-
7/28/2019 6.17.09 Moll Heme Board Review
1/34
Board Review
6/17/2009
-
7/28/2019 6.17.09 Moll Heme Board Review
2/34
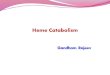
CLOTTINGTESTS
Fibrinogen
VII
TFXII
X
Fibrin
PLPL
PLV
II
VIII
IX
-
7/28/2019 6.17.09 Moll Heme Board Review
3/34
MKSAP-Q1
80 yr man
3 week h/o massive bruising
on no meds; FH negative
Labs: platelets 350,000
PT 12 sec; aPTT 78 sec; Bleeding time: 6 min
fibrinogen 390 g/dL; D-dimer: 1000 ng/mL
aPTT 1:1 mix: 71 sec
LFTs normal
Q: Dx?
acquired F VIII inhibitor
DIC
LA
Factor XII deficiency
chronic liver disease
acquired F VIII inhibitor
DIC
LA
Factor XII deficiency
chronic liver disease
-
7/28/2019 6.17.09 Moll Heme Board Review
4/34
Coag testsMKSAP-Q2
32 yr man; hematemesis x 2 h
Strict vegetarian diet x 4 weeks for weight control and
abstained from alcohol for same period of time
PE: pale, spleen 3 cm enlarged; liver not palpable
Hbg 8.0; MCV 85; WBC 10; plts 75,000
PT 28 sec; aPTT 50 sec; BT 7.5 min; fibrinogen 165 mg/dL
Albumin 2.0; ASAT 75; ALAT 45
PT 1:1 mix: 12 sec; aPTT 1:1 mix: 30 sec
Q: Dx?
A: chronic liver disease
(vitamin K deficiency; DIC; acquired f V inhibitor)
-
7/28/2019 6.17.09 Moll Heme Board Review
5/34
-
7/28/2019 6.17.09 Moll Heme Board Review
6/34
Heparin induced thrombocytopenia
HIT (HIT-1, HIT-2, HAT)
Platelet of> 50 % from baselineafter 5 days of heparin
(earlier if heparin given within last 3 months)
PLUS PT and aPTT normal
Lab demonstration of heparin-dependent antibodies
- HIT ELISA (PF4) or
- HIPA test (heparin induced platelet aggregation test)
Thromboses (arterial and venous)
-
7/28/2019 6.17.09 Moll Heme Board Review
7/34
LMWH and HIT
HIT incidence: 2.7 % standard heparin vs. < 1 % LMWH
but: 90-95 %cross-reactivity!
-
7/28/2019 6.17.09 Moll Heme Board Review
8/34
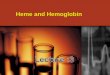
HIT
[ASH 2001, O
clot
X
XII VII
thrombin
Arixtra = Fondaparinux
-
7/28/2019 6.17.09 Moll Heme Board Review
9/34
BleedingMKSAP-Q4
55 yr woman Planned cholecystectomy
Hx: easy bruising, frequent prolonged nosebleeds
Bleeding after nasal surgery
Blood count normal
PT normal; aPTT 64 sec; aPTT 1:1 mix: complete correction
XII 110 %; XI 16%; IX 98 %; VIII 112 %
Q: How will you treat?
A: FFP (Cryo; PCC; Amicar; nothing)
-
7/28/2019 6.17.09 Moll Heme Board Review
10/34
Factor concentrates
PCCs: II, VII, IX, X
Bebulin, FEIBA, Autoplex,
Cryo: fibrinogen, von Willebrand factor (factor VIII) FFP: all
other factors (little fibrinogen and von Willebrand factor)
half-life of factor VII: 4 h
Humate P: von Willebrand factor, factor VIII
-
7/28/2019 6.17.09 Moll Heme Board Review
11/34
BleedingMKSAP-Q5
30 yr man
Lifelong epistaxis + easy bruising
Tooth extractionbleeding for several days
Adopted
Hbg 13.0; MCV 78; plts. 250,000
BT 13.5 min; PT 12 sec; aPTT 40 sec; TCT normal
Platelet aggregation study normal
Q: Dx?
A: von Willebrands disease
(Glanzmann, mild hemophilia A or B, dysfibrinogenemia)
-
7/28/2019 6.17.09 Moll Heme Board Review
12/34
von Willebands disease
Prevalence: 1 % of population
Bruisingmucosal (nose, gums, menstrual, tonsillectomy, tooth
extraction)
Dx: von Willebrand factor activity factor VIII bleeding time,
PFA100von Willebrand factor multimers
type 1: quantitative. 90 % of cases (all multimers present, but
decreased)
type 2: qualitative (missing large multimers). 2A, 2B, 2N,
platelet type
type 3: severe 1 (all multimers missing)
Rx: type 1: DDAVP (0.3 g/kg) i.v., s.c., or intranasaltype 2:
Humate P (= factor VIII concentrate with vWf)
Cryo
-
7/28/2019 6.17.09 Moll Heme Board Review
13/34
MKSAP-Q6
A 86 B 87 E 88C 89 D 90
-
7/28/2019 6.17.09 Moll Heme Board Review
14/34
MKSAP-Q7
27 yr woman
SLE
2 DVTs, now 3rd
PT 13.6 sec; aPTT 43 sec; LA
Standard heparin 5000 U bolus, then 1200 U/h. F/u aPTT 120
sec
Q: How to best give and monitor heparin rx?
heparin
Use anti-Xa level, not aPTT LMWH and follow aPTT
IVC filter
heparin
Use anti-Xa level, not aPTT
LMWH and follow aPTT
IVC filter
-
7/28/2019 6.17.09 Moll Heme Board Review
15/34
Antiphospholipid antibodies
APL
A
ACALA
I) antibody test (ELISA)
anticardiolipin
anti-2-glycoprotein I
II) functional test lupus anticoagulant (inhibitor
2-GP I
-
7/28/2019 6.17.09 Moll Heme Board Review
16/34
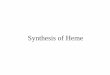
Lupus anticoagulant
1) Screening test (aPTT, dRVVT, KCT, Silica clot
time)prolonged
2) Normal plasma mixing studydoes not correct
3) Confirm (mix with excess of phospholipids)corrects
- hexagonal phospholipid test
- platelet neutralization procedure (PNP)
Fibrinogen
VIITF
XII
X
Fibrin
PPLPL
PLDRVVT
aPTT
-
7/28/2019 6.17.09 Moll Heme Board Review
17/34
MKSAP-Q8
20 yr woman, bleeds after dental extraction
SLEsteroids. No h/o bleeding; plts 160,000;
PT 17.5 sec; corrects with 1:1 mix to 11.4 sec
aPTT 43.3 sec; does not correct with 1:1 mix
Fibrin (ogen) degradation products normal
Q: Cause of the prolonged prothrombin time?
DIC
Congenital XII deficiency
F VIII inhibitor
LA-hypoprothrombinemia syndrome
Vitamin K deficiency
DIC
Congenital XII deficiency
F VIII inhibitor
LA-hypoprothrombinemia syndrome
Vitamin K deficiency
-
7/28/2019 6.17.09 Moll Heme Board Review
18/34
APLA syndrome
1) thrombosis or
2) recurrent abortions
3) pos. APLA test (repeat)
(+ thrombopenia, derm. or neurol. symptoms)
Patient bleeds:
Hypoprothrombinemia
Low platelets
-
7/28/2019 6.17.09 Moll Heme Board Review
19/34
MKSAP-Q9
Homocysteine
Factor V Leiden
Prothrombin 20210 mutation
Antiphospholipid antibodies
Q: Which thrombophilia test is most likely going to be
abnormal?
33 yr man with CP Coro: extensive 3 vessel disease
Non-smoker, normotensive, lipids including
lipoprotein(a) normal
Strong FH of premature CAD and stroke
Homocysteine
Factor V Leiden
Prothrombin 20210 mutation
Antiphospholipid antibodies
-
7/28/2019 6.17.09 Moll Heme Board Review
20/34
-
7/28/2019 6.17.09 Moll Heme Board Review
21/34
venous arterial
Protein S deficiency yes yes
protein C def. yes yes
AT III def. yes yes
factor V Leiden yes no
prothrombin 20210 yes no
homocysteinemia yes yes
MTHFR polymorphism no no
antiphospholipid antibodies yes yes
Thrombophilia
-
7/28/2019 6.17.09 Moll Heme Board Review
22/34
Factor V Leiden
prevalence : 2 - 15 % (western world)
RR for 1st DVT/PE: heterozygotes: 3 - 8
homozygotes: 80
heterozygotes + pill: 30-50
Diagnosis: coagulation test (APC resistance) or genetic test
Not associated with arterial clots (except for selected
patients)
-
7/28/2019 6.17.09 Moll Heme Board Review
23/34
Prothrombin 20210 polymorphism
prevalence: 2.3 % (normal population)
mild risk factor for 1st DVT/PE: RR 2.8
risk for recurrence of DVT/PE: not increased
associated with elevated prothrombin levels
not associated with arterial thrombosis
-
7/28/2019 6.17.09 Moll Heme Board Review
24/34
www.fvleiden.org
-
7/28/2019 6.17.09 Moll Heme Board Review
25/34
MKSAP-Q11
47 year-old man
DVT after 1 h airplane flight
FH: uncle with DVT after hip arthroplasty,
grandfather stroke age 68
Thrombophilia w/u negative
Q: How long to anticoagulate?
A: 3 months (INR 2.03.0)
-
7/28/2019 6.17.09 Moll Heme Board Review
26/34
DVT/PE: Anticoagulationhow long?
1. after transient risk factors short (6 weeks - 3 mo)
2. Idiopathic DVT/PE: at least 3 months
- Factor V Leiden, hetero at least 3 months
- Prothrombin 20210 mutation: at least 3 months
- Protein C or protein S deficiency ???
- ATIII deficiency: indefinite
- homozygote factor V Leiden: indefinite
- Factor V Leiden + prothrombin 20210 mutation: indefinite
- APLA syndrome: indefinite- Tumor indefinite (LMWH)
3. Recurrent DVT/PE indefinite
-
7/28/2019 6.17.09 Moll Heme Board Review
27/34
MKSAP-Q12
56 yr healthy man
DVT calf and popliteal vein
Adamantly refuses hospitalization
Q: Rx options?
A: LMWH s.c. in therapeutic doses + warfarin 5-10 mg qd
(ASA, prophylactic LMWH, daily LMWH monitoring,
15 mg warfarin)
-
7/28/2019 6.17.09 Moll Heme Board Review
28/34
MKSAP-Q13
75 yr man
Calf and popliteal DVT after 10 h car ride
Smoking. Otherwise healthy
Phys. exam nl.
CBC, PT, PTT, routine serum chemistry nl
Q: What should be included in evaluation?
1. Thorough PE and p.a. and lat. CXR
2. Thorough PE, p.a. and lat. CXR, and chest/abdo MRI
3. Thorough PE and p.a. and lat. CXR plus EGD/colonoscop
4. Thorough PE and CEA
1. Thorough PE and p.a. and lat. CXR
2. Thorough PE, p.a. and lat. CXR, and chest/abdo MRI
3. Thorough PE and p.a. and lat. CXR plus EGD/colonoscop
4. Thorough PE and CEA
-
7/28/2019 6.17.09 Moll Heme Board Review
29/34
MKSAP-Q14
28 yr woman
ACA
three 1st trimester pregnancy losses
Now 6 weeks pregnant
Q: What is the most appropriate treatment?
-
7/28/2019 6.17.09 Moll Heme Board Review
30/34
MKSAP-Q14
28 yr woman
ACA
three 1st trimester pregnancy losses
Now 6 weeks pregnant
Q: What is the most appropriate treatment?
Careful observation only
Prednisone 40 mg qd
Aspirin IvIg infusions
Heparin and ASA
Careful observation only
Prednisone 40 mg qd
Aspirin IvIg infusions
Heparin and ASA
-
7/28/2019 6.17.09 Moll Heme Board Review
31/34
MKSAP-Q15
35 yr woman
epistaxis and bruising
Plt: 5,000
Refractory ITP (fails steroids)
Q: What therapy is best for long-term response?
A: splenectomy(?Rituxan = Rituximab?)
-
7/28/2019 6.17.09 Moll Heme Board Review
32/34
ITP
1:20,000
Antibodies against platelets, often against GPIIb/IIIa
Dx: negative history, r/o all other causes:
- iron studies (deficiency?)
- vitamin B12, folate- blood smear (clumping?)
- TSH (hypo?)
- HIV
(- ANA)
- PT, PTT
- bone marrow aspirate and biopsy: controversial
-
7/28/2019 6.17.09 Moll Heme Board Review
33/34
ITP - Therapy
Guided by patients bleeding symptoms
Treat when platelets < approx. 2050,000 or when bleeding
Prednisone 1 mg/kg
Slow taper when platelet count > 50,000
Iv Ig 1 g/kg q d x 2 d
Anti-D antibody (WinRho) single dose. Response in 2-3 d.
Duration of
response: 1 month
Relapse: splenectomy. Good response in 60-70%. Rituximab.
If splenectomy fails: cyclophosphamide, azathioprine, danazol,
multi-
agent chemotherapy
-
7/28/2019 6.17.09 Moll Heme Board Review
34/34
Questions?
Comments?