Embed Size (px)
DESCRIPTION
A Brief History of Tufts Medical Center. 1796: Boston Dispensary founded. 1981: World’s first pediatric trauma center established at the Floating Hospital. 1894: Floating Hospital takes ill children & mothers out on Boston Harbor. Notable benefactors: Sam Adams & Paul Revere - PowerPoint PPT Presentation
Citation preview
1Combining Art & Science, Innovations in Healthcare II, June 19, 2009
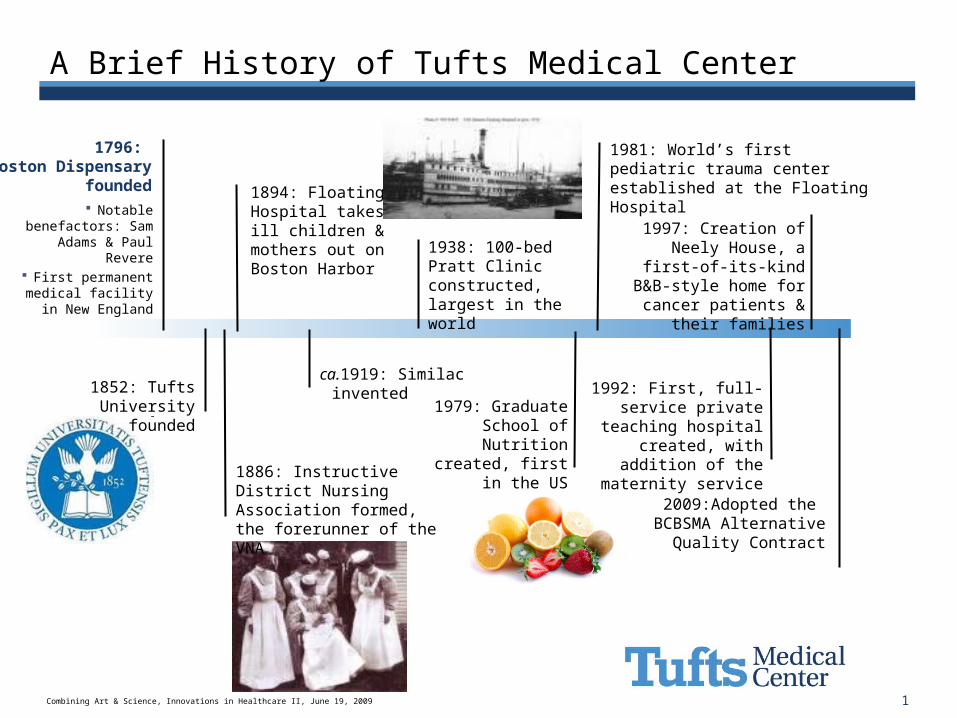
A Brief History of Tufts Medical Center
1894: Floating Hospital takes ill children & mothers out on Boston Harbor
1979: Graduate School of
Nutrition created, first in the US
1796: Boston Dispensary
founded
1981: World’s first pediatric trauma center established at the Floating Hospital
Notable benefactors: Sam
Adams & Paul Revere
First permanent medical facility in
New England
1886: Instructive District Nursing Association formed, the forerunner of the VNA
ca.1919: Similac invented
1938: 100-bed Pratt Clinic constructed, largest in the world
1997: Creation of Neely House, a first-of-its-kind
B&B-style home for cancer patients & their
families
2009:Adopted the BCBSMA Alternative
Quality Contract
1992: First, full-service private
teaching hospital created, with
addition of the maternity service
1852: Tufts University founded
The principal teaching hospital for Tufts University School of Medicine
Combining Art and Science to Create Value for Patients and Staff
Margaret M. Vosburgh, EVP, COOJune 19, 2009
3Combining Art & Science, Innovations in Healthcare II, June 19, 2009
What is value1?
A fair return or equivalent in good and services, or money for something exchanged
1 value. (2009). In Merriam-Webster Online Dictionary.Retrieved June 16, 2009, from http://www.merriam-webster.com/dictionary/value
4Combining Art & Science, Innovations in Healthcare II, June 19, 2009
Defining our Value Proposition
Patients and Families
Access to world-class healthcare Welcoming, calm environment
Physicians
Cases Reliable processes Educational experiences for medical students,
residents, and fellows
Staff
Predictable environment Support to provide top-notch service
5Combining Art & Science, Innovations in Healthcare II, June 19, 2009
The ART and SCIENCE
Trust Relationships Safety Compassion
Best Practices Voice of the
Customer Lean and Six Sigma Outcomes
Art Science
6Combining Art & Science, Innovations in Healthcare II, June 19, 2009
Throughput

7Combining Art & Science, Innovations in Healthcare II, June 19, 2009
Previous State of Hospital Throughput
?
?
?
?
?
8Combining Art & Science, Innovations in Healthcare II, June 19, 2009
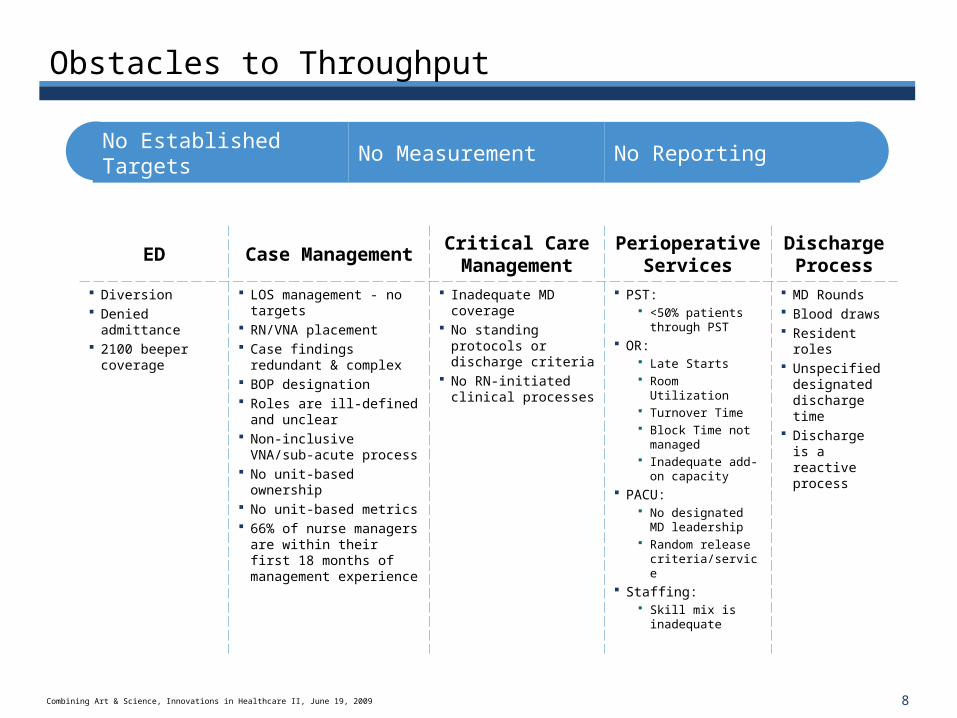
Obstacles to Throughput
EDCase
ManagementCritical Care Management
Perioperative Services
Discharge Process
Diversion Denied
admittance 2100 beeper
coverage
LOS management - no targets
RN/VNA placement Case findings redundant
& complex BOP designation Roles are ill-defined and
unclear Non-inclusive VNA/sub-
acute process No unit-based ownership No unit-based metrics 66% of nurse managers
are within their first 18 months of management experience
Inadequate MD coverage
No standing protocols or discharge criteria
No RN-initiated clinical processes
PST: <50% patients
through PST OR:
Late Starts Room Utilization Turnover Time Block Time not
managed Inadequate add-
on capacity PACU:
No designated MD leadership
Random release criteria/service
Staffing: Skill mix is
inadequate
MD Rounds Blood draws Resident roles Unspecified
designated discharge time
Discharge is a reactive process
No Established Targets
No Measurement No Reporting
9Combining Art & Science, Innovations in Healthcare II, June 19, 2009
Optimization Task Force
Purpose To fast track organizational change by having process
owners analyze current systems and propose alternatives.
Participants MD, RN, and Staff leaders from across the hospital
Process Standing meetings and agenda report outs Formal template, complete for presentation
10Combining Art & Science, Innovations in Healthcare II, June 19, 2009
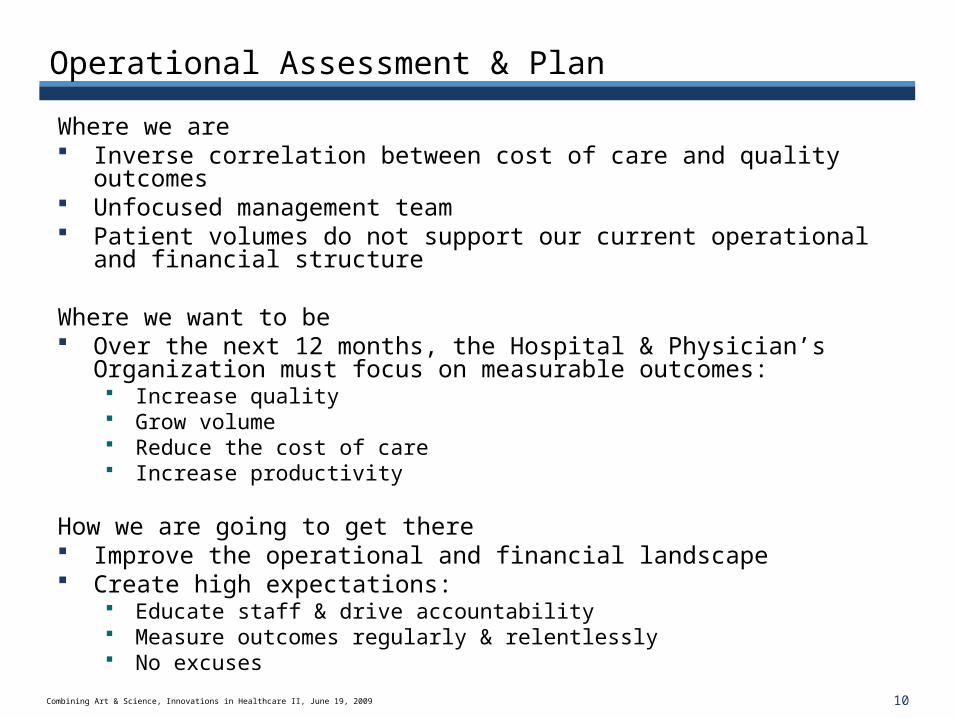
Operational Assessment & Plan
Where we are Inverse correlation between cost of care and quality outcomes Unfocused management team Patient volumes do not support our current operational and
financial structure
Where we want to be Over the next 12 months, the Hospital & Physician’s Organization
must focus on measurable outcomes: Increase quality Grow volume Reduce the cost of care Increase productivity
How we are going to get there Improve the operational and financial landscape Create high expectations:
Educate staff & drive accountability Measure outcomes regularly & relentlessly No excuses
11Combining Art & Science, Innovations in Healthcare II, June 19, 2009
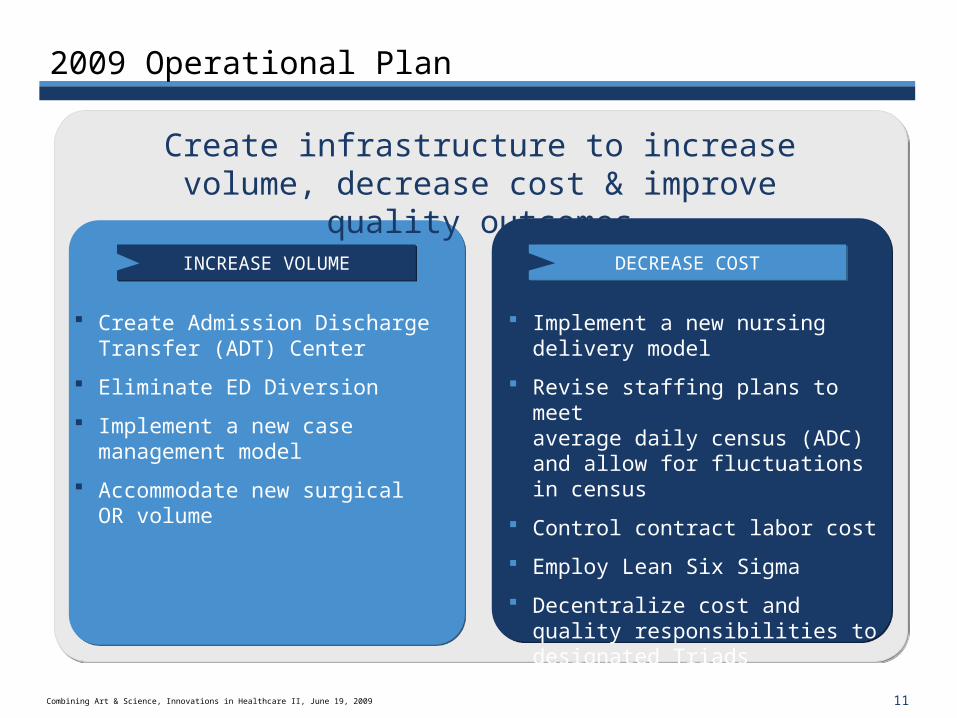
2009 Operational Plan
INCREASE VOLUMEINCREASE VOLUME DECREASE COSTDECREASE COST
Create Admission Discharge Transfer (ADT) Center
Eliminate ED Diversion
Implement a new case management model
Accommodate new surgical OR volume
Implement a new nursing delivery model
Revise staffing plans to meet average daily census (ADC) and allow for fluctuations in census
Control contract labor cost
Employ Lean Six Sigma
Decentralize cost and quality responsibilities to designated Triads
Create infrastructure to increase volume, decrease cost & improve quality outcomes
12Combining Art & Science, Innovations in Healthcare II, June 19, 2009
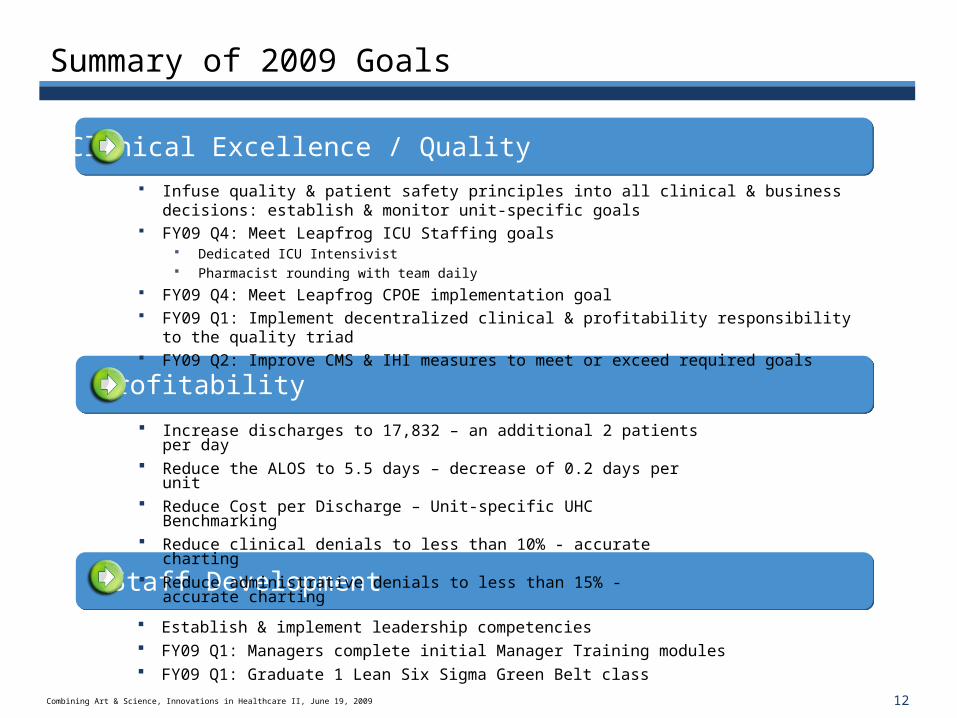
Summary of 2009 Goals
Staff Development
Clinical Excellence / Quality
Profitability
Establish & implement leadership competencies FY09 Q1: Managers complete initial Manager Training modules FY09 Q1: Graduate 1 Lean Six Sigma Green Belt class
Infuse quality & patient safety principles into all clinical & business decisions: establish & monitor unit-specific goals
FY09 Q4: Meet Leapfrog ICU Staffing goals Dedicated ICU Intensivist Pharmacist rounding with team daily
FY09 Q4: Meet Leapfrog CPOE implementation goal FY09 Q1: Implement decentralized clinical & profitability responsibility to the quality
triad FY09 Q2: Improve CMS & IHI measures to meet or exceed required goals
Increase discharges to 17,832 – an additional 2 patients per day Reduce the ALOS to 5.5 days – decrease of 0.2 days per unit Reduce Cost per Discharge – Unit-specific UHC Benchmarking Reduce clinical denials to less than 10% - accurate charting Reduce administrative denials to less than 15% - accurate
charting
13Combining Art & Science, Innovations in Healthcare II, June 19, 2009
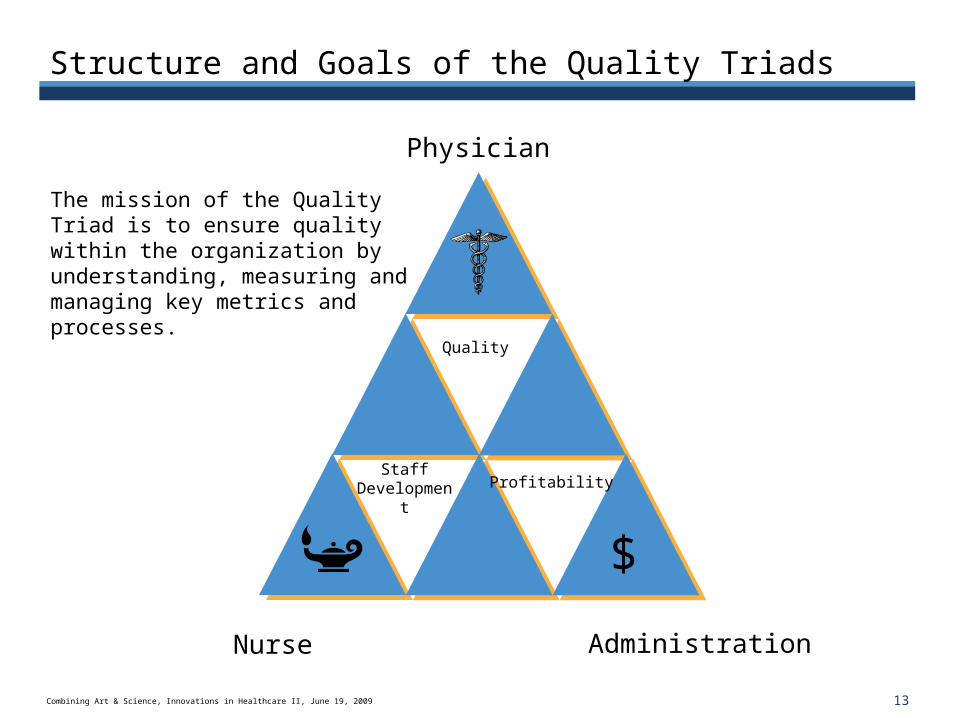
Structure and Goals of the Quality Triads
Quality
Profitability
Administration
Physician
Staff Development
Nurse
$
The mission of the Quality Triad is to ensure quality within the organization by understanding, measuring and managing key metrics and processes.
14Combining Art & Science, Innovations in Healthcare II, June 19, 2009
Foster a Culture of Quality
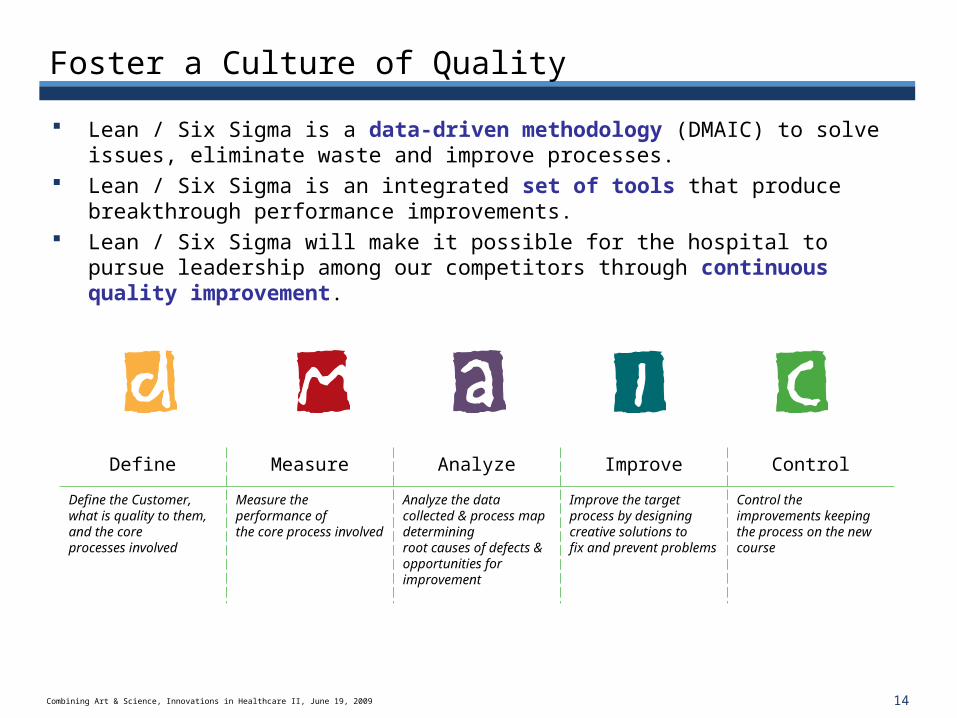
Lean / Six Sigma is a data-driven methodology (DMAIC) to solve issues, eliminate waste and improve processes.
Lean / Six Sigma is an integrated set of tools that produce breakthrough performance improvements.
Lean / Six Sigma will make it possible for the hospital to pursue leadership among our competitors through continuous quality improvement.
Define Measure Analyze Improve Control
Define the Customer, what is quality to them, and the core processes involved
Measure the performance of the core process involved
Analyze the data collected & process map determining root causes of defects & opportunities for improvement
Improve the target process by designing creative solutions to fix and prevent problems
Control the improvements keeping the process on the new course
15Combining Art & Science, Innovations in Healthcare II, June 19, 2009
Optimization Initiatives
ADT Center
Optimization Task Force
OR Leadership Forum
Critical Care Task Force
16Combining Art & Science, Innovations in Healthcare II, June 19, 2009
Solutions
ADT Center
Optimization Task Force Outpatient Scheduling Project Phlebotomy Improvement Project
OR Leadership Forum
Critical Care Task Force
17Combining Art & Science, Innovations in Healthcare II, June 19, 2009
I. ADT Center
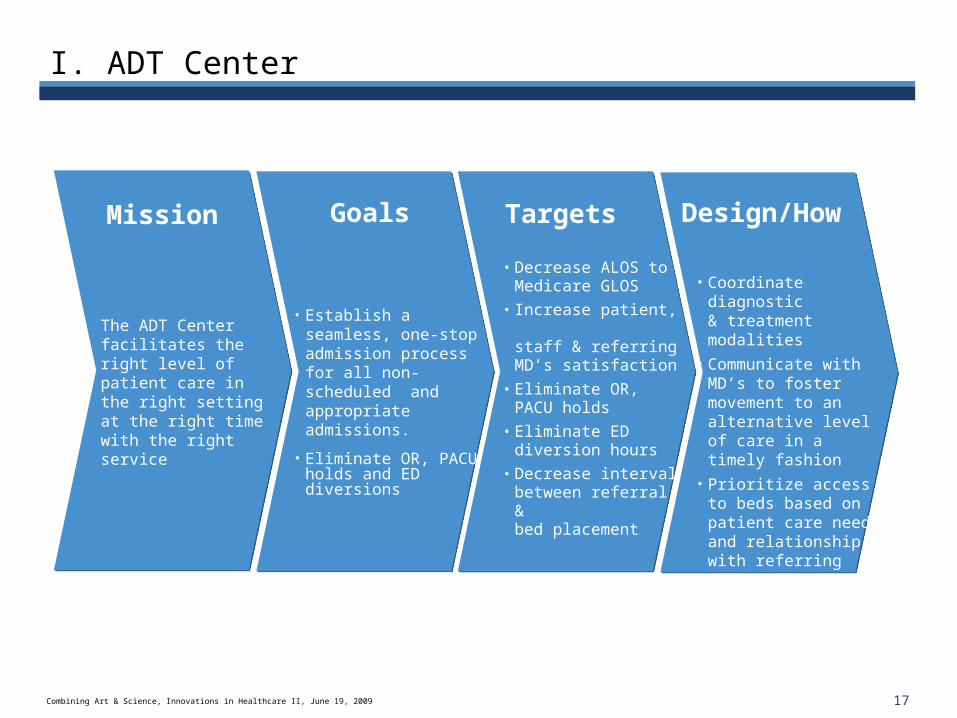
The ADT Center facilitates the right level of patient care in the right setting at the right time with the right service
• Establish a seamless, one-stop admission process for all non-scheduled and appropriate admissions.
• Eliminate OR, PACU holds and ED diversions
• Coordinate diagnostic & treatment modalities
• Communicate with MD’s to foster movement to an alternative level of care in a timely fashion
• Prioritize access to beds based on patient care need and relationship with referring party
Mission Goals Design/HowTargets
• Decrease ALOS to Medicare GLOS
• Increase patient, staff & referring MD’s satisfaction
• Eliminate OR, PACU holds
• Eliminate ED diversion hours
• Decrease interval between referral &bed placement
18Combining Art & Science, Innovations in Healthcare II, June 19, 2009
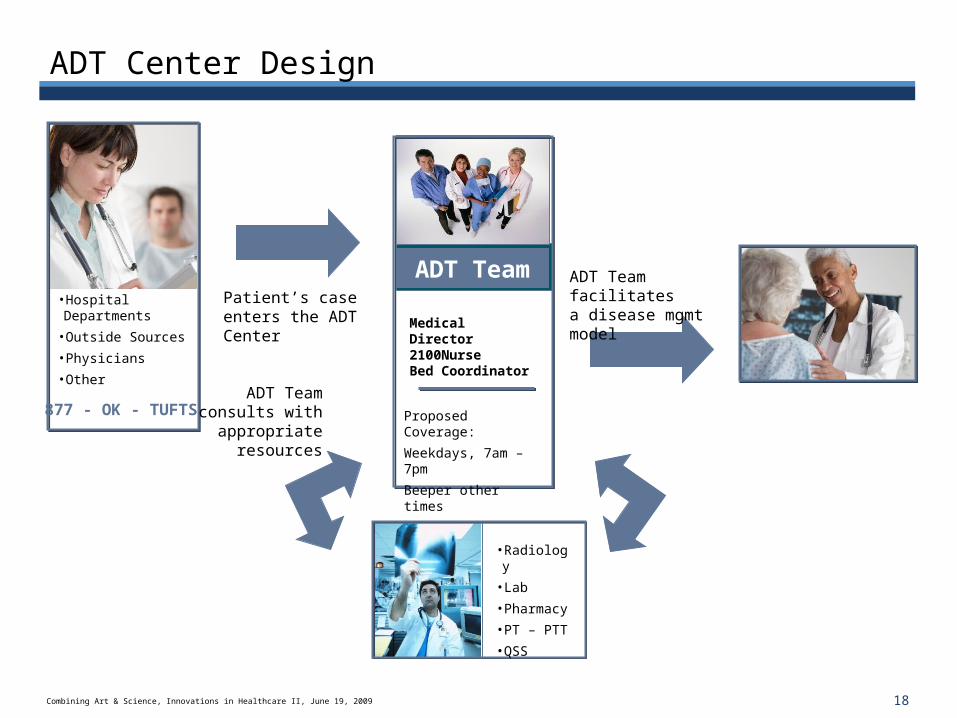
ADT Center Design
Patient’s case enters the ADT Center
ADT Team consults with
appropriate resources
ADT Team facilitates a disease mgmt model•Hospital Departments
•Outside Sources
•Physicians
•Other
•Radiology
•Lab
•Pharmacy
•PT – PTT
•QSS
ADT Team
Medical Director2100NurseBed Coordinator
Proposed Coverage:
Weekdays, 7am – 7pm
Beeper other times
877 - OK - TUFTS
19Combining Art & Science, Innovations in Healthcare II, June 19, 2009
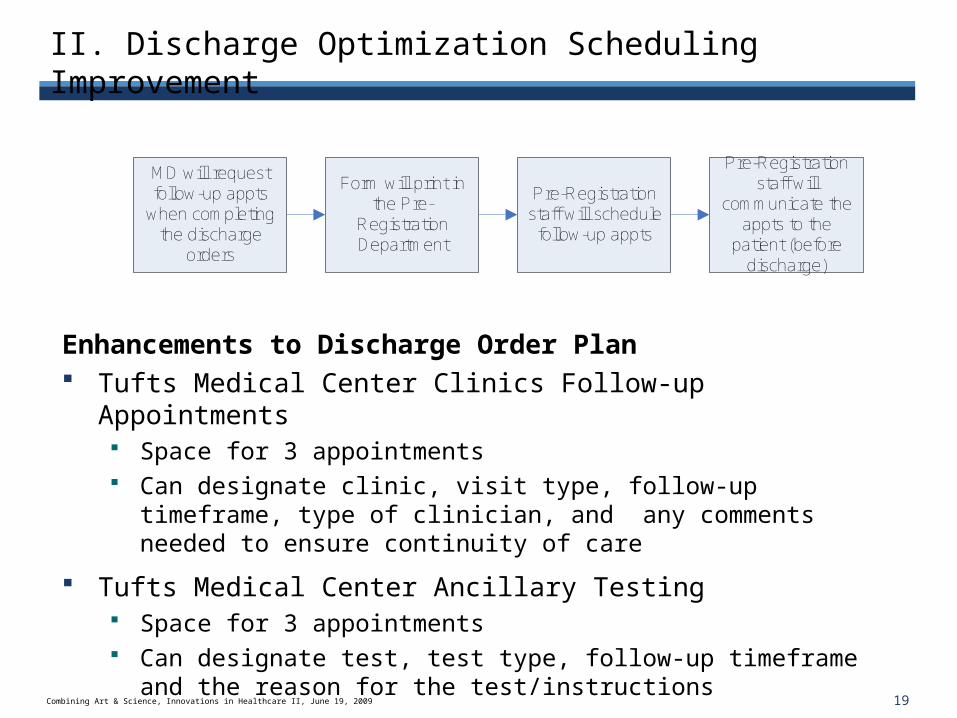
II. Discharge Optimization Scheduling Improvement
MD will request follow-up appts
when completing the discharge
orders
Form will print in the Pre-
Registration Department
Pre-Registration staff will schedule
follow-up appts
Pre-Registration staff will
communicate the appts to the
patient (before discharge)
Enhancements to Discharge Order Plan Tufts Medical Center Clinics Follow-up Appointments
Space for 3 appointments Can designate clinic, visit type, follow-up timeframe, type of
clinician, and any comments needed to ensure continuity of care
Tufts Medical Center Ancillary Testing Space for 3 appointments Can designate test, test type, follow-up timeframe and the
reason for the test/instructions

20Combining Art & Science, Innovations in Healthcare II, June 19, 2009
Discharge Orders
21Combining Art & Science, Innovations in Healthcare II, June 19, 2009
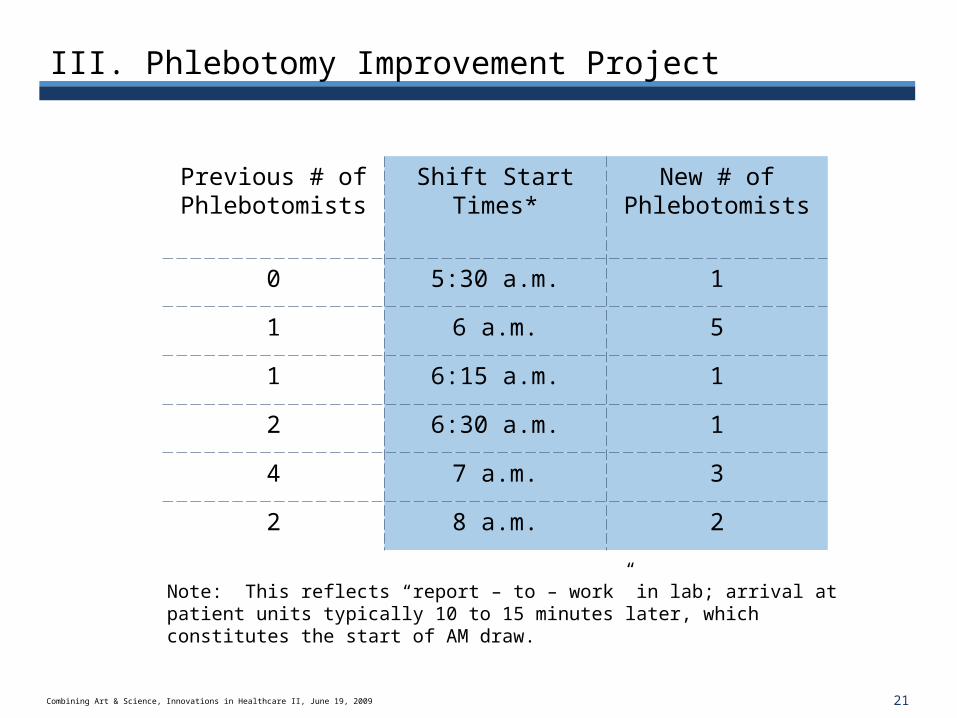
III. Phlebotomy Improvement Project
Previous # of Phlebotomists
Shift Start Times*
New # of Phlebotomists
0 5:30 a.m. 1
1 6 a.m. 5
1 6:15 a.m. 1
2 6:30 a.m. 1
4 7 a.m. 3
2 8 a.m. 2
Note: This reflects “report – to – work” in lab; arrival at patient units typically 10 to 15 minutes later, which constitutes the start of AM draw.
22Combining Art & Science, Innovations in Healthcare II, June 19, 2009
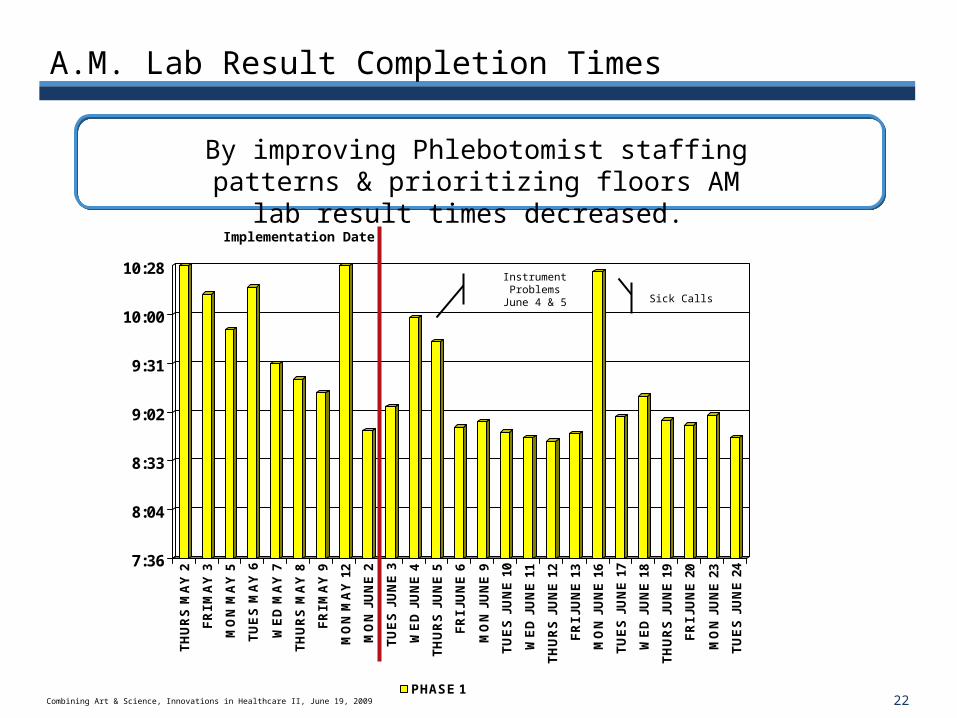
A.M. Lab Result Completion Times
7:36
8:04
8:33
9:02
9:31
10:00
10:28
TH
UR
S M
AY
2
FR
I M
AY
3
MO
N M
AY
5
TU
ES
MA
Y 6
WE
D M
AY
7
TH
UR
S M
AY
8
FR
I M
AY
9
MO
N M
AY
12
MO
N J
UN
E 2
TU
ES
JU
NE
3
WE
D J
UN
E 4
TH
UR
S J
UN
E 5
FR
I JU
NE
6
MO
N J
UN
E 9
TU
ES
JU
NE
10
WE
D J
UN
E 1
1
TH
UR
S J
UN
E 1
2
FR
I JU
NE
13
MO
N J
UN
E 1
6
TU
ES
JU
NE
17
WE
D J
UN
E 1
8
TH
UR
S J
UN
E 1
9
FR
I JU
NE
20
MO
N J
UN
E 2
3
TU
ES
JU
NE
24
PHASE 1
Sick Calls
Instrument ProblemsJune 4 & 5
Implementation Date
By improving Phlebotomist staffing patterns & prioritizing floors AM lab result times decreased.
23Combining Art & Science, Innovations in Healthcare II, June 19, 2009
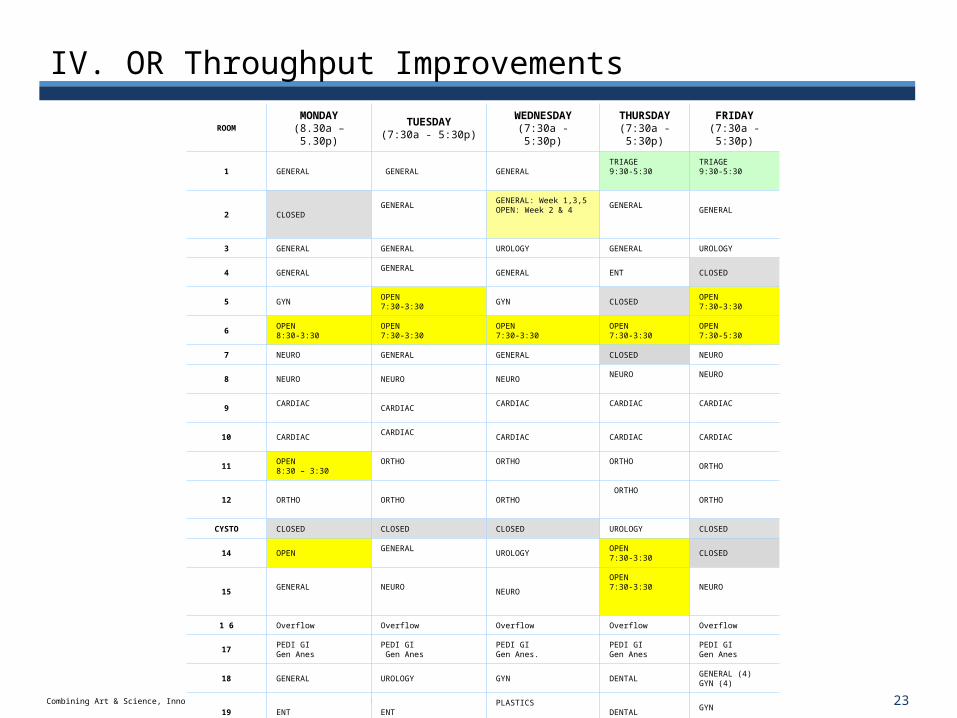
IV. OR Throughput Improvements
ROOMMONDAY
(8.30a – 5.30p)TUESDAY
(7:30a - 5:30p)WEDNESDAY(7:30a - 5:30p)
THURSDAY(7:30a - 5:30p)
FRIDAY(7:30a - 5:30p)
1 GENERAL GENERAL GENERAL TRIAGE9:30-5:30
TRIAGE9:30-5:30
2 CLOSEDGENERAL
GENERAL: Week 1,3,5OPEN: Week 2 & 4
GENERAL
GENERAL
3 GENERAL GENERAL UROLOGY GENERAL UROLOGY
4 GENERAL GENERAL GENERAL ENT CLOSED
5 GYN OPEN7:30-3:30
GYN CLOSEDOPEN7:30-3:30
6OPEN8:30-3:30
OPEN7:30-3:30
OPEN7:30-3:30
OPEN7:30-3:30
OPEN7:30-5:30
7 NEURO GENERAL GENERAL CLOSED NEURO
8 NEURO NEURO NEURO NEURO
NEURO
9CARDIAC
CARDIAC CARDIAC CARDIAC
CARDIAC
10 CARDIAC CARDIAC CARDIAC CARDIAC CARDIAC
11OPEN8:30 – 3:30
ORTHO ORTHO ORTHO
ORTHO
12 ORTHO ORTHO ORTHO ORTHO
ORTHO
CYSTO CLOSED CLOSED CLOSED UROLOGY CLOSED
14 OPENGENERAL
UROLOGYOPEN7:30-3:30
CLOSED
15 GENERAL NEURO
NEURO OPEN7:30-3:30
NEURO
1 6 Overflow Overflow Overflow Overflow Overflow
17PEDI GI Gen Anes
PEDI GI Gen Anes
PEDI GIGen Anes.
PEDI GIGen Anes
PEDI GIGen Anes
18 GENERAL UROLOGY GYN DENTALGENERAL (4)GYN (4)
19 ENT ENTPLASTICS
DENTAL GYN
20
OPEN 8:30-12:30PLASTICS12:30-4:30
DENTAL7:30-12:30 GENERAL 12:30 – 5:30
ENTORTHO Trauma
GENERALLocal
21ENT
ORTHO NEURO ORTHO ORTHO
22 EYE EYE EYE EYE EYE
23 EYE EYE EYE EYE EYE
The principal teaching hospital for Tufts University School of Medicine
Model of Care
25Combining Art & Science, Innovations in Healthcare II, June 19, 2009
The Need to Re-evaluate the Current Care Model
Consumers are not satisfied with current care models
Current systems do not work
Dissatisfaction of clinical staff – moving away from the bedside
Need to deliver care in a more efficient and less costly manner
Need to reduce variation and improve outcomes
Public mandate / Pay for Performance
Current service delivery model has not been able to provide desired outcomes
Creating a new Model of Care is the most sustainable long-term strategy for Tufts Medical Center
26Combining Art & Science, Innovations in Healthcare II, June 19, 2009
New Model of Care
Patient Centered
Environmentally Aware
Forward Looking
Professionally Rewarding
27Combining Art & Science, Innovations in Healthcare II, June 19, 2009
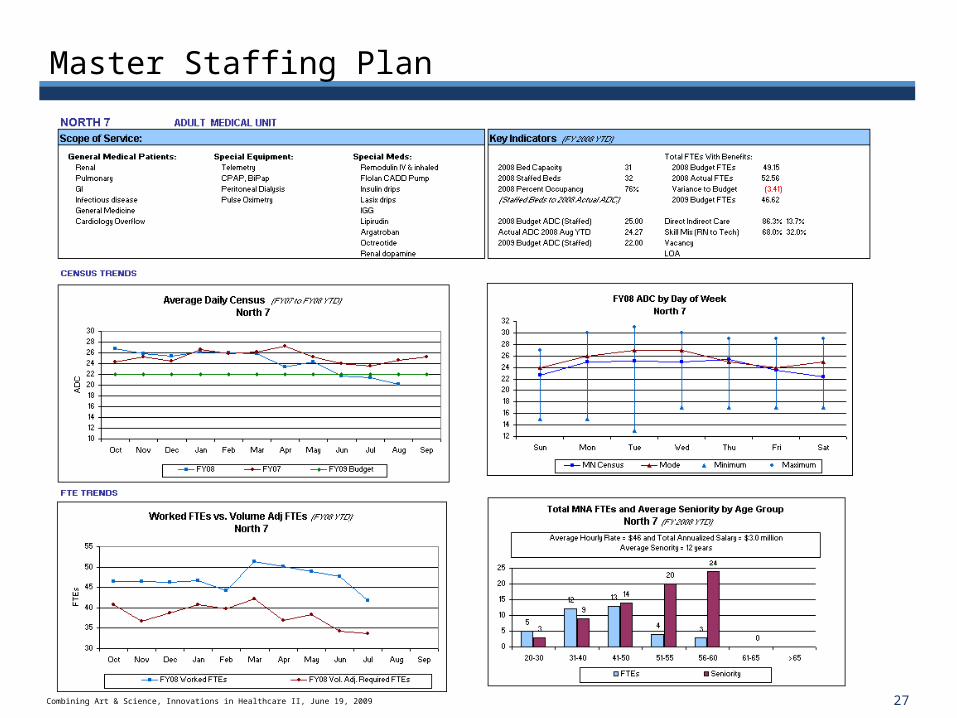
Master Staffing Plan
The principal teaching hospital for Tufts University School of Medicine
Results: Increase Volume
29Combining Art & Science, Innovations in Healthcare II, June 19, 2009
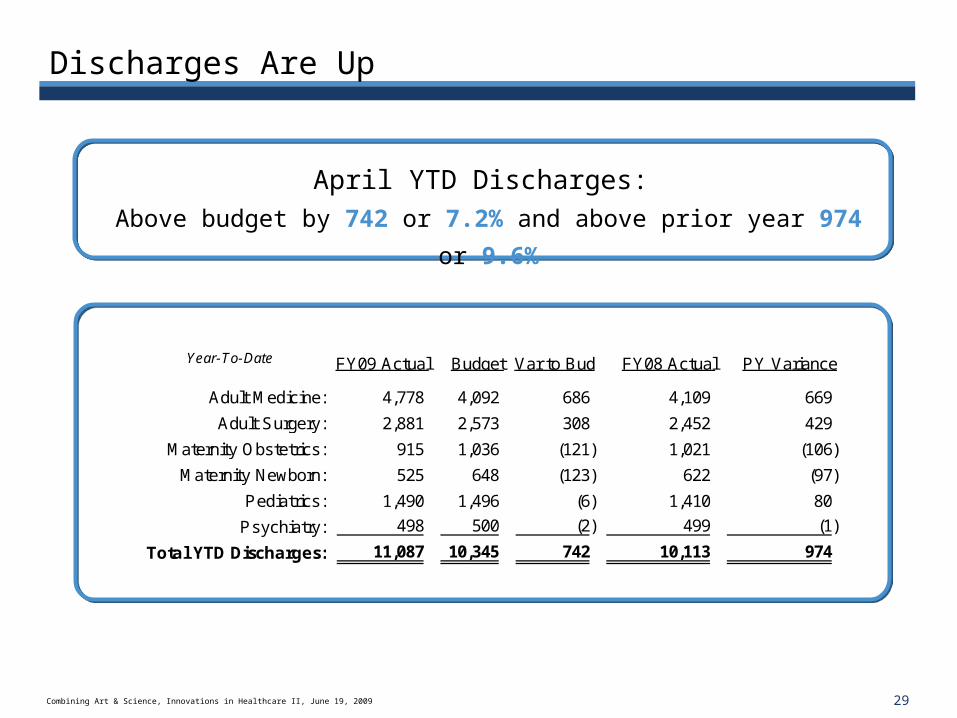
Discharges Are Up
April YTD Discharges:
Above budget by 742 or 7.2% and above prior year 974 or 9.6%
FY09 Actual Budget Var to Bud FY08 Actual PY Variance
4,778 4,092 686 4,109 669
2,881 2,573 308 2,452 429
915 1,036 (121) 1,021 (106)
525 648 (123) 622 (97)
1,490 1,496 (6) 1,410 80
498 500 (2) 499 (1)
11,087 10,345 742 10,113 974
Year-To-Date
Adult Medicine:
Adult Surgery:
Maternity Obstetrics:
Maternity Newborn:
Pediatrics:
Total YTD Discharges:
Psychiatry:
30Combining Art & Science, Innovations in Healthcare II, June 19, 2009
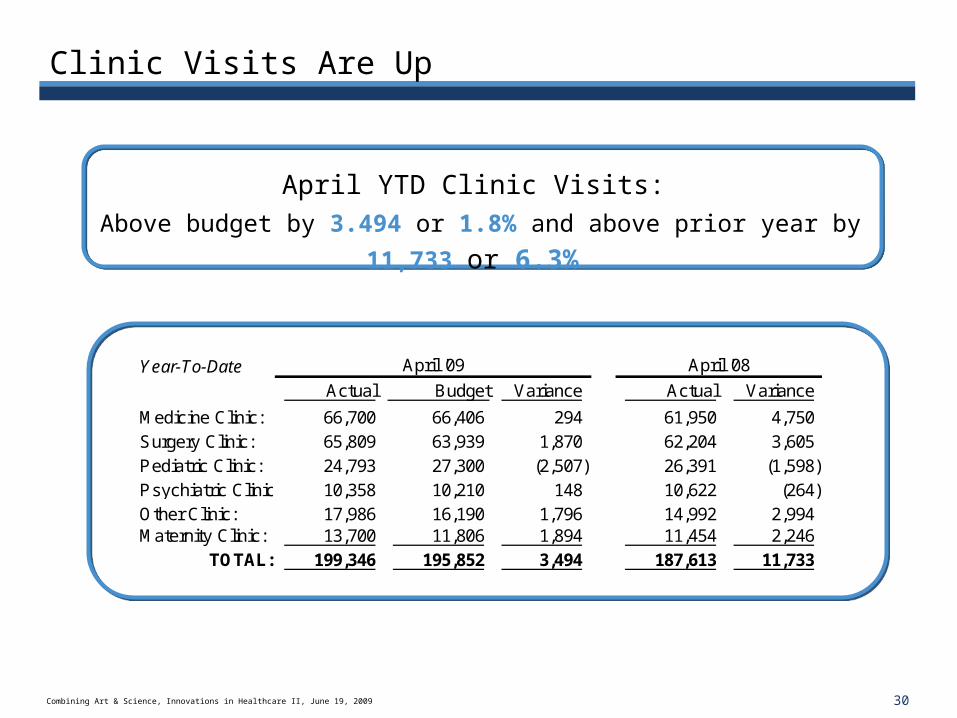
Clinic Visits Are Up
April YTD Clinic Visits:
Above budget by 3.494 or 1.8% and above prior year by 11,733 or 6.3%
Year-To-Date April '09 April '08
Actual Budget Variance Actual Variance
Medicine Clinic: 66,700 66,406 294 61,950 4,750 Surgery Clinic: 65,809 63,939 1,870 62,204 3,605 Pediatric Clinic: 24,793 27,300 (2,507) 26,391 (1,598) Psychiatric Clinic: 10,358 10,210 148 10,622 (264) Other Clinic: 17,986 16,190 1,796 14,992 2,994 Maternity Clinic: 13,700 11,806 1,894 11,454 2,246
TOTAL: 199,346 195,852 3,494 187,613 11,733
31Combining Art & Science, Innovations in Healthcare II, June 19, 2009
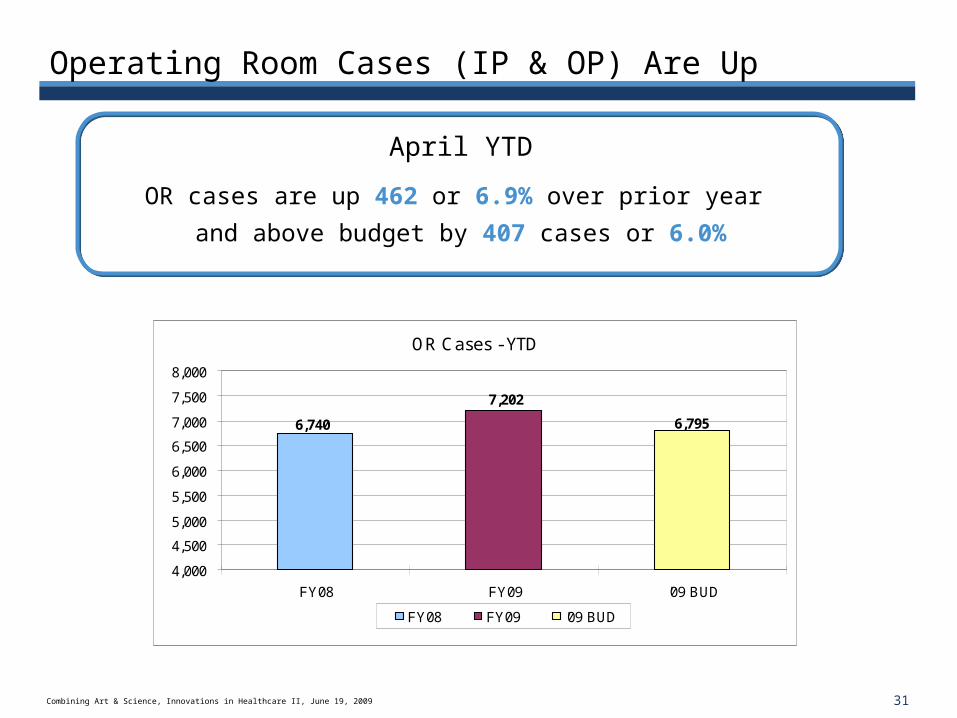
Operating Room Cases (IP & OP) Are Up
April YTD
OR cases are up 462 or 6.9% over prior year
and above budget by 407 cases or 6.0%
OR Cases - YTD
7,202
6,7956,740
4,000
4,500
5,000
5,500
6,000
6,500
7,000
7,500
8,000
FY08 FY09 '09 BUD
FY08 FY09 '09 BUD
32Combining Art & Science, Innovations in Healthcare II, June 19, 2009
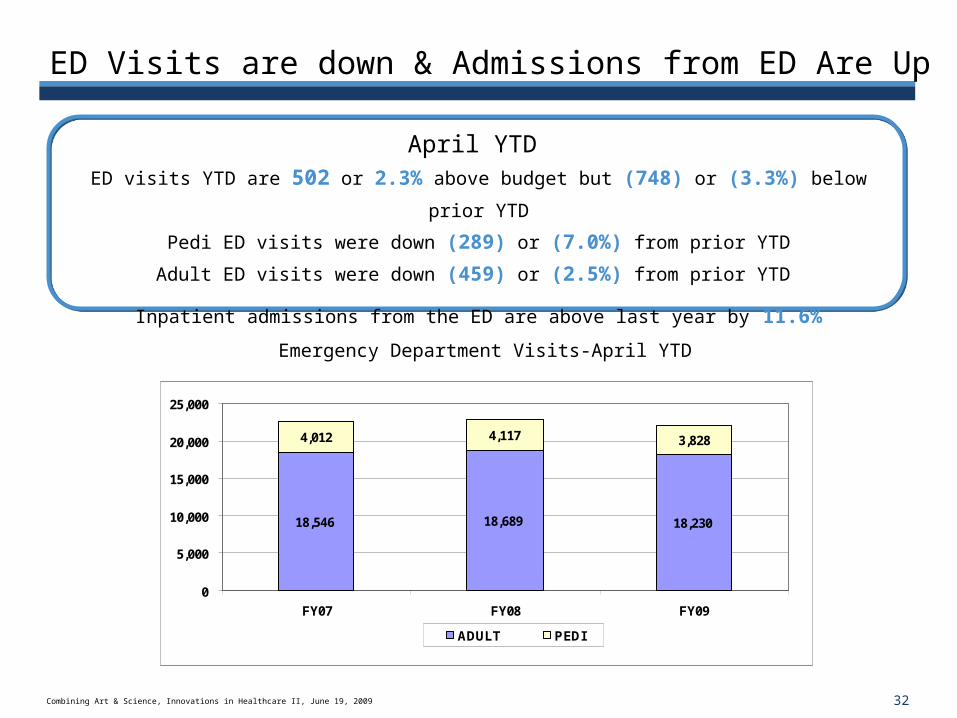
ED Visits are down & Admissions from ED Are Up
April YTD
ED visits YTD are 502 or 2.3% above budget but (748) or (3.3%) below prior YTD
Pedi ED visits were down (289) or (7.0%) from prior YTD
Adult ED visits were down (459) or (2.5%) from prior YTD
Inpatient admissions from the ED are above last year by 11.6%
18,546 18,689 18,230
4,012 4,117 3,828
0
5,000
10,000
15,000
20,000
25,000
FY07 FY08 FY09
ADULT PEDI
Emergency Department Visits-April YTD
33Combining Art & Science, Innovations in Healthcare II, June 19, 2009
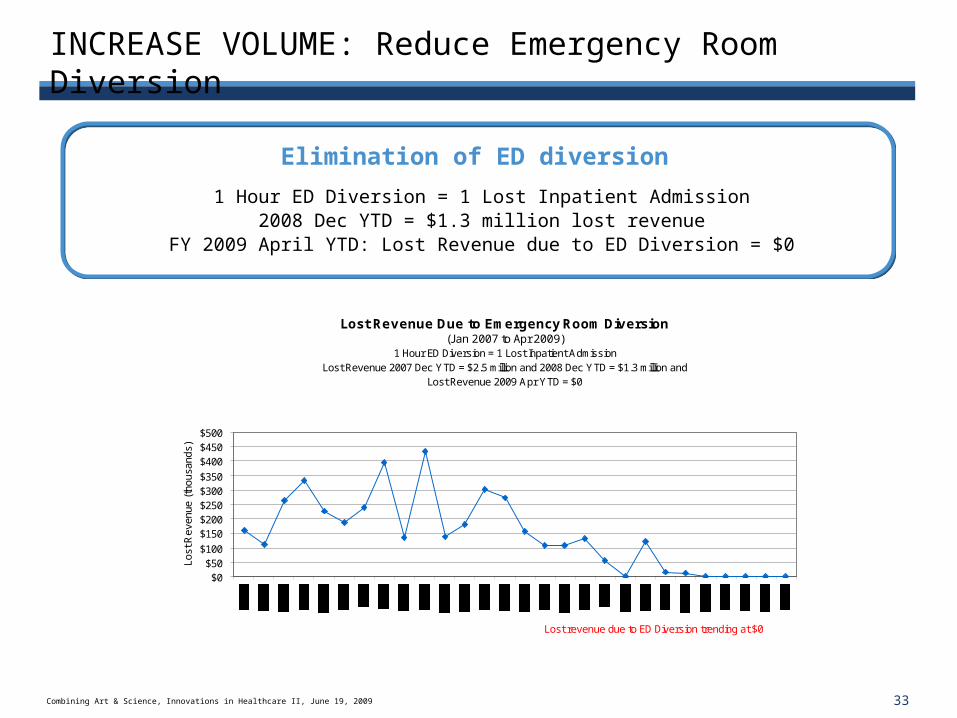
INCREASE VOLUME: Reduce Emergency Room Diversion
Elimination of ED diversion
1 Hour ED Diversion = 1 Lost Inpatient Admission2008 Dec YTD = $1.3 million lost revenue
FY 2009 April YTD: Lost Revenue due to ED Diversion = $0
Lost Revenue Due to Emergency Room Diversion (Jan 2007 to Apr 2009)
1 Hour ED Diversion = 1 Lost Inpatient AdmissionLost Revenue 2007 Dec YTD = $2.5 million and 2008 Dec YTD = $1.3 million and
Lost Revenue 2009 Apr YTD = $0
$0$50
$100
$150$200$250$300$350
$400$450$500
Lost revenue due to ED Diversion trending at $0
Lost
Rev
enue
(th
ousa
nds)
34Combining Art & Science, Innovations in Healthcare II, June 19, 2009
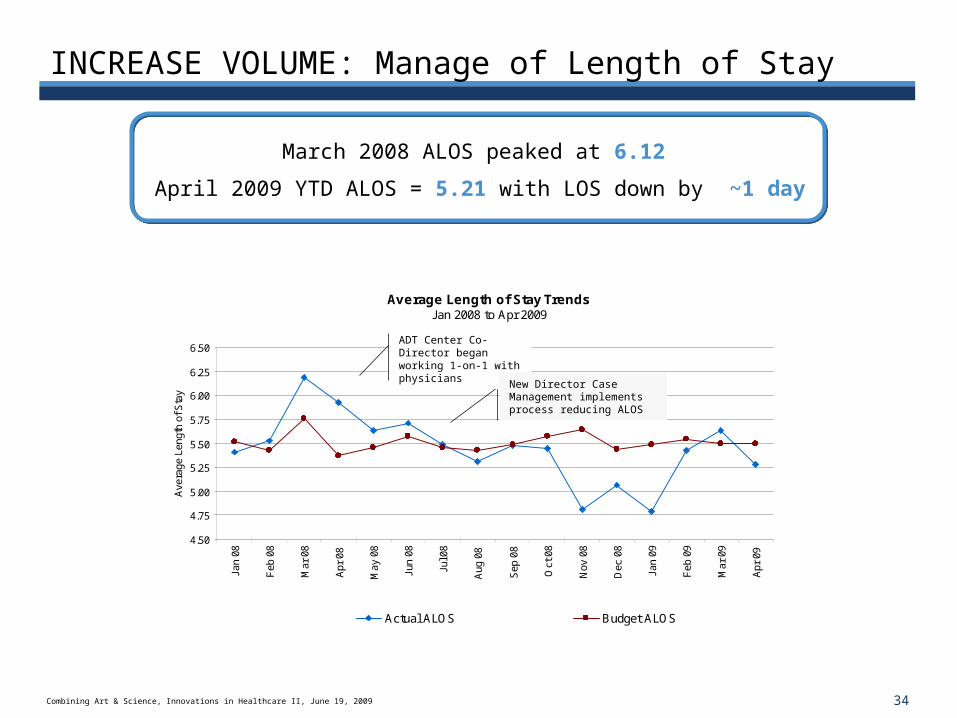
Average Length of Stay TrendsJan 2008 to Apr 2009
4.50
4.75
5.00
5.25
5.50
5.75
6.00
6.25
6.50
Jan
08
Feb
08
Mar
08
Apr
08
May
08
Jun
08
Jul 0
8
Aug
08
Sep
08
Oct
08
Nov
08
Dec
08
Jan
09
Feb
09
Mar
09
Apr
09
Ave
rage
Len
gth
of S
tay
Actual ALOS Budget ALOS
INCREASE VOLUME: Manage of Length of Stay
March 2008 ALOS peaked at 6.12
April 2009 YTD ALOS = 5.21 with LOS down by ~1 day
ADT Center Co-Director began working 1-on-1 with physicians
New Director Case Management implements process reducing ALOS
35Combining Art & Science, Innovations in Healthcare II, June 19, 2009
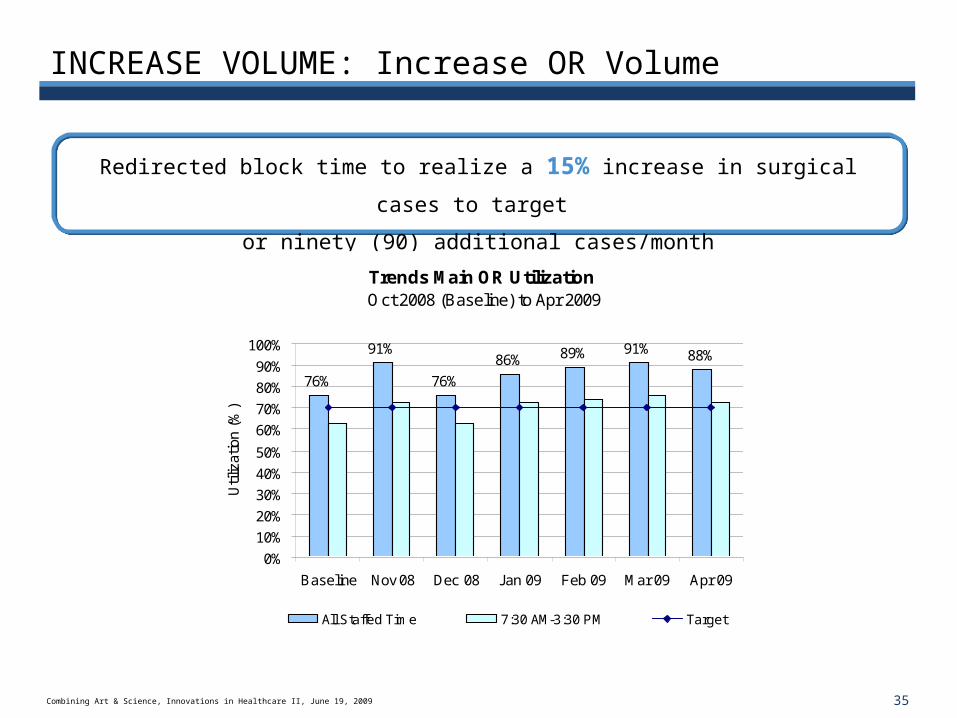
INCREASE VOLUME: Increase OR Volume
Redirected block time to realize a 15% increase in surgical cases to target
or ninety (90) additional cases/month
Trends Main OR Utilization Oct 2008 (Baseline) to Apr 2009
76%
91%
76%
86% 89% 91% 88%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Baseline Nov 08 Dec 08 Jan 09 Feb 09 Mar 09 Apr 09
Util
izat
ion
(%)
All Staffed Time 7:30 AM-3:30 PM Target

36Combining Art & Science, Innovations in Healthcare II, June 19, 2009
Volume Has Grown
April YTD discharges are 742 over budget and 974 over prior YTD
April YTD surgery cases are 407 over budget and 462 over prior YTD
Operating Statistics (April MTD) Percent Achieved of Budget
111% 115%123%
107%117% 120%
0%
20%
40%
60%
80%
100%
120%
140%
InpatientDischarges
OR Cases Clinic Visits ED Visits ED Admits CATH LabPatients
% A
chie
ved
% of Budget Budget
The principal teaching hospital for Tufts University School of Medicine
Results: Decrease Cost
38Combining Art & Science, Innovations in Healthcare II, June 19, 2009
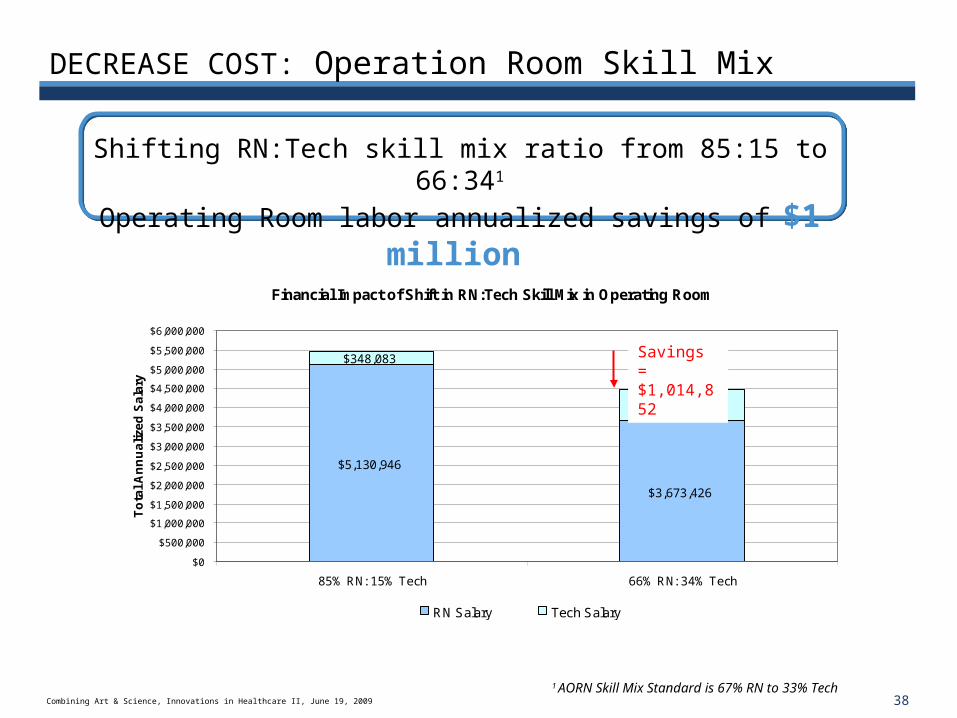
Financial Impact of Shift in RN:Tech Skill Mix in Operating Room
$5,130,946
$3,673,426
$348,083
$790,752
$0
$500,000
$1,000,000
$1,500,000
$2,000,000
$2,500,000
$3,000,000
$3,500,000
$4,000,000
$4,500,000
$5,000,000
$5,500,000
$6,000,000
85% RN: 15% Tech 66% RN: 34% Tech
To
tal
An
nu
ali
zed
Sa
lary
RN Salary Tech Salary
DECREASE COST: Operation Room Skill Mix
Shifting RN:Tech skill mix ratio from 85:15 to 66:341
Operating Room labor annualized savings of $1 million
Savings = $1,014,852
1 AORN Skill Mix Standard is 67% RN to 33% Tech
39Combining Art & Science, Innovations in Healthcare II, June 19, 2009
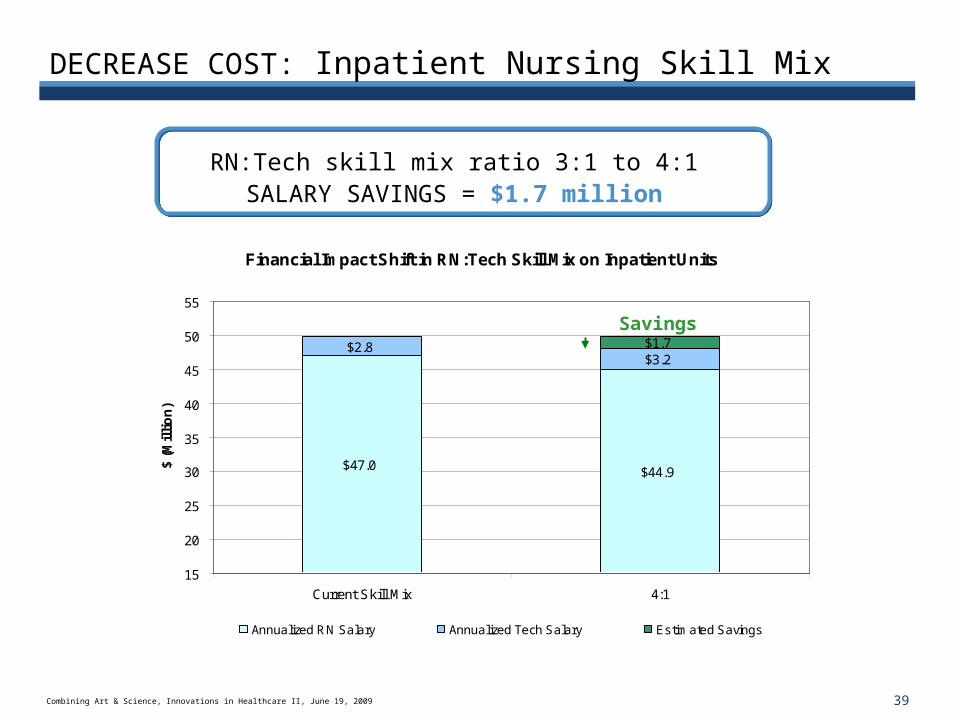
Financial Impact Shift in RN:Tech Skill Mix on Inpatient Units
$47.0 $44.9
$2.8$3.2$1.7
$0.0
15
20
25
30
35
40
45
50
55
Current Skill Mix 4:1
$ (M
illi
on
)
Annualized RN Salary Annualized Tech Salary Estimated Savings
DECREASE COST: Inpatient Nursing Skill Mix
RN:Tech skill mix ratio 3:1 to 4:1 SALARY SAVINGS = $1.7 million
Savings
40Combining Art & Science, Innovations in Healthcare II, June 19, 2009
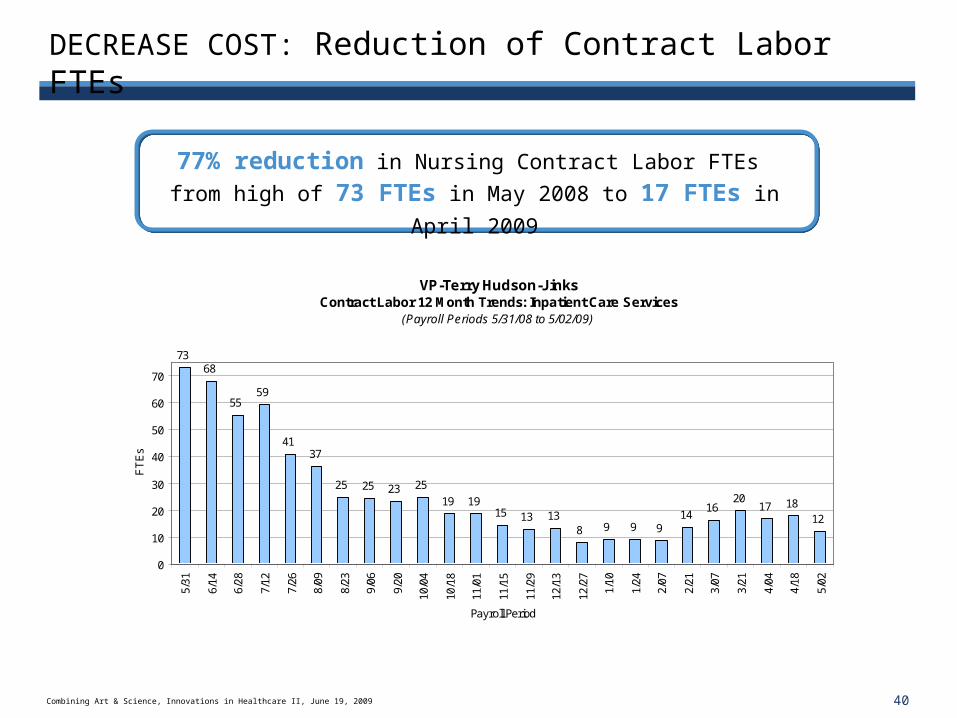
DECREASE COST: Reduction of Contract Labor FTEs
77% reduction in Nursing Contract Labor FTEs
from high of 73 FTEs in May 2008 to 17 FTEs in April 2009
VP-Terry Hudson-JinksContract Labor 12 Month Trends: Inpatient Care Services
(Payroll Periods 5/31/08 to 5/02/09)
7368
5559
4137
25 25 23 25
19 1915 13 13
8 9 9 914
1620
17 1812
0
10
20
30
40
50
60
70
5/31
6/14
6/28
7/12
7/26
8/09
8/23
9/06
9/20
10/0
4
10/1
8
11/0
1
11/1
5
11/2
9
12/1
3
12/2
7
1/10
1/24
2/07
2/21
3/07
3/21
4/04
4/18
5/02
Payroll Period
FT
Es
41Combining Art & Science, Innovations in Healthcare II, June 19, 2009
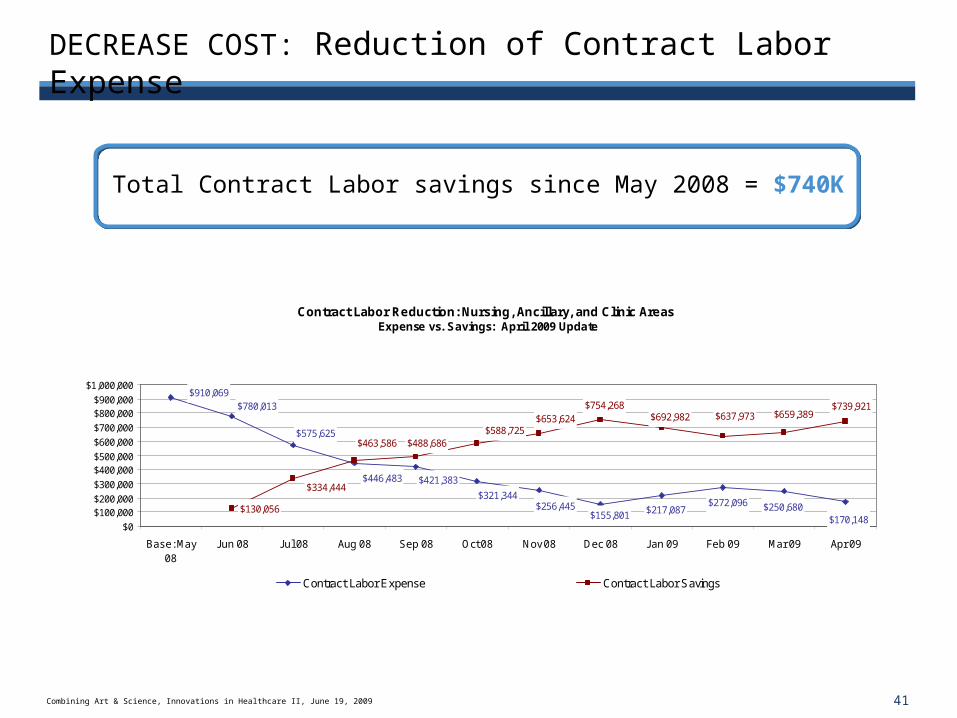
DECREASE COST: Reduction of Contract Labor Expense
Total Contract Labor savings since May 2008 = $740K
Contract Labor Reduction: Nursing, Ancillary, and Clinic Areas Expense vs. Savings: April 2009 Update
$421,383
$321,344$256,445
$155,801
$910,069$780,013
$575,625
$446,483
$217,087$272,096 $250,680
$170,148
$588,725$488,686
$653,624$754,268
$334,444
$130,056
$463,586
$692,982 $637,973 $659,389$739,921
$0
$100,000$200,000
$300,000
$400,000$500,000
$600,000
$700,000
$800,000$900,000
$1,000,000
Base: May08
Jun 08 Jul 08 Aug 08 Sep 08 Oct 08 Nov 08 Dec 08 Jan 09 Feb 09 Mar 09 Apr 09
Contract Labor Expense Contract Labor Savings
42Combining Art & Science, Innovations in Healthcare II, June 19, 2009
Summary
Successful outcomes occur when Art and Science are combined.
Involving people, providing data & encouraging innovation will always lead to success.





























