Embed Size (px)
Citation preview

Keratosis punctata of the palmar creases (KPPC)has been reported marked differences in prevalancerate among races. In black, the condition is a com-mon finding, and even some authors described it as anormal variant ; To review the literature, about100 cases have been published worldwide, almostexclusively in black. But, it is a very rare disease inother races including Asian. Only one case1 of KPPCwas reported in Korea. Herein, we report a case ofKPPC in a 22-year-old Asian man.
CASE REPORT
A 22-year-old Bangladeshian man presentedwith slightly painful, multiple, craterlike depres-sions confined to the palmar creases of the digits andpalms. The first lesions, which were punctiformhyperkeratotic plugs, were noticed 4 years before.Occasionally, some lesions became painful, thickerand then were removed spontaneously, leavingtiny pits, where a new plug developed again a few
days later. He was a manual worker with neitherhistory of arsenic exposure nor syphilis. No lesionwas detected on the soles. There was no familialhistory of similar palmar lesions.
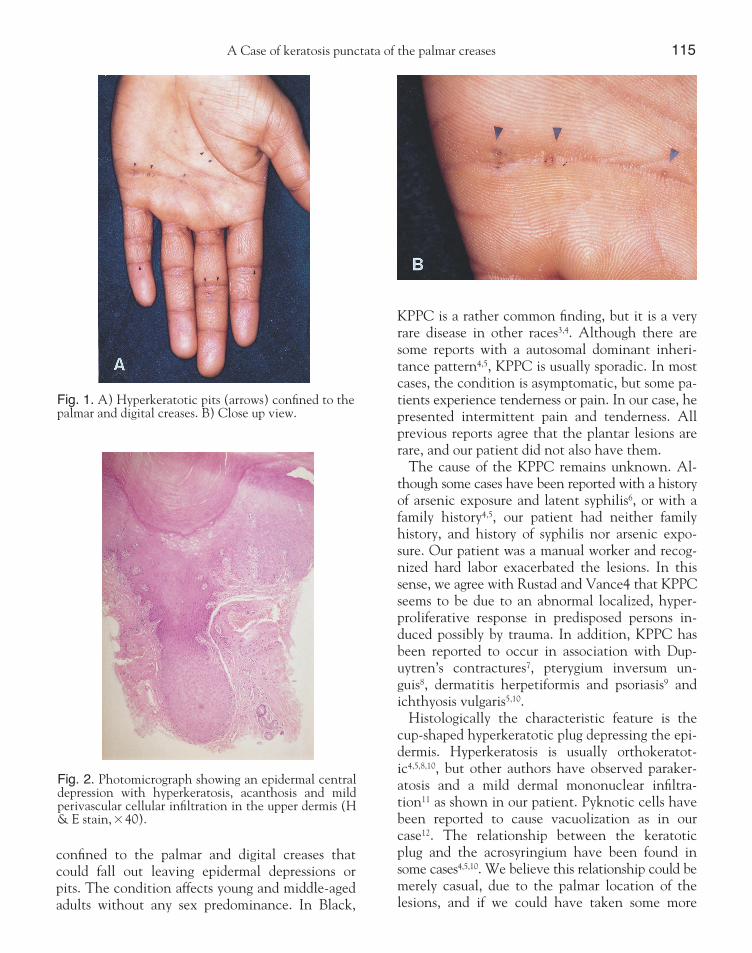
On cutaneous examination, numerous, tiny, hy-perkeratotic, skin colored pits were found on thepalmar creases of both hands, with a predilection forthe transpalmar crease and the proximal interpha-langeal joint crease of the left hand (Fig. 1). Hewas generally in good condition and had no otherskin lesion.
Histologic examination of the serial section of ahyperkeratotic pit revealed cup-shaped epidermalcentral depression with marked parakeratotic hy-perkeratosis and acanthosis. Mild perivascular lym-phohistiocytic cell infiltration was seen in the upperdermis. Focal vacuolated cells were shown in theepidermis, but vertical tiers of parakeratotic cells,clumped keratohyaline grunules and hypergranulosiswere not shown (Fig. 2).
He was treated with only topical emollients, re-sulting in moderate improvement.
DISCUSSION
Keratosis punctata of the palmar creases (KPPC)was first described by Arnold2 in 1947, in a whitemale, as a variant of Kyrle’s disease. The condition isdefined as the presence of punctiform hyperkera-totic plugs, with a raised horn, 1-4mm in diameter
A Case of Keratosis Punctata of the Palmar CreasesHyun Jin Mo, M.D., Tae Yoon Kim, M.D., Jun Young Lee, M.D., Chul Jong Park, M.D.
Departments of Dermatology, Uijongbu St. Mary’s hospital, College of Medicine, The CatholicUniversity of Korea, Uijongbu, Korea.
Keratosis punctata of the palmar creases (KPPC) is a rare skin condition characterized bypunctiform hyperkeratotic pits confined to the palmar and digital creases. Although thiscondition has been regarded as a variant of classical punctate keratoses, there are some dif-ferences between classical punctate keratosis and KPPC. We herein report a case of KPPC ina 22-year-old man who had numerous, tiny, hyperkeratotic pits limited to the palmarcreases of both hands with typical histologic findings.
(Ann Dermatol 14(2) 114-116, 2002).
Key Words : Keratosis punctata of the palmar creases (KPPC)
Received July 7, 2001.
Accepted for publication February 25, 2002.
Reprint request to : Hyun Jin Mo, M.D., Department of
DermatologyUijongbu St. Mary’s Hospital The Catholic
University of Korea
65-1, Kumoh-dong, Uijongbu, Kyonggi-do, 480-130,
Korea
Tel. (031)820-3123, Fax. (031)846-4799
114
A Case of keratosis punctata of the palmar creases 115
confined to the palmar and digital creases thatcould fall out leaving epidermal depressions orpits. The condition affects young and middle-agedadults without any sex predominance. In Black,
KPPC is a rather common finding, but it is a veryrare disease in other races3,4. Although there aresome reports with a autosomal dominant inheri-tance pattern4,5, KPPC is usually sporadic. In mostcases, the condition is asymptomatic, but some pa-tients experience tenderness or pain. In our case, hepresented intermittent pain and tenderness. Allprevious reports agree that the plantar lesions arerare, and our patient did not also have them.
The cause of the KPPC remains unknown. Al-though some cases have been reported with a historyof arsenic exposure and latent syphilis6, or with afamily history4,5, our patient had neither familyhistory, and history of syphilis nor arsenic expo-sure. Our patient was a manual worker and recog-nized hard labor exacerbated the lesions. In thissense, we agree with Rustad and Vance4 that KPPCseems to be due to an abnormal localized, hyper-proliferative response in predisposed persons in-duced possibly by trauma. In addition, KPPC hasbeen reported to occur in association with Dup-uytren’s contractures7, pterygium inversum un-guis8, dermatitis herpetiformis and psoriasis9 andichthyosis vulgaris5,10.
Histologically the characteristic feature is thecup-shaped hyperkeratotic plug depressing the epi-dermis. Hyperkeratosis is usually orthokeratot-ic4,5,8,10, but other authors have observed paraker-atosis and a mild dermal mononuclear infiltra-tion11 as shown in our patient. Pyknotic cells havebeen reported to cause vacuolization as in ourcase12. The relationship between the keratoticplug and the acrosyringium have been found insome cases4,5,10. We believe this relationship could bemerely casual, due to the palmar location of thelesions, and if we could have taken some more
Fig. 1. A) Hyperkeratotic pits (arrows) confined to thepalmar and digital creases. B) Close up view.
Fig. 2. Photomicrograph showing an epidermal centraldepression with hyperkeratosis, acanthosis and mildperivascular cellular infiltration in the upper dermis (H& E stain,×40).

116 HJ Mo, et al.Annals of Dermatology
Vol. 14, No. 2, April 2002
sections of other pits, we would have found it. Although KPPC has been regarded as a variant of
classical punctate keratoses, there are some differ-ences between classical punctate keratosis and KP-PC4. Rustad and Vance considered KPPC as a dis-tinct condition, and proposed the term “keratoticpits of the palmar creases” to distinguish it fromclassical punctate keratoses, which were described as“hyperkeratotic papules scattered diffusely on thepalms and occasionally the soles”4. In brief, “keratoticpits of palmar creases” is a better term in that itdescribes both distinguishing characteristics ofthese lesions-pits rather than papules-and theirdistribution in the creases rather than diffuse distri-bution on the palms and soles. Our case showedcharacteristic keratotic pits confined to the palmarcreases. In addition, the differential diagnosis3 in-cludes basal cell nevus syndrome, palmoplantarporokeratosis, arsenic exposure, acrokeratoelastoi-dosis, and focal acral hyperkeratosis.
The management of KPPC includes simpleemollients, topical tretinoin, oral retinoids4. Surgicaltreatment has also been used for severe and localizeddisease. Owing to lack of symptoms associatedwith KPPC, treatment other than simple emol-lients is seldom required in most cases as well as inour case.
REFERENCES
1. JS Lee, KS Kwon, TA Chung. A case of keratosis
punctata of the palmar creases. Kor J Der 1981;
19:325-329.
2. Arnold HL. Hyperkeratosis penetrans: report of a
case of a probable variant of Kyrle disease. Arch
Dermatol 1947;55:633-638.
3. Kalter DC, Stone MS, Kettler A, Siegel DM,
Rosen T. Keratosis punctata of the palmar crease:
Extremely uncommon? (letter). J Am Acad Derma-
tol 1986;14:510-511.
4. Rustad OJ, Vance JC. Punctate keratosis of the
palms and soles and keratotic pits of the palmar
creases. J Am Acad Dermatol 1990;22:468-76.
5. Del Rio E, Vazques-Veiga H, Aguilar A et al. Ker-
atosis punctata of the palmar creases. A report on
three generations demonstrating an association
with ichthyosis vulgaris and evidence of involve-
ment of the acrosyringium. Clin Exp Dermatol
1994;19:165-167.
6. Dupre A, Christol B, Sorbara AM, Ghrenassia S.
Hyperkeratose ponctuee des plis plamaires. Ann
Dermatol Venereol 1977;104:195-199.
7. Schepart BS, Schwartz RA, Southwick GJ et al.
Dupuytren’s disease presenting as palmar pits. J
Med 1978;9:347-350.
8. Dupre A, Chistol B, Bonafe JL et al. Pterygium in-
versum unguis et atrophie ponctuee des plis pal-
maires. Dermatologica 1981;162:209-212.
9. Thankappan TP, Harilal KR, Zacharia J. Keratosis
punctata of palmar creases [case report]. Indian J
Dermatol Venereol Lepr 1982;48:176-178.
10. M.Just, M.Ribera, I.Bielsa et al. Keratosis punctata of
the palmar crease : report of two cases associated with
ichthyosis vulgaris. Br J Dermatol 1999;141:551-553.
11. Weiss R, Rasmussen J. Keratosis punctata of the
palmar creases. Arch Dermatol 1980;116:669-671.
12. Dobson RL, Young MR, Pinto JS. Palmar keratosis
and cancer. Arch Dermatol 1965;92:553-556.





























