-
11
96 The Body Systems: Clinical and Applied Topics
The CardiovascularSystemThe components of the cardiovascular
systeminclude the blood, heart, and blood vessels. Bloodflows
through a network of thousands of miles ofvessels within the body,
transporting nutrients,gases, wastes, hormones, and electrolytes
andredistributing the heat generated by active tissues.The exchange
of materials between the blood andperipheral tissues occurs across
the walls of tinycapillaries that are situated between the
arterialand venous systems. The total capillary surfacearea for
exchange is truly enormous, averagingaround 6300 square meters, 50
percent larger thanthe area of a football field.
Because the cardiovascular system plays a keyrole in supporting
all other systems, disorders ofthis system will affect virtually
every cell in the
body. One method of organizing the many potentialdisorders
involving this system is by the nature ofthe primary problem,
whether it affects the blood,the heart, or the vascular network.
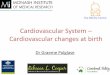
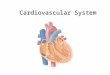
Figure A-34provides an overview of major blood disorders, andFigure
A-35 summarizes heart and blood vesseldisorders that are discussed
in the text and in latersections of the Applications Manual.
THE PHYSICAL EXAMINATIONAND THE CARDIOVASCULARSYSTEMIndividuals
with cardiovascular problems oftenseek medical attention with one
or more of the fol-lowing as chief complaints:
1. Weakness and fatigue: These symptoms devel-op when the
cardiovascular system can no
ThalassemiasSickle cell anemia (SCA)Hemophilia
Secondary disorders
Congenital disorders
Degenerative disorders
Excessive coagulationTrauma
Tumors
LeukemiaMyeloidLymphoid
Nutritional disorders
Iron deficiency anemiaIron loadingPernicious anemiaVitamin K
deficiency
Infection
BacteremiaViremiaSepticemiaPuerperal feverMalariaHemolytic
anemia
BLOODDISORDERS
Urinary system: Erythrocytosis
Immune problems: Hemolytic disease of the newborn
Hemorrhagic anemiaAplastic anemia
Figure A-34 Blood Disorders
Cardio.eap3am 8/21/02 9:36 AM Page 96
-
11
The Cardiovascular System 97
longer meet tissue demands for oxygen andnutrients. These
symptoms may occur becausecardiac function is impaired, as in heart
failure(p. 115) or cardiomyopathy (p. 104), or becausethe blood is
unable to carry normal amounts ofoxygen, as in the various forms of
anemia (p.102). In the early stages of these conditions,
theindividual feels healthy at rest, but becomesweak and fatigued
with any significant degree ofexertion because the cardiovascular
systemcannot keep pace with the rising tissue oxygendemands. In
more advanced stages of these dis-orders, weakness and fatigue are
chronic prob-lems that continue, even at rest.
2. Cardiac pain: This is a deep pain felt in thesubsternal
region and often radiating down theleft arm or up into the shoulder
and neck.There are two major causes of cardiac pain:
Constant severe pain can result frominflammation of the
pericardial sac, a condi-tion known as pericarditis. This
pericardialpain may superficially resemble the painexperienced in a
myocardial infarction (MI),or heart attack. Pericardial pain
differs from
the pain of an MI in that (a) it may berelieved by leaning
forward, (b) a fever maybe present, and (c) the pain does
notrespond to the administration of drugs,such as nitroglycerin,
that dilate coronaryblood vessels. Nitroglycerin, which is
effec-tive in relieving angina pectoris, does notrelieve the pain
associated with pericarditis.
Cardiac pain can also result from inade-quate blood flow to the
myocardium. Thistype of pain is called myocardial ischemicpain.
Ischemic pain occurs in angina pec-toris and in a myocardial
infarction. Anginapectoris (p. 106) most often results fromthe
constriction of coronary blood vesselsby atherosclerosis. The
associated painappears during physical exertion, whenmyocardial
oxygen demands increase, andthe pain is relieved by drugs such as
nitro-glycerin, which dilate coronary vessels andimprove coronary
blood flow. The painassociated with a myocardial infarction
isusually felt as a heavy weight or a constric-tion of the chest.
The pain of an MI is alsodistinctive because (a) it is not
necessarily
(b)
Patent foramen ovale and ductus arteriosusVentricular septal
defectsTetralogy of Fallot
Blood supply problems
Congenital disorders
Degenerative disorders
Cardiomyopathy
Tumors
MyxomaSarcoma
Functional disorders
Inflammation
ArteritisPhlebitis Thrombophlebitis
Degenerative disorders
Arteriosclerosis Focal calcification
AtherosclerosisAneurysmVaricose veins
Infection and inflammation
Carditis Endocarditis Myocarditis PericarditisRheumatic heart
disease (RHD)
CARDIOVASCULARDISORDERS
Coronary artery disease (CAD)Shock Circulatory Cardiogenic
Obstructive Neurogenic Septic Anaphylactic
HypertensionHypotensionEdemaCerebrovascular accident (CVA)
BloodvesselsHeart
Figure A-35 Disorders of the Heart and Blood Vessels
Cardio.eap3am 8/21/02 9:36 AM Page 97
-
11
98 The Body Systems: Clinical and Applied Topics
linked to exertion, (b) it is not relieved bynitroglycerin or
other coronary vasodila-tors, and (c) nausea, vomiting, and
sweat-ing may occur during the attack.
3. Palpitations: Palpitations are a persons percep-tion of an
altered heart rate. The individualmay complain of the heart
skipping a beat orracing. The most likely cause of palpitationsis
an abnormal pattern of cardiac activityknown as an arrhythmia. The
detection andanalysis of arrhythmias are considered in alater
section (p. 108).
4. Pain on movement: Individuals with advancedatherosclerosis
often experience pain in theextremities during muscle use. The pain
maybecome so severe that the person is unwillingor unable to walk
or perform other commonactivities. The underlying problem is
constric-tion or partial occlusion of major arteries, suchas the
external iliac arteries to the lower limbs,by plaque formation.
These are only a few of the many symptomsthat can be caused by
cardiovascular disorders. Inaddition, the individual may notice the
appearanceof characteristic signs of other cardiovascular
prob-lems. A partial listing of important cardiovascularsigns
includes the following:
Edema is an increase of fluid in the tissuesthat occurs when (a)
the pumping efficiencyof the heart is decreased, (b) the plasma
pro-tein content of the blood is reduced, or (c)venous pressures
are abnormally high. Thetissues of the lungs and the legs are
mostoften affected, and individuals experienceswollen feet and
ankles. When edema is sosevere that pressing on the affected
arealeaves an indention, the sign is called pittingedema. Edema is
discussed in Chapter 13 ofthe text (p. 397).
Breathlessness, or dyspnea, occurs when car-diac output is
inadequate for tissue oxygendemands. Dyspnea may also occur with
pul-monary edema, a buildup of fluid within thealveoli of the
lungs. Pulmonary edema and dys-pnea are often associated with
congestive heartfailure (p. 115).
Varicose veins are dilated superficial veins thatare visible at
the skin surface. This condition,which develops when venous valves
malfunc-tion, can be caused or exaggerated byincreased systemic
venous pressures. Varicoseveins are considered further on p.
112.
There may be characteristic and distinctivechanges in skin
coloration. For example, palloris the lack of normal red or pinkish
color to theskin of a Caucasian or the conjunctiva and oralmucosa
of darker-skinned individuals. Palloraccompanies many forms of
anemia, but mayalso be the result of inadequate cardiac output,
shock (p. 113), or circulatory collapse. Cyanosisis the bluish
color of the skin occurring with adeficiency of oxygen to the
tissues. Cyanosisusually results from either cardiovascular
orrespiratory disorders.
Vascular skin lesions were introduced in the dis-cussion of skin
disorders on p. 38. Characteristicvascular lesions may occur in
primary clottingdisorders (p. 104) and as a result of leukemia(p.
102). For example, abnormal bruising maybe the result of a disorder
affecting the clot-ting system, platelet production, or
vesselstructure. Petechiae, which appear as purplespots on the skin
surface, are often seen incertain types of leukemia or other
diseasesassociated with low platelet counts.
CARDIOVASCULAR DISORDERSAND DIAGNOSTIC PROCEDURESOften the
initial detection of a cardiovascular disor-der occurs during the
assessment stage of a physi-cal examination.
1. When the vital signs are taken, the pulse ischecked for
vigor, rate, and rhythm. Weak orirregular heart beats will often be
noticed atthis time.
2. The blood pressure is monitored with a stetho-scope, blood
pressure cuff, and sphygmo-manometer. Unusually high or low
readingscan alert the examiner to potential problemswith cardiac or
vascular function. However, adiagnosis of hypotension or
hypertension is notmade on the basis of a single reading, but
afterseveral readings over a period of time.Hypertension and
hypotension are discussed indetail on p. 112.
3. The heart sounds are monitored by ausculta-tion with a
stethoscope:
Cardiac rate and rhythm can be checkedand arrhythmias
detected.
Abnormal heart sound, or murmurs, mayindicate problems with
atrioventricular orsemilunar valves. Murmurs are noted inrelation
to their location in the heart (asdetermined by the position of the
stetho-scope on the chest wall), the time of occur-rence in the
cardiac cycle, and whether thesound is low or high pitched.
Nothing is usually heard during ausculta-tion of normal vessels
of the circulatorysystem. Bruits are the sounds resultingfrom
turbulent blood flow around anobstruction within a vessel. Bruits
are typi-cally heard where large atheroscleroticplaques have
formed.
Functional abnormalities of the heart andblood vessels can often
be detected through physi-
Cardio.eap3am 8/21/02 9:36 AM Page 98
-
cal assessment and the recognition of characteris-tic signs and
symptoms. The structural basis forthese problems is usually
determined through theuse of scans, X-rays, and the monitoring of
electri-cal activity in the heart. For problems with a
hema-tological basis, laboratory tests performed on bloodsamples
usually provide the information necessaryto reach a diagnosis.
Polycythemia EAP p. 347An elevated hematocrit with a normal
blood volumeconstitutes polycythemia (po-l-s-TH-m-uh).There are
several different types of polycythemia.Erythrocytosis
(e-rith-r|-s-T-sis), a polycythemiaaffecting only red blood cells,
will be consideredlater in the chapter. Polycythemia vera
(truepolycythemia) results from an increase in thenumbers of all
blood cells. The hematocrit mayreach 8090, at which point the
tissues becomeoxygen-starved because red blood cells are block-ing
the smaller vessels. This condition seldomstrikes young people;
most cases involve patientsage 6080. There are several treatment
options,but none cures the condition. The cause of poly-cythemia
vera is unknown, although there is someevidence that the condition
is linked to radiationexposure.
Thalassemia EAP p. 349The thalassemias are a diverse group of
inheritedblood disorders caused by an inability to produceadequate
amounts of the normal protein subunitsof hemoglobin. Each
hemoglobin molecule has twoalpha ()chains and two beta () chains. A
specificcondition is categorized as an alpha-thalassemiaor
beta-thalassemia depending on whether the or hemoglobin subunits
are affected. Normal indi-viduals inherit two alpha chain genes
from eachparent, and alpha- thalassemia develops when oneor more of
these genes are missing or inactive. Theseverity of the symptoms
varies depending on howmany normal alpha chain genes remain
functional.For example, an individual with three normal alphachain
genes will not develop symptoms at all, butthis person can be a
carrier, passing the defect tothe next generation. A child born of
parents whoare both carriers is likely to develop a more severeform
of the disease:
Individuals with two copies of the normal alphachain gene,
rather than four copies, havesomewhat impaired hemoglobin
synthesis. Thered blood cells are small and contain less thanthe
normal quantity of hemoglobin. This condi-tion, known as
alpha-thalassemia trait, affectsroughly 2 percent of African
Americans andmany Southeast Asians.
Individuals with one copy of the alpha chaingene have very small
(microcytic) red blood cellsthat are relatively fragile.
Individuals with no functional copies of thealpha chain gene
usually die shortly after birth,because the hemoglobin synthesized
cannotbind and transport oxygen normally. The inci-dence of fatal
alpha-thalassemia is highestamong Southeast Asians.
Each person inherits only one gene for the betahemoglobin chain
from each parent. If an individ-ual does not receive a copy of the
normal gene fromeither parent, the condition of
beta-thalassemiamajor, or Cooleys disease, develops. Symptoms
ofthis condition include severe anemia; microcytosis;a low
hematocrit (under 20); and enlargement ofthe spleen, liver, heart,
and areas of red bone mar-row. Potential treatments for those with
severesymptoms include transfusions, splenectomy (toslow the rate
of RBC recycling), and bone marrowtransplantation. Inheriting one
normal gene resultsin beta-thalassemia minor, or
beta-thalassemiatrait, which seldom produces clinical symptoms.The
rates of hemoglobin synthesis are depressed byroughly 15 percent,
but this decrease does notaffect their functional abilities, and no
treatment isnecessary.
Sickle Cell Anemia EAP p. 349Sickle cell anemia (SCA) results
from the produc-tion of an abnormal form of hemoglobin. The chains
are involved, and the abnormal subunit iscalled hemoglobin S.
Sickle cell anemia affects60,00080,000 African Americans today;
this rep-resents roughly 0.14 percent of the African-American
population.
An individual with sickle-cell anemia carriestwo copies of the
abnormal gene, one from eachparent. If only one copy is present,
the individualhas a sickling trait. One African American in 12
car-ries the sickling trait. Although it is now knownthat the genes
are present in Americans ofMediterranean, Middle Eastern, and East
Indianancestry, statistics on the incidence of sickling traitand
SCA in these groups are as yet unavailable.
In individuals with the sickling trait, most ofthe hemoglobin is
of the normal form and the ery-throcytes function normally. But the
presence ofthe abnormal hemoglobin gives the individual theability
to resist the parasitic infections that causemalaria, a
mosquito-borne illness. The malariaparasites enter the bloodstream
when an individualis bitten by an infected mosquito. The
microorgan-isms then invade and reproduce within the ery-throcytes.
But when they enter an erythrocyte froma person with the sickling
trait, the cell respondsby sickling. Either the sickling itself
kills the para-site, or the sickling attracts the attention of
aphagocyte that engulfs the RBC and kills the para-site. In either
event the individual remains unaf-fected by the disease, while
normal individualssicken and often die.
Symptoms of sickle cell anemia include painand damage to a
variety of organs and systems,
The Cardiovascular System 99
11
Cardio.eap3am 8/21/02 9:36 AM Page 99
-
11
100 The Body Systems: Clinical and Applied Topics
depending on the location of the obstructions. Inaddition, the
trapped red blood cells eventuallydie and break down, producing a
characteristicanemia. Transfusions of normal blood can tem-porarily
prevent additional complications, andthere are experimental drugs
that can control orreduce sickling. Hydroxyurea is an
anticancerdrug that stimulates production of fetal hemoglo-bin, a
slightly different form of hemoglobin pro-duced during development.
It is effective, but hastoxic side effects (not surprising in an
anticancerdrug). The food additive butyrate, found in but-ter and
other foods, appears to be even moreeffective in promoting the
synthesis of fetalhemoglobin. In clinical trials it has been
effectivein treating sickle cell anemia and other condi-tions
caused by abnormal hemoglobin structure,such as
beta-thalassemia.
Bilirubin Tests and JaundiceEAP p. 349
When hemoglobin is broken down, the heme units(minus the iron)
are converted to bilirubin.Normal serum bilirubin concentrations
rangefrom 0.1 to 1.2 mg/dl. Of that amount, roughly85 percent will
be metabolized and removed bythe liver. Several different clinical
conditions arecharacterized by an increase in the total
plasmabilirubin concentration. In such conditions,bilirubin
diffuses into peripheral tissues, givingthem a yellow coloration
that is most apparent inthe skin and over the sclera of the eyes.
This com-bination of signs (yellow skin and eyes) is calledjaundice
(JAWN-dis).
Jaundice can have many different causes, butblood tests that
determine the concentration of dif-ferent forms of bilirubin can
provide useful diagnos-tic clues. For example, hemolytic jaundice
resultsfrom the destruction of large numbers of red bloodcells.
When this occurs, phagocytes release massivequantities of one form
of bilirubin (unconjugated)into the blood. Because the liver cells
accelerate thesecretion of bilirubin in the bile, the blood
concen-tration of another form of bilirubin (conjugated) doesnot
increase proportionately. A blood test from apatient with hemolytic
jaundice would reveal (1) ele-vated total bilirubin, (2) high
concentrations ofunconjugated bilirubin, and (3) conjugated
bilirubincontributing much less than 15 percent to the
totalbilirubin concentration.
These results are quite different from thoseseen in obstructive
jaundice. In this condition,the ducts that remove bile from the
liver are con-stricted or blocked. Liver cells cannot get rid
ofconjugated bilirubin, and large quantities diffuseinto the blood.
In this case, diagnostic tests wouldshow (1) elevated total
bilirubin, (2) unconjugatedbilirubin contributing much less than 85
percentto the total bilirubin concentration, and (3)
highconcentrations of conjugated bilirubin.
Iron Deficiencies and ExcessesEAP p. 350
If dietary supplies of iron are inadequate, hemoglo-bin
production slows down, and symptoms of irondeficiency anemia
appear. This form of anemia canalso be caused by any condition that
produces ablood loss, since the iron in the lost blood cannot
berecycled. As the red blood cells are replaced, ironreserves must
be mobilized for use in the synthesisof new hemoglobin molecules.
If those reserves areexhausted, or dietary sources are
inadequate,symptoms of iron deficiency appear. In iron defi-ciency
anemia, the red blood cells are unable tosynthesize functional
hemoglobin, and they areunusually small when they enter the
circulation.The hematocrit declines, and the hemoglobin con-tent
and oxygen-carrying capacity of the blood aresubstantially reduced.
Symptoms include weaknessand a tendency to fatigue easily.
Women are especially dependent on a normaldietary supply of
iron, because their iron reservesare smaller than those of men. The
body of a nor-mal man contains around 3.5 g of iron in the
ionicform Fe2+. Of that amount, 2.5 g are bound to thehemoglobin of
circulating red blood cells, and therest is stored in the liver and
bone marrow. Inwomen, the total body iron content averages 2.4
g,with roughly 1.9 g incorporated into red bloodcells. Thus a
womans iron reserves consist of only0.5 ghalf that of a typical
man.
Because their reserves are relatively small,women are dependent
on a reliable dietary supplyof iron. When the demand for iron
increases out ofproportion with dietary supplies, iron
deficiencydevelops. An estimated 20 percent of menstruatingwomen in
the United States show signs of iron defi-ciency. Pregnancy also
stresses iron reserves, forthe woman must provide the iron needed
to pro-duce both maternal and fetal erythrocytes.
Good dietary sources of iron include liver, redmeats, kidney
beans, egg yolks, spinach, and car-rots. Iron supplements can help
prevent iron defi-ciency, but too much iron can be as dangerous
astoo little. Iron absorption across the digestivetract normally
keeps pace with physiologicaldemands. When the diet contains
abnormallyhigh concentrations of iron, or hereditary
factorsincrease the rate of absorption, the excess irongets stored
in peripheral tissues. This is callediron loading. Eventually cells
begin to malfunctionas massive iron deposits accumulate in the
cyto-plasm. For example, iron deposits in pancreaticcells can lead
to diabetes mellitus; deposits incardiac muscle cells lead to
abnormal heart con-tractions and heart failure. (There is evidence
thatiron deposits in the heart caused by the overcon-sumption of
red meats may contribute to heartdisease.) Liver cells become
nonfunctional, andliver cirrhosis may develop.
Comparable symptoms of iron loading mayappear following repeated
transfusions of whole
Cardio.eap3am 8/21/02 9:36 AM Page 100
-
11
The Cardiovascular System 101
blood, because each unit of whole blood containsroughly 250 mg
of iron. For example, as notedabove, the various forms of
thalassemia result froma genetic inability to produce adequate
amounts ofone of the four globin chains in hemoglobin.Erythrocyte
production and survival are reduced,and so is the oxygen-carrying
capacity of the blood.Individuals with severe untreated thalassemia
usu-ally die in their twenties, but not because of theanemia. These
patients are treated for severe ane-mia with frequent blood
transfusions that prolonglife, but the excessive iron loading
eventually leadsto fatal heart problems.
Erythrocytosis and Blood Doping EAP p. 351
In erythrocytosis (e-rith-r|-s-T-sis), the bloodcontains
abnormally large numbers of red bloodcells. Erythrocytosis usually
results from the mas-sive release of erythropoietin by tissues
(especiallythe kidneys) deprived of oxygen. People moving tohigh
altitudes usually experience erythrocytosisfollowing their arrival,
because the air contains lessoxygen than it does at sea level. The
increasednumber of red blood cells compensates for the factthat
individually each RBC is carrying less oxygenthan it would at sea
level. Mountaineers and thoseliving at altitudes of 10,00012,000
feet may havehematocrits as high as 65.
Individuals whose hearts or lungs are function-ing inadequately
may also develop erythrocytosis.For example, this condition is
often seen in heartfailure and emphysema, two conditions
discussedin later chapters. Whether the blood fails to circu-late
efficiently or the lungs do not deliver enoughoxygen to the blood,
peripheral tissues remain oxy-gen-poor despite the rising
hematocrit. Having ahigher concentration of red blood cells
increasesthe oxygen-carrying capacity of the blood, but italso
makes the blood thicker and harder to pusharound the circulatory
system. This increases thework load on the heart, making a bad
situationeven worse.
The practice of blood doping was temporari-ly widespread among
competi t ive athletesinvolved with endurance sports such as
cycling.The procedure entails removing whole blood fromthe athlete
in the weeks before an event. Thepacked red cells are separated
from the plasmaand stored. By the time of the race, the
competi-tors bone marrow will have replaced the lostblood.
Immediately before the event the packedred cells are reinfused,
increasing the hemat-ocrit. The objective is to elevate the
oxygen-car-rying capacity of the blood, and so increaseendurance.
The consequence is that the athletesheart is placed under a
tremendous strain. Thelong-term effects are unknown, but the
practiceobviously carries a significant risk. Once EPObecame
available, its ease of use replaced blooddoping. Both have been
banned in amateur
sports. Attempts to circumvent this rule by theuse of EPO in
19921993 resulted in the tragicdeaths of 18 European cyclists.
Blood Tests and RBCs EAP p. 351This section describes several
common blood teststhat assess circulating RBCs.
RETICULOCYTE COUNT. Reticulocytes are imma-ture red blood cells
that are still synthesizinghemoglobin. Most reticulocytes remain in
the bonemarrow until they complete their maturation, butsome enter
the circulation. Reticulocytes normallyaccount for around 0.8
percent of the erythrocytepopulation. Values above 1.5 percent or
below 0.5percent indicate that something is wrong with therates of
RBC survival or maturation.
HEMATOCRIT (Hct). The hematocrit value is thepercentage of whole
blood occupied by cells.Normal adult hematocrits average 46 for men
and42 for women, with ranges of 4252 for men and3747 for women.
HEMOGLOBIN CONCENTRATION (Hb). This testdetermines the amount of
hemoglobin in the blood,expressed in grams per deciliter (g/dl).
Normalranges are 1418 g/dl in males and 1216 g/dl infemales. The
differences in hemoglobin concentra-tion reflect the differences in
hematocrit. For bothsexes, a normal RBC contains 2733 picograms(pg)
of hemoglobin.
RBC COUNT. Calculations of the RBC count, thenumber of RBCs per
microliter of blood, are basedon the hematocrit and hemoglobin
content, andcan be used to develop a better picture of the
con-dition of the RBCs. Values often reported in bloodscreens
include
Mean corpuscular volume (MCV), the averagevolume of an
individual red blood cell, in cubicmicrometers. It is calculated by
dividing thevolume of red cells per microliter by the RBCcount,
using the formula
Normal values range from 80 to 98. For a rep-resentative
hematocrit of 46 and an RBC countof 5.2 million, the mean
corpuscular volumewould be
Cells of normal size are normocytic, whereaslarger-than-normal
or smaller-than-normalRBCs are called macrocytic or
microcytic,respectively.
MCV =Hct 10
RBC count (in millions)
MCV =465.2
10 = 88.5 m3
Cardio.eap3am 8/21/02 9:36 AM Page 101
-
11
102 The Body Systems: Clinical and Applied Topics
Mean corpuscular hemoglobin concentration(MCHC), the amount of
hemoglobin within asingle RBC, expressed in picograms. Normalvalues
range from 27 to 31 pg. The MCHC iscalculated as
RBCs containing normal amounts of hemoglobinare termed
normochromic, while hyperchromicand hypochromic indicate higher or
lower thannormal hemoglobin content, respectively.
Anemia (a-N-m-uh) exists when the oxygen-carrying capacity of
the blood is reduced, diminish-ing the delivery of oxygen to
peripheral tissues.Such a reduction causes a variety of
symptoms,including premature muscle fatigue, weakness,lethargy, and
a general lack of energy. Anemia mayexist because the hematocrit is
abnormally low orbecause the amount of hemoglobin in the RBCs
isreduced. Standard laboratory tests can be used todifferentiate
between the various forms of anemiaon the basis of the number,
size, shape, and hemo-globin content of red blood cells. As an
example,Table A-20 shows how this information can be usedto
distinguish among four major types of anemia.
1. Hemorrhagic anemia results from severeblood loss.
Erythrocytes are of normal size,each contains a normal amount of
hemoglobin,and reticulocytes are present in normal con-centrations,
at least initially. Blood tests wouldtherefore show a low
hematocrit and low hemo-globin, but the MCV, MCHC, and
reticulocytecounts would be normal.
2. In aplastic (-PLAS-tik) anemia, the bone mar-row fails to
produce new red blood cells. The1986 nuclear accident in Chernobyl
(USSR)caused a number of cases of aplastic anemia.The condition is
fatal unless surviving stemcells repopulate the marrow or a bone
marrowtransplant is performed. In aplastic anemia thecirculating
red blood cells are normal in allrespects, but because new RBCs are
not beingproduced, the RBC count, Hct, Hb, and reticu-locyte count
are extremely low.
3. In iron deficiency anemia, normal hemoglo-bin synthesis
cannot occur, because ironreserves are inadequate. Developing red
bloodcells cannot synthesize functional hemoglobin,
and as a result they are unusually small. Ablood test therefore
shows a low hematocrit,low hemoglobin content, low MCV, and
lowMCHC, but a normal reticulocyte count. Anestimated 60 million
women worldwide haveiron deficiency anemia. (See the discussion
oniron deficiencies and excesses on p. 100.)
4. In pernicious (per-NISH-us) anemia, normal redblood cell
maturation ceases because of an inad-equate supply of vitamin B12.
Erythrocyte pro-duction declines, and the red blood cells
areabnormally large and may develop a variety ofbizarre shapes.
Blood tests from a person withpernicious anemia indicate a low
hematocrit witha very high MCV and a low reticulocyte count.
Hemolytic Disease of the NewbornEAP p. 354
Hemolytic disease of the newborn results from thematernal
production of anti-Rh antibodies thatcross the placenta to attack
fetal Rh-positive redblood cells. Within 6 months after delivery,
roughly20 percent of Rh-negative mothers who were preg-nant with
Rh-positive children have become sensi-tized and produce anti-Rh
antibodies. For theentire sequence of events, see Figure A-36.
Withouttreatment, the fetus will probably die before deliv-ery or
shortly thereafter.
A newborn with severe HDN is anemic, and thehigh concentration
of circulating bilirubin pro-duces jaundice. Because the maternal
antibodiesremain active for 1 to 2 months after delivery,
theinfants entire blood volume may need to bereplaced by an
exchange transfusion. Bloodreplacement removes most of the maternal
anti-bodies as well as the affected erythrocytes, reduc-ing the
complications and the chance the infantwill die.
When there is a danger that the fetus may notsurvive to full
term, premature delivery may beinduced after 7 to 8 months of
development. In asevere case affecting a fetus at an earlier stage,
oneor more transfusions can be given while the fetuscontinues to
develop within the uterus.
To avoid the problem, the maternal productionof Rh antibodies is
prevented by administering Rhantibodies (available under the name
RhoGam)after delivery or miscarriage or abortion. Theseforeign
antibodies quickly destroy any fetal redblood cells that enter the
maternal circulation.Thus there are no exposed antigens to
stimulatethe maternal immune system, sensitization doesnot occur,
and Rh antibodies are not produced.This relatively simple procedure
could almostentirely prevent HDN mortality caused by
Rhincompatibilities.
The Leukemias EAP p. 356
Leukemias characterized by the presence of abnor-mal
granulocytes or other cells of the bone marroware called myeloid;
leukemias that involve abnor-
Table A-20 RBC Tests and Anemias
Reticu-locyte
Anemia type Hct Hb count MCV MCHC
Hemorrhagic low low normal normal normalAplastic low low very
low normal normalIron deficiency low low normal low lowPernicious
low low very low high high
MCHC =Hb
10RBC count (in millions)
Cardio.eap3am 8/21/02 9:36 AM Page 102
-
11
The Cardiovascular System 103
mal lymphocytes are termed lymphoid. The firstsymptoms appear as
immature and abnormalwhite blood cells appear in the circulation.
Astheir numbers increase, they travel through thecirculation,
invading tissues and organs through-out the body.
These cells are extremely active, and theyrequire abnormally
large amounts of energy. As inother cancers, described in Chapter 3
of the text andelsewhere in this Applications Manual (p. 33),
invad-ing leukemic cells gradually replace the normal
cells,especially in the bone marrow. Red blood cell, nor-
mal WBC, and platelet formation decline, withresulting anemia,
infection, and impaired blood clot-ting. Untreated leukemias are
invariably fatal.
Leukemias are classified as acute (short andsevere) or chronic
(prolonged). Acute leukemias maybe linked to radiation exposure,
hereditary suscep-tibility, viral infections, or unknown
causes.Chronic leukemias may be related to chromosomalabnormalities
or immune system malfunctions.Survival in untreated acute leukemia
averagesabout three months; individuals with chronicleukemia may
survive for years.
Rh
Rh Rh
Rh
Rh+
Rh+ Rh+
Rh+
Rh Rh
Rh
Rh+
Rh+
Rh+
Rh+
Rh+
Rh+
Rh
RhRh
Rh
Rh
RhRh
Rh
Rh+ Rh+
Rh+
First pregnancy
Maternalblood
Maternaltissue
Fetaltissue
Fetalblood
Placenta
Maternaltissue
Fetaltissue
Maternaltissue
Maternaltissue
Fetaltissue
Rh
Second pregnancyMaternal agglutinin production
(anti-Rh)
Hemorrhagingat delivery
FIGURE A-36 Rh Factors and Pregnancy
When an Rh-negative woman has her first Rh-positive child,
mixing of fetal and maternal blood occurs at delivery when the
placentalconnection breaks down. The appearance of Rh-positive
blood cells in the maternal circulation sensitizes the mother,
stimulating theproduction of anti-Rh agglutinins. If another
pregnancy occurs with an Rh-positive fetus, maternal agglutinins
can cross the placentalbarrier and attack fetal blood cells,
producing symptoms of HDN (hemolytic disease of the newborn).
Cardio.eap3am 8/21/02 9:36 AM Page 103
-
11
104 The Body Systems: Clinical and Applied Topics
Effective treatments exist for some forms ofleukemia and not
others. For example, when acutelymphoid leukemia is detected early,
8590 percentof patients can be held in remission for 5 years
orlonger, but only 1015 percent of patients withacute myeloid
leukemia survive 5 years or more.The yearly mortality rate for
leukemia (all types) inthe United States has not declined
appreciably inthe past 30 years, remaining at around 6.8 per100,000
population. However, new treatments arebeing developed that show
promise when usedagainst specific forms of leukemia. For
example,administration of -interferon, a hormone of theimmune
system, has been very effective in treatinghairy cell leukemia and
chronic myeloid leukemia.
One option for treating acute leukemias is toperform a bone
marrow transplant. In this proce-dure, massive chemotherapy or
radiation treatmentis given, enough to kill all the cancerous
cells.Unfortunately, this also destroys the patientsblood cells and
stem cells in the bone marrow andother blood-forming tissues. The
individual thenreceives an infusion of healthy bone marrow
cellsthat repopulate the blood and marrow tissues.
If the bone marrow is extracted from anotherperson (a
heterologous marrow transplant), caremust be taken to ensure that
the blood types andtissue types are compatible (see Chapters 11
and14 of the text). If they are not, the new lymphocytesmay attack
the patients tissues, with potentiallyfatal results. Best results
are obtained when thedonor is a close relative. In an autologous
marrowtransplant bone marrow is removed from thepatient, cleansed
of cancer cells, and reintroducedafter radiation or chemotherapy
treatment.Although there are fewer complications, the prepa-ration
and cleansing of the marrow are technicallydifficult and time
consuming.
Bone marrow transplants are also performed totreat patients
whose bone marrow has beendestroyed by toxic chemicals or
radiation. Forexample, heterologous transplants were used
suc-cessfully in the USSR to treat survivors of theChernobyl
nuclear reactor accident in 1986.
Testing the Clotting SystemEAP p. 359
Several clinical tests check the efficiency of theclotting
system:
BLEEDING TIME. This test measures the time ittakes for a small
skin wound to seal itself. Thereare several variations on this
procedure, with nor-mal values ranging from 1 to 9 minutes. The
non-prescription drug aspirin prolongs the bleedingtime by
affecting platelet function and suppressingthe extrinsic
pathway.
COAGULATION TIME. In this test, a sample ofwhole blood is
allowed to stand under controlledconditions until a visible clot
has formed. Normalvalues range from 3 to 15 minutes. The test
hasseveral potential sources of error, and so is not
very accurate. Nevertheless, it is the simplest testthat can be
performed on a blood sample.
PARTIAL THROMBOPLASTIN TIME (PTT). In thistest, a plasma sample
is mixed with chemicals thatmimic the effects of activated
platelets. Calcium ionsare then introduced, and the clotting time
is record-ed. Clotting normally occurs in 3550 seconds if
theenzymes and clotting factors of the intrinsic pathwayare present
in normal concentrations.
PLASMA PROTHROMBIN TIME (PROTHROMBINTIME, PT). This test checks
the performance of theextrinsic pathway. The procedure is similar
to thatin the PTT test, but the clotting process is triggeredby
exposure to a combination of tissue prothrombi-nase (formerly
called thromboplastin) and calciumions. Clotting normally occurs in
1214 seconds.
Infection and Inflammation of the Heart EAP p. 369
Many different microorganisms may infect hearttissue, leading to
serious cardiac abnormalities.Carditis (kar-D-tis) is a general
term indicatinginflammation of the heart. Clinical
conditionsresulting from cardiac infection are usually identi-fied
by the primary site of infection. For example,those affecting the
endocardium produce symp-toms of endocarditis. Endocarditis
primarilyaffects the chordae tendineae and heart valves, andthe
mortality rate may reach 2135 percent. Themost severe complications
result from the forma-tion of blood clots on the damaged surfaces.
Theseclots subsequently break free, entering the circula-tion as
drifting emboli (see p. 361 of the text) thatmay cause strokes,
heart attacks, or kidney failure.Destruction of heart valves by
infection may lead tovalve leakage, heart failure, and death.
Bacteria, viruses, protozoa, and fungalpathogens that either
attack the myocardiumdirectly or release toxins that do,
producemyocarditis. The microorganisms implicatedinclude those
responsible for many of the condi-tions discussed in earlier
chapters, includingdiphtheria, syphilis, polio, and malaria. The
mem-branes of infected heart muscle cells become facili-tated, and
the heart rate may rise dramatically.Over time, abnormal
contractions may appear, theheart muscle weakens, and these may
eventuallyprove fatal.
The Cardiomyopathies EAP p. 370The cardiomyopathies
(kar-d-|-m-OP-a-thz)include an assortment of diseases with a
commonsymptom: the progressive, irreversible degenerationof the
myocardium. Cardiac muscle fibers are dam-aged and replaced by
fibrous tissue, and the mus-cular walls of the heart become thin
and weak. Asmuscle tone declines, the ventricular chambersbecome
greatly enlarged. When the remainingfibers cannot develop enough
force to maintain car-diac output, symptoms of heart failure
develop.
Cardio.eap3am 8/21/02 9:36 AM Page 104
-
Chronic alcoholism and coronary artery diseaseare probably the
most common causes of cardiomy-opathy in the United States.
Infectious agents,including viruses, bacteria, fungi, and
protozoans,can also produce cardiomyopathies. Diseases affect-ing
neuromuscular performance, such as musculardystrophy (discussed
elsewhere in this manual),can also damage cardiac muscle fibers, as
can star-vation or chronic variations in the extracellular
con-centrations of calcium or potassium ions.
There are also several inherited forms of car-diomyopathy.
Hypertrophic cardiomyopathy(HCM) is an inherited disorder that
makes the wallof the left ventricle thicken to the point at which
ithas difficulty pumping blood. Most people withHCM do not become
aware of it until relatively latein life. However, HCM can also
cause a fatalarrhythmia; it has been implicated in the suddendeaths
of several young athletes. The implantationof an electronic cardiac
pacemaker has proved tobe beneficial in controlling these
arrhythmias.
Finally, there are a significant number of casesof idiopathic
cardiomyopathy, a term used when theprimary cause cannot be
determined.
Heart Transplants and AssistDevices EAP p. 370
Individuals with severe cardiomyopathy may beconsidered as
candidates for heart transplants.This surgery involves the complete
removal of theweakened heart and its replacement with a hearttaken
from a suitable donor. To survive thesurgery, the recipient must be
in otherwise satis-factory health. Because the number of
suitabledonors is limited, the available hearts are usuallyassigned
to individuals younger than age 50. Outof the 8,00010,000 U.S.
patients each year whohave potentially fatal cardiomyopathies, only
about1,000 receive heart transplants. After
successfultransplantation, there is an 8085 percent one-year
survival rate and a 5070 percent five-yearsurvival rate. These
rates are quite good, consider-ing that these patients would have
died if thetransplant had not been performed.
Many individuals with cardiomyopathy who areinitially selected
for transplant surgery succumb tothe disease before a suitable
donor becomes avail-able. For this reason there continues to be
consid-erable interest in the development of an artificialheart.
One model, the Jarvik-7, had limited clinicaluse in the 1980s.
Attempts to implant it on a per-manent basis were unsuccessful,
primarilybecause of the formation of blood clots on themechanical
valves and infections involving itsexternal power source. When the
clots broke free,they formed drifting emboli that plugged
peripheralvessels, producing strokes, kidney failure, andother
complications. In 1989 the federal govern-ment prohibited further
experimental use of theJarvik-7 as a permanent heart implant.
Modifiedversions of this unit and others now under devel-opment may
still be used to maintain transplant
candidates while awaiting the arrival of a donororgan. These are
called left ventricular assistdevices (LVAD). As the name implies,
these devicesassist, rather than replace, the damaged heart.
Amechanical left ventricular assist device has beenused to support
a patient awaiting a transplant.
An experimental approach, which has yet to betried with human
patients, involves the insertion offetal heart muscle cells in a
damaged adult heart.The fetal cells appear to adapt to their
surroundingsand differentiate into functional contractile
cells.
RHD and Valvular StenosisEAP p. 373
Rheumatic (roo-MA-tik) fever is an inflammatorycondition that
may develop following untreatedinfection by streptococcal bacteria
(strep throat).Rheumatic fever most often affects children of
age515 years; symptoms include high fever, jointpain and stiffness,
and a distinctive full-body rash.Obvious symptoms usually persist
for less than 6weeks, although severe cases may linger for 6months
or more. The longer the duration of theinflammation, the more
likely it is that carditis willdevelop. The carditis that does
develop in 5060percent of patients often escapes detection, andscar
tissue forms gradually in the myocardium andthe heart valves. Valve
condition deteriorates overtime, and valve problems serious enough
to affectcardiac function may not appear until 1020 yearsafter the
initial infection.
Over the interim the affected valves becomethickened and often
calcified to some degree.This thickening narrows the opening
guarded bythe valves, producing a condition called valvularstenosis
(ste-N-sis; stenos, narrow). The result-ing clinical disorder is
known as rheumaticheart disease, or RHD. The thickened cuspsstiffen
in a partially closed position, but thevalves do not completely
block the circulation,because the edges of the cusps are rough
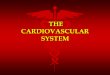
andirregular (Figure A-37). Regurgitation may occur,and much of the
blood pumped out of the heartmay flow right back in. The abnormal
valves arealso much more susceptible to bacterial infection,a type
of endocarditis.
Mitral stenosis and aortic stenosis are themost common forms of
valvular heart disease.About 40 percent of patients with RHD
developmitral stenosis, and two-thirds of them are women.The reason
for the correlation between gender andmitral stenosis is unknown.
In mitral stenosis bloodenters the left ventricle at a slower than
normalrate, and when the ventricle contracts, blood flowsback into
the left atrium as well as into the aortictrunk. As a result, the
left ventricle has to workmuch harder to maintain adequate systemic
circu-lation. The right and left ventricles discharge identi-cal
amounts of blood with each beat, and as theoutput of the left
ventricle declines, blood backsup in the pulmonary circuit. Venous
pressuresthen rise in the pulmonary circuit, and the right
The Cardiovascular System 105
12
Cardio.eap3am 8/21/02 9:36 AM Page 105
-
ventricle must develop greater pressures to forceblood into the
pulmonary trunk. In severe cases ofmitral stenosis, the ventricular
musculature is notup to the task. The heart weakens, and
peripheraltissues begin to suffer from oxygen and
nutrientdeprivation. (This condition, called heart failure,
isdiscussed in more detail in a later section.)
Symptoms of aortic stenosis develop in roughly25 percent of
patients with RHD; 80 percent ofthese individuals are males.
Symptoms of aorticstenosis are initially less severe than those
ofmitral stenosis. Although the left ventricle enlargesand works
harder, normal circulatory function canoften be maintained for
years. Clinical problemsdevelop only when the opening narrows
enough toprevent adequate blood flow. Symptoms thenresemble those
of mitral stenosis.
One reasonably successful treatment for severestenosis involves
the replacement of the damagedvalve with a prosthetic (artificial)
valve. Figure A-37ashows a stenotic heart valve; two possible
replace-ments are a valve from a pig (Figure A-37b) and asynthetic
valve (Figure A-37c), one of a number ofdesigns that have been
employed. Pig valves do notrequire anticoagulant therapy, but may
wear outand begin leaking after roughly 10 years in service.The
plastic or stainless steel components of the arti-ficial valve are
more durable but activate the clottingsystem of the recipient,
leading to inflammation, clotformation, and other potential
complications.Synthetic valve recipients must take
anticoagulantdrugs to prevent strokes and other disorders causedby
embolus formation. Valve replacement operationsare quite
successful, with about 95 percent of thesurgical patients surviving
for 3 years or more and70 percent surviving over 5 years.
Coronary Artery Disease EAP p. 374The term coronary artery
disease (CAD) refers todegenerative changes in the coronary
circulation.Cardiac muscle fibers need a constant supply of
oxygen and nutrients, and any reduction in coro-nary circulation
produces a corresponding reduc-tion in cardiac performance. Such
reducedcirculatory supply, known as coronary ischemia(is-K-m-uh),
usually results from partial or com-plete blockage of the coronary
arteries. The usualcause is the formation of a fatty deposit, or
plaque,in the wall of a coronary vessel. The plaque, or
anassociated thrombus, then narrows the passage-way and reduces
blood flow. Spasms in the smoothmuscles of the vessel wall can
further decreaseblood flow or even stop it altogether. Plaque
devel-opment and growth are considered in Chapter 13.
One of the first symptoms of CAD is often angi-na pectoris
(an-JI-nuh PEK-tor-is; angina, painspasm + pectoris, of the chest).
In the most com-mon form of angina, temporary insufficiency
andischemia develop when the workload of the heartincreases.
Although the individual may feel com-fortable at rest, any unusual
exertion or emotionalstress can produce a sensation of pressure,
chestconstriction, and pain that may radiate from thesternal area
to the arms, back, and neck.
Angina can often be controlled by a combina-tion of drug
treatment and changes in lifestyle.Lifestyle changes to combat
angina include (1) lim-iting activities known to trigger angina
attacks,such as strenuous exercise, and avoiding
stressfulsituations; (2) stopping smoking; and (3) modifyingthe
diet to lower fat consumption. Medications use-ful for controlling
angina include drugs that blocksympathetic stimulation (propranolol
or metoprolol);vasodilators such as nitroglycerin
(n-tr|-GLIS-er-in); and drugs that block calcium movement intothe
cardiac muscle cells (calcium channel blockers).
Angina can also be treated surgically. A single,soft plaque may
be reduced with the aid of a slen-der, elongate catheter
(KATH-e-ter). The catheter, asmall-diameter tube, is inserted into
a large arteryand guided into a coronary artery to the plaque.
Avariety of surgical tools can be slid into thecatheter, and the
plaque can then be removed with
106 The Body Systems: Clinical and Applied Topics
12
(b) (c)(a)
Figure A-37 Artificial Heart Valves
(a) A stenotic semilunar valve; note the irregular, stiff cusps.
(b) Intact BioprostheticTM heart valve,which uses the valve from a
pigs heart. (c) Medtronic HallTM prosthetic heart valve.
Cardio.eap3am 8/21/02 9:36 AM Page 106
-
laser beams or chewed to pieces by a miniature ver-sion of the
Roto-Rooter machine. Debris createdduring plaque destruction is
sucked up by thecatheter, preventing blockage of smaller
vessels.
In balloon angioplasty (AN-j-|-plas-t;angeion, vessel) the
catheter tip contains an inflat-able balloon. Once in position, the
balloon is inflat-ed, pressing the plaque against the vessel
walls.This procedure works best in small (under 10 mm)soft plaques.
Several factors make this a highlyattractive treatment: (1) The
mortality rate duringsurgery is only around 1 percent; (2) the
successrate is over 90 percent; and (3) it can be performedon an
outpatient basis. Although in about 20 per-cent of patients the
plaque deposit returns to itsoriginal size within 6 months, the
process can berepeated as needed.
A coronary artery bypass graft (CABG) involvestaking a small
section from either a small artery(often the internal thoracic
artery) or a peripheral vein(such as the great saphenous vein of
the leg) andusing it to create a detour around the
obstructedportion of a coronary artery. As many as four coro-nary
arteries can be rerouted this way during a sin-gle operation. The
procedures are named accordingto the number of vessels repaired, so
one speaks ofsingle, double, triple, or quadruple coronary
bypassoperations. The mortality rate during surgery foroperations
performed before significant heart damagehas occurred is relatively
low (12 percent). Underthese conditions the procedure completely
eliminatesthe angina symptoms in 70 percent of the cases
andprovides partial relief in another 20 percent.
Although it does offer certain advantages,recent studies have
shown that for mild angina,coronary bypass surgery does not yield
significant-ly better results than drug therapy. Current
recom-mendations are that coronary bypass surgery bereserved for
cases of severe angina that do notrespond to other treatment.
Heart Attacks EAP p. 375
In a myocardial (m-|-KAR-d-al) infarction (MI), orheart attack,
the coronary circulation becomesblocked and the cardiac muscle
cells die from lack ofoxygen. The affected tissue then degenerates,
creat-ing a nonfunctional area known as an infarct. Heartattacks
most often result from severe coronaryartery disease. The
consequences depend on the siteand nature of the circulatory
blockage. If it occursnear the base of one of the coronary
arteries, thedamage will be widespread and the heart will proba-bly
stop beating. If the blockage involves one of thesmaller arterial
branches, the individual may survivethe immediate crisis, but there
are many potentialcomplications, all unpleasant. As scar tissue
formsin the damaged area, the heartbeat may becomeirregular and
other vessels can become constricted,creating additional
circulatory problems.
Myocardial infarctions are most often associat-ed with
pre-existing fixed partial blockages, such as
those seen in CAD. When the crisis developsbecause of complete
blockage by a thrombus (clot)formation at a plaque, the condition
is called coro-nary thrombosis. A vessel already narrowed byplaque
formation may also become blocked by asudden spasm in the smooth
muscles of the vascu-lar wall. The individual then may experience
intensepain, similar to that of an angina attack but persist-ing
even at rest. However, pain does not alwaysaccompany a heart
attack. These silent heartattacks may be even more dangerous,
because thecondition may not be diagnosed and treated beforea fatal
MI occurs. Roughly 25 percent of heartattacks are not recognized
when they occur.
The cytoplasm of a damaged cardiac musclecell differs from that
of a normal muscle cell. Asthe supply of oxygen decreases, the
cells becomemore dependent on anaerobic metabolism to meettheir
energy needs. Over time the cytoplasm accu-mulates large numbers of
enzymes involved withanaerobic energy production.
As the cardiac muscle cell membranes deterio-rate, these enzymes
leak into the surroundingintercellular fluids. The appearance of
suchenzymes in the circulation thus indicates that aninfarct has
occurred. The enzymes tested for in adiagnostic blood test include
lactate dehydroge-nase (LDH), serum glutamic
oxaloacetictransaminase (SGOT, also called aspartate
amino-transferase), creatine phosphokinase (CPK, orCK), and a
special form of creatine phosphokinasefound only in cardiac muscle
(CK-MB).
Roughly 25 percent of MI patients die beforeobtaining medical
assistance, and 65 percent of MIdeaths among those under age 50
occur within anhour after the initial infarct. The goals of
treatmentare to limit the size of the infarct and prevent
addi-tional complications by preventing irregular con-tractions,
improving circulation with vasodilators,providing additional
oxygen, reducing the cardiacworkload, and, if possible, eliminating
the cause ofthe circulatory blockage. Anticoagulants may
helpprevent the formation of additional thrombi, andclot-dissolving
enzymes, such as t-PA, may reducethe extent of the damage if they
are administeredwithin 6 hours after the MI has occurred. Follow-up
treatment with heparin or aspirin or both is rec-ommended; without
further treatment thecirculatory blockages will reappear in roughly
20percent of patients.
A number of factors increase the risk of a heartattack: smoking,
high blood pressure, high bloodcholesterol levels, high circulating
levels of low-density lipoproteins (LDL), diabetes, increasing
age,male gender (below age 70), and obesity. The role
oflipoproteins and cholesterol in plaque formationand heart disease
are considered in Chapter 13.Hereditary factors may also predispose
an individ-ual to coronary artery disease. Although the rate
ofheart attacks of women under age 70 is lower thanthat of men,
their mortality rate is actually high-erperhaps because heart
disease in women is
The Cardiovascular System 107
12
Cardio.eap3am 8/21/02 9:36 AM Page 107
-
neither diagnosed as early nor treated as aggres-sively as is
heart disease in men.
The presence of two risk factors more thandoubles the risk, so
eliminating as many risk fac-tors as possible will improve ones
chances of pre-venting or surviving a heart attack. Changes in
dietto limit cholesterol, exercise to lower weight, notsmoking, and
seeking treatment for high bloodpressure are steps in the right
direction. As publichealth knowledge and education about risk
factorsfor heart disease and treatment for hypertensionand high
cholesterol have improved death rateshave declined. Data from the
CDC shows a drop ofdeath rates from coronary artery disease from
over200 per 100,000 to 134 per 100,000 between 1963and 1996. In
1996, they estimate there were621,000 fewer deaths from CAD than
would havebeen expected had the rates stayed as high.
Diagnosing Abnormal Heartbeats EAP p. 378
Damage to the conduction pathways caused bymechanical
distortion, ischemia, infection, orinflammation can affect the
normal rhythm of theheart. The resulting condition is called a
conduc-tion deficit, or heart block. Heart blocks of vary-ing
severity are illustrated in Figure A-38. In afirst-degree heart
block (Figure A-38b), the AVnode and proximal portion of the AV
bundle slowthe passage of impulses heading for the
ventricularmyocardium. As a result, a pause appears betweenthe
atrial and ventricular contractions. Although adelay exists, the
regular rhythm of the heart con-tinues, and each atrial beat is
followed by a ven-tricular contraction.
If the delay lasts long enough, the nodal cellswill still be
repolarizing from the previous beatwhen the next impulse arrives
from the pacemak-er. The arriving impulse will then be ignored,
theventricles will not be stimulated, and the
normalatria-ventricles, atria-ventricles pattern will dis-appear.
This condition is a second-degree heartblock (Figure A-38c). A mild
second-degree blockmay produce only an occasional skipped beat,
butwith more substantial delays the ventricles willfollow every
second atrial beat. The resulting pat-tern of atria,
atria-ventricles, atria, atria-ventri-cles is known as a two-to-one
(2:1) block.Three-to-one or even four-to-one blocks are
alsoencountered.
In a third-degree heart block, or completeheart block, the
conducting pathway stops func-tioning altogether (Figure A-38d).
The atria andventricles continue to beat, but their activities
areno longer synchronized. The atria follow the paceset by the SA
node, beating 7080 times perminute, and the ventricles follow the
commands ofthe AV node, beating at a rate of 4060 per minute.A
temporary heart block can be induced by stimu-lating the vagus
nerve. In addition to slowing therate of impulse generation by the
SA node, such
stimulation inhibits the AV nodal cells to the pointthat they
cannot respond to normal stimulation.Comments such as my heart
stopped or myheart skipped a beat usually refer to this
phenom-enon. The pause typically lasts for just a few sec-onds.
Longer delays end when a conducting cell,usually one of the
Purkinje fibers, depolarizes tothreshold. This phenomenon is called
ventricularescape because the ventricles are escaping fromthe
control of the SA node. Ventricular escape canbe a lifesaving event
if the conduction system isdamaged. Even without instructions from
the SA orAV nodes, the ventricles will continue to pumpblood at a
slow but steady rate.
Tachycardia and FibrillationAdditional important examples of
arrhythmias areshown in Figure A-39. Premature atrial contrac-tions
(PACs), indicated in Figure A-39b, oftenoccur in normal
individuals. In a PAC the normalatrial rhythm is momentarily
interrupted by a sur-prise atrial contraction. Stress, caffeine,
and vari-ous drugs may increase the frequency of PACincidence,
presumably by increasing the perme-abilities of the SA pacemakers.
The impulse
108 The Body Systems: Clinical and Applied Topics
12
P T P
SQ QS
R
T
R
(a) Normal
2:1 Block (ventricles follow every other atrial beat)
3:1 Block(ventricles follow every third atrial beat)
(c) Second-degree blocks
(d) Complete block (third-degree block) (atrial beats occur
regularly, ventricular beats occur at slower, unrelated pace)
(b) First-degree heart block (long P-R interval)
P P
R R
T T
QS QS
Skipped ventricular beat
P P P
1 2 1 2
1 2 3 1 2 3
p p p p p p p
Figure A-38 Heart Blocks (ECG tracings)
Cardio.eap3am 8/21/02 9:36 AM Page 108
-
The Cardiovascular System 109
12
(a) Normal
(b) Premature atrial contraction (PAC)
(c) Paroxysmal atrial tachycardia (PAT)
(d) Atrial fibrillation
(g) Ventricular fibrillation (VF)
(f) Ventricular tachycardia (VT)
(e) Premature ventricular contraction (PVC)
Q S Q S
P PT T
R R
P P P
P P P P P
P PT T
P
Figure A-39 Cardiac Arrhythmias (ECG tracings)
spreads along the conduction pathway, and a nor-mal ventricular
contraction follows the atrial beat.
In paroxysmal atrial tachycardia (par-ok-SIZ-mal), or PAT
(Figure A-39c), a premature atrialcontraction triggers a flurry of
atrial activity. Theventricles are still able to keep pace, and the
heartrate jumps to about 180 beats per minute. In atrialflutter the
atria are contracting in a coordinatedmanner, but the contractions
are occurring veryfrequently. During a bout of atrial fibrillation
(fi-bri-L-shun), Figure A-39d, the impulses are mov-ing over the
atrial surface at rates of perhaps 500beats per minute. The atrial
wall quivers instead ofproducing an organized contraction. The
ventricu-lar rate in atrial flutter or atrial fibrillation
cannotfollow the atrial rate, and may remain within nor-mal limits.
Despite the fact that the atria are nowessentially nonfunctional,
the condition may gounnoticed, especially in older individuals
leadingsedentary lives. PACs, PAT, atrial flutter, and evenatrial
fibrillation are not considered very dangerousunless they are
prolonged or associated with some
more serious indications of cardiac damage, suchas coronary
artery disease or valve problems.
In contrast, ventricular arrhythmias may beserious and even
fatal. Because the conductionsystem functions in one direction
only, a ventricu-lar arrhythmia is not linked to atrial
activities.Premature ventricular contractions (PVCs;Figure A-39e)
occur when a Purkinje cell or ven-tricular myocardial cell
depolarizes to thresholdand triggers a premature contraction. The
cellresponsible is called an ectopic pacemaker. The fre-quency of
PVCs can be increased by exposure toepinephrine and other
stimulatory drugs or toionic changes that depolarize cardiac muscle
fibermembranes. Similar factors may be responsible forperiods of
ventricular tachycardia, also known asVT, or V-tach (Figure
A-39f).
Multiple PVCs and VT often precede the mostserious type of
arrhythmia, ventricular fibrilla-tion (VF; Figure A-39g). The
resulting condition,known as cardiac arrest, is rapidly fatal
becausethe heart quivers and stops pumping blood.During ventricular
fibrillation, cardiac musclefibers are overly sensitive to
stimulation and theimpulses are traveling from cell to cell around
andaround the ventricular walls. A normal rhythmcannot become
established, because the ventricu-lar muscle fibers are stimulating
one another at arapid rate. The problem is exaggerated by a
sus-tained rise in free intracellular calcium ion concen-trations,
due to massive stimulation of alpha andbeta receptors following
sympathetic activation.
A defibrillator is a device that attempts toeliminate
ventricular fibrillation and restore nor-mal cardiac rhythm. Two
electrodes are placed incontact with the chest, and a powerful
electricalshock is administered. The electrical stimulusdepolarizes
the entire myocardium simultaneously.With luck, after
repolarization the SA node will bethe first area of the heart to
reach threshold. Thusthe primary goal of defibrillation is not just
to stopthe fibrillation, but to give the ventricles a chanceto
respond to normal SA commands. Early defibril-lation can result in
dramatic recovery of an uncon-scious cardiac arrest victim.
In treating arrhythmias there are several med-ications that can
slow down rapid heart rates, orthe abnormal portions of the
conducting systemcan be destroyed. Pacemakers are used to
acceler-ate slow heart rates. Implantable pacemakers ableto sense
ventricular fibrillation and deliver animmediate defibrillating
shock have been success-ful in preventing sudden death in patients
withprevious episodes of ventricular tachycardia andventricular
fibrillation.
Aneurysms EAP p. 391An aneurysm (AN--rizm) is a bulge in the
weak-ened wall of a blood vessel, usually an artery.This bulge
resembles a bubble in the wall of atire, and like a bad tire, the
affected artery may
Cardio.eap3am 8/21/02 9:36 AM Page 109
-
suffer a catastrophic blowout. The most danger-ous aneurysms are
those involving arteries of thebrain, where they cause strokes, and
of the aorta,where a blowout will cause fatal bleeding in amatter
of seconds.
Aneurysms are most often caused by chronichigh blood pressure,
although any trauma or infec-tion that weakens vessel walls can
lead to ananeurysm. Some aortic aneurysms have beenlinked to
inherited disorders, such as Marfanssyndrome, that have weakened
connective tissuesin vessel walls. It is not known whether
othergenetic factors are involved in the development ofother
aneurysms.
An aneurysm usually forms gradually, as ves-sel walls become
less elastic. When a weak pointdevelops, the arterial pressures
distort the wall,creating an aneurysm. Unfortunately, because
theyare often painless, they are likely to go undetected.
When aneurysms are detected by ultrasound orother scanning
procedures, the risk of rupture cansometimes be estimated on the
basis of their size.For example, an aortic aneurysm larger than 6
cmhas a 50:50 chance of rupturing in the next 10years. Treatment
often begins with the reduction ofblood pressure by means of
vasodilators or beta-blockers (drugs that decrease heart rate and
forceof concentration). An aneurysm in an accessiblearea, such as
the abdomen, may be surgicallyremoved and the vessel repaired.
Figure A-40shows a large aortic aneurysm before and aftersurgical
repair with a synthetic patch.
Arteriosclerosis EAP p. 393Arteriosclerosis
(ar-t-r-|-skle-R-sis) is a thick-ening and toughening of arterial
walls. Althoughthis condition may not sound life-threatening,
com-plications related to arteriosclerosis account forroughly
one-half of all deaths in the United States.There are many
different forms of arteriosclerosis;for example, arteriosclerosis
of coronary vessels isresponsible for coronary artery disease
(CAD), andarteriosclerosis of arteries supplying the brain canlead
to strokes.
There are two major forms of arteriosclerosis:
Focal calcification is the gradual degenerationof smooth muscle
in the tunica media and thesubsequent deposition of calcium salts.
Thisprocess typically involves arteries of the limbs.Some focal
calcification occurs as part of theaging process, and it may
develop in associa-tion with atherosclerosis. Rapid and severe
cal-cification may occur as a complication ofdiabetes mellitus, an
endocrine disorder con-sidered in Chapter 10.
Atherosclerosis (ath-er-|-skle-R-sis) is asso-ciated with damage
to the endothelial liningand the formation of lipid deposits in the
tuni-ca media. This is the most common form ofarteriosclerosis.
Many factors may be involved in the develop-ment of
atherosclerosis. One major factor is lipidlevels in the blood.
Atherosclerosis tends to develop
110 The Body Systems: Clinical and Applied Topics
13
Aorta
Clamp
Aneurysm
Left atrium
Intercostalarteries
Intercostalarteries
(sewn up)
Scissors
ClampStep 1
Arteriofemoralbypass
Step 2Step 3
Sutures
Prosthesis
Step 4Step 5
Figure A-40 Repair ofan Aneurysm
Cardio.eap3am 8/21/02 9:36 AM Page 110
-
The Cardiovascular System 111
13
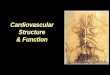
FIGURE A-41 A Plaque Blocking a Peripheral Artery
(a) A section of a coronary artery narrowed by plaque
forma-tion. (b) Sectional view of a large plaque. (LM 18)
Plaque deposit in vessel wall(a) (b)
in persons whose blood contains elevated levels ofplasma lipids,
specifically cholesterol. Circulatingcholesterol is transported to
peripheral tissues inlipoproteins, protein-lipid complexes. (The
varioustypes of lipoproteins and their interrelationshipsare
discussed in Chapter 17.) Recent evidenceindicates that many forms
of atherosclerosis areassociated with either (1) low levels of
apolipopro-tein-E (ApoE), a transport protein whose lipids
arequickly removed by peripheral tissues, or (2) highlevels of
lipo-protein(a), a low-density lipoprotein(LDL) that is removed at
a much slower rate.
When ApoE levels are low, or lipoprotein(a) lev-els are high,
cholesterol-rich lipoproteins remain incirculation for an extended
period. Circulatingmonocytes then begin removing them from
thebloodstream. Eventually the monocytes becomefilled with lipid
droplets. Now called foam cells,they attach themselves to the
endothelial walls ofblood vessels, where they release growth
factors.These cytokines stimulate the divisions of smoothmuscle
fibers near the tunica interna, thickeningthe vessel wall.
Other monocytes then invade the area, migrat-ing between the
endothelial cells. As these changesoccur, the monocytes, smooth
muscle fibers, andendothelial cells begin phagocytizing lipids as
well.The result is a plaque, a fatty mass of tissue thatprojects
into the lumen of the vessel. At this pointthe plaque has a
relatively simple structure, andthere is evidence that the process
can be reversedif appropriate dietary adjustments are made.
If the conditions persist, the endothelial cellsbecome swollen
with lipids, and gaps appear in theendothelial lining. Platelets
now begin sticking tothe exposed collagen fibers, and the
combinationof platelet adhesion and aggregation leads to
theformation of a localized blood clot that will furtherrestrict
blood flow through the artery. The struc-ture of the plaque is now
relatively complex.Plaque growth may be halted, but the
structuralchanges are usually permanent.
Typical plaques can be seen in Figure A-41.Elderly individuals,
especially elderly men, are
most likely to develop atherosclerotic plaques.There is evidence
that estrogens may slow plaqueformation; this may account for the
lower inci-dence of coronary artery disease, myocardialinfarctions
(MIs), and strokes in younger women.After menopause, when estrogen
productiondeclines, the risk of CAD, MIs, and strokes inwomen
increases markedly.
In addition to advanced age and male sex, otherimportant risk
factors include high blood cholesterollevels, high blood pressure,
and cigarette smoking.Roughly 20 percent of middle-aged men have
allthree of these risk factors; these individuals are fourtimes
more likely to experience an MI or cardiacarrest than are other men
in their age group.Although fewer women develop this condition,
elder-ly women smokers with high blood cholesterol andhigh blood
pressure are at much greater risk thanother women. Other factors
that promote develop-ment of atherosclerosis in both men and
womeninclude diabetes mellitus, obesity, and stress. Thereis also
evidence that at least some forms of athero-sclerosis may be linked
to chronic infection withChlamydia pneumoniae, a bacterium
responsible forseveral types of respiratory infections,
includingsome forms of pneumonia.
Potential treatments for atherosclerotic plaques,such as
catheterization, balloon angioplasty and stents, and bypass
surgery, were discussed onp. 106. In cases where dietary
modifications do notlower circulating LDL levels sufficiently,
there aredrug therapies that can bring them under control.Genetic
engineering techniques have recently beenused to treat an inherited
form of hypercholes-terolemia (high blood cholesterol) linked to
exten-sive plaque formation. (The patients were unableto absorb and
recycle cholesterol in the liver.) Inthis experimental procedure,
circulating choles-terol levels declined after copies of
appropriategenes were inserted into some of the individualsliver
cells.
Without question, the best approach to athero-sclerosis is to
try to avoid it by eliminating orreducing associated risk factors.
Suggestionsinclude: (1) reducing the amount of dietary choles-terol
and saturated fats by restricting consumptionof fatty meats (such
as beef, lamb, and pork), eggyolks, and cream; (2) giving up
smoking (or neverstarting to begin with); (3) checking your
bloodpressure and taking steps to lower it if necessary;(4) having
your blood cholesterol levels checked atannual physical
examinations; (5) controlling yourweight; and (6) exercising
regularly.
Problems with Venous ValveFunction EAP p. 394
Chapter 4 of the text notes that one of the conse-quences of
aging is a loss of elasticity andresilience in connective tissues
throughout thebody. Blood vessels are no exception, and with agethe
walls of veins begin to sag. This change usually
Cardio.eap3am 8/21/02 9:36 AM Page 111
-
affects the superficial veins of the legs first,because at these
locations gravity opposes bloodflow. The situation is aggravated by
a lack of exer-cise or an occupation requiring long hours stand-ing
or sitting. Because there is no muscularactivity to help keep the
blood moving, venousblood pools on the proximal (heart) side of
eachvalve. As the venous walls are distorted, the valvesbecome less
effective, and gravity can then pullblood back toward the
capillaries. This furtherimpedes normal blood flow, and the veins
becomegrossly distended. These sagging, swollen vesselsare called
varicose (VAR-i-k|s) veins. Varicoseveins are relatively harmless
but unsightly; surgi-cal procedures are sometimes used to remove
orconstrict the offending vessels.
Varicose veins are not limited to the extremi-ties, and another
common site involves a networkof veins in the walls of the anus.
Pressures withinthe abdominopelvic cavity rise dramatically whenthe
abdominal muscles are tensed. Straining toforce defecation can
force blood into these veins,and repeated incidents leave them
permanentlydistended. These distended veins, known as hem-orrhoids
(HEM-|-roydz), can be uncomfortable andin severe cases extremely
painful.
Hemorrhoids are often associated with preg-nancy, due to changes
in circulation and abdomi-nal pressures. Minor cases can be treated
by thetopical application of drugs that promote contrac-tion of
smooth muscles within the venous walls.More severe cases may
require the surgical removalor destruction of the distended
veins.
Hypertension and HypotensionEAP p. 395
Elevated blood pressure is considered primaryhypertension, or
essential hypertension, if noobvious cause can be determined. Known
risk fac-tors include a hereditary history of hypertension,sex
(males are at higher risk), high plasma choles-terol, obesity,
chronic stresses, and cigarette smok-ing. Secondary hypertension
appears as theresult of abnormal hormonal production outsidethe
cardiovascular system. For example, a condi-tion resulting in
excessive production of antidiuret-ic hormone (ADH), renin,
aldosterone, orepinephrine will probably produce hypertension,and
many forms of kidney disease will lead tohypertension caused by
fluid retention or excessiverenin production.
Hypertension significantly increases the workload on the heart,
and the left ventricle graduallyenlarges. More muscle mass requires
a greater oxy-gen demand, and when the coronary circulationcannot
keep pace, symptoms of coronary ischemiaappear.
Increased arterial pressures also place a physi-cal stress on
the walls of blood vessels throughoutthe body. This stress promotes
or accelerates thedevelopment of arteriosclerosis and increases
the
risks of aneurysms, heart attacks, and strokes.Vessels supplying
the retinas of the eyes are oftenaffected, and hemorrhages and
associated circula-tory changes can produce disturbances in
vision.Because these vessels are examined in a normalphysical exam,
retinal changes may provide thefirst evidence that hypertension is
affecting periph-eral circulation.
One of the most difficult aspects of hyperten-sion is that there
are usually no obvious symp-toms. As a result, clinical problems do
not appearuntil the condition has reached the crisis stage.There
is, therefore, considerable interest in earlydetection and prompt
treatment of hypertension.
Treatment consists of a combination of life-stylechanges and
physiological therapies. Quittingsmoking, getting regular exercise,
and restrictingdietary intake of salt, fats, and calories will
improveperipheral circulation, prevent increases in bloodvolume and
total body weight, and reduce plasmacholesterol levels. These
strategies may be sufficientto control hypertension if it has been
detectedbefore significant cardiovascular damage hasoccurred.
Therapies usually involve antihyperten-sive drugs, such as calcium
channel blockers, beta-blockers, diuretics, and vasodilators,
singly or incombination. Beta-blockers eliminate the effects
ofsympathetic stimulation on the heart, and theunopposed
parasympathetic system lowers the rest-ing heart rate and blood
pressure. Diuretics pro-mote the loss of water and sodium ions at
thekidneys, lowering blood volume, and vasodilatorsfurther reduce
blood pressure. A new class of anti-hypertensive drugs lowers blood
pressure by pre-venting the production of angiotensin II.
Theseangiotensin-converting enzyme (ACE) inhibitors,such as
captopril, are being used to treat chronichypertension and
congestive heart failure.
In hypotension, blood pressure declines, andperipheral systems
begin to suffer from oxygen andnutrient deprivation. One clinically
important formof hypotension can develop following the
administra-tion of antihypertensive drugs. Problems may appearwhen
the individual changes position, going fromlying down to sitting,
or sitting to standing. Normallyeach time you sit or stand, blood
pressure in thecarotid sinus drops, for the heart must
suddenlycounteract gravity to push blood up to the brain.The fall
in pressure triggers the carotid reflex, andblood pressure returns
to normal. But if the carotidresponse is blunted by beta-blockers
or other drugs,blood pressure at the brain may fall so low that
theindividual becomes weak, dizzy, disoriented, orunconscious. This
condition is known as orthostat-ic hypotension (|r-tho-STAT-ik;
orthos, straight +statikos, causing to stand), or simply
orthostasis(|r-th|-ST-sis). Most readers will have experiencedbrief
episodes of orthostasis when standing up sud-denly after reclining
for an extended period. Thecarotid reflex frequently slows with
age, and olderpeople learn to sit and stand more carefully to
avoidthe effects of orthostatic hypotension.
112 The Body Systems: Clinical and Applied Topics
13
Cardio.eap3am 8/21/02 9:36 AM Page 112
-
The Cardiovascular System 113
13
Shock EAP p. 404Shock is an acute circulatory crisis marked by
lowblood pressure (hypotension) and inadequateperipheral blood
flow. Severe and potentially fatalsymptoms develop as vital tissues
become starvedfor oxygen and nutrients. Common causes of shockare
(1) a fall in cardiac output after hemorrhaging orother fluid
losses, (2) damage to the heart, (3) exter-nal pressure on the
heart, and (4) extensive periph-eral vasodilation.
CIRCULATORY SHOCK A severe loss of blood vol-ume produces
symptoms of circulatory shock.Symptoms of circulatory shock appear
after fluidlosses of about 30 percent of the total blood vol-ume.
The cause can be hemorrhaging or fluid loss-es to the environment,
as in dehydration or aftersevere burns. All cases of circulatory
shock sharethe same basic symptoms:
1. Hypotension, with systolic pressures below 90mm Hg.
2. Pale, cool, and moist (clammy) skin. The skinis pale and cool
because of peripheral vasocon-striction; the moisture reflects
sympatheticactivation of the sweat glands.
3. Frequent confusion and disorientation, due toa fall in blood
pressure at the brain.
4. Rapid, weak pulse.
5. No urination, because the reduced blood flowto the kidneys
slows or stops urine production.
6. A drop in blood pH (acidosis), due to lactic acidgeneration
in oxygen-deprived tissues.
Circulatory shock is often divided into compen-sated,
progressive, and irreversible stages.
THE COMPENSATED STAGE (STAGE I) Duringthe compensated stage
homeostatic adjustmentscan cope with the situation; the short-term
andlong-term responses detailed in Figure A-42 arepart of the
compensation process. During the peri-od of compensation,
peripheral blood flow isreduced but remains within tolerable
limits.
THE PROGRESSIVE STAGE (STAGE II) Whenblood volume declines by
more than 35 percent, theindividual enters the progressive stage of
circulatoryshock. Homeostatic mechanisms are now unable tocope with
the situation. Despite sustained vasocon-striction and the
mobilization of the venous reserve,blood pressure remains
abnormally low, venousreturn is reduced, and cardiac output is
inadequate.A vicious cycle begins when the low cardiac outputcauses
myocardial damage. This damage leads to afurther reduction in
cardiac output and subsequentreductions in blood pressure and
venous return. Thesequence is diagrammed in Figure A-42a.
When the mean arterial blood pressure falls toabout 50 mm Hg,
carotid sinus baroreceptors trigger
a massive activation of the vasomotor centers. Inessence, the
goal now is to preserve the circulationto the brain at any cost.
Blood flow to cerebral ves-sels is not affected, and the blood
pressure in thecarotid arteries remains relatively high (70 mm
Hg).But in other organs sympathetic output causes asustained and
maximal vasoconstriction. This reflex,called the central ischemic
response, reducesperipheral circulation to an absolute minimum.
The central ischemic response is a last-ditcheffort that
maintains adequate blood flow to thebrain at the expense of other
tissues. Unlessprompt treatment is provided, the condition willsoon
prove fatal. Treatment must concentrate on(1) preventing further
fluid losses and (2) giving atransfusion of whole blood, plasma
expanders, orblood substitutes.
THE IRREVERSIBLE STAGE (STAGE III) In theabsence of treatment,
progressive shock will soonturn into irreversible shock (Figure
A-42b). At thispoint, conditions in the heart, liver, kidneys,
andCNS are rapidly deteriorating to the point thatdeath will occur,
even with medical treatment.
Irreversible shock begins when conditions in thetissues become
so abnormal that the arteriolarsmooth muscles and precapillary
sphinctersbecome unable to contract, despite the commandsof the
vasomotor center. The result is a widespreadperipheral vasodilation
and an immediate and fataldecline in blood pressure. This event is
called circu-latory collapse. The blood pressure in many tis-sues
then falls so low that the capillaries collapselike deflating
balloons. Blood flow through thesecapillary beds then stops
completely, and the cellsin the affected tissues die. The dying
cells releasemore abnormal chemicals, and the effect quicklyspreads
throughout the body.
Other Types of Shock EAP p. 404
Although the text focuses on circulatory shockcaused by low
blood volume, shock can developwhen the blood volume is normal.
Cardiogenic(kar-d-|-JEN-ik) shock occurs when the heartbecomes
unable to maintain a normal cardiac out-put. The most common cause
is failure of the leftventricle as a result of a myocardial
infarction.Between 5 and 10 percent of patients surviving aheart
attack must be treated for cardiogenic shock.The use of
thrombolytic drugs, such as t-PA andstreptokinase, can be very
effective in restoringcoronary circulation and ventricular
function,thereby relieving the peripheral symptoms.Cardiogenic
shock may also be the result ofarrhythmias, valvular heart disease,
advancedcoronary artery disease, cardiomyopathy, or ven-tricular
arrhythmias (see p. 109).
In obstructive shock, ventricular output isreduced because
tissues or fluids are restrictingthe expansion and contraction of
the heart. Forexample, fluid buildup in the pericardial cavity
Cardio.eap3am 8/22/02 11:05 AM Page 113
-
(cardiac tamponade) due to infection or trauma cancompress the
heart and limit ventricular filling.
Distributive shock results from a widespread,uncontrolled
vasodilation. This produces a dramat-ic fall in blood pressure that
leads to a reduction inblood flow and the onset of shock. Three
importantexamples are neurogenic shock, septic shock,
andanaphylactic shock.
Neurogenic (noo-r|-JEN-ik) shock can becaused by general or
spinal anesthesia and bytrauma or inflammation of the brain stem.
Theunderlying problem is damage to the vasomotorcenter or to the
sympathetic tracts or nerves, lead-ing to a loss of vasomotor
tone.
Septic shock results from the massive releaseof endotoxins,
poisons derived from the cell wallsof bacteria during a systemic
infection. These com-pounds cause a vasodilation of
precapillarysphincters throughout the body, resulting in a
drop in peripheral resistance and a decline inblood pressure.
Symptoms of septic shock general-ly resemble those of other types
of shock, but theskin is flushed and the individual may have a
highfever. For this reason septic shock is also knownas warm shock.
One interesting example of sep-tic shock, called toxic shock
syndrome (TSS),results from an infection by the
bacteriumStaphylococcus aureus. This disease was unrecog-nized
before 1978, when it appeared in a group ofchildren. Since that
time there have been morecases in the United States, most (95
percent)affecting women. Although other sources of infec-tion are
possible, infection most often appears tooccur during menstruation,
and the chances ofinfection are increased with the use of
superab-sorbent tampons. (The brands involved have beentaken off
the market, and the incidence hasdeclined steadily since 1980.)
114 The Body Systems: Clinical and Applied Topics
13
Severe reductionof blood volume
Decreasedcardiacoutput
Decreasedarterial
pressure
Decreasedperipheralblood flow
Tissueoxygen
starvation
Increased lacticacid
Decreased pHIncreased PCO2
Clottingwithin
vessels
Decreasedvenousreturn Decreased
cardiacblood flow
Damageto heartmuscle
POSITIVE FEEDBACKLOOP 2
POSITIVEFEEDBACK
LOOP 3
POSITIVEFEEDBACK
LOOP 1
HOMEOSTATICFAILURES
Increasedcapillary
permeability
Sympatheticactivation and
central ischemicresponse
If BP falls below50 mm Hg
If damage reachescritical levels
(a) Progessive shock
FIGURE A-42 Shock
(a) The progressive stage is characterized by a gradualdecline
in systemic blood pressure, tissue blood flow,and cardiac output.
(b) The irreversible stage involvesa series of integrated chain
reactions leading to arapid decline in cardiac output, a dramatic
and irre-versible fall in blood pressure,circulatory collapse, and
even-tual death.
Cardio.eap3am 8/21/02 9:36 AM Page 114
-
The Cardiovascular System 115
13
tricular muscle (see the discussion of myocardialinfarctions on
p. 107) or high arterial pressures(hypertension, p. 112). In
effect, the left ventriclecan no longer keep pace with the right
ventricle,and blood backs up into the pulmonary circuit.This venous
congestion is responsible for the termcongestive heart failure. The
right ventricle nowneeds to works harder, elevating pulmonary
arteri-al pressures and forcing blood through the lungsand into the
weakened left ventricle.
At the capillaries of the lungs, arterial andvenous pressures
are now elevated. This elevatedpressure pushes additional fluid out
of the capillariesand into the interstitial fluids. The fluid
buildup andcompression of the airways reduces the effectivenessof
gas exchange, leading to shortness of breath, oftenthe first
obvious sign of congestive failure. This fluidbuildup begins at a
postcapillary pressure of around25 mm Hg. At a capillary pressure
of around 30 mmHg, fluid not only enters the tissues of the lungs
butcrosses the alveolar walls and begins filling the air-spaces.
This condition is called pulmonary edema.
Over time, the less muscular right ventriclemay become unable to
generate enough pressure toforce blood through the pulmonary
circuit. Venouscongestion now occurs in the systemic circuit,
andcardiac output declines further. When the reduc-tion in systemic
pressures lowers blood flow to thekidneys, renin and erythropoietin
are released.This in turn elevates blood volume, due toincreased
salt and water retention at the kidneys,and accelerated red blood
cell production. This risein blood volume actually complicates the
situation,as it tends to increase venous congestion andcause
widespread edema.
The increased volume of blood in the venoussystem leads to a
distension of the veins, makingsuperficial veins more prominent.
When the heartcontracts, the rise in pressure at the right
atriumproduces a pressure pulse in the large veins. Thisvenous
pulse can be seen and palpated most easilyover the right external
jugular vein.
Treatment of congestive heart failure oftenincludes:
Restriction of salt intake. The expression waterfollows salt
applies here, because when sodi-um and chloride ions are absorbed
acros