Embed Size (px)
Citation preview

1
A comparison of denture base retention and adaptation between CAD-CAM and
conventional fabrication techniques
Mahmoud Amin Faty*
B.D.S, (2009), M.D.S (2016) Ain Shams University
Assistant lecturer, Oral and Maxillofacial Prosthodontics department, Faculty of Dentistry, Ain Shams
University, Cairo, Egypt.
Prof. Dr. Marwa Ezzat Sabet
B.D.S, (1994), M.D.S (1999), P.H.D (2002)
Chairman of Oral and Maxillofacial Prosthodontics Department, Faculty of Dentistry, Ain Shams
University, Cairo, Egypt.
Dr. Yasmine Galaleldin Thabet
B.D.S, (2002), M.D.S (2009), P.H.D (2013)
Associate Professor, Oral and Maxillofacial Prosthodontics department, Faculty of Dentistry, Ain Shams
University, Cairo, Egypt.
Corresponding author: Mahmoud Amin Faty
Address : 130 El Tawfik city, Nasr city, Cairo, Egypt.
Telephone : (+20) 1221402018
(+20) 22629419
Email address : [email protected]
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

2
Submitted June 7, 2020; accepted February 16, 2021
Purpose: To assess the retention and adaptation of milled and printed denture bases and to compare
them to conventional ones. Materials and Methods: A total of 24 completely edentulous patients were
selected. For each patient, three maxillary denture bases were constructed. Three groups were defined
according to fabrication technique: group I = denture bases were constructed by a conventional
technique; group II = denture bases were milled from prepolymerized blocks of polymethyl
methacrylate; and group III = denture bases were fabricated by a 3D printing technique. A digital force
gauge was used for measuring the retention of the denture bases intraorally, while Geomagic Control X
64 software was used to evaluate the adaptation of the denture bases with their corresponding master
casts. Analysis of variance for repeated measures was used for comparison among the groups, followed
by pairwise comparison with Bonferroni correction as a post hoc test. The significance level was set at α
= .05. Results: Statistical analysis showed significant differences among the three groups regarding
retention and adaptation. The highest values of retention and adaptation of denture bases were found in
group II (milling group). Conclusion: Within the limitations of this study, the following could be
concuded: milled denture bases demonstrated better retention and adaptation than the conventional heat-
polymerized and the printed denture bases; and printed denture bases showed better adaptation but
similar retention to conventional heat-polymerized denture bases. Int J Prosthodont 2021. doi:
10.11607/ijp.7193
Introduction
Well adapted denture bases are a prerequisite for attaining adequate retention and stability of
complete dentures. Several techniques have been introduced for the construction of complete denture
bases. The ultimate goal of each technique is to find balance between biocompatibility, esthetics,
minimal distortion and adaptation. (1, 2)
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.
3
The conventional protocol for the construction of complete dentures involves several processing
techniques that have been introduced and efficiently used since 1936.(3) However, it involves a sequence
of multiple clinical and laboratory steps that are time consuming. The polymerization shrinkage of poly-
methyl methacrylate (PMMA) and the difficulty to create a duplicate denture are considered as
drawbacks of this protocol. (3)
A recent protocol for the construction of complete dentures has been proposed utilizing
CAD/CAM (computer-aided design and computer-aided manufacturing) technology. CAD/CAM implies
the use of computers to aid in designing, and manufacturing of products. It includes additive and
subtractive manufacturing techniques. (4) In additive manufacturing, 3-dimensional (3D) printing, images
from a digital file are used to create an object by laying down successive layers of a liquid or powder
material which are then solidified upon exposure to UV light (photopolymerization) or LASER (selective
LASER sintering or selective LASER melting). On the other hand, in subtractive manufacturing, images
from the file are used to create an object by milling to physically remove material from a pre-fabricated
block to achieve the desired geometry. (4)
CAD/CAM technology has been widely used in the field of Prosthodontics. However, few
studies have reported its use for fabrication of complete dentures.(5-8)This can be attributed to themultiple
steps required for the construction of complete dentures. In addition to the difficulty in acquiring digital
impressions due to the flexibility of the oral mucosa. The saliva on the smooth soft tissues and the
dynamic movements of the vestibules may also influence the quality of digital impressions.(9, 10)
Moreover, digitalization of the maxillo-mandibular relationship record is still not reliable due to the
unavoidable movement of the record bases which adversely affects the results. (11)
Construction of complete dentures using CAD/CAM is characterized by ease of fabrication with
reduced laboratory procedures. It also leads to higher dimensional accuracy and standardized fabrication.
(9, 12-14)
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

4
Digital design ensures consistent thickness of denture bases which can be adjusted and kept
minimal for patient comfort. In addition, the presence of digital data enables future fabrication of
dentures in case of lost or damaged ones. (15)
Goodacre et al (17)compared the accuracy and reproducibility of milled denture bases with
conventionally fabricated bases where the milled denture bases attained better results. While Hwang et al
(16) evaluated the trueness and adaptation of milled, printed and conventional denture bases and reported
that the printed bases attained the best results. Yet further clinical research is required to evaluate the
different qualities of CAD/CAM dentures. The purpose of this study was to assess the retention and
adaptation of milled and printed denture bases and to compare them with conventional heat polymerized
denture bases. The first null hypothesis was that no difference would be found in the retention of the
denture bases fabricated by the three techniques. The second null hypothesis was that no difference
would be found among the three fabrication techniques in the tissue surface adaptation of the denture
bases to the edentulous maxillary casts.
Materials and methods
Participants:
Twenty four male patients with an age range from 55 to 65 years were selected from the outpatient clinic
of the Removable Prosthodontics Department, Faculty of Dentistry, Ain Shams University to participate
in this study. Detailed information about the study was given to all participants who signed a written
consent for approval.
Patients were selected to have the following inclusion criteria: completely edentulous maxillary and
mandibular well-formed ridges with a firm and healthy covering muco-periostium. Patients were selected
with minimal bony or soft tissue undercuts, adequate salivary flow with moderate consistency and Angle
class I maxillo-mandibular relationship
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

5
Patients having the following criteria were excluded: severely resorbed maxillary ridge, torus palatinus
and V shaped palatal vault. Also, patients with neuromuscular and Tempromandibular joint disorders,
limited mouth opening and allergy to acrylic resin were excluded.
The protocol of the research was approved by the ethical committee of the Faculty of Dentistry, Ain
Shams university on 20/9/2017 (no. of approval: FDASU – REC D 091722). There were no conflicts of
interest in thisstudy.
For each patient three maxillary denture bases were constructed. Thus three groups were defined
according to the technique of construction of the denture base. Group I: Denture bases were constructed
by the conventional (compression molding) technique using heat polymerizing resin. Group II: Denture
bases were digitally designed and milled from prepolymerized blocks of PMMA. Group III: Denture
bases were digitally designed and fabricated by rapid prototyping (3D printing) technique. Denture bases
in group II and III were constructed using the scanned data of the definitive casts.
Designing and printing of denture bases were performed in the Digital center of the Removable
Prosthodontics department, Faculty of Dentistry, Ain Shams University, Egypt.
Construction of the denture bases:
Primary impressions were taken in properly selected and modified stock trays using alginate impression
material(Cavex alginate, Cavex, Holland) and then poured in dental stone to obtain diagnostic casts.
Custom trays were fabricated over the diagnostic casts using autopolymerizing acrylic resin (Acrostone
cold cure denture base material, Acrostone, Egypt). The borders of the tray were trimmed 2-3 mm shorter
than the depth of the vestibule.
Border moulding was done using putty consistency addition silicone impression material (Elite HD+
Putty Soft – Zhermack) and the final wash impression was made using medium consistency
polyether impression material (Impregum Soft Medium Body – 3M ESPE, United States) (Fig. 1).
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

6
Definitive impressions were boxed then poured to obtain definitive casts (Gypsano Lab Dental Stone
(Type 3), Gypsano, UAE).
The geometrical center of the maxillary arch was determined on the cast before the beginning of the
scanning and designing processes. The midline of the maxillary cast was drawn from the center of the
incisive papilla to a point in the middle of a line drawn between the two hamular notches. Then a
midpoint was marked on the midline to represent the center of the arch.(18, 19) Arbitrary scrapping of the
posterior palatal seal area was done on the definitive cast extending through both hamular notches and
across the palate between the anterior and posterior vibrating lines prior to construction of denture bases.
The borders of the denture bases were then drawn on the casts following the depth of the vestibule. (Fig.
2).
In group I, a 2mm layer base plate wax (Cavex Set Up Regular, Modelling wax, Cavex, Holland) was
adapted and trimmed on the definitive cast. A sphere of wax was added to the outer surface of the waxed
up denture base in the position of the center of the arch which is marked on the cast and visible through
the wax (Fig. 3).
The denture base was then processed following the long curing cycle (74°C for 8 hours). Then the
polished surface of the denture base was finished using fine sandpaper fixed to mandrill and polished
using brushes and pumice (excessive heat generation was avoided) (Fig 4).
The 3Shape D850 desktop scanner (D850, 3Shape, Copenhagen, Denmark) and 3Shape dental system
software (3shape dental designer, 3Shape A/S, Copenhagen, Denmark) were used to scan the casts and
design the denture bases for groups II and III . The scanning and designing steps were followed
according to the protocol of the software. The borders of the denture bases were traced following the
depth of the vestibule of the virtual casts guided by the borders previously drawn on the definitive casts.
The denture bases were set to be 2 mm in thickness and with no relief space with their corresponding
virtual casts. A pin attachment was placed on the outer surface of the maxillary denture base to mark the
geometrical center of the arch (fig. 5).
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

7
In group II, pink pre-polymerized polymethyl methacrylate of 98 mm diameter and 25 mm height
(Glorious dental materials, Shandong, China) were used to fabricate the milled denture bases using a 5-
axis milling machine (ARUM 5X-200, Doowon, Daejeon, Korea). The denture bases were retrieved from
the block by cutting the supporting arms using carbide discs, and then the outer surface was finished and
polished as outlined in group I (Fig. 6).
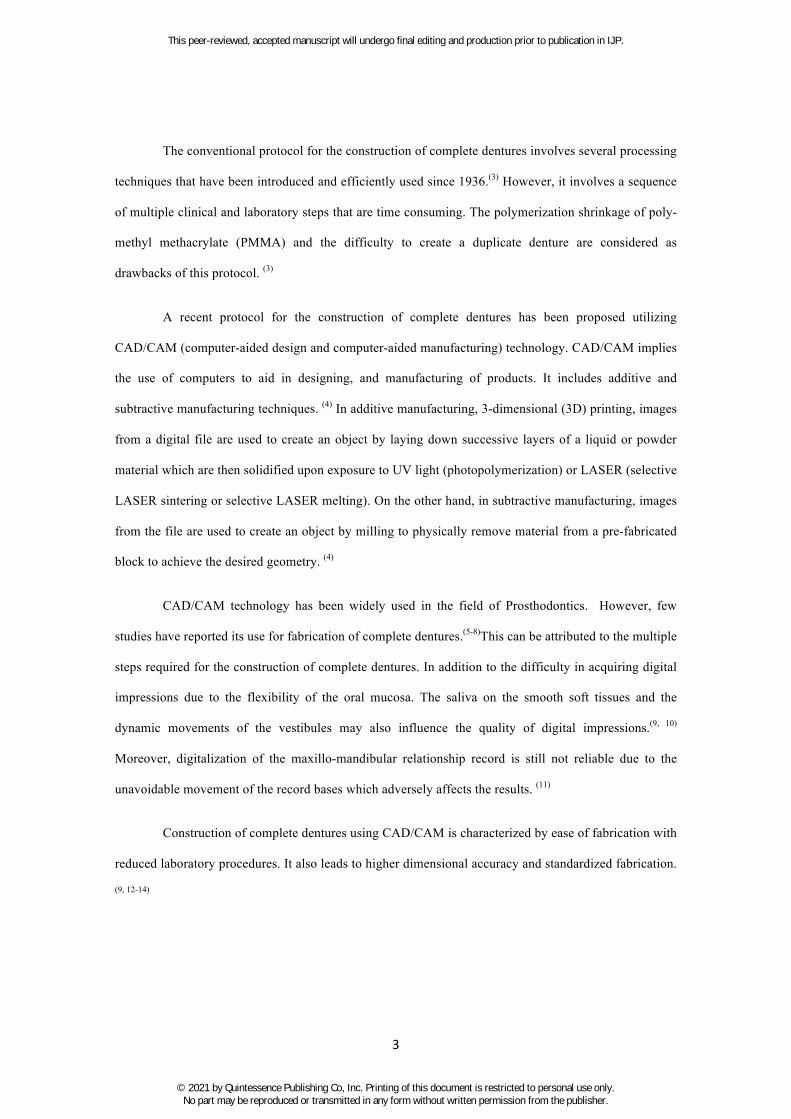
In group III, the STL file of the denture base was imported to the Netfab software to create the
supporting arms generating a new STL file of the denture base with its supporting arms (Fig. 7). The 3d
printing machine (MOGASSAM Dent2 3D Printer, Mogassam, Egypt) was loaded with pink denture
base printing resin (NextDent Base, NextDent, Soesterberg, Netherlands) to fabricate the printed denture
bases. After the printing process was completed, the denture bases were separated from the platform of
the machine and rinsed twice in a 96% ethanol solution in an ultrasonic bath. A first rinse of 3 minutes
was followed by a second rinse in clean 96% ethanol solution for approximately 2 minutes. Finally the
denture bases were dried, then placed in an ultraviolet light box (MOGASSAM Dentcure, Mogassam,
Egypt) for 20 minutes for additional polymerization. The light box delivers a wavelength of blue UV-A
315 to 400 nm and an output of 43.2 kJ. The outer surface of the denture base was finished and polished
in the same manner as group I and II.
All denture bases were immersed in water for 24 hours before the evaluation of retention and
adaptation.(20)
Evaluation of the retention of the denture bases:
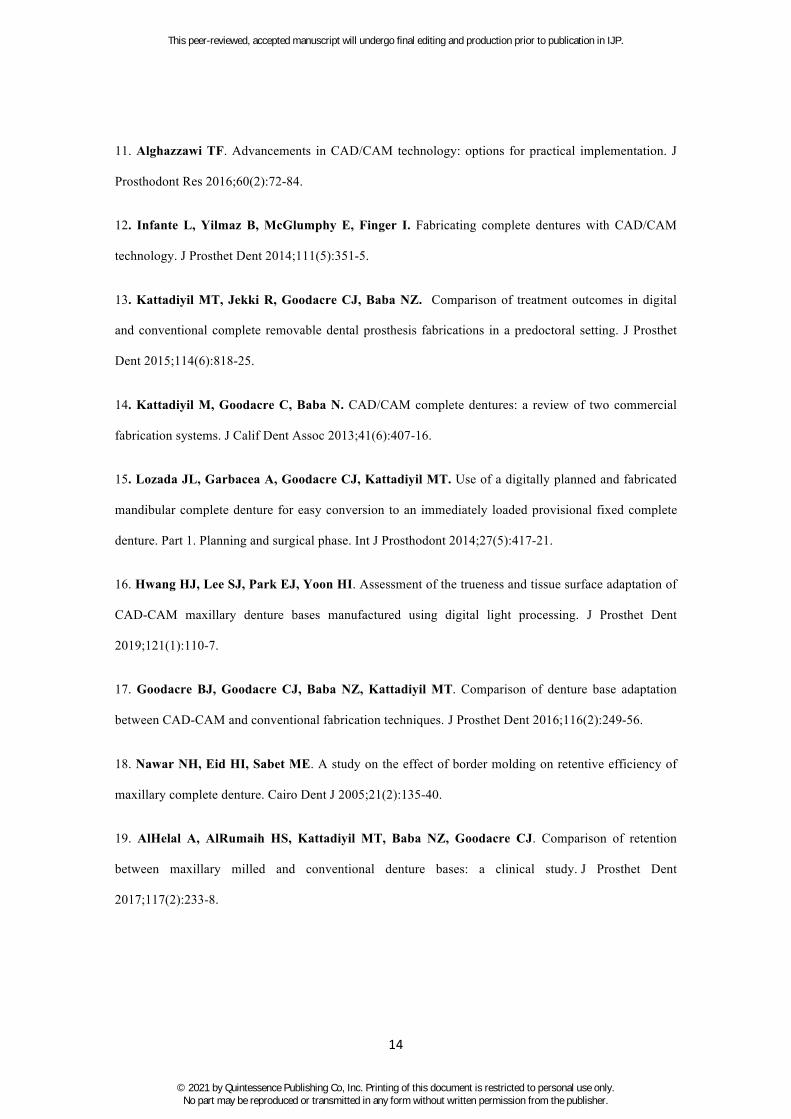
A metallic ring was attached to the outer surface of the denture bases at the position of the geometric
center by autopolymerizing acrylic resin (Acrostone cold cure denture base material, Acrostone, Egypt)
(Fig. 8). A digital force gauge (HF-100 Digital Force Gauge, Jinan Hensgrand Instrumentation Co., Ltd.,
Jinan, China) was used to record the retention of the denture bases. The device has a capacity of 100N,
Min unit is 0.1 N and its accuracy is 0.5%. The display before each measurement was adjusted to zero
via the zero button.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

8
The denture base was inserted in the patient’s mouth and allowed to remain for 5 minutes to ensure its
adaptation before the metallic ring was engaged and dislodging load was applied. )19(
The patient was seated in an upright position in the dental chair with the mouth half opened and lips
relaxed. The patient was instructed to tilt the head backward till the palate and the maxillary ridge were
at nearly 45 degrees to the floor so the applied dislodging force wasnearlyperpendicular to the denture
base. The metallic ring was engaged by the force gauge and a dislodging force was applied to the
denture base until it was forced out of its position (Fig. 9). Retention force was considered as the
maximum force needed to dislodge the denture. The measurement procedures were repeated 5 times at 5
minutes intervals for each denture base and the average value was recorded. All measurements were
performed by the same operator. (19)
Evaluation of adaptation of the denture bases:
All denture bases were lightly coated with antiglare spray (Okklu-Exact, Germany) before their fitting
surfaces were scanned using a 3shape desktop scanner, outputting an STL file which was imported to the
(Meshmixer software) to flip the fitting surface of the denture base (Fig. 10). The STL file of the fitting
surface of the denture base was superimposed on the STL file of the corresponding definitive cast by
using surface matching software (Geomagic Control X 64 software) using the best fit alignment option.
The 3D compare option was used to evaluate the adaptation of the measured data.
The adaptation of the denture base to the cast was presented in the form of a color scale where yellow to
red colors indicated impingement of denture base on the cast. The blue color indicated space between the
denture base and the cast and the green color indicated contact between the denture base and the cast.
It was also presented in the form of numerical values. The negative values indicated gap areas, while the
positive values indicated pressure areas between the denture base and the cast. In addition the average
value of the overall deviation of the denture base from the cast was provided (Fig. 11).
The mean values and standard deviation of the measured data were statistically analyzed by statistical
software (IBM® SPSS® Statistics Version 25). ANOVA for repeated measures was used for comparison
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

9
between the groups followed by pairwise comparison with Bonferroni correction as a post hoc test. The
significance level was set at α =0.05.
Results
A - Retention of the denture bases
Statistical analysis using ANOVA for repeated measures showed a statistically significant difference
between the three groups (Pp= 0.018), where the highest retentive value was found in group II and the
least retentive value was found in group I. However by using Bonferroni test, it showed that there is a
statistically significant difference only between group II and group I (p= 0.035) as shown in tables I and
II.
B - Adaptation of the denture bases
i- Negative average values (gap areas)
Statistical analysis showed significant difference between the three groups (p <0.001) , where the greatest
gap distance was found in group III then group I and the smallest gap distance was found with group II
as shown in table III. The post hoc test showed a statistically significant difference (p <0.001) between
all groups as shown in table IV.
ii- Positive average values (pressure areas)
.StatisticalanalysisdemonstratedthatthelargestpressurewasfoundingroupIII,followedbygroupI,
whilethesmallestpressurewasfoundingroupII(P=0.004)(TableV).
However the post hoc test showed that there is a statistically significant difference only between group
III and group II (p=0.004) (Table VI).
iii- Average values
( p<0.001).
Statistical analysis demonstrated the best adaptation was found in group II, followed by group III, while
the least adaptation was found in group I (p<0.001) (Table VII).
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

10
Discussion
The results of this study suggested that the milled denture bases had significantly higher
retentive force values than conventional denture bases. Hence, the first null hypothesis was rejected.
Moreover, statistically significant differences were found in the adaptation of the denture bases
fabricated by the three techniques, thus the second null hypothesis was also rejected.
Adaptation of the denture bases to the denture bearing tissues is essential for adequate retention,
stability and support of complete dentures. Minimal distortion in processing is mandatory for attaining
adequate mucosal adaptation. Distortion of denture bases during processing is affected by the thickness
and the material of the denture base as well as the processing technique. (2, 21)
In this study the selected patients had healthy and firm muco-periosteum without any signs of
inflammation or flabby tissues which could affect denture base stability and consequently result in false
records during testing the retentive quality of the denture bases. (18) The geometrical center of the arch
was selected to measure the retention of the denture bases as it has been reported as the most reliable
region for measuring the retention of maxillary complete dentures. (18, 19)
The exact geometrical center of the denture base could be accurately determined during the
designing process; however, it was difficult to transfer this position to the conventional denture base.
Consequently, the center of the arch was determined on the definitive cast manually before scanning and
was later transferred to the denture bases for standardization.
In group II, milling was processed by subtraction of an industrially pre-polymerized PMMA
block that has a final dimension. Consequently, dimensional deformation resulting from the
polymerization process was avoided. (20) A five axis dry milling machine was used due to its ability to
produce very complex geometries and smooth external surfaces. Dry milling was used for the purpose of
simplifying the process as it is quicker and has reduced cutting forces, increased tool life and potentially
better surface quality. (22)
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

11
In group III, the Netfab software was used to design and create the supporting system of the
denture bases. The denture bases were oriented in a position directing the contact with the supporting
arms at the polished surface to preserve the accuracy of the fitting surface and to avoid affecting the
results of the adaptation of the denture bases. The location and the number of the supporting arms were
automatically designed by the software.
Denture bases were immersed in water for 24 hours before making the measurements so as to
represent the ultimate base fit obtained after a patient wears a denture and it becomes completely
hydrated.(2, 23, 24) All bases have been tested on the same patients and the same casts, so potential variables
were eliminated.
Previous studies that evaluated the adaptation of denture bases relied on physical measurements
(25-28). In this study, surface matching and best-fit algorithms were used to adapt the denture bases and the
casts as closely as possible then digital measurements were recorded.
The Geomagic software was used to assess the adaptation of the denture bases and it created
color maps that revealed the varying degrees of adaptation produced by the three processing techniques.
While no processing technique produced a color map that was entirely green (which indicates intimate
contact between the denture base and the cast), it was evident that group II had the most uniform
adaptation of the denture base to the cast, and statistical analysis of the digital measurements confirmed
this finding. Since denture base retention depends on multiple factors including adaptation, dimensional
changes and accuracy of construction technique, thus group II attained the highest values.
Manufacturing the denture bases from pre-polymerized PMMA blocks avoids dimensional
changes and porosities caused by packing of the material as well as the polymerization process.(21, 29)
Thus, theoretically there was no dimensional deformation of the denture bases, which can explain the
high values of retention and adaptation attained by group II.
In the 3D printing technique, unpolymerized resins were utilized for manufacturing the denture
bases, and once processed; it required an additional final light-polymerization step to complete the
process. During the 3D printing workflow, polymerization shrinkage is theoretically possible, as the
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

12
denture bases are not completely polymerized before the final light-polymerization procedure. The
deformation can also occur while demounting the partially polymerized denture base from the building
platform. (29)
Despite the higher values of adaptation attained in group II than group III found in the present
study, the milling technique has several disadvantages. Milling units are expensive and mainly suitable
for commercial manufacturing centers. They may not be practical for individual practices or smaller
dental laboratories. Furthermore, these units consume a considerable amount of energy during the
manufacturing process and lead to a considerable amount of material wastage.(29)
In the conventional heat polymerized fabrication technique, factors such as the complexity of
manipulation, time-consuming procedures of waxing up, investing, and wax elimination as well as the
deformation of heat polymerized PMMA might diminish the degree of base adaptation.(2, 21, 30)
Evaluation of the retention of the denture bases was entirely based on the values obtained by the
digital force gauge.
The results of this study support previous studies(13, 19) that showed the superior retentive values
of milled denture bases, which is most likely because of the lack of polymerization shrinkage associated
with the milled denture bases resulting in an improved fit, thereby improved retention. However, further
research is required to assess the different qualities of complete dentures fabricated by CAD/CAM
techniques to verify the superiority of one of them.
Conclusion
Based on the findings of this study the following could be concluded:
• Milled denture bases demonstrated better retention and adaptation than the conventional heat
polymerized and the printed denture bases.
• Printed denture bases showed better adaptation but similar retention to conventional heat
polymerized denture bases.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

13
References
1. Takamata T, Setcos JC. Resin denture bases: review of accuracy and methods of polymerization. Int
J Prosthodont 1989;2(6):555-62.
2. Sykora O, Sutow EJ. Posterior palatal seal adaptation: influence of processing technique, palate
shape and immersion. J Oral Rehabil 1993;20(1):19-31.
3. Christensen GJ. Removable prosthodontics: a forgotten part of dentistry. The Alpha Omegan.
2006;99(1):26-8.
4. Saponaro PC, Yilmaz B, Heshmati RH, McGlumphy EA. Clinical performance of CAD-CAM-
fabricated complete dentures: a cross-sectional study. J Prosthet Dent 2016;116(3):431-5.
5. Miyazaki T, Hotta Y, Kunii J, Kuriyama S, Tamaki Y. A review of dental CAD/CAM: current
status and future perspectives from 20 years of experience. Dent Mater J 2009;28(1):44-56.
6. Maeda Y, Minoura M, Tsutsumi S, Okada M, Nokubi T. A CAD/CAM system for removable
denture. Part I: Fabrication of complete dentures. Int J Prosthodont 1994;7(1):17-21.
7. Busch M, Kordass B. Concept and development of a computerized positioning of prosthetic teeth for
complete dentures. Int J Comput Dent 2006;9(2):113-20.
8. Sun Y, Lü P, Wang Y. Study on CAD&RP for removable complete denture . Comput Meth Prog Bio
2009;93(3):266-72.
9. Goodacre CJ, Garbacea A, Naylor WP, Daher T, Marchack CB, Lowry J. CAD/CAM fabricated
complete dentures: concepts and clinical methods of obtaining required morphological data. J Prosthet
Dent 2012;107(1):34-46.
10. Patzelt SB, Vonau S, Stampf S, Att W. Assessing the feasibility and accuracy of digitizing
edentulous jaws. J Am Dent Assoc 2013;144(8):914-20.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.
14
11. Alghazzawi TF. Advancements in CAD/CAM technology: options for practical implementation. J
Prosthodont Res 2016;60(2):72-84.
12. Infante L, Yilmaz B, McGlumphy E, Finger I. Fabricating complete dentures with CAD/CAM
technology. J Prosthet Dent 2014;111(5):351-5.
13. Kattadiyil MT, Jekki R, Goodacre CJ, Baba NZ. Comparison of treatment outcomes in digital
and conventional complete removable dental prosthesis fabrications in a predoctoral setting. J Prosthet
Dent 2015;114(6):818-25.
14. Kattadiyil M, Goodacre C, Baba N. CAD/CAM complete dentures: a review of two commercial
fabrication systems. J Calif Dent Assoc 2013;41(6):407-16.
15. Lozada JL, Garbacea A, Goodacre CJ, Kattadiyil MT. Use of a digitally planned and fabricated
mandibular complete denture for easy conversion to an immediately loaded provisional fixed complete
denture. Part 1. Planning and surgical phase. Int J Prosthodont 2014;27(5):417-21.
16. Hwang HJ, Lee SJ, Park EJ, Yoon HI. Assessment of the trueness and tissue surface adaptation of
CAD-CAM maxillary denture bases manufactured using digital light processing. J Prosthet Dent
2019;121(1):110-7.
17. Goodacre BJ, Goodacre CJ, Baba NZ, Kattadiyil MT. Comparison of denture base adaptation
between CAD-CAM and conventional fabrication techniques. J Prosthet Dent 2016;116(2):249-56.
18. Nawar NH, Eid HI, Sabet ME. A study on the effect of border molding on retentive efficiency of
maxillary complete denture. Cairo Dent J 2005;21(2):135-40.
19. AlHelal A, AlRumaih HS, Kattadiyil MT, Baba NZ, Goodacre CJ. Comparison of retention
between maxillary milled and conventional denture bases: a clinical study. J Prosthet Dent
2017;117(2):233-8.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

15
20. Lee S, Hong S-J, Paek J, Pae A, Kwon K-R, Noh K. Comparing accuracy of denture bases
fabricated by injection molding, CAD/CAM milling, and rapid prototyping method. J Adv Prosthodont
2019;11(1):55-64.
21 Artopoulos A, Juszczyk AS, Rodriguez JM, Clark RK, Radford DR. Three-dimensional
processing deformation of three denture base materials. J Prosthet Dent 2013;110(6):481-7.
22. Kanazawa M, Inokoshi M, Minakuchi S, Ohbayashi N. Trial of a CAD/CAM system for
fabricating complete dentures. Dent Mater J 2011;30(1):93-6.
23. Woelfel JB, Paffenbarger GC, Sweeney WT. Changes in dentures during storage in water and in
service. J Am Dent Assoc 1961;62(6):643-57.
24. Komiyama O, Kawara M. Stress relaxation of heat-activated acrylic denture base resin in the mold
after processing. J Prosthet Dent 1998;79(2):175-81.
25. Consani RLX, Mesquita MF, de Arruda Nobilo MA, Henriques GE. Influence of simulated
microwave disinfection on complete denture base adaptation using different flask closure methods. J
Prosthet Dent 2007;97(3):173-8.
26. Ganzarolli S, Rached R, Garcia R, Del Bel Cury AA. Effect of cooling procedure on final denture
base adaptation. J Oral Rehabil 2002;29(8):787-90.
27. Lee CJ, Bok SB, Bae JY, Lee HH. Comparative adaptation accuracy of acrylic denture bases
evaluated by two different methods. Dent Mater J 2010;29(4):411-7.
28. Sartori EA, Schmidt CB, Walber LF, Shinkai RS. Effect of microwave disinfection on denture
base adaptation and resin surface roughness. Braz Dent J 2006;17(3):195-200.
29. Kalberer N, Mehl A, Schimmel M, Müller F, Srinivasan M. CAD-CAM milled versus rapidly
prototyped (3D-printed) complete dentures: An in vitro evaluation of trueness. J Prosthet Dent
2019;121(4):637-43.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

16
30. Yeung K, Chow T, Clark RK. Temperature and dimensional changes in the two-stage processing
technique for complete dentures. J Dent 1995;23(4):245-53.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

17
Figures
Figure 1 Maxillary secondary impression.
Figure 2 The geometric center marked on the definitive cast.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

18
Figure 3 Sphere of wax added to the geometric center of the waxed up denture base.
Figure 4 Heat polymerized denture base after processing.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

19
Figure 5 Placement of the attachment at the center of the arch.
Figure 6 Denture base after milling.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.
20
Figure 7 STL file of the denture base with the supporting arms.
Figure 8 Metallic ring attached to the geometrical center of the denture base.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

21
Figure 9 Evaluation of the retention of the denture bases.
Figure 10 STL file of the flipped fitting surface of the denture base.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

22
Figure 11 Geomagic control report.
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

23
Table1Mean,standarddeviationandpvalueofANOVAforrepeatedmeasurestestoftheretentivevaluesofthe
threegroups.
Group I Group II
Group III
Minimum 41.4 47.8 42.8
Maximum 67.8 73.4 68.8
Mean 54.2208 60.9063 58.9475
+/-S.D. 8.84045 8.17038 9.18263
P value 0.018
Table2Pairwisecomparisonbetweentheretentivevaluesofthethreegroups.
(I) factor1
Mean Difference
(I-J) Std. Error Sig.b
95% Confidence Interval for Difference
Lower Bound
Upper Bound
Group IGroup II -6.685* 2.444 0.035 -12.995 -0.376
Group III -4.727 2.100 0.103 -10.149 0.696
Group II Group I 6.685* 2.444 0.035 0.376 12.995
Group III 1.959 2.404 1.000 -4.249 8.166
Group IIIGroup I 4.727 2.100 0.103 -0.696 10.149
Group II -1.959 2.404 1.000 -8.166 4.249
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

24
Table3Mean,standarddeviationandpvalueofANOVAforrepeatedmeasurestestofthenegativeaveragevalues
oftheadaptation(gapareas)ofthethreegroups.
Group I Group II
Group III
Minimum 0.05 0.03 0.08
Maximum 0.11 0.07 0.16
Mean .0804 .0542 .1161
+/-S.D. .01437 .00941 .02141
P value <0.001
Table4Pairwisecomparisonbetweenthenegativeaveragevaluesoftheadaptation(gapareas)ofthethree
groups.
(I) factor1
Mean Difference
(I-J) Std. Error Sig.b
95% Confidence Interval for Difference
Lower Bound
Upper Bound
Group IGroup II .026* 0.004 0.000 0.017 0.036
Group III -.036* 0.005 0.000 -0.050 -0.022
Group II Group I -.026* 0.004 0.000 -0.036 -0.017
Group III -.062* 0.005 0.000 -0.075 -0.049
Group IIIGroup I .036* 0.005 0.000 0.022 0.050
Group II .062* 0.005 0.000 0.049 0.075
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

25
Table5Mean,standarddeviationandpvalueofANOVAforrepeatedmeasurestestofthepositiveaveragevalues
oftheadaptation(pressureareas)ofthethreegroups.
Group I Group II
Group III
Minimum 0.07 0.08 0.11
Maximum 0.18 0.16 0.23
Mean .1348ab .1259b .1505a
+/-S.D. .02639 .02484 .02571
P value 0.004
Table6Pairwisecomparisonbetweenthepositiveaveragevaluesoftheadaptation(pressureareas)ofthethree
groups.
(I) factor1
Mean Difference
(I-J) Std. Error Sig.b
95% Confidence Interval for Difference
Lower Bound
Upper Bound
Group IGroup II 0.009 0.007 0.719 -0.010 0.028
Group III -0.016 0.007 0.107 -0.034 0.002
Group II Group I -0.009 0.007 0.719 -0.028 0.010
Group III -.025* 0.007 0.004 -0.042 -0.007
Group IIIGroup I 0.016 0.007 0.107 -0.002 0.034
Group II .025* 0.007 0.004 0.007 0.042
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.

26
Table7Mean,standarddeviationandpvalueofANOVAforrepeatedmeasurestestoftheaveragevaluesofthe
adaptationofthethreegroups.
Group I Group II
Group III
Minimum 0.03 0.00 0.03
Maximum 0.06 0.01 0.05
Mean .0443 .0039 .0393
+/-S.D. .00784 .00071 .00773
P value <0.001
Table8Pairwisecomparisonbetweentheaveragevaluesoftheadaptation(3Dcomparison)ofthethreegroups.
(I) factor1
Mean Difference
(I-J) Std. Error Sig.b
95% Confidence Interval for Difference
Lower Bound
Upper Bound
Group IGroup II .040* 0.002 0.000 0.036 0.044
Group III .005* 0.002 0.029 0.000 0.010
Group II Group I -.040* 0.002 0.000 -0.044 -0.036
Group III -.035* 0.002 0.000 -0.039 -0.031
Group IIIGroup I -.005* 0.002 0.029 -0.010 0.000
Group II .035* 0.002 0.000 0.031 0.039
This peer-reviewed, accepted manuscript will undergo final editing and production prior to publication in IJP.
© 2021 by Quintessence Publishing Co, Inc. Printing of this document is restricted to personal use only. No part may be reproduced or transmitted in any form without written permission from the publisher.