Embed Size (px)
Citation preview

S d 11 A il 2010 ViSunday, 11 April 2010, ViennaECCMID 2010
Grand Rounds
A Case of Persisting or Recurrent gMeningitis
Stephanie B. Troy, M.D.p y,
ESCMID www.escmid.org page 1
ESCMID Online Lecture Library
© by author

History of Present Illness32-year-old woman originally from Mexico with:
Two day history of:– Two day history of:– headache– less-than-five minute episodes of right eye
vision loss, right-sided weakness, and right-, g , gsided numbness.
– No F/C/NS neck stiffness or photophobiaNo F/C/NS, neck stiffness, or photophobia.– No similar headache or any focal neurologic
symptoms in the three years prior to thissymptoms in the three years prior to this presentation.
ESCMID www.escmid.org page 2
ESCMID Online Lecture Library
© by author

Past Medical HistoryOnly significant for a presumptive diagnosis of
tuberculous meningitis three years prior At thattuberculous meningitis three years prior. At that time:Headache neck stiffness and fevers– Headache, neck stiffness and fevers.
– Lumbar puncture: 83 WBCs/µL (53% lymphs, 19% l d 28% ) l f 2 /dL dpolys, and 28% monos), glucose of 2 mg/dL, and a
protein of 548 mg/dL (normal 10-45). – All CSF cultures/serologies were negative. – Brain MRI: mild communicating hydrocephalus.Brain MRI: mild communicating hydrocephalus.– PPD: + at 25 mm (chext X-ray negative).
ESCMID www.escmid.org page 3
ESCMID Online Lecture Library
© by author

Past Medical History– Treated with prednisone and more than nine
months of 4-drug therapy for tuberculousmonths of 4 drug therapy for tuberculous meningitis.Her symptoms resolved after several days– Her symptoms resolved after several days.
– She denied any recurrence of her symptoms until t d i t th t d i itwo days prior to the present admission.
ESCMID www.escmid.org page 4
ESCMID Online Lecture Library
© by author

Social History– Moved from Mexico 6
years prior (no visitsyears prior (no visits since). Several drives to Los– Several drives to Los Angeles on I-5.
S C– Lived in Santa Clara with her brother and 3-year-old daughter.
– No pets or sick contacts.– Worked as a housekeeper.
ESCMID www.escmid.org page 5
ESCMID Online Lecture Library
© by author

Physical ExaminationVitals: Tm 37.1, P 70, BP 110/70, RR 18, O2 sat 100%
General: alert and oriented x 3
HEENT: +papilledema, pupils round and reactive to light, extraocular movements intact. Normocephalic.
Neck: supple
Lymph nodes: no lymphadenopathyLymph nodes: no lymphadenopathy
Lungs: clear to auscultation bilaterally
H l d h h NHeart: regular rate and rhythm. No murmurs.
Abdomen: Soft. Nontender, nondistended. Normal bowel sounds.
Extremities: no edema
Neurology: No focal deficits on initial exam.
ESCMID www.escmid.org page 6
gy
ESCMID Online Lecture Library
© by author
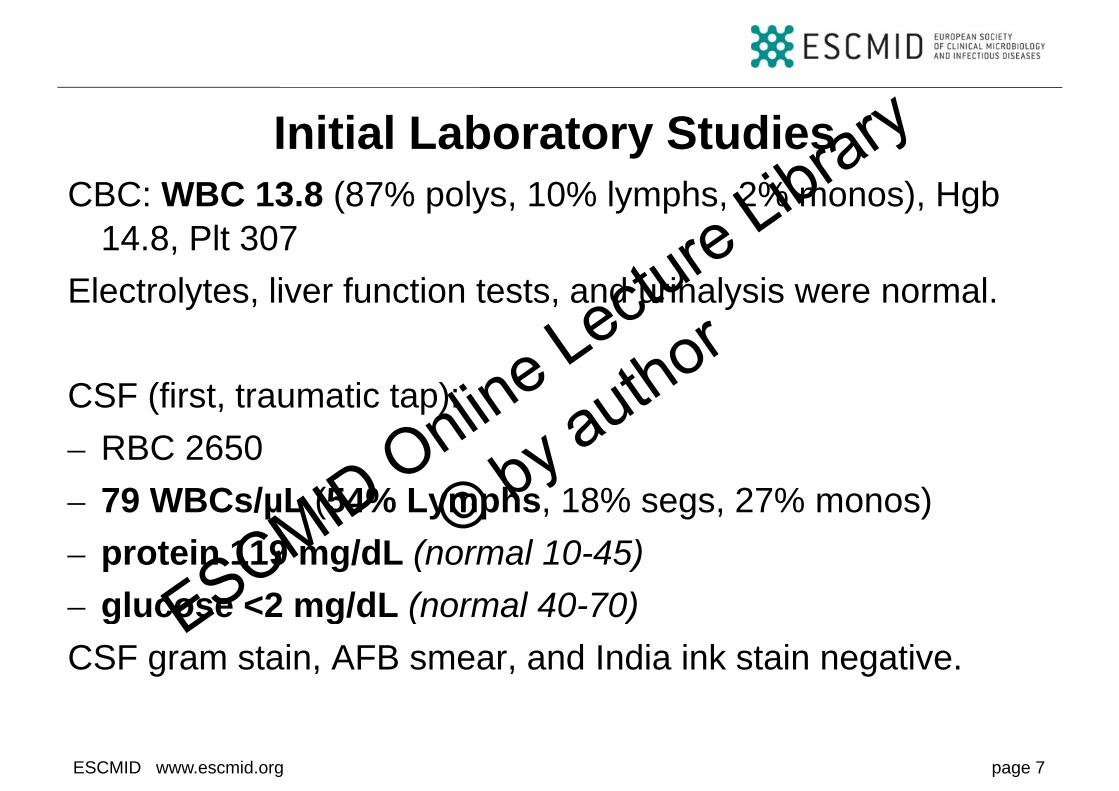
Initial Laboratory StudiesCBC: WBC 13.8 (87% polys, 10% lymphs, 2% monos), Hgb
14.8, Plt 307Electrolytes, liver function tests, and urinalysis were normal.
CSF (first, traumatic tap): RBC 2650– RBC 2650
– 79 WBCs/µL (54% Lymphs, 18% segs, 27% monos)– protein 119 mg/dL (normal 10-45)– glucose <2 mg/dL (normal 40-70)glucose 2 mg/dL (normal 40 70)CSF gram stain, AFB smear, and India ink stain negative.
ESCMID www.escmid.org page 7
ESCMID Online Lecture Library
© by author

Imaging Studies: Brain MRI
ESCMID www.escmid.org page 8
ESCMID Online Lecture Library
© by author

Radiologist Interpretation: Brain MRI– Moderate communicating
hydrocephalus (increased)hydrocephalus (increased).– Mild leptomeningeal
enhancement along theenhancement along the inferior cerebellum, medulla, and most superior portion ofand most superior portion of the spinal cord.C it l b lit– Congenital abnormality consistent with, e.g. mega-i tcisterna magna.
ESCMID www.escmid.org page 9
ESCMID Online Lecture Library
© by author

Hospital CourseA tibi ti t d ft lt f th fi t LP O llAntibiotics were stopped after results of the first LP. Overall,
the patient was asymptomatic. However, she had:– Opthamology exam showing constricted visual fields.– 2 more <5 minute episodes of R eye blindness.p y– 1 episode of L hand numbness.
Intermittent unsteadiness when walking– Intermittent unsteadiness when walking.
CSF (multiple subsequent taps over next 2 weeks): – 10-79 WBCs/µLwith lymphocytic predominance (54-94%).µ y p y p ( )– protein 80-119 mg/dL (normal 10-45).
glucose <2 mg/dL (normal 40 70)
ESCMID www.escmid.org page 10
– glucose <2 mg/dL (normal 40-70).
ESCMID Online Lecture Library
© by author

Wh t th t t ld d ?What other tests would you order?
ESCMID www.escmid.org page 11
ESCMID Online Lecture Library
© by author

Further Diagnostic TestsCSF f l i l b t i l d AFB lt ti t d t– CSF fungal, viral, bacterial, and AFB cultures negative to date
– CSF MTB PCR –– HIV –– ANA –ANA – CSF lyme PCR and lyme C6 –
B ll l– Brucella serology –– Urine histoplasma Ag –– CSF cryptococcal Ag –– CSF HSV PCR –– RPR and TPPA –
CSF cytology : “mixed inflammatory cells”
ESCMID www.escmid.org page 12
– CSF cytology : mixed inflammatory cells
ESCMID Online Lecture Library
© by author

Further Diagnostic Tests: Gadolinium Enhanced MRI Spinep
ESCMID www.escmid.org page 13
ESCMID Online Lecture Library
© by author

Gadolinium Enhanced MRI Spine
ESCMID www.escmid.org page 14
ESCMID Online Lecture Library
© by author

Radiologist Interpretation: MRI Spine– Multi-focal plaque-like
leptomeningeal and duralleptomeningeal and dural enhancement throughout the spine basal cisterns and sellaspine, basal cisterns, and sella.
– Hydrocephalus.
Cl i f h– Clumping of the nerve roots compatible with leptomeningitis.
ESCMID www.escmid.org page 15
ESCMID Online Lecture Library
© by author
A diagnostic test was performed.
What is the most likely diagnosis?y g
ESCMID www.escmid.org page 16
ESCMID Online Lecture Library
© by author

Diagnosis: NeurocysticercosisCSF cysticercosis ELISA was positive at 26.53 (normal is <0.75).CSF and serum cysticercosis western blots were positiveCSF and serum cysticercosis western blots were positive.Coccidioides serum and CSF serology were negative.Neurosurgery placed a ventriculostomy at which time a number of racemose cysts were extirpated from the cisterna magna. H&E Stain showed an area of well-preserved, folded tegument of a cysticerci.
ESCMID www.escmid.org page 17
ESCMID Online Lecture Library
© by author

Diagnosis: Neurocysticercosis
ESCMID www.escmid.org page 18T��� SB �� ��� IDCP 2009�17�5�323�325�
ESCMID Online Lecture Library
© by author

NeurocysticercosisIngestion of Taenia solium eggs.
Most common cause of acquiredMost common cause of acquired epilepsy.
E d i i L ti A i A iEndemic in Latin America, Asia, and Africa.
Can remain latent for 2-5 years.
Cysts can be:
Parenchymal (91%)
Ventricular(6%)Ventricular(6%)
Subarachnoid (2%)
S i l (0 2%)
ESCMID www.escmid.org page 19
Spinal (0.2%)
ESCMID Online Lecture Library
© by author

Subarachnoid NeurocysticercosisCan grow abnormally as a membranous and/or cystic mass (racemose cysticercosis)(racemose cysticercosis).Commonly present with symptoms of increased intracranial pressure meningeal irritation and focal neurologic deficitspressure, meningeal irritation, and focal neurologic deficits.Hydrocephalus and abnormal basilar leptomeningeal
h t th t di hi fi dienhancement are the most common radiographic findings.CSF findings are variable (in two case series of all types of neurocysticercosis, 38-83% had CSF pleocytosis, 30-45% had elevated CSF protein, and 6-45% had hypoglycorrhachia, defined as CSF glucose <50 mg/dL).
ESCMID www.escmid.org page 20
ESCMID Online Lecture Library
© by author
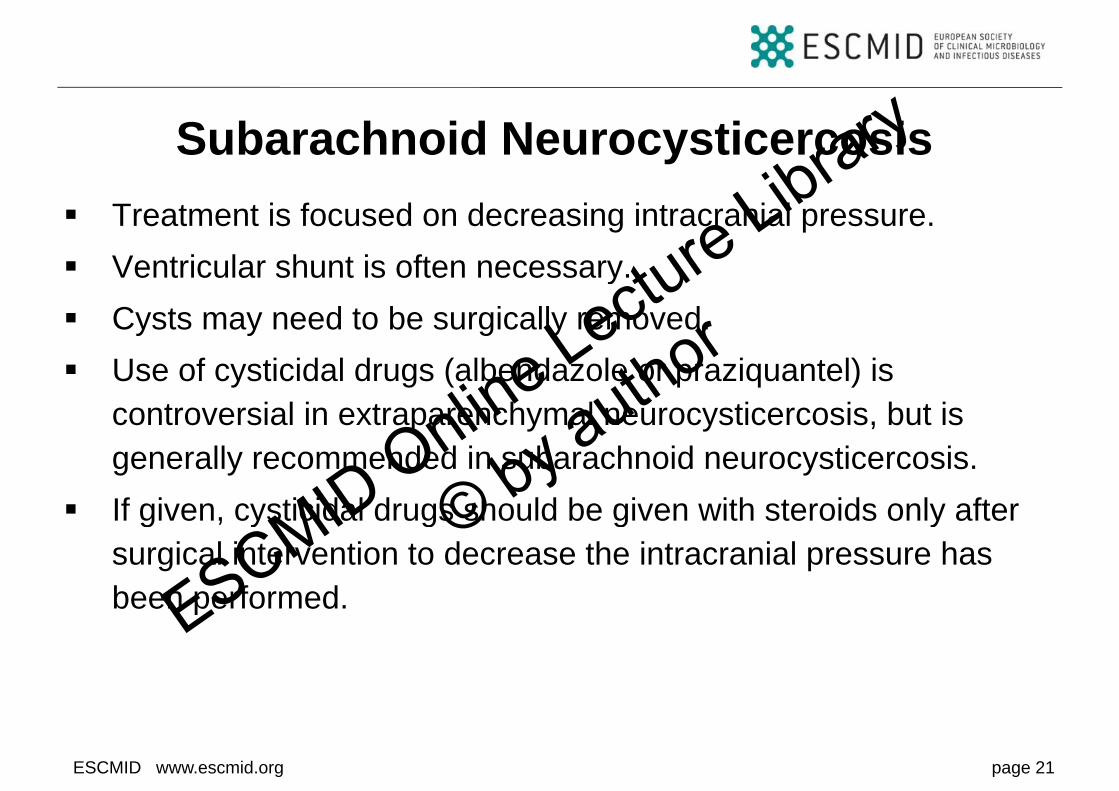
Subarachnoid NeurocysticercosisTreatment is focused on decreasing intracranial pressure.Ventricular shunt is often necessaryVentricular shunt is often necessary.Cysts may need to be surgically removed.Use of cysticidal drugs (albendazole or praziquantel) is controversial in extraparenchymal neurocysticercosis, but is generally recommended in subarachnoid neurocysticercosis.If given, cysticidal drugs should be given with steroids only after g y g g ysurgical intervention to decrease the intracranial pressure has been performed.
ESCMID www.escmid.org page 21
ESCMID Online Lecture Library
© by author

Case ConclusionPatient had neurosurgery. A number of racemose cysts were extirpated from the posterior fossa; and a ventriculostomy wasextirpated from the posterior fossa; and a ventriculostomy was placed.She was then treated with four weeks of albendazole andShe was then treated with four weeks of albendazole and steroids.H t d d h lti t l i dHer symptoms recurred, and she ultimately required a ventriculoperitoneal shunt.She was asymptomatic four months after shunt placement when she moved back to Mexico.
ESCMID www.escmid.org page 22
ESCMID Online Lecture Library
© by author
AcknowledgementsI am indebted to Drs. Gulshan Bhatia, Andrea Polesky, and
Aarthi Chary for their assistance in initially writing up theAarthi Chary for their assistance in initially writing up the case for publication.
(Troy SB, Chary A, Polesky A, Bhatia G. A Woman with Hydrocephalus and Severe Hypoglycorrhachia. Infectious Diseases in Clinical Practice. 2009;17(5):323-325.)
I am indebted to Professor Robert Read and Doctor Stan Deresinski for their assistance in preparing the case for presentation at ECCMID.
ESCMID www.escmid.org page 23
p
ESCMID Online Lecture Library
© by author

Bibliography1. García H, Gonzalez A, Evans C, Gilman R. Taenia solium cysticercosis. Lancet
2003 Aug;362(9383):547-562003 Aug;362(9383):547-56.
2. Garcia H, Del Brutto O. Neurocysticercosis: updated concepts about an old
disease Lancet Neurol 2005 Oct;4(10):653-61disease. Lancet Neurol 2005 Oct;4(10):653-61.3. Wallin M, Kurtzke J. Neurocysticercosis in the United States: review of an
important emerging infection Neurology 2004 Nov;63(9):1559-64important emerging infection. Neurology 2004 Nov;63(9):1559-64.
4. Cuetter A, Garcia-Bobadilla J, Guerra L, Martinez F, Kaim B.
Neurocysticercosis: focus on intraventricular disease Clin Infect Dis 1997Neurocysticercosis: focus on intraventricular disease. Clin Infect Dis 1997Feb;24(2):157-64.
5 Garcia H Del Brutto O Nash T White AJ Tsang V Gilman R New concepts in5. Garcia H, Del Brutto O, Nash T, White AJ, Tsang V, Gilman R. New concepts in the diagnosis and management of neurocysticercosis (Taenia solium). Am J
Trop Med Hyg 2005 Jan;72(1):3-9
ESCMID www.escmid.org page 24
Trop Med Hyg 2005 Jan;72(1):3-9.
ESCMID Online Lecture Library
© by author
Bibliography6. Cuetter A, Andrews R. Intraventricular neurocysticercosis: 18 consecutive
patients and review of the literature Neurosurg Focus 2002 Jun;12(6):e5patients and review of the literature. Neurosurg Focus 2002 Jun;12(6):e5.
7. Shandera W, White AJ, Chen J, Diaz P, Armstrong R. Neurocysticercosis in
Houston Texas A report of 112 cases Medicine (Baltimore) 1994Houston, Texas. A report of 112 cases. Medicine (Baltimore) 1994Jan;73(1):37-52.
8 Loo L Braude A Cerebral cysticercosis in San Diego A report of 23 cases and8. Loo L, Braude A. Cerebral cysticercosis in San Diego. A report of 23 cases and
a review of the literature. Medicine (Baltimore) 1982 Nov;61(6):341-59.
9 Del Brutto O Neurocysticercosis Semin Neurol 2005 Sep;25(3):243-519. Del Brutto O. Neurocysticercosis. Semin Neurol 2005 Sep;25(3):243-51.
ESCMID www.escmid.org page 25
ESCMID Online Lecture Library
© by author