Embed Size (px)
Citation preview

A Clinically Integrated Network
Community Care of NC Innovation Forum
January 13th, 2015

Course Objectives:
Participants will understand what a Clinically Integrated (CIN) is and the role they will play in health care reform.
Participants will understand and be able to discuss different perspectives on health reform and CINs – primary care, safety net providers and hospitals.

Clinical Integration Defined
• A network of physicians working collaboratively to improve the quality and efficiency of patient care – led by physicians and supported by a population health management infrastructure (CCNC).
• To be the health care delivery solution for “all” systems by demonstrating value and quality of care.
• Physicians are the leaders in the development of all facets of the program.
• Facilitating the delivery and coordination of patient care across conditions, providers, settings and time.
• Focusing on patient populations.

Vision and Principles
• Several provider organizations, in an effort to better serve the needs of their members, have requested that CCNC help support the development of a Clinically Integrated Network (CIN) demonstrating enhanced quality, efficiency and access to health care services.
• Participating providers must demonstrate commitment to improving the qualify of care for their patients.
• Starting with primary care providers but will add aligned specialists and hospitals interested in improving health outcomes and moving towards a value-based model.

5
LargeHealth System
Owned344,655
Other(RHC, LHD, other)
96,226
Established Provider-led
ACO’s73,887
Independents644,602
FQHC100,800
OtherHospital Owned
120,869
Unenrolled355,413
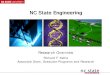
CCNC Medical Home Network: Where are
Medicaid Beneficiaries Seen?
*Numbers represent estimated number of members enrolled in each type of practice (total member months divided by 10).

6
Federally Qualified Community Health CentersOther Safety Net (RHC, LHD, other)IndependentsEstablished Provider-led ACO’sLarge Health System Owned PracticesOther Hospital Owned Practices
Who Provides Primary Care Medical Homes for NC Medicaid Recipients?

7

Initial Steps in the Formation of the CIN:
• Network Name and Logo
• Geographic Coverage
– State-wide (with potential for regional contracts)
• Legal Structure
– LLC – Limited Liability Company
• Provider Relations and Recruitment Effort
– Marketing material
– Letter of Intent
– Participation Agreement
• Initial Governing Board Members Identified

Initial Governing Board Identified
• Dr. Deborah L. Ainsworth, FAAP
• Mr. Charles. T. Frock, MHA
• Dr. Stephen Hsieh
• Mr. E. Benjamin Money, Jr., MPH
• Dr. Joe Ponzi
• Dr. Thomas R. White
• Dr. Kerry Willis

Panelists:
• Deborah L. Ainsworth, MD, FAAP – Chapter President, North Carolina Pediatric Society
• Charles T. Frock, MHA– Former Chief Executive Officer, FirstHealth of the Carolinas
• E. Benjamin Money, Jr., MPH– President and CEO, North Carolina Community Health Center
Association• Thomas R. White, MD
– President, North Carolina Academy of Family Physicians, Inc.
Moderator: Denise Levis Hewson, RN, BSN, MSPH
Senior Vice President of Network Development and State Programs, CCNC

North Carolina’s Community Health
CentersA Model of Patient Governed Integrated Health Care

Community Health Center Movement• Movement grew out of 1960s Civil Rights
Movement and War on Poverty in an effort to bring health services to impoverished inner-city and rural communities without access to care.
• First health centers established as pilots through the Office of Economic Opportunity in Boston, MA and Mound Bayou, MS in 1965.
• Movement based on community-oriented primary care, where community members accessed and shaped the services delivered by their health center.
• Health Center Program is now administered by the Bureau of Primary Health Care in the Health Resources and Services Administration.
12

Types of Health CentersGrant-Supported Federally Qualified Health Centers are public and private non-profit health care organizations that meet certain criteria under the Medicare and Medicaid Programs and receive funds under the Health Center Program (Section 330 of the Public Health Service Act).
• Community Health Centers serve a variety of underserved populations and areas.
• Migrant Health Centers serve migrant and seasonal agricultural workers.
• Healthcare for the Homeless Programs reach out to homeless individuals and families and provide primary care and substance abuse services.
• Public Housing Primary Care Programs serve residents of public housing and are located in or adjacent to the communities they serve.
13

Other Types of Health Centers
• Federally Qualified Health Center Look-Alikes are health centers that have been identified by HRSA and certified by the CMS as meeting the definition of “health center” under Section 330 of the PHS Act, although they do not receive grant funding under Section 330.
• Outpatient health programs/facilities operated by tribal organizations (under the Indian Self-Determination Act, P.L. 96-638) or urban Indian organizations (under the Indian Health Care Improvement Act, P.L. 94-437).
14

Health Center Program Fundamentals• Located in or serve a high need community identified as having elevated
poverty, higher than average infant mortality, and where few physicians practice.
• Governed by a community board composed of a majority (51% or more) of health center patients who represent the population served.
• Provide comprehensive primary health care services as well as enabling services (education, translation and transportation, etc.) that promote access to health care.
• Provide services to all with fees adjusted based on ability to pay.
• Meet other performance and accountability requirements regarding administrative, clinical, and financial operations.
15

Health Center Program Requirements
1. Demonstrate & document need
2. Provide all required services and additional services as necessary
3. Maintain core staff necessary for services provided
4. Provide accessible hours of operation/locations
5. Provide after-hours coverage
6. Have admitting privileges or other arrangement to ensure continuity of care
7. Implement sliding fee discounts
8. Have an ongoing Quality Improvement/Quality Assurance program
9. Maintain fully staffed management team
10. Exercise oversight and authority over all contracted services
11. Establish and maintain collaborative relationships with other providers
12. Maintain financial management and control policies
13. Implement systems to maximize collections and reimbursement
14. Develop a budget to align with service delivery plan
15. Have systems in place to collect and organize data for program reporting
16. Maintain funded scope of project
17. Governing board maintains appropriate authority to oversee operations
18. Maintain appropriate board composition
19. Enforce a strict conflict of interest policy
16

Community Health Centers are Health Care Homes
Health Center Required Services
• Comprehensive primary care
• Prenatal and perinatal services
• Family planning services
• Well child services
• Immunizations
• Cancer and other disease screening
• Screening for blood lead levels, communicable diseases and cholesterol
• Preventive dental services
• Diagnostic lab and radiological services
• Pharmacy
• Enabling services
• Eligibility workers
• Referrals
• Substance abuse and mental health services
• Emergency medical and dental services
• 24/7 access to care
17

FQHC Integrated Services

2013 NC Health Center Centers
FQHC Look-Alike
Site Funded in CY2013
19

35 Health Center Organizations 34 FQHCs 1 FQHC Look-Alike
1 Migrant Voucher Program 179 clinical service sites in 66 of 100 NC counties
North Carolina’s Health Centers
Serving nearly 470,000 North Carolinians through:
20

Goshen – Rosewood site

Blue Ridge Health Services

Roanoke Chowan Community Health Center – Ahoskie Comprehensive
Health Center

Snapshot of NC Health Center Staffing
24

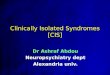
NC CHC Patients vs. State Population
Hispanic/Latino
African American
White
Private
Medicare
Uninsured
Medicaid
<200% FPL
<100% FPL
8%
22%
69%
51%
15%
17%
16%
42%
21%
29%
33%
44%
14%
13%
48%
25%
96%
52%
CHC NC
North Carolina’s Health Centers Serve the Most Vulnerable Populations
INCOME LEVEL
INSURANCESTATUS
RACE/ETHNICITY
NC CHC Patients
NC Pop.96% of NC CHC patients have incomes below 200% of the Federal Poverty Level (FPL)
Nearly 73% of NC health center patients have Medicaid or no insurance
NC Health Center patients are more racially/ethnically diverse than the overall state population
25

Uninsured48%
Medicaid 25%
Medicare13%
Private14%
2013 National data Versus nc data
Payer Mix:
26
Uninsured35%
Medicaid41%
Medicare8%
Other Public2%
Private14%

Considerations for FQHCs with ACO Design• In many cases, FQHCs serve multiple communities and their delivery sites cross
county and regional areas. • FQHCs depend upon hospital system and community partnerships in multiple
locales. • Delivery sites under the same FQHC umbrella fall in different ACO geographies.
FQHC tax ID numbers are the same for all providers regardless of delivery site, and some providers serve at multiple sites.
• Exclusivity puts health centers in violation of federal regulations*. FQHCs must be able to serve all Medicaid patients that present for care and Federal Section 330 funds cannot be used to underwrite Medicaid services
* Section 330 of the Public Health Service Act (42 USCS § 254b) Authorizing Legislation of the Health Center Program. 42 U.S.C § 254b(j)(3)(E-F)

Accountable Care Organizations Must Use Detailed Cost Data to Risk-Adjust the Patient Population
• FQHCs serve a greater share of medically complex patients and patients with social determinants (e.g., housing transportation, language and education) that negatively impact their health.
• Risk adjustments must take into account detailed patient cost data and social determinants of health factors to ensure the risk burden is accurately calculated.
• ACO risk expectations should be predicated upon the health risk of the population served because it is very difficult to achieve savings among the highest cost patient population.