Embed Size (px)
DESCRIPTION
x
Citation preview

9E.A. Gabriel and T. Salerno (eds.), Principles of Pulmonary Protection in Heart Surgery, DOI: 10.1007/978-1-84996-308-4_2, © Springer-Verlag London Limited 2010
2.1 Introduction
Organic evolution has been essentially linked to oxygen (O
2) since it was first introduced in the earth’s atmo-
sphere by photosynthesis of early cyanobacteria species some 2.5 billion years ago. In the steady state (i.e., nor-moxia), most of the oxygen consumed by a cell is used by mitochondria in the generation of adenosine triphos-phate (ATP) via oxidative phos phorylation, providing eukaryotic cells with a highly sophisticated survival advantage. Whereas a total of 38 molecules of ATP are generated per molecule of glucose via oxidative phos-phorylation, only 2 are produced via anaerobic metabo-lism. In fact, more than 90% of the oxygen consumption of the body is used for oxidative phosphorylation. Thus, since the chemical reduction of molecular oxygen is the primary source of metabolic energy for most eukaryotic cells, a constant oxygen supply is critical for continued cell function and survival.
Therefore, it is not surprising that dysoxia (i.e., inade-quate supply of tissue oxygenation at levels impairing mitochondrial respiration)1 and oxygen debt are major factors in the development and propagation of multiple-organ failures, especially in critically ill patients. Dysoxia is the result of an abnormal relationship between O
2 sup-
ply and O2 demand. In mammals, the function of the
lungs, heart, and vasculature must ensure a continuous and adequate supply of oxygen and nutrients to the tis-sues to maintain cellular integrity and function.
The respiratory system allows gases to transfer by convective and diffusive processes between the atmo-spheric air and the blood. Furthermore, it also plays a central role in the maintenance of the acid–base bal-ance and is related to other functions associated with the immune system and metabolism. This chapter focuses on the respiratory mechanisms that avoid tis-sue hypoxia by means of the analysis of the determi-nants of lung function.
2.2 Oxygen Delivery
The most important function of the respiratory and cir-culatory systems is the supply of oxygen to the cells of the body in adequate quantity and at satisfactory par-tial pressure.2 On the one hand, the respiratory system allows appropriate partial oxygen pressure for the dif-fusion of gases through the alveolar-capillary barrier. On the other hand, the cardiovascular system favors an appropriate sanguineous flow to optimize the delivery, at the tissue level, of the oxygen already incorporated into the blood. The oxygen delivery ( )
2OD expresses
this joint function of both systems. The quantity of oxygen made available to the body in 1 min is the product of the cardiac output (CO) and the arterial oxygen content ( )2CaO :
2 2( )O O = CO * Ca ( / min)*10D l dl (2.1)
Under normal physiological conditions, the amount of oxygen delivered to the tissues is approximately 1,000 mL/min. Anaerobic metabolism occurs when
2OD falls below about 3.03 ± 1.08 mL/kg/min (dysoxia), when oxygen demands exceed oxygen supply and
Respiratory Physiology
Jesús Armando Sánchez-Godoy
J.A. Sánchez-Godoy Departamento de Ciencias Fisiológicas, Pontificia Universidad Javeriana, Universidad Militar “Nueva Granada”, Bogotá D.C., Colombia e-mail: [email protected]
2

10 J.A. Sánchez-Godoy
tissue extraction to meet that need (e.g., beyond
2O maxV with severe exercise), or when the mitochon-dria are unable to utilize the oxygen. The essential feature of hypoxia is the cessation of oxidative phos-phorylation when the mitochondrial Po
2 falls below a
critical level. That is, hypoxia occurs when there is a reduction of 2OD due to hypoxemia (i.e., a reduced amount of oxygen being carried in the blood), to a restriction of the blood supply to the tissues, or to both.
Oxygen is carried by the blood in two forms: as solu-tion (i.e., dissolved in the plasma) and as oxyhemoglo-bin. The quantity of hemoglobin (Hb) in solution in plasma at 37°C is defined by the capacitance coefficient, which is approximately 0.003 mL O
2/dL
blood × mmHg.
The amount of oxygen that can be transported into the blood can be expressed by the equation describing 2CaO:
(2.2)
where 1.39 (Huffner’s constant) is the amount of O2
(mL) carried per gram of Hb at sea level. Therefore,
2CaO could be impaired by a decrease in the Hb con-centration or in the arterial oxygen pressure (
2OPa ).The function of the lung and its control system
allows the maintenance of 2CaO and avoids the hypoxia throughout four processes:
The generation of a pressure gradient between the •alveolar space and either the mouth or the airway opening, transairway pressure3 to maintain an ade-quate alveolar oxygen pressure (
2OPA ) and alveo-lar pressure of carbon dioxide (
2COPA ) by the cyclic ventilation of alveolar gas with atmospheric air.Gas exchange across the blood–air barrier. This •requires a large, thin, moist exchange surface; a pump to move air; and a circulatory system to transport gases to the cells.Perfusion as the process by which deoxygenated •blood passes through the lung and becomes reoxy-genated, given an appropriate ventilation–perfusion ratio AV Q .1
The maintenance of a control system that allows •permanent “sensing” of specific chemical and
physical conditions of the blood, especially gas pressures and acid–base status, which must follow the actual requirements of the body.
2.3 Pulmonary Ventilation
Ventilation is the process by which fresh gas moves in and out of the lung. Minute ventilation ( )VE or total is the volume of air that enters or leaves the lung per minute and can be expressed by the equation
(2.3)
where f is the number of breaths per minute, and TV is the tidal volume or volume of air inspired (or exhaled) with each breath. Tidal volume varies with age, gender, body position, and metabolic activity. In an average-size adult, TV is 500 mL (6–7 mL/kg). In children, the tidal volume is 3–5 mL/kg.5 The initial portion of the tidal volume is directed into the alveoli to effect gas exchange. However, the last portion remains in the air-way conducts and is commonly referred to as anatomi-cal dead space ( ( )D anatV ). Therefore, the volume that enters the alveoli per breath AV is
(2.4)
and the alveolar ventilation can be expressed as
(2.5)
or
(2.6)
Thus, the alveolar ventilation depends on the breath-ing pattern and the volume of dead space. This dead space is called anatomic dead space because it repre-sents the wasted ventilation of the airways that do not participate in gas exchange. The total volume of gas in each breath not participating in gas exchange is called the physiological dead space ( )D physiolV . Normally,
( )D physiolV is approximately equal to ( )D anatV and accounts for 25–30% of the TV . It includes two separate com-ponents: (1) the anatomical dead space and (2) the dead space secondary to ventilated, but not perfused, alveoli or alveoli overventilated relative to the amount of perfusion. The physiological dead space may be determined by de Bohr’s equation:
(2.7)
2
2
2 ( ) 2
2.
[1.39( ) ]
[ ( ) 0.0031( )]
= ´ ´ +
´
mlO gg dlO Hb
mlOmmHg dl mmHgO
Ca Hb SaO
Pa
VE f VT= �
( )= -A T D anatV V V
( )´= - ´A T D anatV V f V f
= [ ]A T DV f V V-
2
2
2( ) ( )-=
ED CO COphysiol
T CO
Pa PVV Pa
1The special symbols in respiratory physiology compiled by Pappenheimer et al.4 are used throughout this chapter.

112 Respiratory Physiology
where 2COPE is the mixed expired
2COP . It is assumed that the
2COP of the exchanging (i.e., perfused) alveoli equals the
2COP of the arterial blood. As a consequence, a decrease in ventilation out of proportion to any decrease in metabolic
2COV (amount of CO2 evolved
from the body each minute) results in a high arterial
2COP . Hence, increase in dead space is a cause of hypercarbia.
At any given rate of metabolic CO2 production, the
steady-state value for 2COPA is therefore inversely related,
in a hyperbolic fashion, to the rate of alveolar ventila-tion. The determinants of VA were expressed in (2.6).
2.3.1 Lung Volumes
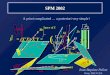
The amount of gas in the lungs at different levels of inflation is represented as volumes (when they are single components) and capacities (when they are composed of two or more components). The balances between the elastic recoil properties of the lung and the properties of the chest wall and its muscles determine lung volumes. All lung volumes are subdivisions of the total lung capacity (TLC), and they are measured in liters. The static volumes of the lungs are shown in Fig. 2.1.6
The functional residual capacity (FRC) is the rest-ing volume of the lung. It is determined by the balance
between the lung elastic recoil pressure, which oper-ates to decrease the lung volume, and the pressure gen-erated by the chest wall to become larger. At FRC, the pressure difference across the respiratory system is zero, and it is approximately 50–60% of TLC (see the forces shown in Fig. 2.2 at resting volume). The inter-action between elastic recoil forces of the chest wall, which pull the chest wall outward, and the elastic recoil forces of lung, which pull inward, creates a negative pressure in the intrapleural space with respect to atmo-spheric pressure (see section 2.3.2).
Vital capacity, tidal volume, inspiratory reserve, and expiratory reserve can all be measured with a simple spirometer. Total lung capacity, FRC, and residual vol-ume (RV) all contain a fraction that cannot be measured by simple spirometry. However, RV and TLC can be measured using other methods: body plethysmogra-phy,6,8,9 nitrogen washout,10 or helium dilution11 or using imaging techniques.12 The methods more commonly used are nitrogen (N
2) washout (in its modern form, an
open-circuit method) and helium (He) dilution (a closed-circuit method). The former method uses nitrogen wash-out by breathing 100% oxygen. Total quantity of nitrogen eliminated is measured as the product of the expired volume collected and the concentration of nitro-gen. For example, if 4 L of nitrogen are collected and
Volume and capacities1.9-2.50.4-0.51.1-1.51.5-1.94.9-6.42.3-3.02.6-3.43.4-4.5
Typical ranges (liters)
IRV
VC
VT
IC
ERV
TLC
FRC
RV
IRV: Inspiratory reserve volumeVT: Tidal volume
ERV: Expiratory reserve volumeRV: Residual volume
TLC: Total lung capacityIC: Inspiratory capacity
FRC: Functional Residual capacityVC: Vital capacity
Fig. 2.1 Standard lung volumes and capacities. Typical values for a 70-kg adult are shown
100
80
60
40
20
0
−20 −10 0 10 20 30 cm. H2O
PC PL PT
PC = O
FRC
Resting Volume
% V
ITA
L C
APA
CIT
Y
PC = PL
Fig. 2.2 Sitting pressure–volume curve of lung (PL), thoracic
cage (PC), and the result of these two forces, the total respiratory
system (PT). Diagrams on the right side indicate direction and
magnitude of forces for the two elastic systems of the chest at various lung volumes. Dotted arrows indicate lung tensions and solid arrows the thoracic-cage tension. Average vital capacity was 4,730 cm3 ATPS (Ambient temperature, ambient pressure, saturated with water vapor conditions of a volume of gas) at 26°C. Standard errors are indicated by brackets unless smaller than width of the line (From 7 with permission)

12 J.A. Sánchez-Godoy
the initial alveolar concentration was 80%, the estimated initial lung volume is 5 L. The latter method uses wash-in of a tracer gas such as helium (preferred for its low solubility in blood), which can be measured by katha-rometry. For example, if 50 mL of helium are introduced into the lungs and the helium concentration is then found to be 1%, the estimated lung volume is 5 L.
Measurements of lung volumes by radiographic, plethysmographic, gas dilution, or washout techniques produce on average similar results when normal subjects are tested. In contrast, the results of these techniques can differ significantly when ill patients are evaluated.12
2.3.2 Forces Involved in Breathing (Gradient Pressures)
Airflow in any system is directly proportional to the gradients of pressure and inversely related to the resis-tance to airflow, as expressed by Ohm’s law:
(2.8)
where P1 is the circuit initial pressure, P
2 is the pressure
at the end, and R is the flow resistance. In the lung, the pressure gradient of concern is the difference between atmospheric (barometric) and alveolar pressure:
(2.9)
where BP is the barometric pressure, and Palv
is the alveolar pressure. Alternatively, it is described as the pressure gradient between the alveolar space and either the mouth (P
m) or the airway opening (P
oa), the tran-
sairway pressure.3 Raw
represents the airway resistance. If the subject is breathing ambient air, atmospheric pressure (P
atm) does not change. This means that gas
flow in the lungs results from changes in alveolar pres-sure; this is brought about by changes in the dimension of the thorax. Inspirations lead to expansion of the tho-rax, causing a fall in alveolar pressure sustained until the end of inspiration, when alveolar pressure equals atmospheric pressure. During expiration, the inspira-tion muscles relax, and the intrapleural pressure (P
pl)
becomes less negative with respect to the atmospheric pressure. The elastic recoil of the lung then compresses the alveolar gas and raises its pressure above that of the mouth. If P
alv > P
atm, then, air flows out the lung
(Fig. 2.3). During quiet breathing in the supine posi-tion, the process occurs passively without much par-ticipation of the expiratory muscles because the energy required is provided by the elastic recoil of the lungs aided by the weight of the abdominal contents pushing the diaphragm in the cephalad direction. In the upright posture and during stimulated ventilation, the internal intercostal muscles and the abdominal wall muscles are active in returning the rib cage and diaphragm to the resting position.
Barometric pressure (PB): Dalton’s law (also called
Dalton’s law of partial pressures) states that the total pressure exerted by a gaseous mixture is equal to the
1 2-=
P PQ
R
B alv
aw
P P
R
-=Q -1
+1
-0.5
+0.5
0
0
-8
-7
-6
-5
0
0.1
0.2
0.3
0.4
0.5
FRC
A
A
A
C
C
D
D
B
B
Time
Alv
eola
r pr
essu
re(c
m H
2O)
Exp
irato
ry fl
ow(li
ters
/ sec
)P
leur
al p
ress
ure
(cm
H2O
)V
olum
e(li
ters
)
Inspiration Expiration
Fig. 2.3 Volume, pressure, and airflow changes during a single respiratory cycle

132 Respiratory Physiology
sum of the partial pressures of each individual compo-nent in the mixture. This empirical law was observed by John Dalton in 1801 and is related to the ideal gas laws. Thus, the barometric pressure at a given location depends on the weight of the column of atmosphere directly over that point. Hence, places closer to sea level have “higher columns” of air above them and con-sequently greater “atmospheric” or “barometric” pres-sures. The air density and pressure decrease almost linearly with increasing altitude. It should be remem-bered that the atmospheric air is a mixture of gases, mostly nitrogen (78.09%), oxygen (20.95%), and small amounts of other gases. This remains largely unchanged around the globe. In other words, at high altitude the air contains the same percentage of oxygen as at sea level. However, since the air is less dense, a given volume of air contains fewer gas molecules, including oxygen. Thus, the partial pressure of oxygen (Po
2) is lower at
high altitude due to the reduced barometric pressure.Maximal inspiratory (P
I,mo,max, MIP, or P
I,max
) and expiratory pressure (P
E,mo,max, MEP, or P
E,max
) at the mouth. Both of these are simple indexes of ventila-tory or respiratory muscle endurance. They are the most widely used measures of global inspiratory and expiratory muscle strength.13–15 MIP decreases with age independent of gender. However, the decline is larger in men than in women.16 The measurement is the maximal sustained pressure over 1 s, and the result is the maximal value of three measures. The result is compared with standardized values that take into account age, height, gender, and body mass. Typically, an MIP value that does not reach −80 cm H
2O is likely
to be abnormal. Diaphragm contraction force can be estimated from the transdiaphragmatic pressure P
di,
which is the difference between pressure above and below the diaphragm, measured as intragastric and intraesophageal pressure, respectively. Maximal con-traction of the diaphragm is obtained by performing a maximal sniff maneuver or by phrenic nerve stimula-tion. Inspiratory muscle strength is often better reflected by esophageal pressure during a maximal sniff (sniff P
oes). Sniff P
oes is performed from FRC without a nose
clip. In such a case, the volume increases about 500 mL, and diaphragm contraction is therefore relatively iso-metric. The normal mean sniff P
oes is 93 ± 20 cm H
2O,
ranging between 74 and 135 cm H2O.17
Alveolar pressure (Palv
): Boyle’s law describes pres-sure–volume relationships of gases. Thus, in the alveo-lar space the pressure is determined for the size of the
container (i.e., the alveolus). If the size of the container is reduced, the collisions between gas molecules and the walls become more frequent, and the pressure rises (i.e., at expiration, P
alv becomes greater than P
B, and the air
flows out of the lungs). Therefore, the alveolar pressure depends on the alveolar volume, and the alveolar vol-ume is determined by the relationship between forces involved in elastic lung and chest wall recoil. Hence, P
alv
is simply the sum of the intrinsic recoil pressure (Precoil
) of the lung (at that volume) and the applied intrapleural pressure (P
pl). Therefore, to develop a change in P
alv, it is
necessary to adjust the amount of Precoil
, Ppl, or both.
Causes of lung recoil: The lung tends to recoil to a lower volume even after a maximal volitional exhala-tion (i.e., at residual volume). Two basic factors account for this retractive, or recoil, force: elastic recoil and lung surface tension.
1. Elastic recoil18: Elastic and collagen fibers are pres-ent in the alveolar walls and bronchial tree and, when distended, tend to return to equilibrium con-figuration. During inspiration, contraction of respi-ratory muscles stretches the elastic and collagen tissue network of the lungs and pleura, also over-coming the surface tension that is present at the interfaces between the air and alveoli, and the fluid lines alveolar walls. These features constitute an elastic hindrance to inspiration. At most lung vol-umes, the hindrance is mainly due to surface ten-sion, but if lungs are nearly fully distended the recoil of the elastic and collagen fibers contributes as well. The work that is done in stretching the lung is not dissipated as heat. Instead, the energy is stored in the stretched structures and then spent in driving the subsequent expiration. This entails shrinking the lungs back to their previous volume. Hence, normal expiration is affected by the elastic recoil of the lung tissue. The energy applied to the lung in inspiration is not recovered in expiration. The property of dissipating energy is called hyster-esis. Lung hysteresis can be quantified because it applies to the area between the ascending and descending portions of the pressure–volume curve and depends specifically on surface tension as dis-cussed in item 219 (see also Fig. 2.4).
The network of fiber confers stability on the lungs because a local change in volume causes enlargement or shortening of collagen or elastic fibers in the immediate surrounding area. This is defined as interdependence.

14 J.A. Sánchez-Godoy
Interdependence mitigates the effect of local stress. The lung parenchyma, the airways, and the pulmonary and bronchial vascular systems are continuously sub-jected to a wide range of passive and active physical forces as a result of the dynamic nature of lung func-tion. These forces include changes in stress (i.e., force per unit area) or strain (i.e., any forced change in length in relation to the initial length) and shear stress (i.e., the stress component parallel to a given surface).21 The response to stress will be further analyzed in chap-ter number four.
2. Lung surface tension: In 1929, Kurt von Neergaard evacuated air from an isolated porcine lung, which he then filled with an isotonic gum solution to elimi-nate surface tension of the air tissue interfaces. Von Neergaard then obtained pressure–volume measure-ments and constructed curves based on the induced expansion of the lungs with air and liquid. From these experiments, he arrived at two main conclu-sions: (1) Surface tension is responsible for the greater part of total lung recoil compared to tissue elasticity. (2) A lower surface tension would be use-ful for the respiratory mechanism because without it pulmonary retraction might become too great, inter-fering with adequate expansion.22,23 Surface tension is a measure of the force acting to pull a the surface
molecules of a liquid together at an air–liquid inter-face. Alveolar surface tension is similar to that exist-ing in a spherical bubble. The surface tension created by the thin film of fluid is directed toward the center of the bubble and creates pressure in the interior. The law of Laplace is an expression of this pressure.
If the surface tension of the fluid was the same in the small and large alveoli, then small alveoli would have higher inwardly directed pressure than larger alveoli and consequently an increased resistance to stretch. As a result, more work would be needed to expand smaller alveoli. However, a surfactant reduces the surface ten-sion, especially in the smaller alveoli, where higher concentrations are accumulated. Alveolar surfactant is well known for its ability to reduce minimal surface tension at the alveolar air–liquid interface to values below 5 mN/m. Hence, surfactant avoids collapse of the smaller alveoli. For this reason, alveoli with differ-ent diameters would have the same pressure (Fig. 2.5).
2.0
1.5
1.0
0.5
0 -5 -10 -15 -20
Volume (L)
Intraesophageal pressure(cmH20)
Fig. 2.4 The effect of tidal volume on hysteresis. Hysteresis is minimal at low tidal volumes but becomes larger as the tidal
volume increases (From 20, with permission.)
P
P
Law of LaPlace
(pressure) = 2γ (surface tension)
r (radius)
r
r
A B
γ
γ
Fig. 2.5 According to Laplace’s law, the surface tension in alve-oli has to be dynamic. When the airway pressure is similar (pres-sure 1/4P) in alveoli of different sizes (difference in radius 1/4r), the surface tension (g) has to change accordingly. In this dia-gram, the surface tension in alveolus A will be higher than the surface tension in B to maintain alveolar stability. Pulmonary surfactant is able to dynamically reduce the surface tension (From 24, with permission)

152 Respiratory Physiology
Production of surfactant is reduced when the lung parenchyma is damaged by breathing oxygen-enriched air, by severe shock, and by diversion of pulmonary blood flow through an extracorporeal circulation.
The surface tension also occurs in the airways. The airway surfactant existence reduces surface tension at the air–liquid interface of conducting airways.25 This decreases the tendency of airway liquid to form bridges in the narrower airway lumen (film collapse). In addi-tion, a low surface tension minimizes the amount of negative pressure in the airway wall and its adjacent liquid layer, which in turn decreases the tendency for airway wall (compliant) collapse. According to the law of Laplace, it becomes obvious that the smaller the air-ways, the higher the pressure would increase if surface-active material lowering the value of g were absent. Surface tension in the conducting airways has been shown to be in the range between 25 and 30 mN/m.
Pleural (intrapleural) pressure (Ppl) depends on the
elastic and chest wall recoil interaction forces. The recoil of the lung causes it to attempt to retract to its equilibrium volume (effectively that of a gas-free lung). The elastic properties of the chest wall cause it to expand to adopt its own equilibrium point (which is half the volume of the fully expanded state). Thus, at the same time elastic recoil of the lungs creates an inwardly directed force that tends to pull the lungs away from the chest wall. As a consequence, at the end of normal (passive) expiration (FRC), the combination of the outward pull of the thoracic cage and inward recoil
of the elastic lungs creates a subatmospheric intrapleu-ral pressure of about −3 mmHg. When a person is in the upright position, the weight of the lungs pulls the lungs away from the chest wall at the top of the lungs and squeezes them against the chest wall at the base of the lungs. This means that intrapleural pressure is more negative at the top of the lungs and less negative at the bases. Consequently, the alveolar volume is different between apex and bases because the alveolar volume is determined by transpulmonary pressure (P
alv − P
pl). In
any posture, the pleural fluid pressure with respect to atmospheric pressure is more negative at the top than at the bottom of the lung (Fig. 2.6).
The pleural space does not contain gas. This is because the sum of the tissue gas tensions is consider-ably less than atmospheric pressure, leading to the reabsorption of any gas in the pleural space. Also, the concentration of protein in the pleural fluid is low (1–2%), leading to a lower osmotic pressure than in the plasma. Therefore, the fluid is reabsorbed, and as a result the pleural space is relatively dry.
Respiratory muscles and Ppl: At FRC, neither the
lung nor the chest wall are in equilibrium. However, the combined chest wall system adopts an equilibrium position due to the absence of volitional contraction of muscles of breathing applied to the chest wall. However, when respiratory muscles are contracted, the P
pl changes. The fall in P
pl obtained in response to a
given stimulation of the phrenic nerves decreases rap-idly as the lung volume is passively increased above
0 20
RV FRC
40 60 80
00
20
20 40 60 80 100
40
60
80
100100
% VC0 20 40 60 80 100
% VC0
RV FRC
D = 21.4 cmD = 14.0 cmD = 3.9 cm
20 40 60 80 100% VC
% TLC0 20 40 60 80 100
% TLC0 20 40 60 80 100
% TLC
RE
GIO
NA
L LU
NG
VO
LUM
E (
% T
LCr)
RV FRC
Fig. 2.6 Correlation between percentage total lung capacity (% TLC) and regional lung volume. Abscissa lower axis is the overall lung volume expressed as percentage TLC, and the upper axis is the overall lung volume expressed as percentage vital capacity (VC).
The broken line (line of identity) indicates percentile degree of expansion of the regions equal to that of the entire lungs. The verti-cal distance (D) from the top of the lungs (in centimeters) to the center of each counter is indicated (From 26, with permission).

16 J.A. Sánchez-Godoy
FRC, and muscle length is decreased. Inspiration is effected by three groups of muscles, diaphragm, exter-nal intercostals, and some accessory muscles (e.g., scalenes, sternocleidomastoids, and trapezius come into play at high rates of ventilation). When the dia-phragm contracts, it loses its dome shape and drops down toward the abdomen. In quiet breathing, the dia-phragm moves about 1.5 cm. This movement increases thoracic volume by flattening its floor. Contraction of the diaphragm causes between 60 and 75% of inspira-tory volume change during normal breathing. Movement of the rib cage creates the remaining 25–40% of the volume change (Fig. 2.7). During inha-lation in the upright position, the external intercostals and scalene muscles contract and pull the ribs upward and out.
Weakness of inspiratory or expiratory muscles reduces inspiratory capacity and expiratory reserve volume, respectively. That weakness can be caused by mechanical derangement, in association with critical or chronic illness and as a result of a neurological or muscular disorder. For this reason, on both accounts the vital capacity and TLC are reduced. If the reduc-tion in vital capacity exceeds 50%, the hypoventilation is likely to occur with hypercapnia, and it can lead to hypoxemia.
Lung compliance (C) is the capability of the lungs to distend under pressure, as measured by pulmonary volume change per unit pressure change. The dis-tending pressure across the lung is the difference in
pressures between the inside and outside of the lung, that is, the transpulmonary pressure (P
alv − P
pl)2:
(2.10)
The measurement of lung compliance under condi-tions of no airflow (i.e., under static conditions) allows establishing the intrinsic elasticity or stiffness of the lungs without the confounding influence of needing additional pulmonary pressures to overcome the resis-tance to airflow. At the end of inspiration and expiration, P
alv must be exactly equal to P
atm because the airflow is
zero. Thus, to measure static lung compliance only, the changes in the lung volume and intrapleural pressure are needed. The lung volume can be readily measured with a simple spirometer, and the pleural pressure is normally estimated by measuring the intraesophageal pressure. For normal adults, a change of P
pl from −4 to −6 cm H
2O
would induce a volume change, a tidal volume, of approximately 600 mL. The compliance in this case would be 200 mL/cm H
2O. In a normal adult, it has a
mean value of 240 mL/cm H2O (Fig. 2.8). Recent stud-
ies have found that regular use of pressure–volume curves provides useful physiological data that help to optimize mechanical ventilation at the bedside and, more interestingly, to improve outcome.28,29 In a normal subject on mechanical ventilation, compliance should
( ) ( )
( )2( )
D D= Þ =
D D -ml ml
cmH Otp alv pl
V VC C
P P P
RIBCAGE
LUNG
INTERCOASTALACCESORYMUSCLES
ABDOMEN
COSTAL DIAPHRAGM
CRURAL DIAPHRAGM
Fig. 2.7 Mechanical model of inspiratory musculature. Intercostal and accessory muscles are mechanically parallel with costal dia-phragm. Bar into which crural and costal fibers insert represents central tendon. Inverted L-shaped structure represents rib cage, and springs attached to its upper surface indicate the elastic properties of the rib cage. The hatched area represents the rest of bony skeleton. Right: more anatomically realistic drawing of diaphragm illustrating separation of costal and crural parts (From 27, with permission)
2A positive transpulmonary pressure is needed to increase the lung volume.

172 Respiratory Physiology
be greater than 50–100 mL/cm H2O.30 Lower values are
obtained in children and in women compared with men, mainly due to absolutely smaller lungs. However, when the lung volume is considered in relative terms (e.g., as a fraction of the TLC), no significant differences are found due to age and gender. This has the effect that the compliance per liter of lung volume, which is the spe-cific compliance (sC), is effectively constant.
(2.11)
The specific compliance is usually reported for expi-ration at FRC; it then has a value in normal subjects of 0.08 cm H
2O (range 0.03–0.14 cm H
2O). Loss of com-
pliance increases the work of breathing (WOB).Measurements of transpulmonary pressure and vol-
ume also can be recorded continuously during tidal breathing. Then, the so-called dynamic compliance (C
dyn) can be obtained – usually on a plot of pressure
vs. volume – by measuring the slope of a line crossing values of esophageal pressure and volume at end expi-ration and end inspiration as determined by zero air-flow at the mouth. In normal subjects, dynamic compliance is only slightly less than static compliance. In patients with airway disease, redistribution of air continues through narrowed intrapulmonary airways even when flow at the mouth ceases. Consequently, some of the transpulmonary pressure apparently over-coming elastic forces is dissipated against resistive forces, and the apparent compliance is less than esti-mated statically. This effect goes along with increases in breathing frequency. Thus, in patients with even mild diffuse airway disease, the dynamic compliance falls as frequency increases.31
Compliance is different from elastance (elasticity). The fact that a lung stretches easily (high compliance) does not necessarily mean that it will return to its rest-ing volume when the stretching force is released. For example, when destruction of elastin occurs, the lungs exhibit high compliance and stretch easily during inspiration. However, these lungs also have decreased elastance, so they do not recoil to their resting position during expiration. Thus, people with emphysema have more difficulty exhaling than inhaling.
Chest wall compliance is the relationship of the pressure change across the chest wall to thoracic vol-ume. In normal subjects, it is on average 230 mL/cm H
2O. It can correlate negatively with age, disease of
chondrovertebral joints, damage to thoracic vertebrae, scarring of the skin of the chest, large bosom, or cen-tral obesity.
Closing volume (CV) is the lung volume at which the dependent lung zones cease to ventilate, presum-ably as a result of airway closure (Fig. 2.9). At the point of maximal closure, the volume of gas remaining in the lungs is the residual volume. This volume is reached when the pleural pressure is greater than the airway pressure in the terminal bronchi (in normal subjects). Premature closure increases the residual volume; the most common cause is the loss of lung elasticity = measuredsC C FCR
10 20 30 40
4321 kPa
cm H2O
TLC8
6
4
2
FRC
RV
Vmax
V0
Vmax
PL max
TLC
FRC
A
Shapefactor = k
Static chordcompliance
Dynamiccompliance
Lung elastic recoil pressure (PL)
Lung elastic recoil pressure (PL)
Vol
ume
(L)
Vol
ume
0
0
a
b
Fig. 2.8 (a) Static lung pressure–volume (PV) curve. Lung recoil pressure ( LP ) plotted against absolute lung volume and total lung capacity (TLC), measured separately. Different sym-bols indicate measurements made during five separate inter-rupted expirations from TLC. At volumes below functional residual capacity (FRC), the slope of the PV curve becomes shal-lower. Note that maximum LP in this healthy young individual is unusually high at approximately 50 cm H
2O. (b) Measurements
from static lung PV curve and dynamic lung compliance. Heavy line is a diagrammatic static PV curve of lungs from TLC to FRC with extrapolation to V
max and V
0 (difference = A) to allow calcu-
lation of shape factor “k.” In general, the greater the value of k, the more distensible the lungs (From 31, with permission)

18 J.A. Sánchez-Godoy
(increased compliance), which occurs with increasing age and with emphysema. Premature generalized clo-sure can also occur as a consequence of narrowing of airways from other causes, including contraction of bronchial muscles and thickening of air walls.32
Several factors as well as the elastic recoil of the lungs and the chest wall must be overcome to move air into or out of the lungs. These factors include the inertia of the respiratory system and the frictional resistance of the air-ways to the flow of air. Inertial forces are of negligible magnitude except when a high-frequency oscillation is applied for mechanical ventilation or in experimental conditions. Pulmonary tissue resistance (R
ti) is caused
by the friction encountered as the lung tissues move against each other during lung expansion. The R
ti itself is
bigger in pulmonary fibrosis and other conditions in which the quantity of interstitial lung tissue is increased.
The airways resistance (Raw
) plus the pulmonary tissue resistance is often referred to as the pulmonary resis-tance (Rl). Pulmonary tissue resistance normally con-tributes about 10–20% of the pulmonary resistance, with airways resistance responsible for the rest. Pulmonary tissue resistance can be augmented in such conditions as pulmonary sarcoidosis and fibrosis. Since airways resis-tance is the major component of the total resistance, this chapter concentrates on airways resistance.
Raw
, as a part of pulmonary function testing, is the ratio of driving pressure to the rate of airflow. Three parameters contribute to resistance: the system’s length L, the viscosity of the fluid ( h ), and the radius of the tubes in the system r. Poiseuille’s law relates these fac-tors to one another:
(2.12)4µR L rh
Closed airways
Bolus inspired Tracer gasconcentration
Proportionof airwaysclosed
RV Lung volume TLC CC RV
CV
Closedairways
Expiredgases
Alveolargases
a b c d e f
Fig. 2.9 The proposed mechanism for the closing volume (CV) maneuver with a tracer gas. A The lung is at residual volume (RV), and a bolus of tracer gas is inspired, passing into lung regions served by airways that remain open. Lung regions with closed airways do not receive any tracer gas. B The tracer gas bolus is followed by unlabeled air. As this unlabeled air is inspired, it dilutes the tracer gas according to the regional venti-lation pattern of the lung. Regions previously closed are then open and receive air. C Total lung capacity (TLC) is reached. The alveoli that were open at RV contain tracer gas; the alveoli that were closed, and the airways, contain air only. D Expiration has
started, and airway gas containing no tracer is exhaled; this is dead-space gas. E The “alveolar plateau” contains slightly vary-ing contributions from different lung regions (partly because of cardiac movement). The exhaled concentration represents this variation in contributions from different regions. F As airway clo-sure starts, the lung regions that contain less or no tracer gas cease to contribute to expired gas. Consequently, the tracer gas concentration in the expired gas increases as it is now only emerg-ing from labeled lung regions. The lung volume at which airway closure starts is called the closing capacity (CC), and the differ-ence between CC and RV is the CV (From 32, with permission)

192 Respiratory Physiology
In normal conditions, the length and viscosity are constant; then, the radius of the airways becomes the pri-mary determinant of R
aw. However, the work needed by
a normal subject to overcome resistance of the airways to airflow is much less than work needed to overcome the resistance of the lungs and thoracic cage to stretch.
Because the airways behave like a circuit in parallel, the resistance at each level of the airways depends on the cross-sectional area. For this reason, the resistance is greater in the proximal airway (e.g., trachea 2–2.5 cm2) than in the distal airway (5 × 103 cm2). The first eight airway generations are the major site of airway resis-tance. R
aw varies with lung volume because the airways
diameter, as well as the alveoli, depends on the changes in the pleural pressure. The resistance is lower at large volumes when the airways are expanded; it rises during expiration as the airways diminish in size and becomes infinite at residual volume when some airways close.
The Raw
also depends on the pattern of flow. The airway resistance is the sum of its laminar and turbu-lent components. The determinants of this pattern were described by Reynolds:
(2.13)
where v is the bulk flow gas, A is the cross-sectional area, D is the diameter, r is the gas density, and h is the gas viscosity. Re numbers less than 100 and more than 4,000 are associated, respectively, with completely laminar and fully turbulent flow. With other values, Re would be intermediate. Thus, on the trachea it is inter-mediate, and in the bronchioles it is nearly laminar.
Work of breathing: The two main components of the WOB are the elastic recoil of the lungs and chest wall and the resistance to airflow. The inertia of the airway is also part of impedance, but its contribution is negligible in respiratory physiology. Impedance can be estimated through measurements of the WOB. In respiratory physiology, WOB describes the energy required as the flow begins to perform the task of ventilation. Breathing requires the use of respiratory muscles (diaphragm, intercostals, etc.), which expend energy. In general, the work performed during each respiratory cycle is math-ematically expressed as WOB = ´ò P V (i.e., the area on a pressure–volume diagram).3 The volume change is
the volume of air moved into and out of the lung, the tidal volume. The pressure change is the change in transpulmonary pressure necessary to overcome the elastic WOB and the resistive WOB. Impedance to air-flow includes the resistance to airflow as well as the force required to overcome the elasticity of the lungs and chest wall. The calculation of the WOB is usually associated with inspiratory effort because expiration is generally a passive process. However, in patients with air trapping or acute respiratory failure, expiration can be an active process and can require significant work.33 Although ventilation normally requires 5% of total oxy-gen delivery,34 this requirement increases during lung pathological states, such that the metabolic demand for oxygen may reach 25% of total oxygen delivery.
2.3.3 Alveolar Gas Pressures
The levels of oxygen and carbon dioxide in alveolar gas are determined by the altitude ( BP ), the composi-tion of the inspired air, the alveolar ventilation volume (VA ), the rate of oxygen consumption ( 2OV ), and the carbon dioxide production of the body (
2COV ).35,36
The partial pressure of oxygen changes as it flows through the airway. The partial pressure of oxygen in the ambient air is determined by BP . Hence, the dry
2OP can be calculated from the fraction of oxygen (
2OF ) in the gas mixture times the total or ambient (barometric) pressure. At sea level, that is,
(2.14)
Evidently, 2OP will be altered if the subject is at alti-
tude or if using supplemental oxygen.As inspiration begins, inspired gases become saturated
with water vapor, which exerts a partial pressure (47 mmHg at normal body temperature). Because the total pressure remains constant at BP , water vapor dilutes the total pres-sure of the other gases. Hence, in the conducting airways the partial pressure of oxygen may be calculated as
(2.15)
At the end of inspiration or expiration, with the glottis open, the total alveolar pressure is equal to BP . The gas
Re = vD Ar h
2 2 2
2
760
0.21 159.6
= ´ Þ =
´ Þ =
BO O O
O
P P F P mmHg
P mmHg
2 2 22( )
0.21 (760 47)
= ´ - ¾¾¾¾®
= ´ -O O O
at sea levelI I B H O I
mmHg
P F P P P
3In a healthy subject, the work per liter of ventilation (work per cycle divided by tidal volume) normal value is around 2.4 J/min, with 1 joule (J) the energy needed to move 1 L of gas through a 10-cm H
2O pressure gradient.

20 J.A. Sánchez-Godoy
exchange decreases the 2OP and increases the
2COP . Therefore, the alveolar oxygen pressure (
2OPA ) is slightly lower than
2OPI and can be calculated by the alveolar gas equation:
(2.16)
The respiratory exchange ratio is the ratio of the rate at which carbon dioxide leaves the lung in expired gas (
2COV ) to the rate of oxygen consumption (2OV ).
Under steady-state conditions, such a ratio is repre-sentative of the metabolism of the subject and is called the respiratory quotient (R). R varies between 0.7 and 1.0 when the metabolism is exclusively from fatty acid or when there is exclusive carbohydrate metabolism, respectively. R in a mixed diet is approx-imately 0.8.
The concentration of carbon dioxide in the alveolar gas is dependent on VA and on 2COV (and its delivery to the lung in the mixed venous blood). The volume of carbon dioxide expired per unit of time (
2COVE ) is equal to VA times the alveolar fractional concentration of CO
2 (
2COFA ). No carbon dioxide comes from the dead space. This relationship is defined by the alveolar car-bon dioxide equation:
(2.17)
since the 2COPA is defined by
(2.18)
then,
(2.19)
Therefore, there is an inverse relationship between
2COPA and VA . 2COPA is tightly regulated to
remain constant around 40 mmHg at sea level via a ventilatory control system. In a normal subject,
2COPA is in equilibrium with arterial carbon dioxide pressure (
2COPa ). Thus, when VA decreases (hypo-ventilation),
2COPa becomes greater, causing respi-ratory acidosis. Hyperventilation has the opposite effect (Fig. 2.10).
When the alveolar oxygen equation and alveolar carbon dioxide equation are related to each other, it is possible to demonstrate that PaO
2 depends on the
composition of the inspired air, 2OV (mL/min) and VA (mL/min):
(2.20)
Distribution of ventilation: Studies performed on normal subjects seated upright have shown that alveoli in the lower regions of the lungs receive more ventila-tion per unit volume than those in the upper regions of the lung. As described previously, alveolar volume depends on transpulmonary pressure. Alveolar pres-sure is the same everywhere in the lungs, but because of these regional differences in P
pl, alveoli at the top of
the lungs are at a larger volume (due to a more negative P
pl) than those at the base (less-negative P
pl).4 Thus, at
the beginning of a breath, some alveoli start at a larger volume than the other alveoli. As described, alveolar compliance depends on volume changes. At the begin-ning of a breath, intrapleural pressure decreases the same amount everywhere. However, because the alve-oli at the top of the lungs start at a larger volume, they
2
2 2 2
2
2
CO
O O O
COB H OO 2(P )
= - Þ
= - -
PAPA PI PA
RPA
FI PR
2 2CO CO= ´V VA FA
2 2CO CO 2(PB H O)= ´ -PA FA P
2
2
CO 2
CO
(PB H O)´ -=
V PPA
VA
2
2 2
O
O O (PB 47)= - -V
PA PIVA
Alveolar Ventilation (L/min)
Alv
eola
r P
artia
l Pre
ssur
e (P
A)
in m
mH
g
2 4 6 8 10 12
PACO2PACO2
VA
VA
Q
Q
PAO2PAO2
NormalVentilation120
90
60
30
0
Fig. 2.10 2OPA and
2COPA are inversely related due the converse effects of ventilation. Hyperventilation ( 2COPa <40 mmHg) results in increased
2OPa and decreased 2COPa . Hypoventilation
(2OPa >40 mmHg) causes decreased
2OPA and hypoxemia (From 37, with permission)
4This is because the pleural pressure is lower at the apex than at the base because the weight of the lungs tends to pull it downward, away from the chest wall. If the pleural pressure is decreased, the transpulmonary pressure must be increased, and the alveolar volume increases in this area.

212 Respiratory Physiology
are less compliant and consequently change their vol-ume less than alveoli of the bases despite the same fall in the P
pl (Fig. 2.6). Therefore, the weight of the lungs
sets alveoli at different initial volumes, which affects how much their volume can be increased during a breath. Those at the base are ventilated more than those at the top of the lung.
In a theoretically constructed model of the lung, complete gas exchange equilibrium is reached between alveolar gas and pulmonary capillary blood, and par-tial pressures for CO
2 and O
2 in arterial blood are equal
to those in alveolar gas. In fact, under basal conditions, most O
2 transfer across the alveolar–capillary mem-
brane occurs within one third of the transit time for blood in the pulmonary capillaries.
In real lungs, partial pressure differences between alveolar gas and arterialized blood – an alveolar-to-arte-rial PO
2 difference (AaDO
2) and arterial-to-alveolar
PCO2 difference (aADCO
2) – are found. In the conven-
tional model analysis of alveolar gas exchange, these differences are attributed to three mechanisms: (1) unequal distribution of alveolar ventilation to pulmonary blood flow; (2) shunt; and (3) diffusion limitation.
2.3.4 Unequal Distribution of Ventilation to Perfusion
Perfusion: The systemic and pulmonary circulations differ significantly with regard to blood flow and pres-sure–volume relationship. The pulmonary circulation is a low-pressure and low-resistance system with a driving pressure that is almost a 13th of the systemic circulation. This difference is partially caused by greater compliance of the pulmonary vessels than the systemic vessels. In contrast to systemic arterial ves-sels, the anatomical structure of pulmonary arteries is characterized by a thinner media and fewer smooth muscle cells surrounding precapillary resistance ves-sels. The pulmonary vessels are seven times more compliant than the systemic vessels. Hence, increased vascular distensibility causes decreased pulmonary vascular resistance (PVR) when compared with sys-temic vascular resistance despite an equal blood flow. This resistance is about ten times less than in the sys-temic circulation. Using an equation like Ohm’s law, PVR can be calculated as the difference between mean
pulmonary artery pressure (MPAP) and pressure of left atrium (PLA) divided by the cardiac output. PLA can be replaced with pulmonary artery wedge pressure (PAWP):
(2.21)
Lung volume can affect PVR through its influence on alveolar vessels, mainly on the capillaries. At the end of inspiration, the fully distended air-filled alveoli compress the alveolar capillaries and increase PVR. In contrast to the capillary beds in the systemic circula-tion, the capillary bed in the lung has a major influence on PVR, and it accounts for about 40% of the resis-tance. This stretching effect during inspiration has an opposite effect on larger extra-alveolar vessels, which increase in diameter due to radial traction by the con-nective tissue and alveolar septa holding the larger ves-sels in place in the lung (Fig. 2.11). The extra-alveolar vessels are not influenced by alveolar pressure changes, but they are affected by intrapleural and interstitial pressure changes. As lung volume is increased by making the intrapleural pressure more negative, the transmural pressure gradient of the larger arteries and veins increases, and they distend.38
pulmonary pulmonary
MPAP PLA
Cardiac output
MPAP PAWP
Cardiac output
-= Þ
-=
R R
Expanded Partially defected
a b
Fig. 2.11 The mechanism of radial traction on blood vessels. When the lungs are expanded (a) the capillaries in the alveolar walls are attenuated, and the volume of blood that they contain is less than when the lung is partially deflated. (b) By contrast, the alveolar corner vessels and the extra-alveolar vessels in the interstitial spaces are increased in size due to traction from sur-rounding structures (From 38, with permission)

22 J.A. Sánchez-Godoy
PVR usually decreases with increases in pulmonary blood flow, pulmonary artery pressure, left atrial pres-sure, or pulmonary capillary blood volume because of distention of already open blood vessels, recruitment of previously unopened vessels, or both.39 Therefore, recruitment of physiologically collapsed pulmonary vessels at rest provides constant PVR even in the pres-ence of increased cardiac output during exercise40 (Fig. 2.12). This effect is due to a decrease of the PVR occurring when the blood vessels are recruited and dis-tended. Alveolar hypoxia (or hypercapnia) can cause constriction of precapillary pulmonary vessels, divert-ing blood flow away from poorly ventilated or unven-tilated alveoli. However, local hypoxia does not alter PVR. Approximately 20% of the vessels need to be hypoxic before a change in PVR can be measured. Low inspired oxygen levels due to exposure to high altitude will have a greater effect on PVR.
Regional perfusion changes because of gravity: In upright, resting subjects, blood flow increases lin-early from the apex of the lung to the base of the lung, where the flow is the greatest. The marked effect of gravity on pulmonary circulation stems from the low arterial pulmonary pressure and the very different densities of blood and air. Because there is a hydro-static gradient in blood but practically none in alveo-lar air, the transmural pressure in pulmonary vessels increases vertically from top to bottom, leading to distension of vessels and increased blood volume and blood flow in the lower (dependent) lung regions. The interplay of alveolar pressure, flow rate, and vascular resistance is best considered by dividing the lung field into four zones. Zone 1 represents the apex region, where blood does not flow under certain con-ditions. Under normal conditions, zone 1 does not exist; nevertheless, this state is reached during posi-tive-pressure mechanical ventilation and conditions with severe decrease of the arterial pressure (Pa). In zone 2, which comprises the upper one third of the lung, Pa is greater than the PA, which is greater than
venous pressure (Pv). In zone 3, Pa is greater than Pv, which is greater than PA, and blood flow in this area parallels the pressure gradients.41 In zone 4, in the most dependent part of the lung the intravascular hydrostatic pressure is relatively high. This can lead to fluid passing into the interstitial tissue. In normal circumstances, the quantity of fluid is small. It can increase dramatically if pulmonary venous pressure or the permeability of the pulmonary capillary mem-brane is increased or if the plasma osmotic pressure is reduced, thus causing alveolar interstitial edema (Fig. 2.13).
It has been known for many years that the distribu-tion of ventilation–perfusion ratios ( AV Q ) is uneven in the lungs of normal subjects. The 1953 work of Martin, Cline, and Marshall42 demonstrated interlo-bar differences in O
2 and CO
2 concentrations best
explained by regional differences in ventilation and blood flow. On average, AV Q is approximately 1. However, as described in previous sections, the effect of gravity produces differences in ventilation and perfusion from the top to the bottom of the lungs. Relative to the top of the lung, the base of the lung is ventilated (approximately 3 times) and perfused (18 times) better. However, because the change in venti-lation from the top to the bottom of lungs is not as great as the change in blood flow, AV Q decreases from the top to the bottom of the lungs (approxi-mately five times). This means that the top of the lungs is overventilated relative to its blood flow, and the base of the lung is overperfused relative to its ven-tilation. In other words, AV Q is high at the top of the lung and low at the base of the lung. This imbalance between alveolar ventilation and blood flow is also called -VA Q mismatch.
Regional differences in AV Q result in regional dif-ferences in gas exchanges from the top to the bottom of the normal lung. Thus, blood leaving the top of the lung has a higher
2OP and a lower 2COP than the blood
leaving the base of the lung.
Increase inperfusionpressure
Furtherincreaseperfusionpressure
Fig. 2.12 Recruitment and distention of alveolar vessels

232 Respiratory Physiology
Ventilation and perfusion must be matched on the alveolar–capillary level for optimal gas exchange. The alveolar–arterial
2OP difference (2OAaD ) due to AV Q
inequality may amount to 10–15 mmHg in normal individuals, the alveolar-arterial
2COP difference to 2–4 mmHg. The extreme cases are of particular inter-est. 0=AV Q means lack of ventilation and therefore absence of gas exchange, its perfusion constituting shunt or venous admixture. = ¥AV Q , due to 0=Q , designates the presence of ventilated but unperfused alveoli (Fig. 2.14). Again, there is no gas exchange, and the ventilation of such a compartment is function-ally a dead space ventilation. It is called parallel or alveolar dead space ventilation, as distinguished from conducting airway ventilation, which is series or ana-tomic dead space ventilation. The sum of both is
equivalent to total ventilation not contributing to gas exchange. It is termed physiologic dead space ventila-tion. It can be calculated from Bohr’s equation as described previously. Ventilation–perfusion ratios close to 1.0 result in alveolar PO
2s of approximately
100 mmHg and PCO2s close to 40 mmHg (at sea
level); ventilation–perfusion ratios greater than 1.0 increase the PO
2 and decrease the PCO
2; ventilation–
perfusion ratios lower than 1.0 decrease the PO2 and
increase the PCO2.
2.3.5 Shunt or Venous Admixture
A short circuit of blood passing gas-exchanging regions of the lungs leads to admixture of venous blood to arte-rialized blood and thus to a decrease of PO
2 and
increase of PCO2 in the arterial blood. Shunt refers to a
condition in which AV Q tends to zero because of no ventilation. The lack of ventilation may occur for two reasons: either the vasculature does not have access to alveoli or alveoli do not permit gas exchange because they are either physically plugged (not ventilated) or impermeable to gas. There are two types of shunts, anatomic and absolute. Anatomic (extrapulmonary) shunt refers to the amount of systemic venous blood that mixes with the pulmonary end-capillary blood on the arterial side of the circulation. In a normal healthy adult, about 2–5% of the cardiac output, including venous blood from the bronchial veins, the Thebesian veins, and the pleural veins, enters the left side of the circulation directly without passing through the pul-monary capillaries. In contrast, mixed venous blood perfusing pulmonary capillaries, associated with totally unventilated or collapsed alveoli, constitutes an
PA>Pa>PV
Pa >PA>PV
Pa
PAPV
Pa >PV>PA
PV = Pa
Pa = PA
Some flowoccurs viaalveolar cornervessels
Distance
Blood flow
1
2
3
4
Fig. 2.13 Model to explain the effect of gravity on the vertical distribution of blood flow in lungs (Modified from 41, with permission)
PVO2PVO2
PAO2PAO2 = PVO2 PAO2 = PIO2
Dead spaceShunt
V/Q = 0 V/Q = 1 V/Q = ∞
PaO2 = PVO2 PaO2
Fig. 2.14 Three different lung regions with ventilation-to-perfusion ratios (V/Q ratios) of 0 (left), 1 (middle), and µ (right). The expected PO
2s are shown for each
region. PvO2, venous PO
2
(From 37, with permission)

24 J.A. Sánchez-Godoy
absolute shunt because no gas exchange occurs as the blood passes through the lung. Absolute shunt is some-times also referred to as true shunt, alveolar shunt, or intrapulmonary shunt. Alveolar–capillary units with low AV Q also act to lower the arterial oxygen content because the blood draining these units has a lower PO
2
than blood from units with well-matched ventilation and perfusion. These are referred to as “shuntlike states.” The combined effect of anatomical shunt, alve-olar shunt, and “shuntlike” states is called physiologi-cal shunt and can be calculated by the shunt equation:
(2.22)
where C is content of oxygen; c¢, a, and v refer, respectively, to the end-capillary, arterial, and mixed venous blood. In a healthy young adult at rest, 2% of cardiac output does not participate in gas exchange. At age 60, the average proportion is approximately 4%.43 Among the intrapulmonary causes for an increased venous admixture effect, an enlarged ana-tomical shunt occurs in some cases of bronchiectasis, atelectasis, and pulmonary edema. Extrapulmonary causes include cyanotic congenital heart disease and portal cirrhosis.
According to experimental results, a substantial part of the AV Q inequality appears not to be due to gravity but to anatomical heterogeneity of airways and blood vessels. The gravitational model of ventilation–perfusion distribution might fail to explain adequately several important observations regarding the distribu-tion of ventilation and perfusion: heterogeneity at the same vertical level, postural inequality, and the persis-tence of heterogeneity in the absence of gravity. The underlying structure of the bronchial and pulmonary vascular anatomy with nonsymmetrical branching is now considered an important factor in causing hetero-geneity in pulmonary perfusion and ventilation in both health and disease.44
2.3.6 Gas Diffusion
Diffusion is important for gas movement from the smaller airways to the alveoli and for gas movement across the alveoli into the blood and from the blood to the tissue and mitochondria (oxygen) and conversely
from the tissue to blood, from the blood to the alveoli, and from alveoli to the smaller airways (carbon diox-ide). Four factors determine the amount of gas diffus-ing through a sheet of tissue over time, but only one changes under normal conditions, the pressure gradi-ent. Fick’s law states that the rate of diffusion (V ) of a gas across a sheet of tissue is directly related to the surface area A of the tissue, the diffusion constant D of the specific gas, and the partial pressure difference P
1
− P2 of each gas on each side of the tissue, and it is
inversely related to the tissue thickness T. Thus,
(2.23)
Two properties of the gas contribute to the diffusing capacity of the lungs D
L: solubility S and molecular
weight MW (S MW ). First, the mobility of the gas should decrease as its molecular weight increases. Indeed, Graham’s law states that the diffusion is inversely proportional to the square root of MW. Second, Fick’s law states that the flow of the gas across the wet barrier is proportional to the concentration gra-dient of the gas dissolved in water. According to Henry’s law, these concentrations are proportional to the respective partial pressures, and the proportionality constant is the solubility of gas. Therefore, poorly sol-uble gases like N
2 and helium diffuse poorly across the
alveolar wall. The ratio ´A D T represents the con-ductance of a gas from alveolus to the blood. The physical properties of oxygen and carbon dioxide enable them to diffuse rapidly between the alveolar air and the blood. Therefore, the amount of these gases in the blood is not limited by diffusion. Nevertheless, the amount of these gases in the blood is limited by blood flow.6 As carbon monoxide has a low solubility in the capillary membrane, it is limited by diffusion across the alveolar–capillary membrane. For this reason, CO is a useful gas for calculating D
L, also named the trans-
fer factor, as follows:
(2.24)
2 2
2 2
O CaO(%) 100
O O
-¢= ´
-¢CcQs
Cc CvQt
1 2( )gas
- ´ ´=
P P A DV
T
CO
ACO
=V
DLP
6If the partial pressure of a gas in the plasma equilibrates with the alveolar partial pressure of the gas within the amount of time the blood is in the pulmonary capillary, its transfer is perfusion limited; if equilibration does not occur within the time the blood is in the capillary, its transfer is diffusion limited.

252 Respiratory Physiology
The oxygen-diffusing capacity of the lung (2ODL ) is
its conductance ( ´A D T ) when considered for the entire lung; thus, applying Fick’s equation, the
2ODL can be calculated (theoretically) as follows:
(2.25)
where 2OV is the net diffusion of O
2, and
2OPc is the mean pulmonary capillary
2OP . But, as 2ODL cannot be
calculated directly, CODL is most frequently used in determinations of the diffusing capacity because the mean pulmonary capillary partial pressure of carbon monoxide is virtually zero when nonlethal alveolar partial pressures of carbon monoxide are used.
Although diffusion per se involves no expenditure of energy, the body must do work, in the form of ventilation and circulation, to create the concentration gradients under which O
2 and CO
2 diffuse as discussed.
References
1. Connett RJ, Honig CR, Gayeski TE, Brooks GA. Defining hypoxia: a systems view of VO
2, glycolysis, energetics, and
intracellular PO2. J Appl Physiol. 1990;68:833-842.
2. Nathan AT, Singer M. The oxygen trail: tissue oxygenation. Br Med Bull. 1999;55:96-108.
3. Wolfe DF, Sorbello JG. Comparison of published pressure gradient symbols and equations in mechanics of breathing. Respir Care. 2006;51:1450-1457.
4. Pappenheimer JR, Comroe JH, Cournand A, et al. Standardization of definitions and symbols in respiratory physiology. Fed Proc. 1950;9:602-605.
5. Berne RM, Levy M, Koeppen B, Stanton B. Physiology. St Louis: Mosby; 2004.
6. Wanger J, Clausen JL, Coates A, et al. Standardisation of the measurement of lung volumes. Eur Respir J. 2005;26:511-522.
7. Knowles JH, Hong SK, Rahn H. Possible errors using esophageal balloon in determination of pressure–volume characteristics of the lung and thoracic cage. J Appl Physiol. 1959;14:525-530.
8. Coates AL, Peslin R, Rodenstein D, Stocks J. Measurement of lung volumes by plethysmography. Eur Respir J. 1997;10:1415-1427.
9. Dubois AB, Botelho SY, Bedell GN, Marshall R, Comroe JH Jr. A rapid plethysmographic method for measuring tho-racic gas volume: a comparison with a nitrogen washout method for measuring functional residual capacity in normal subjects. J Clin Invest. 1956;35:322-326.
10. Newth CJ, Enright P, Johnson RL. Multiple-breath nitrogen washout techniques: including measurements with patients on ventilators. Eur Respir J. 1997;10:2174-2185.
11. Meneely GR, Kaltreider NL. The volume of the lung deter-mined by helium dilution. Description of the method and com-parison with other procedures. J Clin Invest. 1949;28:129-139.
12. Clausen J. Measurement of absolute lung volumes by imag-ing techniques. Eur Respir J. 1997;10:2427-2431.
13. Rochester DF. Tests of respiratory muscle function. Clin Chest Med. 1988;9:249-261.
14. Syabbalo N. Assessment of respiratory muscle function and strength. Postgrad Med J. 1998;74:208-215.
15. Pacia EB, Aldrich TK. Assessment of diaphragm function. Chest Surg Clin N Am. 1998;8:225-236.
16. Harik-Khan RI, Wise RA, Fozard JL. Determinants of maxi-mal inspiratory pressure. The Baltimore Longitudinal Study of Aging. Am J Respir Crit Care Med. 1998;158:1459-1464.
17. Koulouris N, Mulvey DA, Laroche CM, Sawicka EH, Green M, Moxham J. The measurement of inspiratory muscle strength by sniff esophageal, nasopharyngeal, and mouth pressures. Am Rev Respir Dis. 1989;139:641-646.
18. Cotes JE, Chinn DJ, Miller MR. Lung function. Physiology, measurement and application in medicine. Oxford: Blackwell; 2006.
19. Escolar JD, Escolar A. Lung hysteresis: a morphological view. Histol Histopathol. 2004;19:159-166.
20. Mead J, Whittenberg JL, Radford EP Jr. Surface tension as a factor in pulmonary volume–pressure hysteresis. J Appl Physiol. 1957;10:191-196.
21. Garcia CS, Prota LF, Morales MM, Romero PV, Zin WA, Rocco PR. Understanding the mechanisms of lung mechani-cal stress. Braz J Med Biol Res. 2006;39:697-706.
22. Halliday HL. Surfactants: past, present and future. J Perinatol. 2008;28(suppl 1):S47-S56.
23. Neegaard KV. Neue auffassungen uber einen grundbegriff der atemmechanik. Die retraktionskraft der lunge, abhangig von der oberflachenspannung in den alveolen. Gesund Wohlfahrt. 1948;28:231-260.
24. Haitsma JJ. Physiology of mechanical ventilation. Crit Care Clin. 2007;23:117–134,vii
25. Bernhard W, Haagsman HP, Tschernig T, et al. Conductive airway surfactant: surface-tension function, biochemical composition, and possible alveolar origin. Am J Respir Cell Mol Biol. 1997;17:41-50.
26. Milic-Emili J, Henderson JA, Dolovich MB, Trop D, Kaneko K. Regional distribution of inspired gas in the lung. J Appl Physiol. 1966;21:749-759.
27. Macklem PT, Macklem DM, De TA. A model of inspiratory muscle mechanics. J Appl Physiol. 1983;55:547-557.
28. Albaiceta GM, Garcia E, Taboada F. Comparative study of four sigmoid models of pressure–volume curve in acute lung injury. Biomed Eng Online. 2007;6:7.
29. Albaiceta GM, Blanch L, Lucangelo U. Static pressure–vol-ume curves of the respiratory system: were they just a pass-ing fad? Curr Opin Crit Care. 2008;14:80-86.
30. MacIntyre NR. Evidence-based ventilator weaning and dis-continuation. Respir Care. 2004;49:830-836.
31. Gibson GJ. Lung volumes and elasticity. Clin Chest Med. 2001;22:623–635,vii
32. Drummond GB, Milic-Emili J. Forty years of closing vol-ume. Br J Anaesth. 2007;99:772-774.
33. Grinnan DC, Truwit JD. Clinical review: respiratory mechan-ics in spontaneous and assisted ventilation. Crit Care. 2005;9:472-484.
2
2
2 2
O
OO O
=-
VDL
PA Pc

26 J.A. Sánchez-Godoy
34. Roussos C, Macklem PT. The respiratory muscles. N Engl J Med. 1982;307:786-797.
35. Fenn WO, Rahn H, Otis AB. A theoretical study of the com-position of the alveolar air at altitude. Am J Physiol. 1946;146:637-653.
36. Curran-Everett D. A classic learning opportunity from Fenn, Rahn, and Otis (1946): the alveolar gas equation. Adv Physiol Educ. 2006;30:58-62.
37. Glenny RW. Teaching ventilation/perfusion relationships in the lung. Adv Physiol Educ. 2008;32:192-195.
38. Howell JB, Permutt S, Proctor DF, Riley RL. Effect of inflation of the lung on different parts of pulmonary vascular bed. J Appl Physiol. 1961;16:71-76.
39. Levitzky MG. Pulmonary Physiology. New York: McGraw-Hill; 2007.
40. Dembinski R, Henzler D, Rossaint R. Modulating the pul-monary circulation: an update. Minerva Anestesiol. 2004;70:239-243.
41. West JB, Dollery CT, Naimark A. Distribution of blood flow in isolated lung; relation to vascular and alveolar pressures. J Appl Physiol. 1964;19:713-724.
42. Martin CJ, Marshall H, Cline F Jr. Lobar alveolar gas con-centrations; effect of body position. J Clin Invest. 1953;32:617-621.
43. Harris EA, Seelye ER, Whitlock RM. Gas exchange during exercise in healthy people II. Venous admixture. Clin Sci Mol Med. 1976;51:335-344.
44. Galvin I, Drummond GB, Nirmalan M. Distribution of blood flow and ventilation in the lung: gravity is not the only fac-tor. Br J Anaesth. 2007;98:420-428.

http://www.springer.com/978-1-84996-307-7














![MERKI MINICATALOGUE2013 [Mode de compatibilité] · C1 IST/702-avec réglage de niveau C1 IST/703-avec réglage de niveau ... C1 RMD/181M * C1 RMD/100M* C1 RMD/102M* C1 RMD/101M*](https://img.pdfslide.net/doc/110x75/5b87a8ef7f8b9aaf728bdd63/merki-minicatalogue2013-mode-de-compatibilite-c1-ist702-avec-reglage-de.jpg)







![VIII Seminário “Desenvolvimento ... - ibracon.org.br1].pdf · C1 C2 C3 C1 C2 C3 C1 C2 C3 C1 C2 C3 C1 C2 C3 C1 C2 C3 R EVEVC R EVEVC 91dias 300dias Volume Total Intrudido de Hg](https://img.pdfslide.net/doc/110x75/5c0a1db209d3f2411a8b59c1/viii-seminario-desenvolvimento-1pdf-c1-c2-c3-c1-c2-c3-c1-c2-c3-c1.jpg)





