Embed Size (px)
Citation preview

الرحمن الله بسمالرحيمBirth Injury

Birth Injury
Definition: The term birth injury is used to denote avoidable and unavoidable mechanical and anoxic trauma incurred by the infant during labor and delivery.

Birth Injury
Predisposing factors
Maternal factors: Primiparity, small maternal stature, or maternal pelvic anomalies.
Delivery factors: Prolonged or extremely rapid labor, or use of midforceps or vacuum extraction.
Fetal factors: Prematurity, fetal macrosomia, or abnormal presentation (i.e. breech).

Cranial Injuries
Caput succedaneum Cephalhematoma

Differentiation between Caput Succedaneum and Cephalhematoma
Item Caput Succedaneum Cephalhematoma
Composition Serosanginous infiltration of skin and subcutaneous tissue of the scalp
Subperiosteal hematoma (between the bone and its periosteum)
Site Over the presenting site Any bone, usually the parietal bone
Onset of appearance At birth Few hours after birth
Consistency Soft, edematous Firm, feeling of depressed fracture on palpation of the calcified rim
Extent Diffuse crossing the suture lines
Localized over the bone
Resolution Few days 2 wk-3 months
Associated with Ecchymotic skin patches Anemia and jaundice if large
Management Nothing Management of anemia and hyperbilirubinemia

3. Erythema, abrasions, and ecchymoses of the skin.

4. Subconjunctival hemorrhage and petechiae of the skin of the head and neck:
They are common secondary to increased intrathoracic pressure
during delivery of the chest

5. Fractures of the skull:
They may occur due to pressure from forceps or from maternal symphysis pubis, sacral promontory, or ischial
spines.

Intracranial Hemorrhages (ICH)
Incidence: ICH often involves the ventricles (intraventricular hemorrhage, IVH). The incidence of IVH increases with decreasing birthweight and gestational age: 60-70% of 500-750 gm infants and 10-20% of 1,000-1,500 gm infants.
Sites: Bleeding within the skull can occur:1. Extra cerebrally: Epidural, subdural, or
subarachnoid spaces.2. Into the parenchyma of the cerebrum or
cerebellum.3. Into the ventricles from subependymal germinal
matrix.

Etiological factors
1. Trauma: It occurs especially in precipitate labor, prolonged or difficult labor, breech delivery, forceps or ventouse delivery, increased manipulation of the newborn, and when the fetal head is large in proportion to the size of pelvic outlet.
2. Hypoxic-ischemic injury to germinal matrix or its vessels.
3. Congenital vascular anomalies.4. Primary hemorrhagic disturbance:
Thrombocytopenia, DIC, or hemophilia of the newborn.

Clinical manifestations
Onset: Usually within the first 3 days of life and 10-15% after the 1st wk of life.
1. Signs of blood loss: Pallor, shock, unconjugated hyperbilirubinemia, and respiratory distress.
2. Manifestations of increased intracranial pressure: Bulging and tense anterior fontanel and increasing head circumference, weakness, hypotonia, seizures, lethargy, irritability, failure to suck well, high-pitched cry, muscular twitching, and temperature instability.
3. Manifestations of intracerebral hemorrhage (if present)
A. Focal neurologic signs: Focal seizures or hemiparesis.B. Coma.

Diagnosis
1. History.
2. Clinical manifestations.
3. Laboratory data A. A significant fall in hematocrite without
evidence of hemolysis should suggest either ICH or subcapsular hemorrhage of the liver.
B. Unconjugated hyperbilirubinemia without evidence of hemolysis.
C. Thrombocytopenia and prolonged PT and PTT in DIC.

Diagnosis
4. Cerebral ultrasonography (the method of choice in diagnosis)
A. Routine: It is done for preterm babies less than 1,500 gm weight or gestational age <30 wk, within the 1st 7-14 days of life, and again at 36-40 wk postmenstrual age.
B. Otherwise with clinical manifestations.
5. CT scan or MRI: The stress associated with transport is a relative contraindication to the test.

Prognosis
1. Post-hemorrhagic hydrocephalus: Both communicating (reduced CSF absorption by arachnoid villi) and obstructive (reduced CSF outflow through 4th ventricle).
2. Parenchymal injury: Motor impairments, educational difficulties, or cerebral palsy.
3. Death: Patients with massive hemorrhage.

Prevention
1. Judicious management of cephalopelvic disproportion and operative (forceps or cesarean section) delivery.
2. Avoid unnecessary manipulations of the newborns, especially the preterm.
3. Maternal ITP: Antenatal treatment of the mother by steroids and cesarean section.

Treatment
1. Avoid excessive suctioning and manipulation.
2. Incubator care: Close observation, O2 for cyanosis, and good temperature control.
3. Slow administration of fresh whole blood in cases of anemia or shock.
4. Vitamin K administration.
5. Anticonvulsant drugs for seizures.
6. Management of hyperbilirubinemia.

Treatment
7. Management of DIC.
8. Repeat lumbar punctures for relieving increased intracranial pressure in case of post-hemorrhagic hydrocephalus.
9. Neurosurgical consultation. .

Peripheral Nerve Injuries
1. Brachial plexus injury
It occurs when lateral traction is exerted on the head and neck during delivery of the shoulders in a vertex presentation, or when the arms are extended over the head in a breech presentation.

Peripheral Nerve Injuries
Erb’s paralysis Site of injury: C5 and C6 nerves. Muscles affected: Deltoid, supraspinatus,
infraspinatus, supinator, brachioradialis, and biceps muscles. Weakness leads to loss of the power to abduct the arm from the shoulder, to rotate the arm externally, and to supinate the forearm.
The characteristic position: Adduction and internal rotation of the arm and pronation of the forearm.

Erb's Palsy

Motor manifestations
A. Weakness, hypotonia, and hyporeflexia of the affected muscles.
B. Moro reflex is absent on the affected side.
C. The hand grasp is preserved (favorable prognostic sign) unless C7, C8, and T1 nerves are also injured.
D. Diaphragmatic palsy occurs if C4 is also injured (fluroscopy can detect it).

Motor manifestations
Sensory manifestations: Loss of sensation over the outer aspect of the arm.
Prognosis: It depends on the nature of injury.
1. Transient: It occurs in cases of edema or hemorrhage within the nerve sheath.
2. Permanent: It occurs in case of laceration of nerve fibers.

Motor manifestations
Treatment
1. Positioning and partial immobilization
90o adduction and external rotation of the arm,
with full supination of the forearm.
2. Physiotherapy: Gentle massage and range
motion exercises are started on the 2nd wk.
3. Surgical (neuroplasty and tendon transfers): It is indicated if no improvement.

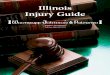
2. Facial nerve palsy
It occurs as a result of pressure on the 7th nerve in utero, during labor, or from forceps.
It is manifested as LMNL with complete paralysis of the same side of the face.
The prognosis of the peripheral injury: Improvement when edema or hemorrhage is present within the nerve fibers. Neuroplasty is indicated if the nerve fibers are torn.
Care of the exposed eye is essential (artificial tears drops).

Facial Nerve Palsy of the Newborn

Injury of the Visceral Organs
1. Liver
The Predisposing factors: Large infant's size, asphyxia, and hepatomegaly.
Etiology A. Pressure on the liver during head delivery in
breech presentation.
B. Incorrect cardiac massage.
Pathology: Rupture of the liver with formation of large subcapsular hematoma.

Injury of the Visceral Organs
Clinical manifestationsA. The infant usually appears normal for the first 1-
3 days.
B. Manifestations of blood loss: Pallor, jaundice, tachycardia, tachypnea, poor feeding and lethargy. Shock and death occur if the hematoma breaks through the capsule into peritoneal cavity.
C. A mass may be palpable in the right upper quadrant of abdomen.

Injury of the Visceral Organs
Diagnosis: Clinical manifestations and ultrasonography.
TreatmentA. Blood transfusion in marked anemia
and/or shock.
B. Exchange transfusion in marked jaundice.
C. Surgical repair may be required.

Injury of the Visceral Organs
2. Spleen
A. Injury may occur alone or in association with liver injury.
B. Causes, clinical manifestations, and treatment are similar to those of liver injury.

Injury of the Visceral Organs
3. Adrenal gland
Causes: Usually after breech delivery, trauma, anoxia, overwhelming infections.
Clinical manifestationsA. Profound shock and cyanosis (acute adrenal
failure).B. Jaundice and pallor.C. A mass may be palpable in the flank.D. Calcified adrenal hematoma may be discovered
accidentally on X-ray.Diagnosis: Abdominal ultrasonography.
Treatment of acute adrenal failure.

Injury of Sternocleidomastoid Muscle (SCM)
Etiology: Bleeding occurs within the muscle tissue as the result of muscle or fascia disruption during delivery.
Pathology: Hematoma formation appears few hours after delivery. Later on, fibrosis leads to shortening of the muscle and torticollis.
Diagnosis: A palpable mass in SCM muscle.
Treatment: Physiotherapy. Recovery usually occurs after 3-4 mo.

Fractures
Any bone may be fractured and any joint may be dislocated in cases of difficult delivery.
Fracture clavicle is more frequently occurring than any other bone as a result of difficult delivery of shoulders in vertex or breech presentations.
The infant doesn’t move the arm with absent Moro reflex on the same side and crepitus and bony irregularity may be palpated.
Immobilization of the limb on the same side is indicated.
The prognosis is excellent.

Perinatal Asphyxia, Hypoxic-Ischemic Encephalopathy (HIE)
Definitions Anoxia: The consequences of a complete lack of
oxygen. Hypoxia: An arterial concentration of oxygen is
less than normal. Ischemia: Blood flow to cells or organs is
insufficient to maintain their normal function. Perinatal asphyxia is an insult to the fetus or
newborn due to lack of oxygen (hypoxia) and/or lack of perfusion (ischemia) to various organs.
Hypoxic-ischemic encephalopathy is the primary cause of permanent damage to CNS cells which may result in death or which may manifest later as cerebral palsy or mental retardation.

Etiology
I. Fetal hypoxia (placental insufficiency) (90% of causes)
1. Maternal hypoventilation (leading to reduced PaO2 of maternal blood). It may occur during anesthesia, cyanotic heart disease, or respiratory failure of the mother.
2. Maternal hypotension: Spinal anesthesia, compression of vena cava and aorta by gravid uterus, or dehydration.
3. Uterine causes: Uterine tetany due to excessive oxytocin dose, leading to reduced placental filling, or uterine vessel vasoconstriction by cocaine.
4. Umbilical cord: Compression or knotting.5. Placental: a. Premature separation. b. Placental insufficiency (toxemia).

Etiology
II. Neonatal hypoxia (10% of causes).
1. Severe anemia: Hemolysis or hemorrhage.
2. Shock: Adrenal or intracranial hemorrhage, overwhelming infection, or massive blood loss.
3. CNS depression: Narcosis, injury, or anomalies.
4. Pulmonary: Respiratory distress syndrome and others.
5. Congenital cyanotic heart diseases.

Pathology
1. Cortical necrosis or infarcts (focal or multifocal): Neuronal death resulting in cystic encephalomalacia (gray mater injury) that produce focal seizures and hemiplegia. Infarcts are best visualized with CT scanning or MRI.
2. Periventricular leukomalacia (PVL): Periventricular white mater injury. Cerebral edema can be detected by cranial ultrasonography.

Clinical manifestations of HIE
1. The presence of yellow meconium-stained amniotic fluid is evidence that fetal distress has occurred.
2. The neurological manifestations: The infants are frequently depressed and fail to breathe spontaneously. Pallor, cyanosis, apnea, a slow heart rate, seizures, and unresponsiveness to stimulation are common.
3. The clinical manifestations of other organs affected by perinatal asphyxia

Multi-organ Affection due to Asphyxia
System Effect
Cardiovascular
Pulmonary
Renal
Adrenal
Gastrointestinal
Metabolic
Skin
Hematology
Myocardial ischemia, poor contractility, tricuspid insufficiency, hypotension
Pulmonary hypertension, pulmonary hemorrhage, respiratory distress syndrome
Acute tubular or cortical necrosis (acute renal failure)
Adrenal hemorrhage
Perforation, ulceration with hemorrhage, necrosis
Hypoglycemia, hypocalcemia
Subcutaneous fat necrosis
Disseminated intravascular coagulopathy

Prevention
Prevention of fetal hypoxia by monitoring the fetal conditions and maternal O2 supply.
Management
Perinatal management
1. Monitoring of fetal well being during pregnancy and labor.
2. Resuscitation in the delivery room.
3. Treatment of meconium aspiration.

Postnatal management of asphyxia
I. Investigations 1. EEG: It is indicated to detect seizure foci.
2. Ultrasonic examination: It can be done early to detect associated hemorrhage and extent of edema.
3. CT scan: Early (2-4 days) to detect the extent of edema.
Late (2-4 wk) to detect the extent of cerebral injury.

Postnatal management of asphyxia
II. Treatment
1. O2 level: Hypoxia should be treated with O2
supply and/or assisted ventilation.
2. Perfusion: Dobutamine (inotropic drug) can be used to help perfusion.
3. Glucose level: Keep it at 75-100 mg/ dL. Hypoglycemia may lead to convulsion.
4. Temperature and calcium level should be kept in a normal range.

Postnatal management of asphyxia
II. Treatment 5. Seizures: They should be controlled by
anticonvulsant drugs as seizures may lead to energy failure and intracranial hemorrhage due to increased blood pressure.
6. Cerebral edema: Avoid fluid overload by reducing the fluid intake to volume that equals insensible water loss and urine output = about 60 mL/ kg/ day.

Postnatal management of asphyxia
II. Treatment 7. Management of the cardiac effects of asphyxia:
Adequate ventilation with correction of hypoxemia, acidosis, and hypoglycemia. Volume overload must be avoided. Dopamine and/or dobutamine are used in case of cardiac collapse.
8. Management of the renal effects of asphyxia: Monitoring of urine output, urinalysis, urine specific gravity, and urine and serum osmolarity and electrolytes. Measurement of the renal failure index to help confirm the renal failure. Dopamine infusion at 1.25-2.5 g per kg per hour IV may aid renal perfusion.

Postnatal management of asphyxia
II. Treatment
9. Management of the gastrointestinal effects of asphyxia: We usually do not feed severely asphyxiated infants for 5-7 days after the insult or until good bowel sounds are heard and stools are negative for blood (necrotizing enterocolitis).
10. Management of the hematological effects of asphyxia: Management of DIC.
11. Management of the pulmonary effects of asphyxia: Oxygenation and ventilation

THANK YOUTHANK YOU