B|2) elements to P1(9) Take another (|1113957B|2) elements to P2(10) Remove (|1113957B|2) elements from 1113957B(11) Find subroute pcount
1 of P1(12) Pcount
1 ⟵ Pcount1 cup pcount
11113864 1113865(13) Find subroute pcount
2 of P2(14) Pcount
2 ⟵ Pcount2 cup pcount
21113864 1113865(15) for each p1 isin P1 do(16) P⟵ P ⊎ p11113864 1113865(17) for each p2 isin P2 do(18) P⟵ P ⊎ p21113864 1113865
ALGORITHM 2 Data Collection Planning Algorithm (DCPA)
8 Journal of Healthcare Engineering
DCA respectively e average total time cost of our al-gorithms and DCA is 885 hours and 244 hours respec-tivelye average data quality of our algorithms and DCA is7576 and 9475 respectively e results show that ouralgorithms can reduce 7238 of total time cost of DCA onaverage and improve 2506 of data quality of DCA re-spectively is indicates that the proposed algorithmssignificantly outperform DCA is is because the dataquality of our algorithms is better than the those obtained byDCA respectively
Figures 8 and 9 show the impact of communities on totaltime cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 575 hours and 163 hours respectively eaverage data quality of our algorithms and DCA is 7327and 9759 respectively e results show that our
Table 2 Parameter settings
Parameter Valuen 10m 10|T| 10cij [001 005]τi [1 10] hours|Ai| [100 500]
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Figure 4 Medical community for EMRHER data collection ered nodes represent locations of medical institutions and the greennodes represent locations of communities
Table 3 Locations of medical institutions
i Longitude Latitude1 31629934025445163 120745726947073172 31637070592885376 120744987234992693 31641308857555806 120742605433500614 31644304755694158 1207431204176075 31639559503878488 120739966849915396 3163350810894618 120741081938852527 31634421579375328 120735202536971168 31640051243952147 120743342172446979 3163600474671818 1207442755811459110 31640862982947134 12074781351639375
Table 4 Locations of communities
i Longitude Latitude1 31633639306384033 120736407142357452 31635638094098336 120744138979835573 3164162333734517 120746486600514814 31638983794798012 120748808703562535 31641820359193588 120738421187636156 3163745217402931 120743756215726587 31643893501251643 120747443511151158 3163659402090503 1207420720531559 31634475760812066 1207435393159863510 31634834238968633 12074956147326746
7 8 9 10 11 12 13 14 15 16 170
2
4
6
8
Time
Pred
ictio
n er
ror (
)
March 10 2018
October 20 2018
Figure 5 Prediction errors on March 10 2018 and October 202018
2 4 6 8 10
5
10
15
Number of medical institutions
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 6 Total time cost vs number of medical institutions
Journal of Healthcare Engineering 9
algorithms reduces 7167 of total time cost of DCA onaverage and improves 3320 of data quality of DCArespectively
Figures 10 and 11 show the impact of days of month ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 1615 hours and 999 hours respectively eaverage data quality of our algorithms and DCA is 6331and 9401 respectively e results show that our
algorithms can reduce 3812 of total time cost of DCA onaverage and improve 4849 of data quality of DCArespectively
Figures 12 and 13 show the impact of communities ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 892 hours and 286 hours respectively eaverage data quality of our algorithms and DCA is 6844and 9521 respectively e results show that our
2 4 6 8 1050
60
70
80
90
100
Number of medical institutions
Dat
a qua
lity
()
DCAOurs
Figure 7 Data quality vs number of medical institutions
2 4 6 8 10
2
4
6
8
10
Number of communities
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 8 Total time cost vs number of communities
10 Journal of Healthcare Engineering
algorithms can reduce 6776 of total time cost of DCA onaverage and improve 3911 of data quality of DCArespectively
Overall our algorithms can significantly decrease thetotal time cost and improve the data quality through thedesigned data direction prediction algorithm and datacollection planning algorithm
7 Conclusion
In this article we have designed the 5G edge computingarchitecture for medical community to improve the effec-tiveness and efficiency of EMREHR data collection Firstwe formulate the directional data collection (DDC) problemto gather the EMRHER data from the medical communityfor minimizing the service error under the deadline con-straint of data collection deadline Second we design thedata direction prediction algorithm (DDPA) to predict thedata collection direction and propose the data collection
10 15 2050
60
70
80
90
100
Days of month
Dat
a qua
lity
()
DCAOurs
Figure 11 Data quality vs days of month
20 40 60 80 1000
2
4
6
8
10
12
Number of residents of a community
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 12 Total time cost vs number of residents of a community
20 40 60 80 10060
70
80
90
100
Number of residents of a community
Dat
a qua
lity
()
DCAOurs
Figure 13 Data quality vs number of residents of a community
2 4 6 8 1060
70
80
90
100
Number of communities
Dat
a qua
lity
()
DCAOurs
Figure 9 Data quality vs number of communities
10 15 208
10
12
14
16
18
20
Days of month
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 10 Total time cost vs days of month
Journal of Healthcare Engineering 11
planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering

A aij1113966 1113967mn
i1j1
1113945m
i1Ai minus eiBi( 1113857
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus eiBi⎛⎜⎝ ⎞⎟⎠
1113945m
i11113944
Ai| |
k11113946 ai(k)
tdt minus ei 1113944
n
j1b
ji
⎛⎜⎝ ⎞⎟⎠
(4)
Here we redefine the data sample ai(k) in Ai as ai(k)twhich is calculated according to the time dependence of edgecomputing Note that we can update the mapping rela-tionship between each community and different medicalinstitutions through the following equation
cij
0 if 0ltaij
ei
lt cij
1 ifaij
ei
ge cij
⎧⎪⎪⎪⎪⎪⎨
⎪⎪⎪⎪⎪⎩
(5)
Here cij is the tolerance threshold of the data collectionerror which is a given empirical value
In order to analyze the direction accuracy of data col-lection conveniently we give the following definition of datacollection aggregation reliability
Definition 2 (data collection task) For m data collectiontasks and n communities the direction of data collection isaccurate when each task satisfies the following conditions
(1) e i-th task and j-th community have the mappingrelationship ie cij 1
(2) Ai and Bi have the same rank for each task ti(3) All the data samples collected by all the medical
institutions have consistency ie the followingfunction f(A) is valid
f(A) limn⟶infin
limm⟶infinA
1113936iiprime1 riprime + 1113936eisinTi
te
(6)
(4) Let Γ(ti) denote the data collection time cost etime cost of the i-th task is not larger than thedeadline τi
42 Problem Formulation e objective of directional datacollection (DDC) problem is to design a data collectionscheme based on 5G edge computing system to gather theEMRHER data from the medical community to minimizethe service error under the deadline constraint of datacollection xij is a binary variable to indicate whether data of
task ti is collected from j-th community xij 1 if data oftask ti is collected from j-th community xij 0 otherwise
e DDC problem can be formulated as follows
DDCmin xij 1113944
m
i1ei
st
(a) xij isin 0 1 forallti isin T
(b) r Ai( 1113857 r Bi( 1113857 forallti isin T
(c) 1113945m
i11113945
n
j1cij 1
(d) Γ ti( 1113857le τi forallti isin T
(7)
Constraint (a) gives the value range of xij Constraint (b)ensures that the rank of candidate data sample set is equal tothat of data in task ti on the basis of C Constraint (c) ensuresthat each mapping between the task and its correspondingcommunity is valid Constraint (d) ensures that the time costof data collection in each task is not larger than its deadline
We list the frequently used notations in Table 1
5 Intelligent Data Collection Scheme
In this section we propose our 5G edge computing enableddirectional data collection (5EDDC) algorithm en thedetailed description of the proposed algorithm is presentedin two phases data direction prediction and data collectionplanning
51 Data Direction Prediction Algorithm Medical behaviorsand requirements of residents in different communitiesactually reflect the regeneration direction of EMR whichcontains a lot of medical information such as commondiseases and medical habits Based on the implementation ofa variant of algorithms [19] we design Algorithm 1 forsolving the problem of data direction prediction
First we predict the medical behavior of residentsthrough the following steps
Step 1 Feature extraction takes into account the fol-lowing features for each behavior in community gen-erating along the historical records Bi with the last datacollection task ti and candidate sample set Ai of currentmedical community time of day medical behaviorstarting time medical community name and its loca-tion resident ID and medical treatment time of eachlocation e above procedure is denoted as functionFeature Extraction(dataset)Step 2 Random forest-based prediction needs the inputvector nt representing the information of a residentwhich includes the origin community and destinationmedical institute as well as the corresponding extractedfeatures from step 1 en the data generating time ofany community can be predicted based on temporal
6 Journal of Healthcare Engineering
data dependencies and spatial data correlations eabove process is denoted as function RandomForests
Second we can predict the data direction of communityfor collecting data via the Interval-based Historical Average(IHA) [20] as shown in the following equation
IHA E ta1113858 1113859 λ( 1113857 1
2λ + 11113944
λ
pminusλ1113944
days
q1tp minus E ta1113858 1113859 minus q1113872 1113873⎛⎝ ⎞⎠ (8)
Here E[ta] is the expectation of data generating time oftask ta based on historical EMRHER data λ is the meanabsolute error of the random forests [21] for data generatingtime prediction and days is the days of historical EMREHRdataset tp is the first data collection starting time afterE[ta] + q in the p-th day of the dataset where E[ta] + q is thegenerating time of EMRHER data for recording residents ina-th community at the q-th day us tp minus E[ta] minus q is thehistorical data collection time on the q-th day Finally wecalculate the EMREHR data generating time of commu-nities and data collection direction of medical community
In Algorithm 1 the Sink(F B) function is used to find allthe data collection sinks of EMREHR at its medical com-munity In addition Algorithm 1 updates all the datasamples and records between any two communities andcomputes their collecting time through the following steps
(1) Find all ai which can satisfy the tolerance(2) Extract all the features from historical dataset
52 Data Collection Planning Algorithm Based on the di-rection prediction of data collection the DDC problem isequivalent to finding a data route to collect the EMRHERdata for all selected medical communities with minimumtime cost e above data collection planning (DCP)problem can be formulated as follows
DCPmin 1113944C
01Γ to( 1113857 (9)
Moreover we design the data collection planning al-gorithm (DCPA) to solve the DCP probleme basic idea isgiven as follows (see Algorithm 2)
(1) Transform Ai and integrate into 1113957A (line 5)(2) Update 1113957B (line 6)(3) For each element in 1113957B we first divide it into two
separate sets P1 and P2 and then remove half ofelements in 1113957B (lines 8ndash10) and then find the cor-responding subroutes (lines 11ndash14)
(4) Integrate all the subroutes into the final data col-lection planning P (lines 15ndash18) where the symbol ⊎represents the integration of some routes
6 Numerical Experiments
In this section we conduct extensive simulations to verifythe performance of our proposed algorithms with differentnumber of medical institutions number of communitiesdays of month and number of residents of a community
61DataDescription e dataset used in our experiments isfrom the electronic records system of Changshu No 1Peoplersquos Hospital e dataset shows a kind of representativemedical community data It is generated by the medicalcommunity supported by Changshu No 1 Peoplersquos Hospitalwhich covers the period from January 1 2018 to November30 2018 e dataset includes the record data of medicalinstitute and residents and GPS data of medical institutese data record contains various fields such as time of daymedical behavior starting time medical community nameand its location resident ID medical treatment time of each
Table 1 Frequently used notations
Notation Descriptioncij Mapping relationship between i-th community and j-th different medical institutionC Set of mappingsti i-th data collection taskT Set of tasksAi Set of candidate data samples belonging to i-th taskai(k) k-th data sample in Ai
|Ai| Size of data sample in Ai
ai(0) Optimal data sample corresponding to task ti
ei Data error caused by task ti
bji Data in task ti provided by the j-th community when the i-th task is initiated by i-th medical institution
Bi Set of data in task ti on the basis of C
ai(k)t k-th data sample calculated according to the time dependence of edge computingcij Tolerance threshold of the data collection error between the i-th task and j-th communityf(A) Consistence functionτi Deadline of task ti
Journal of Healthcare Engineering 7
location and the number of patients of the correspondingmedical institute etc e GPS data contains latitude lon-gitude and treatment time of medical institute
62 Simulation Setup andBenchmark We assume that thereare 10 medical institutions to provide medical care for 10communities which are supported by Changshu No 1Peoplersquos Hospital e residents receive medical treatmentfrom the above medical institutions In our simulation weevaluate the total time cost of data collection and dataquality calculated by equation (2) All the simulations wererun on a cloud server ECS [23] with 12-core Intel XeonPlatinum 8269CY and 48GB memory e other parametersettings of our simulations are listed in Table 2
We develop the data collection algorithm DCA in [22] asthe benchmark algorithm for comparison which can makean efficient tradeoff between the data collection efficiency
and energy consumption through the combination of theenergy of the emotional device wireless device
63 Performance Evaluation In this subsection we evaluatethe performance of our algorithms and DCA in the scenarioshown in Figure 4 Tables 3 and 4 give the locations ofmedical institutions and communities in the area respec-tively e above information is calculated based on GoogleMaps
Figure 5 shows the prediction errors on two differentdays ie March 10 2018 and October 20 2018 e pre-diction results demonstrate the effectiveness of our proposedprediction algorithm DDPA e average prediction erroron March 10 2018 and October 20 2018 is 321 and193 respectively
Figures 6 and 7 show the impact of medical institutionson total time cost and data quality of our algorithms and
Input T datasetOutput A B
(1) for i 2 tom do(2) ei⟵ (1|Ai|)(1113936
|Ai |
k1 ai(k) minus ai(0))
(3) Ai⟵ ai|ai lt ei1113864 1113865(4) for j 1 to n do(5) b
ji⟵ ai(j)
(6) for each a isin A do(7) F⟵ Feature Extraction(dataset)(8) B⟵ Sink(F B)(9) for each b isin B do(10) (A B)⟵ RandomForests(F A B)
ALGORITHM 1 Data direction prediction algorithm (DDPA)
Input A B
Output P
(1) count⟵ 0 1113954A⟵A 1113957B⟵empty
(2) while countle log B minus 1 do(3) for i 1 tom do(4) for j 1 to n do(5) 1113957A⟵ 1113957ai(1) 1113957ai(2) 1113957ai(|Ai|)1113864 1113865
(6) 1113957B⟵ 1113957bj
i1113882 1113883cup 1113957B
(7) for each 1113957b isin 1113957B do(8) Take (|1113957B|2) elements to P1(9) Take another (|1113957B|2) elements to P2(10) Remove (|1113957B|2) elements from 1113957B(11) Find subroute pcount
1 of P1(12) Pcount
1 ⟵ Pcount1 cup pcount
11113864 1113865(13) Find subroute pcount
2 of P2(14) Pcount
2 ⟵ Pcount2 cup pcount
21113864 1113865(15) for each p1 isin P1 do(16) P⟵ P ⊎ p11113864 1113865(17) for each p2 isin P2 do(18) P⟵ P ⊎ p21113864 1113865
ALGORITHM 2 Data Collection Planning Algorithm (DCPA)
8 Journal of Healthcare Engineering
DCA respectively e average total time cost of our al-gorithms and DCA is 885 hours and 244 hours respec-tivelye average data quality of our algorithms and DCA is7576 and 9475 respectively e results show that ouralgorithms can reduce 7238 of total time cost of DCA onaverage and improve 2506 of data quality of DCA re-spectively is indicates that the proposed algorithmssignificantly outperform DCA is is because the dataquality of our algorithms is better than the those obtained byDCA respectively
Figures 8 and 9 show the impact of communities on totaltime cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 575 hours and 163 hours respectively eaverage data quality of our algorithms and DCA is 7327and 9759 respectively e results show that our
Table 2 Parameter settings
Parameter Valuen 10m 10|T| 10cij [001 005]τi [1 10] hours|Ai| [100 500]
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Figure 4 Medical community for EMRHER data collection ered nodes represent locations of medical institutions and the greennodes represent locations of communities
Table 3 Locations of medical institutions
i Longitude Latitude1 31629934025445163 120745726947073172 31637070592885376 120744987234992693 31641308857555806 120742605433500614 31644304755694158 1207431204176075 31639559503878488 120739966849915396 3163350810894618 120741081938852527 31634421579375328 120735202536971168 31640051243952147 120743342172446979 3163600474671818 1207442755811459110 31640862982947134 12074781351639375
Table 4 Locations of communities
i Longitude Latitude1 31633639306384033 120736407142357452 31635638094098336 120744138979835573 3164162333734517 120746486600514814 31638983794798012 120748808703562535 31641820359193588 120738421187636156 3163745217402931 120743756215726587 31643893501251643 120747443511151158 3163659402090503 1207420720531559 31634475760812066 1207435393159863510 31634834238968633 12074956147326746
7 8 9 10 11 12 13 14 15 16 170
2
4
6
8
Time
Pred
ictio
n er
ror (
)
March 10 2018
October 20 2018
Figure 5 Prediction errors on March 10 2018 and October 202018
2 4 6 8 10
5
10
15
Number of medical institutions
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 6 Total time cost vs number of medical institutions
Journal of Healthcare Engineering 9
algorithms reduces 7167 of total time cost of DCA onaverage and improves 3320 of data quality of DCArespectively
Figures 10 and 11 show the impact of days of month ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 1615 hours and 999 hours respectively eaverage data quality of our algorithms and DCA is 6331and 9401 respectively e results show that our
algorithms can reduce 3812 of total time cost of DCA onaverage and improve 4849 of data quality of DCArespectively
Figures 12 and 13 show the impact of communities ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 892 hours and 286 hours respectively eaverage data quality of our algorithms and DCA is 6844and 9521 respectively e results show that our
2 4 6 8 1050
60
70
80
90
100
Number of medical institutions
Dat
a qua
lity
()
DCAOurs
Figure 7 Data quality vs number of medical institutions
2 4 6 8 10
2
4
6
8
10
Number of communities
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 8 Total time cost vs number of communities
10 Journal of Healthcare Engineering
algorithms can reduce 6776 of total time cost of DCA onaverage and improve 3911 of data quality of DCArespectively
Overall our algorithms can significantly decrease thetotal time cost and improve the data quality through thedesigned data direction prediction algorithm and datacollection planning algorithm
7 Conclusion
In this article we have designed the 5G edge computingarchitecture for medical community to improve the effec-tiveness and efficiency of EMREHR data collection Firstwe formulate the directional data collection (DDC) problemto gather the EMRHER data from the medical communityfor minimizing the service error under the deadline con-straint of data collection deadline Second we design thedata direction prediction algorithm (DDPA) to predict thedata collection direction and propose the data collection
10 15 2050
60
70
80
90
100
Days of month
Dat
a qua
lity
()
DCAOurs
Figure 11 Data quality vs days of month
20 40 60 80 1000
2
4
6
8
10
12
Number of residents of a community
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 12 Total time cost vs number of residents of a community
20 40 60 80 10060
70
80
90
100
Number of residents of a community
Dat
a qua
lity
()
DCAOurs
Figure 13 Data quality vs number of residents of a community
2 4 6 8 1060
70
80
90
100
Number of communities
Dat
a qua
lity
()
DCAOurs
Figure 9 Data quality vs number of communities
10 15 208
10
12
14
16
18
20
Days of month
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 10 Total time cost vs days of month
Journal of Healthcare Engineering 11
planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering

data dependencies and spatial data correlations eabove process is denoted as function RandomForests
Second we can predict the data direction of communityfor collecting data via the Interval-based Historical Average(IHA) [20] as shown in the following equation
IHA E ta1113858 1113859 λ( 1113857 1
2λ + 11113944
λ
pminusλ1113944
days
q1tp minus E ta1113858 1113859 minus q1113872 1113873⎛⎝ ⎞⎠ (8)
Here E[ta] is the expectation of data generating time oftask ta based on historical EMRHER data λ is the meanabsolute error of the random forests [21] for data generatingtime prediction and days is the days of historical EMREHRdataset tp is the first data collection starting time afterE[ta] + q in the p-th day of the dataset where E[ta] + q is thegenerating time of EMRHER data for recording residents ina-th community at the q-th day us tp minus E[ta] minus q is thehistorical data collection time on the q-th day Finally wecalculate the EMREHR data generating time of commu-nities and data collection direction of medical community
In Algorithm 1 the Sink(F B) function is used to find allthe data collection sinks of EMREHR at its medical com-munity In addition Algorithm 1 updates all the datasamples and records between any two communities andcomputes their collecting time through the following steps
(1) Find all ai which can satisfy the tolerance(2) Extract all the features from historical dataset
52 Data Collection Planning Algorithm Based on the di-rection prediction of data collection the DDC problem isequivalent to finding a data route to collect the EMRHERdata for all selected medical communities with minimumtime cost e above data collection planning (DCP)problem can be formulated as follows
DCPmin 1113944C
01Γ to( 1113857 (9)
Moreover we design the data collection planning al-gorithm (DCPA) to solve the DCP probleme basic idea isgiven as follows (see Algorithm 2)
(1) Transform Ai and integrate into 1113957A (line 5)(2) Update 1113957B (line 6)(3) For each element in 1113957B we first divide it into two
separate sets P1 and P2 and then remove half ofelements in 1113957B (lines 8ndash10) and then find the cor-responding subroutes (lines 11ndash14)
(4) Integrate all the subroutes into the final data col-lection planning P (lines 15ndash18) where the symbol ⊎represents the integration of some routes
6 Numerical Experiments
In this section we conduct extensive simulations to verifythe performance of our proposed algorithms with differentnumber of medical institutions number of communitiesdays of month and number of residents of a community
61DataDescription e dataset used in our experiments isfrom the electronic records system of Changshu No 1Peoplersquos Hospital e dataset shows a kind of representativemedical community data It is generated by the medicalcommunity supported by Changshu No 1 Peoplersquos Hospitalwhich covers the period from January 1 2018 to November30 2018 e dataset includes the record data of medicalinstitute and residents and GPS data of medical institutese data record contains various fields such as time of daymedical behavior starting time medical community nameand its location resident ID medical treatment time of each
Table 1 Frequently used notations
Notation Descriptioncij Mapping relationship between i-th community and j-th different medical institutionC Set of mappingsti i-th data collection taskT Set of tasksAi Set of candidate data samples belonging to i-th taskai(k) k-th data sample in Ai
|Ai| Size of data sample in Ai
ai(0) Optimal data sample corresponding to task ti
ei Data error caused by task ti
bji Data in task ti provided by the j-th community when the i-th task is initiated by i-th medical institution
Bi Set of data in task ti on the basis of C
ai(k)t k-th data sample calculated according to the time dependence of edge computingcij Tolerance threshold of the data collection error between the i-th task and j-th communityf(A) Consistence functionτi Deadline of task ti
Journal of Healthcare Engineering 7
location and the number of patients of the correspondingmedical institute etc e GPS data contains latitude lon-gitude and treatment time of medical institute
62 Simulation Setup andBenchmark We assume that thereare 10 medical institutions to provide medical care for 10communities which are supported by Changshu No 1Peoplersquos Hospital e residents receive medical treatmentfrom the above medical institutions In our simulation weevaluate the total time cost of data collection and dataquality calculated by equation (2) All the simulations wererun on a cloud server ECS [23] with 12-core Intel XeonPlatinum 8269CY and 48GB memory e other parametersettings of our simulations are listed in Table 2
We develop the data collection algorithm DCA in [22] asthe benchmark algorithm for comparison which can makean efficient tradeoff between the data collection efficiency
and energy consumption through the combination of theenergy of the emotional device wireless device
63 Performance Evaluation In this subsection we evaluatethe performance of our algorithms and DCA in the scenarioshown in Figure 4 Tables 3 and 4 give the locations ofmedical institutions and communities in the area respec-tively e above information is calculated based on GoogleMaps
Figure 5 shows the prediction errors on two differentdays ie March 10 2018 and October 20 2018 e pre-diction results demonstrate the effectiveness of our proposedprediction algorithm DDPA e average prediction erroron March 10 2018 and October 20 2018 is 321 and193 respectively
Figures 6 and 7 show the impact of medical institutionson total time cost and data quality of our algorithms and
Input T datasetOutput A B
(1) for i 2 tom do(2) ei⟵ (1|Ai|)(1113936
|Ai |
k1 ai(k) minus ai(0))
(3) Ai⟵ ai|ai lt ei1113864 1113865(4) for j 1 to n do(5) b
ji⟵ ai(j)
(6) for each a isin A do(7) F⟵ Feature Extraction(dataset)(8) B⟵ Sink(F B)(9) for each b isin B do(10) (A B)⟵ RandomForests(F A B)
ALGORITHM 1 Data direction prediction algorithm (DDPA)
Input A B
Output P
(1) count⟵ 0 1113954A⟵A 1113957B⟵empty
(2) while countle log B minus 1 do(3) for i 1 tom do(4) for j 1 to n do(5) 1113957A⟵ 1113957ai(1) 1113957ai(2) 1113957ai(|Ai|)1113864 1113865
(6) 1113957B⟵ 1113957bj
i1113882 1113883cup 1113957B
(7) for each 1113957b isin 1113957B do(8) Take (|1113957B|2) elements to P1(9) Take another (|1113957B|2) elements to P2(10) Remove (|1113957B|2) elements from 1113957B(11) Find subroute pcount
1 of P1(12) Pcount
1 ⟵ Pcount1 cup pcount
11113864 1113865(13) Find subroute pcount
2 of P2(14) Pcount
2 ⟵ Pcount2 cup pcount
21113864 1113865(15) for each p1 isin P1 do(16) P⟵ P ⊎ p11113864 1113865(17) for each p2 isin P2 do(18) P⟵ P ⊎ p21113864 1113865
ALGORITHM 2 Data Collection Planning Algorithm (DCPA)
8 Journal of Healthcare Engineering
DCA respectively e average total time cost of our al-gorithms and DCA is 885 hours and 244 hours respec-tivelye average data quality of our algorithms and DCA is7576 and 9475 respectively e results show that ouralgorithms can reduce 7238 of total time cost of DCA onaverage and improve 2506 of data quality of DCA re-spectively is indicates that the proposed algorithmssignificantly outperform DCA is is because the dataquality of our algorithms is better than the those obtained byDCA respectively
Figures 8 and 9 show the impact of communities on totaltime cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 575 hours and 163 hours respectively eaverage data quality of our algorithms and DCA is 7327and 9759 respectively e results show that our
Table 2 Parameter settings
Parameter Valuen 10m 10|T| 10cij [001 005]τi [1 10] hours|Ai| [100 500]
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Figure 4 Medical community for EMRHER data collection ered nodes represent locations of medical institutions and the greennodes represent locations of communities
Table 3 Locations of medical institutions
i Longitude Latitude1 31629934025445163 120745726947073172 31637070592885376 120744987234992693 31641308857555806 120742605433500614 31644304755694158 1207431204176075 31639559503878488 120739966849915396 3163350810894618 120741081938852527 31634421579375328 120735202536971168 31640051243952147 120743342172446979 3163600474671818 1207442755811459110 31640862982947134 12074781351639375
Table 4 Locations of communities
i Longitude Latitude1 31633639306384033 120736407142357452 31635638094098336 120744138979835573 3164162333734517 120746486600514814 31638983794798012 120748808703562535 31641820359193588 120738421187636156 3163745217402931 120743756215726587 31643893501251643 120747443511151158 3163659402090503 1207420720531559 31634475760812066 1207435393159863510 31634834238968633 12074956147326746
7 8 9 10 11 12 13 14 15 16 170
2
4
6
8
Time
Pred
ictio
n er
ror (
)
March 10 2018
October 20 2018
Figure 5 Prediction errors on March 10 2018 and October 202018
2 4 6 8 10
5
10
15
Number of medical institutions
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 6 Total time cost vs number of medical institutions
Journal of Healthcare Engineering 9
algorithms reduces 7167 of total time cost of DCA onaverage and improves 3320 of data quality of DCArespectively
Figures 10 and 11 show the impact of days of month ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 1615 hours and 999 hours respectively eaverage data quality of our algorithms and DCA is 6331and 9401 respectively e results show that our
algorithms can reduce 3812 of total time cost of DCA onaverage and improve 4849 of data quality of DCArespectively
Figures 12 and 13 show the impact of communities ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 892 hours and 286 hours respectively eaverage data quality of our algorithms and DCA is 6844and 9521 respectively e results show that our
2 4 6 8 1050
60
70
80
90
100
Number of medical institutions
Dat
a qua
lity
()
DCAOurs
Figure 7 Data quality vs number of medical institutions
2 4 6 8 10
2
4
6
8
10
Number of communities
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 8 Total time cost vs number of communities
10 Journal of Healthcare Engineering
algorithms can reduce 6776 of total time cost of DCA onaverage and improve 3911 of data quality of DCArespectively
Overall our algorithms can significantly decrease thetotal time cost and improve the data quality through thedesigned data direction prediction algorithm and datacollection planning algorithm
7 Conclusion
In this article we have designed the 5G edge computingarchitecture for medical community to improve the effec-tiveness and efficiency of EMREHR data collection Firstwe formulate the directional data collection (DDC) problemto gather the EMRHER data from the medical communityfor minimizing the service error under the deadline con-straint of data collection deadline Second we design thedata direction prediction algorithm (DDPA) to predict thedata collection direction and propose the data collection
10 15 2050
60
70
80
90
100
Days of month
Dat
a qua
lity
()
DCAOurs
Figure 11 Data quality vs days of month
20 40 60 80 1000
2
4
6
8
10
12
Number of residents of a community
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 12 Total time cost vs number of residents of a community
20 40 60 80 10060
70
80
90
100
Number of residents of a community
Dat
a qua
lity
()
DCAOurs
Figure 13 Data quality vs number of residents of a community
2 4 6 8 1060
70
80
90
100
Number of communities
Dat
a qua
lity
()
DCAOurs
Figure 9 Data quality vs number of communities
10 15 208
10
12
14
16
18
20
Days of month
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 10 Total time cost vs days of month
Journal of Healthcare Engineering 11
planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering

location and the number of patients of the correspondingmedical institute etc e GPS data contains latitude lon-gitude and treatment time of medical institute
62 Simulation Setup andBenchmark We assume that thereare 10 medical institutions to provide medical care for 10communities which are supported by Changshu No 1Peoplersquos Hospital e residents receive medical treatmentfrom the above medical institutions In our simulation weevaluate the total time cost of data collection and dataquality calculated by equation (2) All the simulations wererun on a cloud server ECS [23] with 12-core Intel XeonPlatinum 8269CY and 48GB memory e other parametersettings of our simulations are listed in Table 2
We develop the data collection algorithm DCA in [22] asthe benchmark algorithm for comparison which can makean efficient tradeoff between the data collection efficiency
and energy consumption through the combination of theenergy of the emotional device wireless device
63 Performance Evaluation In this subsection we evaluatethe performance of our algorithms and DCA in the scenarioshown in Figure 4 Tables 3 and 4 give the locations ofmedical institutions and communities in the area respec-tively e above information is calculated based on GoogleMaps
Figure 5 shows the prediction errors on two differentdays ie March 10 2018 and October 20 2018 e pre-diction results demonstrate the effectiveness of our proposedprediction algorithm DDPA e average prediction erroron March 10 2018 and October 20 2018 is 321 and193 respectively
Figures 6 and 7 show the impact of medical institutionson total time cost and data quality of our algorithms and
Input T datasetOutput A B
(1) for i 2 tom do(2) ei⟵ (1|Ai|)(1113936
|Ai |
k1 ai(k) minus ai(0))
(3) Ai⟵ ai|ai lt ei1113864 1113865(4) for j 1 to n do(5) b
ji⟵ ai(j)
(6) for each a isin A do(7) F⟵ Feature Extraction(dataset)(8) B⟵ Sink(F B)(9) for each b isin B do(10) (A B)⟵ RandomForests(F A B)
ALGORITHM 1 Data direction prediction algorithm (DDPA)
Input A B
Output P
(1) count⟵ 0 1113954A⟵A 1113957B⟵empty
(2) while countle log B minus 1 do(3) for i 1 tom do(4) for j 1 to n do(5) 1113957A⟵ 1113957ai(1) 1113957ai(2) 1113957ai(|Ai|)1113864 1113865
(6) 1113957B⟵ 1113957bj
i1113882 1113883cup 1113957B
(7) for each 1113957b isin 1113957B do(8) Take (|1113957B|2) elements to P1(9) Take another (|1113957B|2) elements to P2(10) Remove (|1113957B|2) elements from 1113957B(11) Find subroute pcount
1 of P1(12) Pcount
1 ⟵ Pcount1 cup pcount
11113864 1113865(13) Find subroute pcount
2 of P2(14) Pcount
2 ⟵ Pcount2 cup pcount
21113864 1113865(15) for each p1 isin P1 do(16) P⟵ P ⊎ p11113864 1113865(17) for each p2 isin P2 do(18) P⟵ P ⊎ p21113864 1113865
ALGORITHM 2 Data Collection Planning Algorithm (DCPA)
8 Journal of Healthcare Engineering
DCA respectively e average total time cost of our al-gorithms and DCA is 885 hours and 244 hours respec-tivelye average data quality of our algorithms and DCA is7576 and 9475 respectively e results show that ouralgorithms can reduce 7238 of total time cost of DCA onaverage and improve 2506 of data quality of DCA re-spectively is indicates that the proposed algorithmssignificantly outperform DCA is is because the dataquality of our algorithms is better than the those obtained byDCA respectively
Figures 8 and 9 show the impact of communities on totaltime cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 575 hours and 163 hours respectively eaverage data quality of our algorithms and DCA is 7327and 9759 respectively e results show that our
Table 2 Parameter settings
Parameter Valuen 10m 10|T| 10cij [001 005]τi [1 10] hours|Ai| [100 500]
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Figure 4 Medical community for EMRHER data collection ered nodes represent locations of medical institutions and the greennodes represent locations of communities
Table 3 Locations of medical institutions
i Longitude Latitude1 31629934025445163 120745726947073172 31637070592885376 120744987234992693 31641308857555806 120742605433500614 31644304755694158 1207431204176075 31639559503878488 120739966849915396 3163350810894618 120741081938852527 31634421579375328 120735202536971168 31640051243952147 120743342172446979 3163600474671818 1207442755811459110 31640862982947134 12074781351639375
Table 4 Locations of communities
i Longitude Latitude1 31633639306384033 120736407142357452 31635638094098336 120744138979835573 3164162333734517 120746486600514814 31638983794798012 120748808703562535 31641820359193588 120738421187636156 3163745217402931 120743756215726587 31643893501251643 120747443511151158 3163659402090503 1207420720531559 31634475760812066 1207435393159863510 31634834238968633 12074956147326746
7 8 9 10 11 12 13 14 15 16 170
2
4
6
8
Time
Pred
ictio
n er
ror (
)
March 10 2018
October 20 2018
Figure 5 Prediction errors on March 10 2018 and October 202018
2 4 6 8 10
5
10
15
Number of medical institutions
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 6 Total time cost vs number of medical institutions
Journal of Healthcare Engineering 9
algorithms reduces 7167 of total time cost of DCA onaverage and improves 3320 of data quality of DCArespectively
Figures 10 and 11 show the impact of days of month ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 1615 hours and 999 hours respectively eaverage data quality of our algorithms and DCA is 6331and 9401 respectively e results show that our
algorithms can reduce 3812 of total time cost of DCA onaverage and improve 4849 of data quality of DCArespectively
Figures 12 and 13 show the impact of communities ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 892 hours and 286 hours respectively eaverage data quality of our algorithms and DCA is 6844and 9521 respectively e results show that our
2 4 6 8 1050
60
70
80
90
100
Number of medical institutions
Dat
a qua
lity
()
DCAOurs
Figure 7 Data quality vs number of medical institutions
2 4 6 8 10
2
4
6
8
10
Number of communities
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 8 Total time cost vs number of communities
10 Journal of Healthcare Engineering
algorithms can reduce 6776 of total time cost of DCA onaverage and improve 3911 of data quality of DCArespectively
Overall our algorithms can significantly decrease thetotal time cost and improve the data quality through thedesigned data direction prediction algorithm and datacollection planning algorithm
7 Conclusion
In this article we have designed the 5G edge computingarchitecture for medical community to improve the effec-tiveness and efficiency of EMREHR data collection Firstwe formulate the directional data collection (DDC) problemto gather the EMRHER data from the medical communityfor minimizing the service error under the deadline con-straint of data collection deadline Second we design thedata direction prediction algorithm (DDPA) to predict thedata collection direction and propose the data collection
10 15 2050
60
70
80
90
100
Days of month
Dat
a qua
lity
()
DCAOurs
Figure 11 Data quality vs days of month
20 40 60 80 1000
2
4
6
8
10
12
Number of residents of a community
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 12 Total time cost vs number of residents of a community
20 40 60 80 10060
70
80
90
100
Number of residents of a community
Dat
a qua
lity
()
DCAOurs
Figure 13 Data quality vs number of residents of a community
2 4 6 8 1060
70
80
90
100
Number of communities
Dat
a qua
lity
()
DCAOurs
Figure 9 Data quality vs number of communities
10 15 208
10
12
14
16
18
20
Days of month
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 10 Total time cost vs days of month
Journal of Healthcare Engineering 11
planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering

DCA respectively e average total time cost of our al-gorithms and DCA is 885 hours and 244 hours respec-tivelye average data quality of our algorithms and DCA is7576 and 9475 respectively e results show that ouralgorithms can reduce 7238 of total time cost of DCA onaverage and improve 2506 of data quality of DCA re-spectively is indicates that the proposed algorithmssignificantly outperform DCA is is because the dataquality of our algorithms is better than the those obtained byDCA respectively
Figures 8 and 9 show the impact of communities on totaltime cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 575 hours and 163 hours respectively eaverage data quality of our algorithms and DCA is 7327and 9759 respectively e results show that our
Table 2 Parameter settings
Parameter Valuen 10m 10|T| 10cij [001 005]τi [1 10] hours|Ai| [100 500]
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Figure 4 Medical community for EMRHER data collection ered nodes represent locations of medical institutions and the greennodes represent locations of communities
Table 3 Locations of medical institutions
i Longitude Latitude1 31629934025445163 120745726947073172 31637070592885376 120744987234992693 31641308857555806 120742605433500614 31644304755694158 1207431204176075 31639559503878488 120739966849915396 3163350810894618 120741081938852527 31634421579375328 120735202536971168 31640051243952147 120743342172446979 3163600474671818 1207442755811459110 31640862982947134 12074781351639375
Table 4 Locations of communities
i Longitude Latitude1 31633639306384033 120736407142357452 31635638094098336 120744138979835573 3164162333734517 120746486600514814 31638983794798012 120748808703562535 31641820359193588 120738421187636156 3163745217402931 120743756215726587 31643893501251643 120747443511151158 3163659402090503 1207420720531559 31634475760812066 1207435393159863510 31634834238968633 12074956147326746
7 8 9 10 11 12 13 14 15 16 170
2
4
6
8
Time
Pred
ictio
n er
ror (
)
March 10 2018
October 20 2018
Figure 5 Prediction errors on March 10 2018 and October 202018
2 4 6 8 10
5
10
15
Number of medical institutions
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 6 Total time cost vs number of medical institutions
Journal of Healthcare Engineering 9
algorithms reduces 7167 of total time cost of DCA onaverage and improves 3320 of data quality of DCArespectively
Figures 10 and 11 show the impact of days of month ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 1615 hours and 999 hours respectively eaverage data quality of our algorithms and DCA is 6331and 9401 respectively e results show that our
algorithms can reduce 3812 of total time cost of DCA onaverage and improve 4849 of data quality of DCArespectively
Figures 12 and 13 show the impact of communities ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 892 hours and 286 hours respectively eaverage data quality of our algorithms and DCA is 6844and 9521 respectively e results show that our
2 4 6 8 1050
60
70
80
90
100
Number of medical institutions
Dat
a qua
lity
()
DCAOurs
Figure 7 Data quality vs number of medical institutions
2 4 6 8 10
2
4
6
8
10
Number of communities
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 8 Total time cost vs number of communities
10 Journal of Healthcare Engineering
algorithms can reduce 6776 of total time cost of DCA onaverage and improve 3911 of data quality of DCArespectively
Overall our algorithms can significantly decrease thetotal time cost and improve the data quality through thedesigned data direction prediction algorithm and datacollection planning algorithm
7 Conclusion
In this article we have designed the 5G edge computingarchitecture for medical community to improve the effec-tiveness and efficiency of EMREHR data collection Firstwe formulate the directional data collection (DDC) problemto gather the EMRHER data from the medical communityfor minimizing the service error under the deadline con-straint of data collection deadline Second we design thedata direction prediction algorithm (DDPA) to predict thedata collection direction and propose the data collection
10 15 2050
60
70
80
90
100
Days of month
Dat
a qua
lity
()
DCAOurs
Figure 11 Data quality vs days of month
20 40 60 80 1000
2
4
6
8
10
12
Number of residents of a community
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 12 Total time cost vs number of residents of a community
20 40 60 80 10060
70
80
90
100
Number of residents of a community
Dat
a qua
lity
()
DCAOurs
Figure 13 Data quality vs number of residents of a community
2 4 6 8 1060
70
80
90
100
Number of communities
Dat
a qua
lity
()
DCAOurs
Figure 9 Data quality vs number of communities
10 15 208
10
12
14
16
18
20
Days of month
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 10 Total time cost vs days of month
Journal of Healthcare Engineering 11
planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering

algorithms reduces 7167 of total time cost of DCA onaverage and improves 3320 of data quality of DCArespectively
Figures 10 and 11 show the impact of days of month ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 1615 hours and 999 hours respectively eaverage data quality of our algorithms and DCA is 6331and 9401 respectively e results show that our
algorithms can reduce 3812 of total time cost of DCA onaverage and improve 4849 of data quality of DCArespectively
Figures 12 and 13 show the impact of communities ontotal time cost and data quality of our algorithms and DCArespectively e average total time cost of our algorithmsand DCA is 892 hours and 286 hours respectively eaverage data quality of our algorithms and DCA is 6844and 9521 respectively e results show that our
2 4 6 8 1050
60
70
80
90
100
Number of medical institutions
Dat
a qua
lity
()
DCAOurs
Figure 7 Data quality vs number of medical institutions
2 4 6 8 10
2
4
6
8
10
Number of communities
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 8 Total time cost vs number of communities
10 Journal of Healthcare Engineering
algorithms can reduce 6776 of total time cost of DCA onaverage and improve 3911 of data quality of DCArespectively
Overall our algorithms can significantly decrease thetotal time cost and improve the data quality through thedesigned data direction prediction algorithm and datacollection planning algorithm
7 Conclusion
In this article we have designed the 5G edge computingarchitecture for medical community to improve the effec-tiveness and efficiency of EMREHR data collection Firstwe formulate the directional data collection (DDC) problemto gather the EMRHER data from the medical communityfor minimizing the service error under the deadline con-straint of data collection deadline Second we design thedata direction prediction algorithm (DDPA) to predict thedata collection direction and propose the data collection
10 15 2050
60
70
80
90
100
Days of month
Dat
a qua
lity
()
DCAOurs
Figure 11 Data quality vs days of month
20 40 60 80 1000
2
4
6
8
10
12
Number of residents of a community
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 12 Total time cost vs number of residents of a community
20 40 60 80 10060
70
80
90
100
Number of residents of a community
Dat
a qua
lity
()
DCAOurs
Figure 13 Data quality vs number of residents of a community
2 4 6 8 1060
70
80
90
100
Number of communities
Dat
a qua
lity
()
DCAOurs
Figure 9 Data quality vs number of communities
10 15 208
10
12
14
16
18
20
Days of month
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 10 Total time cost vs days of month
Journal of Healthcare Engineering 11
planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering

algorithms can reduce 6776 of total time cost of DCA onaverage and improve 3911 of data quality of DCArespectively
Overall our algorithms can significantly decrease thetotal time cost and improve the data quality through thedesigned data direction prediction algorithm and datacollection planning algorithm
7 Conclusion
In this article we have designed the 5G edge computingarchitecture for medical community to improve the effec-tiveness and efficiency of EMREHR data collection Firstwe formulate the directional data collection (DDC) problemto gather the EMRHER data from the medical communityfor minimizing the service error under the deadline con-straint of data collection deadline Second we design thedata direction prediction algorithm (DDPA) to predict thedata collection direction and propose the data collection
10 15 2050
60
70
80
90
100
Days of month
Dat
a qua
lity
()
DCAOurs
Figure 11 Data quality vs days of month
20 40 60 80 1000
2
4
6
8
10
12
Number of residents of a community
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 12 Total time cost vs number of residents of a community
20 40 60 80 10060
70
80
90
100
Number of residents of a community
Dat
a qua
lity
()
DCAOurs
Figure 13 Data quality vs number of residents of a community
2 4 6 8 1060
70
80
90
100
Number of communities
Dat
a qua
lity
()
DCAOurs
Figure 9 Data quality vs number of communities
10 15 208
10
12
14
16
18
20
Days of month
Tota
l tim
e cos
t (ho
urs)
DCAOurs
Figure 10 Total time cost vs days of month
Journal of Healthcare Engineering 11
planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering

planning algorithm (DCPA) to minimize the data collectingtime cost Finally through the numerical simulation ex-periments we demonstrate that our proposed algorithmscan decrease the total time cost by 6248 and improve thedata quality by 3647 through the designed systemrespectively
Data Availability
e labeled dataset used to support the findings of this studyis available from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] Z Liu C Bai H Yu et al ldquoAn adaptive deep learning modelto differentiate syndromes of infectious fever in smartmedicinerdquo Future Generation Computer Systems vol 111pp 853ndash858 2020
[2] A K Jha C M DesRoches E G Campbell et al ldquoUse ofelectronic health records in US hospitalsrdquo New EnglandJournal of Medicine vol 360 no 16 pp 1628ndash1638 2009
[3] P Elanthiraiyan andD S Babu ldquoSmart medicine and physicalhealth system using IoTrdquo International Journal of ComputerScience and Mobile Computing vol 4 no 3 pp 333ndash3382015
[4] National Health Commission of the Peoplersquos Republic ofChina httpwwwnhcgovcn
[5] D Blumenthal and M Tavenner ldquoe ldquomeaningful userdquoregulation for electronic health recordsrdquoNew England Journalof Medicine vol 363 no 6 pp 501ndash504 2010
[6] F Mostashari M Tripathi and M Kendall ldquoA tale of twolarge community electronic health record extension projectsrdquoHealth Affairs vol 28 no 2 pp 345ndash356 2009
[7] M Z Hydari R Telang and W M Marella ldquoElectronichealth records and patient safetyrdquo Communications of theACM vol 58 no 11 pp 30ndash32 2015
[8] R H Miller and C E West ldquoe value of electronic healthrecords in community health centers policy implicationsrdquoHealth Affairs vol 26 no 1 pp 206ndash214 2007
[9] G P Samsa D B Matchar L B Goldstein et al ldquoQuality ofanticoagulation management among patients with atrial fi-brillation results of a review of medical records from 2communitiesrdquo Archives of Internal Medicine vol 160 no 7pp 967ndash973 2000
[10] D J Katzelnick G E Simon S D Pearson et al ldquoRan-domized trial of a depression management program in highutilizers of medical carerdquo Archives of Family Medicine vol 9no 4 pp 345ndash351 2000
[11] F Qiu ldquoHospital archives intelligent management systembased on 5G network and internet of things systemrdquo Mi-croprocessors and Microsystems vol 80 Article ID 1035642021
[12] L Meng M Pammi A Saronwala et al ldquoUse of exomesequencing for infants in intensive care unitsrdquo JAMA Pedi-atrics vol 171 no 12 Article ID e173438 2017
[13] F Jamil L Hang K Kim and D Kim ldquoA novel medicalblockchain model for drug supply chain integrity manage-ment in a smart hospitalrdquo Electronics vol 8 no 5 p 5052019
[14] H Xie Z Yan Z Yao et al ldquoData collection for securitymeasurement in wireless sensor networks a surveyrdquo IEEEInternet of 13ings Journal vol 6 no 2 pp 2205ndash2224 2018
[15] J P Choi D-S Jeon and B-C Kim ldquoPrivacy and personaldata collection with information externalitiesrdquo Journal ofPublic Economics vol 173 pp 113ndash124 2019
[16] J Gong T-H Chang C Shen and X Chen ldquoFlight timeminimization of UAV for data collection over wireless sensornetworksrdquo IEEE Journal on Selected Areas in Communica-tions vol 36 no 9 pp 1942ndash1954 2018
[17] J TanW Liu M Xie et al ldquoA low redundancy data collectionscheme to maximize lifetime using matrix completion tech-niquerdquo EURASIP Journal on Wireless Communications andNetworking vol 2019 no 1 pp 1ndash29 2019
[18] E Luo M Z A Bhuiyan GWang M A Rahman J Wu andM Atiquzzaman ldquoPrivacyProtector privacy-protected pa-tient data collection in IoT-based healthcare systemsrdquo IEEECommunications Magazine vol 56 no 2 pp 163ndash168 2018
[19] Y Wang S T Xia Q Tang J Wu and X Zhu ldquoA novelconsistent random forest framework Bernoulli randomforestsrdquo IEEE Transactions on Neural Networks and LearningSystems vol 29 no 8 pp 3510ndash3523 2018
[20] P He G Jiang S Lam et al ldquoTravel-time prediction of busjourney with multiple bus tripsrdquo IEEE Transactions on In-telligent Transportation Systems vol 20 no 11 pp 4192ndash4205 2019
[21] L Breiman ldquoRandom forestsrdquo Machine Learning vol 45no 1 pp 5ndash32 2001
[22] ldquoAliyun ECS cloud serverrdquo 2021 httpswwwaliyuncomproductecs
[23] Y Jin Z Qian and S Chen ldquoData collection scheme withminimum cost and location of emotional recognition edgedevicesrdquo Personal and Ubiquitous Computing vol 23 no 3-4pp 595ndash606 2019
12 Journal of Healthcare Engineering