Embed Size (px)
Citation preview
Article ID: WMC001366 ISSN 2046-1690
A Comparison Of The Vulnerability Of The BeckDepression Inventory And The Modified StroopProcedure To Intentional Response AlterationCorresponding Author:Dr. Eugene Lubliner,Assistant Adjunct Professor, Hofstra University, Hauser Hall, Room 220, Hofstra University, 11549 - UnitedStates of America
Submitting Author:Dr. Eugene P Lubliner,Assistant Adjunct Professor, Hofstra University, Hauser Hall, Room 220, Hofstra University, 11549 - UnitedStates of America
Article ID: WMC001366
Article Type: Research articles
Submitted on:07-Jan-2011, 02:48:58 PM GMT Published on: 08-Jan-2011, 07:34:59 PM GMT
Article URL: http://www.webmedcentral.com/article_view/1366
Subject Categories:PSYCHOLOGY
Keywords:Beck Depression Inventory, Modified Stroop Procedure, Stroop, Depression, Response Alteration,Lying
How to cite the article:Lubliner E, Motta R. A Comparison Of The Vulnerability Of The Beck DepressionInventory And The Modified Stroop Procedure To Intentional Response Alteration . WebmedCentralPSYCHOLOGY 2011;2(1):WMC001366
Source(s) of Funding:
None.
Competing Interests:
None.
WebmedCentral > Research articles Page 1 of 22
WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
A Comparison Of The Vulnerability Of The BeckDepression Inventory And The Modified StroopProcedure To Intentional Response AlterationAuthor(s): Lubliner E, Motta R
Abstract
The Beck Depression Inventory – Second Edition hasbeen validated in numerous populations and is themost widely used depression assessment tool inresearch and in practice. The obvious nature of itsitems makes the instrument vulnerable to intentionalefforts to distort one’s level of depression. Thepurpose of this study was to examine the relativeresistance to intentional response distortion on theBDI-II in comparison to a modified Stroop procedureinvolving the color naming of depression relevantwords. Mildly depressed and non-depressedparticipants were asked to present themselves aseither depressed or non-depressed on each of the twoinstruments. Each participant was provided with avignette that encouraged them to respond in adepressed or non-depressed manner. Thus, the studyinvolved a 2 x 2 design with two levels of affect(depressed and non-depressed) and two levels ofresponse distortion (in a depressed or non-depresseddirection). Study results indicated that both depressedand non-depressed participants were able tointentionally alter their responses to appear more orless depressed on the BDI-II but were unable to dothis on the modified Stroop.
Introduction
The Beck Depression Inventory – Second Edition1 is apopular self-report measure of depression. The currentversion of the inventory and its predecessors has beenshown to be reliable and valid across a wide agerange of samples.1 Additionally, the BDI-II andprevious versions have been standardized in differentcountries and cultures. It has been shown to bereliable and valid in Bulgaria2, Spain3, Cuba4, China5,Japan6, and many subcultures.7-9 Despite the volume of research supporting the use ofthe BDI-II, there are certain instances when theinventory might be insufficient or inaccurate inassessing a person’s level of depression. One suchscenario is when a researcher is interested in studyingtrait depression, as opposed to state depression. The
BDI-II is sensitive to minor fluctuations in a person’smood.10,11 Therefore, if one wishes to examine traitdepression, it may be an ineffective measure. Anothersituation in which the BDI-II may be ineffective is whenthe person being assessed is motivated to alter thedepression level of their responses.12,13 Throughoutthe years many questions have been raised regardinga person’s ability to fabricate responses on theBDI-II.12-15 A person might intentionally distortresponses to appear to have emotional difficulties ordeny these difficulties altogether. In these specific instances that weaken the validity ofthe BDI-II, an alternative measure might be used. Ameasure such as the modified Stroop may be lesssusceptible to attempts to give preferred responses.The modified Stroop procedure, as used here,involves color-naming depression related words. Theperson who is depressed will take longer to name thecolor of a depression related word because the worditself is troubling and therefore interferes with colornaming. This delay in color naming is known as theStroop interference effect. In terms of Beck’s model ofdepression, the modified Stroop indirectly assesses aperson’s cognitive schema for depression. If a personhas a pervasive schema for depression, thendepression related words would cause high amountsof disturbance on a Stroop task. There might be a number of testing situations where aperson might wish to appear more or less depressed.If this were the case, it would be relatively easy to alterone’s responses on the BDI-II as the items arerelatively obvious with regard to what constitutes adepressed or non-depressed response. In contrast, itwould be far more difficult to alter one’s responses onthe Stroop as the task is simply one of responselatency in color naming and it is not obvious as to howone should respond so as to appear more or lessdepressed.While the Stroop appears to be far more resistant thanthe BDI-II to deliberate response alteration, it does nothave the cutoff scores that the BDI-II has andtherefore is relatively lacking in incremental validity.When using the Stroop to identify depressedresponding, one cannot state that a given responsetime represents, say, mild or moderate depression.However, initial findings from the current study do
WebmedCentral > Research articles Page 2 of 22

WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
show significant correlations between the Stroopresponse times and known measures of depression(i.e. the Revised Hamilton Rating Scale forDepression16 and the Zung Self-Rating DepressionScale17, r = .39 - .49, p < .05). The purpose of this study is to determine how resistantthe BDI-II and the modified Stroop task are towardattempts at manipulating one’s responses. This will beaccomplished by creating situations where one ismotivated to fabricate responses. Participants whohave elevated levels of depression and non-depressedcontrols will be identified. These participants will thenbe read vignettes that encourage response distortionto appear depressed or non-depressed andcomparisons between scores on BDI-II and latencytimes on the modified Stroop will be examined.Overview of the BDI-IIBeck18 theorized that depressed individuals havebiased schemata—meaning they encode, store, andretrieve information differently than a non-depressedindividual. This bias leads to the misinterpretation ofevents and actions. Strengths of the BDI include its ease of use, itsapplicability to diverse samples, and the fact that it hasbeen the subject of numerous studies since itscreation. Research has shown that the BDI is able toconsistently and accurately measure current levels ofdepression in many different settings. Meta-analysesthat examine the BDI have shown that the instrumenthas an overall test-retest reliability of 0.72.19 Otherresearch that examines the internal consistency of theBDI shows that all items on the inventory load ontoone overall factor that can be characterized as generaldepression.20 These studies support the BDI as avalid instrument for assessing depression. The BDI is easy to use.21 It is convenient to have ashort and easily administered assessment tool thatcan reliably predict symptoms of depression and canbe completed with only minimal involvement from aresearcher or mental health professional. By simplyreading through the test items of the BDI, it is clearthat the inventory has a high degree of face validity.However, ease of administration might be outweighedby the potential to incorrectly classify someone asdepressed or non-depressed.The major critiques of the BDI-II can be categorized inthe following groups: lack of specificity, sensitivity tominor mood fluctuations, and demand characteristicsthat confound results. One of the greatest strengths ofthe BDI-II is also its greatest weakness: it is sensitiveto slight changes in response patterns. These changescould be caused by fluctuating levels of overalldepression, but changes could also be caused byother psychopathologies aside from depression, by
temporal changes in current mood that do not speak tomore general mood patterns, or by willfullymanipulating answers to achieve a desired result. The BDI has been shown to lack low-12 and high-endspecificity22. Low-end specificity is the ability of aninstrument to correctly identify people exhibiting lowlevels of a certain behavior by scoring low on theinstrument. High-end specificity is the opposite, wherean instrument can correctly identify people with highlevels of a certain behavior by scoring high on theinstrument. Factors such as malingering, denial, andoverall level of psychopathology affect how a personanswers the BDI-II at the high and low ends.Test-retest reliability of the BDI is affected when aperson is read a depression-related vignette inbetween testing sessions.23 The level of depressionat the second testing, as assessed by the BDI,increased based on the level of depression of thevignette. This demonstrates that the BDI is sensitive tominor mood influences and does not assess pervasivetrait levels of depression. The demand characteristics of the BDI-II are its final,and perhaps greatest, weakness. The inventory isconcisely organized, with headings before eachquestion that identify the aspect of depression beingassessed. Although this makes the questions clear forboth the examiner and the examinee, it also makes itquite easy to fabricate answers. One study wherenon-depressed participants were given vignettes thatencouraged people to feign symptoms of depressionshowed that 96% of the participants were able to fakedepression on the BDI, and 58% were able to fakesevere depression.13 Other studies have examined organization of the BDIas a demand characteristic. The clearly labeled titlesof each section, along with the ordered item responsesthat go from least depressed symptoms to mostdepressed symptoms, leave little to the imagination.One study demonstrated that when the responseitems of the BDI are randomly presented, moreaccurate results were obtained.14 This randompresentation seems to be able to counteract some ofthe demand characteristics inherent in the currentpresentation of the questionnaire. These weaknesses of the BDI-II might be addressedby using a different measure to assess depression.One such assessment measure is the modified Stroopprocedure.Overview of the Modified Stroop ProcedureThe modified Stroop (or emotional Stroop) task is analternative version of the classic Stroop procedure.24This task uses emotionally charged words printed indifferent colored inks as the stimulus. Words that havean emotional significance to the person performing the
WebmedCentral > Research articles Page 3 of 22

WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
task are likely to cause more interference than theywould to a person who is emotionally unaffected bythe words. This will result in longer color naming timesfor the people experiencing greater interference. Themodified Stroop task has been shown to be able tosuccessfully discriminate between people withdepression versus people without depression.25-30Less consistent f indings have also beenreported.31-33The major strength of the modified Stroop procedure isits relative stability over time. Research suggests thatthe modified Stroop for depression is consistent overmany months between testing intervals.34 Thisstability is what provides the basis for the hypothesisthat the modified Stroop may be resistant to attemptsat fabricating responses. Since the items in a Strooptask are novel to most people, the Stroop is resistantto response manipulation attempts. Research has demonstrated that the modified Stroopprocedure more consistently discriminates betweendepressed and non-depressed people than the BDIover the span of a year.34 This implies that themodified Stroop assesses more stable trait depression,whereas the BDI may be affected by transient statedepression. Longitudinal studies have shown thatdepressed psychiatric patients show a decrease inStroop interference times after a psychotherapeuticintervention.29,35 If the modified Stroop measurestrait depression, then it seems reasonable that Strooptimes decrease after an intervention for depression. Ifa person’s overall level of depression decreases, thiswill in turn create less interference on the Stroop task.In a modified Stroop procedure, response delaysshould only be the result of cognitive disruptioncaused by inadvertently reading an emotionallycharged word while trying to name its color. Someother reasons that word items can delay responselatency are because they have longer syllable length,are used less frequently in the English language, orare less concrete and salient. Unfortunately,emotionally charged words have a higher probability ofbeing longer in length, used less frequently, and beingless concrete and salient.36 Therefore, carefulselection of neutral words must be considered in anyexperiment. They have to meet the characteristics ofthe selected emotional words.It also may be possible to create longer interferencetimes within the neutral word items. By increasing theamount of emotional disruption a person experienceson the neutral words one would eliminate anyobservable Stroop effect, because there would be littleor no time difference between neutral and emotionallycharged items. When neutral words and emotionallycharged words are presented in a mixed presentation,
carryover effects from reading an emotionally chargedword can spill over to delay the color naming decisionon neutral words.37,38 This is why current researchsuggests the best way to evaluate a modified Stroopeffect is to present items in block form.39,40 In oneunusual example, researchers were able to create areverse modified Stroop effect by ordering items in apseudo-random pattern where an emotionally chargedword is always followed by two neutral words. Whenthis pattern was used, color naming for neutral wordswas significantly longer than color naming foremotionally charged words.37 Another critique of the modified Stroop procedure isthat there is a paucity of knowledge of the underlyingcognitive mechanisms that explain the modified Stroopprocedure. The original belief held by mostresearchers investigating the modified Stroop was thatthe cognitive mechanisms behind this phenomenonwere the same as those in the classic Stroopprocedure. The classic Stroop procedure uses itemsthat are semantically related to each other (i.e. colorwords and actual ink color). Alternately, the modifiedStroop uses items that are not semantically related tocolor. There is no ink color that is logically associatedwith the word “failure.” Current research shows that aclassic Stroop task involves immediate cognitivedisruption due to processing two semantically relateditems simultaneously.39 The modified Stroopprocedure appears to involve a slowing of responsetimes caused by the word item incorporating itself intoa person’s cognitive schema.37-39 Thus, when a wordlike “failure” is printed in green, it takes longer for adepressed person to say, “green,” than if theunderlying word is neutral such as “window.” An additional critique of the Stroop procedure, asmentioned earlier is its lack of incremental validity.While significant relationships exist between paperand pencil measures of depression and Stroop colornaming times of depression related words, cutoffresponse times have not been established that wouldspecifically correspond to varying levels of depression.Thus, it appears that both the Stroop procedure andthe BDI-II have strengths and weaknesses. Thestrength of the BDI-II is its ability to delineate levels ofdepression. Its weakness is the obvious nature of itsitems. The items on the Stroop are not easily seen asdepression related because the task involves colornaming; however, the measure lacks cutoff scores.One final critique of the both the Stroop and BDI-II,and perhaps a number of similar assessment devices,is their relative lack of discriminant validity. It cannotbe shown that the Stroop or the BDI-II assesses onlydepression and not other types of pathology. Giventhe overlap among different types of pathology and the
WebmedCentral > Research articles Page 4 of 22

WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
comorbidity that exists in most forms of psychologicaldistress, it cannot be argued that these measuresvalidly discriminate depression from other forms ofpsychological distress.The present study investigates a participant’s ability tointentionally alter responses on the BDI-II and themodified Stroop task. Because there are numeroussituations in which a person being assessed may bemotivated to fabricate responses, the sensitivity ofthese two measures toward active attempts to distortone’s level of depressive affect is important.Hypotheses Concerning Main EffectsDepressed participants will have significantly longerStroop interference times than non-depressedparticipants on the modified Stroop card withdepression related words, regardless of whether theywere instructed to respond in a depressed ornon-depressed manner. This is expected because themodified Stroop appears resistant to efforts tointentionally alter one’s responses.Depressed and non-depressed participants will notdiffer from each other on the modified Stroop card withneutral words regardless of whether they wereinst ructed to respond in a depressed ornon-depressed manner. This is expected because theneutral words will not activate depressive cognitions oraffect that may create additional task interference.Participants who are told to respond in a depressedmanner will have significantly higher scores on theBDI-II than participants who are told to respond in anon-depressed manner, regardless of whether theywere initially depressed or initially non-depressed. Thisis because the BDI-II may be sensitive to attempts todeliberately alter one’s responses.Hypotheses Within the Initial Level of DepressionConditionWithin the initially depressed group, participants whoare instructed to respond in a depressed andnon-depressed manner will not differ from each otherin Stroop response times for either the neutral ordepression related word cards. Again, the Stroop isexpected to be resistant to deliberate attempts atmanipulating one’s responses.Similarly, within the initially non-depressed group,participants who are instructed to respond in adepressed and non-depressed manner will not differfrom each other in Stroop response times for either theneutral or depression related word cards.Hypotheses Within the Vignette ConditionWithin the group of participants encouraged torespond in a depressed manner, participants who areinitially depressed and initially non-depressed will notdiffer from each other on BDI-II scores. This isexpected because the BDI-II may be vulnerable to
efforts of participants to manipulate their scores so asto appear depressed.Similarly, within the group of participants encouragedto respond in a non-depressed manner, participantswho are initially depressed and initially non-depressedwill not differ from each other on BDI-II scores.
Method
Participants and SettingsThere were 4 groups in this study, each of whichcontained 18 participants, for a total of 72 articipants(36 depressed, 36 non-depressed). The participantswere drawn from a community mental health centerand a physical therapy rehabilitation facility. In order tobe included in the study, participants had to meetcertain criteria. A potential participant had to be anative speaker of English, could not be color-blind,and could not be diagnosed with a psychotic disorderor bipolar disorder. To be included in the depressedgroup, a participant had to be initially identified by thefacility as having a psychiatric disorder, to be receivingtreatment at the time of testing, but most importantly,had to score in at least the mildly depressed range onthe two standardized depression diagnostic measuresdescribed below. In order to be included in thenon-depressed group, a participant had to have nohistory of mental illness or had to be out of treatmentfor any psychiatric condition for at least one year andhad to score in the non-depressed range on the twodepression diagnostic measures.Of the 36 participants in the depressed group, 29 wererecruited from the community mental health center and7 were recruited from the physical therapyrehabilitation facility. The mean age of the depressedgroup was 46.36 (SD = 16.19). There were a total of10 males and 26 females. All of the 36 participants inthe non-depressed group were recruited from thephysical therapy rehabilitation facility. The mean ageof the non-depressed group was 42.72 (SD = 16.30).There were a total of 19 males and 17 females. Depression Diagnostic Measures Revised Hamilton Rating Scale for Depression.41 TheRHRSD is a self-report instrument used to measurethe severity of depressive symptoms in adults. Theinventory has 76 items and has a check built into theinstrument to assess item response validity and anyinconsistency in responding. Each item is grouped intoa set of depression related symptoms, such as“feelings of guilt,” “loss of insight,” or “weight loss.” Theitems in each group increase in severity of symptoms,and also increase in point value towards totaldepression score. The participant is asked to endorse
WebmedCentral > Research articles Page 5 of 22

WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
each item with a “True” or a “False” response,depending on whether the item is deemed to bedescriptive or non-descriptive of the person completingthe form. The highest item endorsed by the participantwithin the item group is the one that receives pointstowards the total depression score. Scores on theRHRSD can range from 0 to 54, where higher scoresrepresent a higher level of depressive symptoms. Thescores can fall in the following ranges: 0 to 10 isnon-depressed, 11 to 16 is minor depression, 17 to 25is major depression, and 26 and above is severedepression. A participant had to have a minimumscore of 11 on this measure in order to be consideredfor the initially depressed group.The self-report form of the RHRSD has been shown tohave high internal consistency, with a Cronbach’salpha of .81.41 This study also demonstrated that theself-report form of the RHRSD highly correlates withscores on the Depression scale of the MinnesotaMultiphasic Personality Inventory – 2nd Edition(MMPI-2)42 r = .80, p < .01.41 Additionally, theRHRSD self-report form was moderately correlatedwith clinician’s independent observations ofparticipant’s behavior, with correlation values rangingfrom .27 to .58.43 Zung Self-Rating Depression Scale.17 The SDS is a20-item self-report instrument used to measures theseverity of depressive symptoms in adults. The itemsare presented as a 4-point Likert scale with eachsymptom displayed on the left side and choicesregarding the frequency of each symptom next to theitem. The symptom frequency choices are, “A little ofthe time,” “Some of the time,” “Good part of the time,”and, “Most of the time.” Half of the items are coded sothat higher frequency of occurrence results in a largerpoint value for that item, and the other half of the itemsare reversed such that reporting a lower frequency ofoccurrence results in a higher point value. The sum ofa person’s item scores translates into a totaldepression score. This total score is interpreted asone of four different descriptive categories: 20 to 39 isnon-depressed, 40 to 47 is mildly depressed, 48 to 55is moderately depressed, and 56 and above isseverely depressed. A participant had to have aminimum score of 40 in order to be considered for theinitially depressed group on this measure.Since the items of the SDS have remained unchangedfor over 40 years, there are numerous studies thathave assessed its reliability and validity. One recentstudy concluded that the SDS is highly correlated withthe Depression scale of the MMPI-2, r = .74, p <.001.44 This study also demonstrated that the SDShas high positive predictive power (PPP) and highnegative predictive power (NPP). PPP means that a
person who receives a high score on the SDS actuallydisplays symptoms of depression based on clinicalobservation. NPP means that a person who receives alow score on the SDS does not display symptoms ofdepression. When SDS results were compared toactual clinician reports, the SDS had a PPP of .75 andan NPP of .68.44 This indicates that the SDS has ahigh level of diagnostic discrimination.Dependent MeasureBeck Depression Inventory – Second Edition.1 TheBDI-II is a self-report instrument used to measure theseverity of depressive symptoms in adults andadolescents. The inventory has 21 items and can beused with participants from ages 13 and older. Theitem wordings and instructions were designed to beconsistent with the DSM-IV criteria for majordepression. The BDI-II utilizes a four-point scaleranging from 0 to 3 points. As each statementincreases in point value, this reflects an increase in theseverity of the depressive symptom. Scores on theBDI-II can range from 0 to 63. The sum of aparticipants item scores generates an overalldepression score which translates into four descriptivecategories: 0 to 13 is minimal depression, 14 to 19 ismild depression, 20 to 28 is moderate depression, and29 to 63 is severe depression.The BDI-II has been shown to have a high internalconsistency, with a coefficient alpha for a sample of120 college students of .93, and a coefficient alpha fora sample of 277 psychiatric outpatients of .92.1Additionally, the inventory has a high test-retestreliability for a sample of 26 psychiatric outpatients, r =.93, p < .01. The inventory has also been shown tohave high convergent validity. Scores on the BDI-II arehighly correlated with scores on the previous versionof the inventory, r = .93, p < .01. The convergentvalidity was also demonstrated when the BDI-II wascorrelated with the Hamilton Rating Scale forDepression, r = .71, p < .05.16Modified Stroop Procedure.24 The modified Stroopprocedure is a modified version of the original Strooptask. In this version of the task, participants are askedto name the ink color of words with varying emotionalvalences, as opposed to color word names in theoriginal task. For this task, participants are asked toname the color in which the word is printed whileignoring the actual content of the word.For the current study, words were derived from Kliegerand Cordner27, who used ten negative words and tenneutral words that were paired based on frequencyusing Kucera and Francis,45 length, and beginningletter. These 20 words were piloted by a randomsample of 25 adults to determine the 5 most negativewords. This was to ensure that the negative words
WebmedCentral > Research articles Page 6 of 22

WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
were the most relevant to the sample of similar agepeers. When the five most negative words weredetermined, they were paired with the five neutralwords previously established by Klieger andCordner.27The five negative words identified by a pilot study were“depressed,” “failure,” “gloomy,” “hopeless,” and“unhappy.” The five neutral words selected by the pilotstudy were “disguised,” “follows,” “gamble,”“harmless,” and “utility.” The five negative and neutralwords were placed on individual cards (8.5 x 11).Additionally, a card was used that consisted of controlstimuli (i.e., 00000). Each card had the 5 word itemspresented 20 times each, for a total of 100 items percard. Each word appeared four times in a given inkcolor (red, yellow, green, black, and blue), and thecards were arranged in such a way that neither thesame word nor the same color were repeated next to,above, or below one another. Each participantreceived the cards in the following order: the controlcard, the neutral word card, and then the negativeword card. This was done to ensure that any practiceeffect would go against the specific researchhypotheses. By taking the time used to complete thecontrol card and subtracting it from the time it took tocomplete the neutral and negative word cards, amodified Stroop interference time was calculated. Themodified Stroop interference times for neutral andnegative words were treated as two separatedependent variables during data analysis. ModifiedStroop response time was calculated by subtractingthe time to name the colors of items (colored zeros) onthe control card from the times to color name items onthe neutral or negative cards.ProcedureParticipants at the two sites mentioned above signedinformed consent forms and indicated whether or notthey were in treatment for a psychological disorder.They also indicated whether or not they were colorblind. In order to be categorized as depressed,participants had to fall in the mildly depressed range orabove on both the SDS and RHRSD. In order to becategorized as non-depressed, participants had to fallin the non-depressed range on both the SDS and theRHRSD and could not be currently receivingpsychiatric treatment. Participants who scored in thedepressed range on one self-report measure and thenon-depressed range on the other measure were notasked to take part in the second half of the study.After meeting all the initial criteria, the qualifyingdepressed and non-depressed participants wereadministered the second half of the study within onehour of completing the screening measures.Participants were randomly assigned into one of two
conditions: either (1) being read a vignette thatencouraged minimizing depressive symptoms (seeAppendix A) or (2) being read a vignette thatencouraged enhancing depressive symptoms (seeAppendix B). Because the participants were all adultsthat were participating in some form of weeklytherapeutic service, both vignettes focused on salientissues a client might encounter.The participants were then instructed to answer theitems of the two dependent measures as if they wereexperiencing the situation described in the vignette.The two dependent measures were presented toparticipants in a counterbalanced fashion, where halfthe participants in each of the four conditions receivedthe BDI-II first and the other half received the modifiedStroop first. Participants were given specificinstructions for each of the measures immediatelybefore they were presented. Before the participantreceived the BDI-II the instructions that appear on topof the BDI-II form were read aloud. Then theparticipant was given as much time as needed tocomplete the form.When the participant was given the modified Stroopprocedure, they were given the following instructions,“Starting on the top of the page, and going from left toright, please name the ink color of each item aloudwithout paying attention to the word itself. The worditself is of no concern, only focus on the ink color.Perform this task as quickly as you can without makingany mistakes.” Then each stimulus card was timedwith a stopwatch that was accurate to 1/100 of asecond. Time started when the researcher promptedthe participant to begin, and time ended when theparticipant called out the color of the last word item onthe card. After the participant completed all therequired measures they were debriefed and thankedfor their time.Design and Statistical AnalysisThis study employed a 2x2 factorial design, with initiallevel of depression (initially depressed or initiallynon-depressed) and vignette condition (enhancingdepression or minimizing depression) serving as thetwo grouping variables. A two-way multivariateanalysis of covariance (MANCOVA) was used toexamine the effect of initial level of depression andvignette condition on the three dependent variables ofBDI-II scores, modified Stroop interference time forneutral words, and modified Stroop interference fordepression words. MANCOVA main effects werefurther analyzed with separate univariate factorialANCOVAs.
WebmedCentral > Research articles Page 7 of 22

WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
Results
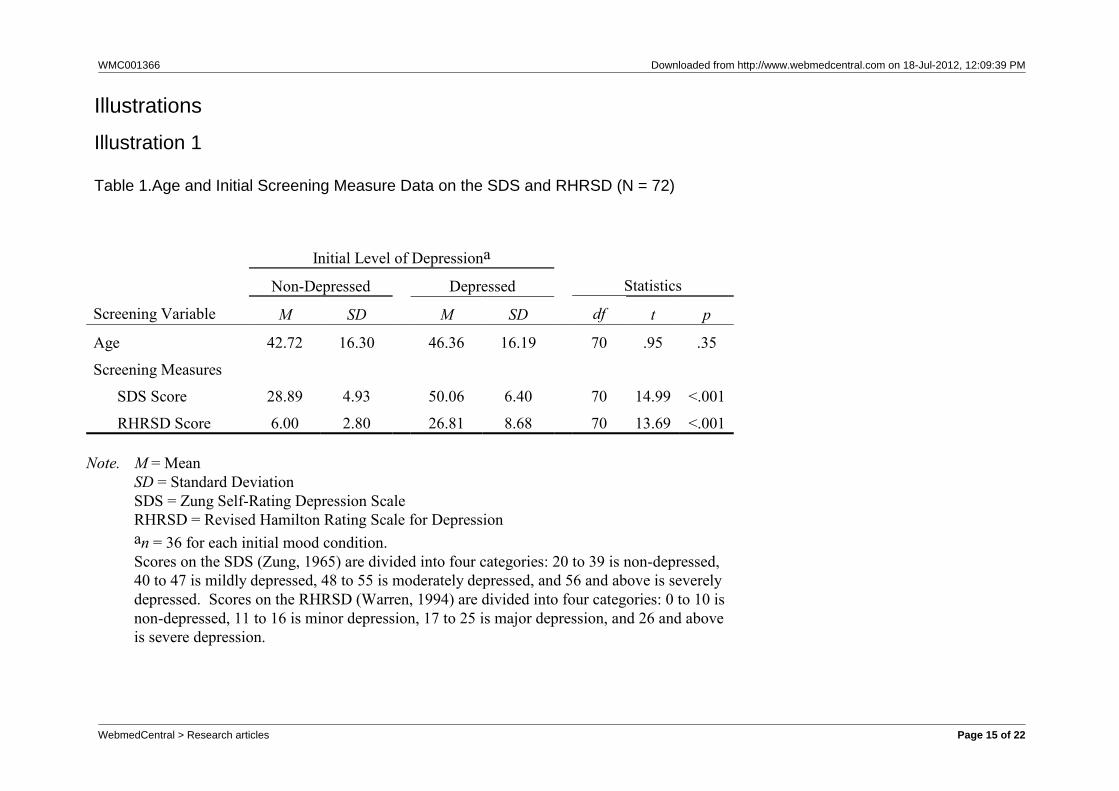
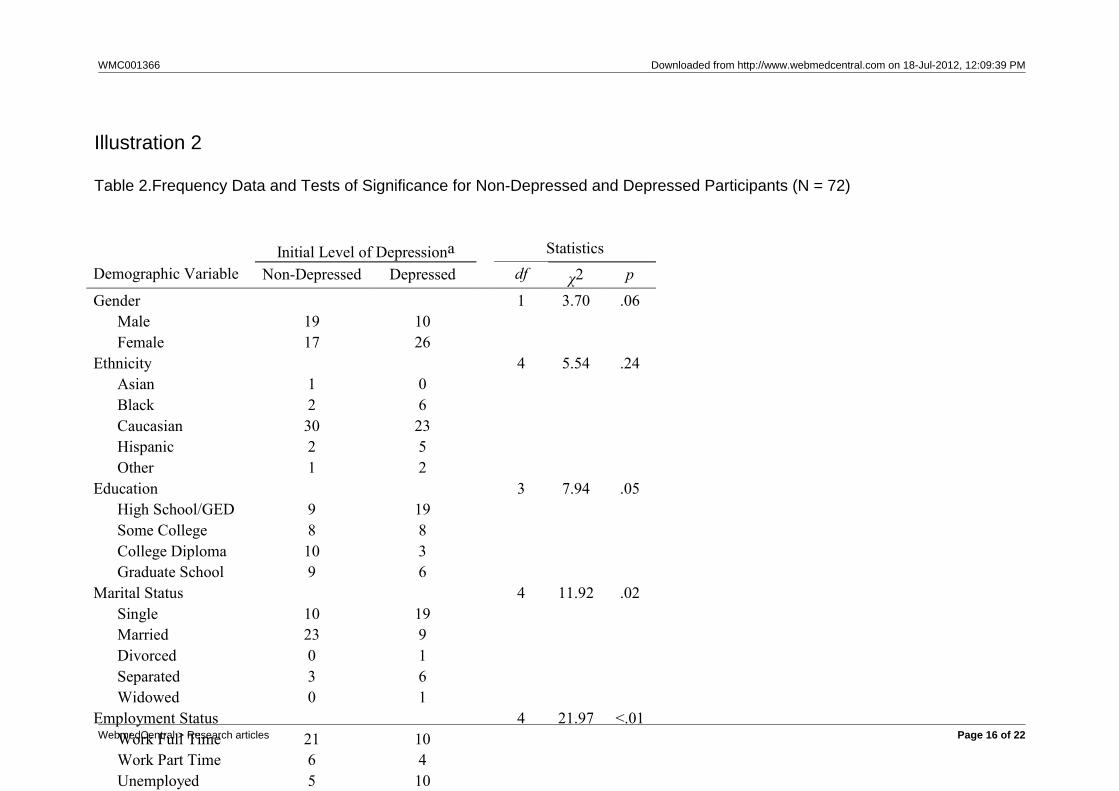
Descriptive statistics generated from the screeningprocedure for the initially depressed and initiallynon-depressed participants are presented in Table 1.Frequency information regarding the demographicmakeup of both groups, and tests of significance todetermine if either of the groups is demographicallydifferent, are presented in Table 2. An examination ofthe demographic characteristics revealed that thedepressed and non-depressed participants differedsignificantly in terms of employment status, χ2 (4) =21.97, p < .01, marital status, χ2 (4) = 11.92, p = .02,and level of education, χ2 (3) = 7.94, p = .05.Di f ferences between the depressed andnon-depressed participants came close to beingstatistically significant within the category of gender, χ2 (1) = 3.70, p = .06. These four variables werecontrolled for in the MANCOVA.Examination of Overall MANCOVADescriptive data for the dependent variables,categorized by the two independent grouping variables,are presented in Table 3. A significant main effect wasobserved for initial level of depression (ILD), L = .83, F(3, 62) = 4.20, p = .01, = .17, 1 - b = .84. Additionally,a significant main effect was observed for vignettecondition (VC), L = .11, F (3, 62) = 171.10, p < .001, =.89, 1 - b = 1.00. These two main effects warrantadditional statistical analysis with separate univariatefactorial ANCOVAs for the three dependent variables.Table 4 provides a table of all obtained F-values forthe MANCOVA and subsequent post-hoc ANCOVAs.Examination of HypothesesHypothesis One. The first hypothesis was thatdepressed participants would have significantly longerStroop interference times than non-depressedparticipants on the modified Stroop card withdepression related words, regardless of whether theywere instructed to respond in a depressed ornon-depressed manner. Hypothesis one was testedwith a univariate factorial ANCOVA. The ANCOVAshowed a significant main effect for ILD on Stroopinterference time for depression related words, F (1,64) = 5.40, p = .02, = .08, 1 - b = .63, which supportsthe hypothesis that, regardless of which vignettecondition participants were exposed to, there is asignificant difference in Stroop interference times fordepressed participants as compared to non-depressedparticipants. Hypothesis Two. The second hypothesis was thatdepressed and non-depressed participants would notdiffer from each other on the modified Stroop card with
neutral words regardless of whether they wereinst ructed to respond in a depressed ornon-depressed manner. This hypothesis was alsosupported by the statistical evidence, as there was nomain effect found for ILD, F (1, 64) = .72, p = .40, =.01, 1 - b = .13, or for VC, F (1, 64) = 1.71, p = .20, =.03, 1 - b = .25. All participants experienced roughlyequal amounts of Stroop interference for the neutralword card. Refer back to Table 3 for the mean amountof Stroop interference time for neutral words for eachexperimental group. Hypothesis Three. The third hypothesis was thatparticipants who were given the depressed vignettewould score significantly higher on the BDI-II thanparticipants who were given the non-depressedvignette, regardless of whether they were initiallydepressed or non-depressed. Even though a maineffect for VC on BDI-II scores was observed, F (1, 64)= 522.19, p < .001, = .89, 1 - b = 1.00, this hypothesiscan not be fully supported by ANCOVA data becauseof a significant ILD × VC interaction, F (1, 64) = 6.69, p= .01, = .10, 1 - b = .72.This hypothesis was further examined by placingparticipants’ BDI-II scores into the descriptivecategories that their scores reflected. Table 5 shows afrequency count of the descriptive categories groupedby the two independent conditions. When examined bydescriptive category, all 18 participants who wereinit ial ly depressed and told to answer in anon-depressed manner were able to complete theBDI-II showing minimal depression. This same findingis true for all 18 non-depressed participants who weretold to respond in a non-depressed manner.Additionally all 18 non-depressed participants, whenasked to answer in a depressed manner, scored in theseverely depressed range on the BDI-II. Of the 18depressed participants who were told to respond in adepressed manner, 14 rated themselves as havingsevere depression, and 4 rated themselves as havingmoderate depression. This finding lends support to thefourth hypothesis. While initially depressed andnon-depressed participants may have slightly differentresponse patterns when fabricating answers, bothgroups ultimately appear capable of altering theirresponses to change their current level of depressionon the BDI-II. Data analysis indicates partial supportfor this hypothesis.Further analysis of this interaction was conducted withtraditional t-tests. Within the VC, it appears thatdepressed participants who were told to respond in adepressed manner (M = 44.28, SD = 14.66) scoredsignificantly higher than depressed participants told torespond in a non-depressed manner (M = 2.94, SD =3.72), t (34) = 11.60, p < .001. Furthermore,
WebmedCentral > Research articles Page 8 of 22

WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
non-depressed participants told to respond in adepressed manner (M = 53.78, SD = 10.00) scoredsignificantly higher than non-depressed participantstold to respond in a non-depressed manner (M = .83,SD = 1.50), t (34) = 22.23, p < .001. Furtherexamination of this interaction was conducted inhypotheses six and seven, which both examine BDI-IIscores within ILD.Hypothesis Four. The fourth hypothesis was that,within the initially depressed group, participants whowere instructed to respond in a depressed andnon-depressed manner would not differ from eachother in Stroop response times for either the neutral ordepression related word cards. It was expected thatthe Stroop is resistant at attempts to manipulate one’sresponses. This finding is initially supported becausethere was no observable main effect for VC for boththe depressed Stroop word card, F (1, 64) = .66, p =.42, = .01, 1 - b = .13, and the neutral Stroop wordcard, F (1, 64) = 1.71, p = .20, = .03, 1 - b = .25.Further t-test analysis confirmed that there was nosignificant difference between depressed Stroopinterference times for depressed participants told torespond depressed (M = 17.55, SD = 14.53) ascompared to depressed participants told to respondnon-depressed (M = 16.16, SD = 13.65), t (34) = .30, p= .77. There was also no significant differencebetween neutral Stroop interference times fordepressed participants told to respond depressed (M =10.40, SD = 11.23) as compared to depressedparticipants told to respond non-depressed (M = 8.83,SD = 9.65), t (34) = .45, p = .65.Hypothesis Five. The fifth hypothesis was that, withinthe initially non-depressed group, participants whowere instructed to respond in a depressed andnon-depressed manner would not differ from eachother in Stroop response times for either the neutral ordepression related word cards. The previouslymentioned fact that no main effect was observed forVC for both the depressed Stroop word card, F (1, 64)= .66, p = .42, = .01, 1 - b = .13, and the neutral Stroopword card, F (1, 64) = 1.71, p = .20, = .03, 1 - b = .25also provides support for this hypothesis.Further t-test analysis confirmed that there was nosignificant difference between depressed Stroopinterference times for non-depressed participants toldto respond depressed (M = 10.03, SD = 13.85) ascompared to non-depressed participants told torespond non-depressed (M = 5.30, SD = 7.22), t (34) =1.29, p = .21. There was a significant differencebetween neutral Stroop interference times fornon-depressed participants told to respond depressed(M = 9.68, SD = 7.04) as compared to non-depressedparticipants told to respond non-depressed (M = 5.09,
SD = 6.32), t (34) = 2.05, p = .05.Hypothesis Six. The sixth hypothesis was that, withinthe depressed vignette condition, participants wouldnot differ from each other in BDI-II scores, regardlessof whether they were initially depressed or initiallynon-depressed. This hypothesis is not supportedbecause of the significant ILD × VC interaction, F (1,64) = 6.69, p = .01, = .10, 1 - b = .72. T-tests wereconducted in order to further examine this interaction.It appears that when an initially depressed participantis told to pretend to be depressed, their scores on theBDI-II (M = 44.28, SD = 14.66) are significantly lowerthan that of an initially non-depressed participant toldto pretend to be depressed (M = 53.78, SD = 10.00), t(34) = -2.27, p = .03.Hypothesis Seven. The seventh and final hypothesiswas that, within the non-depressed vignette condition,participants would not differ from each other in BDI-IIscores, regardless of whether they were initiallydepressed or initially non-depressed. This hypothesisis also not supported because of the significant ILD ×VC interaction, F (1, 64) = 6.69, p = .01, = .10, 1 - b =.72. T-test analysis further revealed that when aninitially depressed participant is told to pretend to benon-depressed, their total BDI-II score (M = 2.94, SD =3.72) is significantly higher than initially non-depressedparticipants told to pretend to be non-depressed (M =.83, SD = 19.47), t (34) = 2.24, p = .03.
Discussion
Study results indicated that the BDI-II was highlysensitive to attempts at manipulation, with varyingdegrees of vulnerability depending on whether theparticipant was initially depressed or non-depressed.More importantly, it was demonstrated that whileparticipants were generally successful at manipulatingresults on the BDI-II, they were unsuccessful atmanipulating response patterns on the modifiedStroop procedure. Regardless of whether theparticipant was told to respond in a depressed ornon-depressed manner, the modified Stroop wassuccessfully able to differentiate between depressedand non-depressed participants.It was hypothesized that depressed participants wouldhave significantly longer Stroop interference times fordepression related words when compared tonon-depressed participants, regardless of whetherthey were told to respond as depressed ornon-depressed. The data analysis supported thishypothesis. This finding was also consistent withprevious research that has shown simi larfindings.25-30
WebmedCentral > Research articles Page 9 of 22

WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
This significant difference suggests that the modifiedStroop procedure was able to assess cognitiveinterference associated with increased levels ofdepression. This interference was expressed byincreased response latency on the depression relatedword card. Information processing theory suggeststhat depressed participants exhibited an attention biasfor depression related material, and this attention biaswas not present in non-depressed participants. Theattention bias that depressed participants possessedlimited the amount of attention they could use to focuson the color-naming task, thus resulting in increasedinterference times. In terms of Beck’s model ofdepression, when depressed participants engaged inthe color-naming task, they were also activating theirschema for depression by inadvertently reading theword-item. When their schema was activated, itcaused processing delays for color naming, thuscreating longer interference times when compared tonon-depressed participants.Additionally, it has been shown that the modifiedStroop procedure was impervious to attempts atmanipulating one’s responses. This finding widens theimplications discussed by Gotlib and McCann26 whenthey demonstrated that participants would only showincreased Stroop interference times if they have ahistory of depressed mood, and not if their mood istemporarily altered to a state of depression. Thecurrent study demonstrated that willful attempts atmanipulating responses did not affect Stroopinterference times.It was also hypothesized that depressed andnon-depressed participants would not differ from eachother on the modified Stroop procedure with neutralwords, regardless of whether they were told torespond as depressed or non-depressed. Thishypothesis was supported. This finding was consistentwith research on the modified Stroop procedure thatdemonstrated participants showed equal amountsinterference for neutral material, regardless of whetheror not the participant was depressed.25-27, 29,30In terms of information processing theory, depressedand non-depressed participants did not show anyattention biases towards neutral material. Therefore,they were all able to focus the same amount ofattention on the color-naming task. Beck’s model ofdepression would assert that these neutral words didnot activate the participants’ schema for depression.Therefore, everyone experienced roughly the sameamount of interference because depressedparticipants did not have the handicap of additionalschema activation when compared to non-depressedparticipants. The task was equally challenging to allparticipants.
It was hypothesized that, within the depressed andnon-depressed groups, participants would not show adifference on Stroop interference times, regardless ofwhether they were instructed to respond in adepressed manner or non-depressed manner. Thisfinding was supported and provided evidence for theability of the modified Stroop procedure to assesswhether a par t ic ipant was depressed ornon-depressed, even if they were trying to mask theirtrue mood. Thus, depressed and non-depressedparticipants were equally poor at influencing theirresponse times on the modified Stroop procedure andthis was consistent with prior research that examinesthe modified Stroop procedure’s ability to measurestate versus trait depression.34 If the modified Stroopprocedure assessed trait depression, as discussed byWilliam and Nulty34, then not only would Stroopinterference times be stable over an extended periodof time, but they would also be resistant to attempts atmanipulation. The modified Stroop procedure indirectlyassessed the development of a person’s schema fordepression. As such, it is difficult to alter over time,and difficult for a person to willfully manipulate.There was one significant difference within the t-testanalysis examining neutral Stroop times. It appearsthat there is a statistically significant differencebetween neutral Stroop interference times fornon-depressed participants told to respond depressedas compared to non-depressed participants told torespond non-depressed. While this finding isstatistically significant, the difference between the twogroups is only 4.59 seconds. This difference is slightlyless than the difference between depressedparticipants told to respond depressed as compared todepressed participants told to respond non-depressed(4.73 seconds). This significant difference may not bedue to any real difference in performance, and may bedue to random statistical effects.These findings demonstrate that the modified Stroopprocedure could be a useful tool for depressionassessment, especially if a researcher or cliniciansuspects the participant may be engaging in deception.From a practical standpoint, all participants (whetherdepressed or non-depressed) possess equally weakabilities in creating deception on the modified Stroopprocedure.According to information processing theory, thissuggests that depressed participants had a stableinformation bias for depression. This bias was presentregardless of whether or not a person was told to “act”depressed or non-depressed. It did not matter how theparticipant willingly tried to act, their attention biascreated interference without the depressed participantbeing able to control this effort.
WebmedCentral > Research articles Page 10 of 22

WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
Finally, it was hypothesized that participants who weretold to respond in a depressed manner would havesignificantly higher scores on the BDI-II thanparticipants who were told to respond in anon-depressed manner, regardless of whether or notthey were initially depressed or initially non-depressed.Analysis of the data provided mixed support for thishypothesis. If one examines actual scores on theBDI-II, it appears that depressed participants scoredslightly higher than non-depressed participants whentold to respond in a depressed manner.Support for this hypothesis occurs when one examinesthe descriptive categories that these BDI-II scoresrepresent. Ultimately, when a depressed participantwas asked to respond in a non-depressed manner,their scores fell in the non-depressed range. When adepressed participant was asked to respond in adepressed manner, all scores fell in the depressedrange. This shows that the BDI-II was highly sensitivetoward attempts at manipulation, and was consistentwith past research specifically examining a person’sability to fabricate results on a BDI.12,13 This findingalso confirms suspicions that were raised in previousresearch regarding a person’s ability to fabricateanswers on paper and pencil psychometric tests.12-15In the present study, all participants were able tochange their response pattern at will.The fact that non-depressed participants were able tosuccessfully fabricate responses on the BDI-IIsupported the research of Lees-Haley13 when it wasobserved that non-depressed participants were adeptat altering their responses on the BDI in order toappear depressed. The current study expands thesefindings one step further by showing that individualswith high levels of depression were equally adept atappearing non-depressed on the BDI-II. These resultsshow that participants of varying levels of educationand various ethnicities were quite capable ofdeliberately manipulating their responses on the BDI-II.Results relevant to the sixth and seventh hypothesesrevealed some unexpected interaction findings wheninitially depressed and non-depressed participantswere asked to fake responses in a particular directionon the BDI-II. However, the overall implication of theseresults is to further support the vulnerability of theBDI-II to intentional response alteration.Limitations of the Current StudyOne potential weakness of the study was that acategorical approach was utilized to distinguishbetween depressed and non-depressed participants.Most current research shows that depression is acontinuous variable, with people falling somewherebetween two extremes of either “completely depressed”or “completely non-depressed.”46,47 The choice to
examine depression categorically was made becausethis reflects the current state of clinical practice inpsychology. In the clinical sphere, individuals areusually diagnosed categorically, not along a continuum.Another potential limitation is our use of the SDS andthe RHRSD self-report inventories in the selection ofthe depressed sample. It might be argued that if weare critiquing the BDI-II as too obtrusive, why usesimilar measures to select depressed participants?This is a valid concern and yet it is hoped that byrelying on two inventories rather than one, theselection error would be somewhat lessened. The lackof available alternative methods of assessingdepression, to some extent, forced a reliance on thetype of measures that we critique.An additional limitation is that this study did not includea control group that was not asked to fake responseson either the BDI-II or the Stroop. Including such acontrol group would be important in future research asit would provide baseline data from which one couldassess the degree to which responses change on theBDI-II and Stroop with willful efforts to distort. Ourexpectation, based upon current findings, is that themagnitude of change of depression level would begreater on the BDI-II than on the Stroop, but this is animportant empirical issue that awaits further research.Clinical Implications and Suggestions forResearchThe results of this study provide evidence to practicingclinicians that they may wish to consider the use ofalternative measures to the BDI-II for assessingdepression when the client they are examining may bemotivated to distort their responses. Since themodified Stroop procedure appears to be relativelyimpervious to attempts at manipulating responsepatterns, it can be considered as a possible aid inguiding a clinician toward a diagnosis. For acceptanceas a clinical measure of depression, it is important tounderstand what the BDI-II and the modified Stroopprocedure measure, and how these scales are used.A needed, but involved, avenue of research would befurther validation of the modified Stroop procedure asa depression assessment tool, and perhaps thedevelopment of standardized Stroop interferencetimes, which would generate cutoff scores that wouldindicate whether or not a person is depressed andtheir level of depression. The establishment of cutoffscores for various levels of depression is a complexundertaking. One possible way of establishing cutoffscores is to have various depressed, non-depressed,samples take a series of depression assessmentdevices along with the Stroop, and to also includesamples with forms of psychopathology other thandepression. One could then compare various levels of
WebmedCentral > Research articles Page 11 of 22
WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
depression, across multiple samples, with responselatencies on the Stroop. One would then be in adefensible position to establish the Stroop’sincremental and discriminant validity after havingassessed a large number of varied samples.Due to the lack of standardized items andstandardized presentation protocols for the modifiedStroop procedure, the amount of Stroop interferencecan vary greatly between studies. Research in thisarea would have to focus on identifying universallyaccepted depression related words, and developingaverage Stroop interference times based ondemographic characteristics for both depressed andnon-depressed populations. Eventually, one may beable to determine if a person exhibits symptoms ofdepression by examining an individual’s discrepancybetween modified Stroop interference times for neutralwords and modified Stroop interference times fordepression related words.A potential methodological improvement might be topresent individual stimuli by computer rather thanhaving participants respond to stimuli on cards, as wasdone in the current study. Jensen,48 for example,presents research on visual and auditory reactiontimes for accessing various cognitive skills and abilityareas. It should be noted that although the Stroop iscomparatively impervious to willful attempts to alterresponses, Jensen’s work suggest that some degreeof response alteration is possible even on “reactiontime” tasks such as the Stroop. A large amount ofresearch using the Stroop to assess emotional states,however, has not relied on computer presentationsand it is for this reason that the card formatpresentation was used here. Nevertheless, the abilityto measure cognitive task performance withinmilliseconds makes the use of computers a promisingavenue of future research.ConclusionIn conclusion, the modified Stroop procedure provedto be resistant to participants’ attempts at fabricatingresponses in order to appear depressed ornon-depressed. The BDI-II was susceptible toattempts at manipulation. While depressed andnon-depressed participants fabricate responses on theBDI-II with slightly different response patterns, allparticipants are capable of achieving the ultimate goalor appearing depressed or non-depressed. Thefindings of this study provide empirical evidence thatthe validity of the BDI-II is weakened in specificsituations, such as when a participant is motivated tofabricate responses, and there are alternativemeasures like the modified Stroop procedure that stillsuccessfully differentiate between depressed andnon-depressed participants in these situations.
References
1. Beck AT, Steer GD, Brown GK. Beck DepressionInventory Manual. 2nd ed. San Antonio, TX: ThePsycholgical Corporation; 1996. 2. Byrne B, Baron P, Balev J. The Beck DepressionInventory: A cross-validated test of second orderfactorial structure for Bulgarian adolescents. EducPsychol Meas. 1998; 58(2):241-251.3. Sanz J, Vasqez C: Fiabilidad, validez, y datosnormativos del Inventario para la Depresion de Beck[Reliability, Validity, and normative data of the BeckDepression Inventory]. Psicothema. 1998;10:303-318.4. Carro IL, Bernal IL, Vea HB: La Depresion in Cuba:Validacion del Inventario de Depresion de Beck y de laEscala de Actitudes Disfuncionales en poblacionCubana [Deppresion in Cuba: Validation of BeckDepression Inventory (BDI) and the DysfunctionalAttitudes Scale (DAS-A) with Cuban population].Avances en Psicologia Clinica Latinoamerica.1998;16:111-120.5. Byrne BM, Stewart SM, Lee PWH: Validating theBeck Depression Inventory-II for Hong KongCommunity adolescents. International Journal ofTesting. 2004;4:199-216.6. Kojima M, Furukawa TA, Takahashi H, Kawai M,Nagaya T, Tokudome S: Cross-cultural validation ofthe Beck Depression Inventory-II in Japan. PsychiatryRes. 2002;110:291-299.7. Cole JC, Grossman I, Prilliman C, Hunsaker E:Multimethod validation of the Beck DepressionInventory-II and Grossman-Cole Depression Inventorywi th an inpat ient sample . Psycho l Rep.2003;93:1115-1129.8. Luty J, O’Gara C: Validation of the 13-Item beckDepression Inventory in alcohol-dependent people. IntJ Psychiatry Clin Pract. 2006;10:45-51.9. Wang YP, Andrade LH, Gorenstein C: Validation oft h e B e c k D e p r e s s i o n I n v e n t o r y f o r aPortuguese-speaking Chinese community in Brazil.Braz J Med Biol Res.2005;38:399-408.10. Endler NS, Macrodimitris SD, Kocovski NL:Depression: The complexity of self-report measures. JAppl Biobehav Res. 2000;5:26-46.11. Rude SS, Covich J, Jarrold W, Hedlund S, ZentnerM: Detecting depressive schemata in vulnerableindividuals: Questionnaires versus laboratory tasks.Cognit Ther Res. 2001;25:103-116.12. Joiner Jr TE, Schmidt KL, Metalsky GI: Low-endspecificity of the Beck Depression Inventory. CognitTher Res. 1994;18:55-68.13. Lees-Haley PR: Malingering traumatic mental
WebmedCentral > Research articles Page 12 of 22
WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
disorder on the Beck Depression Inventory:Cancerphobia and toxic exposure. Psychol Rep.1989;65:623-626.14. Dahlstrom WG, Brooks JD, Peterson CD: TheBeck Depression Inventory: Item order and the impactof response sets: J Pers Assess. 1990;55:224-233.15. Sackeim HA, Gur RC: Self-deception,other-deception, and self-reported psychopathology. JConsult Clin Psychol. 1979;47(1):213-215. 16. Hamilton M: A rating scale for depression. Journalof neurology and neurosurgical psychiatry.1960;23:56-62. 17. Zung WWK, A self-rating depression scale. ArchGen Psychiatry. 1965;12:63-70.18. Beck AT, Cognitive Therapy and EmotionalDisorders. New York, NY: International UniversityPress; 1976.19. Yin P, Fan X: Assessing the reliability of the BeckDepression Inventory scores: Reliability generalizationacross studies. Educ Psychol Meas. 2000;60:201-223.20. Shafer AB: Meta-analysis of the factor structuresof four depression questionnaires: Beck, CES-D,Hamilton and Zung. J Clin Psychol. 2006;62:123-146.21. Dozois DJA, Covin R: The Beck DepressionInventory-II (BDI-II), beck Hopelessness Scale (BHS),and Beck Scale for Suicide Ideation (BSS). In:Hilsenroth MJ, Segal DL, eds. ComprehensiveHandbook of Psychological Assessment, Vol. 2:Personality Assessment. Hoboken, NJ: John Wileyand Sons, Inc;2004.22. Kendall PC, Hollon SD, Beck AT, Hammen CL,Ingram RE: Issues and recommendations regardinguse of the beck Depression Inventory. Cognit TherRes.1987;11:289-299.23. Ritterabnd LM, Spielberger CD: Construct validityof the Beck Depression Inventory as a measure ofstate and trait depression in nonclinical populations.Depression and Stress. 1996;2:123-145.24. Stroop, JR. Studies of interference in serial verbalreactions. J Exp Psychol. 1935;18:643-662.25. Dozois DJA, Dobson KS. Information processingand cognitive organization in unipolar depression:Specificity and comorbidity issues. J Abnorm Psychol.2001;110:236-236.26. Gotlib IH, McCann CD. Construct accessibility anddepression: An examination of cognitive and affectivefactors. J Pers Soc Psychol. 1984;47:427-439.27. Klieger DM, Cordner MD. The Stroop task as ameasure of construct accessibility in depression. PersIndivid Dif. 1990;11:19.27.28. Mogg K, Bradley BP. Attentional bias ingeneralized anxiety disorder versus depressivedisorder. Cognit Ther Res. 2005;29:29-45.29. Segal ZV, Gemar M. Changes in cognitive
organization for negative self-referent materialfollowing cognitive behaviour therapy for depression: Aprimed Stroop study. Cogn Emot. 1997;11:501-516.30. Segal ZV, Gemar M, Truchon C, Guirguis M,Horowitz LM. A priming methodology for studyingself-representation in major depressive disorder. JAbnorm Psychol. 1995;104:205-213.31. Bradley BP, Mogg K, Miller N, White J. Selectiveprocessing of negative information: Effects of clinicalanxiety, concurrent depression, and awareness. JAbnorm Psychol. 1995;104:532-536.32. Doost HTN, Taghavi MR, Moradi AR, Yule W,Dalgleish T. The performance of clinically depressedchildren and adolescents on the modified Stroopparadigm. Pers Individ Dif. 1997;23:753-759.33. Mogg K, Bradley BP, Williams R, Matthews A.Subliminal processing of emotional information in bothanxiety and depression. J Abnorm Psychol.1993;102:304-311.34. Williams JMG, Nulty D. Construct accessibility,depression and the emotional Stroop task: Transientmood or stable structure? Pers Individ Dif.1986;7:485-491. 35. Gotlib IH, Cane DB. Construct accessibility andclinical depression: A longitudinal study. J AbnormPsychol. 1987;96:199-204.36. Larsen RJ, Mercer KA, Balota DA. Lexicalcharacteristics of words used in emotional Stroopexperiments. Emotion. 2006;6:62-72.37. McKenna FP, Sharma D. Reversing the emotionalStroop effect reveals that it is not what it seems: Therole of fast and slow components. J Exp Psychol.2004;29:29-45.38. Waters AJ, Sayette MA, Franken IHA, SchwartzJE. Generalizeability of carry-over effects in theemot ional Stroop task. Behav Res Ther.2005;43:715-732.39. Algom D, Chajut E, Lev S. A rational look at theemotional Stroop phenomenon: A generic slowdown,not a Stroop effect. J Exp Psychol. 2004;133:323-338.40. Phaf RH, Kan J. The automaticity of emotionalStroop: A meta-analysis. J Behav Ther Exp Psychiatry.2007;38:184-199.41. Warren WL. Revised Hamilton Scale forDepression (RHRSD) Manual. Los Angeles: WesternPsychological Services; 1994.42. Butcher JN, Dahlstrom WG, Graham JR, TellegenA, Kaemmer B. The Minnestora MultiphasicPersonality Inventory-2 (MMPI-2): Manual forAdministration and Scoring. Minneapolis: University ofMinnesota Press; 1989.43. Nelson JC, Mazure CM. A scale for rating tricyclicresponse to major depression: The TRIM. J ClinPsychopharmacol. 1990;10:252-260.
WebmedCentral > Research articles Page 13 of 22

WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
44. Thurber S, Snow M, Honts CR. The ZungSelf-Rating Depression Scale: Convergent validity andd iagnost ic d iscr iminat ion. Assessment .2002;9:401-405.45. Kucera H, Francis WN. Computational Analysis ofPresent-Day American English. Providence: BrownUniversity Press; 1967.46. Baldwin G, Shean GD. A taxometric study for theepidemiological studies depression scale. Genet SocGen Psychol Monogr. 2006;132:101-128.47. Solomon A, Ruscio J, Seeley JR, Lewinsohn, PM.A taxonomic investigation of unipolar depression in alarge community sample. Psychol Med. 2006; 36:973-985.48. Jensen AR, Clocking the Mind: MentalChronometry and Individual Differences. Amsterdam,The Netherlands: Elsevier; 2006.
WebmedCentral > Research articles Page 14 of 22
WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
Initial Level of Depressiona
Non-Depressed Depressed Statistics
Screening Variable M SD M SD df t p
Age 42.72 16.30 46.36 16.19 70 .95 .35
Screening Measures
SDS Score
RHRSD Score
28.89
6.00
4.93
2.80
50.06
26.81
6.40
8.68
70
70
14.99
13.69
<.001
<.001
Note. M = MeanSD = Standard Deviation
SDS = Zung Self-Rating Depression Scale RHRSD = Revised Hamilton Rating Scale for Depression
an = 36 for each initial mood condition.Scores on the SDS (Zung, 1965) are divided into four categories: 20 to 39 is non-depressed,40 to 47 is mildly depressed, 48 to 55 is moderately depressed, and 56 and above is severelydepressed. Scores on the RHRSD (Warren, 1994) are divided into four categories: 0 to 10 isnon-depressed, 11 to 16 is minor depression, 17 to 25 is major depression, and 26 and aboveis severe depression.
Illustrations
Illustration 1
Table 1.Age and Initial Screening Measure Data on the SDS and RHRSD (N = 72)
WebmedCentral > Research articles Page 15 of 22
WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
Initial Level of Depressiona StatisticsDemographic Variable Non-Depressed Depressed df χ2 pGender Male Female
1917
1026
1 3.70 .06
Ethnicity Asian Black Caucasian Hispanic Other
123021
062352
4 5.54 .24
Education High School/GED Some College College Diploma Graduate School
98109
19836
3 7.94 .05
Marital Status Single Married Divorced Separated Widowed
1023030
199161
4 11.92 .02
Employment Status Work Full Time Work Part Time Unemployed Disabled Retired
216504
10410120
4 21.97 <.01
Note. an = 36 for each initial mood condition.
Illustration 2
Table 2.Frequency Data and Tests of Significance for Non-Depressed and Depressed Participants (N = 72)
WebmedCentral > Research articles Page 16 of 22
WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
Initial Level of Depressiona
Non-Depressed Depressed
Vignette Condition M SD M SD
Non-Depressed Vignette
BDI-II Score
Neutral Stroop Interference
Depressed Stroop Interference
.83
5.08
5.30
1.47
6.32
7.22
2.94
8.83
16.16
3.72
9.65
13.65
Depressed Vignette
BDI-II Score
Neutral Stroop Interference
Depressed Stroop Interference
53.78
9.68
10.03
10.00
7.04
13.85
44.28
10.41
17.55
14.66
11.23
14.53
Note. M = MeanSD = Standard Deviation
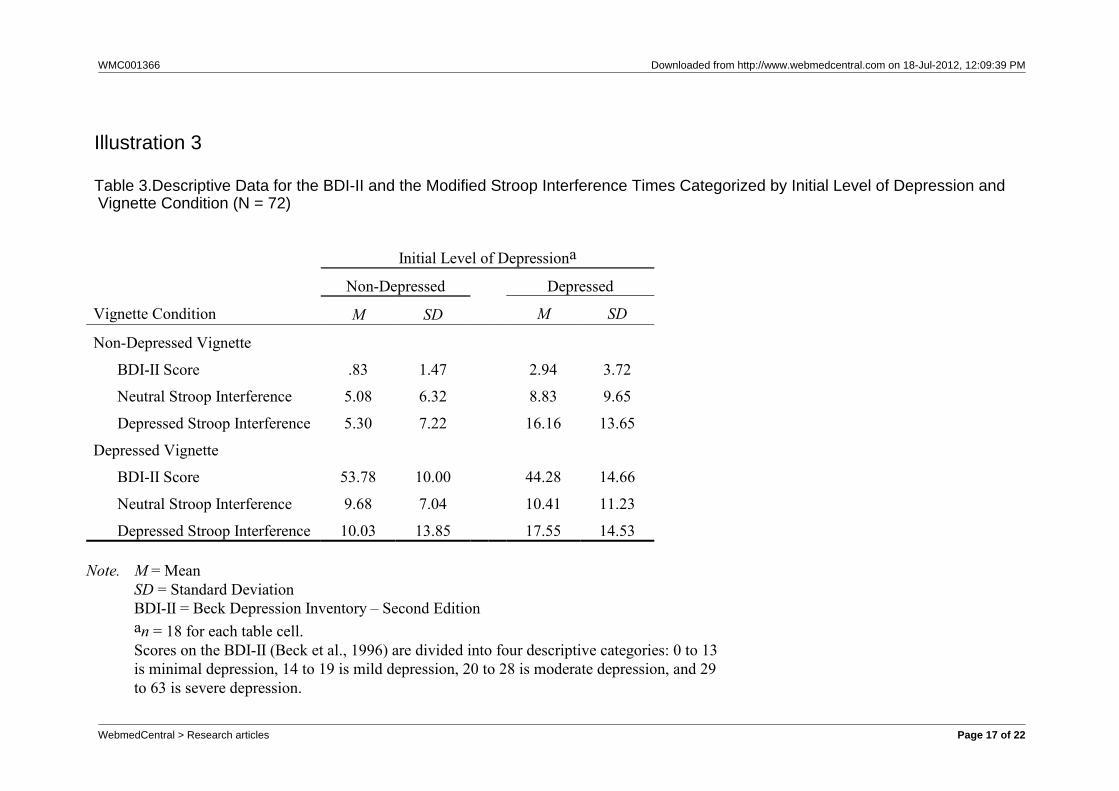
BDI-II = Beck Depression Inventory – Second Editionan = 18 for each table cell.Scores on the BDI-II (Beck et al., 1996) are divided into four descriptive categories: 0 to 13is minimal depression, 14 to 19 is mild depression, 20 to 28 is moderate depression, and 29to 63 is severe depression.
Illustration 3
Table 3.Descriptive Data for the BDI-II and the Modified Stroop Interference Times Categorized by Initial Level of Depression andVignette Condition (N = 72)
WebmedCentral > Research articles Page 17 of 22
WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
df F p 1 –
Overall MANCOVA
Initial Level of Depression (ILD) 3, 62 .83 4.20 .01 .17 .84
Vignette Condition (VC) 3, 62 .11 171.10 <.001 .89 1.00
ILD � VC 3, 62 .90 2.31 .09 .10 .55
Depressed Word Stroop Interference
ILD 1, 64 — 5.40 .02 .08 .63
VC 1, 64 — .66 .42 .01 .13
ILD � VC 1, 64 — .63 .43 .01 .12
Neutral Word Stroop Interference
ILD 1, 64 — .72 .40 .01 .13
VC 1, 64 — 1.71 .20 .03 .25
ILD � VC 1, 64 — .83 .37 .01 .15
BDI-II Scores
ILD 1, 64 — 1.68 .20 .03 .25
VC 1, 64 — 522.19 <.001 .89 1.00
ILD � VC 1, 64 — 6.69 .01 .10 .72
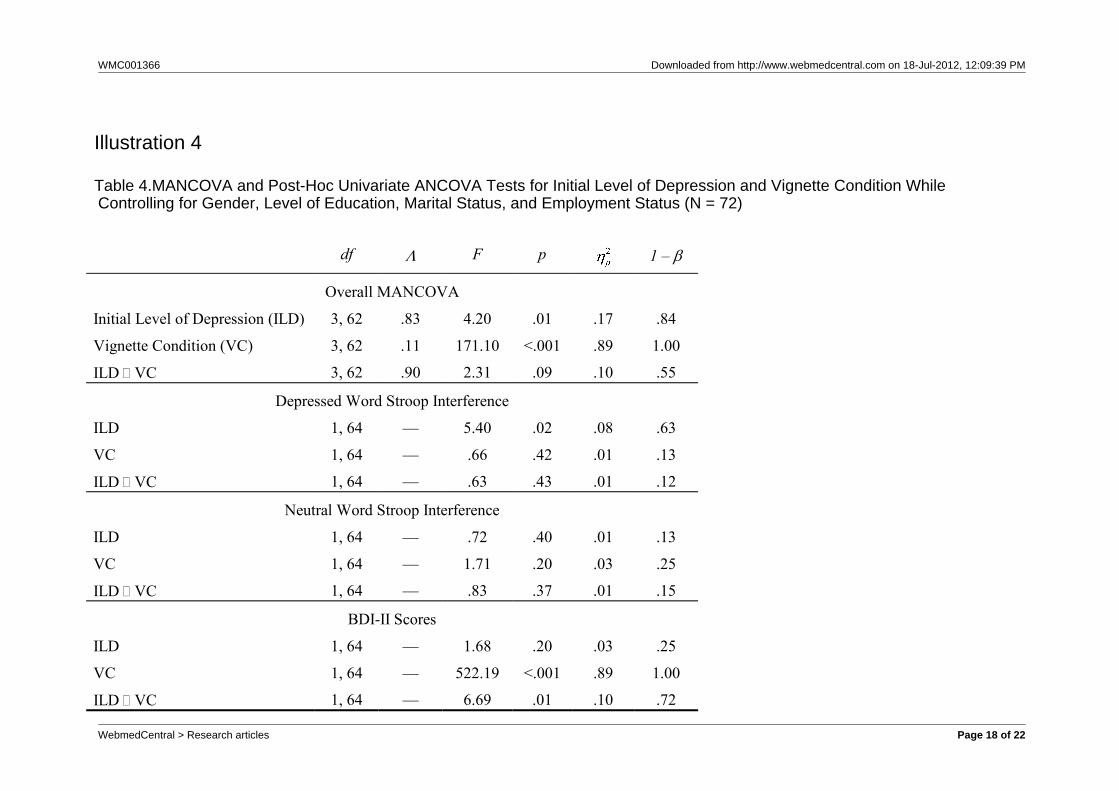
Illustration 4
Table 4.MANCOVA and Post-Hoc Univariate ANCOVA Tests for Initial Level of Depression and Vignette Condition WhileControlling for Gender, Level of Education, Marital Status, and Employment Status (N = 72)
WebmedCentral > Research articles Page 18 of 22
WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
Initial Level of Depressiona
Vignette Condition Non-Depressed Depressed
Non-Depressed Vignette
Minimal Depression
Mild Depression
Moderate Depression
Severe Depression
18
0
0
0
18
0
0
0
Depressed Vignette
Minimal Depression
Mild Depression
Moderate Depression
Severe Depression
0
0
0
18
0
0
4
14
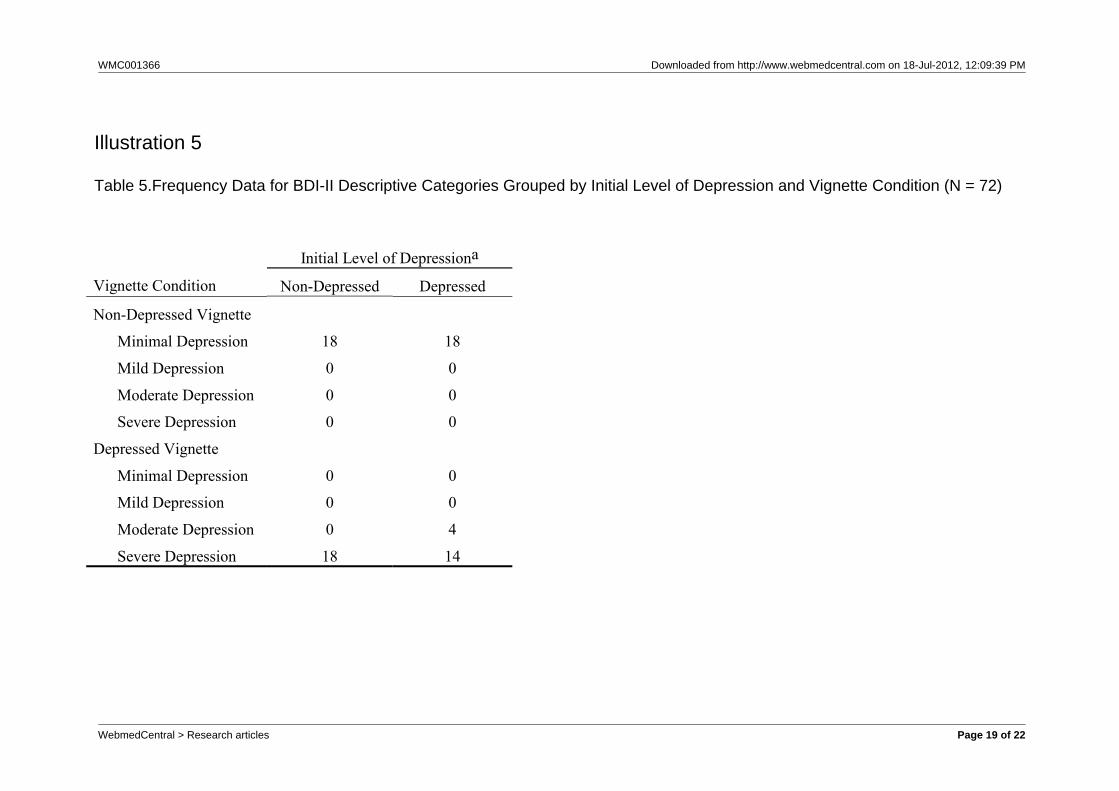
Note. BDI-II = Beck Depression Inventory – Second Editionan = 18 for each table cell.Scores on the BDI-II (Beck et al., 1996) are divided into four descriptive categories: 0 to 13is minimal depression, 14 to 19 is mild depression, 20 to 28 is moderate depression, and 29to 63 is severe depression.
Illustration 5
Table 5.Frequency Data for BDI-II Descriptive Categories Grouped by Initial Level of Depression and Vignette Condition (N = 72)
WebmedCentral > Research articles Page 19 of 22
WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
In this study, you are being asked to imagine that you are having a psychological evaluation by yourinsurance company. Your insurance has instituted a new policy, and has mandated everyone toundergo a psychological evaluation to determine if any of the company’s customers requirepsychotherapy. One way a person can receive therapy is if they have an emotional disorder, such asdepression. However, you feel that you do not need any therapy and are able to handle your lifeproblems on your own. The psychologist conducting the evaluation has presented you with twotests and tells you that these tests will determine whether or not you have an emotional disorder. Complete the following tests so the results ensure that it will appear that you do not have anemotional disorder.
Illustration 6
Appendix A.Vignette that Minimizes Depressive Symptoms
WebmedCentral > Research articles Page 20 of 22
WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
In this study, you are being asked to imagine that you are having a psychological evaluation by yourinsurance company. Your insurance has instituted a new policy, and has mandated everyone toundergo a psychological evaluation to determine if any of the company’s customers requirepsychotherapy. One way a person can receive therapy is if they have an emotional disorder, such asdepression. Coincidently, you feel that you need therapy because you are unable to handle your lifeproblems on your own. The psychologist conducting the evaluation has presented you with twotests and tells you that these tests will determine whether or not you have an emotional disorder. Complete the following tests so the results ensure that it will appear that you have anemotional disorder.
Illustration 7
Appendix B.Vignette that Maximizes Depressive Symptoms
WebmedCentral > Research articles Page 21 of 22

WMC001366 Downloaded from http://www.webmedcentral.com on 18-Jul-2012, 12:09:39 PM
DisclaimerThis article has been downloaded from WebmedCentral. With our unique author driven post publication peerreview, contents posted on this web portal do not undergo any prepublication peer or editorial review. It iscompletely the responsibility of the authors to ensure not only scientific and ethical standards of the manuscriptbut also its grammatical accuracy. Authors must ensure that they obtain all the necessary permissions beforesubmitting any information that requires obtaining a consent or approval from a third party. Authors should alsoensure not to submit any information which they do not have the copyright of or of which they have transferredthe copyrights to a third party.
Contents on WebmedCentral are purely for biomedical researchers and scientists. They are not meant to cater tothe needs of an individual patient. The web portal or any content(s) therein is neither designed to support, norreplace, the relationship that exists between a patient/site visitor and his/her physician. Your use of theWebmedCentral site and its contents is entirely at your own risk. We do not take any responsibility for any harmthat you may suffer or inflict on a third person by following the contents of this website.
WebmedCentral > Research articles Page 22 of 22