Embed Size (px)
Citation preview

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 1/25
0
A
TERM WORK REPORT
on
RP in Medicine: Application of Rapid Prototyping in Medical models
Submitted by
AMANPREET SINGH (801382002)
Submitted to
Dr. Anant Kumar Singh
Assistant Professor
MECHANICAL ENGINEERING DEPARTMENT
THAPAR UNIVERSTY, PATIALA
April, 2014

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 2/25
1
Acknowledgment
Any sustained effort by untrained minds in a new work environment requires for culmination,
a guiding hand that shows the way. It gives me immense pleasure to be able to present this
Term Work Report in the present form for which I would like to express my sincere and
devoted gratitude to the Assistant Professor, Dr. Anant Kumar Singh, for his continuous
encouragement, support, and guidance throughout this Term Work and has always stood for
any problem, difficult situation whatsoever.
I am also thankful to faculty of Department of Mechanical Engineering for their
invaluable advice, suggestions and encouragement. Under their able leadership and guidance,
I was able to meet the goals of the project in time.
I would like to express my heartfelt appreciation to my loving parents; I am unable to
find words to embed my deep sense of gratitude for them. In the end I am indebted to my
colleagues, who encourage me.
Knowledge is power and unity is strength.
Amanpreet Singh
801382002
ME Production

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 3/25
2
Contents
Acknowledgment 1
Introduction 3
Rapid Prototyping techniques 3
Materials 4
RP model fabrication 5
Literature Review 7
Subburaj et al., 2007 ( Customize prosthesis implant) 7
Mahaisavariya et al., 2006 (Preoperative planning) 8
Ciocca et al., 2009; Sachlos and Czernuszka, 2003 (Tissue engineering) 9
Gopakumar 2000 (Cranial reconstructive surgery) 10
New Contribution 12
Surgical planning 12
Medical education and training 12
Design and development of medical devices and instrumentation 13
Customized implant design 13
Scaffoldings and tissue engineering 13
Prosthetics and orthotics 14
Mechanical bone replicas 14
Forensics 14
Anthropology 15
Results and Discussion 16
Conclusion 18
References 19

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 4/25
3
Introduction
Rapid Prototyping (RP), a layer-by-layer material deposition technique, started during the
early 1980s, has significantly improved the ability to fabricate physical models with precise
geometries using computer aided designs or data from medical imaging technologies .RP is
beneficial in the field of medicine as this technology has the ability to fabricate complex
shaped anatomical parts directly from scanned data such as computerized tomography (CT)
images. These models provide a better illustration of the human anatomy, use for precise pre-
surgical planning, assistance in the intensive planning of surgical procedures and also help
the surgeons, medical students to rehearse different surgical procedures realistically (Kai et
al ., 1998; Liu et al ., 2006,). RP models can also be used for designing customized implants,
prosthesis, and function as a communication tool between surgeons and patients (Dhakshyani
et al ., 2011).
Rapid prototyping process can be divided into two phases: virtual (modelling and simulating)
and physical (model fabrication) (Rosa et al ., 2004). Before the fabrication of physical
models, firstly comes the virtual phase in which computer aided design (CAD) is prepared by
using medical imaging technology such as CT, magnetic resonance imaging (MRI) and laser
digitizing The fabrication of the physical model is the second phase, a process in which
suitable RP system uses CAD data to develop the physical model. Now a day’s variety of
materials (instead of normal RP material) and some medical grade materials are available,
which can be used to fabricate RP models on the basis of their use in different medical
applications.
Rapid Prototyping techni ques
There are currently a number of RP techniques in the market, based on special sintering,
layering or deposition methods. Each technique has its own limitations and applications in
constructing prototype models. Established RP techniques which are commercially available
are summarized in Table1 and precisely discussed below.

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 5/25
4
Table 1 Features of commercial available RP techniques (Pham and Gault, 1998; Mousah,
2011)
Materials
In case of medical applications, the RP models can be fabricated with a variety of materials
and the selection of material depends on the purpose of fabrication. However, some medical
applications (surgical tools or medical implants) require models which have the ability to be
sterilized or remain compatible with human tissue like biomaterials. A biomaterial can be
classified as any material used to manufacture devices that replace a part or a function of the
body in a safe and reliable way. Metallic biomaterials are mainly used in areas of high static
or cyclic stress and well suited for medical implants such as cranial plates and ace tabular
implants. Ceramic materials are typically solid inert compounds and are used where
resistance to wear is of primary importance such as dental implants, crowns, whereas medical
grade polymers are used in various medical applications where stability, flexibility and
controlled porosity are demanded such as tissue repair, drug delivery devices, and medical
implants (Brennan, 2010). Some of categorized biomaterials for medical use are shown in
Table 2
Table 2 Categorized biomaterials for medical applications (Brennan, 2010; Mour, 2010; Vail
et al ., 1999)

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 6/25
5
RP model fabrication
RP machine needs CAD information to fabricate a physical model so for that purpose RP
process can be divided into two phases: virtual and physical. As mentioned earlier firstly
comes the virtual phase, which consists of using imaging processing tools
(1) Data Acquisition
(2) Image Processing
(3) Model Fabrication
Data acquisit ion
Data acquisition is a process of capturing the three dimensional (3D) shape of an existing part
by using contact and non contact measuring devices, only non contact methods (medical
imaging technologies) are considered here. Medical imaging technologies are generally used
to visualize the configurations of bones, organs and tissues, but they also have the ability to
export scanned image data and additional information in commonly known medical file
format, such as DICOM (Digital Imaging and Communications in Medicine) (Berce et al .,
2005; Rengier et al ., 2010) and finally make possible to convert scanned image data fromDICOM to STL file format, which is universally accepted RP file format (Milovanovic and
Trajanovic, 2007). Most commonly, CT, MRI and Laser digitizing techniques are used for
this purpose; others are cone beam tomography, X ray, ultrasound etc. (Abbott et al ., 1998;
Chang et al ., 1991; Lambrecht et al ., 2009; Liu et al ., 2006; Meakin et al ., 2004; Schievano
et al ., 2010). It provides important scanned data of anatomical structure for diagnostic
reasons and same data can be used to obtain geometrical information of the body structures
for three-dimensional modeling.
Image processing
Images of the body are taken in thin cross sectional “slices” which can then be layered by
using commercial available software like MIMICS, 3D Doctor and Voxim to create a 3D
model of anatomical parts. These software systems performs the necessary segmentation of
the anatomy through sophisticated 3D selection and editing tools and provides the interface
between scanned data of CT, MRI or technical scanners and RP systems (Noorani, 2006).
These software systems allow, modifying the images by defining various tissue densities for

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 7/25
6
display, to select the regions of interest from the general information available from the
scanner. It enables the surgeons and radiologists to control and select the correct
segmentation of CT or MRI scan images. After completing the segmentation and
visualization the data is converted to a standard tessellation language (STL) format. This
format is compatible with most commonly used rapid prototyping machines (Gibson et al .,
2004; Liu et al ., 2006; Tukuru et al ., 2008).
Model fabri cation
This step includes choosing the right rapid prototyping technique according to the demand of
medical application. As we know every RP system has its strength and weaknesses so a
suitable RP system or technique needs to be chosen to fulfil various requirements of a
medical application like accuracy, surface finish, cost, visual appearance of internal
structures, number of desired colours in the model, strength, materials availability,
mechanical properties, etc. Then finally 3D virtual model in STL file format is transferred to
the RP system and building starts. After the fabrication of model, it needs to be evaluated and
validated by the team and in particular surgeon so as to ensure that it is accurate and serves
the purpose. Furthermore, depending on the use of the model, it can be sterilised for
assistance in an operating theatre (Petzold et al ., 1999).

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 8/25
7
Literature Review
Subburaj et al ., 2007 (Custom ize prosth esis implant)
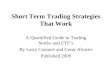
Researchers (Subburaj et al ., 2007) in the Department of Mechanical Engineering (IIT,
Mumbai) and Department of Prosthodontics (Government Dental College and Hospital,
Mumbai) considered a patient (male, 19 years) with congenital absence of the right ear for
investigation as presented in Figure 1. The purpose was to use CAD and RP technologies for
the rapid development of auricular prosthesis, and demonstrated a real life case study. The
anatomic morphology of the prosthesis, matching the morphology of the contralateral ear,
was obtained by following these five steps:
(i) tomography images of deficient and contralateral ears with the help of finer CT scanning(0.63 mm slice thickness),
(ii) econstruction of the corresponding 3D models in which the correct geometry and position
of the prosthesis were ensured by stacking the CT scan images of the contralateral normal ear
in reverse order, and joining them using medical modeling software, MIMICS (Materialise,
Belgium)
(iii) design of the final model of missing ear (prosthesis) was obtained by subtracting the
CAD model of the remnant portion of the defective ear from the CAD model of the mirrored
contralateral ear using a haptic CAD system (FreeForm, SensAble Technologies, USA),
(iv) fabrication of prosthesis master using a suitable RP system (FDM), the dimensions of
fabricated model was measured as per the standards (standard auricular morphological
measurement) and compared with the original CAD model to determine the accuracy
(dimensional error)
Figure 1 A patient (male, 19 years) with congenital absence of the right ear (Subburaj et al .,
2007)then finally,

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 9/25
8
(v) the fabrication of the final prosthesis using a mould made from the master (FDM model)
in which medical grade silicone rubber of the appropriate color was packed into the mould to
fabricate the final ear prosthesis. The final fabricated prosthesis was also measured as per
standards, and percentage difference was calculated with respect to the CAD model and then
successfully fitted to the deficient side of the patient using medical grade adhesive. The
prosthesis may change its color or deteriorate over time, and may require replacement in
future. This can be facilitated by the availability of the digital model of the prosthesis. The
postoperative appearance showed the excellent result in terms of aesthetics.
Mahaisavariya et al ., 2006 (Preoperative planning)
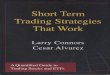
Report of two cases (female patients of age 23 and 18 years with cubitus deformity) as shown
in Figure 2 are presented by a group of researchers (Mahaisavariya et al ., 2006) in which they
reported some work on surgical planning of corrective osteotomy for cubitus varus using RP
models. First of all a CT scan was performed on both the deformed and normal elbow using a
Philip spiral CT scanner (Thomoscan, AV), CT scan acquisition was performed with 2mm
slice thickness and reconstruction was performed with 1 mm slice thickness then this scanned
data was used to construct a 3D CAD model using medical imaging and digital CAD
software ( MIMICS and Magics RP, Materialise, N.V. Belgium) and surgical planning of
corrective osteotomy was virtually planned and simulated in the 3D CAD model. The proper
location of osteotomy, the amount of wedging bone and the tilting of the plane for osteotomy
cut was measured by performing 3D evaluation of the deformed and mirrored normal
humerus on screen. After calculating and determining the optimal configuration, the data of
deformed and normal humerus was used to fabricate
Figure 2 A patient (female, 18 years) with cubitus varus of left elbow (Mahaisavariya et al .,
2006)
RP models using 3D printing machine (Z Corp Inc.). These RP models were used by
surgeons to rehearse the osteotomy before a real surgery. Both patients were successfully

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 10/25
9
operated as surgical planning and shown excellent post operative results in terms of cosmetic
and functional result. This case study clearly shows that RP and associated technology (CT)
can facilitate surgeons in preoperative planning for certain complex cases like planning of
osteotomy of complex deformity of hip, pelvis and spine, also allows the surgeons to choose
proper configuration and most appropriate location of osteotomy according to individual
patient need.
Ciocca et al ., 2009; Sachlos and Czernuszka, 2003 (Tissue engineering)
RP has been used as an alternative to conventional scaffold fabrication methods within the
tissue engineering field. Tissue engineering is process of growing the relevant cell(s) in vitro
into required 3D organ or tissue (Ciocca et al ., 2009; Sachlos and Czernuszka, 2003). This
method has been used for the pair of damaged tissue and organs. The main element for cell
structure is scaffold, a prefabricated porous structure which is seeded with cells or nutritants
and provides necessary support and shape to growing tissue (Armillotta and Pelzer, 2008).
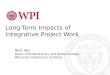
Researchers (Williams et al ., 2005) at the University of Michigan have explored the potential
of SLS (a RP technique) to fabricate polycaprolactone (PCL) scaffolds as presented in Figure
3. Polycaprolactone (PCL) is bioresorbable polymer which has sufficient mechanical
properties for bone tissue engineering applications. Furthermore, researchers evaluated the
biological properties of these SLS manufactured scaffolds by seeding with bone
morphogenetic protein -7 (BMP-7) transduced human fibroblasts and evaluated the growth of
generated tissue. They found that SLS fabricated scaffolds matched the design well, had
mechanical strength within the range of trabecular bone and supported the growth of tissue. It
is concluded that PCL scaffolds fabricated by SLS have great potential for the replacement of
skelton tissue in the field of tissue engineering.
Figure 3 (a) STL design file for the porous scaffold. (b) PCL scaffold fabricated by SLS
(Williams et al .2005)

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 11/25
10
Gopakumar 2000 (Cranial reconstructive surgery)
A patient was selected for the case study with a cranial injury, sustained during an accident,
on the frontal region of the skull cage. The injured area measured 100mm in length and
around 80mm in width approximately. CT scans were performed on the patient using a spiral
CT scanner. Slice images were taken at a 2mm inter-slice distance. Traditionally in CT
scanning, an X-ray tube and a detector array travel on a circular path around the patient
collecting a complete set of data over 3608; thereafter, the respective image is reconstructed
and the patient is shifted a small distance through the gantry for the next transverse section to
be measured. This procedure is repeated slice by slice. In spiral CT, the data from the
scanned area of the patient are acquired as the patient is moved continuously through the
gantry while the X-ray tube and detector system rotate around the patient. The patient travels
at a speed of typically one slice thickness per 360 rotation (Kalendar and Polacin, 1991).
Figure 4 shows the approaches that are possible to manufacture the implant, starting with the
CT scans.
Figure 4 Three approaches to manufacture from CT (Gopakumar, 2000)
Figure 5 3D reconstructed image of the trauma location (Gopakumar, 2000)

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 12/25
11
Figure 6 Implant design methodology
Figure 7 Implant obtained in medical modeller Figure 8 2D image of the fit of
implant in 2D in medical modeler
Figure 9 Fit of designed implant in 3D

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 13/25
12
New Contribution
Rapid prototyping has been recently introduced in the field of medicine when compared to its
longstanding use in various engineering applications so numerous researchers have reported
the influence of RP technology in various areas of medical field. Some of areas in which RP
technology has been successfully contributed are discussed below.
Surgical planni ng
RP has proven to be beneficial to surgical planning as the these models provide the physician
and surgical team a visual aid that can be used in order to better plan a surgery, to study the
bone structure of patient before the surgery, to decrease surgery time and risk during surgeryas well as costs, to predict problem cause during operation and to facilitate the diagnostic
quality. These RP models can be used to rehearse complex procedure and for better
understanding the complex anomaly so these models are especially beneficial in surgeries
where there are anatomical abnormalities and deformities (Kai et al ., 1998; Liu et al ., 2006).
Some studies in heart surgery (Sodian et al ., 2007), spine surgery (Guarino et al ., 2007;
Mizutani, et al ,. 2008; Paiva, 2007), craniofacial and maxillofacial surgery (Faber et al .,
2006; Maravelakis et al ., 2008; Mehra et al ., 2011; Peltola et al ., 2012; Poukens et al ., 2003;
Zenha et al ., 2011) and hip surgery (Dhakshyani, et al ., 2012; Monahan. and Shimada, 2007)
have shown the potential and benefit of RP models in the field of surgery and reported a
significant improvement in diagnosis. In addition, surgeons estimated that the use of RP
models reduced operating time by a mean of 17.63% (D'urso, et al ., 1999).
Medical education and train ing
RP models provide a better demonstration of external and internal structure of human
anatomy, can be made in many colors so these models can be used as teaching aids in
research, medical education and in museums for educational and display purposes. RP
models can be distributed in kits to schools and museums for a better illustration of anatomy
and medical training purposes. Furthermore these models can be used by medical students or
young doctors to better understand the problems or surgical procedures without causing
discomfort to an actual patient (Liu et al ., 2006; Mori et al ., 2009; Nyaluke et al ., 1995).

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 14/25
13
Design and development of medical devices and instrumentati on
Another application of RP is in fabricating medical devices and instrumentations. RP
techniques can be used to design, develop, and manufacture medical devices and instruments.
It includes dental devices, hearing aids, and surgical aid tools (Noort, 2012).
Customized implant design
RP technology is very much able to fabricate customized implants and fixtures due to the
inherent strength of this technology to fabricate complex geometry with in very short time.
The combination of medical imaging technologies, rapid prototyping, and CAD packages
makes it possible to manufacture customized implants and fixtures that precisely fit a patient
at a reasonable cost (Balazic and Kopac, 2007). This technology allows the physicians to
create accurate implants for their patients rather than the use of standard sized implants such
as dental implants, hip sockets, knee joints and spinal implants could greatly benefit the
patients (Milovanovic and Trajanovic, 2007). Using RP, surgical implants have become more
precise, surgery time and risk of surgical complication has been significantly reduced, and to
make customized implants it’s an alternative to standard implants (Liu et al ., 2006; Noorani,
2006).
Scaff oldings and tissue engineering
RP techniques are very much suitable for generating implants with special geometrical
characteristics, such as scaffolds for the restoration of tissues and serve as an alternative to
conventional scaffold fabrication methods (Hutmacher et al ., 2004). Scaffolds are porous
supporting structures serve as an adhesion substrate for the cells and provide temporary
mechanical support and guidance to the growing tissue in damaged or defective bones of the
patient (Kim and Mooney, 1998; Yeong et al ., 2004). RP techniques like SLS, 3DP and FDM
have proved to be suitable for fabricating controlled porous structures through the use of
biomaterials and it has significantly contributed in the field of scaffolding and tissue
engineering. RP technology has increased the ability to create complex geometries,
customized products and provide high accuracy features, and also enhance the possibilities to
control pore size and distribution of pores within the scaffold (Peltola et al ., 2008).

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 15/25
14
Prosthetics and orthotics
Rapid prototyping has proven to be beneficial to the fields of prosthetics and orthotics as it
starts with specific patient anatomy. The patient’s specific alignment characteristics are
included in the model, allowing for development of a biomechanically correct geometry that
improves the fit, comfort, and stability (Noorani, 2006). There are always patients outside the
standard range, between sizes, or with special requirements caused by disease or genetics.
With the aid of RP, it becomes possible to manufacture a custom prosthesis that precisely fits
a patient at reasonable cost. For example, patterns for dental crowns and implant structures
can be fabricated using an RP machine (Liu et al ., 2006).
Mechanical bone replicas
Rapid prototyping can be used for the fabrication of mechanical bone replicas. With the aid
of RP, it becomes easy to replicate the material variations and mechanical characteristics
within a bone. A composite structure built with a lattice structure of SLA can create two
distinct regions that have properties similar to cortical and trabecular bones. These replicas of
bones can be used to observe the bone strength under different conditions. Additionally, it
can be beneficial to recreate events and the stresses, fractures, and other changes in the bone
can be observed, which would definitely help the doctors and researchers (Noorani, 2006;
http://www.rpc.msoe.edu/medical).
Forensics
RP can be a beneficial tool in criminal investigation especially in the homicide cases, where it
is very important to reconstruct the crime scene for investigation. RP models can be kept as
evidence in criminal investigation and will help investigators find answers to some questions.
In many cases, the ability to reconstruct scenes and events accurately would help forensic
experts to understand and solve the cases more quickly. These models are accurate enough to
see the effects of wounds and allow for accurate predictions of the forces, implements and
other key events can be determined using these models.
Especially, in the case of a surviving victim where a wound is of difficult access, e.g. for the
skull, a model can be used for detailed analysis. Using RP models, scenes can be re-created in
the court room as well as it can help prosecutors to throw some light on what really happened
(Liu et al ., 2006; http://www.rpc.msoe.edu/medical).

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 16/25
15
Anthropology
This is an another application where RP technology can be very beneficial to anthropologists
because replication of delicate bones, teeth and other artifact can be made so that molding,
measuring, and dissecting of the remains can be performed without causing harm to original
finding. Especially, in cases where only one or two specimens exist, research can be done on
built models without harming the original or rare specimen. The models that are built can also
be used to show changes in evolution that have taken place over vast periods of time
(Noorani, 2006; http://www.rpc.msoe.edu/medical).

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 17/25
16
Results and Discussion
In Customize prosthesis implant (Subburaj et al ., 2007), The prosthesis may change its color
or deteriorate over time, and may require replacement in future. This can be facilitated by the
availability of the digital model of the prosthesis. The postoperative appearance showed the
excellent result in terms of aesthetics. Researchers concluded that the use of RP and
associated technology provided a high degree of accuracy in term of shape, size and position
of the prosthesis, and enabled accurate reproduction customized prosthesis without requiring
sculpting skills, and was much faster than the conventional (manual) method.
Preoperative planning (Mahaisavariya et al ., 2006), the proper location of osteotomy, theamount of wedging bone and the tilting of the plane for osteotomy cut was measured by
performing 3D evaluation of the deformed and mirrored normal humerus on screen. After
calculating and determining the optimal configuration, the data of deformed and normal
humerus was used to fabricate RP models using 3D printing machine (Z Corp Inc.). These RP
models were used by surgeons to rehearse the osteotomy before a real surgery. Both patients
were successfully operated as surgical planning and shown excellent post operative results in
terms of cosmetic and functional result. Result clearly shows that RP and associated
technology (CT) can facilitate surgeons in preoperative planning for certain complex cases
like planning of osteotomy of complex deformity of hip, pelvis and spine, also allows the
surgeons to choose proper configuration and most appropriate location of osteotomy
according to individual patient need.
Tissue engineering (Ciocca et al ., 2009; Sachlos and Czernuszka, 2003), they found that
SLS fabricated scaffolds matched the design well, had mechanical strength within the range
of trabecular bone and supported the growth of tissue. It is concluded that PCL scaffolds
fabricated by SLS have great potential for the replacement of skelton tissue in the field of
tissue engineering.
Cranial reconstructive surgery (Gopakumar, 2000), during the surgery, the skin flap was
raised and the skull defect location was exposed. The cranial implant was then inserted on to
the defect and checked for proper fit. Once, the fit was confirmed, stainless steel wires were

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 18/25
17
used to secure the implant to the skull, after holes were drilled in the overlap area of the
implant with the skull. The implant designed had a good degree of fit with the skull. The cost
of an implant, for a case study such as the one above, cannot be estimated directly. The cost
of the implant depends primarily on the complexity of the part that is built in the RP machine.
The above case study was conducted as a part of a feasibility study of the manufacture of
customized implant in the south eastern region and hence, a direct estimation of the cost of
the implant was not done. Moreover, the saving in surgery times, pre-operation planning, and
patient recovery time are not easily quantifiable. The build time of the RP implant in the
FDM was nearly 8 h.

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 19/25
18
Conclusion
RP is making a significant effect in the field of medicine with a variety of medical
applications also itspotential has been demonstrated in several studies (Dhakshyani et al .,
2012; Esses et al . 2011; Mao et al , 2010; Sanghera et al ., 2001). A prospective trial (45
patients with craniofacial, maxillofacial, and skull base cervical spinal pathology cases were
selected) with the objective of assessing the utility of 3D models in complex surgery
performed by researchers (D'urso, et al ., 1999), concluded that these models significantly
improved the quality of pre-operative planning and diagnosis, reduced operative time and
risk, enhances team communication, and assists the patients to better understand their
pathology. Another study of 47 complex mandibular reconstruction cases (between 2003 and2009), concluded that 95.7% of the patients were found to have at least a satisfactory result
and the majority (38 out of 47) of patients were in a good and very good end result categories
(Zenha et al ., 2011).. Additionally, this technology makes the previously manual operations
much faster, accurate, and cheaper (Noort, 2012). The outcome based on literature review
and four case studies strongly suggests that RP technology might become part of standard
protocol in medical sector in the near future. However, presently this technology cannot be
employed in daily clinical practices due to some issues such as suitable material, time, and
high cost of the procedure. Therefore, these issues restrict the utilization of RP in complex
cases where considerable cost savings and quality benefits are generally expected (Giannatsis
and Dedoussis, 2009). Furthermore, this technology can be used as an alternative to
conventional fabrication methods with in the field of tissue engineering (Leong et al ., 2003),
customize implants (Noort, 2012; Traini et al ., 2008), and medical devices (Bertol et al .,
2010). Further research is required to reduce the overall cost (virtual planning and fabrication
cost) of RP technology, for the development of suitable biomaterials and development of RP
systems designed specifically for medical applications.
The design of the implant was carried out for the case study and the prototype of the implant
was manufactured. Further to the work, the medical implant produced from the RP model
was successfully implanted on the patient and the cosmetic effects of the surgery were found
to be good. There was a considerable reduction in the operation time. The model of the
implant also proved useful for the surgeons to rehearse the surgery prior to the actual
operation.

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 20/25
19
References
Abbott, J.R., Netherway D.J., Wingate P.G., Abbott A.H., David D.J., Trott, J.A. and Yuen,
T. (1998),“Computer generated mandibular model: surgical role”, Australian Dental Journal ,
Vol. 43 No. 6, pp. 373-378.
Ahn, D.G., Lee, J.Y. and Yang, D.Y. (2006), “Rapid prototyping and reverse engineering
applccation for orthopedic surgery planning”, Journal of Mechanical Science and
Technology, Vol. 20 No 1, pp. 19-28.
Armillotta, A. and Pelzer, R. (2008), “Modeling of porous structures for rapid prototyping of
tissue engineering scaffolds”, International Journal of Advanced Manufacturing Technology,
Vol. 39, pp. 501-511.
Balazic, M. and Kopac, J. (2007), “Improvements of medical implants based on moder n
materials and new technologies”, Journal of Achievements in Materials and Manufacturing
Engineering , Vol. 25, No 2, pp. 31-34.
Berce, P., Chezan, H. and Balc, N. (2005), “The application of rapid prototyping technologies
for manufacturing the custom implants”, in ESAFORM Conference, proceedings of the
ESAFORM conference in Cluj-Napoca, Romania, 2005, Rapid prototyping and rapid tooling,
pp. 679-682
.
Bertol L.S., Junior, W.K., Silva, F.P. and Kopp, C.A. (2010), “Medical design: direct metal
laser sintering of Ti – 6Al –4V”, Materials and Design, Vol. 31, pp. 3982 – 3988.
Bill, J.S., Reuther J.F., Dittmann, W., Kubler, N., Meier, J.L., Pistner, H. and Wittenberg, G.
(1995), “Stereolithography in oral and maxillofacial operation planning”, International
Journal of Oral and Maxillofacial Surgery, Vol. 24, pp. 98-103.
Brennan, J. (2010) “Production of anatomical models from CT scan data”, Masters
Dissertation, De Montfort University, Leicester, United Kingdom, 2010.

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 21/25
20
Chang, L.W., Chen H.W. and Ho, J.R. (1991), “Reconstruction of 3D medical images: a
nonlinear interpolation technique for reconstruction of 3D medical images”, Graphical
Models and Image Processing , Vol. 53 No. 4, pp. 382-391.
Chockalingam, K., Jawahara, N., Chandrasekarb, U. and Ramanathana, K.N. (2008),
“Establishment of process model for part strength in stereolithography”, Journal of Materials
Processing Technology, Vol. 208, pp. 348-365.
Chua C.K., Leong, K.F. and Lim, C.S. (2003), Rapid prototyping: principles and
applications, World Scientific Publishing Company, 5 Toh Tuck Link, Singapore.
Ciocca, L., Crescenzio F.D., Fantini, M. and Scotti, R. (2009), “CAD/CAM and rapid
prototyped scaffold construction for bone regenerative medicine and surgical transfer of
virtual planning: A pilot study”, Computerized Medical Imaging and Graphics, Vol. 33, pp.
58-62.
Cohen, A., Laviv, A., Berman, P., Nashef, R. and Abu, T.J. (2009), “Mandibular
reconstruction using stereolithographic 3-dimensional printing modeling technology” Oral
Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, Vol. 108 No.
5, pp. 661-666.
Dhakshyani, R., Nukman, Y., Abu Osman, A.N., and Vijay, C. (2011), “Preliminary report:
rapid prototyping models for dysplastic hip surgery” Central European Journal of Medicine,
Vol. 6 No.3, pp. 266-270.
Dhakshyani, R., Nukman, Y. and Abu Osman, A.N. (2012), “Rapid prototyping models for
dysplastic hip surgeries in Malaysia”, European Journal of Orthopaedic Surgery and
Traumatology, Vol. 22, pp. 41-46.
D'urso, P.S., Barker T.M., Earwaker W.J., Bruce L.J., Atkinson R.L., Lanigan M.W., Arvier
J.F. and Effeney D.J. (1999), “Stereolithographic biomodelling in cranio-maxillofacial
surgery: a prospective trial”, Journal of Cranio-Maxillofacial Surgery, Vol. 27, 30-37.

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 22/25
21
Esses, S.J., Berman, P, Bloom, A.I., and Sosna, J. (2011) “Clinical applications of physical
3D models derived from MDCT data and created by rapid prototyping” American Journal of
Roentgenology, Vol. 196, pp. W683-W688.
Faber, J., Berto, P.M. and Quaresma, M. (2006), “Rapid prototyping as a tool for diagnosis
and treatment planning for maxillary canine impaction”, American Journal of Orthodontics
and Dentofacial Orthopedics, Vol. 129, pp. 583-589.
Giannatsis, J. and Dedoussis, V. (2009), “Additive fabrication technologies applied to
medicine and health care: a review”, International Journal of Advanced Manufacturing
Technology, Vol. 40, pp.116-127.
Gibson, I., Cheung, L.K., Chow, S.P., Cheung, W.L., Beh, S.L., Savalani1, M. and Lee, S.H.
(2004),“The use of Rapid Prototyping to assist medical applications”, paper presented at 10th
Assises Européennes de Prototypage Rapide, 14 -15 September 2004, available at: http://
newmaker.com/nmsc/u/2010/20109/dld.../2010931138089411.pdf(accessed 27 February
2012).
Guangshen, X., Jing, J., Sheng, L., Ronghua, Q. and Huan, P. (2009), “Research on
optimizing build parameters for stereolithography technology,” in International Conference
on Measuring Technology and Mechatronics 2009, IEEE- Computer Society, pp. 883-886.
Guarino, J., Tennyson, S., McCain, G., Bond, L., Shea, K. and King, H. (2007), “Rapid
prototyping technology for surgeries of the pediatric spine and pelvis: benefits analysis”,
Journal of Pediatric Orthopaedics, Vol. 27 No. 8, pp. 955-960.
Hoque, M.E. (2011), Advanced applications of rapid prototyping technology in modern
engineering , InTech, Janeza Trdine 9, 51000 Rijeka, Croatia.
Hutmacher, D.W., Sittinger, M. and Risbud, M.V. (2004), “Scaffold-based tissue engineering
rationale for computer-aided design and solid free-form fabrication systems”, Trends in
Biotechnology, Vol. 22 No. 7, pp. 354 – 362.

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 23/25
22
Hur, S.M., Choi, K.H., Lee, S.H. and Chang, P.K. (2001), “Determination of fabricating
orientationand packing in SLS process”, Journal of Material Processing Technology, Vol.
112, pp. 236-243.
Kai, C.C., Meng, C.S., Ching, L.S., Hoe, E.K. and Fah, L.K. (1998), “Rapid prototyping
assisted surgery planning” International Journal of Advanced Manufacturing Technology,
Vol. 14, pp. 624- 630.
Kim, B.S. and Mooney, D.J. (1998), “Development of biocompatible synthetic extracellular
matrices for tissue engineering”, Trends in Biotechnology, Vol. 6 No. 5, pp. 224-230.
Lambrecht, J.T., Berndt, D.C., Schumacher, R. and Zehnder, M. (2009), “Generation of
threedimensional prototype models based on cone beam computed tomography”,
International Journal of Computer Assisted Radiology and Surgery, Vol. 4, pp. 175-180.
Lee, B.H., Abdullah, J. and Khan, Z.A. (2005), “Optimization of rapid prototyping
parameters for production of flexible ABS object”, Journal of Materials Processing
Technology, Vol. 169, pp. 54-61.
Lee, C.S., Kim, S.G., Kim, H.J. and Ahn, S.H. (2007), “Measurement of anisotropic
compressive strength of rapid prototyping parts”, Journal of Materials Processing
Technology, Vol. 187 – 188, pp. 627-630.
Leong, K.F., Cheah, C.M. and Chua, C.K. (2003), “Solid freeform fabrication of three-
dimensional scaffolds for engineering replacement tissues and organs”, Biomaterials, Vol.
24, pp. 2363-2378.
Liu Q., Leu, M.C. and Schmitt S.M. (2006), “Rapid prototyping in dentistry: technology and
application” International Journal of Advanced Manufacturing Technology, Vol. 29, pp. 317-
335.
Mao, K., Wang, Y., Xiao, S., Liu, Z., Zhang, Y., Zhang, X., Wang, Z., Lu, N., Shourong, Z.,
Xifeng, Z., Geng, C. and Baowei, L. (2010) “Clinical application of computer -designed
polystyrene models in complex severe spinal deformities: a pilot study” European Spine
Journal , Vol. 19, pp. 797-802.

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 24/25
23
Mahaisavariya, B., Sitthiseripratip, K., Oris, P. and Tongdee, T. (2006), “Rapid prototyping
model for surgical planning of corrective osteotomy for cubitus varus: report of two cases”,
Injury Extra, Vol. 37, pp. 176-180.
Maravelakis, E., David, K., Antoniadis, A., Manios, A., Bilalis, N. and Papaharilaou, Y.
(2008),
“Reverse engineering techniques for cranioplasty: a case study”, Journal of Medical
Engineering and Technology, Vol. 32 No. 2, pp. 115-121.
Meakin, J.R., Shepherd, D.E.T. and Hukins, D.W.L. (2004), “Fused deposition models from
CT scans”, British Journal of Radiology, Vol. 77, pp. 504-507.
Mehra, P., Miner, J., D’Innocenzo, R. and Nadershah, M. (2011), “Use of 3-D
stereolithographic models in oral and maxillofacial surgery”, Journal of Oral and
Maxillofacial Surgery, Vol. 10 No 1, pp. 6-13.
Melchels, F., Feijen, J. and Grijpma, D.W. (2010), “A review on stereolithography and its
applications in biomedical engineering”, Biomaterials, Vol. 31 No. 24, pp. 6121‐ 6130.
Milovanovic, J. and Trajanovic, M. (2007), “Medical applications of rapid prototyping”,
Mechanical Engineering , Vol. 5 No 1, pp. 79-85.
Mizutani, J., Matsubara, T., Fukuoka, M., Tanaka, N., Iguchi, H., Furuya, A., Okamoto, H.,
Wada, I. and Otsuka, T. (2008), “Application of full-scale three-dimensional models in
patients with rheumatoid cervical spine”, European Spine Journal , Vol. 17, pp. 644-649.
Monahan, M. and Shimada K. (2007), “A study of user performance employing a computer -
aided navigation system for arthroscopic hip surgery”, International Journal of Computer
Assisted Radiology and Surgery, Vol. 2, pp. 245-252.
Barker, T.M., Earwaker, W.J.S. and Lisle, D.A. (1994), “Accuracy of stereolithographic
models of human anatomy”,
Australasian Radiology, Vol. 38 No. 2, pp. 106-11.

8/10/2019 801382002 TERM WORK
http://slidepdf.com/reader/full/801382002-term-work 25/25
Beurner, J., Firtell, D. and Curtis, T. (1979), “Current concepts in cranioplasty”, Journal of
Prosthetic Dentistry, Vol. 42, pp. 67-77.
Cheng, A.C. and Wee, A.G. (1999), “Reconstruction of cranial bone defects using alloplastic
implants produced from stereolithographically-generated cranial model”, Annals of the
Academy of Medicine, Singapore, Vol. 28 No. 5, pp. 692-6.
Gopakumar, S. (2000), “Accuracy study in the manufacture of customized implants for
cranioplasty”, Master’s thesis, Asian Institute of Technology, Thailand.
Kalender, W.A. and Polacin, A. (1991), “Physical performance characteristics of spiral CT
scanning”, Medical-Physics, Vol. 18 No. 5, pp. 910-15.
Kermer, C., Linder, A., Friede, I., Wagner, A. and Millesi, W. (1998), “Properative
stereolithographic model planning for primary reconstruction in craniomaxillofacial trauma
surgery”, Journal of Craniomaxillofacial Surgery, Vol. 26, pp. 136-9.
Materialise, (2003), Mimics Software (Technical Manual), available at:
www.materialise.com Naber, H. (1998), “Advances in rapid prototyping technologies”,
Materials and Manufacturing Conference, Metalex,
Thailand.
Swaelens, B. and Kruth, J.P. (1993), “Medical applications of rapid prototyping techniques”,
Proceedings of the Fourth International Conference on Rapid Prototyping, pp. 107-20.
Figure 7 Implant fixation during cranioplasty RP in medicine: a case study in cranial
reconstructive surgery
Sunil Gopakumar Rapid Prototyping Journal
Volume 10 · Number 3 · 2004 · 207 – 211 211