Embed Size (px)
Citation preview

o$0
POSTGRAD. MED. J., 1961, 37, 50
Clinicopathological Conference
A CASE OF CRUSH INJURY OF THE CHESTA Saturday Forum held at the Western Infirmary, Glasgow, on Saturday, October 22, 1960
Chairman: Professor E. J. Wayne, M.Sc., Ph.D., M.D., F.R.C.P., F.R.F.P.S.G.
Editors: H. I. Tankel, M.D., F.R.C.S., andB. Lennox, Ph.D., M.D., F.R.F.P.S.G., M.R.C.P.
A BFIG. i.-(a) Shows the central type of crushed chest in which there is a transverse fracture of the sternum. (b) Shows the
lateral type in which the sternum is intact.(Reproduced by kind permission of the Journal of Bone and Joint Surgery).
MR. D. H. CLARK: Professor Wayne, Ladiesand Gentlemen, I wish to present a case of crushinjury of the chest. There are two common typesof crush injury (Fig. i), a central type in whichthe sternum is fractured, and a lateral type inwhich there is a large number of fractures of theribs on one or both sides. The patient I wish topresent was of the latter type and had two largelateral flail fragments.The patient is a labourer, aged 40, with chronic
bronchitis. On September 8th he and a workmatewere at the bottom of a I2-ft. trench when thesides suddenly caved in. His workmate was killedand the patient sustained a severe crush injury ofthe chest. He was admitted to this hospital and,although not in extremis, he was seriously ill andso distressed that oxygen was immediately ad-ministered. He was sweating, cyanosed and insevere pain. He had marked surgical emphysemaof his chest, fore and aft, on his neck and spreading
copyright. on 1 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.423.50 on 1 January 1961. D
ownloaded from

January 1961 A Case of Crush Injury of the Chest 51
.... ...... ... ''
.........., ,,.. ,.,....... j... ..jFIG. 2.-The patient in bed showing the tracheostomy, a water-seal drain in the second right interspace
and traction applied to wires around the ribs.
on to his face. Paradoxical respiration was obviousin two large lateral segments. The blood pressurewas I50/90 and the pulse rate about Ioo. AnX-ray was taken which showed fore and aftfractures of the 5th to 9th ribs inclusive on bothsides and surgical emphysema, but no evidenceof pneumothorax.We watched the patient while an intravenous
infusion was being installed and reached thefollowing conclusions: (i) He had not lost agreat deal of blood; (2) he had a purely thoraciccage and lung injury and there was no intra-abdominal lesion; and (3) he had no sternal frac-ture. We decided to proceed with the anaesthetic,and this was begun by Dr. Fleming who waslater joined by Dr. Wishart. As in all these casesthe patient improved immediately. However, theimprovement was short-lived; in about o minuteshe began to deteriorate, and the anaesthetistsreported that the amount of pressure required toinflate his lungs was increasing. A spontaneoustension pneumothorax on the left side was diag-nosed and an intercostal water-seal drain wasinserted through the second left interspace,whereupon air came out under pressure. The
operation then proceeded and consisted of puttingslings of wire sheathed in polythene tubing roundthe 7th and 8th ribs on both sides in the mid-axillary line. A tracheostomy was then performed.Towards the end of the operation it was againreported by the anaesthetists that there was diffi-culty in inflating the lungs. Further X-ray of thepatient now revealed a tension pneumothorax onthe opposite (right) side. An intercostal drainwas inserted in the second right interspace andagain air came off under pressure. The patientwas then transferred to the ward and the slingswere attached to weights over the sides of thebed. He was given no oxygen. Further progresswill be discussed under separate headings.The Thoracic CageAfter traction was applied the rib cage gave no
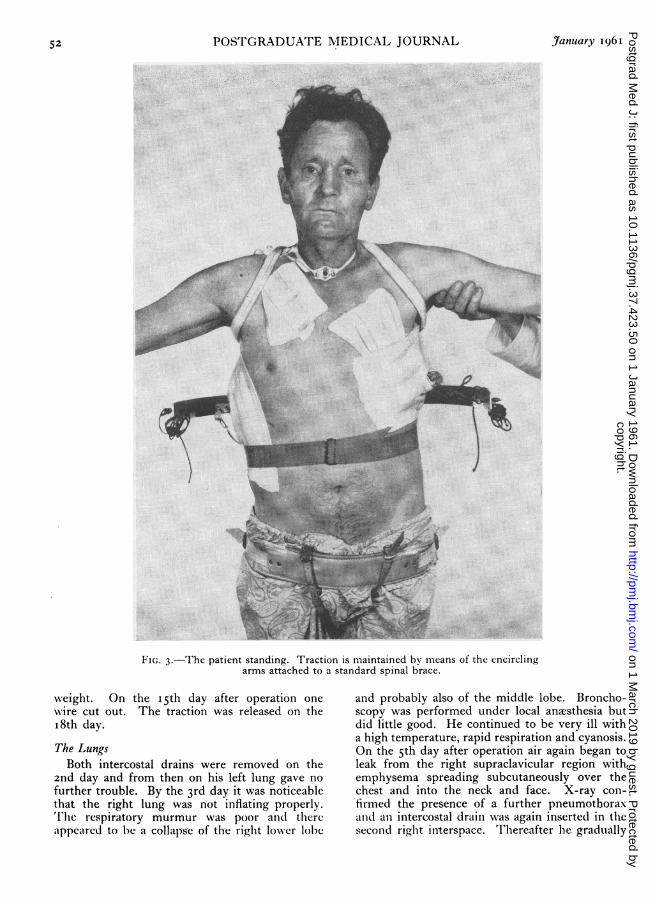
further cause for concern. Fig. 2 shows thepatient in bed with traction applied. He wasallowed up on the I th day, and Fig. 3 shows himstanding with the traction still maintained bymeans of a spinal brace to which encircling armshave been attached. The emphysema subsidedrapidly and he lost a considerable amount of
C2
copyright. on 1 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.423.50 on 1 January 1961. D
ownloaded from
5POSTGRADUATE MEDICAL JOURNAL January 1961
wai<i...
-···;:::; ·sQ |n ..
liani.
*)-* .5.- .. ... ........
. ....... ..s.-........... . '.O .........
i | - l -:
:a . ..............··: :·:. Dig ...........................i~iii~~ii:i:..........i~:: ........
:l ·l :·I: i:ii·.. ··
*Allrtsie0. . . . . . . . . . . . . o ·xsX
..1-11 ::.·:::j: ::1i·' e@1r~
FIG. 3.-The patient standing. Traction is maintained by means of the encirclingarms attached to a standard spinal brace.
weight. On the i5th day after operation onewire cut out. The traction was released on theI8th day.The LungsBoth intercostal drains were removed on the
2nd day and from then on his left lung gave nofurther trouble. By the 3rd day it was noticeablethat the right lung was not inflating properly.lThe respiratory murmur was poor and thereappeared to be a collapse of the right lower lobe
and probably also of the middle lobe. Broncho-scopy was performed under local anaesthesia butdid little good. He continued to be very ill witha high temperature, rapid respiration and cyanosis.On the 5th day after operation air again began toleak from the right supraclavicular region withemphysema spreading subcutaneously over thechest and into the neck and face. X-ray con-firmed the presence of a further pneumothoraxand an intercostal drain was again inserted in thesecond right interspace. Thereafter he gradually
copyright. on 1 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.423.50 on 1 January 1961. D
ownloaded from

January I961 A Case of Crush Injury of the Chest 53
P.D.- BLOOD PRESSUREmm
Hg200
180 -
160
140
120
10080-
60
40
day I 2 3 4 5 6 7 | 28 29 30 31
FIG. 4.-Blood pressure chart showing hypertension due to carbon dioxide retention during thefirst week. The late readings show the patient's normal levels.
improved, despite a haemoptysis on the I4th day,which was felt to be due to secondary haemorrhagefrom lacerated lung or the opening of an area ofatelectasis. The most recent X-ray shows thatthe right lung has cleared considerably thoughthere is probably still a very small pneumothoraxat the apex.
I do not think there is any doubt that this manhad CO2 retention for at least ten days. Unfor-tunately we have no readings of the arterial CO2tension. However, we did record his bloodpressure faithfully and I have summarized thefindings in Fig. 4. His blood pressure on admis-sion was I50/9o, and during the first few daysit rose, until on the 4th and 5th days it was inthe region of 190/120. In the two or three daysprior to his discharge from hospital his bloodpressure remained in the region of I20 to 130systolic, and this would appear to be his normalblood pressure. We submit this as evidence thathe probably did have a significant degree of CO2retention.
The TracheostomyHe had a tracheostomy for 24 days. At first
a cuffed tube was used and we released the cufffor five minutes in every hour. Aspiration of thebronchi through a Tieman's catheter was requiredevery half-hour and sometimes more frequently
as he was a chronic bronchitic. As time passedthe amount of aspiration required became less.After about a week the rubber tracheostomy tubewas changed for a metal one, and he found thismore comfortable. These tubes were changedregularly.
Bacteriology at different times revealed thepresence of staphylococci, B. proteus, diphtheroidsand streptococci. The only antibiotic to which allwere constantly sensitive was chloramphenicol.At this point the patient was presented and the
chest expansion demonstrated to be I inch. Thechest was stable and the wounds healed. There wasno cough.
PROFESSOR WAYNE: Thank you very much,Mr. Clark. It seems that many of the problemshad to do with the anaesthetic and I would askDr. Wishart to talk about these.DR. H. Y. WISHART: The main interest in this
case from our point of view was the fact that thepatient came in without a tension pneumothoraxand that this became evident during anesthesia.The patient was curarized in the normal way andbreathing was being controlled by hand when itwas noticed that increasing pressure was neededto do this. When this happens there may be threecauses: (i) The muscle paralysis may be wearingoff, (2) secretions may be blocking the tracheo-bronchial tree, or (3) a tension pneumothorax
copyright. on 1 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.423.50 on 1 January 1961. D
ownloaded from

54 POSTGRADUATE MEDICAL JOURNAL January 1961
may be developing. In this case the patient wasmaking small respiratory efforts and so he wasrecurarized but without improvement. He wassucked out and again there was no improvement,so of course tension pneumothorax was suspected,although breath sounds could be heard. When adrain was put into the left side of the chest alarge amount of air under pressure came off.When a patient is admitted with a crushed
chest, and surgical emphysema is present, youmust suspect laceration of lung tissue or surgicalemphysema would not be there. You must there-fore expect a pneumothorax to be present, whichmay become the tension type. There is a viewthat if there is surgical emphysema present whenthe patient is admitted one of the first steps afterthe induction of anaesthesia should be to insert adrain intrapleurally to relieve any tension. As analternative I would suggest that if you suspect atension penumothorax a syringe with a needleattached should be inserted into the pleura, andif there is a tension pneumothorax the plungerwill come out. A water-seal drain can then beinserted.
PROFESSOR WAYNE: I wonder if Mr. Fraser hasany comments to make as a thoracic surgeoninterested in this particular problem.MR. KENNETH FRASER: Mr. Chairman, first of
all I want to emphasize that the most importantperson at the admission of these patients to hos-pital is the anaesthetist. By intubating the patientand controlling the respiration he will overcomethe paradoxical movement of the chest. This willin turn control the restlessness of the patient;and this is an opportunity to point out that CO2accumulation can produce extreme restlessnessand irritability. I am sure it is not always appre-ciated just how important this may be.
Next, it is important that having obtained aninitial film with no pneumothorax present youshould not be content to think that this situationis necessarily maintained until the end of theoperation. One has only to open a chest withbroken ribs, and see and feel the sharp edges, torealize that while the control of breathing improvesthe patient it may also produce a pneumothoraxby rubbing the lung against the rough rib ends.A further point is brought out by another
patient I saw recently at the Vale of LevenHospital. In addition to multiple fractures, intra-abdominal injuries and a similar bilateral crushedchest injury, he also had a traumatic hiatus hernia.The X-ray (Fig. 5) shows the stomach bubblewithin the chest about halfway up the clavicle.The point I wish to make is this, that before oneintubates a patient with an injury like this onemust pass a gastric tube to deflate the stomach.
.:::!
i:I
i:iiii..
:·ii:
*i.
FIG. 5.-X-ray of a patient with a traumatic hiatushernia on the left side showing the stomach bubblehigh into the chest, and the mediastinum pushedover to the right. Fractures can be seen on the4th-7th ribs. (Vale of Leven Hospital.)
If the patient is anesthetized, curarized and puton to hand-controlled respiration without thisprecaution, then the right lung will be inflatedand push the mediastinum against the grosslydistended stomach. If the stomach is sufficientlydistended the patient will certainly developasystole during the course of the induction.Where you have such a hernia it is thereforeimperative .to introduce an intragastric tube toreduce the tension before proceeding to anes-thesia. If it is impossible to introduce the tube(due to rotation of the stomach) then I believethat you are justified in putting a trocar andcannula through the chest wall into the stomachand deflating the stomach by passing a Malecotcatheter before doing anything else. In thissecond case I used the method of traction thatMr. Clark has already described with equallygood results.
PROFESSOR WAYNE: We are fortunate in havingwith us this morning Mr. Sillar of the SouthernGeneral Hospital, who has been specially inter-ested in this type of chest injury.MR. W. SILLAR: Sir, this has been a most
interesting case. There are a great many thingsone could comment on, but I would like to bring
copyright. on 1 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.423.50 on 1 January 1961. D
ownloaded from

A Case of Crush Injury of the Chest
up only one aspect of the problem at the momentand this is the question of the early anaesthetic.The patient may be admitted in extremis, he maybe in an agonal state, and his life can be savedonly by the immediate induction of anesthesia;this must never be forgotten. But not all thepatients are so nigh unto death and there are somedisadvantages in immediate anaesthesia. You donot have an opportunity of examining the abdo-men, you do not know what intra-peritonealdamage may have occurred, you do not have anopportunity to examine the central nervoussystem, and you are no longer in a position toassess accurately the damage to the rib cage sincepositive pressure anaesthesia stops paradoxicalnrbvement. All these are serious disadvantageswhich will have to be accepted and overcomewhen the patient is very seriously ill. However,if he is not so ill, a little time will enable us toclear up these points before we are committed tothe operative procedure. If, therefore, the patientcan be resuscitated and an air way guaranteedbefore he isanaesthetized, it might make the assess-ment of his injuries more complete and the plan-ning of the operative procedure much easier. Onthe other hand, if you must anaesthetize him tosave his life then there are some devices whichcan help. If necessary, a small mid-line laparo-tomy can be made and the wartime practice ofplunging a swab on a holder into the four cornersof the abdomen carried out. If the swab comesout clean, the little laparotomy wound can beclosed quickly and not much time is wasted. Itis important to determine the size and shape ofthe flail segment, and the anaesthetist may be ableto oblige at a later stage, after the patient's con-dition has been improved, by allowing spontaneousrespiration to return and then temporarily ob-structing the airway to demonstrate paradoxicalmovement.
I would like to emphasize again the danger ofa pneumothorax developing after anesthesia.This is a real danger and one must be ready atonce to deal with it.
PROFESSOR WAYNE: Thank you, Mr. Sillar, forthat valuable contribution. Perhaps Dr. Pinkertonwould care to comment further on the anaestheticproblem.
DR. PINKERTON: When these patients come tohospital they suffer from three major disabilities-pain, shock and respiratory embarrassment. Thereis no question that the respiratory embarrassmentis the paramount condition and that it is due toparadoxical respiration and the presence of secre-tions. To anaesthetize the patient, intubate himand take control of the respiration produces animmediate and, to those who have not seen it analmost unbelievable improvement. The para-
doxical respiration is cured by the control of therespiration, the sucking out of secretions followsthe intubation.When the operation has been completed and
such fixation as can be achieved has been done,the decision has to be taken on the matter of atracheostomy and I would say no more than thatif there is any doubt whatever as to whether atracheostomy should be performed, and usuallythere is none, it should be performed. I thinkthat there is a great value in biochemical controlof these patients, and I think there is little doubtthat the elevated blood pressure during the firstten days in this case indicated CO2 retention. Itis possible that more prolonged ventilation bymeans of a respirator would have improved this.PROFESSOR WAYNE: I wonder if perhaps Pro-
fessor Barnes as an orthopaedic surgeon interestedin trauma would like to say anything.
PROFESSOR ROLAND BARNES: Like most peoplehere I have very little experience of this type ofinjury, but I would like to ask some questions.One of the problems that we have not dealt withvery effectively to date is the treatment of para-doxical respiration. There are two approaches tothis. The first is the application of some form offixation to the chest, such as the metal platedevised by Mr. Sillar for fixation of the sternum,or, as we have seen this morning, traction wirespassed through the rib cage. The alternative, ofcourse, is the control of paradoxical respiration byhyperventilation. I would like to hear a dis-cussion of the merits of these two methods. Wealso have used wires through the thoracic cage,but it may be that these are liable to cut out, aswe saw in today's case, and as Griffiths (I960) hasmentioned in his recent communication to theRoyal College of Surgeons of Edinburgh. Forthis reason he was a very firm advocate of hyper-ventilation. It may be that there is room for boththese methods. If we have a sternal fracture is itbetter to deal with it by fixing it with a plate ?If we have multiple rib fractures, would it bebetter to consider hyperventilation ?MR. SILLAR: I think that the problem of con-
trolling paradoxical motion by a respirator is adifficult one. We have not had good fortune herein using a mechanical respirator. We used thePneumatron and were not able to synchronizethe patient with the machine. This has been theexperience of others. In general there are fourother methods of overcoming the conflict betweenthe patient and the machine when dealing with aconscious patient who is not paralysed-which isa different problem from that presented by thepatient with poliomyelitis: (i) Muscle relaxants;the patient's resistance can be overcome bymuscle relaxants, though this is not a feasible pro-
January 196I 55copyright.
on 1 March 2019 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.423.50 on 1 January 1961. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
cedure apparently in the conscious patient.(2) Hyperventilation as used by Professor Morchin Chicago (Avery, Morch and Benson, I956).He seems to have had very good results indeedby deliberately over-ventilating the patient, in-ducing alkalosis and apncea, and so keeping thepatient alive for a considerable time without spon-taneous respiration. (3) Dr. Griffiths in Edin-burgh, not wishing to go all out for this methodand not wishing to depress the patient with highdosage of morphine, decided to steer a middlecourse by using some morphine and a littlehyperventilation to try to avoid the danger ofboth. He has three patients at least who haverecovered on this management. (4) Continuousflow, a method of which we have no experience.A continuous flow of oxygen is provided at lowpressure through the tracheostomy without a cuff.The patient's respiration then consists of expira-tory efforts only against a continual gentle inflation.The only method we have tried is, as I have
said, the patient-triggered respirator which issupposed to detect instantly and to instantlyaugment the patient's own inspiratory effortbefore the flail movement of the damaged portioncan occur. We have not been able to make thiswork, because we found it hard to synchronize thepatient with the type of machine available, and sowe have turned again to methods of stabilizing therib cage. It seems to me that if normal respiratoryphysiology can be restored by repairing the ribcage this must be a healthier arrangement thandeliberate1y blowing air down into a patient'slungs over. a considerable number of days at therisk of interfering with the clearing of secretions.MR. H. WAPSHAW: The treatment in this case
has been very successful, but, if I may say so, thesuccess has been partly due to the fact that thepatient had no other injuries. The mortality inthis condition is really dreadful-well over 60%-and that is everybody's experience. In thesevery serious chest injuries there are three main types.Mr. Clark has described two. There is a third,and the French have the only word for it, andthat is bone 'marmalade'; in these cases, verylittle can be done for the patient.MR. A. D. RoY: Why did you maintain the rib
fixation for as long as i8 days ? I would havethought that the ribs might have consolidatedbefore then. How long does it take for thesefractures to stabilize and consolidate if they arenot'fixed ?MR. CLARK: Rib fixation was maintained for so
long only because the patient felt uneasy with-out it.MR. FRASER: It is generally thought that I2 to
14 days is adequate for the ribs to find their ownfixation. I would like to say a further word about
the Morch machine of which we have alreadyheard. It seems to me from reading the literatureto be the one most likely to be suitable. Morchdoes not use an inflated cuffed tube. He claimsthat if sufficient pressure is used, then the secre-tions are blown up the trachea and can be suckedout from the back of the throat or from thetracheostomy.MR. T. B. GARDINER: I think that the point
that Mr. Wapshaw made about associated injuriesis a very important one. I think it worthwhilepointing out that the case with the traumatichiatus hernia mentioned by Mr. Fraser had, inaddition to lateral flail chest, a ruptured spleen,torn omentum and pancreas, and bilateral frac-tures of his transverse processes, femurs an'dankles. His recovery was helped by an extensivetransfusion and the fact that we did not have todo much to the fractures to secure stability.
DR. PINKERTON: I think there is a point we aremissing in the discussion. If, in these crushedchest injuries, the flail segments can be securelyfixed, clearly the patient may recover without theneed of assisted respiration of any kind afterwards.This happened in this morning's case. Spon-taneous respiration has clearly got him through,although at some little cost of CO2 retention, andhe has recovered most admirably as we can see.However, we are slipping past the point of thepatient in whom adequate fixation is not achievedor is not possible. Such people must have somekind of controlled respiration with a mechanicalrespirator for some time. Even those who havehad a reasonable fixation are usually the better forsome form of assisted respiration. I would notattempt to improve on the description which Mr.Sillar has already given of the problems whichface us there. There are plenty of such injuriesbut not many come into the hands of any onegroup, so that it is difficult to compare onemethod of treatment with another. The respira-tors vary in their ability to control and to assistand to go with the patient, and it is agreed thatthe triggering of respirators has not provided theanswer to the problem. The hyperventilationmethod suggested by Griffiths and by M6rch inChicago may possibly be an answer. It sohappens that Dr. Fleming who was the first toanesthetize this patient has recently returnedfrom Switzerland and has seen something of thetreatment of such cases there.
DR. FREDA W. FLEMING: It is sad to hearpeople say that patients cannot be maintainedadequately on respirators, yet I suppose it showsour good fortune in not having many of thesetragic cases to deal with. Both in the UniversityHospital in Lausanne and the Claude BernardHospital in Paris they have been handling respira-
56 January 96rcopyright.
on 1 March 2019 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.423.50 on 1 January 1961. Dow
nloaded from

January 196 A Case of Crush Injury of the Chest 57NORMAL ANTERIOR SEGMENT FLAIL
C~3b 0 0coI/I 3
/
SII VIQA; II8,//// C
INSPIRATI\ON INSPIRATIHON[3XII \"
\'IFIG. 6.-The effect of the flail anterior segment in interfering with the descent of the diaphragm
is shown.(Reproduced by kind permission of the Journal of Bone and Joint Surgery.)
tory catastrophes of many kinds, includingcrushed chests, in special units. They use variouskinds of respirators, but mainly the SwedishEngstrom which seems to overcome many of thedifficulties which have been mentioned (Engstr6m,I953); patients can be adequately triggered, andthey can continue using this machine even whenmore or less fully conscious and co-operative.Gases can be supplied in varying proportions asrequired and for a considerable time. The chestinjuries are fixed mechanically as well, but theuse of the respirator with adequate suction per-mitted the normal blood physiology to be pre-served until it was quite obvious that thesepatients could maintain this function for them-selves. It means, of course, an elaborate set-upwith individual cubicles, much apparatus andspecially trained nurses and physiotherapists.MR. H. I. TANKEL: Mr. Sillar, in what propor-
tion of these chest injuries is fracture of thesternum the main factor ? Could you tell ussomething of your results to date with fixationof the sternum by means of a plate, and do youfeel that internal fixation of the ribs is of anyvalue ?MR. SILLAR: Of 35 patients seen in Glasgow
TABLE I35 PATIENTS WITH FLAIL SEGMENTS
Deaths15 pure lateral segments .. .. 88 pure anterior segments .. .. 74 mixed type .. .. . 38 details insufficient .. 7
(Reproduced by permission of the Journal of Bone and oint Surgery.)
hospitals in four or five years up to I960 (Table i),15 had a pure lateral injury, and of these therewere seven survivors; but of the eight cases inwhich the anterior segment bore the brunt of thedamage there was only one. I think the reasonfor this significant difference is as follows. If thesternum is flail and a large part of the rib marginforms part of the flail segment also, then thediaphragm is denied its usual fixed anchorageanteriorly. The xiphisternum falls back duringinspiration and so the diaphragm slides ineffec-tively over the underlying viscera but does notdescend (Fig. 6). Thus there is a very seriousinroad into the patient's vital capacity. Whenthere is a lateral segment injury I do not thinkthe diaphragm is usually affected to such anextent. We therefore searched for a method offixing the sternum. Since collecting the 35 casesmentioned earlier, we know of six cases where
copyright. on 1 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.423.50 on 1 January 1961. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
the sternum has been fixed by rigid internalfixation (Sillar, 1961) and with no slings; thesehave shown that this procedure can be effective.Two of them died, neither from causes relatedto the chest, and in every case paradoxical move-ment was controlled. We have tried to deal atthe same time with the ribs by using little medul-lary rods of Kirchner wire, and this has some-times been successful.
I hasten to say that it would be very, veryfoolish to regard this as a matter of competitionbetween chest fixation and respirators. With thesedesperately ill patients, each presents a differentproblem. In the cases of multiple comminutedrib fractures the only possible chance lies in theuse of a positive pressure respirator. The methodsare complementary and I am sure we must beversatile, we must have a lot of methods at ourfinger-tips and in our minds if we are going todo the best for these patients.
PROFESSOR WAYNE: Thank you, Mr. Sillar.Could I just ask a question myself as a physician ?Do you do electrocardiograms on these patients ?Barber (I944), of course, showed that electro-cardiographic abnormalities were very frequentin crush injuries.MR. CLARK: We did not in this case.PROFESSOR WAYNE: Is it generally done by
surgeons or not ? We have Barber's opinionthat it should be; has this been assimilated bythoracic surgeons ? I have only seen this pointas a rule referred to in medico-legal circles, whereit has been shown that there is a very considerableincidence of what has been called bruising of theheart, which must on occasions be of clinicalsignificance.MR. SILLAR: It was in fact shown at the
Glasgow Royal Infirmary by Dr. MalcolmFletcher (I960), when routine ECGs were doneon a series of chest injuries, that some hadtracings which were indistinguishable from thoseof coronary thrombosis. These tracings returnedto normal, usually in two or three weeks.MR. JACK STEVENS: On the matter of the
tension pneumothorax which may occur duringthe induction of the anesthetic, I think there isa good deal to be said for needling both sides ofthe chest as a routine at the time of induction ofthe anesthetic for diagnostic purposes. Thiswould also help in the diagnosis of hamothorax.Griffiths (i960) describes a series of 38 patientswith crushed chests, 29 of whom died; 21 ofthese 29 deaths he thought might have beenavoided by better treatment of asphyxia, respira-tory insufficiency and hemorrhage. So there isa good deal of hope that we should be able to domore for these patients than we have been doingin the past.
DR. M. T. HARRISON: The danger of tensionpneumothorax arising in this sort of injury hasbeen very much stressed and rightly so. Thereis one other complication, however, which maybe seen, namely, surgical emphysema of themediastinum. This may produce angina-like pain,if the patient is conscious, and a crunching soundover the heart as the air churns around during theheart-beat (Hamman's sign). Later one findssubcutaneous emphysema in the neck and finallyobstruction of the superior vena cava, cardiactamponade and death. I wonder if we couldhear a word about the incidence of this in thethoracic surgeon's experience and the best wayto treat it. I wondered also if fat embolismshould be considered as another possible cause forhypertension.DR. W. C. DYKES: In the earliest stage of
surgical emphysema, while the air is still confinedto the pulmonary interstitial tissue, it can alreadymake for ventilatory difficulty and reduced circu-lation and add to the difficulty of inflation fromthe anaesthetist's point of view. When the airreaches the mediastinum, and the mediastinalpressure rises, it produces the further effectsDr. Harrison has mentioned. As pointed out byMacklin (I937), tension pneumothorax may alsobe produced indirectly in surgical emphysema bysplitting of the visceral pleura. As an interestingaside I understand that during the I918 influenzaepidemic a lot of people died in extreme cyanosis,dyspncea and circulatory collapse and were foundat necropsy to have extensive interstitial emphy-sema of the mediastinum. This complication canoccur also with positive pressure respiration,whether intermittent or continuous.MR. SILLAR: May I say one word about fat
embolism ? We had a patient in 1957 whoappeared to be getting into great difficulties withhis respirator before he died. At post portemhe was found to have widespread fat embolism.Indeed, the evidence was there before death inthe form of small petechiae. If fat embolism is afactor there should be signs of it providing thepossibility is kept in mind, and the urine and lungfields examined.
DR. BERNARD LENNOX: In cases in which thechest has to be opened in the course of operationit should be simple to diagnose fat embolism veryearly by lung biopsy. Incidentally, I do not knowof any evidence that fat embolism can causehypertension under any circumstances.
PROFESSOR WAYNE: Would you care to sayanything in summary, Mr. Clark ?MR. CLARK: I think that we have learned a
number of lessons from this case. Here we hadan example of a pure thoracic cage and lunginjury in which tracheostomy and traction on the
January 196icopyright.
on 1 March 2019 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.423.50 on 1 January 1961. Dow
nloaded from

January I961 A Case of Crush Injury of the Chest
flail fragments alone were successful. This isnot always so. In more severe cases where fixa-tion may be inadequate the use of a mechanicalrespirator will be necessary for a prolonged period.The value of tracheostomy is not in doubt, but
the aseptic management of it is very importantand difficult to achieve.The early induction of anaesthesia with positive
pressure may be life-saving, but attention must bepaid to the possible development of tensionpneumothorax and hamothorax. In severe casesit may be advisable to anticipate this by insertingintrapleural water-seal drains immediately afterinduction.
In the case of multiple extra-thoracic injuries,team-work is essential. It would seem to be idealto have special facilities for this purpose. It isour opinion that more lives will be saved whensuch teams gain more experience in their manage-ment, are more aware of the problems involved,and become more skilled in the handling of thetechnological aids that are available.
AcknowledgmentFigs. i (a and b) and 6, and Table i are re-
produced by kind permission of the Editor of theJournal of Bone and Joint Surgery
REFERENCESAVERY, E. E., MORCH, E. T., and BENSON, D. W. (1956): A New Method of Treatment with Continuous Mechanical
Hyperventilation to Produce Alkalotic Apncea and Internal Pneumatic Stabilization, J. thorac. Surg., 32, 291.BARBER, H. (I944): The Effects of Trauma, Direct and Indirect, on the Heart, Quart. J. Med., 13, 137.ENGSTROM, C. G. (I953): Respirator Designed According to a New Principle, Svenska Lak.-Tidn., 50, 545.FLETCHER, M. (1960): Personal communication.GRIFFITHS, H. W. C. (1960): Crush Injuries of the Chest, J. roy. Coll. Surg. Edinb., 6, 13.MACKLIN, C. C. (1937): Pneumothorax with Massive Collapse from Experimental Local Overinflation of the Lung
Substance, Canad. med. Ass. J., 36, 414.SILLAR, W. (1961): The Crushed Chest-Management of the Flail Anterior Segment, J. Bone Jt Surg. In press.
copyright. on 1 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.423.50 on 1 January 1961. D
ownloaded from





























