Embed Size (px)
Citation preview

J Med Syst (2018) 42:181 https://doi.org/10.1007/s10916-018-1034-2
SYSTEMS-LEVEL QUALITY IMPROVEMENT
A BPMN Based Notation for the Representation of Workflowsin Hospital Protocols
Mateo Ramos-Merino1 · Luis M. Alvarez-Sabucedo1 · Juan M. Santos-Gago1 · Javier Sanz-Valero2
Received: 3 July 2018 / Accepted: 15 August 2018© Springer Science+Business Media, LLC, part of Springer Nature 2018
AbstractFlowcharts used for hospital protocols have a series of ambiguities and limitations in order to express some types ofinformation. In this article, a notation proposal for flowcharts that partially avoids these problems is presented. This newnotation is an adaptation of BPMNE2, an extension of the Business Process Model and Notation (BPMN), which allowsdirect modelling of procedures that follow the Hazard Analysis and Critical Control Points (HACCP) model. The newnotation has been validated in the hospital context, specifically in the field of hazardous drugs (HDs). To measure usabilityfrom the perspective of the health staff and auditors, the System Usability Scale (SUS) was used. A total of 47 experts tookpart in the assessment, resulting in a SUS score of 71, that corresponds to an acceptable level of usability. The feedbackprovided by these participants allows us to discover benefits and drawbacks of the proposal. Also, it is noteworthy that76.6% of professionals prefer to migrate to the new notation from the ISO 5807:1985 notation, the most commonly usedmodel. In addition to the direct benefits of this notation from the human point of view, its machine-understandable natureprovides the required support for its integration into software tools for intelligent monitoring and auditing.
Keywords BPMN · Hospital protocols · HACCP · Hazardous drugs · Flowcharts · System usability scale
Introduction andmotivation
The implementation of hospital processes is a critical taskthat must be handled holistically. Any error at specificpoints on its execution may cause severe consequencesfor the staff and for the patients. A common practice tominimise these undesired situations is the early definition ofaction protocols, i.e., standardised procedures that identifyall the possible situations and define systematically theactivities involved in the processes under consideration.This definition process requires an effort on analysis andmodelling, which is reflected in a set of formal documents.
This article is part of the Topical Collection on Health InformationSystems & Technologies
� Mateo [email protected]
1 Escola de Enxenarıa de Telecomunicacion, Universidadede Vigo, Campus Lagoas-Marcosende, 36.310 Vigo,Galicia, Spain
2 Departmento de Salud Publica, Historia de la Cienciay Ginecologıa, Universidad Miguel Hernandez,Campus Sant Joan, 03.550 Alicante, Spain
The generated documentation typically consists of textand tables that specify, as unambiguously as possible, theactivities or tasks to be performed, their sequencing, theset of restrictions that must be met at each point in theprocess and the actions that must be carried out in caseof detecting an error or a problem. It usually includesalso graphic representations of the most relevant or morecomplex execution flows along with the text descriptions,improving the legibility of the documentation.
The flowcharts facilitate the interpretation of theprotocols and, thus, streamline the work of both the healthand service staff (the persons in charge of executing theactivities defined therein), and the managers and auditors(the people who check compliance with the protocols).Flowcharts are a standardised method that offers theseactors an overview of the nature of the processes quicklyand visually.
Despite these benefits, the flowcharts used in thedocumentation of hospital protocols often present someproblems [28]:
– They are, on occasion, partially ambiguous. This isthe result of the generic and informal nature used forthese representations. Logically, this is not usually a

181 Page 2 of 10 J Med Syst (2018) 42:181
significant barrier for those people who interpret theflowcharts. This is because they only interact with theserepresentations casually (they do not need to check thelow-level details), and, also because their experiencein the domain allows them to resolve the ambiguitiesimmediately.
– They incorporate insufficient information about theprocedure they model. They represent the sequencing ofactivities, but, in most cases, the information about eachactivity is reduced to a title. To correctly understand thenature of the activities and the process, it is necessaryto read and study additional documentation representedin natural language.
These problems can make the task of interpreting hospitalprotocols a bit tricky both by health personnel and auditors.However, the biggest drawback lies in the developmentof software applications that are capable of interpretingthese protocols to supply computer support to humanactors. These software applications need representations ina formal language and unambiguous models as complete aspossible to be interpreted automatically.
In recent years, the authors developed the BPMNE2notation [28], an extension of the BPMN standard (BusinessProcess Model and Notation) [21] that provides directsupport for HACCP (Hazard Analysis and Critical ControlPoints) [25]. The HACCP system can be characterised asa preventive methodological process aimed at identifyingspecific hazards and defining measures for their controlin the processes inherent to the life cycle (elaboration,processing, and distribution, among others) of products forhuman [20]. This methodology is increasingly used in thehealth field.
The use of BPMNE2 in flowcharts of a formal natureenhance the readability from the perspective of the humanuser. This notation includes elements that allow moregraphic information to be included in the flowcharts,making them more useful both for human users and for thesoftware applications. In this way, BPMNE2 can be seen asan option that can contribute to solving the problems presentin the flowcharts usually present in hospital environments.
This article extends the work presented at the WorldCIST2018 congress [27]. In particular, it describes a proposalto adapt the BPMNE2 notation for a hospital context andexposes the results of a validation carried out with thesupport of a group of auditors and experts in the domain.In the following section, the most remarkable related worksare described. Section “Proposal”, presents the adaptationof the developed notation that the interested reader cancomplement with [28]. Section “Validation” discussesthe validation of the proposal introduciong a particularapplication case in a real context. Finally, the conclusions ofthis work are discussed in Section “Conclusions”.
Related work
For years, the most commonly used notation for therepresentation of flowcharts in hospital environments wasthe standard ISO 5807:1985 [17]. This notation definessymbols to describe processes and gives guidance onconventions about data flowcharts, and program networkcharts, among others. Despite its popularity within thehospital processes, partly thanks to its simplicity, it doesnot allow to express in detail relevant features, in particularthose related to HACCP based models.
For years, several works have tried to improve therepresentation of information related to medical procedures.In this line, [16] suggests representing medical informationthat supports human review, decision support applications,ad-hoc queries, statistical analysis, and natural languageprocessing. However, it does not pay attention to thegraphical representation, a fundamental feature to forhuman users. In the same line, [14] must be acknowledged.This work also provides an analysis of a ComputationalModeling of Medical Concepts since it understands thatthe representation of data structures will be crucial for thedevelopment of computer based applications. In this aspect,it matches with the gist of our proposal.
In recent years, many alternatives to ISO 5807:1985 hasbeen proposed. This is the case, for example, of [26], whichuses the Unified Modeling Language (UML) to describe theinteraction among involved entities. Other approaches haveproposed the use of semantic technologies, in particular,OWL ontologies [12, 33]. Likewise, in [19] it is showna review of other alternatives to support the healthcaredomain such as YAWL, FLOWer, ADEPT and DECLARE.However, undoubtedly, the most used base notation isBPMN. Its importance in the medical field is clear, both atsimulation level [22] (see [18]), and in practical contexts[7, 24]. According to these papers, the flexible architecturederived from the use of BPMN supports the creation ofdifferent perspectives and enables the creation of ad-hocstereotypes for a specific field. In this line, a large numberof proposals have been made to extend BPMN to improverepresentativeness in different clinical contexts. Domain-specific concepts about Clinical Pathways are proposedin [7, 8] by establishing different types of activities andstereotypes related to diagnosis, therapy or support. In[31] it is proposed a new way to represent clinical careprocesses with the objective of identifying high-cost tasksor stays. Similarly, other works (such as [23]) focus onthe application of Process Mining techniques. In othercontributions, the focus has been placed on different aspectsrelated to security [29] or on the measurement of KPIs (KeyPerformance Indicators) [13]. These proposals are BPMNadaptations to solve problems in particular applicationcontexts.

J Med Syst (2018) 42:181 Page 3 of 10 181
It may be stated that the most commonly used notationis ISO 5807:1985. The existing alternatives (many of thembased on BPMN) directly tackle some of the identifieddeficiencies, improving the ability to represent informationin specific-contexts and providing a notation interpretableby machines. However, no proposal allows representingcritical information in hospital processes for the monitoringand traceability of drugs. This information is crucial forauditing processes, a key mechanism for assessing qualityand ensuring adherence to protocols.
Proposal
The notation proposed in this article is based on thework previously done by the authors in [28]. This workpresents BPMNE2, an extension for the BPMN languagethat supports the representation of information commonlyused by experts in the hazard analysis and critical controlpoints domain. The extension addresses two pre-establishedkey requirements: i) transfer the most relevant informationpresented in natural language to a machine-understandablerepresentation and ii) improve the visual representation forhuman users.
The application of BPMNE2 to hospital environmentsrequires the assimilation of the fundamental principles ofthis context to actually meet the HACCP philosophy. Thisrisk management methodology is gaining momentum in thehealth field [2] and imposes the adoption of certain artefacts.These artefacts are intended to represent more naturally theactual workflow of hospital staff and auditors. In particular,the concepts of Control Point (CP), Critical Control Point(CCP) and Monitoring Point (MP) emerge as fundamental.
BPMNE2 can be considered as a very suitable option asit supports all required artefacts and allows graphicallyrepresenting the most relevant elements within HACCP.
After the initial meetings with the experts, the need toadapt some of the graphic elements defined in BPMNE2,as well as certain parts of its vocabulary, becameevident. These modifications facilitate the description andunderstanding of specific hospital processes. In this way, aseries of changes are introduced:
– Monitoring Point (MP). It represents a point ofmeasurement of a variable or a set of variables thattakes place at a specific time in the workflow (i.e., in anactivity) (cf. Fig. 1a)
– Activity Effect. It represents the effect that an activitycauses on the product when this activity takes place(cf. Fig. 1b). This description was usually presented innatural language documents attached to the flowchart.
– Activity Duration. It describes the estimated timerequired for an activity to be completed (cf. Fig. 1c).
– Control Point (CP) and Critical Control Point(CCP). They establish the precise place where theHACCP plan defines the situation of a CP or a CCP aswell as the critical limit that must be satisfied at thatpoint (cf. Fig. 1d).
With these changes, two fundamental concepts areemphasised in this type of hospital processes: the ControlPoints and the Critical Control Points. The inclusion ofthese points in strategic places of the flowchart has a directimplication on the safety of the patient and the clinicalstaff. With this notation, auditors can identify these pointsimmediately only by looking at the flowchart, as well asunderstanding the requirements demanded. This feature was
Fig. 1 BPMNE2 elementexamples
Variable1Variable2
...
Task with amonitoring point
Monitoring point
{modification}
Task that modifiesthe charcteristics of
the product
Activity Effect
{Time}
Task that takes a
specific time to be
completed
Activity Duration
{Condition}
{Condition}
Task with aControl Point
Task with aCritical Control
Point
Control Point and Critical Control Point
a b
c d

181 Page 4 of 10 J Med Syst (2018) 42:181
Check theconformance
between medicationand prescription
Reception ofmedication
yes
no
Return topharmacy
Handwashing PPE*
collocation
Urinary catheter administration
Intravenous administration
Subcutaneous administration
Ophthalmic administration
Prepare purgingand clamping of
the HD* shaft
Check purging andclamping of the
HD* shaft
Place CDTS* and
needle Place CDTS*
Prepareadministration
no
yes
Purgingadminsitration line
Connect the HD*with to the
administration line
Place towel underthe administration
line
Administration
Pull backPPEs*
Handwashing
Wastemanagement
Inspect usedequipment
Check usedequipment
Manage thebreaks in PPEs
¿conformace?
¿conformace?
no
yes
¿conformace?
*PPE = Personal Protective Equipment *HD = Hazarous Drug
*CDTS = Closed Drugs Transfer System
Fig. 2 The ISO 5807:1985 notation applied in the flowchart

J Med Syst (2018) 42:181 Page 5 of 10 181
Check theconformance
between medicationand prescription
Reception ofmedication
OK
Not OK
Return topharmacy
Handwashing PPE*collocation
Prepare purgingand clamping of
the HD* shaft
Check purgingand clamping of
the HD* shaft
PlaceCDTS* and
needle Place CDTS*
Prepareadministration
Not OK
OK
Purgingadminsitration
line
Connect theHD* with to theadministration
line
Place towelunder the
administrationline
Administration
Pull backPPEs*
Handwashing
Prescription.patient = PatientID
AdministrationPatientID
Prescription
equipment = 'PPE4'
?Administration='intravenous'
PurgingClamping
?Administration='urinary catheter'
?Administration=
'ophthalmic'
?Administration='subcutaneous'
Wastemanagement
10 min
Purging = 'ok'Clamping = 'ok'
WasteHourDate
HourVolume
Time
Time
equipment = ''
Inspect usedequipment Breaks
Check usedequipment
Breaks = 'no'
OKManage thebreaks in PPEs
Not OK
*PPE = Personal Protective Equipment*HD = Hazarous Drug
*CDTS = Closed Drugs Transfer System
Fig. 3 New proposed notation applied in the flowchart

181 Page 6 of 10 J Med Syst (2018) 42:181
considered of great importance by the experts in the domainduring the meetings held.
Validation
To validate this proposal it was decided to carry out anactual deployment for the management of hazardous drugs(HDs). HDs are those drugs whose handling poses a dangerto people (carcinogenicity, teratogenicity, genotoxicity, etc.)[11]. This is a very sensitive area in which there aresignificant deficiencies and needs for standardization. Asshown in the systematic review presented by the authors in[6], there are currently no globally harmonized protocols forthe handling and risk of exposure to HDs [30], nor adequatecomputer systems that allow managing its quality and itstraceability.
The authors participate in a national research projectconcerned in supporting solutions to alleviate these short-comings. In this project, the researchers of the bio-sanitaryfield focus their efforts on the identification of the stagesthat compose the life cycle of the HDs and, for each of them,action protocols are defined. These procedures are usuallymodelled using notation ISO 5807:1985 flowcharts.
Method
To verify the usability of our proposal, some of theseflowcharts represented with ISO 5807:1985 were convertedto BMPNE2. As an example, the Fig. 2 shows a flowdiagram corresponding to a fragment of the stage for HDadministration and its transformed version in the suggestedmodel is presented in the Fig. 3.
To estimate the acceptance, once presented to the experts,a study based on the well-known System Usability Scale(SUS) [9] was carried out. The SUS consists of a ten-itemquestionnaire that uses a Likert scale (from 1 = “stronglydisagree” to 5 = “strongly agree”) to provide a global viewof subjective assessments of usability. This scale has beenused in more than 3500 jobs, and publications [4, 5] toevaluate a wide range of products and services. From theanswers obtained, the SUS score is calculated to establishhow good or bad the system usability is [4, 10] (cf. Fig. 4).
To ensure the fitness of the test to this case, a minimaladaptation of the original questionnaire was conducted (cf.Table 1). In addition to the ten questions defined in the SUSquestionnaire, and in order to receive more feedback, twonew questions were included (cf. Table 2).
To measure the internal consistency of the answers, theCronbach’s alpha coefficient [15] will be used. Values above0.7 are acceptable (cf. Table 3).
A
B
C
D
AC
CE
PTA
BL
EM
AR
GIN
AL
F
NO
T A
CC
EP
TAB
LE
100
90
60
30
20
SCOREGRADE RANGE
80
70
50
40
10
0Fig. 4 System Usability Scale: grade, score and range
Results
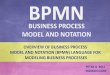
The questionnaire was sent to several groups of practitionersand auditors of hospital processes who, after a brief useof the proposed model, completed the survey previouslydescribed resulting in 47 valid answers. The results arepresented in the Fig. 5 and in the Table 4. It is interesting tolook individually at the results of some of the base questionsof the SUS questionnaire. Question Q1 (I think that I wouldlike to use this notation frequently) obtained the best score(i.e., the one most heeled to the expected side). Likewise, thequestion Q2 (I found the notation unnecessarily complex)obtained the score furthest from the expected value.
The resultant SUS Score is 71.064, which correspondsto an acceptable level of usability, in particular with agrade C (cf. Fig. 4). Also, question Q11 shows that 36people (76.6 %) would prefer to migrate to the new notation

J Med Syst (2018) 42:181 Page 7 of 10 181
Table 1 Original and adapted questionnaire
Original questionnaire Adapted questionnaire
Q1 I think that I would like to use this system frequently I think that I would like to use this notation frequently
Q2 I found the system unnecessarily complex I found the notation unnecessarily complex
Q3 I thought the system was easy to use I thought the notation was easy to understand
Q4 I think that I would need thesupport of a technical person tobe able to use this system
I think that I would need thesupport of a technical personto be able to understand thisnotation
Q5 I found the various functions inthis system were well integrated
I found the various introduced elements in this system were well integrated
Q6 I thought there was too much inconsistency in this system I thought there was too much inconsistency in this notation
Q7 I would imagine that most peoplewould learn to use this systemvery quickly
I would imagine that most peoplewould learn to understand thisnotation very quickly
Q8 I found the system very cumbersome to use I found the notation very cumbersome to understand
Q9 I felt very confident using the system I felt very confident using the notation
Q10 I needed to learn a lot of thingsbefore I could get going with thissystem
I needed to learn a lot of things before I could get going with this notation
while 11 (23.4%) would choose to continue using thecurrent notation. Question Q12 offers interesting subjectiveassessments discussed in the next section. The response tothe question Q12 is not mandatory. In this case, 24 people(51.1%) have completed the response to this question.
As for the study of Cronbach’s alpha, we have obtaineda value of α = 0.871, which corresponds to a goodinternal consistency of the answers. The reader can checkthe interpretation of this coefficient in Table 3.
Discussion
At first glance, a broad comparison of both workflowsallows appreciating the increase of information offered withthe new notation. In particular, CPs and CCPs can be easilynoted and, therefore, those activities that are critical for theprocedure can be identified with no effort. Likewise, thepoints in which a monitorization of the characteristics of theproduct is carried out are also perfectly identified and allpossible ambiguities are eliminated.
Table 2 Extra questions
Q11 Would you prefer to continue usingthe current notation or would youlike to migrate to the new notation?
Q12 What positive and negative aspectsdo you find in the new notation?
Another issue in the original model is related to forksin the execution (p.e., after the activities such as “PPECollocation” and “Administration”). In those cases, it is notpossible to distinguish whether it is a parallel execution oran activity that progresses through just one of the availableoptions. This can be solved using the BPMN stereotypes“Parallel Gateway” and “Exclusive Gateway”, respectively.Also, another advantage from using a BPMN-based notationthat cannot be seen visually is the capacity to generate aformal representation in XML that can be easily interpretedby machines to enable its later processing by softwareagents.
The experts surveyed have shown the usefulness of thenew notation for the final user. Although the usabilityobtained (grade C) is not optimal, the answers to questionQ11 show that the vast majority (76.6%) of experts prefer tomigrate to the new notation. These results can be considered
Table 3 Chronbach’s alpha coefficient interpretation
Cronbach’s alpha Internal consistency
0.9 ≤ α Excellent
0.8 ≤ α < 0.9 Good
0.7 ≤ α < 0.8 Acceptable
0.6 ≤ α < 0.7 Questionable
0.5 ≤ α < 0.6 Poor
α < 0.5 Unacceptable
181 Page 8 of 10 J Med Syst (2018) 42:181
Fig. 5 Boxplot for the responsesto the SUS questionnaire
a success especially taking into account the initial reluctanceto changes present in any organisation.
A careful review of the comments collected in questionQ12 suggests some weak and strong points worth noting:
– In general, the increase in information represented inthe flowchart is recognised as a positive aspect. Eventhough, some cases can present a slight visual rechargeas a secondary effect.
– It is also admitted that in the short term there may be aninevitable learning curve (as in any system change), butthat it will be worth in the end due to the improvementspreviously described.
– Also, to a lesser extent, some comments state that thenew notation is friendlier, improves the efficiency ofthe work and that it seems a good starting point for thetraining of new staff.
– Some opinions suggest that certain stereotypes caneasily be confused with each other.
– In general terms, it is agreed that these new modelsmake more visible the critical aspects of the process thatmay pose a risk to the lives of patients and workers.Therefore, its usage is highly recommended.
Table 4 Main statistics for the responses to the SUS questionnaire
Mean Standard deviation Median
Q1 4.106 0,866 4
Q2 2.340 1,147 2
Q3 3.723 1,192 4
Q4 2.213 1,160 2
Q5 3.979 1,032 4
Q6 2.170 1,070 2
Q7 3.915 1,060 4
Q8 2.255 1,224 2
Q9 3.809 0,947 4
Q10 2.128 1,076 2
Conclusions
In the present work, the drawbacks regularly present inflowcharts used for the modelling of hospital protocolshave been shown. To solve them, it has been proposed touse a version adapted to the hospital environments of theBPMNE2 notation, an extension to the BPMN languagethat has been developed in recent years by the authors. Itwas explicitly designed to support the HACCP system, tobe intuitive for human beings and easily processable bysoftware agents.
The proposed adaptation was born from a series ofmeetings with experts in the hospital domain who havehelped to identify the concrete modelling needs presentedin the context procedures. In particular, special attentionhas been paid to concepts such as CP and CCP, bothfundamental to control the safety of clinical staff, patientsand medications.
Through a proof of concept in the scenario of HDs,the expressive benefits of the proposal and its practicalviability have been assessed. Although any change has toovercome inertia, the results obtained through the SUSquestionnaire allow being optimistic regarding its practicalimplementation.
As future lines, two main issues are set. Firstly, todevelop a tool that allows editing of the new flowdiagrams in a simple way. In this line, the integrationwith the platform Tracking of Control Points (ToCP) [1, 3]developed previously by the authors is planned. On theother hand, the development of new software techniquesthat use the new information represented now in a formatinterpretable by machines is intended. This opens the doorto a large number of analyses, mainly: reducing humanerrors, finding new behaviours and patterns unknown todate, predicting dangerous situations before they occur orproposing a workflow enrichment by analysing the pathsfollowed by the already executed process instances. It isvery interesting to study the software techniques under the

J Med Syst (2018) 42:181 Page 9 of 10 181
scope of Process Mining [32], in particular, those relatedto Conformance Checking. The latter focuses its efforts onverifying the adherence of the execution of a procedure withrespect to the predefined theoretical flow diagram and cansuppose a significant improvement in the audit and qualitymanagement processes.
Funding This work has been partially funded by Instituto de SaludCarlos III through the PI16/00788 project (Quality control andtraceability of biohazardous medicinal products (BPM) through theHospital at Home using Big Data models applied to risk analysis).
Compliance with Ethical Standards
Conflict of interests Mateo Ramos-Merino declares that he has noconflict of interest. Luis M. Alvarez-Sabucedo declares that he hasno conflict of interest. Juan M. Santos-Gago declares that he has noconflict of interest. Javier Sanz-Valero declares that he has no conflictof interest.
Ethical approval This article does not contain any studies with humanparticipants or animals performed by any of the authors.
References
1. Alonso-Rorıs, V. M., Alvarez-Sabucedo, L., Santos-Gago, J. M.,and Ramos-Merino, M., Towards a cost-effective and reusabletraceability system. A semantic approach. Comput. Ind. 83:1–11,2016.
2. Alonso-Rorıs, V. M., Santos-Gago, J. M., Alvarez-Sabucedo,L. M., Ramos-Merino, M., and Sanz-Valero, J., An ICT-basedplatform to monitor protocols in the healthcare environment. J.Med. Syst. 40(10):225, 2016.
3. Alonso-Rorıs, V. M. A., Sabucedo, L. M. A., Wanden-Berghe,C., Gago, J. M. S., and Sanz-Valero, J., Towards a mobile-basedplatform for traceability control and hazard analysis in the contextof parenteral nutrition: description of a framework and a prototypeapp. JMIR Res. Protocols. 5(2), 2016.
4. Bangor, A., Kortum, P., and Miller, J., Determining whatindividual SUS scores mean: Adding an adjective rating scale. J.Usab. Stud. 4(3):114–123, 2009.
5. Bangor, A., Kortum, P. T., and Miller, J. T., An empiricalevaluation of the system usability scale. Intl. J. Human–Comput.Interact. 24(6):574–594, 2008.
6. Bernabeu-Martınez, M. A., Ramos-Merino, M., Santos-Gago, J.M., Alvarez-Sabucedo, L. M., Wanden-Berghe, C., and Sanz-Valero, J., Guidelines for safe handling of hazardous drugs: Asystematic review. PloS One 13(5):e0197172, 2018.
7. Braun, R., Burwitz, M., Schlieter, H., and Benedict, M., Clinicalprocesses from various angles-amplifying BPMN for integratedhospital management. In: 2015 IEEE International Conferenceon Bioinformatics and Biomedicine (BIBM), pp. 837–845. IEEE,2015.
8. Braun, R., Schlieter, H., Burwitz, M., and Esswein, W.,BPMN4CP revised - extending BPMN for multi-perspectivemodeling of clinical pathways. In: 2016 49th Hawaii InternationalConference on System Sciences (HICSS), pp. 3249–3258. IEEE,2016.
9. Brooke, J., SUS: A retrospective. J. Usab. Stud.s 8(2):29–40,2013.
10. Brooke, J. et al., SUS - A quick and dirty usability scale. Usab.Eval. Indus. 189(194):4–7, 1996.
11. Connor, T. H., and McDiarmid, M. A., Preventing occupationalexposures to antineoplastic drugs in health care settings. CA:Cancer J. Clinicians 56(6):354–365, 2006.
12. Dang, J., Hedayati, A., Hampel, K., and Toklu, C., An ontologicalknowledge framework for adaptive medical workflow. J. Biomed.Inform. 41(5):829–836, 2008.
13. Di Leva, A., Sulis, E., and Vinai, M., Business process analysisand simulation: The contact center of a public health and socialinformation office. Intell. Inf. Manag. 9(05):189, 2017.
14. Evans, D. A., Cimino, J. J., Hersh, W. R., Huff, S. M., Bell,D. S., and Group, C., Toward a medical-concept representationlanguage. J. Amer. Med. Inf. Assoc. 1(3):207–217, 1994.
15. Gliem, J. A., and Gliem, R. R., Calculating, interpreting, andreporting Cronbach’s alpha reliability coefficient for Likert-type scales. Midwest Research-to-Practice Conference in Adult,Continuing, and Community Education, 2003.
16. Huff, S. M., Rocha, R. A., Bray, B. E., Warner, H. R., and Haug, P.J., An event model of medical information representation. J. Am.Med. Inform. Assoc. 2(2):116–134, 1995.
17. ISO, ISO 5807:1985: Information processing - Documentationsymbols and conventions for data, program and system flowcharts,program network charts and system resources charts Standard,1985.
18. Kunkler, K., The role of medical simulation: An overview. Int. J.Med. Robot. Comput. Assisted Surgery 2(3):203–210, 2006.
19. Mans, R., Workflow support for the healthcare domain. Technis-che Universiteit Eindhoven, 2011.
20. Mortimore, S., and Wallace, C., An introduction to HACCP. In:HACCP, pp. 1–11. Springer, 1998.
21. OMG, Business process model and notation (BPMN) version 2.0,2011.
22. Onggo, B. S. S., Proudlove, N., D’Ambrogio, S., Calabrese,A., Bisogno, S., and Levialdi Ghiron, N., A BPMN extensionto support discrete-event simulation for healthcare applications:An explicit representation of queues, attributes and data-drivendecision points. J. Oper. Res. Soc. 69(5):788–802, 2018.
23. Partington, A., Wynn, M., Suriadi, S., Ouyang, C., and Karnon,J., Process mining for clinical processes: A comparative analysisof four Australian hospitals. ACM Trans. Manag. Inf. Syst. (TMIS)5(4):19, 2015.
24. Patkar, V., South, M., and Thomson, R., From guidelines tocarefflows: Modelling and supporting complex clinical processes.Comput.-Based Med. Guidelines Protocols: Primer Curr. Trends139:44–62, 2008.
25. Pierson, M. D., HACCP: principles and applications. SpringerScience & Business Media, 2012.
26. Ramaiah, M., Subrahmanian, E., Sriram, R. D., and Lide, B. B.,Workflow and electronic health records in small medical practices.Perspectives in Health Information Management/AHIMA Ameri-can Health Information Management Association 9(Spring), 2012.
27. Ramos-Merino, M., Alvarez-Sabucedo, L. M., Santos-Gago, J.M., and Alonso-Rorıs, V. M., A BPMN extension for theannotation of HACCP plans in hospital protocols. In: WorldConference on Information Systems and Technologies, pp. 606–615. Springer, 2018.
28. Ramos-Merino, M., Santos-Gago, J. M., Alvarez-Sabucedo, L.M., Alonso-Roris, V. M., and Sanz-Valero, J., BPMN-E2: ABPMN extension for an enhanced workflow description. Softw.Syst. Model. 1–21, 2018.
29. Sang, K. S., and Zhou, B., BPMN security extensionsfor healthcare process. In: 2015 IEEE International Con-ference on Computer and Information Technology; Ubiqui-tous Computing and Communications; Dependable, Autonomic

181 Page 10 of 10 J Med Syst (2018) 42:181
and Secure Computing; Pervasive Intelligence and Computing(CIT/IUCC/DASC/PICOM), pp. 2340–2345. IEEE, 2015.
30. Sessink, P., Sewell, G., and Vandenbroucke, J., Preventingoccupational exposure to cytotoxic and other hazardous drugsEuropean policy recommendations, 2015.
31. Strasser, M., Pfeifer, F., Helm, E., Schuler, A., and Altmann, J.,Defining and reconstructing clinical processes based on IHE andBPMN 2.0. Stud. Health Technolo. Inf. 169:482–486, 2011.
32. Van Der Aalst, W., Adriansyah, A., De Medeiros, A. K. A.,Arcieri, F., Baier, T., Blickle, T., Bose, J. C., van den Brand,P., Brandtjen, R., Buijs, J. et al., Process mining manifesto. In:International Conference on Business Process Management, pp.169–194. Springer, 2011.
33. Yao, W., and Kumar, A., Conflexflow: Integrating flexible clinicalpathways into clinical decision support systems using context andrules. Decis. Support. Syst. 55(2):499–515, 2013.