Embed Size (px)
Citation preview
CASE REPORT
A case of significantly increased mitral regurgitation earlyafter atrial septal defect closure
Masataka Nishiga • Chisato Izumi • Hayato Matsutani • Sumiyo Hashiwada •
Shuichi Takahashi • Yukiko Hayama • Seiko Nakajima • Jiro Sakamoto •
Koji Hanazawa • Makoto Miyake • Toshihiro Tamura • Hirokazu Kondo •
Makoto Motooka • Kazuaki Kaitani • Yoshihisa Nakagawa
Received: 15 February 2012 / Revised: 4 April 2012 / Accepted: 5 April 2012 / Published online: 19 April 2012
� Japanese Society of Echocardiography 2012
Abstract We report a rare case in which mitral regurgi-
tation (MR) was exacerbated to a severe level early after
atrial septal defect (ASD) closure, even though the female
patient had preoperatively mild MR and mild changes in
mitral valve (MV) and sinus rhythm. The mechanism of
increased MR was considered as poor coaptation and
tethering of the MV due to the restricted motion of the
posterior leaflet in addition to geometric changes of the left
ventricle (LV) after ASD closure.
Keywords Atrial septal defect � Mitral regurgitation �ASD plaque � Tethering � Geometric change �Echocardiography
Case report
A 72-year-old woman without symptoms was referred to
our hospital because of a moderately sized atrial septal
defect (ASD). A transthoracic echocardiography (TTE)
(Fig. 1a, c) showed that she had secundum ASD with
enlarged right atrium and ventricle, which is compressing
the left ventricle (LV). The diameter of the defect was
about 20 mm. The LV ejection fraction was normal.
Moderate pulmonary hypertension was detected (tricuspid
regurgitation velocity 3.8 m/s). The leaflets of the mitral
valve (MV) were mildly thickened with mild mitral
regurgitation (MR). A transesophageal echocardiography
(TEE) (Fig. 2a, c) also showed mildly thickened mitral
leaflets without prolapse and the amount of MR was mild.
The patient underwent surgery to repair the ASD. The
defect was directly closed. Tricuspid annuloplasty was also
conducted. She underwent a concomitant Maze procedure
because she had a history of paroxysmal atrial fibrillation.
She was discharged without symptoms. However,
1 month later, she was admitted to our department because
of congestive heart failure. TTE showed normal LV
function, moderate MR, and no leak of the closed ASD.
Also, TTE (Fig. 1b, d) and TEE (Fig. 2b, d) at 2 months
after surgery showed additionally increased MR.
The size of the chambers became close to normal,
improving compression of the LV. Mitral valve leaflets
were the same as before surgery, but they were pulled to
the LV wall, associated with LV enlargement. Motion of
the posterior leaflet was slightly restricted. These resulted
in poor coaptation between the anterior and posterior
leaflets. Severe MR signal showed a wide regurgitant ori-
fice and jetted into the posterior wall of the left atrium.
There was no mitral valve prolapse, perforation, chordal
rupture, nor vegetation. She underwent mitral valve
replacement.
Discussion
There are several reports discussing preoperative and
postoperative MR in adult patients with ASD [1–3]. It is
M. Nishiga (&) � C. Izumi � Y. Hayama � S. Nakajima �J. Sakamoto � K. Hanazawa � M. Miyake � T. Tamura �H. Kondo � M. Motooka � K. Kaitani � Y. Nakagawa
Department of Cardiology, Tenri Hospital, 200 Mishima-cho,
Tenri, Nara 632-8552, Japan
e-mail: [email protected]
H. Matsutani � S. Hashiwada � S. Takahashi
Department of Clinical Pathology, Tenri Hospital, Tenri, Japan
123
J Echocardiogr (2012) 10:69–71
DOI 10.1007/s12574-012-0123-3
noted that, in some cases, MR may increase after ASD
closure. The mechanism of increased MR is commonly due
to heavily thickened anterior leaflet, called ASD plaque [4],
preoperative underestimation of MR due to decreased
trans-mitral flow, or persistent atrial fibrillation. There
seemed to be additional mechanisms in this case.
Generally, after ASD closure, geometric changes such as
improvement of the leftward deviation of the ventricular
septum are seen because of the decrease in left-to-right
shunt [1]. In this case, the mechanism of increased MR is
unclear, but it is assumed that poor coaptation may have
been masked because of the preoperatively reduced LV size
due to left-to-right shunt, though the motion of the posterior
leaflet was mildly restricted and the chordae tendineae were
slightly thickened and shortened with careful attention on
preoperative TTE. After ASD closure, because the LV size
became larger than it had been before surgery, mitral leaf-
lets were pulled to the LV wall and coaptation became
worse, which looked like ‘‘tethering’’ of ischemic MR.
From this case, we learned that it is necessary to pay
attention to the motion of the posterior mitral leaflet and
changes of the chordae tendineae, as well as thickened
anterior leaflet in patients with ASD, and to predict chan-
ges of coaptation and tethering by geometric changes of the
LV after ASD closure. In addition, it is also necessary to
follow MR closely after ASD closure.
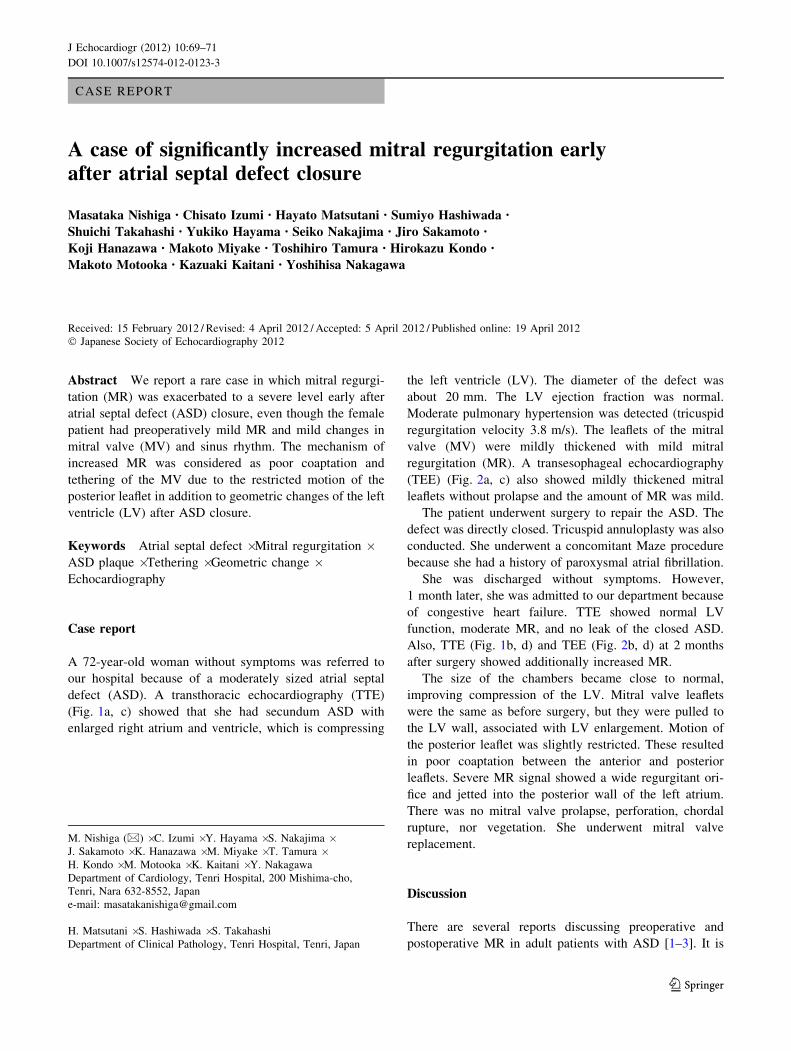
Fig. 1 Coaptation of mitral leaflets became worse after atrial septal
defect (ASD) closure, and mitral regurgitation (MR) was increased.
a, c Parasternal view of transthoracic echocardiography (TTE) before
ASD closure (LVDd/Ds 38/27, tenting area 1.38 cm2, tenting height
7.2 mm, mitral annulus 38.4 mm). b, d Parasternal view of TTE after
ASD closure (LVDd/Ds 44/26, tenting area 1.93 cm2, tenting height
9.4 mm, mitral annulus 37.7 mm)
70 J Echocardiogr (2012) 10:69–71
123
Conflict of interest There is no conflict of interest to disclose.
References
1. Park J-J, Lee SC, Kim JB, et al. Deterioration of mitral valve
competence after the repair of atrial septal defect in adults. Ann
Thorac Surg. 2011;92:1629–33.
2. Izumi C, Iga K, Kondo H, et al. Progression of mitral regurgitation
after patch closure in patients with secundum atrial septal defect.
Cardiovasc Rev Rep. 2001;22:297–301.
3. Toyono M, Pettersson GB, Matsumura Y, et al. Preoperative and
postoperative mitral valve prolapse and regurgitation in adult
patients with secundum atrial septal defects. Echocardiography.
2008;25:1086–93.
4. Nagata S, Nimura Y, Sakakibara H, et al. Mitral valve lesion
associated with secundum atrial septal defect. Analysis by real
time two dimensional echocardiography. Br Heart J. 1983;49:
51–8.
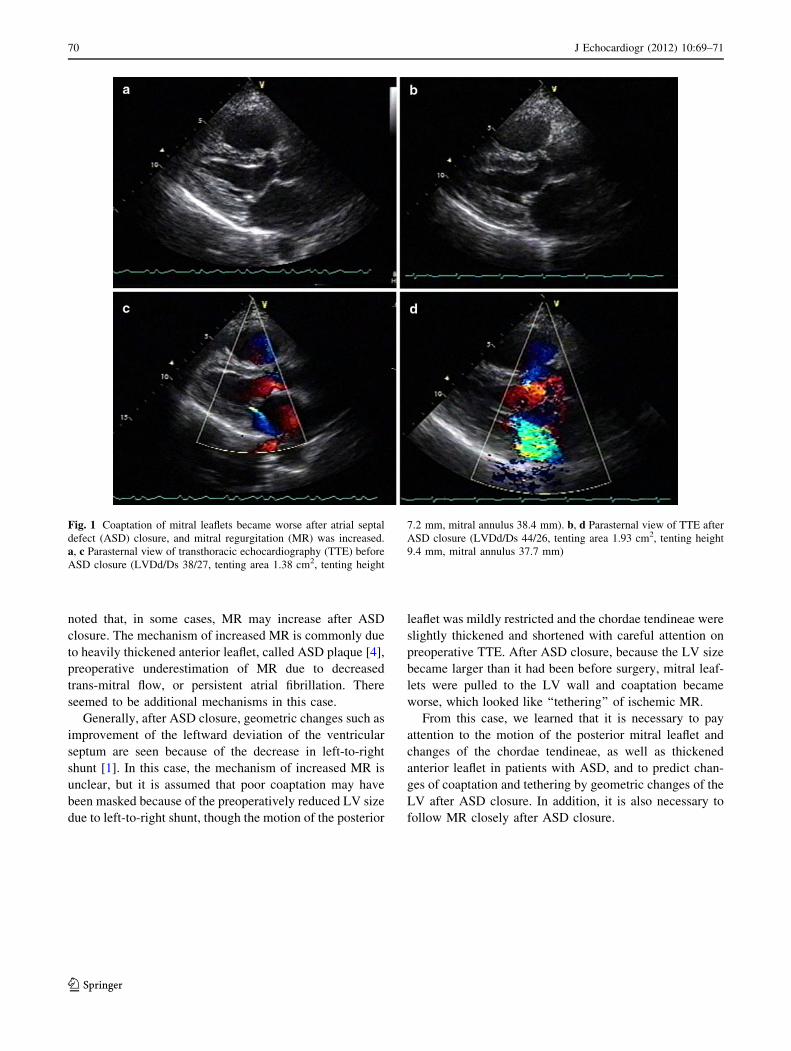
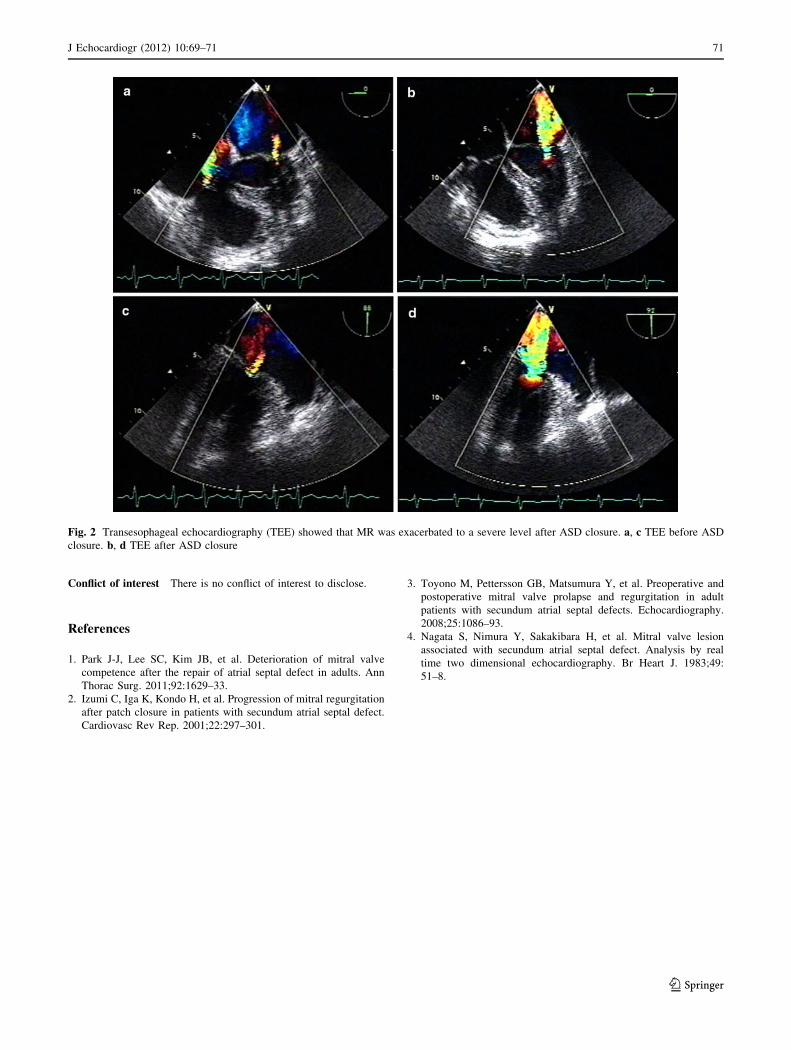
Fig. 2 Transesophageal echocardiography (TEE) showed that MR was exacerbated to a severe level after ASD closure. a, c TEE before ASD
closure. b, d TEE after ASD closure
J Echocardiogr (2012) 10:69–71 71
123





























