Embed Size (px)
Citation preview
ONLINE ONLY
A comparison of miniplates and teeth fororthodontic anchorageSoojin Kim,a Susan Herring,b I-Chung Wang,c Rafael Alcalde,d Victor Mak,e Isaac Fu,f and Greg Huangg
Seoul, Korea, Seattle, Wash, Fort Meyers, Fla, and Vancouver, British Columbia, Canada
Introduction: In this study, we investigated orthodontic space closure of premolar extraction sites withminiplate anchorage compared with conventional tooth-borne anchorage in 8 adult beagle dogs. Methods:A split-mouth design with all 4 quadrants was used. Four premolars were extracted to create adequate spacefor premolar retraction. Retraction was performed with nickel-titanium coil springs. In the control side, thepremolars were retracted against other teeth, and, in the experimental side, the premolars were retractedagainst miniplates. Each quadrant received 2 additional bone screws as bone markers for cephalometricsuperimposition. Lateral cephalograms were taken at initial activation, 6 weeks, and 12 weeks. Threeparameters were measured and evaluated: linear space closure, angular tipping, and amount of anchorageslippage. Results: Overall, the miniplates had a high success rate of 93.8% (15 of 16) during the 12-weekperiod of orthodontic loading. Similar amounts of space closure were observed in the control and theexperimental sites. A statistically significant difference was observed for the amounts of tipping andanchorage slippage of miniplates vs tooth-borne anchorage. In the maxilla, the mean miniplate tipping was0.1°, whereas mean tipping of the anchor teeth was 9° (P � .01). In the mandible, the miniplates tipped anaverage of 3.4°, whereas the mean tipping of the anchor teeth was 13.3° (P � .02). In the maxilla, theminiplates had 1% anchorage loss, whereas the tooth anchors had 37.1% anchorage loss (P � .001). In themandible, the miniplates had a mean anchorage loss of 4.5%, whereas the tooth anchors had a meananchorage loss of 31.1% (P � .001). Conclusions: Although the total amount of space closure was similarin both the control and the experimental groups, the mechanism of space closure was different. In the controlgroup, slippage of the anchor teeth accounted for approximately a third of the space closure. In theexperimental group, the miniplates had minimal movement, and space closure was achieved almost entirelyby movement of the target teeth. These results confirm that miniplates provide virtually absolute anchorage.
(Am J Orthod Dentofacial Orthop 2008;133:189.e1-189.e9)The use of conventional osseointegrated implantsfor orthodontic anchorage has been well docu-mented in the literature,1-5 but they have limi-
tations when used for this purpose—eg, their large size,the need to carefully plan implant location,6 and thepotential difficulty of removal after treatment.
In 1997, Kanomi7 reported the usage of mini-implants for orthodontic anchorage. Since this casereport, there has been an explosion of additional reportsof mini-implants for orthodontic anchorage.8-11 Mini-implants have been used for many situations: open
aOrthodontist, US Army, Seoul, Korea.bProfessor, Department of Orthodontics, University of Washington, Seattle.cClinical associate professor, Department of Periodontics, University of Wash-ington, Seattle.dOral surgeon, private practice, Fort Meyers, Fla.ePeriodontist, private practice, Vancouver, British Columbia, Canada.fOrthodontist, private practice, Seattle, Wash.gAssociate professor, Department of Orthodontics, University of Washington,Seattle.Reprint requests to: Soojin Kim, 618th Dental Company (AS) Unit #15652,Dental Clinic #3, APO, AP. 96205-0652; e-mail, [email protected], February 2007; revised and accepted, July 2007.0889-5406/$34.00Copyright © 2008 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2007.07.016bites, intrusion of supererupted molars, molar uprighting,and retraction of anterior teeth after extraction for bimax-illary protrusion. Miniplates were introduced to offerabsolute orthodontic anchorage a year after the introduc-tion of miniscrews. In 1999, Unemori et al12 reported onthe use of miniplates to intrude the posterior segment tocorrect anterior open bites. Now, there are many optionsfor nontooth-borne anchorage, such as retromolar im-plants,1 mini-implants,7 miniplates,12 onplants,13 palatalimplants,14,15 and miniscrews.16 These additional proce-dures are changing the way we practice orthodontics.
It has been claimed that miniplates offer absoluteanchorage, and that treatment is effective. However, nonedirectly compared the effectiveness of miniplates to tooth-borne anchorage for unilateral space closure. The aim ofthis study was to compare miniplates with conventionaltooth-borne anchorage for orthodontic space closure ofpremolar extraction sites in adult beagle dogs.
MATERIAL AND METHODS
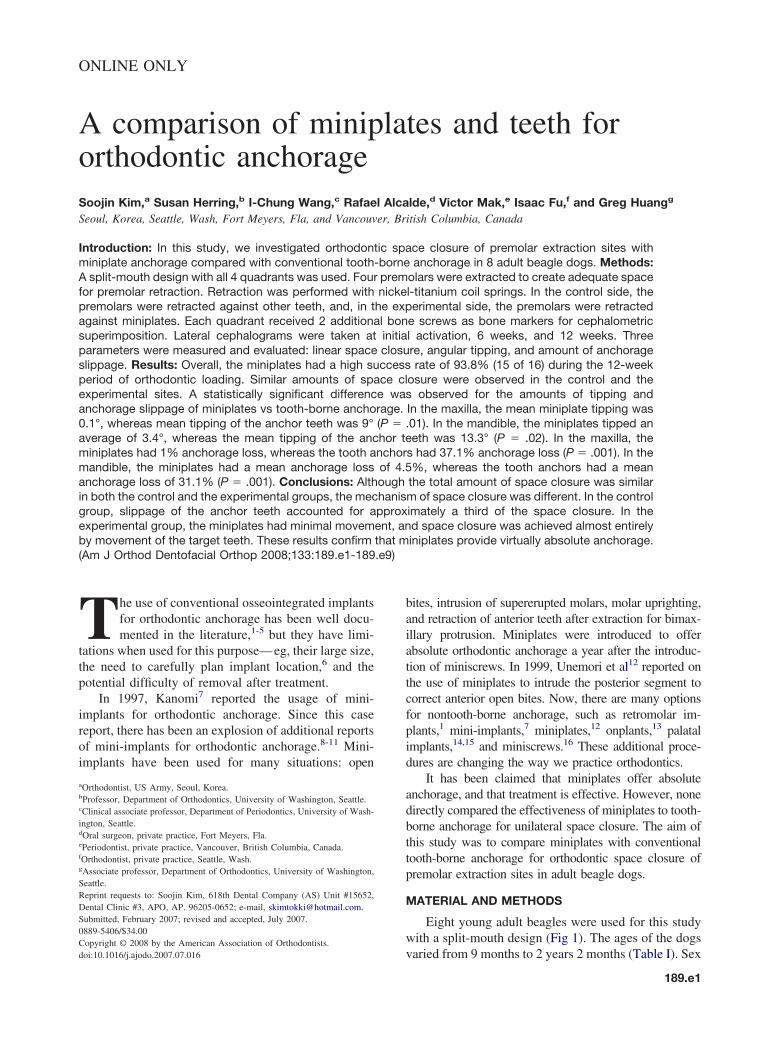
Eight young adult beagles were used for this studywith a split-mouth design (Fig 1). The ages of the dogs
varied from 9 months to 2 years 2 months (Table I). Sex189.e1
American Journal of Orthodontics and Dentofacial OrthopedicsFebruary 2008
189.e2 Kim et al
was distributed equally, with 4 male and 4 female dogs.The weight of the dogs varied from 5.9 to 10.2 kg atinitial activation (T0). In each dog, the initial maxillaryimplant site was randomly assigned. The contralateralmandibular quadrant was then assigned as the implantside, and the 2 remaining quadrants were assigned totooth-borne anchorage. Thus, all 4 quadrants were used.In each quadrant, 2 unloaded bone screws were placed(mesial to the maxillary first premolar or the mandibularsecond premolar, and distal to the anchor tooth orminiplate) as bone markers for superimposition. Theywere also used to compare the survival of loaded vsunloaded miniscrews. The experimental protocol wasapproved by the animal care committee of the Universityof Washington, Seattle.
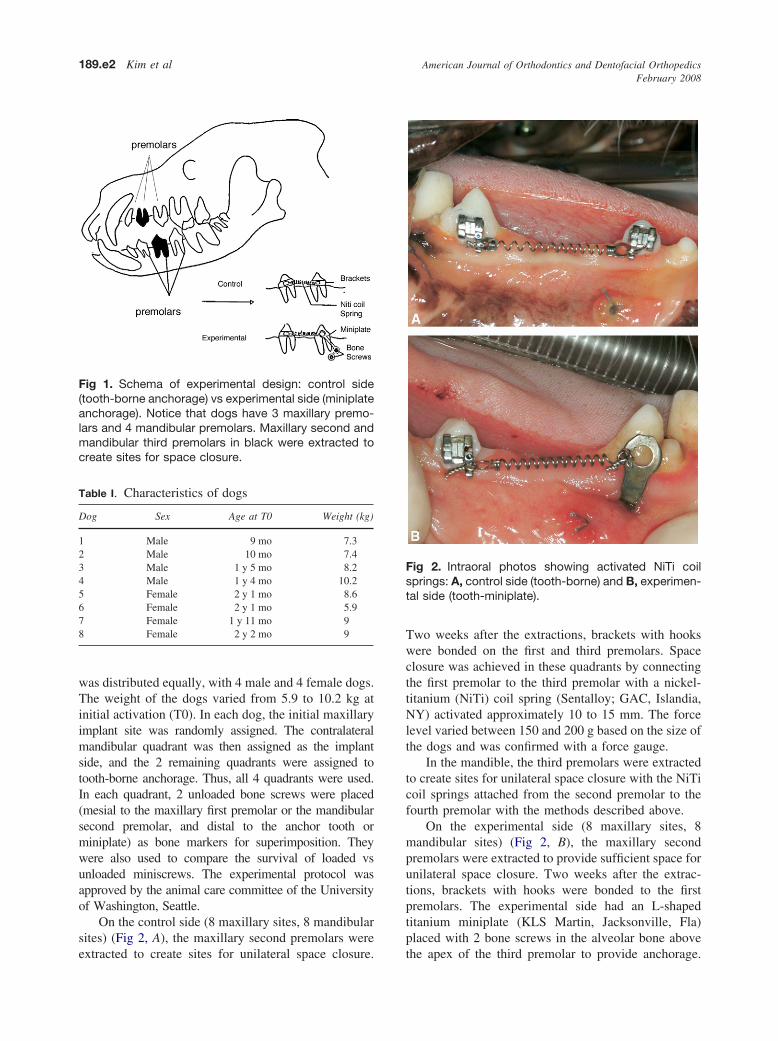
On the control side (8 maxillary sites, 8 mandibularsites) (Fig 2, A), the maxillary second premolars were
Fig 1. Schema of experimental design: control side(tooth-borne anchorage) vs experimental side (miniplateanchorage). Notice that dogs have 3 maxillary premo-lars and 4 mandibular premolars. Maxillary second andmandibular third premolars in black were extracted tocreate sites for space closure.
Table I. Characteristics of dogs
Dog Sex Age at T0 Weight (kg)
1 Male 9 mo 7.32 Male 10 mo 7.43 Male 1 y 5 mo 8.24 Male 1 y 4 mo 10.25 Female 2 y 1 mo 8.66 Female 2 y 1 mo 5.97 Female 1 y 11 mo 98 Female 2 y 2 mo 9
extracted to create sites for unilateral space closure.
Two weeks after the extractions, brackets with hookswere bonded on the first and third premolars. Spaceclosure was achieved in these quadrants by connectingthe first premolar to the third premolar with a nickel-titanium (NiTi) coil spring (Sentalloy; GAC, Islandia,NY) activated approximately 10 to 15 mm. The forcelevel varied between 150 and 200 g based on the size ofthe dogs and was confirmed with a force gauge.
In the mandible, the third premolars were extractedto create sites for unilateral space closure with the NiTicoil springs attached from the second premolar to thefourth premolar with the methods described above.
On the experimental side (8 maxillary sites, 8mandibular sites) (Fig 2, B), the maxillary secondpremolars were extracted to provide sufficient space forunilateral space closure. Two weeks after the extrac-tions, brackets with hooks were bonded to the firstpremolars. The experimental side had an L-shapedtitanium miniplate (KLS Martin, Jacksonville, Fla)placed with 2 bone screws in the alveolar bone above
Fig 2. Intraoral photos showing activated NiTi coilsprings: A, control side (tooth-borne) and B, experimen-tal side (tooth-miniplate).
the apex of the third premolar to provide anchorage.

American Journal of Orthodontics and Dentofacial OrthopedicsVolume 133, Number 2
Kim et al 189.e3
Space closure was achieved by connecting the firstpremolar to the miniplate with a NiTi coil spring. Thesame force level was used as the control side.
In the mandible, the third premolars were extractedto provide sufficient space for unilateral space closure.The experimental side had a L-shaped titaniumminiplate placed with 2 bone screws in the alveolarbone below the apex of the fourth premolar to provideanchorage. Space closure was achieved by connectingthe second premolar to the miniplate with a NiTi coilspring with the same force as the control side.
The miniplate served as a hook for the applicationof orthodontic force. The plate on the experimental sidewas positioned to match the position of the brackets onthe control side buccolingually and mesiodistally.
Two lateral cephalograms for each dog (1 from eachside) were taken at T0, 6 weeks postactivation (T6), and12 weeks postactivation (T12) with the same x-ray ma-chine (Innovet LX 125V; Summit Industries, Chicago, Ill)with the same technique each time (KVP 64, time setting1/30 s at 100 mA). Radiographic exposures were madevertically from a fixed focal film distance of 36 in with25.4 � 30.5 cm general purpose x-ray film (KonicaMinolta, Wayne, NJ). The dogs’ heads were obliquelypositioned directly on the x-ray cassette to preventoverlap of bilateral structures. Once the lateral cepha-lograms were developed, the films were checked foraccurate positioning by superimposing bone markerson the previous films. In only a few instances did thelateral cephalograms need to be repeated to ensureaccurate superimposition. All lateral cephalogramswere taken by a technician who was trained during ourpilot study to optimize reproducibility. Left and rightstructures could be easily distinguished, because eachdog had a miniplate on 1 side in the maxilla and aminiplate on the contralateral side in the mandible. Tominimize distortion and magnification errors, onlystructures on the side closest to the film were measuredon each cephalogram.
The dogs were acclimatized for at least a weekunder experimental conditions, including housing inindividual runs, a diet of ground and soft laboratorychow, water ad libitum, and a 12-hour light/dark cycle(Table II). After implant placement, the dogs wereplaced on a soft diet, and instructions were given toexclude toys or food treats that were hard or chewy.
On surgery day, weights were recorded, and anes-thesia was obtained by using injections of atropine(0.06 mg/kg SQ), acepromazine (0.05 mg/kg SQ),isoflurane (1-3%), ketamine (5.5 mg/kg IV), and diaza-pam (0.275 mg/kg IV). Also, amoxicillin (15 mg/kgIM), buprenex (0.01 mg/kg SQ), and oxymorphine
(0.05 mg/kg SQ) were administered. Prophylaxis wasperformed to remove plaque, calculus, and staining.Under sterile conditions, intraoral anesthesia wasachieved by using lidocaine with 2% epinephrine forextraction of 4 premolars and gingivectomy of themaxillary first premolars and the mandibular secondpremolars. Gingivectomy on those teeth was necessaryto expose enough clinical crown to allow properbracket placement. The divergent roots on the maxil-lary second and the mandibular third premolars weresectioned with a high-speed hand piece with a surgicalcarbide bur. The tissue was reflected with a periostealelevator. The tooth was luxated by using an elevatorand delivered with forceps. Incisions were made forminiplate placement apical to the maxillary third pre-molar and the mandibular fourth premolar. L-shapedminiplates (KLS Martin) were placed with 2 bonescrews at the experimental sites. Incisions were made toplace bone screws in all 4 quadrants as bone markers.Resorbable gut sutures were used to close the flaps.Clavomox (15 mg/kg bid) for 7 days and carprofen (2.2mg/kg bid) for 5 days were administered postopera-tively. The animals were allowed to recover for 2weeks, and we monitored wound healing and weightgain before orthodontic appliance attachment and acti-vation.
For orthodontic appliance attachment, anesthesiawas achieved with the previously described method. Anotch was made on the midpoint of the clinical crownwith a round bur with a high-speed hand piece as areference point in case bracket rebonding was neces-sary in the future. Teeth were cleaned with pumice,etched with 35% phosphoric acid for 20 seconds, rinsedwith water, and dried. One coat of light-cured adhesiveprimer (3M, St Paul, Minn) was applied and light curedfor 10 seconds. Precoated canine brackets (MBT; 3MUnitek, Monrovia, Calif) with hooks were bonded withlight-cured adhesive. NiTi springs were tied to thehooks with wire ties. Then, the dogs received fluoro-chrome bone dye calcein green intravenously (15 mg/kg)(Sigma-Adrich, St Louis, Mo).17 (Histologic resultsfrom this part of the study will be published separately.)
Table II. Procedures and time line
Time line Procedures
Surgery Miniplate placement, 4 premolars extracted, bonemarkers placed, gingivectomy, prophylaxis, 2weeks of healing
T0 Bonded brackets, activated NiTi coil springs,measurements, x-rays
T6 Measurements, x-raysT12 Killed, measurements, x-rays
The dogs were then moved to the x-ray machine for

American Journal of Orthodontics and Dentofacial OrthopedicsFebruary 2008
189.e4 Kim et al
lateral cephalograms. Finally, the space between the 2brackets or between the bracket and the miniplate wasmeasured twice with digital calipers.
At T6, lateral cephalograms were taken as before.Linear measurements were made with digital calipersby using the same landmarks as T0. Broken or missingappliances were replaced as needed.
At T12, the animals were killed with 5 mL ofsodium pentobarbital. Linear measurements and lateralcephalograms were taken as before.
Throughout the 12-week experimental period, theanimals were checked for loose appliances biweekly,and, when discovered, the appliances were repaired asquickly as possible, usually within 3 days. The dogsalso received chlorhexadine rinses and occasional toothbrushing as needed.
The amount of space closure was assessed in 3ways.
1. Linear measurement. Space closure was measuredclinically with digital calipers at T0, T6, and T12.For tooth-borne anchorage, the mesiodistal mid-points of the brackets were used as reference pointsto measure interbracket distance. For implant an-chorage, the most mesial point on the miniplatehole to the midpoint on the bracket was used tomeasure space closure. The measurements weremade twice and averaged.
2. Angular measurement. Lateral cephalograms takenat T0, T6, and T12 were traced and superimposedby using the bone markers. Tipping was measuredby using the long axis of the tooth and the implant.
3. The amount of anchorage loss per tooth or implant.Superimpositions were used to measure the percent-age of anchorage loss. The absolute amount of spaceclosure was measured radiographically in millimeters
Table III. Complications and repairs
DogRepairs to brackets
(quadrant, n)Repairs to
(quadra
1 — LR, 22 — LR, 1; U
3 — UR, 1; L
4 LL, 1 —
5 — —6 UL, 1 UL, 17 — LL, 18 LL, 1 —
UR, Upper right quadrant; UL, upper left quadrant; LR, lower rightpostactivation; T9, 9 weeks postactivation.
along the NiTi springs. Then, the anchorage loss was
calculated by dividing the amount of movement of theanchor tooth or implant by the amount of total spaceclosure, multiplying by 100 to obtain a percentage.
To test the accuracy of the measurements, an errorstudy was performed on a 40% random sample of theoriginal subjects. All measurements were made again(except for space closure) at least a month after themain study measurements, and the differences betweenthe 2 sets of measurements were compared by usingDahlberg’s formula18 (se2 � � d2/2n). The root meansquare error results were 2.43° for tipping measurementerror and 0.21 mm for anchorage loss measurementerror.
The survival rate of miniplates, and miniscrews vsbone markers, was evaluated. The criterion for survivalof miniplates was ability to withstand orthodonticforce. Also, the survival rates of the brackets andsprings were observed (Table III).
Data analysis
Paired t tests were used to analyze the meanmeasurements in the mandible and the maxilla. Thedata were evaluated for significant differences inamount of tooth movement at each interval by using astatistical software package (version 11 for Mac OS X;SPSS, Chicago, Ill). Significance level was establishedat P �.05.
RESULTS
Complications included occasional debonding ofthe brackets (3) and detached NiTi coil springs (8)(Table III). Other complications included gingival in-fection leading to eventual miniplate failure in 1 dog.Of the remaining 15 miniplates, 1 miniplate had slightmobility buccolingually, and 2 miniplates had gingival
Other complications
Missing first premolar, UR (T3)LR, mobility, pus, swelling around miniplate (T6)Killed at T9LR, UR, spring distorted (T3)Mobility of LR miniplate (T9)LR, miniplate bent buccally 90° (T3)UL, mesial bone marker missing (T9)Gingival infectionGingival infection
——
t; LL, lower left quadrant; T3, 3 weeks postactivation; T6, 6 weeks
springsnt, n)
L,1
R, 1
quadran
infection, which required additional antibiotics. One
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 133, Number 2
Kim et al 189.e5
dog was missing the maxillary first premolar at 3 weekspostactivation. Some NiTi springs became distorted.When these springs were removed and checked, theystill maintained their superelastic properties; therefore,we assumed that the springs exerted constant forcedespite their appearance. If both springs in an arch wereinactive at T6, that was the end point for analysis.Otherwise, the end point was 12 weeks of orthodonticloading. Most maxillary quadrants had inactive springsby T6, whereas most mandibular arches continued tohave space closure throughout the 12-week experimen-tal period (Table IV).
The repairs included 3 brackets (3 control, 0 exper-imental) and 8 springs (2 control, 6 experimental).
The survival rate for the loaded miniscrews was 30of 32 bone screws (94%); this was similar to thesuccess rate of 97% demonstrated by Deguchi et al.19
The survival rate for unloaded miniscrews was 31 of 32bone screws (97%). The success rate for the miniplatesduring the 12 weeks of orthodontic loading was 94%(15 of 16).
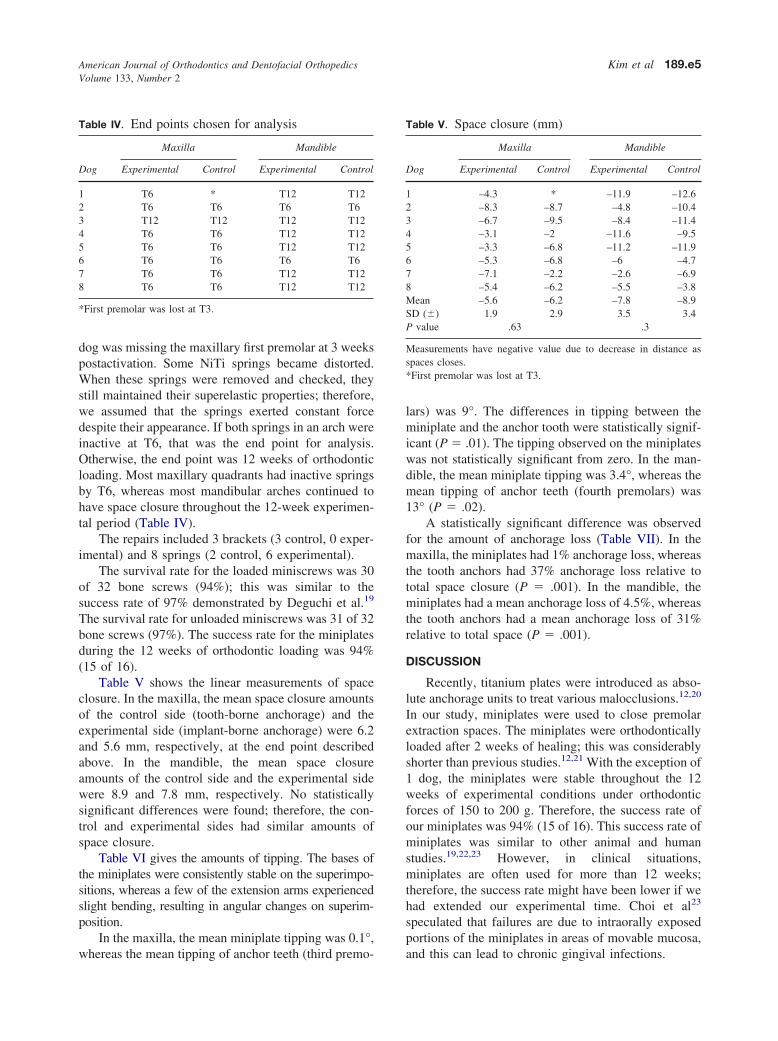
Table V shows the linear measurements of spaceclosure. In the maxilla, the mean space closure amountsof the control side (tooth-borne anchorage) and theexperimental side (implant-borne anchorage) were 6.2and 5.6 mm, respectively, at the end point describedabove. In the mandible, the mean space closureamounts of the control side and the experimental sidewere 8.9 and 7.8 mm, respectively. No statisticallysignificant differences were found; therefore, the con-trol and experimental sides had similar amounts ofspace closure.
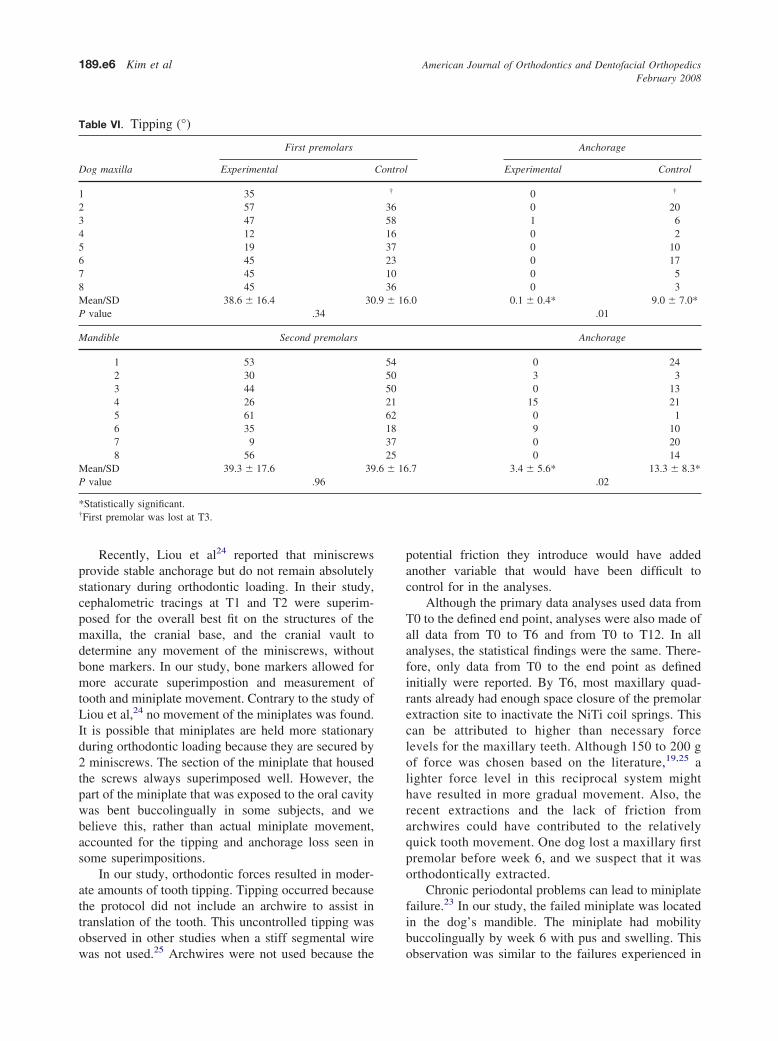
Table VI gives the amounts of tipping. The bases ofthe miniplates were consistently stable on the superimpo-sitions, whereas a few of the extension arms experiencedslight bending, resulting in angular changes on superim-position.
In the maxilla, the mean miniplate tipping was 0.1°,
Table IV. End points chosen for analysis
Dog
Maxilla Mandible
Experimental Control Experimental Control
1 T6 * T12 T122 T6 T6 T6 T63 T12 T12 T12 T124 T6 T6 T12 T125 T6 T6 T12 T126 T6 T6 T6 T67 T6 T6 T12 T128 T6 T6 T12 T12
*First premolar was lost at T3.
whereas the mean tipping of anchor teeth (third premo-
lars) was 9°. The differences in tipping between theminiplate and the anchor tooth were statistically signif-icant (P � .01). The tipping observed on the miniplateswas not statistically significant from zero. In the man-dible, the mean miniplate tipping was 3.4°, whereas themean tipping of anchor teeth (fourth premolars) was13° (P � .02).
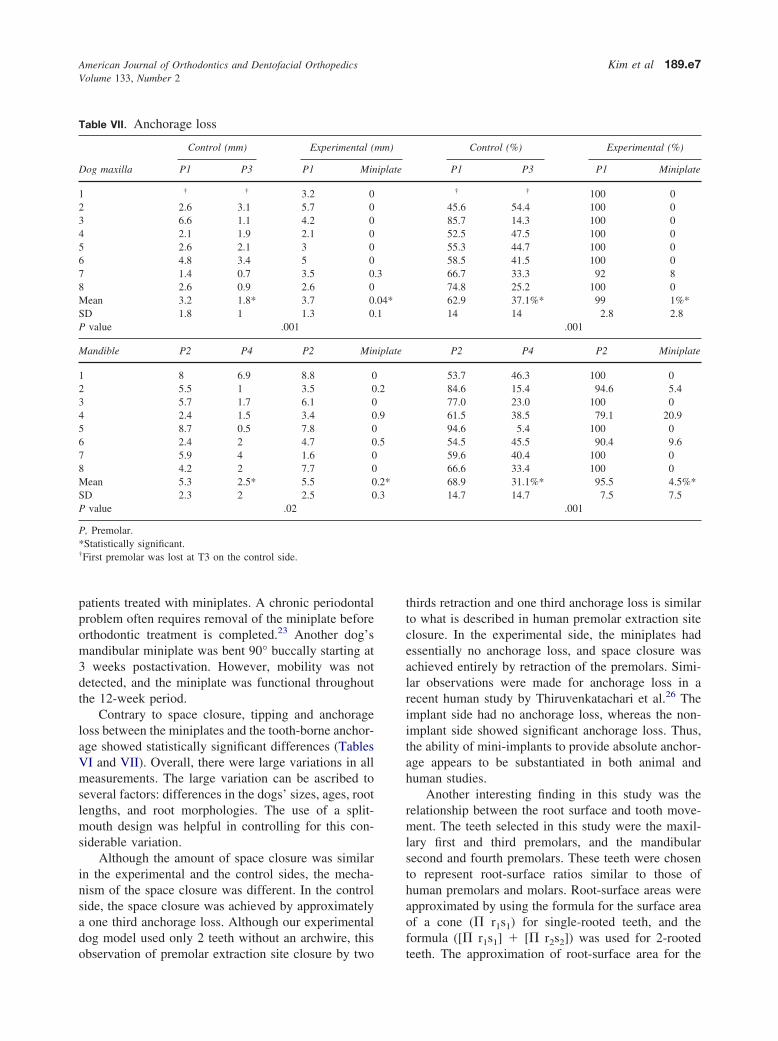
A statistically significant difference was observedfor the amount of anchorage loss (Table VII). In themaxilla, the miniplates had 1% anchorage loss, whereasthe tooth anchors had 37% anchorage loss relative tototal space closure (P � .001). In the mandible, theminiplates had a mean anchorage loss of 4.5%, whereasthe tooth anchors had a mean anchorage loss of 31%relative to total space (P � .001).
DISCUSSION
Recently, titanium plates were introduced as abso-lute anchorage units to treat various malocclusions.12,20
In our study, miniplates were used to close premolarextraction spaces. The miniplates were orthodonticallyloaded after 2 weeks of healing; this was considerablyshorter than previous studies.12,21 With the exception of1 dog, the miniplates were stable throughout the 12weeks of experimental conditions under orthodonticforces of 150 to 200 g. Therefore, the success rate ofour miniplates was 94% (15 of 16). This success rate ofminiplates was similar to other animal and humanstudies.19,22,23 However, in clinical situations,miniplates are often used for more than 12 weeks;therefore, the success rate might have been lower if wehad extended our experimental time. Choi et al23
speculated that failures are due to intraorally exposedportions of the miniplates in areas of movable mucosa,
Table V. Space closure (mm)
Dog
Maxilla Mandible
Experimental Control Experimental Control
1 –4.3 * –11.9 –12.62 –8.3 –8.7 –4.8 –10.43 –6.7 –9.5 –8.4 –11.44 –3.1 –2 –11.6 –9.55 –3.3 –6.8 –11.2 –11.96 –5.3 –6.8 –6 –4.77 –7.1 –2.2 –2.6 –6.98 –5.4 –6.2 –5.5 –3.8Mean –5.6 –6.2 –7.8 –8.9SD (�) 1.9 2.9 3.5 3.4P value .63 .3
Measurements have negative value due to decrease in distance asspaces closes.*First premolar was lost at T3.
and this can lead to chronic gingival infections.
American Journal of Orthodontics and Dentofacial OrthopedicsFebruary 2008
189.e6 Kim et al
Recently, Liou et al24 reported that miniscrewsprovide stable anchorage but do not remain absolutelystationary during orthodontic loading. In their study,cephalometric tracings at T1 and T2 were superim-posed for the overall best fit on the structures of themaxilla, the cranial base, and the cranial vault todetermine any movement of the miniscrews, withoutbone markers. In our study, bone markers allowed formore accurate superimpostion and measurement oftooth and miniplate movement. Contrary to the study ofLiou et al,24 no movement of the miniplates was found.It is possible that miniplates are held more stationaryduring orthodontic loading because they are secured by2 miniscrews. The section of the miniplate that housedthe screws always superimposed well. However, thepart of the miniplate that was exposed to the oral cavitywas bent buccolingually in some subjects, and webelieve this, rather than actual miniplate movement,accounted for the tipping and anchorage loss seen insome superimpositions.
In our study, orthodontic forces resulted in moder-ate amounts of tooth tipping. Tipping occurred becausethe protocol did not include an archwire to assist intranslation of the tooth. This uncontrolled tipping wasobserved in other studies when a stiff segmental wire
Table VI. Tipping (°)
First premolars
Dog maxilla Experimental
1 352 573 474 125 196 457 458 45Mean/SD 38.6 � 16.4 30P value .34
Mandible Second premolars
1 532 303 444 265 616 357 98 56
Mean/SD 39.3 � 17.6 39P value .96
*Statistically significant.†First premolar was lost at T3.
was not used.25 Archwires were not used because the
potential friction they introduce would have addedanother variable that would have been difficult tocontrol for in the analyses.
Although the primary data analyses used data fromT0 to the defined end point, analyses were also made ofall data from T0 to T6 and from T0 to T12. In allanalyses, the statistical findings were the same. There-fore, only data from T0 to the end point as definedinitially were reported. By T6, most maxillary quad-rants already had enough space closure of the premolarextraction site to inactivate the NiTi coil springs. Thiscan be attributed to higher than necessary forcelevels for the maxillary teeth. Although 150 to 200 gof force was chosen based on the literature,19,25 alighter force level in this reciprocal system mighthave resulted in more gradual movement. Also, therecent extractions and the lack of friction fromarchwires could have contributed to the relativelyquick tooth movement. One dog lost a maxillary firstpremolar before week 6, and we suspect that it wasorthodontically extracted.
Chronic periodontal problems can lead to miniplatefailure.23 In our study, the failed miniplate was locatedin the dog’s mandible. The miniplate had mobilitybuccolingually by week 6 with pus and swelling. This
Anchorage
Experimental Control
0 †
0 201 60 20 100 170 50 3
.0 0.1 � 0.4* 9.0 � 7.0*.01
Anchorage
0 243 30 13
15 210 19 100 200 14
.7 3.4 � 5.6* 13.3 � 8.3*.02
Control
†
36581637231036
.9 � 16
5450502162183725
.6 � 16
observation was similar to the failures experienced in
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 133, Number 2
Kim et al 189.e7
patients treated with miniplates. A chronic periodontalproblem often requires removal of the miniplate beforeorthodontic treatment is completed.23 Another dog’smandibular miniplate was bent 90° buccally starting at3 weeks postactivation. However, mobility was notdetected, and the miniplate was functional throughoutthe 12-week period.
Contrary to space closure, tipping and anchorageloss between the miniplates and the tooth-borne anchor-age showed statistically significant differences (TablesVI and VII). Overall, there were large variations in allmeasurements. The large variation can be ascribed toseveral factors: differences in the dogs’ sizes, ages, rootlengths, and root morphologies. The use of a split-mouth design was helpful in controlling for this con-siderable variation.
Although the amount of space closure was similarin the experimental and the control sides, the mecha-nism of the space closure was different. In the controlside, the space closure was achieved by approximatelya one third anchorage loss. Although our experimentaldog model used only 2 teeth without an archwire, this
Table VII. Anchorage loss
Control (mm) Experimental (
Dog maxilla P1 P3 P1 Min
1 † † 3.2 02 2.6 3.1 5.7 03 6.6 1.1 4.2 04 2.1 1.9 2.1 05 2.6 2.1 3 06 4.8 3.4 5 07 1.4 0.7 3.5 08 2.6 0.9 2.6 0Mean 3.2 1.8* 3.7 0SD 1.8 1 1.3 0P value .001
Mandible P2 P4 P2 Min
1 8 6.9 8.8 02 5.5 1 3.5 03 5.7 1.7 6.1 04 2.4 1.5 3.4 05 8.7 0.5 7.8 06 2.4 2 4.7 07 5.9 4 1.6 08 4.2 2 7.7 0Mean 5.3 2.5* 5.5 0SD 2.3 2 2.5 0P value .02
P, Premolar.*Statistically significant.†First premolar was lost at T3 on the control side.
observation of premolar extraction site closure by two
thirds retraction and one third anchorage loss is similarto what is described in human premolar extraction siteclosure. In the experimental side, the miniplates hadessentially no anchorage loss, and space closure wasachieved entirely by retraction of the premolars. Simi-lar observations were made for anchorage loss in arecent human study by Thiruvenkatachari et al.26 Theimplant side had no anchorage loss, whereas the non-implant side showed significant anchorage loss. Thus,the ability of mini-implants to provide absolute anchor-age appears to be substantiated in both animal andhuman studies.
Another interesting finding in this study was therelationship between the root surface and tooth move-ment. The teeth selected in this study were the maxil-lary first and third premolars, and the mandibularsecond and fourth premolars. These teeth were chosento represent root-surface ratios similar to those ofhuman premolars and molars. Root-surface areas wereapproximated by using the formula for the surface areaof a cone (� r1s1) for single-rooted teeth, and theformula ([� r1s1] � [� r2s2]) was used for 2-rooted
Control (%) Experimental (%)
P1 P3 P1 Miniplate
† † 100 045.6 54.4 100 085.7 14.3 100 052.5 47.5 100 055.3 44.7 100 058.5 41.5 100 066.7 33.3 92 874.8 25.2 100 062.9 37.1%* 99 1%*14 14 2.8 2.8
.001
P2 P4 P2 Miniplate
53.7 46.3 100 084.6 15.4 94.6 5.477.0 23.0 100 061.5 38.5 79.1 20.994.6 5.4 100 054.5 45.5 90.4 9.659.6 40.4 100 066.6 33.4 100 068.9 31.1%* 95.5 4.5%*14.7 14.7 7.5 7.5
.001
mm)
iplate
.3
.04*
.1
iplate
.2
.9
.5
.2*
.3
teeth. The approximation of root-surface area for the

American Journal of Orthodontics and Dentofacial OrthopedicsFebruary 2008
189.e8 Kim et al
maxillary first premolar to third premolar ratio was32%:68%; for the mandibular second premolar tofourth premolar, the ratio was 38%:62%. The anchorteeth had about twice the root-surface areas as theretracted premolars. When compared with the rate oftooth movement, the tooth-movement ratio for themaxillary first premolar to third premolar was 66%:34%. Similarly, the tooth-movement ratio observed inthe mandible for the second premolar to the fourthpremolar was 67%:33%. Thus, root surface to toothmovement had an almost perfect inverse relationship inthis reciprocal anchorage system.
There were appliance failures in several dogs (TableIII). The most common failures were detached springs(8) and debonded brackets (3). The dogs were placedon a soft diet to reduce appliance failures. However,they could have bitten their food bowl holder, whichwas made of thin metal attached to the cage. This mighthave contributed to the failed implant and the buccallydisplaced miniplates. The husbandry department wasasked to withhold enrichments such as bones or toys.Despite this request, we occasionally found hard toys inthe dogs’ cages. A few studies have used cast crownsfor appliance attachment.25 This requires considerablelaboratory time and cost. Our bonding techniqueworked fairly well, and repairs usually took less than 5minutes to complete after anesthesia was achieved.
Histologic evaluation of the miniscrews is currentlybeing performed and will be reported in a separatearticle. Also, we concurrently investigated miniscrewsin the palate to determine their response to immediatevs delayed orthodontic loading, and these results willalso be reported soon.
In clinical situations, the decision for using aminiscrew or a miniplate involves several factors,including availability of bone, anatomy of the site,desired vector of force, and the anticipated anchoragerequirements for the planned tooth movements. Bothsystems have advantages and should be further studiedto maximize their potential as orthodontic anchorage.In this study, miniplates offered excellent anchorageover a 12-week period, withstanding continuous forcesof 150 to 200 g. Activation of the miniplates occurredat 2 weeks, suggesting that short-term healing is ade-quate, and further work should test whether immediateloading is advantageous for survival.
CONCLUSIONS
Although the total amount of space closure wassimilar in both the control and the experimental groups,the mechanism of space closure was different. In thecontrol group, slippage of the anchor teeth accounted
for approximately one third of the space closure. In theexperimental group, the miniplates had minimal move-ment, and space closure was achieved almost entirelyby movement of the teeth. These results confirm thatminiplates provide virtually absolute anchorage.
REFERENCES
1. Roberts WE, Marshall JK, Mozsary GP. Rigid endosseousimplant utilized as anchorage to protract molars and close anatrophic extraction site. Angle Orthod 1990;60:35-52.
2. Roberts WE, Smith RK, Zilberman Y, Mozsary PG, Smith RS.Osseous adaptation to continuous loading of rigid endosseousimplants. Am J Orthod 1984;86:95-111.
3. Turley PK, Kean C, Schur J, Stefanac J, Gray J, Hennes J, et al.Orthodontic force application to titanium endosseous implants.Angle Orthod 1988;58:151-62.
4. Wehrbein H, Diedrich P. Endosseous titanium implants duringand after orthodontic load—an experimental study in the dog.Clin Oral Implants Res 1993;4:76-82.
5. Parr JA, Garetto LP, Wolford ME, Arbuckle GR, Roberts WE.Sutural expansion using rigidly integrated endosseous implants:an experimental study in rabbits. Angle Orthod 1997;67:283-90.
6. Smalley W. Implants for tooth movement: determining implantlocation and orientation. J Esthet Dent 1995;7:62-72.
7. Kanomi R. Mini-implant for orthodontic anchorage. J ClinOrthod 1997;31:763-7.
8. Lee JS, Park HS, Kyung HM. Micro-implant anchorage forlingual treatment of a skeletal Class II malocclusion. J ClinOrthod 2001;35:643-7.
9. Park HS, Bae SM, Kyung HM, Sung JH. Micro-implant anchor-age for treatment of skeletal Class I bialveolar protrusion. J ClinOrthod 2001;35:417-22.
10. Bae SM, Park HS, Kyung HM, Kwon O, Sung J. Clinicalapplication of micro-implant anchorage. J Clin Orthod 2002;36:298-302.
11. Park YC, Lee SY. Intrusion of posterior teeth using miniscrewimplants. Am J Orthod Dentofacial Orthop 2003;123:690-4.
12. Unemori M, Sugawara J, Mitani H, Nagasaka H, Kawamura H.Skeletal anchorage system for open bite correction. Am J OrthodDentofacial Orthop 1999;115:166-74.
13. Janssens F, Swennen G, Dujardin T, Glineur R, Malevez C. Useof an onplant as orthodontic anchorage. Am J Orthod DentofacialOrthop 2002;122:566-70.
14. Block M, Hoffman D. A new device for absolute anchorage fororthodontics. Am J Orthod Dentofacial Orthop 1995;107:251-8.
15. Wehrbein H, Glatzmaier J, Mundwiller U, Diedrich P. TheOrthosystem: a new implant system for orthodontic anchorage inthe palate. J Orofac Orthop 1996;57:143-53.
16. Costa A, Raffani M, Melsen B. Miniscrews as orthodonticanchorage: a preliminary report. Int J Adult Orthod OrthognathSurg 1998;13:201-9.
17. Ohmae M, Saito S, Morohashi T, Seki K, Qu H, Kanomi R, et al.A clinical and histological evaluation of titanium mini-implantsas anchor for orthodontic intrusion in the beagle dog. Am JOrthod Dentofacial Orthop 2001;119:489-97.
18. Dahlberg G. Statistical methods for medical and biologicalstudents. New York: Interscience Publications; 1940.
19. Deguchi T, Takano-Yamamoto T, Kanomi R. The use of small tita-nium screws for orthodontic anchorage. J Dent Res 2003;82:377-81.
20. Sugawara J, Daimaruya T, Umemori M, Nagasaka H, TakahashiI, Kawamura H, et al. Distal movement of mandibular molars inadult patients with the skeletal anchorage system. Am J Orthod
Dentofacial Orthop 2004;125:130-8.
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 133, Number 2
Kim et al 189.e9
21. Sherwood K, Burch J, Thompson W. Intrusion of supereruptedmolars with titanium miniplate anchorage. Angle Orthod 2003;73:597-601.
22. Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T,Takano-Yamamoto T. Factors associated with the stability oftitanium screws placed in the posterior region for orthodon-tic anchorage. Am J Orthod Dentofacial Orthop 2003;124:373-8.
23. Choi B, Zhu S, Kim Y. A clinical evaluation of titaniumminiplates as anchors for orthodontic treatment. Am J Orthod
Dentofacial Orthop 2005;128:382-4.24. Liou EJ, Pai BC, Lin JC. Do miniscrews remain stationary underorthodontic forces? Am J Orthod Dentofacial Orthop 2004;126:42-7.
25. Saito S, Sugimoto N. Endosseous titanium implants as anchor formesiodistal tooth movement in beagle dog. Am J Orthod Dento-facial Orthop 2000;118:601-7.
26. Thiruvenkatachari B, Pavithranand A, Rajasigamani K, KyungHM. Comparison and measurement of the amount of anchorageloss of the molars with and without the use of implant anchorageduring canine retraction. Am J Orthod Dentofacial Orthop
2006;129:551-4.













![Dental Extrusion with Orthodontic Miniscrew Anchorage: A ... · Miniscrews for orthodontic treatments are available in severallengths(5–12mm)anddiameters(1.2–2.0mm)[17]. E. Mizrahi](https://img.pdfslide.net/doc/110x75/5ed55049eb5803601c17fbed/dental-extrusion-with-orthodontic-miniscrew-anchorage-a-miniscrews-for-orthodontic.jpg)