Embed Size (px)
Citation preview

ARTICLE IN PRESS
0020-7489/$ - se
doi:10.1016/j.ijn
�CorrespondE-mail addr
International Journal of Nursing Studies 44 (2007) 377–385
www.elsevier.com/locate/ijnurstu
A comparative cross-sectional questionnaire survey of thework of UK and US mental health nurses
Peter Nolana,�, Sayeed Haqueb, Maureen Doranc
aSchool of Health and Sciences, Staffordshire University and South Staffordshire Healthcare Trust, Blackheath Lane,
Stafford, ST18 0AD, UKbDepartment of Psychiatry, University of Birmingham, UK
cAssociative Clinical Director, The Veterans’ Administration Medical Centre, Denver, Colorado, UK
Received 26 June 2005; received in revised form 24 April 2006; accepted 24 April 2006
Abstract
Background: Comparative inter-country research which identifies similarities and differences in the work of mental
health nurses in different social and political contexts is an important means of determining how changes in health care
systems could lead to better outcomes for patients.
Objective: This study sought to compare aspects of the work of nurses in US and UK mental health care settings.
Nurses were invited to reflect on aspects of their role including identifying the most and least satisfying elements of their
work and suggesting ways in which it could be improved.
Methods and participants: A 12-item questionnaire, comprising closed and open-ended questions, based on the
literature and the authors’ own experiences of mental health nursing practice, was piloted and subsequently distributed
to respondents in both countries.
Results: The US nurses tended to be more willing to accept a wider range of clients than their UK counterparts,
although they had lower expectations of their clients’ likelihood of recovery. Both groups of nurses felt that being part
of a team and having direct contact with clients were the most satisfying aspects of their work, while administration was
the least. Although both US and UK nurses utilised a variety of intervention models, it would appear that Cognitive
Behavioural Therapy was the favoured model for the majority of nurses.
Conclusions: The implications of these findings for the work of nurses and mental health care services in the UK and
US, and the purpose, nature and need for future international comparative research are discussed.
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Inter-country research; Cross-cultural exploration; Role of the nurse
What is already known about the topic?
�
The selection, preparation and work of mental healthnurses appear to vary considerably from country to
country.
�
Few comparative international studies focusing onthe work of mental health nurses exist.
e front matter r 2006 Elsevier Ltd. All rights reserve
urstu.2006.04.014
ing author. Tel.: +441785 353702.
ess: [email protected] (P. Nolan).
�
d.
More international studies are needed to compare the
contribution of nurses to alleviating the burden of
mental health problems.
What this paper adds
�
It contributes to our understanding of the work ofnurses in different countries.
ARTICLE IN PRESSP. Nolan et al. / International Journal of Nursing Studies 44 (2007) 377–385378
�
It defines which aspects of their work nurses findmost and least satisfying.
�
It explores nurses’ perceptions of the environmentaland cultural factors which influence how they
approach their work.
1. Introduction
Globalisation, defined as the decoupling of space and
time (Giddens, 2001), is now impacting on many aspects
of people’s lives including the manner in which health
care is provided. Instant communication enables knowl-
edge and culture to be shared around the world in
seconds and has implications not only for those with
responsibility for planning and financing services, but
also for those engaged in delivering them. Health care
programmes need to be responsive to global changes
and health care personnel will need to become compe-
tent in negotiation, analytical and strategic thinking
skills, and the assessment of national and cultural
differences (Spradley and Allender, 1997; Harris et al.,
2001). In mental health, increased sharing of knowledge
has enabled nurses in different parts of the world to
compare and contrast their work in diverse health care
systems and socio-political traditions (Verheis and
Kerkstra, 1993; Smoyak, 1996). Hull (1988) suggests
that cross-cultural exploration enables us to highlight
deficits in our own mental health care and Mead and
Ashcroft (2005) argue that international collaboration is
one of the principal ways of learning how nurses can
improve the work they do.
2. Literature review
Although there are few rigorous international com-
parative studies in mental health nursing, nevertheless
the number of such studies is increasing, resulting in a
clearer understanding of the nature of the work of
mental health nurses worldwide. As this review in-
dicates, studies have been largely researcher-initiated
and undertaken independent of each other. The first
scholarly work relating to the role and function of the
mental health nurse at the beginning of the 20th century
appeared in the United States (Nolan et al., 2002) and
by the middle of the century, literature from other
countries was following suit, seeking to find ways of
strengthening the contribution of the nurse to mental
health services (Callaway, 2002). During the 1950 s and
1960 s, some attention was given to mental health
nursing at professional meetings and international
conferences organised by psychiatrists. Although psy-
chiatrists had been making educational visits abroad
since the second half of the 19th century, it was not until
the 1950s that the first psychiatric nurses from the UK
went to Scandinavia to learn more about their profes-
sion in relation to the work being done in other
countries (Nolan, 1999). In the early 1960 s, Altschul
went to the States for a 1-year study tour and
subsequently wrote her seminal book Patient–Nurse
Interaction: a study of interactive patterns in acute
psychiatric wards, exploring how interpersonal relation-
ships assist recovery from mental illness (Altschul, 1972;
Tilley, 2004). Today, international educational ex-
changes and research collaboration flourish; case man-
agement, the Care Programme Approach, drop-in
centres, and nurse prescribing have all been heavily
influenced by observations made in other countries
(Simpson et al., 2003).
Smoyak (1996) recommended comparative research as
a means of testing the efficacy of nursing in different
contexts, and of defining the work that nurses do and
the conditions in which it yields the best outcomes. She
invited nurse–researchers to go beyond attending con-
ferences in other countries and to seek funding for
international studies, despite the reluctance of many
funding bodies to consider research of this nature.
Work already done in an international context has
proved thought-provoking. Barker (2000) reported that
clients in Canada and Scotland had similar expectations
of the nurse–client relationship, which they saw as
finding its natural context in the clinical situation.
Adejumo and Ehlers (2001), however, found that mental
health nursing was defined very differently in Botswana
and Nigeria, two countries which might have been
expected to have shared a similar understanding by
virtue of their proximity, although in both, the focus of
nursing was on caring for groups of people in their
everyday social contexts.
Bowers et al. (1999) explored the number and nature
of violent incidents in in-patient care in five European
countries. Considerable differences in the number and
nature of such incidents were found. However, the
researchers faced methodological difficulties owing to
there being no shared definition of violence across the
five countries, and no consensus on how to record such
incidents. These disparities provided some explanation
for the variations in incidence and nature, but could not
provide a full explanation. Other factors such as staffing
levels, the therapeutic skills of nurses, and the ways in
which potential conflict was handled were also con-
sidered by the authors to be significant and they called
for further studies to ascertain the true prevalence of
violence in mental health settings in Europe, its causes
and the role of nurses in containing and preventing it. In
a similar smaller study, Nolan et al. (2001) found that
mental health nurses in England encountered more
violence in the course of their work than colleagues in
Sweden, and reported that repeated exposure to violent
incidents eroded nurses’ self-esteem and job-satisfaction.

ARTICLE IN PRESSP. Nolan et al. / International Journal of Nursing Studies 44 (2007) 377–385 379
Swedish nurses experienced less violence and had greater
support, leading to enhanced professional morale.
Weiller et al. (1998) examined provision for patients
with anxiety syndromes and high levels of social
disability in five European countries. This study took
place in the context of European Union and World
Health Organisation directives that planners and provi-
ders should prioritise services for people with mental
health problems in primary care. The researchers
concluded that provision was generally poor; in two
countries, there were no services at all. The poverty of
primary care services meant that some patients would
require more expensive treatment following inevitable
deterioration. General Practitioners were found to need
more training in the management and treatment of
mentally ill people but the researchers considered that
this would be inadequate without a transformation in
the culture of primary care in order to improve mental
health services.
Yamashita (1998) examined the cultural context in
which care is provided, comparing the nature and level
of the involvement of family members in Canada and
Japan with their mentally ill relatives. Profound
differences in how care was described and operationa-
lised were found.
Walmsley’s (2000) study assessed how clients in the
US and Eire with severe and enduring mental illness
were managed using a ‘partial hospitalisation’ strategy.
Economic and cultural factors played a part in the
differences identified, but professional differences ex-
isted over and above these factors. Anders et al. (1999)
compared the care of patients held in secure environ-
ments in Hawaii and Japan, finding differences in the
quality of the working environment and hence in morale
and professional standards, and in the relevance of
policies which the nurses were required to implement.
The authors concluded that nursing practice quickly
regresses and becomes fragmented when the environ-
ment of care is inappropriate.
Lauri et al. (1999) compared nurses’ decision-making
processes in mental health settings in Finland, Northern
Ireland and the US. In Northern Ireland, nurses tended
to use an analytical approach to decision-making;
Finnish nurses combined analytical decision-making
with intuition, and nurses in the US manifested mainly
intuitive decision-making. The researchers could not
explain why this should be so although they hypothe-
sised that the nurses were influenced by factors beyond
the culture in which they worked. Wright and Smith
(1993) found significant differences between the work of
nurses in Australia and the US and attributed this
predominantly to personality differences rather than
environmental or cultural factors. Critically reviewing
comparative studies undertaken to date, Whyte et al.
(1997) suggested that nurses should consider methodol-
ogies that go beyond mere self-reporting by nurses and
instead embark on more rigorous observational studies
which examine what nurses actually do in different
countries.
It has been argued that the close political and
economic ties between the United States and the United
Kingdom mean that what happens in America may
foreshadow developments in health care in the UK
(Putnam, 2001). With this in mind, the present study
aimed to compare some aspects of the work of mental
health nurses in the UK and the US with the intention of
improving understanding of how mental health nursing
in this country may evolve, of avoiding pitfalls and
maximising opportunities.
3. Methodology
Four sites were identified for this study, two in the UK
(Staffordshire and Birmingham) and two in the US
(Kentucky and Denver), principally because of their
proximity to where the authors worked. An opportunistic
sample of respondents was invited to participate as long as
they satisfied the inclusion criteria which were being
appropriately qualified, currently employed in mental
health services, in post for at least 3 years and working
directly with mental health clients. All respondents
described their work as predominantly community-based,
although some in both groups stated that they had contact
with in-patient services, the extent of which was not
explored. Whereas the entire UK sample worked in the
National Health Service, the US nurses worked in three
healthcare systems, all funded and managed differently,
and influencing in their individual ways the type of patients
admitted, the interventions provided by nurses and the
length of time patients were in receipt of services. A
specially designed 12-item questionnaire, based on the
literature and the authors’ own experiences and under-
standing of mental health nursing practice, was piloted and
modified in both countries. The questionnaire comprised
closed and open-ended questions. The results of the pilot
study enabled some modifications to the language used on
the questionnaire to be made, to ensure that all the
questions could be immediately understood by both sets of
respondents. Permission to approach the respondents was
sought from the manger in each setting and each
respondent was given a full verbal explanation of the
study, and given the choice of participating or not. Data
collection took 2 days on each site with respondents
completing the questionnaire at a time convenient to them.
4. Analysis of data
The responses to open-ended questions were cate-
gorised by the researchers working first independently
and then comparing categories. As will be seen from the
ARTICLE IN PRESS
Table 1
Responses to the statements about the work of mental health
nurses
2
P. Nolan et al. / International Journal of Nursing Studies 44 (2007) 377–385380
Findings section, categories were generally easy to
establish and there was little or no disagreement between
the researchers. The w2 test was used to analyse some of
the data.
Statements w df p-ValueMost referrals from
primary care are
inappropriate
10.062 2 0.007 **
The role of
‘Keyworker’ is
understood by each
member of my team
3.119 2 0.210
Disagreement about
care interventions
rarely occurs when
colleagues in my team
are involved with the
same client
2.211 2 0.331
Being cost-effective is
another term for
rationing in mental
health care
0.121 2 0.941
I feel my role is
threatened when
mention is made of
primary care teams
assuming more
responsibility for the
delivery of mental
health services
1.753 2 0.416
There is ample time
for professional
development within
my work
8.890 2 0.012 *
I can refuse new
referrals if my
caseload exceeds an
agreed number
7.767 2 0.021 *
Patients with a
serious mental illness
should always be
discouraged from
stopping medication
5.939 2 0.051
Many staff hold low
expectations of
clients’ abilities to
recover
6.580 2 0.037 *
I feel that community
mental health nurses
are valued in my
organisation
9.335 2 0.009 **
Community mental
health nurses should
be able to prescribe
medication for their
patients
4.720 2 0.095
*Significant at 5% level; **Significant at 1% level.
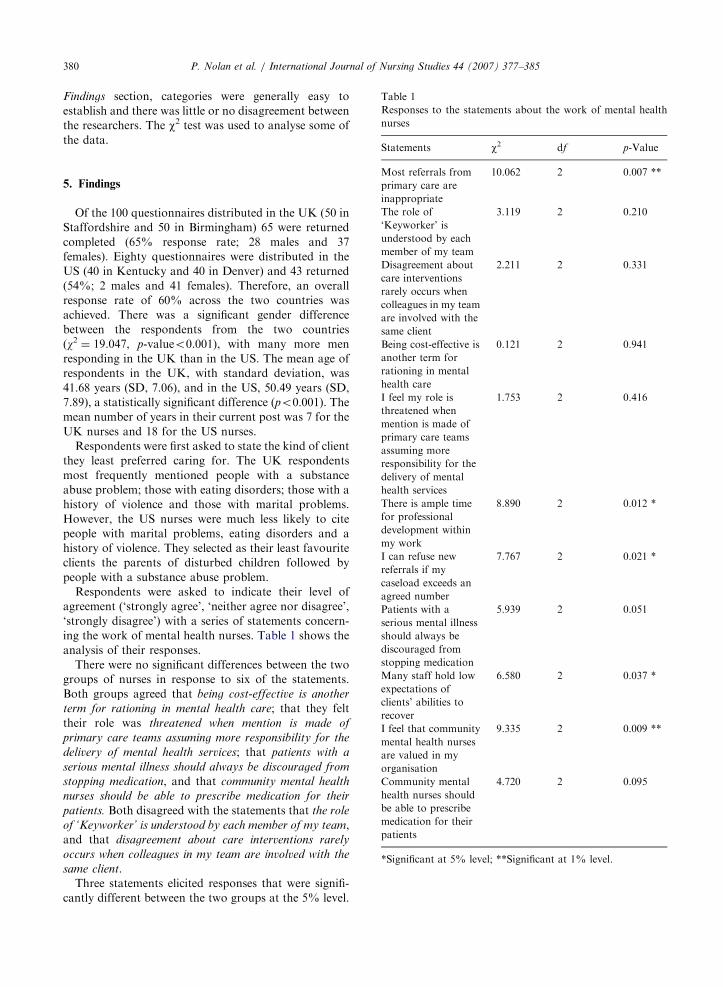
5. Findings
Of the 100 questionnaires distributed in the UK (50 in
Staffordshire and 50 in Birmingham) 65 were returned
completed (65% response rate; 28 males and 37
females). Eighty questionnaires were distributed in the
US (40 in Kentucky and 40 in Denver) and 43 returned
(54%; 2 males and 41 females). Therefore, an overall
response rate of 60% across the two countries was
achieved. There was a significant gender difference
between the respondents from the two countries
(w2 ¼ 19.047, p-valueo0.001), with many more men
responding in the UK than in the US. The mean age of
respondents in the UK, with standard deviation, was
41.68 years (SD, 7.06), and in the US, 50.49 years (SD,
7.89), a statistically significant difference (po0:001). Themean number of years in their current post was 7 for the
UK nurses and 18 for the US nurses.
Respondents were first asked to state the kind of client
they least preferred caring for. The UK respondents
most frequently mentioned people with a substance
abuse problem; those with eating disorders; those with a
history of violence and those with marital problems.
However, the US nurses were much less likely to cite
people with marital problems, eating disorders and a
history of violence. They selected as their least favourite
clients the parents of disturbed children followed by
people with a substance abuse problem.
Respondents were asked to indicate their level of
agreement (‘strongly agree’, ‘neither agree nor disagree’,
‘strongly disagree’) with a series of statements concern-
ing the work of mental health nurses. Table 1 shows the
analysis of their responses.
There were no significant differences between the two
groups of nurses in response to six of the statements.
Both groups agreed that being cost-effective is another
term for rationing in mental health care; that they felt
their role was threatened when mention is made of
primary care teams assuming more responsibility for the
delivery of mental health services; that patients with a
serious mental illness should always be discouraged from
stopping medication, and that community mental health
nurses should be able to prescribe medication for their
patients. Both disagreed with the statements that the role
of ‘Keyworker’ is understood by each member of my team,
and that disagreement about care interventions rarely
occurs when colleagues in my team are involved with the
same client.
Three statements elicited responses that were signifi-
cantly different between the two groups at the 5% level.

ARTICLE IN PRESSP. Nolan et al. / International Journal of Nursing Studies 44 (2007) 377–385 381
Significantly more US nurses disagreed with the state-
ment that most referrals from primary care are inap-
propriate; and significantly more US nurses agreed with
the fact that I can refuse new referrals if my caseload
exceeds an agreed number, and with the assertion that
there is ample time for professional development within
my work. Two statements elicited responses that were
significantly different between the two groups at the 1%
level. Significantly more US nurses felt that many staff
hold low expectations of clients’ ability to recover and
agreed with the statement that I feel that community
mental health nurses are valued in my organization.
Respondents were next requested to state what
aspects of their work gave them most satisfaction. This
question evoked a huge range of responses which were
categorised by the researchers working first indepen-
dently and then together in order to secure agreement.
Table 2 presents the categories in rank order:
For UK respondents, Client Contact meant ‘being
able to assist people’; ‘caring for the enduring mentally
ill in their homes’; ‘communicating with ethnic minority
families’ and ‘engaging with difficult clients’. Under
Using Clinical Skills, respondents mentioned ‘under-
taking assessments’; ‘care planning’; ‘having appropriate
time and skills’; ‘identifying appropriate treatment’ and
‘implementing evidence based practice’. Knowing I am
Doing a Good Job meant ‘seeing patients improve’;
‘having appreciative clients’; ‘helping patients regain
independence’ and ‘making a difference to individuals
and families’. Team Working comprised ‘feeling part of a
team’; ‘sharing ideas and problems and finding team
solutions’ and ‘working with a wide range of profes-
sionals’. The opportunity to mentor students and
improve their own skills as well as the skills of others
was the principal aspect enjoyed under the heading of
Teaching.
US nurses, on the other hand, interpreted Client
Contact as meaning ‘supporting individual clients’ and
‘leading therapy groups’. Using Clinical Skills meant
being involved in ‘crisis intervention’; ‘developing
Table 2
Aspects of your work that give most satisfaction (numbers
rounded to nearest whole figure)
UK respondents (n ¼ 65) US respondents (n ¼ 43)
Client contact 36 (55%) Client contact 25 (58%)
Using clinical
skills
22 (34%) Using clinical
skills
12 (28%)
Knowing I am
doing a good job
22 (34%) Teaching 10 (23%)
Team working 17 (26%) Receiving
positive feedback
7 (16%)
Teaching 7 (11%) Team working 4 (9%)
Personal growth 4 (9%)
patient care programmes’; ‘medication review’; ‘obser-
ving, treating and managing patients’ and ‘doing
psychotherapy’. Under the heading Teaching, respon-
dents mentioned most importantly, ‘being with stu-
dents’; ‘providing clinical supervision’; ‘mentoring and
developing staff’ and ‘teaching and educating patients’.
Two sub-themes emerged under the heading Receiving
Positive Feedback and these were ‘seeing people im-
prove’ and ‘being valued’. Team Working included
‘having support from colleagues’ and ‘working as a
member of a team’. Personal Growth meant having a job
that involved ‘intellectual stimulation’ and which
provided the opportunity for one’s own ‘personal,
spiritual and professional growth’.
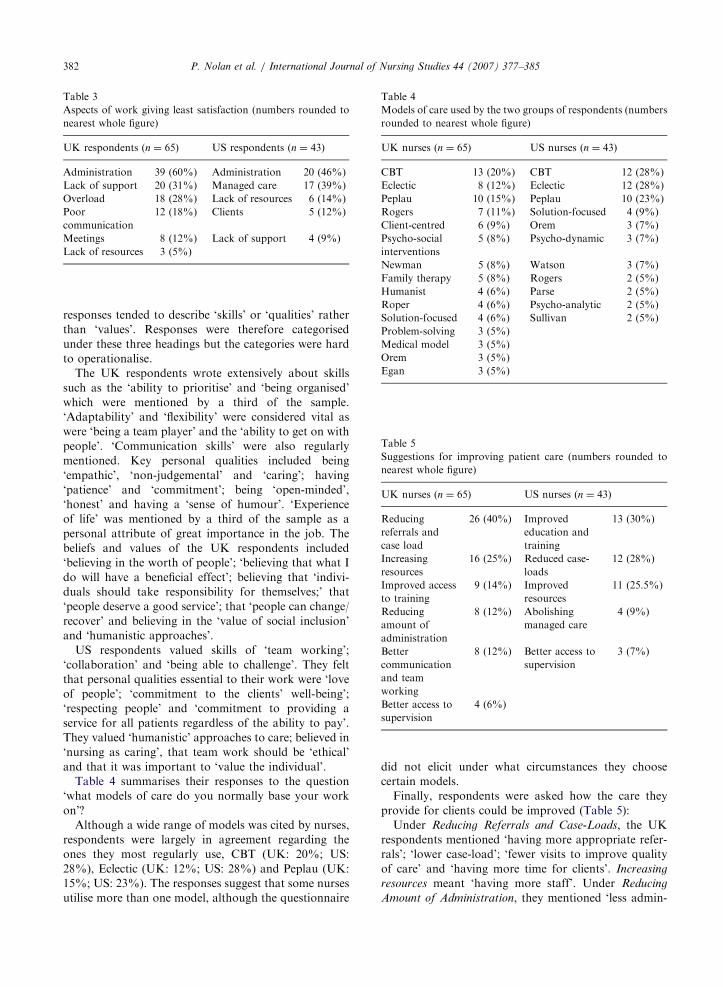
Table 3 provides a summary of respondents’ answers
to What aspects of your work give you least satisfaction?
Under Administration, the UK respondents men-
tioned ‘litigation administration’; ‘mindless paper work’;
‘non-clinical-related paperwork’; ‘pointless administra-
tion’ and ‘lack of admin support staff’. Lack of Support
meant ‘working with difficult staff’; ‘feeling alone’;
‘having work undervalued by other professionals’; ‘lack
of cooperation from other services’; ‘lack of managerial
support’ and ‘isolation’. Overload included comments
such as ‘being expected to know everything’; ‘caring
responsibilities for a large number of patients’; ‘having
too much to do’; ‘insufficient time for clients’; not
having time for one’s self’; ‘too much travelling’ and
‘pressure and stress’. The Poor Communication category
gathered together comments such as ‘assessing inap-
propriate referrals’; ‘un-thoughtful referrals’ and ‘dupli-
cation of information’. Meetings was a category of a
single word not considered to require further definition
by respondents. Lack of Resources was a general
complaint, including specifically for two individuals
‘lack of office space’ and ‘having to write notes in
longhand and then transfer them to a computer later’.
Under ‘Administration’, the US respondents men-
tioned ‘administration for insurance companies’ and
‘billing insurance companies’. Managed Care caused
distress owing to ‘arbitrary decisions made by manage-
ment’; ‘being audited by managed care companies’;
‘arguing for reimbursement’; ‘being controlled’ and
‘needing authorisation’. Clients led to dissatisfaction
when it was a case of ‘chronicity of the patient who does
not improve’; ‘families that want quick fixes’; ‘non-
respectful attitudes’ and ‘parents who will not get
involved’. Under ‘Lack of Support’, US respondents
mentioned ‘dealing with difficult staff’; ‘justifying the
work to the general public’ and ‘little support from
management’. When it was defined, Lack of Resources
meant ‘working with an insufficient budget’; ‘reducing
staff numbers’; ‘limited psychiatric resources’ and ‘lack
of time to treat effectively’.
Respondents were asked to identify the ‘personal
values that assist me most in my work’. Many of the
ARTICLE IN PRESS
Table 3
Aspects of work giving least satisfaction (numbers rounded to
nearest whole figure)
UK respondents (n ¼ 65) US respondents (n ¼ 43)
Administration 39 (60%) Administration 20 (46%)
Lack of support 20 (31%) Managed care 17 (39%)
Overload 18 (28%) Lack of resources 6 (14%)
Poor
communication
12 (18%) Clients 5 (12%)
Meetings 8 (12%) Lack of support 4 (9%)
Lack of resources 3 (5%)
Table 4
Models of care used by the two groups of respondents (numbers
rounded to nearest whole figure)
UK nurses (n ¼ 65) US nurses (n ¼ 43)
CBT 13 (20%) CBT 12 (28%)
Eclectic 8 (12%) Eclectic 12 (28%)
Peplau 10 (15%) Peplau 10 (23%)
Rogers 7 (11%) Solution-focused 4 (9%)
Client-centred 6 (9%) Orem 3 (7%)
Psycho-social
interventions
5 (8%) Psycho-dynamic 3 (7%)
Newman 5 (8%) Watson 3 (7%)
Family therapy 5 (8%) Rogers 2 (5%)
Humanist 4 (6%) Parse 2 (5%)
Roper 4 (6%) Psycho-analytic 2 (5%)
Solution-focused 4 (6%) Sullivan 2 (5%)
Problem-solving 3 (5%)
Medical model 3 (5%)
Orem 3 (5%)
Egan 3 (5%)
Table 5
Suggestions for improving patient care (numbers rounded to
nearest whole figure)
UK nurses (n ¼ 65) US nurses (n ¼ 43)
Reducing
referrals and
case load
26 (40%) Improved
education and
training
13 (30%)
Increasing
resources
16 (25%) Reduced case-
loads
12 (28%)
Improved access
to training
9 (14%) Improved
resources
11 (25.5%)
Reducing
amount of
administration
8 (12%) Abolishing
managed care
4 (9%)
Better
communication
and team
working
8 (12%) Better access to
supervision
3 (7%)
Better access to
supervision
4 (6%)
P. Nolan et al. / International Journal of Nursing Studies 44 (2007) 377–385382
responses tended to describe ‘skills’ or ‘qualities’ rather
than ‘values’. Responses were therefore categorised
under these three headings but the categories were hard
to operationalise.
The UK respondents wrote extensively about skills
such as the ‘ability to prioritise’ and ‘being organised’
which were mentioned by a third of the sample.
‘Adaptability’ and ‘flexibility’ were considered vital as
were ‘being a team player’ and the ‘ability to get on with
people’. ‘Communication skills’ were also regularly
mentioned. Key personal qualities included being
‘empathic’, ‘non-judgemental’ and ‘caring’; having
‘patience’ and ‘commitment’; being ‘open-minded’,
‘honest’ and having a ‘sense of humour’. ‘Experience
of life’ was mentioned by a third of the sample as a
personal attribute of great importance in the job. The
beliefs and values of the UK respondents included
‘believing in the worth of people’; ‘believing that what I
do will have a beneficial effect’; believing that ‘indivi-
duals should take responsibility for themselves;’ that
‘people deserve a good service’; that ‘people can change/
recover’ and believing in the ‘value of social inclusion’
and ‘humanistic approaches’.
US respondents valued skills of ‘team working’;
‘collaboration’ and ‘being able to challenge’. They felt
that personal qualities essential to their work were ‘love
of people’; ‘commitment to the clients’ well-being’;
‘respecting people’ and ‘commitment to providing a
service for all patients regardless of the ability to pay’.
They valued ‘humanistic’ approaches to care; believed in
‘nursing as caring’, that team work should be ‘ethical’
and that it was important to ‘value the individual’.
Table 4 summarises their responses to the question
‘what models of care do you normally base your work
on’?
Although a wide range of models was cited by nurses,
respondents were largely in agreement regarding the
ones they most regularly use, CBT (UK: 20%; US:
28%), Eclectic (UK: 12%; US: 28%) and Peplau (UK:
15%; US: 23%). The responses suggest that some nurses
utilise more than one model, although the questionnaire
did not elicit under what circumstances they choose
certain models.
Finally, respondents were asked how the care they
provide for clients could be improved (Table 5):
Under Reducing Referrals and Case-Loads, the UK
respondents mentioned ‘having more appropriate refer-
rals’; ‘lower case-load’; ‘fewer visits to improve quality
of care’ and ‘having more time for clients’. Increasing
resources meant ‘having more staff’. Under Reducing
Amount of Administration, they mentioned ‘less admin-

ARTICLE IN PRESSP. Nolan et al. / International Journal of Nursing Studies 44 (2007) 377–385 383
istration’ and ‘improved support’. Improved access to
training involved ‘attending courses on Brief Therapy’;
‘CBT training’; ‘having specific training in counselling’;
‘more access to training and education’; ‘more personal
development’ and ‘skills based training’. Better Commu-
nication and Team Working revolved around ‘better
liaison with primary care’; ‘better relationships with
consultants’; ‘better working with other professionals’;
‘better team organisation’ and ‘joint working with GPs
on difficult cases’. Better access to supervision also meant
more supervision.
For the US respondents, Reduced Case-loads would
mean ‘having more time for clients’. Improved education
and training necessitated ‘having access to professional
education’; ‘learning better ways for helping clients’;
‘more psycho-education programmes’ and ‘more perso-
nal development’. Under Improved Resources, respon-
dents mentioned wanting ‘more staff’; ‘more funding’;
‘more space’; ‘more time for admin’ and ‘providing time
for treatment team planning and meetings’. Abolishing
Managed Care was variously expressed as ‘less managed
care involvement’ and ‘less contact with insurance
companies’. Like their UK counterparts, the US nurses
wanted Better access to supervision and this also meant
more supervision.
6. Discussion
Any study exploring the work and attitudes of nurses
working in different countries, even two which share a
common language, and in very different health care
contexts, can be accused of attempting to make
comparisons where none are possible. However, this
study achieved a very high response rate which suggests
that the nurses in both the UK and the US felt that the
questions they were being asked were relevant to their
particular situations. Interpretation of their responses
has been undertaken with caution; yet the considerable
consensus in terms of the words and phrases used by
respondents and the ideas and concepts they put
forward make it possible to feel reasonably confident
about the conclusions drawn in this section.
An important limitation of the study is that very few
male US nurses (n ¼ 2) responded to the questionnaire.
At the time of data collection, only two men expressed
an interest in the study and satisfied the inclusion
criteria. Other males with a nursing background who
were interested in the study had to be ruled out because
of their management roles. It may be the case that males
felt less sympathetic than females towards a study
emanating from the UK, although there was no obvious
evidence of this. The small number of males means that
the comparisons between the two groups of nurses are
not as strong or perhaps as illuminating as they would
otherwise have been.
It needs also to be borne in mind that the nurses who
responded to the study were, in both countries, working
in large towns and cities which may involve them in
different kinds of work, and in facing different
challenges from those working in other settings.
While the small number of respondents must be taken
into account, it is interesting to note that the mean age
of respondents from the US was considerably higher
than in the UK, and that US nurses had also spent many
more years in their current post. This might suggest that
US nurses tend to stay in one post, while their UK
counterparts change jobs more regularly. If this
observation is accurate, it may reflect the diversity of
clients and experiences that US nurses working in
private practice can achieve compared to UK nurses
who may need to change their jobs regularly in order to
achieve the same breadth of experience. It would also
appear that US nurses are less likely to label certain
groups of clients as their ‘least favourite’, perhaps
because they are more confident in their skills to care
for diverse clients, or quite simply because the US
system of Managed Care obliges them to take whichever
clients present to them. UK nurses appeared either to be
anxious about or irritated by people who have substance
abuse problems, those with eating disorders and those
with a history of violence. This is worthy of further
investigation. Does this reluctance arise because nurses
find these clients unrewarding in terms of ‘cure’ rates, or
because they are fearful for their own safety in the case
of violent patients?
On both sides of the Atlantic, there appears to be
cynicism regarding the use of cost-effectiveness as a
euphemism for rationing in mental health care. One
might have expected that the US respondents would feel
positively about community mental health nurses being
able to prescribe as nurse prescribing has a long history
in the States; it is slightly more surprising that the notion
of prescribing is apparently already well-embedded in
the UK nursing mentality.
US mental health nurses appear to exercise greater
control over their work, attracting appropriate referrals
from primary care and being able to limit their case-
loads. They also seem better supported in terms of
professional developmental; all three of these issues
caused concern for UK nurses whose job descriptions
seem to leave them more open to caseload overload
without the buttressing of ongoing training.
Both groups of nurses found their major source of job
satisfaction in direct contact with clients and their major
source of job dissatisfaction in the administrative duties
which took them away from clients. Moves in the UK to
reduce paperwork for some public sector workers such
as police officers need urgently to be translated into the
health care sector to enable people to do the work
for which they originally entered the service and to
which they are presumably best suited. The US nurse

ARTICLE IN PRESSP. Nolan et al. / International Journal of Nursing Studies 44 (2007) 377–385384
respondents appeared to feel much more valued for the
work they were doing that than their UK colleagues.
Desire for recognition may be the reason why UK
nurses cited (perhaps somewhat wistfully?) one of the
components of job satisfaction as ‘knowing I am doing a
good job’, a comment which might hide a lack of such
acknowledgement from others. Future studies could
usefully explore what aspects of the work of US nurses
leads to their feeling more valued than UK nurses,
despite the manifold difficulties which they face working
within an insurance-driven healthcare system.
UK nurses defined the qualities and skills that helped
them in their work in relation to the difficulties they
perceived they faced as nurses. They considered organi-
sational skills important, presumably because these
assisted with a heavy workload, and the ability to work
well in a team, perhaps because they so often felt
undervalued by other team members. For their part, US
nurses valued skills and qualities which helped them in
the US health care context: being able to challenge a
system driven by money rather than by client need;
commitment to the client’s well-being which is perhaps
overlooked when insurance companies determine the
nature and level of care; and commitment to providing a
service regardless of the ability to pay, perhaps
indicating their sense of injustice when only the wealthy
have easy access to services. Thus health care profes-
sionals value qualities that enable them to cope with the
job they have to do in the place they have to do it, over
and above generic qualities which might apply to all
healthcare work. This is despite the fact that both
groups of nurses were using the same models of care.
The request for more training came from both groups
and probably reflects the perceived difficulties of work-
ing with clients with complex and multiple pathologies
when resources do not allow nurses to give the time they
feel individual clients require. The request for more
training may be closely linked to complaints about lack
of support which surfaced in other areas of the
questionnaire. Training needs can never perhaps be
ultimately satisfied, but where nurses feel that their work
is undervalued, and that they are often asked to do work
which they do not see as their principal role, the demand
for more training is likely to emerge as a compensatory
mechanism.
There may be many explanations for why UK nurses
express unease about dealing with violent or potentially
violent patients, and US nurses do not. Speculative
reasons may include inadequate training of UK nurses
in how to defuse potentially violent situations and in
how to handle them should they occur. Media coverage
of adverse incidents where patients were incorrectly
restrained may have fuelled anxiety on the part of UK
nurses generally. UK nurses may feel that support from
medical and management staff is lacking if incidents
occur and that they will shoulder the blame while other
staff groups cover their own backs. In the US, the
situation may be different. Insurance companies may
filter out highly challenging patients, who could prove
costly in terms of the time, human and material
resources they require. It may be that the training of
US nurses in handling violent events is superior to that
of their UK counterparts. The responses of UK and US
nurses to violent patients is an area of difference which is
one of considerable interest and deserves further
research attention.
7. Conclusion
This study confirms the work of Weiller et al. (1998),
Yamashita (1998) and Nolan et al. (2001), in relation to
similarities and differences in the work of mental health
nurses. However, the present study moves a little further
in exploring the key question as to the influence that
different organisational cultures may have on how
individual nurses and teams of nurses construct their
role. Seeking to account for these differences and to
project how changes in the nursing culture in any
particular country might affect outcomes for patients
must now be the focus of research (Wright and Smith
(1993). In terms of helping focus the needs of UK mental
health nurses by contrasting them with those of
colleagues in the US, this study supports Smoyak’s
(1996) claim that there is much to be gained from
comparative studies and the analyses they promote.
References
Adejumo, O., Ehlers, V., 2001. Models of psychiatric nursing
education in developing African countries: a comparative
study of Botswana and Nigeria. Journal of Advanced
Nursing 36, 215–228.
Anders, R., Kawano, M., Mori, C., Kokusho, H., Tomai, J.,
1999. Cross-cultural comparison of long-term psychiatric
patients hospitalised in Tokyo, Japan, Honolulu and
Hawaii. Nursing and Health Sciences 1, 35–44.
Altschul, A., 1972. Patient–Nurse Interaction: A study of
Interactive Patterns in Acute Psychiatric Wards. Churchill
Livingstone, Edinburgh.
Barker, P., 2000. Clients’ reflections on relationships with
nurses: comparisons from Canada and Scotland. Journal of
Psychiatric and Mental Health Nursing 8, 45–51.
Bowers, L., Whittington, R., Almyik, R., Bergman, B., Oud,
N., Savio, M., 1999. A European perspective on psychiatric
nursing and violent incidents: management, education and
service organization. International Journal of Nursing
Studies 36, 217–222.
Callaway, B.J., 2002. Hildegard Peplau—Psychiatric Nurse of
the Century. Springer, New York.
Giddens, A., 2001. Sociology, fourth ed. Polity Press, Cam-
bridge.

ARTICLE IN PRESSP. Nolan et al. / International Journal of Nursing Studies 44 (2007) 377–385 385
Harris, H., Brewster, C., Sparrow, P., 2001. Globalisation and
HR. Chartered Institute of Personnel and Development
(CIPD), London.
Hull, D.L., 1988. Science as a Process. The University of
Chicago Press, Chicago and London.
Lauri, S., Salanterae, S., Gilje, F., Klose, P., 1999. Decision
making of psychiatric nurses in Finland, Northern Ireland
and the United States. Journal of Professional Nursing 15,
275–280.
Mead, G., Ashcroft, J., 2005. The Case for Inter-Professional
Collaboration. Blackwell, Oxford.
Nolan, P., 1999. Community psychiatric nursing. In: Freeman,
H. (Ed.), A Century of Psychiatry. Mosby-Wolfe, London,
pp. 332–333.
Nolan, P., Soares, J., Dallender, J., Thomsen, S., Arnetz, B.,
2001. A comparative study of the experiences of violence of
English and Swedish mental health nurses. International
Journal of Nursing Studies 38, 419–426.
Nolan, P., Bourke, P., Doran, M., 2002. UK and US clinical
mental health nurse specialists’ perceptions of their work.
Journal of Psychiatric and Mental Health Nursing 9,
293–300.
Putnam, R., 2001. Bowling Alone. Simon and Schuster, New
York.
Simpson, A., Miller, C., Bowers, L., 2003. The history of the
Care Programme Approach in England: Where did it come
from? Journal of Mental Health 12, 489–504.
Smoyak, S., 1996. International net-worker: a network for
psychiatric and mental health nurses around the world.
Nursing Times 92, 93.
Spradley, B.W., Allender, J.A., 1997. Readings in Community
Health Nursing. Lippincott, New York.
Tilley, S., 2004. Re-Reading Altschul: A Festschrift. Hypatia
Trust, Penzance.
Verheis, R.A., Kerkstra, A., 1993. International comparative
study of community nursing. Journal of Advanced Nursing
18, 1852–1853.
Walmsley, P., 2000. Partial to holistic care. Nursing Times 96,
38–39.
Weiller, E., Bisserbe, J., Maier, W., Lecrubier, Y., 1998.
Prevalence and recognition of anxiety syndromes in five
European primary care settings. British Journal of Psychia-
try 173, 18–23.
Whyte, C., Motyka, M., Motyka, H., Wsolak, R., 1997. Polish
and British nurses responses to patient need. Nursing
Standard 38, 43–47.
Wright, C., Smith, J., 1993. Personality profiles of nurses: a
comparison between Australia and US research findings.
Australian Journal of Advanced Nursing 10, 10–19.
Yamashita, M., 1998. Family coping with mental illness: a
comparative study. Journal of Psychiatric and Mental
Health Nursing 5, 515–523.





























