Embed Size (px)
Citation preview

A CLINICAL STUDY ON SURGICAL MANAGEMENT OF DIAPHYSEAL FRACTURES
OF TIBIA BY INTRAMEDULLARY INTERLOCKING NAIL
By Dr.BASU VENKATRAMAIAH
Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Karnataka,
Bangalore
In partial fulfillment of the requirements for the degree of
MASTER OF SURGERY in
ORTHOPAEDICS
Under the Guidance of Dr.PRAMOD B.ITAGI
M.S. (Ortho)
Associate Professor
DEPARTMENT OF ORTHOPAEDICS
i

M.R. MEDICAL COLLEGE, GULBARGA-585 105
ii

RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BANGALORE
DECLARATION BY THE CANDIDATE
I here by declare that this dissertation/ thesis entitled “A
CLINICAL STUDY ON SURGICAL MANAGEMENT OF
DIAPHYSEAL FRACTURES OF TIBIA BY
INTRAMEDULLARY INTERLOCKING NAIL” is a
bonafide and genuine research work carried out by me under
the guidance of Dr.PRAMOD B.ITAGI, M.S., (Ortho),
Associate Professor, Dept. of Orthopaedics.
Date:
Place: GULBARGA Dr.BASU VENKATRAMAIAH
iii

RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BANGALORE
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “A
CLINICAL STUDY ON SURGICAL MANAGEMENT OF
DIAPHYSEAL FRACTURES OF TIBIA BY
INTRAMEDULLARY INTERLOCKING NAIL” is a bonafide
research work done by Dr.BASU VENKATRAMAIAH in partial
fulfillment of the requirement for the degree of MASTER OF
SURGERY in ORTHOPAEDICS.
Date:
Place: GULBARGA Dr.PRAMOD B.ITAGI M.S. (Ortho)
Associate Professor Department of Orthopaedics M.R. Medical College, Gulbarga
iv
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BANGALORE
ENDORSEMENT BY THE HOD, PRINCIPAL/
HEAD OF THE INSTITUTION
This is to certify that the dissertation entitled “A
CLINICAL STUDY ON SURGICAL MANAGEMENT OF
DIAPHYSEAL FRACTURES OF TIBIA BY
INTRAMEDULLARY INTERLOCKING NAIL” is a bonafide
research work done by Dr.BASU VENKATRAMAIAH under the
guidance of Dr.PRAMOD B.ITAGI, M.S. (Ortho) Associae
Professor, Department of Orthopaedics.
Dr.B.C.Patil Dr.Mallikarjun B. D.Ortho., M.S. (Ortho) M.D. (Paed) Head of the Dept. Principal Dept. of Orthopaedics M.R. Medical College, Gulbarga M.R. Medical College, Gulbarga Date: Date:
Place: GULBARGA Place: GULBARGA
v
COPYRIGHT
DECLARATION BY THE CANDIDATE
I here by declare that the Rajiv Gandhi University of Health
Sciences, Karnataka shall have the rights to preserve, use
and disseminate this dissertation/ thesis in print or
electronic format for academic/ research purpose.
Date:
Place: GULBARGA Dr.BASU VENKATRAMAIAH
© Rajiv Gandhi University of Health Sciences, Karnataka.
vi

ACKNOWLEDGEMENT
I dedicate this dissertation to my parents and brother for
providing the strength, time, unconditional love, care and especially
for cushioning all my falls in my life and directed me to the path of
success.
I avail this opportunity to express my profound earnest
gratitude to my beloved teacher guide Dr.Pramod Itagi, M.S.
(Ortho), Associate Professor of Orthopaedics, for his esteemed
guidance, unflinching support, keen surveillance, in estimable aid
and continued inspiration, at the same time who has been a source of
sustained illumination to me, whose valuable guidance and generous
support facilitated me to accomplish this dissertation.
I owe my sincere and grateful acknowledgement to
Dr.B.C.Patil, M.S. (Ortho), D.Ortho., Professor and H.O.D.,
Department of Orthopaedics, for his valuable guidance and
encouragement.
My sincere thanks are to Dr.Sanjeev Reddy, M.S. (Ortho),
D.Ortho. and Dr.S.S.Gubbi, M.S.(Ortho), Associate Professors of
Orthopaedics for their constant help and encouragement during the
period of study and while preparing this dissertation.
I also take this opportunity to express my sincere gratitude to
Dr.S.B.Kamareddy, M.S.(Ortho), Assistant Professor,
Dr.Arunkumar Kulkarni, D.Ortho., Senior Registrar, Department of
Orthopaedics, for their help and guidance.
vii

I owe my sincere gratitude to Dr.B.Mallikarjun, M.D. (Paed),
Principal & Dean, M.R.Medical College, for his guidance and
encouragement.
I am very thankful to Dr.Dilip Rampure, M.D.(Med), Medical
Superintendent, Basaveshwar Teaching & General Hospital attached
to M.R.Medical College, for permitting me to utilize the clinical
material for this dissertation.
I gratefully acknowledge the patients, who cooperated to
submit themselves for this study, without whom, this dissertation
would not have been possible.
I would not do justice if I don’t express my sincere and warm
gratitude to my colleagues Dr.Ramesh, Dr.Nishanth, Dr.Akash,
Dr.Prakash, Dr.Naga, Dr.Somshekhar, Dr.Himakanth, Dr.Sudeep,
Dr.Harsha, Dr.Kiran, Dr.Shivkumar, Dr.Veeresh, Dr.Vijay,
Dr.Chaitanya, Dr.Shyam and Dr.Arun for their valuable hints and
timely help ensuring that this dissertation saw the light of the day.
I am also thankful to my friends Dr.Shankar, Dr.Vijay,
Dr.Rajeev, Dr.Sanjeev, Dr.Hari and Dr.Suneel for their moral
support.
I thank all my colleagues and friends for their valuable help
in completing this dissertation.
Date:
Place: Dr.BASU VENKATRAMAIAH
viii

LIST OF ABBREVIATIONS USED
AO................... Arbeitsgemeinschaft fur osteosynthesefragen
ASIF................ Association for the Study of Internal Fixation
ESIN................ Elastic stable intramedullary nail
IM nail............. Intramedullary nail
OTA ................Orthopaedic Trauma Association
POP ................. Plaster of paris
ix

ABSTRACT
Background & Objectives: To assess and study diaphyseal fractures of tibia and to evaluate the functional outcome of patients with tibial shaft fracture treated with locked intramedullary nailing. Materials & Methods: Patients: Patients of both sexes belonging to adult age group presenting with fracture shaft tibia to orthopedic department of Basaveshwar Teaching & General Hospital, Gulbarga attached to M.R.Medical College, Gulbarga are admitted from October 2006 to March 2008 and evaluated. Those satisfying our inclusion criteria and are surgically fit are included in this study. Intervention: All enrolled patients were treated with locked intramedullary nailing of their tibia. Main Outcome Measurements: All enrolled patients were evaluated with Johner & Wruh’s criteria. Final assessment in our series was done at 6 months taking into account of the following objective and subjective symptoms of gait, pain, deformity, range of motion of knee, angle and sub-talar joints, shortening, neurovascular disturbances, ability to do strenuous activities, radiological union and presence or absence of non-union. Functional outcome was graded into excellent, good, fair and poor. Results: The results of interlocking fracture shaft tibia were excellent in 12 patients (60%), good in patients (30%) and fair in 2 patients (10%). The average healing time was 19.1 weeks. There were 2 superficial infections (10%) and 2 patients with anterior knee pain (10%). Conclusion: The method of treatment employing closed intramedullary interlocking nailing to stabilize diaphyseal fractures of tibia is ideal because of its excellent and good results. The method has a long learning curve but with the excellent results. The advantage of rapid rehabilitation and relatively few complications serve to recommend it for wider use. Key Words: Diaphyseal fractures of tibia; Interlocking; Closed nailing.
x
LIST OF CONTENTS
1. Introduction..........................................................................................01
2. Objectives ............................................................................................03
3. Review of Literature ............................................................................04
• Historical Review...........................................................................04
• Review of Literature on Intramedullary Nailing ...........................13
• Surgical Anatomy ..........................................................................26
• Classification of Tibial Shaft Fractures .........................................39
• Fracture Mechanics........................................................................44
• Biomechanics of Intramedullary Locked Nail ...............................47
• Biology of Fracture and Fracture Healing with Intramedullary Locked Nail...........................................................51
• Advantages, Disadvantages and Complications of Intramedullary Interlocking Nailing ..............................................54
• Approaches ....................................................................................57
4. Materials & Methods ...........................................................................59
5. Observations and Results.....................................................................77
6. Discussion............................................................................................98
7. Summary ............................................................................................106
8. Conclusion .........................................................................................108
9. Bibliography ......................................................................................110
10. Annexures ..........................................................................................118
Proforma
Master Chart
Key to Master Chart
xi

LIST OF TABLES
Sl. No. Title Page
No.
1. Age Incidence 77
2. Sex Incidence 78
3. Involved Limb 79
4. Mode of Injury 80
5. Anatomical Location of the Fracture 81
6. Type of Injury 82
7. Type of Fracture 83
8. Weight-bearing 85
9. Fracture Union 86
10. Complications 87
11. Functional Outcome 89
xii

LIST OF FIGURES
Sl. No. Title Page
No. 1. Muscles of Leg – Anterior View 26 2. Muscles of Leg – Posterior View 29 3. Bones of the Leg – Tibia and Fibula 31 4. Anterior tibial and dorsalis pedis arteries 35 5. Posterior Tibial and Peroneal Arteries 37 6. Instrumentation Set for Tibia Intramedullary Locking Nail 74 7. Surgical Technique of Interlocking Tibia 75 8. Age Incidence 77 9. Sex Incidence 78 10. Involved Limb 79 11. Mode of Injury 80 12. Anatomical Location of the Fracture 81 13. Type of Injury 82 14. Type of Fracture 83 15. Weight-bearing 85 16. Fracture Union 86 17. Complications 87 18. Functional Outcome 89 19. Case No. 1: Clinical Photographs of the Patient at Six Months
showing Full Weight Bearing and Movements of Knee & Ankle 90
20. Case No. 1: Radiographs - A/P & Lateral 91 21. Case No. 4: Clinical Photographs of the Patient at 6 months showing
full weight bearing and movements of Knee and Ankle 92
22. Case No. 4: Radiographs - A/P & Lateral 93 23. Case No. 15: Clinical Photographs of the Patient at 6 months
showing full weight bearing and movement of Knee and Ankle 94
24. Case No. 15: Radiographs - A/P & Lateral 95 25. Case No. 16: Clinical photographs of the patient at 6 months
showing full weight bearing and movements of Knee and Ankle 96
26. Case No. 16: Radiographs - A/P & Lateral 97
xiii
INTRODUCTION
With the increasing number of vehicles on roads in India, complex
trauma cases caused by road traffic accidents have increased progressively.
Being sub-cutaneous in location, the tibia is the commonest bone to be
fractured and seen commonly in orthopedic practice.
Open fractures are more common, because one third of its surface is
subcutaneous throughout most of its length. Furthermore, the blood supply to
the tibia is more precarious than that of bones enclosed by heavy muscles.
The presence of hinge joints at the knee and ankle allows no adjustment for
rotatory deformity after a fracture. Delayed union, non-union and infection
are relatively frequent complications especially after open fractures of the
shaft of tibia.
Due to its frequency, topography and mode of injury it has become a
major source of temporary disability and morbidity.
Hence special care and expertise is necessary when treating such
fractures. It requires the widest experience, the greatest wisdom and the nicest
of the clinical judgement in order to choose the most appropriate treatment for
a particular pattern of injury.
1

The major goal in the treatment of fracture tibia is achieving
functionally useful and stable extremity. Yet the spectrum of injuries to tibia
is so great that no single method of treatment is applicable to all fractures.
Management of the fractures of the shaft of the tibia remained a
controversial subject despite advances in both non-operative and operative
care. Sir John Charnley stated that, “we have still a long-way to go before the
best method of treating a fracture of the shaft of tibia can be stated with
finality” in 1961. Several published series regarding treatment of fractures of
the shaft of tibia have shown that closed treatment of fractures can have
excellent results. But the drawbacks of prolonged healing time, fracture
disease, malalignment and non-compliance of the patient has led to the
thought of other modalities of treatment, finally resulting in the use of closed
interlocking intramedullary nailing which has given excellent results.
Now-a-days the well laid principle of biological osteosynthesis is
rightly applied in long bone fracture healing and hence the selection of closed
intramedullary interlocking nailing in this study.
The following study highlights the role of closed interlocking nailing
used for treating the fractures of the shaft of tibia.
2

AIMS AND OBJECTIVES
The tibial diaphyseal fracture is the commonest fracture encountered,
and the locked intramedullary interlocking nailing has revolutionized the
management of tibial diaphyseal fractures.
The use of interlocking nails means that virtually all tibial diaphyseal
fractures can be stabilized with an intramedullary nail, and the well laid
principle of biological osteosynthesis is rightly followed here.
The objectives of the study are:
1. To assess and study diaphyseal fractures of tibia with special
reference to fracture anatomy, pattern and status of stability.
2. To study fracture healing and the union rates with intra-
medullary interlocking nail.
3. To study the functional outcome with regard to knee, ankle and
subtalar joint movements.
4. To prevent angulation, deformity and to maintain limb length
equality.
5. To mobilize the patient as early as possible.
3

REVIEW OF LITERATURE
Historical Review:
The history of intramedullary nailing for the treatment of long bone
fractures and nonunions is long and storied. From the earliest recorded
examples in 16th century Mexico to the current procedures of today, there has
been an evolution of design, materials, and basic science principles, which has
resulted in a well accepted and successful technique for the past several
decades. Interestingly, throughout the early history of intramedullary nailing,
these advances in method, principle, and design appear to parallel advances in
anesthetic and aseptic techniques, allowing for routine operative care of
fractures to emerge. Although intramedullary nailing is now the standard of
care for the treatment of most diaphyseal lower extremity fractures,
introduction of the technique was met with a great deal of skepticism in both
Europe and North America during the first half of the 20th century. In the
latter half of the 20th century, intramedullary nailing of long bone fractures
revolutionized the care of the multiply injured patient.
The Beginnings
Bernardino de Sahagun, a 16th century anthropologist who traveled to
Mexico with Hernando Cortes, recorded the first account of the use of an
intramedullary device.1 De Sahagun witnessed Aztec physicians placing
wooden sticks into the medullary canals of patients with long bone nonunions.
4
Other pre-Twentieth century intramedullary techniques also seemed to
be conducted in patients with nonunions and not in patients with acute long
bone fractures. During the mid 1800s through the first decade of the 1900s,
most of the work in intramedullary nailing of nonunions appear to revolve
around the use of ivory pegs. It had been observed that ivory pegs would
reabsorb in the human body compared to metallic implants, which became
encapsulated with fibrous material. The majority of this work was reported at
the time in the German literature.2,3 During the 1890s, Gluck recorded the first
description of an interlocked intramedullary device.4 The device consisted of
an ivory intramedullary nail that contained holes at the end, through which
ivory interlocking pins could be passed. Around the same time period,
Nicolaysen of Norway described the biomechanical principles of
intramedullary devices in the treatment of proximal femur fractures.5
Nicolaysen proposed that the length of intramedullary implants be maximized
to provide for the best biomechanical advantage. While ivory seemed to be the
material of choice reported in the German literature, Hoglund of the United
States reported the use of autogenous bone as an intramedullary implant in
1917.6
He described a technique in which a span of the cortex was cut out and
then passed up the medullary cavity across the fracture site. During World
War I, Hey Groves of England reported the use of metallic rods for the
treatment of gunshot wounds.7 These rods were passed into the medullary
cavity through an incision made over the fracture site. This technique appeared
5

to have a high infection rate and was not universally accepted. It was not until
Smith-Petersen’s 1931 report of the successful use of stainless steel nails for
the treatment of femoral neck fractures, that the application of metallic
intramedullary implants began to expand rapidly.8 In the United States, Rush
and Rush described the use of metallic Steinman pins placed in the medullary
canal to treat frac-tures of the proximal ulna and proximal femur.9 While these
techniques provided a foundation of principles for the treatment of fractures
with intramedullary fixation, there would be an explosion of principles and
methods in the decades to come.
Origins and Evolution of Küntscher Nailing
Gerhard Küntscher was born in Germany in 1900. His early interest in
intramedullary devices resulted from his work with the Smith-Petersen nail in
the treatment of femoral neck fractures. Küntscher believed the same basic
science principles would be applicable in the treatment of diaphyseal fractures.
During development of his “marrow nail,” he conducted cadaveric and animal
studies. His original intramedullary nail was a V-shaped stainless steel nail
that was inserted antegrade. Küntscher first reported use of the V-shaped nail
in 1940 and proposed the nail would act as an internal splint that created an
elastic union with the inner medullary cavity.10 It appears that early in the
development of his technique, he recommended inserting the nail into the bone
distant to the fracture site, thus, avoiding any disturbance of the zone of injury.
Intraoperative reductions were achieved with the use of multiple slings; while
head worn fluoroscopy was used for bony visualization. Küntscher believed
6

that proper insertion of his nail would allow for immediate functional
mobilization of the patient. Küntscher’s early work was not well received in
Germany, and early in World War II he was sent to the northern Finnish front.
There he collaborated with Finnish surgeons, which resulted in a report, in
1947, of 105 cases using the V-shaped nail.11 By the late 1940s, Küntscher had
begun to abandon use of the V-shaped nail design in favor of another
Küntscher design, the cloverleaf nail. While there was some interest in the use
of Küntscher’s technique in Europe during World War II, his method was
essentially unknown in the US. The use of the Küntscher nail was first
described in the US in a March 12, 1945, Time Magazine article, entitled
“Amazing Thighbone.”
This article discusses the skepticism displayed by American surgeons
on discovering the metallic rods implanted in US servicemen by German
doctors. It would be several more years until the first report of the Küntscher
nail would appear in the English medical literature.11 During the 1940s,
various other intramedullary designs were introduced. Westerborn reported his
experience with a V-shaped nail in the Scandinavian literature in 1944.12 In
1946, Soeur reported on his use of a U-shaped nail in the femur, tibia and
humerus.13
In the US, the Hansen-Street nail was introduced in 1947.14 This was a
solid diamond-shaped nail, designed to resist fracture rotation via its
compressive fit within the cancellous bone. These nails were originally
7
inserted using a closed method in order to avoid the high infection rate
reported earlier by Hey Groves. However, with the utilization of penicillin,
Street transitioned to open retrograde nailing to avoid side effects of the
radiographic techniques of the day.
1950s
During the 1950s, two important techniques were developed and
introduced. In 1942, Fischer had reported, in the German literature, the use of
intramedullary reamers to increase the contact area between the nail and host
bone, with the hope of improving stability of the fracture.15 However, it took
another decade with Küntscher’s introduction of flexible reamers for the
concept to take hold. Fischer also believed that reaming in combination with a
larger diameter nail would enhance the stability of fractures by increasing the
contact area. He felt that, although the intramedullary vascular supply was
obliterated through this technique, the periosteum and surrounding tissues
would promote adequate bone formation for healing. Another currently used
technique introduced in the 1950s was the application of interlocking screws
to enhance stability of the construct. Modny and Bambara introduced the
transfixion intramedullary nail in 1953.16 This nail was cruciate-shaped, with
multiple holes the length of the nail to allow for placement of screws at 90°
angles from each other. Modny and Lewert later reported excellent results in a
series of 261 femur fractures treated with this nail.17
8

1960s
Enthusiasm for compression plating of long bone fractures exploded
during the 1960s, and general advancement in the use of intramedullary nails
“went on hiatus.” Despite the emergence of compression plating, there were
several advancements that changed the future practice of intramedullary
nailing. Cephalomedullary nails were first introduced in the 1960s, highlighted
by the development of the Zickel nail in 1967.18 The Zickel nail contained a
hole in the proximal portion in order that a separate nail could be placed
through the lateral cortex of the proximal femur into the neck and head. A set
screw, which continues to be found on some current cephalomedullary
designs, could be inserted through the proximal portion of the shaft nail to
prevent backout of the head and neck nail.
During the 1940s and 1950s, many surgeons abandoned early
radiological techniques, such as head worn fluoroscopy, because of the
potential side effects to both surgeon and patient. This forced these surgeons
to adopt an open nailing technique. The development of radiological image
intensification, in the 1960s, allowed surgeons to readopt closed nailing
techniques with a much lower risk to patient and surgeon alike.
1970s and 1980s
The exuberance that accompanied the advent of compression plating
for tibias and femurs in the 1960s quickly diminished in the 1970s and, thus, a
renewed interest in refining closed nailing techniques appeared. This
9
reemergence of closed nailing has led to many of today’s current techniques.
As the use of reamed nailing gained more traction, undreamed nailing became
reserved for open fractures. Also during this time, a rapid gain in experience
occurred using reamed nails for treating tibial shaft fractures. The dominant
design during this time period was the slotted cloverleaf-shaped interlocked
nail, e.g., the AO and Grosse-Kempf nails.
As surgical techniques continued to expand during this time, there was
a surge in clinical data regarding the use of reamed interlocking nails of both
the femur and tibia. This was culminated by a three-part study of reamed
interlocked femoral nails by Brumback and colleagues.19-21 This work reported
a 98% (85/87) initial healing rate with statically locked, reamed
intramedullary nails in 87 femur fractures. Union was reported in the
remaining two fractures after dynamization.
1990s and the 21st Century
While there was certain progress as far as nail design and materials is
concerned during the 1990s, the major advancements came with the expansion
of indications for undreamed and reamed intramedullary nailing. Open tibial
shaft fractures were now being treated with intramedullary fixation with good
results. Likewise, open femur fractures that previously were managed with
unreamed nails, were now being treated with reamed nails. In addition, very
proximal and distal tibia and femur fractures, once thought to be unsuitable for
nailing, were benefiting from intramedullary fixation.
10
Design achievements of the 1990s included the introduction of new
titanium nails, cephalomedullary devices such as the Gamma nail, and
retrograde supracondylar intramedullary nails such as the GSH (Green-
Seligson-Henry) nail.22,23
In addition, slotted cloverleaf cross-sectional designs were being
replaced by nonslotted designs that provided greater torsional rigidity. In
1999, Brumback and associates reported a two-part study looking at
immediate weightbearing in patients with comminuted femoral shaft fractures
that were treated with intramedullary nailing.24 These investigators concluded
that immediate weightbearing is advisable in patients who had their femur
fractures fixed with larger diameter nails with high fatigue strength, as this
allows for more rapid mobilization for the trauma patient with multiple
injuries of the extremities.
Future Advancements
While today’s experience with intramedullary fixation for tibial and
femur fractures has been quite good, there will most certainly be continued
research to improve the technique. The most likely two areas of future
research will revolve around different biomaterials and biologically active
agents to promote bone healing. Two types of biomaterials that may hold
promise include biodegradable polymers and shape memory alloys.
Biologically active agents, such as bone morphogenic protein-2 and -7, have
been used with good success in the promotion of bone healing in both animal
11

models and humans. How to combine these bioactive agents with implants in a
cost effective manner is yet to be determined.
Conclusion
Intramedullary nailing has a long and interesting history that dates
back, at least, to the 16th century. Modern intramedullary techniques were
developed by Küntscher in Germany during the 1940s and were originally met
with much skepticism. Despite these early doubters, intramedullary nailing has
become the standard of care for the treatment of femoral shaft fractures and
tibial fractures that require operative stabilization.
12

REVIEW OF LITERATURE ON INTRAMEDULLARY NAILING
Gerhard B.G.Kuntscher25 (1958) opined that intramedullary nailing
represents the ideal treatment of fractures and requires no external fixation or
special postoperative care. The basic principle in this method is stable
osteosynthesis through flexible impingement of nail in the bone.
J.Zucman et al26 (1969) treated 36 two-level tibial fractures by
intramedullary nailing. The results showed that intramedullary nailing in two-
level tibial fractures allows walking with full weight bearing in an average of
3 to 4 months. It decreases the rate of non-union, malunion and it should
decrease the rate of infection, in closed fractures compared with other types of
internal fixation.
Compound tibial fractures treated by nailing are still complicated by
infection, but there are no other studies to conclude that other methods could
lower significantly the infection.
Merle d’Aubigne et al27 (1974) studied the outcome of tibial shaft
fractures treated with plates and screws and intramedullary nailing. Between
1960 and 1972, 849 tibial fractures were treated by intramedullary nailing and
58 by other methods. 23 patients were treated with plates and screws. They
showed more rate of non-union (69.6%) in the fractures by the plates and
screws. The infection rate was 28% including compound and simple fractures.
13

In case of intramedullary nailing non-union was 3.44% and infection was
7.2%.
Johner and Wruh28 (1983) classified tibial fractures based on etiology,
morphology and clinical features, documented in a series, 291 fractures treated
by AO/ASIF rigid internal fixation. The fractures were placed in 9 main
fracture groups, each with three sub-groups according to location in the
proximal, middle or distal segment of the shaft. A includes all simple
fractures, Group B includes fractures with butterfly fragments and Group C all
communited.
They also developed criteria for evaluation of final results as excellent,
good, fair, or poor by using non-union, pain, deformity, movements of joints,
shortening, neurovascular disturbances and gait as parameters for evaluation.
Lawrence B.Bone et al29 (1986) treated 112 cases of tibial fractures by
reaming and intramedullary nailing. They opined that it is also indicated in
the treatment of non-union and malunion in the absence of sepsis. In
segmental fractures, excellent results were noted with average time in union at
19 weeks.
Average time to full weight bearing was 4 weeks, 50% of primary
nailing and 40% of secondary nailing healed within 3 months. They
concluded that interlocking nailing is an excellent management for unstable
14

fractures and for secondary procedures in fractures not associated with
infection.
Kessler SB Hallefeldt et al30 (1986) published articles, stating that
fractures of tibia can be treated successfully with interlocking nailing.
Arne Ekeland et al31 (1988) treated 45 tibial shaft fractures, in 43
patients with Grosse-Kempf interlocking intramedullary nail between 1979 to
1982. Median age of the nailed patient was 35 years, it included 15 females
and 28 males. 23 fractures (51%) were caused by high energy trauma, 5
fractures (11%) were open. Median time of full weight bearing was 30 days.
Median time of bone union was 16 weeks with 29 excellent, 13 good and 2
fair results. 1 patient had non-union. They said that interlocking
intramedullary nailing is the ideal treatment for communited, segmental and
unstable fractures, and in patients with multiple polytrauma.
Scott L.Sledge et al32 (1989) in a study of 51 patients of non-union
tibia, treated with intramedullary reaming and nailing between 1980 to 1986
showed that 49 patients had union of the fracture site at an average time of 7
months postoperatively.
Thus, they concluded that intramedullary nailing with reaming, can
produce union as effectively as other alternatives, while enabling the patient to
function more normally without external immobilization or walking aids.
15

Court Brown et al33 (1990) treated 125 closed and type-I open tibial
fractures. The mean time of union was 16.7 weeks, and no fractures required
bone grafting. There was 1.6% infection rate, 40.8% of patients had knee pain
and 26.4% needed to have the nail removed, other complications were minor.
They used Grosse Kempf interlocking nail in 100 men and 23 women with a
mean age of 32.4 years. There were 114 closed and 11 type-I open fractures,
14 fractures involved only tibia and 111 involved both bones of leg. 6
fractures were in the proximal third of tibia, 46 in the middle third and 64 in
the distal third. 9 fractures were sports injuries and 35 occurred after fall,
while 6 patients were assaulted. Mean time in union was 16.7 weeks, two
patients (1.6%) had non-union, two deep infections (1.6%) developed, 5 mm
shortening in three patients, and unacceptable deformity or shorteining in
2.4% of patients. They suggested that closed intramedullary nailing with an
interlocking nail is an excellent method of treating closed and type-I open
tibial fractures.
Hooper et al34 (1991) reviewed fractures of tibia treated with
conservative treatment and closed intramedullary nailing. The results showed
that the intramedullary nailing gives more rapid union with less malunion and
shortening. Nailed patients had less time off work, with a more predictable
and rapid return to full function. Out of 62 tibial fractures, 33 fractures were
treated by conservative method and 29 fractures by closed nailing. Time of
union in nailed fractures was 15.7 weeks and time off work was 13.52 weeks.
Mean hospital stay was 11.6 days.
16

Habernek H et al35 (1992) showed 109 patients treated by interlocking
nailing for tibial fractures between 1985-1990 by K.H.Schwanz and the LKH
Bad Ischl, Austria. 92 cases were followed up. An increased number of
compound fractures were evaluated. Except for 14 malalignment and 2 leg
infections after new injuries, no other serious complications were detected.
Interlocking nailing can be safely recommended even for open fractures up to
second degree at any level from the second fifth to the fourth fifth of the tibia.
Wu CC, Shih CH36 (1993) have reported in the Canadian Journal of
Surgery on a retrospective study done in 11 tibial shaft fractures with static
interlocking nailing followed by dynamization, wich was carried on average of
7.8 months. The success rate was 54%. The follow up was at least 2 years.
The interval from nailing to dynamization did not correlate with the success
rate, the longest interval associated with successful healing was 20 months.
The authors found that static interlocking without dynamization can still
produce a high union rate and if there is sparse callus formation during the
healing process, due to low osteogenesis, dynamization will result in fracture
union in half of the cases. To improve the union rate cancellous bone grafting
may be necessary.
Wu CC, Shih CH37 (1993) have published an article in the journal of
Orthopaedic Trauma, on segmental tibial shaft fractures treated by
interlocking nailing on 38 patients and followed up for a period of 1 year.
There was 97% union rate and 4.5 months was the union period. The range of
17

motion in the knee and ankle was satisfactory. Significant complications
included 1 aseptic non-union, 3% of which healed after the static locked nail
was dynamized. They reported that whenever possible closed interlocking
nailing should be used to treat closed or mild open segmental tibial shaft
fractures.
Watson JT38 (1994) concluded from a review of literature that unstable
closed and type-I open fractures are preferably treated with intramedullary
nailing with or without reaming.
In grade-II and IIIA fractures, rate of union and rate of infection is
similar in reamed and unreamed intramedullary nails, but secondary surgery
may be needed in reamed nailing.
Watson JT38 (1994) concluded that the presence of a fibular fracture in
association with tibial fracture often indicates an unstable fracture as well as
high energy mechanism of injury. He says that good results have also been
reported with use of techniques with reaming. The reaming of the medullary
cavity allows the insertion of larger nail, thereby increasing the stability of
fixation, because of biomechanical limitations, there may be high rate of
failure of small diameter locking nails. If union is not achieved earlier, fatigue
failure of the nail or interlocking screws with subsequent non-union may
occur.
18

Anglen JO et al39 (1995) have reported in the journal of trauma on
comparison of reamed and unreamed nailing of the tibia. A retrospective
review was done on all tibial fractures treated by interlocking nailing at the
author’s institution, over the past five years, in order to compare reamed and
unreamed nailing. The unreamed nailing had lower average operative time
and lower average estimated blood loss. There was a statistically significant
difference in healing times, with unreamed nailing taking an average of 242
days to heal while reamed nailing took 158. 6 non-unions occurred, 1 in
reamed nailing and 5 in unreamed nailing. Malunions occurred in 4 reamed
nailing 6 unreamed nailing. Patellofemoral complication were more common
in unreamed nailings.
In 1995, Paul Gregory and Roy Sanders40 proposed that interlocked
intramedullary nailing inserted in an unreamed manner has become the
treatment of choice for the closed, unstable tibial shaft fractures in
polytraumatized patients in the authors institution. A high union rate, coupled
with a lack of compartment syndromes or peroneal palsy, makes this
procedure an attractive and alternative to reamed nailing.
In 1995, Gregory41 proposed that infection after unreamed nailing had
fewer complications and a higher success rate for infection control than
reamed nailing.
19

Court Brown et al42 (1996) in their article “Reamed or unreamed
nailing for closed tibial fractures said that reamed nailing showed better results
of union and unreamed nailing showed prolonged union rates.
The average union time is less and the incidence of non-union and
malunion is low in reamed nailing.
Fang Yao Chin et al43 (1996) treated unstable closed tibial shaft
fractures. Randomly 60 tibiae were fixed with interlocking nails and 56 tibiae
were fixed with ender nails. The follow up period was 24 months. They
concluded that in treating more communited tibial shaft fractures, the
interlocking nail is recommended because of its higher success rate.
Blachut PA et al44 (1997) in 152 closed fractures of tibia managed
between 1989 to 1994, with or without reaming, concluded that there are no
major advantages to nailing without reaming as compared to nailing with
reaming for the treatment of the closed fractures of the shaft of the tibia.
There was a higher prevalence of delayed union and breakage of
screws after nailing without reaming. The study included 70 fractures treated
with nailing with remaining and 56 that were treated with nailing without
reaming. Both united without the need for an additional surgery.
Schemitsch et al45 (1998) noted that there was no difference in bone
formation between reamed and unreamed nailing in sheep bone and noted that,
initially blood flow (overall tibial blood flow) decreased as the amount of
20

reaming increased, but 11 weeks after surgery the tibial perfusion had
increased to the same levels in both reamed and unreamed groups. They noted
that no long-term benefit was seen in limited reaming. They found no
evidence that the degree of reaming significantly affected.
Daudel A, Gascia et al46 (1998) concluded that non-reamed flexible
locking nailing provides effective control of axial and rotational stability.
Krettek C et al47 (1999) in a study of 20 patients showed that Poller
screws gave good supplement to stability after fixation with statically locked
intramedullary nails of small diameter in nailing of metaphyseal fractures with
a short proximal or distal fragment where an increase in malalignment can
occur in the coronal plane. Healing was evident in radiographs at 5.4±2.1
months. Mean varus-valgus alignment of –1.0 degree and mean
antecurvatum-recurvatum alignment of 1.6 degrees was noted.
Mohit Bhandari et al48 (1999) conducted a retrospective chart review
of 200 tibial fractures. They showed that plate fixation was associated with a
greater incidence of complications when compared with intramedullary nail
fixation. Complication rates were significantly greater in the delayed surgical
group. Surgical delay results in longer post-operative hospital stays, greater
complication rates, and increased total cost to the health care system.
Hernigou P et al49 (2000) in a report on proximal entry for
intramedullary nailing of the tibia, concluded that it is important to enter the
21
medullary canal at the right point, so that the nail is introduced in line with the
axis of the tibia in both the coronal and sagittal planes. If the entry point is
low, posterior tibia is endangered, if high, then, unrecognized articular
penetration can occur injuring the menisci and ligamentum transversum.
The unrecognized articular penetration was seen commonly and this
caused anterior knee pain. The safe zone is anterior to the ligamentum
transversum and anterior to the anterior horn of each meniscus. In some bones
the safe zone is smaller than the size of the standard reamers and the proximal
part of some nails.
Jarmo AK, Toivanen et al50 (2002) in a prospective randomized study
of intramedullary nailing of fractures of the tibial shaft, compared the results
of anterior knee pain in two different nail insertion techniques. The incidence
of chronic anterior knee pain was seen in up to 56% of patients. They noted
that irrespective of incision used, whether transtendinous, or paratendinous
incision (by a medial longitudinal incision without violating the patellar or its
sheath), the prevalence of anterior knee pain is the same.
They concluded by saying that intramedullary nailing is the treatment
of choice for displaced tibial shaft fractures and any change in approach in nail
insertion does not change the incidence of anterior knee pain.
Andrew Schmidt et al51 (2003) in the instructional course on treatment
of closed tibial fractures, summarized that intramedullary nailing is more
22

convenient, and it may provide superior results, but prospective randomized
studies need to be done to confirm this. Operative treatment is recommended
for open or closed unstable fractures and for fractures that cannot be held in
adequate alignment. Intramedullary nail fixation is the treatment of choice for
majority of tibial fractures that require stabilization.
Joshi et al52 (2004) proposed that the current trend of management of
Gustillo Tpe-I, II and IIIA open fractures of tibia present to emergency
department within 6-8 hours is to perform unreamed intramedullary nailing.
Unreamed nailing in experimental studies has been found to cause less
reduction in cortical circulation as compared to reaming of medullary canal.
Reaming of open fractures had been found to spread the contamination from
open wound along the medullary cavity. Reaming has also been reported to
slow the revascularization and delay osseous union.
Vineet Jain et al53 (2005) concluded that primary unreamed
intramedullary nailing offers advantage of rigid fixation, low incidence of
infection, non-union, good functional results and early return to work. An
adequate soft tissue management is mandatory in treatment of these fractures.
Lascombes et al54 (2006) in their article “use and abuse of flexible
intramedullary nailing in children and adolescents” stated that elastic stable
intramedullary nailing (ESIN) is awell accepted method of osteosynthesis of
diaphyseal fractures in children and adolescents for many reasons including
23

the following: No need for postoperative cast, primary bone union with
avoidance of growth plate injury and minimum invasive surgery.
Thonse et al55 (2007) in their article “antibiotic cement coated
interlocking nail for the treatment of infected non-unions and segmental bone
defects” stated that control of infection and stabilizing to promote union has
traditionally been provided by two separate procedures, methods that have
proved to be efficacious in the past. However, both these goals can be
achieved in half the patients with the use of antibiotic cement coated
intramedullary nail.
Kyung-Cheon Kim et al56 (2008) in their article “Percutaneous
reduction during intramedullary nailing in comminuted tibial shaft fractures”
stated that communited tibial shaft fractures are often associated with severe
soft tissue injury and periosteal stripping and result in major impairment of
blood supply to the communited bony fragment. Consequently the use of
unreamed intramedullary nailing in comminuted tibial shafts has gained favor
because they better preserve the endosteal blood supply and minimally disturb
the soft tissue envelop. Percutaneous reduction with conventional reduction
forceps and unreamed intramedullary nailing is thought to facilitate fracture
reduction and decrease complications, such as non-union, malalignment,
instability and fixation failure.
Vaisto O et al57 (2008) in their article “Anterior knee pain after
intramedullary nailing of fractures of tibial shaft: an eight year follow-up of a
24

prospective, randomized study comparing the different nail-insertion
techniques” stated that anterior knee pain is the most common complication
after intramedullary nailing of the tibia. Dissection of patellar tendon and its
sheath during transtendinous nailing is thought to be a contributing cause of
anterior knee pain compared with a transpatellar tendon approach, a
paratendinous approach for nail insertion does not reduce the prevalence of
chronic anterior knee pain or functional outcome after intramedullary nailing
of tibial shaft fracture. In long term anterior knee pain seems to disappear
from many patients.
25

SURGICAL ANATOMY
Surgical Anatomy of Leg
The leg is divided into 3-compartments:
1. Anterior compartment
2. Lateral compartment
3. Posterior compartment – This is divided into
a) Superficial posterior compartment
b) Deep posterior compartment, by the deep transverse fascia
Figure-1: Muscles of Leg – Anterior View
26

Anterior Compartment:
• The anterior compartment of the leg contains tibialis anterior, extensor
digitorum longus, extensor hallucis longus and peroneus tertius
muscles.
• This compartment is primarily responsible for dorsiflexion of foot and
ankle, along with inversion of foot by tibialis anterior, extension of
hallux by extensor hallucis longus and extension of toes by extensor
digitorum longus.
• Neurological damage or loss of functional integrity of motor tendon
unit itself, may lead to loss of dorsiflexion.
• All anterior crural muscles are supplied by deep peroneal nerve.
Tibialis anterior by L4 and L5 and other by L5 and S1.
• Anterior tibial artery and deep peroneal nerve run deep, andthey are
present anterior to the interosseous membrane.
• They pass in interval between the tibialis anterior and extensor hallucis
longus.
• The muscles in the anterior compartment are enclosed in a relatively
unyielding fascial compartment, which makes the anterior
compartment more at risk for compartment syndrome.
• Near the ankle, tendons of Tibialis anterior, extensor hallucis longus
and extensor digitorum longus are close to the tibia. They may be
injured in fractures near the ankle. They may also be incorporated by
the callus formed during fracture healing.
27

Lateral Compartment
• Lateral crural muscles are the peroneus brevis and longus.
• They evert the foot. The peroneus longus everts and plantar flexes the
foot.
• They are supplied by the superficial peroneal nerve L5, S1 and S2.
• Superficial peroneal nerve runs in septum between peronei and
extensor digitorum longus.
• This nerve is injured with fractures of fibular neck and in traction
injuries of lower extremity. They are also injured in fractures at
junction of middle and distal thirds of the leg, where superficial
sensory branches pass between peroneus brevis and extensor digitorum
longus muscles. Improper positioning of the knee, in flexion without
padding on the fracture table can cause compression of common
peroneal nerve proximally at the fibula.
• Padding and avoiding pressure over proximal fibula will help prevent
the development of the peroneal nerve palsy.
• Compartment syndromes are much less common in lateral
compartment than in the anterior compartment.
28
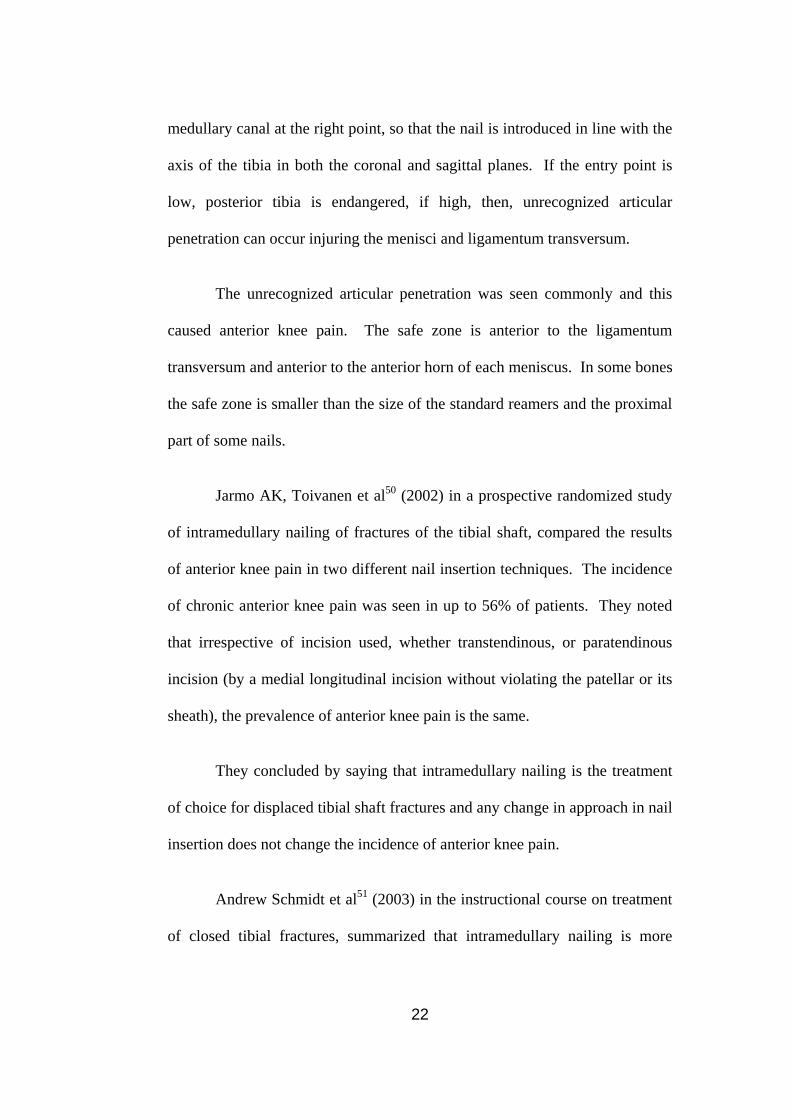
Figure-2: Muscles of Leg – Posterior View Figure-2: Muscles of Leg – Posterior View
29
29

Superficial Posterior Compartment
• Superficial posterior compartment contains gastrocnemius, soleus and
plantaris muscles.
• The gastrocnemius and plantaris act on knee and ankle, soleus acts
only on the ankle.
• They are supplied by the tibial nerve S1 and S2.
• Sural nerve, short and long saphenous veins are also within this
compartment, but there are no arterial structures.
• Gastrocnemius, crossing both knee and ankle is a primary flexor of the
knee and ankle joints.
• Soleus tendon joins gastrocnemius tendon in distal third of the leg to
form triceps surae or Achilles tendon.
• Gastrocnemius propels in walking, running and leaping, while soleus is
said to study the leg on the foot in standing.
• Plantaris has no anatomical significance, but may serve as a source of
tendon graft.
Deep Posterior Compartment
• Contains tibialis posterior, popliteus, flexor digitorum longus and
flexor hallucis longus.
• The flexor hallucis longus and flexor digitorum longus are supplied by
tibial nerve S2 and S3. The popliteus by tibital nerve L4 and L5 and
S1. Tibialis posterior by tibial nerve L4 and L5.
30

• These muscles are involved in plantar flexion of the foot and toes and
inversion of foot through tibialis posterior muscle function.
• Popliteus acts as a leg flexor, internal rotator of tibia and initiation of
knee flexion.
• The peroneal artery and posterior tibial arteries are present in this
compartment.
• Posterior tibial artery, because of its protected nature, frequently, is a
major source of arterial supply after significant open fracture and is a
potential source for anastomosis with free flaps for soft tissue
reconstruction of the leg.
Figure-3: Bones of the Leg – Tibia and Fibula
31
Surgical Anatomy of Tibia
Tibia is the medial and larger bone of the leg. It is stronger than the
fibula and its shaft is prismoid in section with the ends expanded. It is
homologous with the radius of upper limb. It lies vertically in the body. It has
a proximal end, shaft and distal end. It lies subcutaneously in the anterior part.
Proximal End
It is markedly expanded transversely. It is a bearing surface for body
weight transmitted through the femur. It has:
1. Medial and lateral condyle.
2. Intercondylar area – this is present between the condylar articular
surfaces.
3. Tuberosity of tibia – This is present at the proximal end of the
anterior border.
Shaft
It is triangular in section, is thinnest at the junction of middle and distal
third, and slightly expands at both ends. It is prism in shape and has 3-borders
and 3-surfaces. The borders are:
1. Anterior border – it forms shin of the tibia.
2. Medial border.
3. Interosseous border, it provides attachment to interosseous
membrane. The surfaces are medial, lateral and posterior surfaces.
32

Distal End
It is slightly expanded and has five surfaces, which are the anterior,
medial, posterior, lateral and distal surfaces. It projects infero-medially as the
medial malleolus.
Tibia is commonly fractured at the junction of upper 2/3rd and lower
1/3rd of its shaft, where it is most slender. The delayed or non-unions, which
may follow is said to be due to poor blood supply of this part of bone or
tearing of the nutrient artery.
Ossification
It is by three centers, in the shaft and both epiphysis. One primary
center begins in mid shaft by 7th week of intrauterine life. Two secondary
centers are:
1. Proximal epiphyseal center, which is present before birth and fuses
at 16 to 18 years.
2. Distal epiphyseal center appears during 1st year after birth, forms
medial malleolus by 7th year and fuses with shaft by 15 to 17 years.
Vascular supply to the Tibia
• Blood supply to the tibial shaft is derived from nutrient artery and
periosteal vessels.
• Nutrient artery enters middle 1/3rd and may be damaged in a segmental
fracture.
33

• This makes bone dependent on soft tissue envelope for blood spply,
and stripping of soft tissues may render the bone avascular.
• Nutrient artery arises from the post tibial artery and enters
posterolateral cortex of the tibia at the origin of the soleus muscle.
• Artery may traverse a distance of 5.5 cm before entering its oblique
nutrient canal.
• Artery divided into three ascending branches and a single descending
branch, which gives off smaller branches to the endosteal surface.
Nutrient Artery
• Nutrient artery enters into the diaphysis of long bones through an
oblique canal.
• Direction of canal is determined by relative amount of growth that has
occurred at proximal and distal ends of the bone.
• Nutrient canals slope away from the knee in femur, tibia and fibula and
towards elbow in radius, ulna and humerus.
• Nutrient artery divides after reaching the medullary cavity, sending
arterial branches in proximal and distal directions and join with
metaphyseal arteries.
• Some of these branches enter the cortex to supply Haversian canals of
inner two-third of the cortex.
34

Figure-4: Anterior tibial and dorsalis pedis arteries
35

• Other branches of the nutrient artery continue in more or less parallel
alignment to metaphysis.
• In the child, these vessels end on metaphyseal side of epiphyseal plate,
where they participate in enchondral ossification.
Disruption of Nutrient Artery
• In growing bone, can result in necrosis of large portion of the marrow
and of inner two-thirds of the cortex.
• This cortical death does not occur in adult bone, because combined
epiphyseal – metaphyseal collateral circulation has developed enough
to maintain these areas.
• Loss of circulation in terminal vessels of nutrient artery of growing
bone will interface with enchondral ossification.
Epiphyseo-metaphyseal Blood Supply
Formed by medial genicular artery, inferior genicular artery and tibial
recurrent artery.
• Metaphyseal portion of long bone contains numerous small channels.
• Through these channels pass vessels that enter marrow cavity to
anastomose with vessels derived from nutrient artery.
Majority of these metaphyseal channels, however contain veins that
permit egress of blood from the marrow cavity.
36
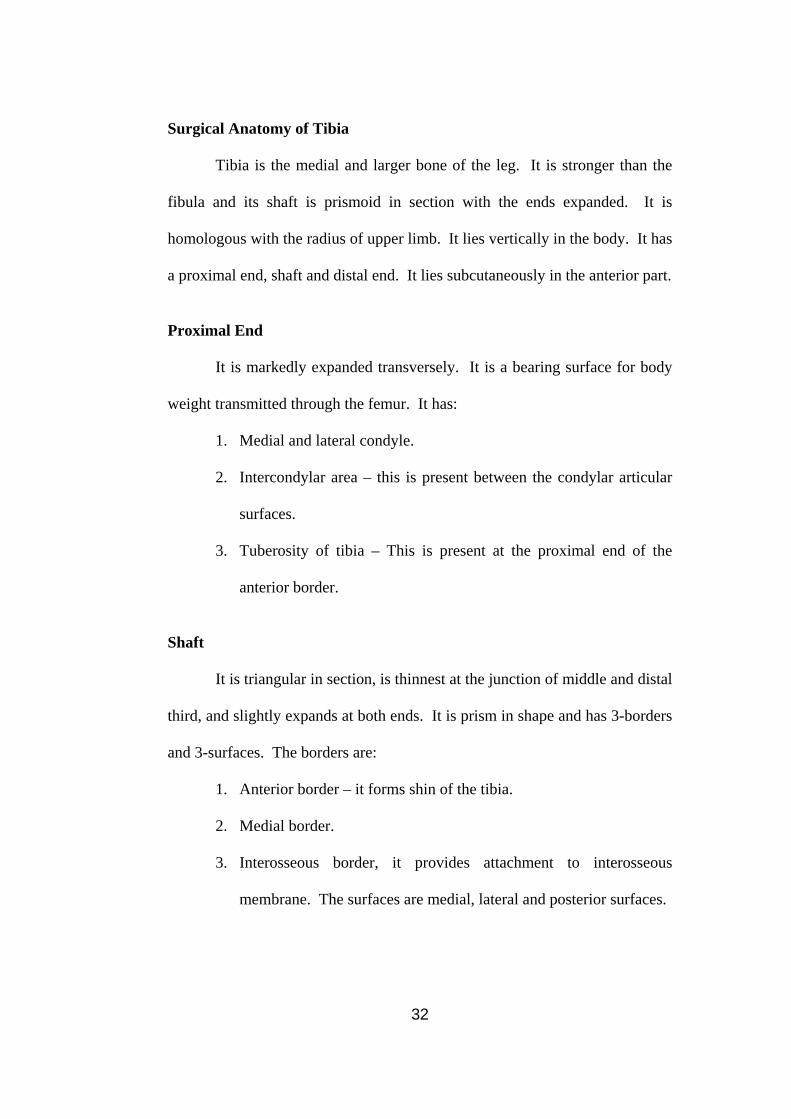
Anterior Tibial Artery
• May be vulnerable to injury after its division from popliteal artery,
where it passes through hiatus in upper interosseous membrane.
• Periosteum has abundant blood supply from anterior tibial artery,
which branches out as it courses down the interosseous membrane.
Figure-5: Posterior Tibial and Peroneal Arteries
37

Posterior Tibial Artery
• Posterior tibial artery enters the posterior compartment of the leg along
with, lying posterior to tibialis posterior and enters plantar aspects of
the foot after passing behind medial malleolus.
• Largest branch is peroneal artery arising high in leg and coursing
downward in the posterior compartment, lying just medial to fibula.
• Gives off branches to adjacent muscles, sends branches through
interosseous membrane to anterior compartment and gives nutrient
artery to the fibula.
• Lateral compartment of the leg has no artery proper to it.
• Tibial nutrient is a large branch of the posterior tibial artery.
• Under flexor retinaculum, the posterior tibial artery divided into the
lateral and medial plantar arteries.
Medial Plantar Artery
• Travels with medial plantar nerve, supplies medial portion of the
plantar aspect of the foot.
• Three medial metatarsal arteries usually receive branches from the
medial plantar artery.
Lateral Plantar Artery
• Travels with lateral plantar nerve and passes across the foot to form
plantar arch, which joins with deep plantar artery from the dorsalis
pedis artery.
38

Classification of Tibial Shaft Fractures
Classification
Numerous classification system, have been proposed for tibial
fractures from the simple stable versus unstable to more detailed alphanumeric
systems as proposed by AO/ ASIF/ OTA classification.
Any classification of injury is useful only if it alerts the physician to
potential dangers or helps to determine appropriate treatment. The most
important morphological variable are:
• Anatomical location
• Pattern or patterns of fracture lines
• Associated injuries of fibula
• Position and number of fragments.
• Extent of soft tissue damages.
Ellis classified tibial fractures into three groups of severity:
• Minor: Non-displaced with minor communition or small open wound.
• Moderate: Total displacement or angulation with small degree of
communition or minor open wound.
• Severe: Complete displacement of fracture fragments with major
communition or major soft tissue damage.
Weissmann and Associates
Also classified tibial fractures. This classification is based on the
initial displacement of fracture. But this is often difficult to ascertain because
39

the fractures may have been reduced from their initial displacement before X-
rays. It depends on:
• Degree of initial displacement.
• Communition
• Soft tissue wounds.
He arbitrarily assigned one of 3-grades from each factor. Nil or slight,
moderate and severe.
OTA (Orthopaedic Trauma Association)/ AO Classification
This was initially described by the AO Group. This is a morphologic
classification based on the initial anteroposterior and lateral radiographs. It
consists of three types subdivided into three groups, each of which are further
sub-divided into three sub-groups.
Type-A fractures or Unifocal Fractures
Their division into sub-groups is based on orientation of the tibial
fracture and the presence or absence of a fibular fractures.
A1 – spiral fractures
A2 – oblique fractures
A3 – transverse fractures.
If there is no fibular fracture, suffix, 1 is used, with 2 being used for
fibular fracture distant from tibial fracture and 3 for fractures where tibial and
fibular fractures are at the same level.
40

Type-B fractures are wedged fractures
BB1 – spiral wedge fractures
B2 – bending wedge fractures
B3 – fragmented wedge fractures
Type-C are classified on severity of tibial fracture, and not on position of
fibular fracture
C1 – complex spiral fractures
C1.1 – two intermediate fragments
C1.2 – three intermediate fragments
C1.3 – more than three intermediate fragments
C2 – segmental fractures
C2.1 – one segmental fragment
C2.2 – segmental fragment and additional wedge fragment
C2.3 Two segmental fragments.
C3 –All communited fractures
C3.1 – two or three intermediate fragments
C3.2 – limited communition (<4 cm)
C3.3 – Extensive communition (>4 cm).
41
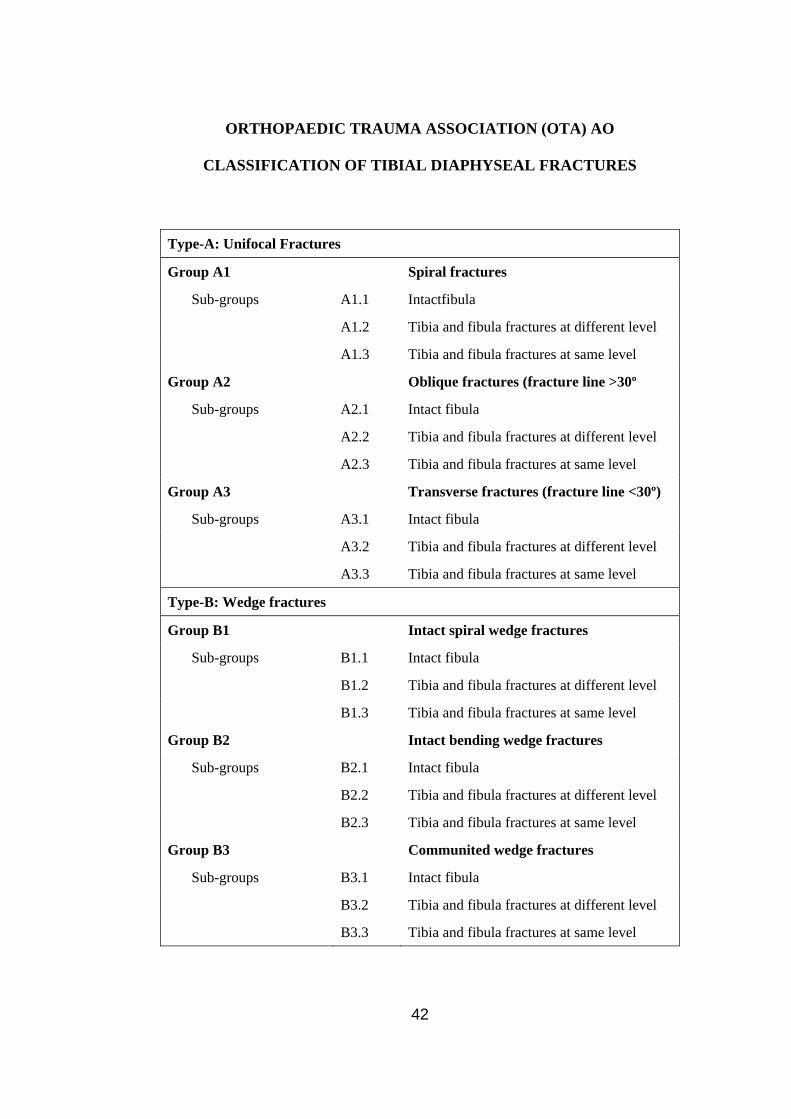
ORTHOPAEDIC TRAUMA ASSOCIATION (OTA) AO
CLASSIFICATION OF TIBIAL DIAPHYSEAL FRACTURES
Type-A: Unifocal Fractures
Group A1 Spiral fractures
Sub-groups A1.1 Intactfibula
A1.2 Tibia and fibula fractures at different level
A1.3 Tibia and fibula fractures at same level
Group A2 Oblique fractures (fracture line >30º
Sub-groups A2.1 Intact fibula
A2.2 Tibia and fibula fractures at different level
A2.3 Tibia and fibula fractures at same level
Group A3 Transverse fractures (fracture line <30º)
Sub-groups A3.1 Intact fibula
A3.2 Tibia and fibula fractures at different level
A3.3 Tibia and fibula fractures at same level
Type-B: Wedge fractures
Group B1 Intact spiral wedge fractures
Sub-groups B1.1 Intact fibula
B1.2 Tibia and fibula fractures at different level
B1.3 Tibia and fibula fractures at same level
Group B2 Intact bending wedge fractures
Sub-groups B2.1 Intact fibula
B2.2 Tibia and fibula fractures at different level
B2.3 Tibia and fibula fractures at same level
Group B3 Communited wedge fractures
Sub-groups B3.1 Intact fibula
B3.2 Tibia and fibula fractures at different level
B3.3 Tibia and fibula fractures at same level
42

Type-C: Complex fractures (multifragmentary, segmental or comminuted fractures)
Group C1 Spiral wedge fractures
Sub-groups C1.1 Two intermediate fragments
C1.2 Three intermediate fragments
C1.3 More than three intermediate fragments
Group C2 Segmental fractures
Sub-groups C2.1 One segmental fragment
C2.2 Segmental fragment and additional wedgement
C2.3 Two segmental fragments
Group C3 Communited fractures
Sub-groups C3.1 Two or three intermediate fragments
C3.2 Limited comminution (<4 cm)
C3.3 Extensive comminution (>4 cm)
43

Fracture Mechanics
Bone is an anisotropic material. It exhibits different stress-strain
relationships depending on the site and direction in which stress is applied.
Cortical bone fracture in vitro, when strain exceeds 2% of the original length.
Numerous classification systems have been proposed for tibial
fractures. Unfortunately none of them have been validated for reproducibility
or sensitivity.
The following classification was followed in the study:
Closed fractures:
1. Transverse
2. Oblique – short/ long
3. Spiral
4. Segmental.
The comminution at the fracture site was graded according to Winquist
et al classification.
Grade I Number of comminution <25% of the circumference
II Comminution <50% of the circumference
III >50% of the circumference
IV Total comminution.
44
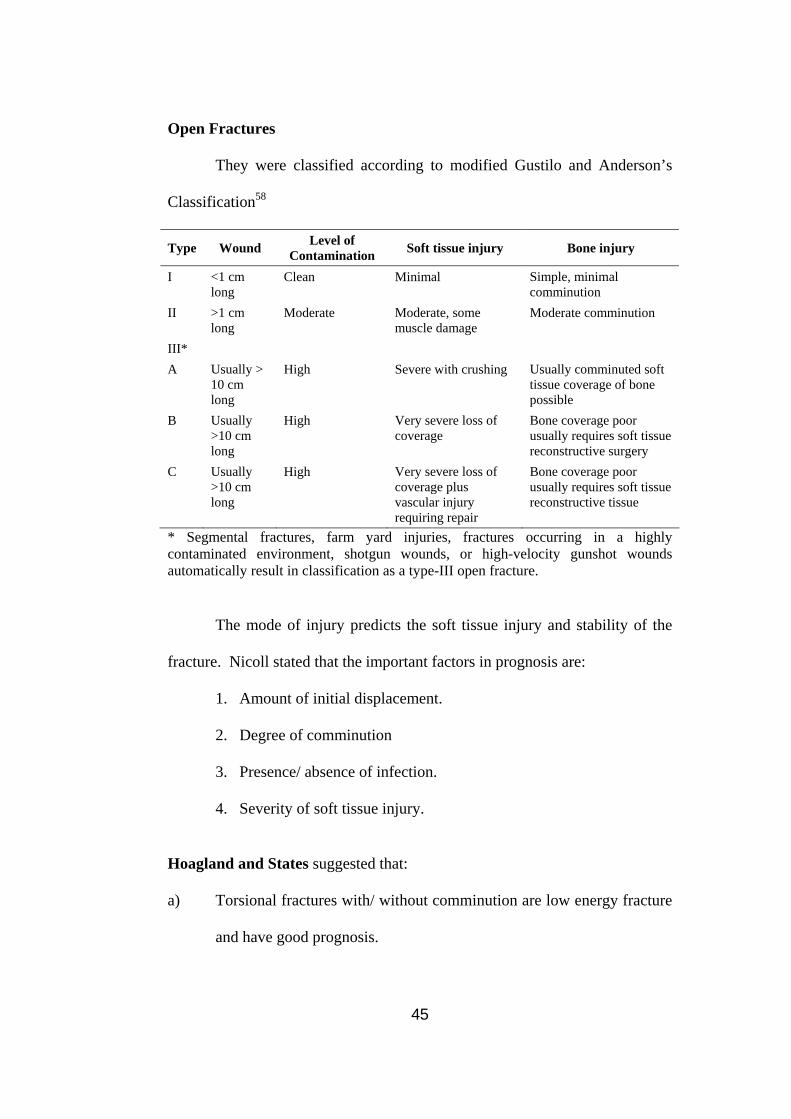
Open Fractures
They were classified according to modified Gustilo and Anderson’s
Classification58
Type Wound Level of Contamination Soft tissue injury Bone injury
I <1 cm long
Clean Minimal Simple, minimal comminution
II >1 cm long
Moderate Moderate, some muscle damage
Moderate comminution
III* A Usually >
10 cm long
High Severe with crushing Usually comminuted soft tissue coverage of bone possible
B Usually >10 cm long
High Very severe loss of coverage
Bone coverage poor usually requires soft tissue reconstructive surgery
C Usually >10 cm long
High Very severe loss of coverage plus vascular injury requiring repair
Bone coverage poor usually requires soft tissue reconstructive tissue
* Segmental fractures, farm yard injuries, fractures occurring in a highly contaminated environment, shotgun wounds, or high-velocity gunshot wounds automatically result in classification as a type-III open fracture. The mode of injury predicts the soft tissue injury and stability of the
fracture. Nicoll stated that the important factors in prognosis are:
1. Amount of initial displacement.
2. Degree of comminution
3. Presence/ absence of infection.
4. Severity of soft tissue injury.
Hoagland and States suggested that:
a) Torsional fractures with/ without comminution are low energy fracture
and have good prognosis.
45

b) Comminuted, transverse and short oblique fractures are high energy
fractures and have bad prognosis.
Long bone fracture biomechanics
Fracture pattern Mechanism of injury
Location of soft tissue hinge
Energy
Transverse Bending Concavity Moderate
Short oblique Compression + bending
Concavity or butterfly side
Moderate
Long oblique Compression + bending + torsion
Concavity (often destroyed)
Moderate to high
Spiral Torsion Vertical segment Low
Comminuted Variable Destroyed High
In analyzing fracture patterns, the mode of loading offers insight into
the mechanism of injury, the energy involved in disruption of the bone and the
prognosis.
46

Biomechanics of Intramedullary Locked Nail
All intramedullary nails, regardless of their types, act as flexible
internal splints, providing stability for the fracture fragments from within,
transferring load across the fracture site and maintaining anatomic alignment
to induce bony union.
This concept of intramedullary fixation was first introduced by Hey
Groves in 1918 and later popularized by Kuntscher in 1940.
The mechanical behavior of intramedullary nails depends on both
material and geometry of the design.
Material
If a structure is placed in a test frame and loaded to failure, the
resulting load-deflection curve would describe the mechanical behavior of that
device59. The shape of the curve can be divided into an elastic region initial
linear portion of the curve and a plastic region the non-linear portion. The
slope of the elastic portion is the stiffness of the structure, the higher the
number, more rigid the structure. Loaded within the elastic range, a structure
will return to its original shape following load removal. This is the working
area of the medullary implant. If the implant is loaded beyond the
proportional limit, a plastic deformation takes place and the shape of the
object changes. This creates a potential for complications from malunion to
non-union in fracture healing. Hence, the implant should not be loaded
beyond the proportional limits.
47
The bending rigidity59 depends on the moment of inertia of the design
which is proportional to the fourth power of the radius and the quantity of the
material, that is to say that the bending stiffness increases as the diameter and
thickness of the nail increases. A 25% increase in diameter of the nail will
double its bending strength.
The rotation stiffness depends on the configuration of the cross section
of the nail. Abolishing the open slot in the cross section increases the
rotational stiffness approximately 50 times, when compared to the same nail
with an open slot.
Clinically, bending strength and stiffness can be increased by using
unslotted thick nail with large diameter.
Stress-strain Curve59
Material properties are defined geometrically in the stress-strain curve.
Stress is defined as load per unit area and strain as the change in length
divided by the original length. The slope of the curve is termed the modulus
of elasticity (E) or Young’s modulus. It defines the elastic behavior of that
material. By multiplying the modulus of elasticity and the moment of inertia,
the structural stiffness of a cross section can be computed.
The yield strength is one at which the implant undergoes plastic
deformation. Fatigue strength is the repeated cyclical stress at which the
implant fails. For metals, the fatigue limit is approximately one-half the yield
48

stress and hence a load bearing or a load sharing implant should be designed
with the fatigue limit as the failure criteria.
Structural characteristics and mechanical factors important in the
design and evaluation of IM nails are strength, stiffness and rigidity of the
device. The working length of a nail is defined as that length which spans the
fracture site between adjacent areas of contact in the proximal and distal
fragments. This dimension also affects the stiffness of a nail. The working
length should be as short as possible to increase the stiffness in both bending
and torsion. However, the total nail contact should be distributed over a
longer section of the bone, proximally and distally to increase the gripping
strength of the nail and thus provide rotation stability. Interlocking IM nails
designed for static maintenance of length, also provide the greatest degree of
rotational stability, by rigidly locking the nail to bone through the use of
screws. Interlocking nails have a longer working length, hence, can be used in
proximal and distal tibial fractures also.
Interlocking can be of the following types:
1. Dynamic locking – placing cross-screws at one end only.
2. Static locking – cross screws are placed at both the ends.
Dynamic fixation controls bending and rotational deformities, but
allows nearly full axial load transfer by bone e.g., instable fractures.
49

Static locking controls rotation, bending and axial loading, and makes
the implant bear the load with potential for fatigue failure e.g., comminuted
and segmental fractures.
Dynamization is conversion of statically locked nail into a dynamic
mode by removal of less critical transverse screw. It is done in case of
delayed union, usually at 6 weeks. It increases fatigue life of the nail.
Clinical study of interlocking nailing did not show much difference in
healing, between dynamic and static nailing. This may be due to inherent
elasticity of the system and gradual loosening of the interlocking screws due to
bone remodeling which gives the effect of mild dynamization.
The controversies lies in the degree of mechanical instability one
should provide with fixation, in order to stimulate bone growth and case the
surgical procedure.
We have to balance between fracture stability, biological effects and
clinical practicability.
50
Biology of Fracture and Fracture Healing with Intramedullary Locked
Nail
Fractures are accompanied by perfusion disturbances of varying
degree. Simple fractures without major soft tissue damage may not lead to
any significant circulatory deficits or may be confined to a limited area of
about 1 mm. In intermediate fractures, perfusion from the intramedullary
vessels is Interrupted. Bone is perfused in the outer one-third by the periosteal
vessels only. Because fractures close to the metaphysis are located largely in
the cancellous bone, they are less likely to suffer circulatory deficiency.
Measurable vascular damage is caused only by major trauma or extensive soft
tissue detachment.
During the repair of a fracture, adjacent intraosseous and extraosseous
arterial circulations proliferate greatly. The greatest proliferation at a simple
fracture is of medulla derived arteries and arterioles. The earliest external
callus is supplied by new extraosseous arterioles derived from torn soft tissue
in the vicinity, but this new supply is only transitory. Detached bone
fragments require maintenance of the new extraosseous supply until they
become incorporated, when the medullary circulation again takes over.
Mechanical Aspects of Nailing
Mechanically, a medullary nail represents a gliding splint. Motion at
the fracture site is restricted, but not eliminated.
51

The fixation rests mainly on elastic three point contact in longitudinal
direction. Rotational stability using conventional nailing is limited.
The interlocking nail allows for insertion of screws through the bone
and the nail, both proximally and distally, preventing shortening, tilting and
torsional displacement. It allows a certain amount of fracture mobility, but the
critical amount of strain for healing is not exceeded.
Effects of Intramedullary Fixation by a Loose Fitting Nail – Unreamed
Nailing
Implantation of a medullary nail without previous reaming causes
relatively minor damage to the already compromised circulation in the
fractured tibia60. The medullary canal is revascularized more quickly
following non-reamed nail systems. Small vessels grow into existing gaps
between the bone and the nail in a short period of time, from where they
penetrate into the neighboring malperfused cortical bone. At the relatively
few sites of close contact between bone and medullary nail, bone lamellae will
be removed by osteoelastic activity, so that vessels can sprout into the newly
formed gap.
Effects of Reaming61
The reaming process results in the destruction of all vessels in the
medullary canal resulting in the necrosis of inner 50%-70% of the cortex. Due
to the anatomy of the medullary blood supply, the first reaming causes the
essential damage. Subsequent reaming has little effect on cortical vascularity
52

or viability. Hence, reaming is performed only to such an extent as to ensure
sufficient fracture stabilization.
Reaming particles possess bone inductive potential and hence is of
great importance in fracture healing, if surrounded by vital tissue. On the
other hand, the reaming dust represents a large amount of necrotic particles or
microsequestrae, if they are deposited in devitalized zones of the medullary
canal, especially in view of the possible bacterial contamination in open
intramedullary nailing or nailing in open fractures.
The medullary canal is irregular in size in the long axis as well as in
cross-section. Stable intramedullary fixation requires a firm fit for a variable
distance. In reaming the medullary canal, a cylindrical channel of uniform
diameter is prepared for the nail, which improves the stabilizing effect of the
implant. Furthermore, the bending stiffness increases with progressively
larger diameter nails. Therefore, it is necessary to ream to a certain extent.
Various processes contribute to revascularization of disrupted bone.
The medullary circulation regenerate slowly, by means of formation of
longitudinally directed intracortical arterioles, derived from the transected
nutrient artery and arterioles within a new endosteal membrane that come to
surround the nail after osteoclastic removal of nercrotic cortex.
The best configuration for an intramedullary nail is one with open
sources or flutes extending longitudinally between flanges. The flanges will
give firm support to all sectors of the endosteal cortex, and the flutes will
permit regeneration of the essential medullary circulation as rapidly as
possible.
53

Advantages, Disadvantages and Complications of Intramedullary Nailing
Advantages of the Intramedullary Interlocking Nailing
• It is a load sharing mechanism.
• Healing occurs biologically
• Fracture haematoma is preserved
• Periosteal vascular damage is minimal.
• Proved method of treatment in delayed and non-union.
• Effective in open fracture type-I and II with clean wound.
• Even in severe compound fractures Grade-III, IIIA and IIIB (it can be
initially treated with external fixators and later secondary interlocking
can be done).
• Additional bone grafting is not needed.
• Stability and length is well maintained.
• Rotational instability checked by locked screws.
• Joint motion preserved.
• Early mobilization and early weight bearing can be started.
• There is no skin necrosis.
Disadvantages of Intramedullary Interlocking Intermedullary Nailing
• Long leaning curve is present, it is technically demanding and
therefore a larger period of exposure and training is required.
• Exposure irradiation occurs by using the C-arm.
• It is not suitable in fixation of proximal and distal 1/5th of tibia.
54

Complications of Intramedullary Nailing
1. Anterior Knee Pain
This is the commonest complication.
• Keating et al reported a 57% incidence of anterior knee pain.
• Court Brown et al reported 56.2% incidence of anterior knee pain.
• Causes of anterior knee pain may be prominent nail or heterotopic
ossification of patellar tendon.
• It may be due to interarticular damage to menisci or associated
ligaments.
2. Neurologic Abnormalities
• 2% incidence of sural and saphenous nerve damage can occur due to
distal cross screw insertion as noted by Court Brown et al.
• Common peroneal nerve lesions have encountered in 19% of cases and
resolved in 80% of them, due to incorrect positioning of the knee on
the nailing table.
3. Vascular Damage
• It is seen as a result of drill damage to popliteal artery in the area of
arterial trifurcation.
• Damage to medial inferior genicular artery has also been noted.
4. Hardware Breakage
• Screw breakage is common in unreamed nails, which use smaller
screws.
55
• Titanium has lower screw breakage rates.
• Broken nails are associated with untreated non-unions.
• Breaking of drill bits are common and they remain in the bone or soft
tissues.
5. Thermal Necrosis
• Is unusual
• It is caused by excessive use of force and blunt reamers.
• Tourniquet should not be used as it eliminates heat convective transfer
by shutting down global blood flow to whole limb.
6. Bone Damage
• Incorrect starting point or failure to aim the nail may damage bone and
splinter the proximal entry point.
7. Intramedullary nailing may precipitate adult respiratory distress
syndrome in patients with blunt thoracic trauma due to bone marrow
emboli and reaming of the bone may precipitate emboli formation.
56

APPROACHES
1. Medial parapatellar approach62
• A longitudinal incision along the medial margin of the patellar tendon.
• The patellar tendon is retracted laterally exposing the point of entry.
• Anterior knee pain is one of the commonest complication.
2. Midline Patellar Splitting Approach63
• A longitudinal incision in the midline anteriorly.
• The portal of entry is approached by splitting the patellar tendon
vertically.
• Anterior knee pain and extensor lag are common complications.
3. Lateral Approach
• Inverted “J’ shaped incision along the lateral border of the patellar
tendon.
• The portal of entry is approached by retracting the patellar tendon
medially.
Guidelines
a) Patellar tendon should be retracted gently.
b) To avoid stress on the medial and posterior cortex, the nail should be
oriented along the long axis of the medullary canal.
57

Point of Entry
The point of entry is proximal to the tibial tuberosity at the level
corresponding to the proximal tip of the fibular head centered on the
medullary canal in the midline62.
Insertion Angle
The insertion angle should be in line with the medullary canal in the
antero-posterior view to prevent valgus/ varus deformity and parallel to the
anterior cortex of the proximal fragment in the lateral view to prevent apex
anterior angulation.
58

MATERIALS AND METHODS
Patients of both sexes belonging to adult age group presenting with
fracture tibia to Orthopaedic Department of Basaveshwar Teaching & General
Hospital, attached to M.R.Medical College, Gulbarga are admitted from
October 2006 to March 2008 and evaluated. Those satisfying our inclusion
criteria and are surgically fit are included in the study. This includes a
prospective study of 20 cases.
Inclusion ad Exclusion Criteria:
Inclusion Criteria
• Transverse and short oblique fractures
• Segmental fractures of shaft of the tibia
• Grade-I (Gustillo Anderson) compound fractures
• Polytrauma cases where early mobilization of patient is indicated.
Exclusion Criteria
• Fractures in children
• Grade-II and III (Gustillo Anderson) compound fractures
• Fractures with intra-articular extension
• Burns/ wounds over the entry portal.
59

1. The name of the patient, age of the patient and sex of the patient
was recorded routinely.
2. The occupation of the patient was noted, and this is considered as
important deciding factor in the early rehabilitation of the patient to
his work.
3. The address of the patient is taken routinely and would be
beneficial in following up the patient.
4. An initial detailed history of the patient, which included mode and
nature of injury, conscious level, any treatment history, signs of
shock and any emergency treatment taken were recorded.
5. A complete clinical examination of the patient was done and the
patient admitted to the ward.
6. A proforma was prepared, which gave complete details of the
patient.
In the history, symptoms of pain, swelling, abnormal mobility,
deformity, loss of function were recorded.
Pain perception may vary according to the fracture, whether fresh or
old fracture, with pain severity being more in fresh fractures.
Swelling is associated with a fracture and is mentioned. Abnormal
mobility is noted. Deformity is also noted in the presenting complaint. The
patient with fracture shaft of the tibia having loss of function is indicated.
60
The mode or nature of injury is noted
• Sports related injuries are low-velocity injuries.
• Direct blow/ assaults are injuries associated with high and significant
soft tissue damage.
• Motor vehicle accidents are high-velocity injuries.
• Gunshot injuries are both low and high-velocity injuries.
• Pathological fractures may be as a result of trivial trauma.
• The injuries is classified in the proforma enclosed.
• Sports injuries are usually closed injuries and simple injuries.
• In cases of fall, sports injuries and direct blow to tibia, a simple
fracture configuration is present.
• Falls from a height and motor vehicle accidents have a more complex
fracture pattern with open wounds.
• The duration of injury is noted.
• Systemic illness is enquired, which includes diabetes, hypertension,
ischemic heart disease and epilepsy and it is recorded in the proforma.
• Personal history is enquired like smoking, alcohol intake, which may
have a bearing on fracture healing.
General Physical Examination
• The assessment is done routinely, to evaluate the fitness of the patient
to undergo surgery and the bearing it would have in the successful
outcome on the surgery.
61
• The patient’s build, nourishment and pallor is evaluated along with his
vital functions.
Systemic Examination
• This is done to assess the cardiovascular, respiratory, central nervous
system and includes an abdominal examination.
• This is a pre-operative assessment, to evaluate fitness of patient from
the proposed surgery and to treat the abnormalities, if any.
Local Examination includes Inspection and Palpation
1. Gait: is assessed to whether the patient is able/ unable to walk.
2. Skin: Is examined with the associated wound if present. Simple falls,
sports injuries have a closed injury pattern with skin being normal.
3. Swelling: is assessed, and according to the severity is graded as present
or absent.
4. Attitude and deformity is assessed, whether there is varus, valgus or
rotational deformity. It is mentioned as present or absent.
5. Tenderness is palpated and may be mild, moderate or severe, at the site
of fracture. It is mentioned as present or absent.
6. Movement of the knee and ankle is mentioned as restricted or normal
and if abnormal mobility is present at fracture site it is assessed and is
noted with associated Crepitus.
7. Shortening is measured in the leg segment and is mentioned as the
amount of shortening in cms.
62

8. Associated injuries were noted in same or contralateral side. Bony
injuries and associated neurovascular injuries like dorsalis pedis,
posterior tibial, common peroneal, and tibial nerve injury is mentioned
as it is.
9. Abnormal mobility is mentioned as present or absent. Complications
like fat embolism, shock and compartment syndrome should be ruled
out and treated if present.
Provisional Diagnosis
• Is made on the basis of history, clinical signs and symptoms.
• Once a provisional diagnosis is made an emergency radiograph is
taken, at the same time giving the patient some analgesics and tetanus
toxoid, and immobilization is done with a splint temporarily.
• If there is low blood pressure, feeble pulse and tachycardia, the
protocol of shock management is initiated.
Investigations
1. Routine
Blood
• Hb%
• PCV
• TC
• DC
• ESR
63

• FBS, if the patient is diabetic
• PPBS, if the patient is diabetic
• RBS
• BT
• CT
• Blood grouping and typing
• Blood urea
• Creatinine
• HIV – After obtaining the patient’s consent.
• HbsAg – After obtaining the patient’s consent.
• VDRL
Urine
• Routine – albumin/ sugar/ microscopy.
Stool
• Ova
• Cyst
• Microscopy
2. ECG – in all chest leads
3. Chest X-ray PA view.
4. X-ray of the leg both antero-posterior and lateral view.
64
A diagnosis of the type of fracture is done, whether it is unifocal
fracture (spiral, oblique and transverse), wedge fracture, or a complex fracture.
The assessment of the level of fracture is also done.
The Tscherne type is assessed radiologically.
Fibular fracture is noted as present or absent.
Preoperatively
1. Once the routine investigation along with the required ECG, CRX-PA
view is done, physician’s advice regarding fitness for surgery is
obtained in the form.
2. In case of anemia adequate transfusions of whole blood, packed cells
and autotransfusions to improve the general condition is carried out.
3. Static quadriceps exercises are taught to the patient and he is educated
regarding surgery and outcome.
4. Active hip, knee and ankle movements are initiated.
5. The limb is immobilized during the pre-operative stage by above knee
POP slab.
6. Pre-anesthetic check-up is done with a bottle of blood as standby.
7. Preparation of part to be operated is done.
8. Preoperative nail selection is done on the basis of preoperative X-ray
to assess the width of nail by measuring the canal diameter at the
narrowest portion in X-rays in the antero-posterior view.
65

9. Length of the nail is assessed by measuring the normal leg from tibial
tuberosity to medial malleolus and subtracting 2 cm from it. The nail
is selected according to the economy of the patient. Bend in tibial nail
takes into account the anatomic angle of 11 degrees formed by axis of
access canal and the medullary canal.
The section in the sagittal plane shows the 11º angle between the insertion (ic)
and the axis (a) of the tibial cavity.
10. The instrumentation required is selected appropriate for the make of
the nail.
66
Operative Procedure
Positioning of the Patient
Patient is operated on a ordinary fracture table with his leg hanging by
the side/ edge of the table.
A pad is used to support the distal femur at a sufficient distance from
the popliteal artery and vein, if it is not properly positioned, circulation is
inhibited by the force used to insert the nail and damages the vascular wall.
• The injured leg is scrubbed, painted with betadine, spirit and draped.
• Longitudinal incision over the patellar ligament at the level of joint, 5
to 6 cm long is used, splitting the tendon longitudinally.
• Entry portal is made 2 cm proximal in the midline or slightly medial
and behind the tibial tuberosity.
• A curved awl is used to open the medullary canal and is pushed as far
as possible into the medullary canal, while the handle should be in line
with the axis of the shaft.
• 3.2 mm guide wire with ball tip is pushed into the canal, past the
fracture site into the malleolar region (0.5 to 1 cm proximal to ankle
joint) assisted by reduction manually.
• If need arises, a small incision is made over fracture site to align the
bones.
• In case of atropic non-union, the fracture site is opened and excision of
the sclerosed ends is done before nailing.
67

• Determination of the length of nail is done by subtracting the exposed
length of guide wire from its overall length using another guide wire of
same size or another nail of same size, which is used with C-arm
assistance.
• The nail with the proximal insertion handle and jig is passed over the
guide wire and is inserted as far as possible, measured hammering is
done to drive the tip of nail to the distal metaphysis and proximal end
should be flush with the surface of cortex at the point of insertion.
• The nail should be centralized as far as possible.
• The guide wire is removed.
• For distal locking by C-arm and free hand technique, the C-arm is
placed to show the locking holes of nail as perfect circles on the
monitor.
• The position is marked with a scalpel and an incision is done on the
skin over the marked locking holes. Steinmann pin is centered on
locking hole under C-arm and a mark is made on the bone with gentle
tap of a mallet.
• Drill bit is inserted through the skin incision down to the bone near the
locking holes and drilled under C-arm with axis of drill centered on the
locking hole with a 4.0 mm drill bit. Drilling hole is done through both
cortices, across locking holes.
• The length is determined with a depth gauge and confirmed with the C-
arm.
68
• The distal locking is done.
• Proximal locking is done with proximal jig and insertion handle.
• Stab-incision is done over appropriate locking hole.
• A 8 mm protection sleeve is inserted and trocar through it, till the
cortex is contacted.
• Trocar is removed and 4.5mm diameter drill sleeve is inserted and
drilled with 4 mm drill bit.
• The drill sleeve is removed, depth of hole is measured with a depth
gauge and a screw/ bolt is inserted which is confirmed with the C-arm.
• The C-arm is used to confirm the locking and nail position and fracture
alignment.
• The wound is closed and dressing is done, compression crepe bandage
is applied to control postoperative swelling.
• Postoperatively the limb is elevated on a pillow.
Post-operative Period
Postoperatively, the limb is elevated on a pillow. Immediate
postoperative complications like fat embolism and compartment syndrome,
neurological damage and vascular injury is looked for. Wound infection is
watched for in the postoperative period.
Parenteral antibiotics are given for 5 days, and continued in the form of
oral antibiotics till suture removal, which is done on 14th day.
69

Active quadriceps exercises are restarted on the first postoperative day
with active ankle and toe movement with knee mobilization, as far as the
patient is comfortable and free of pain.
Radiograph of the leg is taken to assess the fracture alignment, nail
placement and locking screws.
The patient is made to ambulate from the third postoperative day
without bearing weight on the operated leg with crutches or walker. Suture
removal is done after the 14th day if the wound has healed.
Follow Up
It was done using Johner and Wruh’s criteria. Patients were followed
up periodically on an outpatient basis at 4th, 6th, 10th, 12th, 16th, 20th weeks and
6th month and in between if required. The complaints were noted and the
clinical and radiological assessment of the patients were done, for pain,
deformity, shortening, range of motion of knee, ankle and subtalar joints and
radiological union.
Pain was noted as none, occasional, moderate and severe. Deformity was noted as none, anteversion-recurvatum, varus-valgus
and rotation deformity in degrees.
Shortening was noted in the form of measurement and was noted in
cms or was noted as nil if absent.
70
Range of motion of knee, ankle and subtalar joints was noted in
percentage. 100% being normal. More than 80% for knee, more than 75% for
ankle and more than 50% for subtalar joint was considered good.
Radiological assessment is done on the basis of whether there is callus,
or union or if fracture is consolidated.
Radiological union is noted as consolidated for excellent and good
results. Union for fair results and not consolidated for poor results at 6
months.
Angular alignment (varus-valgus, anterior and posterior angulation)
was assessed radiologically. Varus-valgus was determined by measuring the
angle between the line drawn perpendicular to bisecting the tibial plateau and
proximal medullary canal with the line bisecting the distal medullary canal
and tibial plafond.
Anteroposterior alignment was determined by measuring the angle
between the lines parallel to the proximal fragment and distal fragment on
lateral radiographs. Rotations were assessed clinically.
Malunion was considered when varus-valgus angulation was more than
5º, anterior-posterior was more than 10º, internal and external rotations of
more than 10º and shortening of more than 10 mm.
71

Weight bearing was done, initially partial weight bearing at the 4th
week depending on type of fracture and rigidity of fixation.
Full weight bearing is allowed after bridging callus is seen and there is
solid union, usually at 10-12th week.
Late delayed complications like screw breakage, nail bending, mal-
union, non-union, limp, anterior knee pain and infection is noted and any
secondary procedure done is noted in the proforma.
Dynamization if needed is done, if there is a delay in callus formation
and is done of screws further away from fracture site. It is noted whether
dynamization of proximal/ distal screws was done.
Gait was assessed whether normal or associated with a limp.
In this study fracture union was considered when patient was weight
bearing without pain, fracture site was not tender on palpation, radiograph
showed osseous union in antero-posterior and lateral views.
Gait and ability to do strenuous activities was also assessed.
They were graded as excellent, good, fair or poor using Johner &
Wruh’s criteria.
72
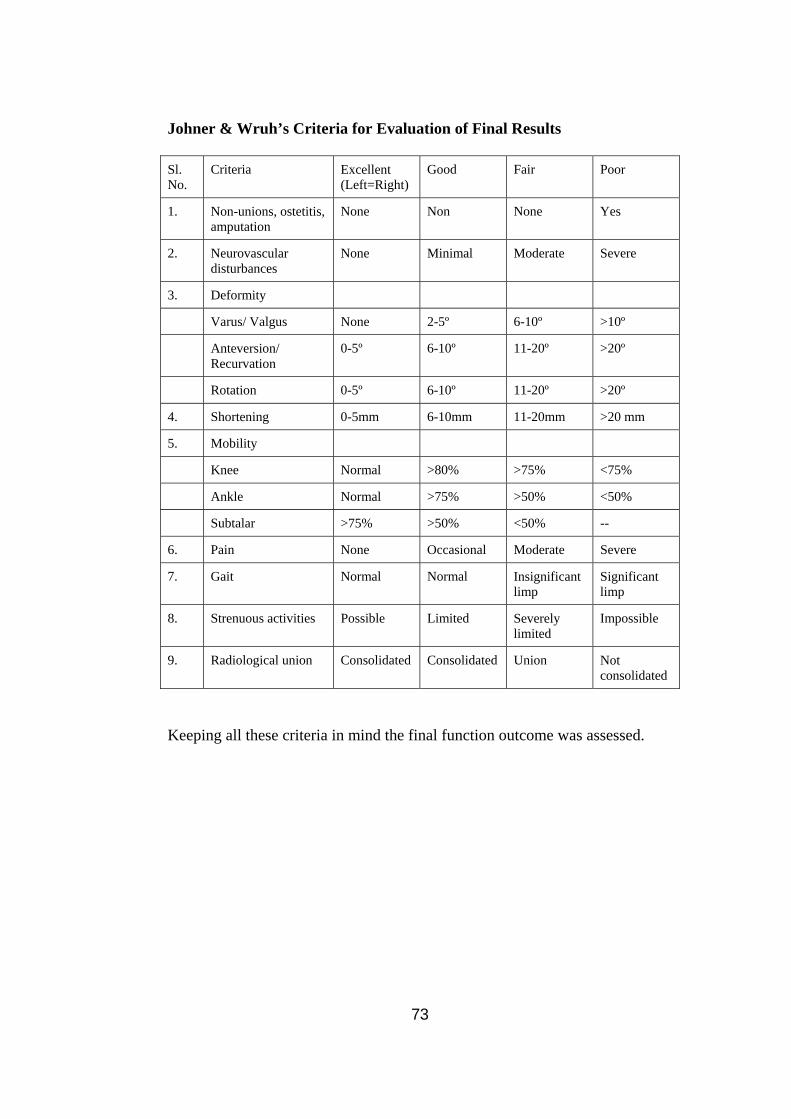
Johner & Wruh’s Criteria for Evaluation of Final Results
Sl. No.
Criteria Excellent (Left=Right)
Good Fair Poor
1. Non-unions, ostetitis, amputation
None Non None Yes
2. Neurovascular disturbances
None Minimal Moderate Severe
3. Deformity
Varus/ Valgus None 2-5º 6-10º >10º
Anteversion/ Recurvation
0-5º 6-10º 11-20º >20º
Rotation 0-5º 6-10º 11-20º >20º
4. Shortening 0-5mm 6-10mm 11-20mm >20 mm
5. Mobility
Knee Normal >80% >75% <75%
Ankle Normal >75% >50% <50%
Subtalar >75% >50% <50% --
6. Pain None Occasional Moderate Severe
7. Gait Normal Normal Insignificant limp
Significant limp
8. Strenuous activities Possible Limited Severely limited
Impossible
9. Radiological union Consolidated Consolidated Union Not consolidated
Keeping all these criteria in mind the final function outcome was assessed.
73

Figure-6: Instrumentation Set for Tibia Intramedullary Locking Nail BASIC STANDARD SET
• CURVED BONE AWL • I.L.GUIDE WIRE - 2.5 MM * 750 MM • SOCKET WRENCH - 10 MM • HEAD FOR INTRODUCER • CURVED JIG • CONICAL BOLT WITH LOCKING NUT, CHECK NUT & TOMY BAR - 8 -
9MM (SP) • CONICAL BOLT WITH LOCKING NUT, CHECK NUT & TOMY BAR - 10 - 13
MM (SP) • S . S . DRILL BIT - 3.2 MM - 200 MM (SP) • S . S . DRILL BIT - 4.0 MM - 200MM (SP) • I . L . DRILL SLEEVE - 3 . 2 MM • I . L . DRILL SLEEVE - 4 . 0MM • PROTECTION SLEEVE - 8 . 0MM • I. . L . DEPTH GUAGE - 4 . 5 MM • POINTER • EXTRACTOR ROD • HANDLE FOR EXTRACTOR • ROUND HAMMER • ALUMINIUM BOX WITH THREE TRAY - 18"
74

75

76

OBSERVATION AND RESULTS
This study was done in the Basaveshwar Teaching & General Hospital,
Gulbarga, 20 patients with fracture shaft of tibia were treated with closed
interlocking nailing. The results are observed here.
Table-1: Age Incidence
Age group (years) No. of Patients Percentage 11 – 20 1 5.00 21 – 30 7 35.00 31 – 40 8 40.00 41 – 50 3 15.00 51 – 60 1 5.00 61 – 70 -- -- 71 – 80 -- -- Total 20 100.00
Figure-8: Showing Age Incidence
0
1
2
3
4
5
6
7
8
No.
of
Cas
es
11 –
20
21 –
30
31 –
40
41 –
50
51 –
60
61 –
70
71 –
80
Age group (years)
77

In this study the minimum age of the patient was 18 years and the
maximum age was 60 years. Average age of the patient in the study was
34.75 years. The tibial shaft fractures were common in the age group of 31-40
years in the present study.
Table-2: Sex Incidence
Sex No. of Patients Percentage
Male 17 85.00
Female 3 15.00
Total 20 100.00
In our study, males predominate the female sex. The present study has
85% males and 15% females.
Figure-9: Sex Incidence
Male 85%
Female15%
78

Table-3: Involved Limb
Involved Limb No. of Patients Percentage
Right 15 75.00
Left 5 25.00
Both -- --
Total 20 100.00
In this study, the right tibia was affected in 75% of all patients and the
left tibia in 25% of all patients.
Figure-10: Showing Involved Limb
0
2
4
6
8
10
12
14
16
No.
of
Cas
es
Righ
t
Left
Both
Involved Limb
79

Table-4: Mode of Injury
Mode of Injury No. of Patients Percentage
Road traffic accident 17 85.00
Fall from a height 2 10.00
Assault 1 5.00
Total 20 100.00
Figure-11: Mode of Injury
0
2
4
6
8
10
12
14
16
18
No.
of
Cas
es
Road
tra
ffic
acci
dent
Fall
from
ahe
ight
Assa
ult
Mode of Injury
In this study, road traffic accidents were the most common mode of
injury causing tibial shaft fractures in 17 of all patients. They accounted for
85% of tibial fractures.
80

Table-5: Anatomical Location of the Fracture
Anatomical location of the fracture No. of Patients Percentage
Upper third 2 10.00 Upper third and middle third junction 1 5.00 Middle third 10 50.00 Middle third and lower third junction 1 5.00 Lower third 5 25.00 Upper third and middle third junction and middle and lower third junction (segmental)
1 5.00
Total 20 100.00 The commonest anatomical location of fracture was at the middle-third
of the tibia. This constituted 50% of tibial shaft fractures.
Figure-12: Anatomical location of the fracture
0
1
2
3
4
5
6
7
8
9
10
No.
of
Cas
es
Upper third Upper third andmiddle third
junct ion
M iddle third M iddle third andlower third
junct ion
Lower third Upper & middle3rd and middleand lower 3rd
junct ions
Anatomical Location of Fracture
81

Table-6: Type of Injury
Type of injury No. of Patients Percentage
Simple 15 75.00
Compound (Grade-I) 5 5.00
Total 20 100.00
In this study 15 fracture were simple (75%) and 5 fractures were
Gustillo Grade-I compound fractures (25%).
Figure-13: Type of Injury
Simple
75%
Compound (Grade-I)
25%
82

Table-7: Type of Fracture
Type of Fracture No. of Patients Percentage
Transverse 4 20.00 Oblique 7 35.00 Wedge (butterfly) 2 10.00 Spiral 1 5.00 Segmental 1 5.00 Communited 5 25.00
Total 20 100.00
In this study, oblique fractures were seen in 35% of patients, followed
by communited fractures in 25% of patients, followed by transverse in 20% of
patients. Wedge fractures were seen in 10% of patients.
Figure-14: Type of fracture
0
1
2
3
4
5
6
7
No.
of
Cas
es
Tran
sver
se
Obl
ique
Wed
ge(b
utte
rfly
)
Spira
l
Segm
enta
l
Com
mun
ited
Type of Fracture
83

Incidence of Intact Fibula
In our study, 15 cases (75%) had ipsilateral fibular fractures, 5 cases
(25%) had an intact fibula.
Associated Injuries
In our study 15 patients had fracture fibula without any neurological
deficit, which were treated conservatively.
One patient had fracture-V metatarsal (right) which was fixed with a
K-wire.
One patient had fracture distal end of radius (right) who was managed
by percutaneous K-wire fixation.
84
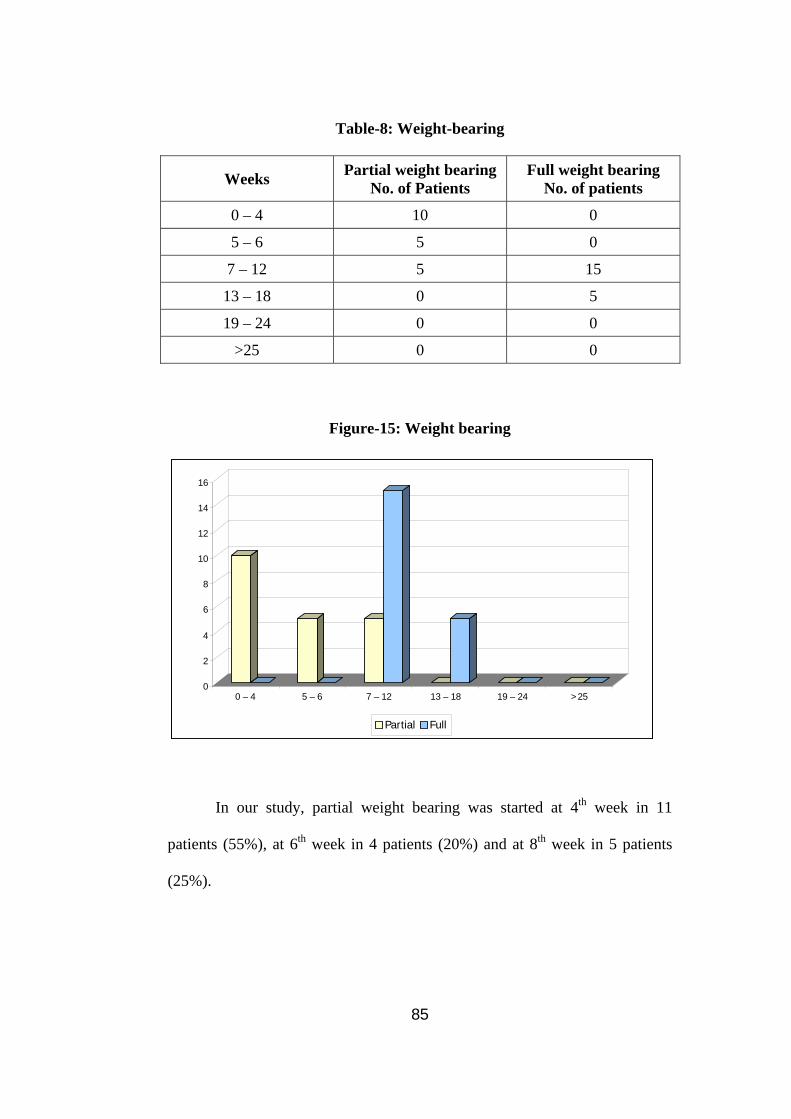
Table-8: Weight-bearing
Weeks Partial weight bearing No. of Patients
Full weight bearing No. of patients
0 – 4 10 0
5 – 6 5 0
7 – 12 5 15
13 – 18 0 5
19 – 24 0 0
>25 0 0
Figure-15: Weight bearing
0
2
4
6
8
10
12
14
16
0 – 4 5 – 6 7 – 12 13 – 18 19 – 24 >25
Partial Full
In our study, partial weight bearing was started at 4th week in 11
patients (55%), at 6th week in 4 patients (20%) and at 8th week in 5 patients
(25%).
85

Full weight bearing was started at 10th week in 10 patients (45%), at
12th week in 6 patients (30%) and at 14th week in 4 patients (20%).
Table-9: Fracture Union
Time taken in weeks No. of Patients Percentage
12 – 16 4 20.00
17 – 20 12 60.00
21 – 24 4 20.00
Total 20 100 In our study, majority of fractures united within 20 weeks. This is
comparable with other series. The average healing time was 19.1 weeks.
Figure-16: Fracture Union
12 – 16
20%
17 – 20
60%
21 – 24
20%
86
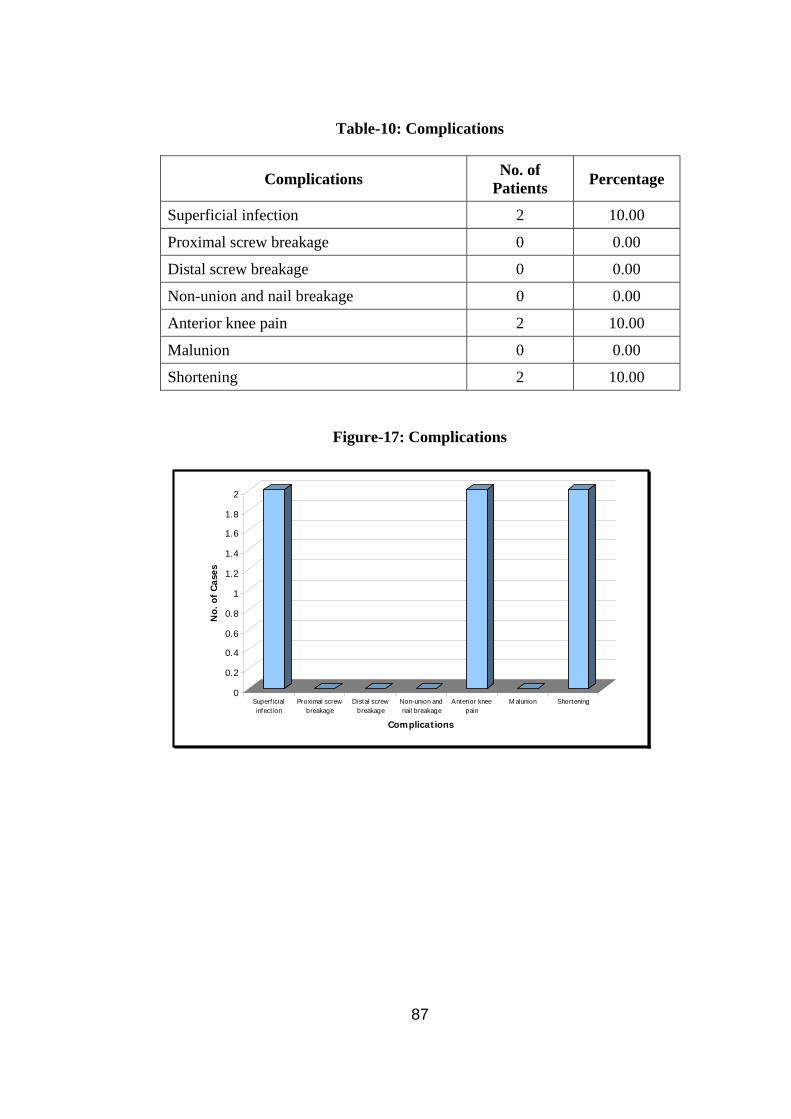
Table-10: Complications
Complications No. of Patients Percentage
Superficial infection 2 10.00
Proximal screw breakage 0 0.00
Distal screw breakage 0 0.00
Non-union and nail breakage 0 0.00
Anterior knee pain 2 10.00
Malunion 0 0.00
Shortening 2 10.00
Figure-17: Complications
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
No.
of
Cas
es
Superf icialinfect ion
Proximal screwbreakage
Distal screwbreakage
Non-union andnail breakage
Anterior kneepain
M alunion Shortening
Complications
87

Complications
• The infection rate was around 10% in our study, which included 2
superficial infections.
• Superficial infections healed by dressing and antibiotics.
• Anterior knee pain was seen in two patients. In one patient, nail was
abutting the patellar tendon and tibial tuberosity and this can be
relieved after removal of the nail.
• Shortening was seen in two patients. One patient had a shortening of 1
cm and the other of 1.5 cms. These were managed by heel raise of the
footwear.
88

Table-11: Functional Outcome
Functional Outcome No. of Patients Percentage
Excellent 12 60.00
Good 6 30.00
Fair 2 10.00
Poor 0 0.00
Total 20 100.00 In our study 60% patients had excellent or good functional results and
30 percent had good functional outcome, while only 10 percent had fair
functional outcome.
Figure-18: Functional Outcome
0
2
4
6
8
10
12
No.
of
Cas
es
Exce
llent
Goo
d
Fair
Poor
Type of Fracture
89

90

Figure-20
91
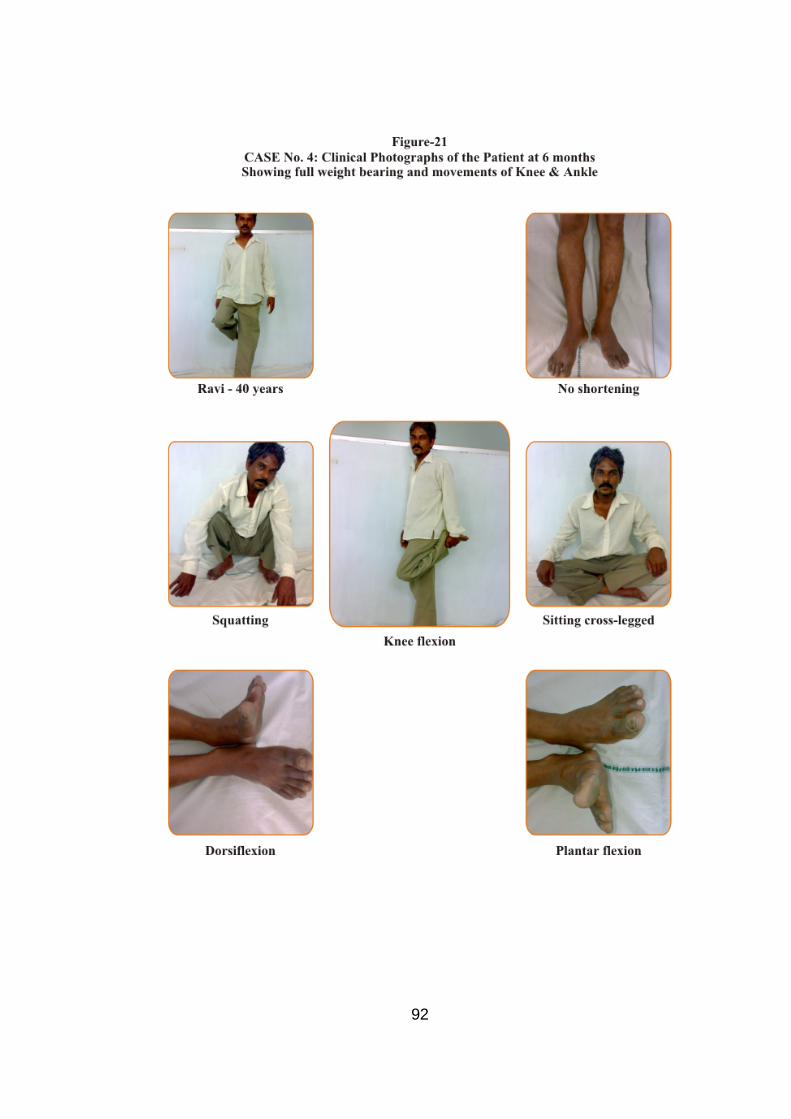
Figure-21
92

Figure-22
93

Figure-23
94
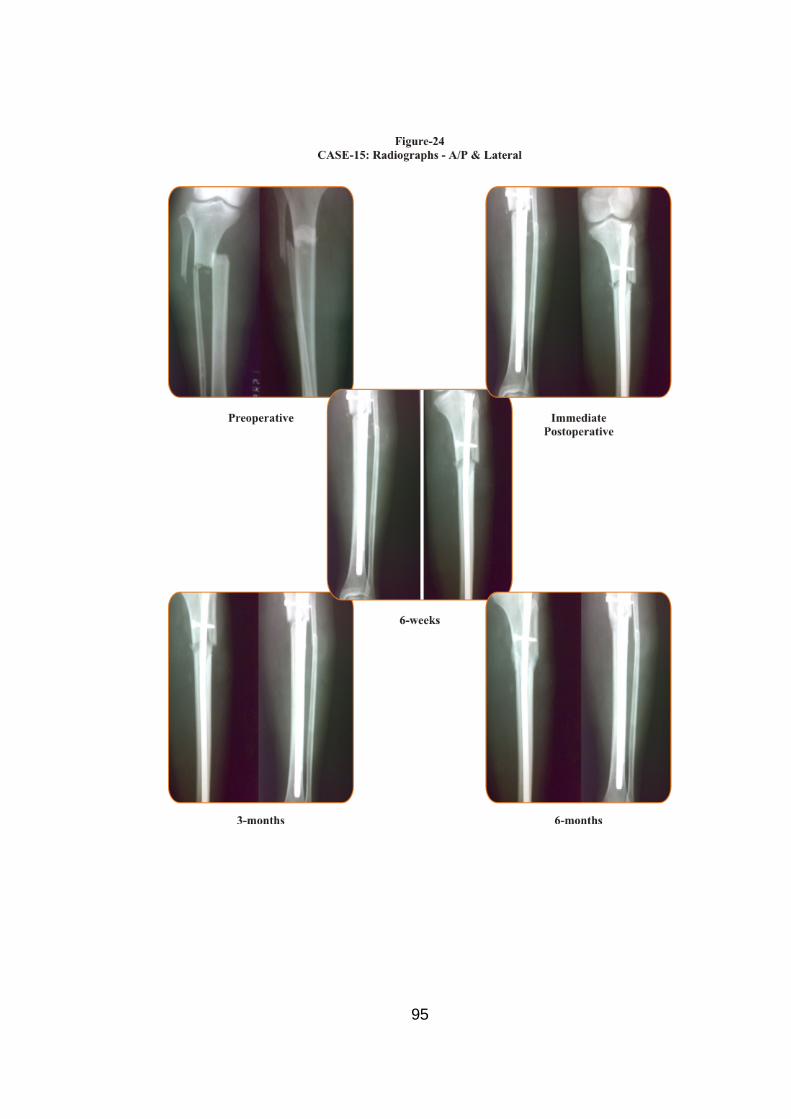
Figure-24
95

Figure-25
96

Figure-26
97

DISCUSSION
This study includes 20 patients who were admitted to the Orthopedics
Wards of Basaveshwar Teaching & General Hospital, Gulbarga.
This series includes various patterns of fractures, closed as well as
open injuries treated by closed method.
Age Incidence
In our study, the majority of the patients were in the age group of 3140
years. There were 8 patients in this age group in our study series. The
average of the patient in our study was 34.75 years. Tibial shaft diaphyseal
fractures were seen in the younger age group as they are the persons who are
physically active, were engaged in increased various outdoor activities and as
a result most of the injuries sustained were high-velocity injuries.
Arne Ekeland et al31 (1988) in a study series of 45 patients noted the
average age of patients to be around 35 years.
Court Brown et al33 (1990) noted the average age to be 32.4 years.
Average age was seen to be around 37 years in a study by Court Brown et al64
in 1995 in a study titled “The Epidemiology of Tibial Fractures”.
Our series with an average age of 34.75 years is comparable to the
other worker’s series, with respect to the average age of the patient in fractures
of the tibial diaphysis.
98

Sex Incidence
In our series, males predominated the females. There were 17 male
patients (85%) and 3 female patients (15%). The incidence of males is higher
because of their more outdoor activities, while women confined themselves to
the domestic activities.
Court Brown et al33 (1990) in their series noted the male incidence to
be around 81.3%, while the female incidence to be around 18.7%.
Hooper et al34 (1991) noted male incidence at 82% and female
incidence at 18%.
Our series of 85% males, the incidence is higher when compared to
above workers series, whereas 15% females in our study is lower when
compared to workers series.
Mode of Injury
In our series, we have found that majority of the tibial diaphyseal
fractures occurred due to road traffic accidents (17 patients). In the majority
of cases, they involved the patients who were the motorists, while the
remaining patients tended to be pedestrians or motor vehicle occupants.
The incidence of fracture shaft of tibia due to road traffic accidents
(85%) seemed to be higher in our series compared to Court Brown et al9
(1995) in whose series, the incidence was around 37.5%. But in this series,
99

also the commonest mode of injury was road traffic accidents followed by
sport injuries. This can be attributed to the poor road traffic sense and poor
quality of roads, leading to a higher incidence of road traffic accidents in our
country.
Lawrence B Bone et al29 (1986) reported in an earlier series a 90%
incidence of Road Traffic Accidents in tibial shaft fractures.
Hooper et al34 (1991) reported a 59% incidence in his series.
Anatomical Location of the Fracture
In our series, the anatomical location of the fracture was in the middle-
third of the shaft of tibia in 10 (50%) patients, followed by the lower third in
25% of the cases.
This is comparable to Lawrence B Bone et al29 (1986) series, where
53.5% were middle-third fractures, Hooper et al34 (1991), where 48% were
middle-third fractures and Court Brown et al64 (1995), where 44% were
middle-third fractures.
The middle-third fractures are common because of anatomical features
of more rigidity of the bone and is subcutaneous nature make it more
vulnerable to the injuring force.
100
Type of Fracture
Our series had an higher incidence of oblique fractures in 35% of
cases, transverse fractures made up 20% cases. Oblique and transverse
fractures made 55% fractures (11 patients).
This is comparable to Sankarsan Patro et al25 (1998) in whose series,
there were 59% of these fractures.
Court Brown et al64 (1995) reported 37.2% and Arne Ekeland31 (1988)
reported 42% of transverse and oblique fractures.
The fibula was fractured along with the shaft of tibia in our series in
55% of cases, this is comparable to the series of Court Brown et al64 (1995),
where the fibula was also fractured in 77.7% of the cases. The associated
fracture of the fibula, in most of the cases reflects on the high-velocity injury
pattern in our series, as most of the injuries are due to road traffic accidents.
Preoperative, Operative and Nailing Procedure
In our series, we have used intramedullary nails ranging from 8 to 10
mm in diameter and from 300 to 360 mm in length.
Unreamed closed intramedullary nailing were done in all the cases in
our series. Static locking was done in all the cases.
Schemitsh et al45 (1998) noted no difference in bone formation
between reamed and unreamed nailing.
101

Postoperatively, in our series, no complications like fat embolism,
compartment syndrome, neurological or vascular injury occurred. Superficial
infections occurred in two patients at the site of surgical incision over knee
and both the superficial infections healed by dressings and antibiotics.
In majority of our patients, active hip, knee, ankle movements and
quadriceps exercises were started on the first postoperative day in all the 20
patients. Majority of the patients were mobilized with the walker from the
third postoperative day, without bearing weight on the operated leg. Suture
removal was done in all patients on 14th day. Complete relief of pain was seen
in majority of patients in two weeks.
Follow up was done at 4th, 6th, 10th, 12th, 16th, 20th week and 6th month.
At follow-ups, clinical and radiological assessment was done regularly with
suitable follow-up advice.
Depending upon the type of fracture and stable fixation of fracture,
partial weight bearing was started. In our series, partial weight bearing was
started in the majority of patients (11) by the 4th week.
Full Weight Bearing
Full weight bearing in our series was started at 10th week in 10 patients
(50%) at 12th week in 6 patients (30%) and at 14 week in 4 patients (20%).
The appearance of bridging callus was used to assess and allow the patient full
weight bearing. The average time of full weight bearing was 9 weeks. Full
102
weight bearing has been delayed in 5 patients as there were communited
fractures.
This is comparable to Lawrence B.Bone et al29 (1986), wherein his
study weight bearing has been delayed in unstable fractures.
Eighteen patients (10%) in our series recovered and got normal knee,
ankle and subtalar joint movements.
In two patients, there was restricted mobility of knee, ankle and
subtalar joints.
Fracture Union
Fracture union was considered when patient was full weight bearing
without pain, fracture site was not tender on palpation and radiograph showed
osseous union.
In our series, majority of fractures united within 20 weeks (16 patiens).
The average time of union 19.1 weeks. This is comparable to the study done
by Lawrence B.Bone et al29 (1986) who reported average union time at 19
weeks. Court Brown et al33 (1990) reported average union time at 16.7 weeks.
Arne Ekeland et al31 (1988) reported average union time at 16 weeks.
In our series, average time of union was 19.1 weeks.
Complications
Lawrence B.Bone et al29 (1986) noted an infection rate of 6.25%.
103

Arne Ekeland et al31 (1988) noted infection rate of 4.4%.
Blachut PA et al44 (1997) noted an infection rate of 1%.
In our series, which is comparable to the above workers study series,
superficial infection rate was 10% and it healed with dressings and antibiotics.
Anterior knee pain was seen in two patients 10%. In these patients the
nail was abutting the patellar tendon and tibial tuberosity, causing anterior
knee pain and this can be relieved after removal of the nail.
Anterior knee pain can be compared to Hernigou P et al49 (2000), who
noted improper entry of nail into medullary canal, may cause anterior knee
pain.
Jarmo AK Toivannen et al50 (2002) noted anterior knee pain to be
common in tibial intramedullary nailing.
Functional Outcome
Final assessment in our series was done at 6 months using the Johner
and Wruh’s criteria28, taking into account the following objective and
subjective symptoms of gait, pain, deformity, range of motion of knee, ankle
and subtalar joints, shortening, neurovascular disturbances, ability to do
strenuous activities, radiological union and presence or absence of non-union.
Functional outcome was graded into excellent, good, fair and poor.
104

In our series, 60% (12 patients) have got excellent, 30% (6 patients)
have good, 10% (2 patients) have fair functional outcome.
Arne Ekeland et al31 (1988) reported 64.4% excellent, 28.8% good and
4.4% as fair.
105

SUMMARY
From October 2006 to March 2008, 20 patients with fractures of the
shaft of tibia were treated by closed intramedullary interlocking nailing at
Basaveshwar Teaching & General Hospital, Gulbarga.
• Majority of the patients were in the age group of 31 to 40 years.
• Average age of the patient in our series is 34.75 years.
• Males predominated the females in the ratio of 85:15.
• Right tibia was affected in 75% of the cases.
• Road traffic accidents were the main mode of injury in 85% of cases.
• 75% of the fractures were closed and 25% were open (Gustillo-I).
• Majority of fractures were located in the middle-third (50%) in 10
patients and in lower-third in 5 patients (25%).
• Transverse and oblique fractures (55%) were common.
• Fibula was fractured in 75% of cases.
• Unreamed closed intramedullary interlocking nailing were done in all
the 20 cases.
• Static locking was done in all (20) cases in our series.
• In our study, partial weight bearing was started at 4th week in 11
patients (55%), at 6th week in 4 patients (20%) and at 8th week in 5
patients (25%).
106
• Full weight bearing was started at 10th week in 10 patients (50%), at
12th week in 6 patients (30%) and at 14th week in 4 patients (20%).
• Final assessment was done after 6 months taking into account gait,
pain, deformity, movement of knee, ankle and subtalar joints, ability to
do strenuous activity, shortening and radiological union, taking into
account neurovascular disturbances.
• The average healing time was 19.1 weeks.
• There were two superficial infections and two patients with anterior
knee pain.
• Two patients had slight shortening.
• In our study 12 patients (60%) had excellent, 6 patients (30%) had
good, 2 patients (10%) had fair functional outcome.
107
CONCLUSION
• Tibial diaphyseal fractures are commonly seen in physically active
young people and are commonly seen as a result of road traffic
accidents.
• The interlocking nailing combines control of length, alignment and
rotation, preserves periosteal blood supply, some amount of endosteal
blood supply and with biological osteosynthesis, lowers the infection
and malunion.
The advantage of locking screws over the conventional methods
reduces the rate of malunion, loss of alignment, angulation and shortening
which are commonly found in a plaster cast or functional brace. The addition
of locking screws extends its indications to within 5 cm of ankle and knee
joint.
• The method of treatment employing closed intramedullary interlocking
nailing to stabilize both principal fragments on the nail, is an excellent
one for closed fractures with communition and open fractures of
Gustillo Grade-I variety.
• Patients operated with this technique can be ambulated early without
external immobilization in majority of cases, patients are allowed to
resume work early as tolerated and this procedure also reduces the
hospital stay and boosts up the morale of the patient.
108

• The method of intramedullary interlocking nailing is ideal because of
excellent (60%) and good results (30%), which is comparable to other
workers series.
• The method has a long learning curve but with the excellent results, the
advantage of rapid rehabilitation and relatively few complications
serve to recommend it for wider use.
109

BIBLIOGRAPHY
1. Farill J. Orthopedics in Mexico. J Bone Joint Surg Am.
1952;24:506-12.
2. Konig F. Uber die Implantation von Elfenbein zum Ersatz von
Knochen und Gelenken. Nach experimentellen und klinischen
Beobachtungen. Beitr Klin Chir. 1913;85:91-114.
3. Bircher H. Eine neue Methode unmittelbarer Retention beiFracturen
der Rohrenknochen. Arch Klin Chir. 1886;34:410-22.
4. Gluck T. Autoplastic transplantation. Implantation von Frem-dkörpern.
Berl Klin Wochenschr. 1890;19.
5. Nicolaysen J. Lidt on Diagnosen og Behandlungen av. Fr. colli
femoris. Nord Med Ark 1897;8:1.
6. Hoglund EJ. New method of applying autogenous intramedul-lary
bone transplants and of making autogenous bone-screws. Surg
Gynecol Obstet. 1917;24:243-46.
7. Hey Groves EW. On the application of the principle of extension to
comminuted fractures of the long bone, with special reference
to gunshot injuries. Br J Surg. 1914;2(7)429-43.
8. Smith-Petersen MN. Intracapsular fractures of the neck of the
femur. Treatment by internal fixation. Arch Surg.
1931;23:715-59.
9. Rush LV, Rush HL. A technique for longitudinal pin fixation of certain
fractures of the ulna and of the femur. J Bone Joint Surg.
1939;21:619-26.
110

10. Küntscher G. Die Marknalung von Knochenbruchen. Langenbecks.
Arch Klin Chir. 1940;200:443-55.
11. Rehnberg SV. Treatment of fractures and pseudarthroses with marrow
nailing. Ann Chir Gynaec Fenn. 1947;36:2.
12. Westerborn A. Marrow nailing of recent fractures and pseudo-
arthrosis. Report of 28 cases. Acta Chir Scand. 1944;90:89.
13. Soeur R. Intramedullary pinning of diaphyseal fractures. J Bone Joint
Surg. 1946; 28:309.
14. Street DM, Hansen HC, Brewer BJ. The medullary nail.
Presentation of a new type and report of 4 cases. Arch Surg.
1947;35:423.
15. Fischer AW, Maatz R. Weitere Erfahrungen mit der Marknage-lung
nach Küntscher. Arch Klin Chir. 1942;203:531.
16. Modny MT, Bambara J. The perforated cruciate intramedullary nail:
Preliminary report of its use in geriatric patients. J Am Geriatr
Soc. 1953;1:579-88.
17. Modny MT, Lewert AH. Transfixion intramedullary nail. Orthop
Rev. 1986;15:83-8.
18. Zickel RE. A new fixation device for subtrochanteric fractures of the
femur: A preliminary report. Clin Orthop Relat Res.
1967;(54):115-23.
19. Brumback RJ, Reilly JP, Poka A, et al. Intramedullary nailing of
femoral shaft fractures. Part I: Decision-making errors with
interlocking fixation. J Bone Joint Surg Am. 1988;70:1441-52.
111

20. Brumback RJ, Uwagie-Ero S, Lakatos RP, et al. Intramedullary nailing
of femoral shaft fractures. Part II: Fracture-healing with static
interlocking fixation. J Bone Joint Surg Am. 1988;70:1453-62.
21. Brumback RJ, Ellison TS, Poka A, et al. Intramedullary nailing of
femoral shaft fractures. Part III: Long-term effects of static
interlocking fixation. J Bone Joint Surg Am. 1992;74:106-12.
22. Stapert JW, Geesing CL, Jacobs PB, et al. First experience and
complications with the long Gamma nail. J Trauma.
1993;34:394-400.
23. Lucas SE, Seligson D, Henry SL. Intramedullary supracondylar
nailing of femoral fractures. A preliminary report of the GSH
supracondylar nail. Clin Orthop Relat Res. 1993;(296):200-
6.
24. Brumback RJ, Toal TR, Murphy-Zane MS, et al. Immediate weight-
bearing after treatment of a comminuted fracture of the femoral
shaft with a statically locked intramedullary nail. J Bone Joint
Surg Am. 1999;81:1538-44.
25. Gerhard BG Kuntscher. The Kuntscher method of intramedullary
fixation. Journal of Bone & Joint Surgery. 1958; 40A: 17-26.
26. Zucmann J et al. Two level fractures of tibia. Journal of Bone and
Joint Surgery, 1969; 51B: 686-693.
27. Merle D’Aubigne, P.Maurer J Zucman, Y Mosse. Blind
intramedullary nailing for tibial fractures. Clinical Orthop.
1974; 105: 267.
112

28. Wruhs O, Johner R. Classification of tibial shaft fractures and
correlation with results after rigid fixation. Clinical Orthop.
1983; 178.
29. Lawrence B Bone, Kenneth D Johnson. Treatment of tibial fractures
by reaming and intramedullary nailing. Journal of Bone & Joint
Surgery. 1986: 68A: 877-886.
30. Kessler SB Hallefeldt, Perren, Schwiberer. The effects of reaming and
intramedullary nailing on fracture healing. Clinical Orthop.
1986: 212.
31. Anglen JO. A comparison of reamed and unreamed nailing of the
tibia. Journal of Trauma, 1995; 351.
32. Scott L, Sledge, Kenneth D, Johnson M, Bradfor Henley J, Tracy
Watson. Intramedullary nailing with reaming to treat non-union
of tibia. Journal of Bone & Joint Surgery. 1989; 71A: 1004-
1019.
33. Court Brown CM, Christie J, McQueen MM. Closed intramedullary
tibial nailing. Journal of Bone & Joint Surgery. 1990; 72B:
605-611.
34. Hooper GJ, Kidell PG, Pennaj ID. Conservative management or
closed nailing for tibial shaft fractures – randomized
prospective trial. Journal of Bone & Joint Surgery. 1991; 73B:
83-85.
35. Habernek H, Kwansy O, Schmid L et al. Complications of
interlocking nailing for lower leg fractures. Journal of Trauma,
1992; 963.
113

36. Wu CC, Shih CH. Effect of dynamization of a static interlocking nail
on fracture healing. Canadian Journal of Surgery, 1993; 302.
37. Wu CC, Shih CH. Treatment of segmental tibial fractures by
interlocking. Journal of Orthopedic Trauma, 1993; 468.
38. Watson JT. Current concepts review, treatment of unstable fractures of
the shaft of tibia. Journal of Bone & Joint Surgery. 1994; 76A:
1575-1583.
39. Anglen JO. A comparison of reamed and unreamed nailing of the
tibia. Journal of Trauma, 1995; 351.
40. Paul Gregory, Roy Sanders. The treatment of closed, unstable tibial
shaft fractures with unreamed interlocking nails. Clinical
Orthopaedics. 1995 June; 315; 48-55.
41. Gregory A. Zych and James J Hutson Jr. Diagnosis and management
of infection after tibial intramedullary nailing. Clinical
Orthopaedics. 1995 June; 315: 153-162.
42. Court Brown CM, Will E, Christie J, McQueen MM. Reamed or
unreamed nailing for closed fractures. Journal of Bone & Joint
Surgery. 1996; 78B: 580-583.
43. Fang-Yao Chiu et al. Treated unstable closed tibial shaft fractures.
Journal of Trauma. 1996 June.
44. Blachut P, A.P.J. O’Brien, R.N.Meek, H.M., Broekhuyse. Interlocking
nailing with or without reaming for the treatment of closed
fractures of tibial shaft. Journal of Bone & Joint Surgery,
1997; 79A: 640-646.
45. Schemitsch EH, Tutchin DC, Kowalski MJ et al. Quantitative
assessment of bone injury and repair after reamed and
114

unreamed locked intramedullary nailing. J Trauma, 1998; 45:
250-255.
46. Daudel A, Gascia A, Dardker Prats and Gomar F Sancho. Non-reamed
flexible locked intramedullary nailing in tibial open fractures.
Clin Orthop. 1998 May; 350: 97-104.
47. Kretteck C et al. The use of poller screws as blocking screws in
stabilizing tibial fractures treated wit small diameter
intramedullary nails. Journal of Bone & Joint Surgery. 1999;
81B: 963-968.
48. Mohit, Bhandari et al. Early v/s delayed operative management of
closed tibial fractures. CORR 1999.
49. Hernigou P et al. Proximal entry for intramedullary nailing of tibia.
Journal of Bone & Joint Surgery. 2000; 82B: 33-41.
50. Jarmo AK, Toivannen et al. Anterior knee pain after intramedullary
nailing of fractures of tibial shaft. Journal of Bone & Joint
Surgery. 2002; 84A: 580-585.
51. Andrew Schmidt et al. Treatment of closed tibial fractures in journal
of JBJS. 2003.
52. Joshi D, Ahmed A, Krishna C, and Lal Y. Unreamed interlocking
nailing in open fractures of tibia. Journal of Orthopaedic
Surgery (Hong Kong). Dec. 2004; 12 (2): 216-21.
53. Jain V, Aggarwal A, Mehtani A, Jain P, Garg V, Dhaon BK. Primary
unreamed intramedullary locked nailing in open fractures of
tibia. Indian J Orthop 2005; 39: 30-2.
115

54. Lascombes P, Harmont T, Journeau P. Use and abuse of flexible
intramedullary nailing in children and adolescents. J Pediatr
Orthop. 2006 Nov-Dec; 26(6): 827-34.
55. Thonse, Raghuram, Janet. Antibiotic cement coated interlocking nail
for the treatment of infected non-unions and segmental bone
defects. Journal of Orthopedic Trauma. 2007 April; 21(4):
258-268.
56. Kyung-Cheon Kim et al. Percutaneous reduction during
intramedullary nailing in comminuted tibial shaft fractures.
Orthopedics 2008; 31: 556.
57. Vaisto O, Toivaren J, Kannus P, Jarvinan M. Anterior knee pain after
intramedullary nailing of fractures of tibial shaft: An eight-year
follow-up of a prospective, randomized study comparing two
different nail-insertion techniques. Journal of Trauma 2008
June; 64(6): 1511-6.
58. Michael WC. Intramedullary fixation in open fractures. Clin Orthop.
1986; 212: 26-33.
59. Richard RT, Donald AW. Mechanics and Biology of IM nails. Clin
Orthop. 1986; 212; 10-17.
60. Rhinelander FW. Effects of medullary nailing on the normal blood
supply of diaphyseal cortex. Instr Course Lect. 1973; 22: 161-
187.
61. Kessler, Hallfeldt, Perren, Schweiberer. The effects of reaming and
intramedullary nailing on fracture healing. Clin Orthop. 1986;
212: 18-25.
62. Paige Whittle. Campbell’s Operative Orthopaedics. 9th Edition, 2068-
2070.
116

63. Keating et al. Knee pain of the tibial nailing. J Orthop Trauma. 1997;
11: 10-13.
64. Court Brown CM, McBrine J. The epidemiology of tibial fractures.
Journal of Bone & Joint Surgery. 1995; 77B: 417-421.
117

ANNEXURES
PROFORMA
Case No.
Name of Patient Age: Sex: IP No.:
Occupation Date of Injury:
Address Date of Admission:
Date of Surgery:
Date of Discharge:
1. Presenting complaints
Pain/ Swelling/ Deformity/ Abnormal mobility/ Loss of function
Nature of injury
• Road traffic accident
• Fall
• Industrial injury
• Farming injury
• Assault
• Fall of an object
• Sports injury
2. General examination
Nourishment Pallor
Pulse Blood pressure Temperature
Respiratory rate
118

3. Systemic examination
• CVS
• RS
• PA
• CNS and neurological status
4. Local Examination
1. Gait
2. Involved limb Present/ Absent
3. Deformity Present/ Absent
4. Swelling Present/ Absent
5. Type of fracture Closed
6. Tenderness Present/ Absent
7. Crepitus Present/ Absent
8. Abnormal mobility Present/ Absent
9. Shortening _________ cms
10. Complications Shock/ Fat
Embolism/ compartment
Syndrome
a) Associated injuries
b) Associated diseases
c) Personal habits
d) Treatment given in the casualty
* Injection – Tetanus toxoid
119
* Splinting/ Skeletal traction
5. Radiological examination: AP/ Lateral view
a) Level of the fracture and site
1. Upper 1/3rd
2. Upper and middle 1/3rd junction
3. Middle 1/3rd junction
4. Middle and lower 1/3rd
5. Lower 1/3rd
b) Type of fracture
* Unifocal (spiral/ oblique/ transverse fracture)
* Wedge (spiral wedge/ bending wedge/ communited wedge)
* Complex (spiral wedge/ segmental/ communited)
* Tscherne type – C0/ C1 / C2 / C3
* Fibular fracture – Present / Absent
6. Investigations
Hb% RBS Urine
PCV Blood urea * Albumin
TC Serum creatinine * Sugar
DC ECG in all chest levels * Microscopy
ESR Chest X-ray in PA view Stool
HIV Blood grouping & typing * Ova
HbsAg * Cyst
VDRL * Microscopy
120
7. Preoperative Planning for Surgery
1. Type of nail and size:
2. Preparation of the patient:
3. Low molecular weight heparin: Administered/ not administered
4. Education of the patient regarding surgery and outcome:
5. Consent for surgery:
8. Surgical Treatment
* Date of operation:
* Type of anesthesia:
* Approach: Vertical patellar splitting
* Nailing: Reamed/ Unreamed
* Locking of nail: Static/ Dynamic
i) Proximal i) Done (1 screw/ 2 screws) ii) Not done
ii) Distal i) Done (1 screw/ 2 screws) ii) Not done
9. Intraoperative complications
Splintering of bone/ breakage of drill bit
a) Intermediate postoperative complications:
Fat embolism/ neurological damage/ compartment syndrome/
hypotension/ vascular injury.
b) Wound infection: Superficial/ Deep
c) Suture removal done: _______ day (between 1 to 2 weeks).
d) Weight bearing: Non-weight bearing – Till 4th week.
* Partial: At 4th week/ 6th week/ 8th week/ 12th week/ 16th week
121

* Full weight bearing: 10th week/ 12th week/ 14th week/ 16th week/
20th week with/ without walking aids
10. Follow up
4th week
6th week
10th week
12th week
16th week
20th week
6 months & above
1. Pain
2. Deformity
3. Range of motion
* Knee
* Ankle
* Subtalar
4. Shortening
5. Radiological union
11. Late of Delayed Complications
• Screw breakage
• Nail bending/ breakage
• Anterior knee pain
• Infection – superficial / deep
• Malunion
• Shortening
• Non-union.
a) Secondary procedures
Dynamization
• Proximal
122

• Distal
b) Procedure done in nail bending/ screw breakage
c) Gait: Normal/ Limping (significant/ insignificant limp)
d) Functional outcome
• Excellent
• Good
• Fair
• Poor
123

KEY TO MASTER CHART
DOA................Date of admission
DOD................Date of discharge
DOHS..............Duration of hospital stay
DOI .................Date of injury
DOS................. Date of surgery
FWB................ Full weight bearing
PWB................ Partial weight bearing
RTA................. Road traffic accident
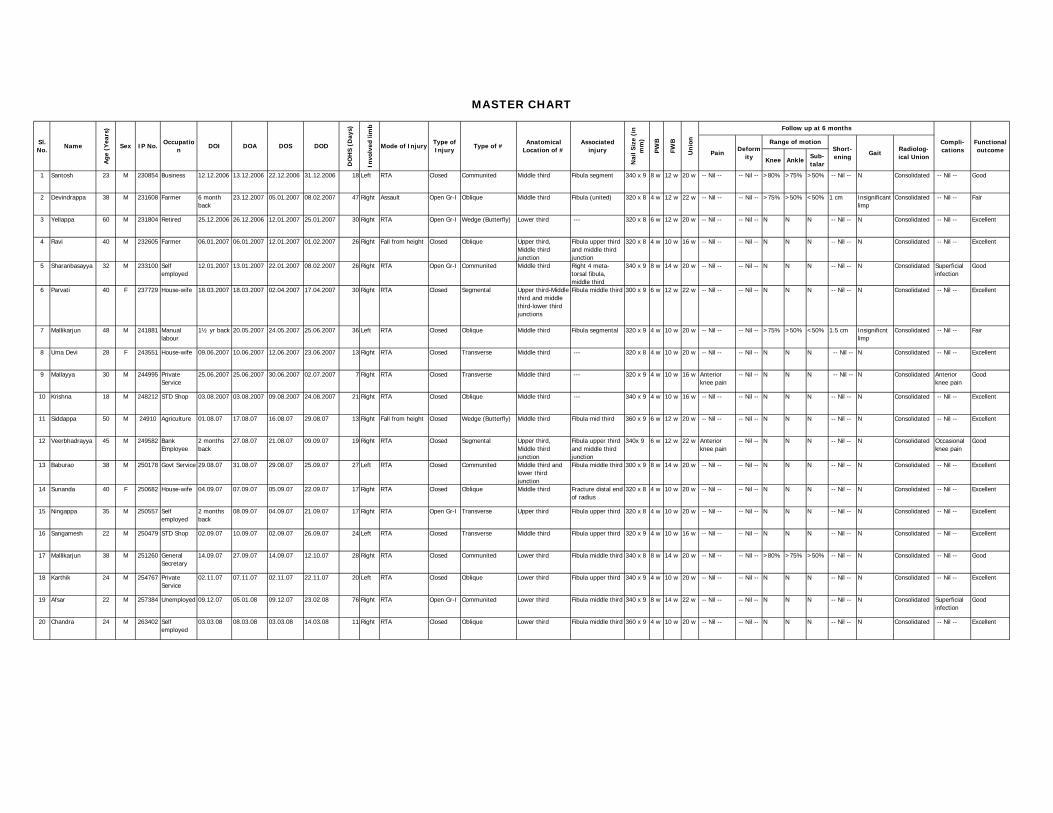
Knee AnkleSub-talar
1 Santosh 23 M 230854 Business 12.12.2006 13.12.2006 22.12.2006 31.12.2006 18 Left RTA Closed Communited Middle third Fibula segment 340 x 9 8 w 12 w 20 w -- Nil -- -- Nil -- >80% >75% >50% -- Nil -- N Consolidated -- Nil -- Good
2 Devindrappa 38 M 231608 Farmer 6 month back
23.12.2007 05.01.2007 08.02.2007 47 Right Assault Open Gr-I Oblique Middle third Fibula (united) 320 x 8 4 w 12 w 22 w -- Nil -- -- Nil -- >75% >50% <50% 1 cm Insignificant limp
Consolidated -- Nil -- Fair
3 Yellappa 60 M 231804 Retired 25.12.2006 26.12.2006 12.01.2007 25.01.2007 30 Right RTA Open Gr-I Wedge (Butterfly) Lower third --- 320 x 8 6 w 12 w 20 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
4 Ravi 40 M 232605 Farmer 06.01.2007 06.01.2007 12.01.2007 01.02.2007 26 Right Fall from height Closed Oblique Upper third, Middle third junction
Fibula upper third and middle third junction
320 x 8 4 w 10 w 16 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
5 Sharanbasayya 32 M 233100 Self employed
12.01.2007 13.01.2007 22.01.2007 08.02.2007 26 Right RTA Open Gr-I Communited Middle third Right 4 meta-torsal fibula, middle third
340 x 9 8 w 14 w 20 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated Superficial infection
Good
6 Parvati 40 F 237729 House-wife 18.03.2007 18.03.2007 02.04.2007 17.04.2007 30 Right RTA Closed Segmental Upper third-Middle third and middle third-lower third junctions
Fibula middle third 300 x 9 6 w 12 w 22 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
7 Mallikarjun 48 M 241881 Manual labour
1½ yr back 20.05.2007 24.05.2007 25.06.2007 36 Left RTA Closed Oblique Middle third Fibula segmental 320 x 9 4 w 10 w 20 w -- Nil -- -- Nil -- >75% >50% <50% 1.5 cm Insignificnt limp
Consolidated -- Nil -- Fair
8 Uma Devi 28 F 243551 House-wife 09.06.2007 10.06.2007 12.06.2007 23.06.2007 13 Right RTA Closed Transverse Middle third --- 320 x 8 4 w 10 w 20 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
9 Mallayya 30 M 244995 Private Service
25.06.2007 25.06.2007 30.06.2007 02.07.2007 7 Right RTA Closed Transverse Middle third --- 320 x 9 4 w 10 w 16 w Anterior knee pain
-- Nil -- N N N -- Nil -- N Consolidated Anterior knee pain
Good
10 Krishna 18 M 248212 STD Shop 03.08.2007 03.08.2007 09.08.2007 24.08.2007 21 Right RTA Closed Oblique Middle third --- 340 x 9 4 w 10 w 16 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
11 Siddappa 50 M 24910 Agriculture 01.08.07 17.08.07 16.08.07 29.08.07 13 Right Fall from height Closed Wedge (Butterfly) Middle third Fibula mid third 360 x 9 6 w 12 w 20 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
12 Veerbhadrayya 45 M 249582 Bank Employee
2 months back
27.08.07 21.08.07 09.09.07 19 Right RTA Closed Segmental Upper third, Middle third junction
Fibula upper third and middle third junction
340x 9 6 w 12 w 22 w Anterior knee pain
-- Nil -- N N N -- Nil -- N Consolidated Occasional knee pain
Good
13 Baburao 38 M 250178 Govt Service 29.08.07 31.08.07 29.08.07 25.09.07 27 Left RTA Closed Communited Middle third and lower third junction
Fibula middle third 300 x 9 8 w 14 w 20 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
14 Sunanda 40 F 250682 House-wife 04.09.07 07.09.07 05.09.07 22.09.07 17 Right RTA Closed Oblique Middle third Fracture distal end of radius
320 x 8 4 w 10 w 20 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
15 Ningappa 35 M 250557 Self employed
2 months back
08.09.07 04.09.07 21.09.07 17 Right RTA Open Gr-I Transverse Upper third Fibula upper third 320 x 8 4 w 10 w 20 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
16 Sangamesh 22 M 250479 STD Shop 02.09.07 10.09.07 02.09.07 26.09.07 24 Left RTA Closed Transverse Middle third Fibula upper third 320 x 9 4 w 10 w 16 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
17 Mallikarjun 38 M 251260 General Secretary
14.09.07 27.09.07 14.09.07 12.10.07 28 Right RTA Closed Communited Lower third Fibula middle third 340 x 8 8 w 14 w 20 w -- Nil -- -- Nil -- >80% >75% >50% -- Nil -- N Consolidated -- Nil -- Good
18 Karthik 24 M 254767 Private Service
02.11.07 07.11.07 02.11.07 22.11.07 20 Left RTA Closed Oblique Lower third Fibula upper third 340 x 9 4 w 10 w 20 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
19 Afsar 22 M 257384 Unemployed 09.12.07 05.01.08 09.12.07 23.02.08 76 Right RTA Open Gr-I Communited Lower third Fibula middle third 340 x 9 8 w 14 w 22 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated Superficial infection
Good
20 Chandra 24 M 263402 Self employed
03.03.08 08.03.08 03.03.08 14.03.08 11 Right RTA Closed Oblique Lower third Fibula middle third 360 x 9 4 w 10 w 20 w -- Nil -- -- Nil -- N N N -- Nil -- N Consolidated -- Nil -- Excellent
MASTER CHART
Sl. No.
Name
Age
(Y
ears
)
Sex IP No.Occupatio
nDOI DOA DOS DOD
DO
HS
(Day
s)
Invo
lved
lim
b
Mode of InjuryType of Injury
Type of #Anatomical
Location of #Associated
injury
Nai
l Siz
e (i
n
mm
)
PW
B
FWB
Un
ion Compli-
cationsFunctional outcome
Follow up at 6 months
PainDeform
ity
Range of motionShort-ening
GaitRadiolog-ical Union



![Clinical Study …downloads.hindawi.com/journals/tswj/2012/386478.pdfembolism during deep vein aneurysm surgical repair [2, 18] or when thrombosis recurred in venous surgical area](https://img.pdfslide.net/doc/110x75/5f78114f0b793b21a578ee8f/clinical-study-embolism-during-deep-vein-aneurysm-surgical-repair-2-18-or-when.jpg)

























