Embed Size (px)
Citation preview
1
A Comprehensive Overview of the Risks and Benefits of Coffee Consumption 1
2
Authors: L. Kirsty Pourshahidi*1, Luciano Navarini2, Marino Petracco2 & JJ Strain1 3
4
Affiliations: 1Northern Ireland Centre for Food and Health (NICHE), University of Ulster, 5
Coleraine, BT52 1SA, UK 6
2illycaffè s.p.a, Trieste, Italy 7
8
*Corresponding author: Dr Kirsty Pourshahidi, Room W2038, Northern Ireland Centre for 9
Food and Health (NICHE), University of Ulster, Coleraine, BT52 1SA, UK 10
Tel: +44 (0) 28 7012 4030; Fax: +44 (0) 28 7012 4965; Email: [email protected] 11
12
13
Short title: Coffee consumption and human health 14
15
Keywords: Coffee; human; health; risk; benefit 16
17
18
19
Manuscript number: CRF3-2015-1797.R1 20
21
22
23
24
Word count (including abstract & references, but excluding tables & figures): 11,657 25
Number of tables: 10 26
Number of figures: 1 27
Supplementary documents: 1 (pdf file) 28
2
Contents: 29
30
ABSTRACT 31
1. Introduction 32
2. Methods 33
3. Results 34
3.1. Cancer 35
3.2. Cardiovascular disease (CVD) 36
3.3. Metabolic health 37
3.4. Neurological disorders 38
3.5. Gastrointestinal conditions 39
3.6. Liver disorders 40
3.7. Mortality 41
3.8. Other conditions/health outcomes 42
3.9. Additional risks 43
4. Conclusions 44
5. Future work 45
6. Acknowledgements 46
7. Author contributions 47
8. References 48
3
ABSTRACT 49
Findings on both the health benefits and the potentially harmful effects of coffee consumption 50
have been contradictory. However, the general scientific consensus is that moderate, regular 51
coffee drinking by healthy individuals is either essentially benign or mildly beneficial. Results 52
and generalizations are complicated by a number of factors, including differences in age, 53
gender, health status, type of coffee preparation, serving size, source of coffee. Coffee may 54
have potential health benefits as well as risks, but causality cannot be established for either 55
with the research currently available as these are largely based on observational data. This 56
review aimed to provide a comprehensive overview of the risks and benefits of coffee 57
consumption on health outcomes. A systematic search [search terms: ‘coffee’ OR ‘coffee adj3 58
(consum* or intake* or drink*)] of the literature (from 1970; humans; in English) using the 59
electronic databases ‘OVID’, ‘CINAHL’, and ‘Web of Knowledge’ returned 12,405 results. 60
Duplicates were removed, studies were screened (based on inclusion/exclusion criteria) and 61
the remaining eligible studies (n=1,277) were used to collate an exhaustive list of the potential 62
health benefits and risks of coffee consumption, which were grouped and are discussed with 63
regard to major diseases/conditions (mortality, CVD, cancer and metabolic/liver/neurological 64
disorders), at-risk/vulnerable groups, and specific coffee constituents. This qualitative 65
assessment has shown that the health benefits (or null effects) clearly outweigh the risks of 66
moderate coffee consumption in adult consumers for the majority of health outcomes 67
considered. Results from this research may aid further qualitative and quantitative 68
deterministic risk-benefit assessments of coffee consumption. 69
70
250 words 71
4
1. Introduction 72
Coffee is a widely consumed beverage worldwide and extensive scientific research has 73
been conducted to examine the relationship between coffee consumption and a wide range of 74
chronic diseases and health outcomes, including total mortality, many cancers, 75
cardiometabolic risk, liver disorders, and neurological conditions. Such effects have been 76
attributed to many different bioactive constituents of coffee, including caffeine 77
(methylxanthine), chlorogenic acids (polyphenol), diterpenes, and other phenolics, some of 78
which may also potentially have additive or synergistic effects. 79
Although both findings on the potential health benefits and harmful effects of coffee 80
consumption have historically been reported, the general consensus is that moderate, regular 81
coffee drinking by healthy individuals is either essentially benign or mildly beneficial (George 82
and others 2008; Cano-Marquina and others 2013; O'Keefe and others 2013; Fardet and 83
Boirie 2014). Findings to-date are largely based on observational data, albeit from large 84
prospective cohort studies as well as case-control and cross-sectional data. However, 85
heterogeneity between study populations and designs, and also lack of control for many other 86
confounding factors, add limitations to the existing literature. Moreover, studies or meta-87
analyses to-date typically focus on single disease outcomes or endpoints and few (if any) 88
weigh up the benefits and risks on multiple health outcomes. 89
Therefore, the aim of this review was to provide a comprehensive overview of the risks and 90
benefits of coffee consumption on health outcomes. 91
92
2. Methods 93
A systematic search for the appropriate literature (from 1970, limited to humans and 94
available in English) was conducted using the online electronic databases ‘OVID’ (AMED, 95
FSTA, EMBASE, MEDLINE (PubMED), PSYCinfo), ‘CINAHL’ (academic journals only), and 96
‘Web of Knowledge: Web of Science with Conference Proceedings’, together with manual 97
searches of reference lists. 98
5
Searches were conducted using coffee as a broad search term, or within 3 words of 99
consumption/consume(r), intake(s) or drink(s) [‘coffee’ OR ‘coffee adj3 (consum* or intake* or 100
drink*)]. Duplicates were then removed, and remaining studies were screened for eligibility 101
based on set inclusion and exclusion criteria (Table 1). To be eligible for inclusion, studies 102
must have been conducted in humans and have reported original data linking the effect of 103
coffee consumption on a specified health outcome(s). All types of coffee were included as 104
relevant (such as instant, filtered, cafetiere, or boiled), although those studies concerned with 105
the effect of caffeine per se, were excluded. 106
Eligible studies were then qualitatively evaluated and were used to collate an exhaustive 107
list of the potential health benefits and harmful effects of coffee consumption. Health benefits 108
and risks were grouped and discussed with regard to: 109
total mortality; 110
cardiovascular disease (CVD); 111
cancers; 112
metabolic health (for example, diabetes, metabolic syndrome, insulin resistance, 113
weight gain); 114
liver disorders (for example, non-alcoholic fatty liver disease, cirrhosis); 115
gastrointestinal conditions (for example, peptic/gastric ulcers, dyspepsia, bowel 116
function); 117
neurological disorders (for example, Alzheimer’s disease, dementia, cognitive 118
function/decline, mental health); 119
other miscellaneous health outcomes/conditions. 120
121
Additional risks of coffee consumption were also discussed according to at-risk/vulnerable 122
groups (for example, pregnancy, elderly) and specific ‘bioactive’ constituents identified during 123
the literature search (such as, caffeine, diterpenes, acrylamide, furan, mycotoxins). 124
125
6
3. Results 126
The study selection and screening process is illustrated in Figure 1. Initially, 12,329 results 127
were returned following the literature searches. An additional 76 studies were identified by 128
email alerts updating the searches within the Web of Knowledge database (total, n=12,405 129
studies). 130
After screening to remove duplicate citations (n=6,047) and exclusion of the studies 131
deemed unsuitable for inclusion (n=5,081) based on the pre-determined inclusion/exclusion 132
criteria, a total of 1,277 studies were included in the review. This represented approximately 133
10% of those studies identified by the original search strategy. 134
For each category of the health conditions/outcome discussed below, example citations 135
are included to highlight the key points. A complete bibliography list of all studies reviewed is 136
included as Supplementary Material. 137
138
3.1. Cancer 139
Coffee consumption has been linked to cancer risk or incidence in virtually every tissue 140
type in the body, with the most commonly reported sub-sites being colorectal, bladder/urinary 141
tract, pancreatic, and female-specific and breast cancers. A total of 352 (27.6%) studies have 142
reported links between coffee consumption and cancer, and these are typically observational 143
(Table 2). Only the more mechanistic studies are tested using an intervention study design. 144
Observational findings have for the majority reported a beneficial or null effect of coffee 145
consumption on cancer, with the exception of bladder/urinary tract cancers where the risks of 146
coffee consumption are more commonly reported. An increased risk of bladder/urinary 147
cancer, however, was typically only reported in males, not females (Hartge and others 1983; 148
Marrett and others 1983; Clavel and Cordier 1991; Zeegers and others 2001) and non-149
smokers compared to smokers (Pujolar and others 1993). Negative interactions with alcohol 150
(Donato and others 1997) were also evident, together with an influence of certain genetic 151
polymorphisms (such as CYP1A2) (Pavanello and others 2010). Moreover, other studies only 152
reported an increased risk of cancer of the urinary system to be evident in consumers of 153
7
Turkish coffee (Akdas and others 1990), high coffee consumers (40+ cups per week) (Slattery 154
and others 1988) or have failed to demonstrate a dose-response (Simon and others 1975; 155
D'Avanzo and others 1992) which suggested that such associations are noncausal. 156
Similar modifiers of risk are also noted in the observational evidence for other types of 157
cancer. Coffee drinking appears to increase the risk of gastric (Galanis and others 1998) and 158
colorectal cancer in men (Slattery and others 1990; Boutron-Ruault and others 1999; Yamada 159
and others 2014) but not in women (Lee and others 2007), although the authors queried if the 160
former was just a chance finding (Galanis and others 1998). The risk of pancreatic cancer 161
also appears to be higher in smokers (Gorham and others 1988; Harnack and others 1997) 162
and non consumers of alcohol (Clavel and others 1989), whilst genetic polymorphisms 163
(CYP1A2 and GSTM1/GSTT1) can modify the relationship between coffee consumption and 164
risk of breast (Kotsopoulos and others 2007; Bageman and others 2008; Ayari and others 165
2013), ovarian (Goodman and others 2003) and skin (Fortes and others 2009, 2013) cancer. 166
In some instances, only caffeinated coffee appears to be protective when compared with 167
decaffeinated coffee (for example, in skin, endometrial and some gastric cancers) (Abel and 168
others 2007; Bhoo-Pathy and others 2015; Sanikini and others 2015) but in other studies, the 169
opposite is true (for example, for ovarian, rectal and lung cancers) (Michels and others 2005; 170
Baker and others 2005; Baker and others 2007). Comparisons between other types of coffee 171
preparations also produce equivocal results within the literature, for example for boiled (not 172
filtered) versus filtered coffee (Nilsson and others 2010; Tverdal 2015) or hot versus iced 173
coffee (Green and others 2014), and risks are also typically associated with heavy coffee 174
consumption (Gullo and others 1995; Efird and others 2004; Luo and others 2007; Lueth and 175
others 2008; Bissonauth and others 2009) or coffee abuse (Uzcudun and others 2002) 176
compared to light/moderate coffee consumption. Finally, for some cancers, risks also appear 177
to be more apparent in younger adults (<60 years) (Gallus and others 2007), with a null or 178
beneficial (inverse) effect of coffee consumption on cancer risk becoming apparent only in 179
older adults after more than 35 years coffee consumption (Kokic and others 1996), or in post- 180
compared to pre-menopausal females (Kuper and others 2000; Koizumi and others 2008). 181
8
More consistently, positive or beneficial associations between coffee consumption and 182
cancer risk are evident in the mechanistic studies, and as alluded to above, this evidence more 183
often than not comes from intervention studies. Such research reports a protective or 184
beneficial effect of coffee consumption on antioxidant status (Bakuradze and others 2011), 185
oxidative DNA damage (Steinkellner and others 2005; Hoelzl and others 2010; Misik and 186
others 2010; Bakuradze and others 2011; Hori and others 2014), urine mutagenicity 187
(Aeschbacher and Chappuis 1981) and DNA strand breaks/integrity (Bakuradze and others 188
2014, 2015). Overall, these data from intervention studies would suggest that coffee can have 189
a beneficial role in terms of reducing the risk of some cancers. 190
191
3.2. Cardiovascular disease (CVD) 192
A total of 273 (21.4%) studies have reported links between coffee consumption and CVD, 193
and they are mainly observational, although some evidence from intervention studies is 194
reported, particularly for hyperlipidemias, hypercholesterolemia, and blood pressure (Table 3). 195
Such studies have reported on a number of different outcomes or disease endpoints, ranging 196
from mechanistic studies focusing on individual risk factors (or causes of such) to those 197
reporting adverse events such as myocardial infarction, heart failure, or stroke. 198
Within CVD, the majority of evidence has reported negative (or null) associations between 199
coffee consumption and blood cholesterol (that is, an increased risk of hypercholesterolemia). 200
Such inverse associations though are mainly caused by the consumption of cafetiere (Urgert 201
and others 1995, 1996), French-press (De Roos and others 2000), Arabic (el Shabrawy Ali 202
and Felimban 1993) or boiled coffee (Bonaa and others 1988; Bak and Grobbee 1989; 203
Pietinen and others 1990; Lindahl and others 1991; Van Dusseldorp and others 1991; Ahola 204
and others 1991; Fried and others 1992), as compared to filtered coffee preparations. A direct 205
dose-dependent effect is also evident (Aro and others 1990; D'Avanzo and others 1993) and 206
another study has quantified a 1.66 and 1.58 mg/dL increase in LDL-cholesterol per daily cup 207
of coffee consumed by men and women, respectively (Berndt and others 1993). Moreover, 208
abstinence from coffee for at least 6 weeks will lower cholesterol concentrations in the general 209
9
population (Christensen and others 2001) as well as in hypercholesterolemic patients (Forde 210
and others 1985). This negative effect of coffee on cholesterol concentrations, particularly 211
from boiled coffee, is owing to higher concentrations of diterpenes (kahweol and cafestol) in 212
such coffee preparations (deGroot and others 1996; Gross and others 1997; Naidoo and 213
others 2011). On the other hand, 4 randomized controlled trials have shown that diterpenes 214
have lipoprotein(a)-reducing potential, but the authors concluded that their well-known 215
adverse side effects on LDL cholesterol preclude their use as such (Urgert and others 1997). 216
Of interest, an inverse relationship has been reported between coffee consumption and 217
triglyceride concentrations (Carson and others 1994; Lancaster and others 1994; Miyake and 218
others 1999) which requires further investigation. 219
Risks of raised blood pressure/hypertension in coffee consumers are also apparent within 220
the literature, and this pressor effect may be caused by a coffee-induced increase in 221
adrenaline concentrations (Smits and others 1986a; Smits and others 1986b; Palatini and 222
others 2009). The pressor effect, however, was observed more often than not in coffee naïve 223
individuals, with no effect seen in habitual drinkers (Corti and others 2002) or those who have 224
adapted to heavy coffee consumption (8 cups per day for 4 weeks) (Ammon and others 1983). 225
Furthermore, whilst abstinence from coffee for 9 weeks was able to decrease blood pressure 226
in normotensives (Bak and Grobbee 1990), others have shown no effect on ambulatory blood 227
pressure measurements (Eggertsen and others 1993), nor on the prospective risk of 228
developing hypertension over 33 years (Basile 2002). Indeed, benefits of coffee consumption 229
on blood pressure have also been reported in human intervention studies conducted in both 230
normotensive and mildly hypertensive adults (Awaad and others 2011), as well as in coffee 231
drinkers with the rapid *1A/*1A genotype, compared to the increased risk observed in those 232
with the slow CYP1A2*1F genotype (rapid versus slow caffeine metabolizers, respectively) 233
(Palatini and others 2009). 234
Coffee consumers also appear to be at an increased risk of higher homocysteine 235
concentrations, an independent risk factor for CVD (Strandhagen and others 2003; 236
Strandhagen and others 2004; Slow and others 2004). This relationship may be driven by the 237
10
chlorogenic acid (Piters and others 1985) rather than the trigonelline content of coffee (Slow 238
and others 2004), but, can be modified by folic acid (Strandhagen and others 2003), 239
particularly in those with the TT polymorphism of the methylenetetrahydrofolate reductase 240
(MTHFR) gene which codes for the MTHFR enzyme. 241
For some outcomes (such as myocardial infarction), the increased risk seen in coffee 242
drinkers is dependent on family history (Azevedo and Barros 2006), CYP1A2 genotype 243
(Cornelis and others 2006) and type of coffee preparation (boiled versus filtered) (Hammar 244
and others 2003), thus highlighting the importance of adequately controlling for these and 245
other confounders in such studies. Although, coffee polyphenols (extracted from green coffee 246
beans and given as a single oral ingestion) have been reported to have a beneficial effect on 247
endothelial function (Ochiai and others 2014), the opposite or at least a null effect is seen 248
when either caffeinated or decaffeinated coffee, respectively, is consumed as a beverage 249
(Buscemi and others 2010). For other outcomes, U- or J-shaped risks of coffee consumption 250
have been reported (Panagiotakos and others 2003; Enga and others 2011). Although such 251
a relationship would suggest that the cardiovascular benefits are achieved by moderate 252
(compared to null/little or heavy/high) coffee consumption, differences in the definition of 253
‘moderate consumption’ make it difficult to compare and draw adequate conclusions between 254
the studies. 255
256
3.3. Metabolic health 257
The vast majority of evidence investigating coffee consumption and metabolic health (Table 258
4) consistently shows a beneficial (inverse) association with the risk of type 2 diabetes (n=126; 259
9.9% studies). These associations are at least in part mediated by a decreased insulin 260
resistance (or improved insulin sensitivity) and/or improved glucose tolerance. Direct effects 261
on glucose tolerance appear to be caused by the antagonistic effect of chlorogenic acid 262
(with/without caffeine) on glucose transport, shifting glucose absorption to more distal parts of 263
the intestine (Johnston and others 2003), rather than acting through the incretin hormones. 264
Other mechanisms of action suggested include associations with low-grade systematic 265
11
inflammation (C-reactive protein and sCD163) (Arsenault and others 2009; Chacon 2014), 266
oxidative stress (Bakuradze and others 2011) and sex-hormone binding globulin (Goto and 267
others 2011, 2014). Results may also be different depending on the range of body mass index 268
(BMI) categories included within the study (Arsenault and others 2009; Otake and others 269
2014), as well as the use of hormone replacement therapy (HRT) (Catalano and others 2008; 270
Arsenault and others 2009), again highlighting these as important confounders. 271
Coffee intake (3 x 250 mL/day for 4 weeks) can also decrease energy intake, by improving 272
satiety hormones (ghrelin and serotonin) and therefore decreasing levels of body fat 273
(Bakuradze and others 2014). Moreover, others have shown that either the 274
mannooligosaccharides (Kumao and Fujii 2006) or polyphenols (chlorogenic acid) (Soga and 275
others 2013) in coffee can increase or stimulate postprandial fat utilization, thus promoting 276
excretion of fat in the feces. 277
Although some studies have shown an adverse effect on the risk of metabolic syndrome, 278
this has only been shown, for example, for higher coffee consumption (>3 cups/day), 279
particularly of instant coffees with excess sugar and powdered creamer (Kim and others 2014), 280
and therefore these results must be interpreted with caution. 281
282
3.4. Neurological disorders 283
Coffee consumption has been positively linked to improvements in (or a decreased risk of) 284
a number of neurological disorders, with the most commonly reported being Parkinson’s 285
disease, cognitive decline/function and mental health. A total of 94 (7.4%) studies have 286
reported links between coffee consumption and neurological outcomes, and they are typically 287
observational (Table 5). 288
Overall, coffee has been shown to be beneficially associated with the risk of Parkinson’s 289
disease (Ross and others 2000; Tan and others 2003; Hosseini Tabatabaei and others 2013; 290
van der Mark and others 2014), with a dose-response protective relationship apparent (Tan 291
and others 2003), but possibly only in males (Savica and others 2013; Ascherio and others 292
2001) and female non-HRT users (Ascherio and others 2004; Ascherio and others Mar 2003). 293
12
Additive effects were also apparent with preceding diabetes (D'Amelio and others 2009) and 294
smoking (Grandinetti and others 1994; Powers and others 2008). Whilst some studies 295
reported an effect of certain genetic polymorphisms (for example, adenosine A2A receptor, 296
CYP1A2, and AP06) (Tan and others 2006; McCulloch and others 2008; Popat and others 297
2011), others have shown no such generic-environmental interactions (Facheris and others 298
2008; Chung and others 2013). The protective effect of coffee on the risk of Parkinson’s 299
disease is at least in part due to certain alkaloid compounds within coffee acting as 300
monoamine oxidase (MAO) inhibitors (Herraiz and Chaparro 2006). 301
The protective effect of coffee on cognitive decline/function may be more apparent in 302
females compared to males (Johnson-Kozlow and others 2002; Arab and others 2011) and 303
such effects on psychomotor/cognitive performance (Natu and Agarwal 1997) are more likely 304
to be due to caffeine consumption (Johnson-Kozlow and others 2002), rather than the 305
chlorogenic acids within coffee (Camfield and others 2013). Furthermore, it has been 306
postulated that antioxidants in coffee capable of decreasing reactive oxygen species may give 307
rise to a reduction in the risk of Alzheimer’s disease (Kotyczka and others 2011). 308
309
3.5. Gastrointestinal (GI) conditions 310
GI complaints have been traditionally linked in the literature with coffee consumption, with 311
null/adverse associations with reflux, ulcers, heartburn and dyspepsia most commonly 312
reported. A total of 73 (5.7%) studies have reported links between coffee consumption and 313
GI conditions, the majority being observational studies (Table 6). 314
While negative findings are apparent, suggesting an increased risk of GI complaints in 315
coffee consumers, such negative associations are weak at best, and are only reported in 316
univariate, not multivariate analyses (Bhatia and others 2011); for (unusually) high coffee 317
consumption (Schlemper and others 1996); they are perceived side effects by the consumer 318
or patient rather than being tested/diagnosed (Ostensen and others 1985; Eisig and others 319
1989; Sihvo and Hemminki 1999); or they are only reported in coffee-sensitive/susceptible 320
individuals (Cohen 1980; DiBaise 2003). Moreover, some of the adverse effects are from 321

13
acute feeding studies where coffee is either directly instilled into the stomach or given intra- 322
or orogastrically (Cohen 1980; Coffey and others 1986; Boekema and others 2001) so results 323
are not comparable to normal habitual coffee consumption. Others have suggested that 324
variability in coffee-induced gastric responses may be caused by differences in bean 325
processing (Van Deventer and others 1992; DiBaise 2003; Rubach and others 2014), such as 326
dark or light roasting. 327
Lastly, beneficial effects of moderate coffee consumption on gut health offer some promise 328
for additional benefits of coffee drinking among the general population. Such effects have 329
been reported by 4 intervention studies to-date and include improvements in the fecal 330
microbiota (Umemura and others 2004; Jaquet and others 2009; Walton and others 2010), as 331
well as improved colonic fermentation (Scazzina and others 2011). These positive findings 332
warrant confirmation in larger, and longer-term studies. 333
334
3.6. Liver disorders 335
A total number of 72 (5.6%) studies have investigated the effect of coffee consumption 336
on liver disorders, namely, liver function/enzymes in general and gallstones/gallstone disease 337
(Table 7). Overall, this evidence, largely from observational studies, is showing coffee to have 338
a protective effect on the liver. In general, coffee may offer protection against alcohol-induced 339
liver damage/impairment (Corrao and others 1994; Tanaka and others 1998; Honjo and others 340
2001; Klatsky and others 2006; Ikeda and others 2010; Marotta and others 2013) and alcohol-341
induced hepatic inflammation (Maki and others 2010), which does not appear to be related to 342
the caffeine content (Corrao and others 2001; Xiao and others 2014), or antioxidant activity 343
(Gutierrez-Grobe and others 2012). In some studies, such beneficial effects are more evident 344
in males (Pintus and Mascia 1996; Danielsson and others 2013) and smokers (Kono and 345
others 1994), compared to females and non smokers respectively. Strong cafetiere (versus 346
filtered) coffee, however, may show the opposite effect. Drinking 5-6 cups per day negatively 347
affected the integrity of liver cells in a 24-week randomized-controlled intervention study 348
(Urgert and others 1996). There is debate in the literature, however, if the compounds which 349
14
might be responsible for such effects are the diterpenes, e.g. kahweol within coffee oil (Urgert 350
and others 1996; Boekschoten and others 2004). 351
352
3.7. Mortality 353
Overall, coffee consumption has been associated with a reduced risk of total/all-cause 354
and cause-specific mortality, particularly for CVD and coronary heart disease (CHD) (n=62; 355
4.9% studies) (Table 8). In contrast, in some of the earlier studies conducted 20+ years ago, 356
CHD or ischemic heart disease (IHD) mortality was inversely associated with coffee 357
consumption (Heyden and others 1976; Hennekens and others 1976; Hemminki and Pesonen 358
1977; LeGrady and others 1987; Tverdal and others 1990; Klatsky and others 1993). In these 359
studies, however, risks were related to sale of coffee, not consumption (Hemminki and 360
Pesonen 1977), none/very low (0-1 cups) or very high (6-9+ cups) daily consumption (LeGrady 361
and others 1987; Tverdal and others 1990), or associated risks were minimal (Hennekens and 362
others 1976) and therefore results should be interpreted with caution. Similar to the discussion 363
previously for other conditions, the link between coffee consumption and mortality seems to 364
vary inconsistently by gender (Tverdal and others 1990; Jazbec and others 2003; Leurs and 365
others 2010; Liu and others 2013), HRT users versus non-users (Ascherio and others 2004), 366
and smoking status (Rosengren and Wilhelmsen 1991; Odegaard and others 2015), but 367
remains beneficial in the majority of evidence, when populations are considered as a whole. 368
369
3.8. Other conditions/health outcomes 370
In addition to all of the health relationships outlined above, a number of other conditions or 371
health outcomes have also been linked to coffee consumption. A total of 155 (12.1%) studies 372
are listed in Table 9 and corresponding conditions within each category are listed in Table 10. 373
Overall, the other most frequently reported condition associated with coffee consumption 374
is poor bone health. Although approximately half of the studies included in the current review 375
have shown a null effect on bone outcomes (22 out of 43), a similar proportion has also 376
reported adverse effects (18 out of 43). These adverse effects are reported only in lean 377
15
compared to overweight/obese individuals (Korpelainen and others 2003), and in females, not 378
males (Meyer and others 1997), with high daily coffee consumption (Meyer and others 1997; 379
El Maghraoui and others 2010). Nevertheless, others have shown that the adverse effects on 380
bone mineral density can be offset by milk, typically consumed with coffee (Barrett-Connor 381
and others 1994), and are only evident in those with the rapid CYP1A2 CC genotype 382
(Hallstrom and others 2010), and may not translate into an increase in fracture risk in the 383
longer-term (Trimpou and others 2010; Hallstrom and others 2013). Additional research is 384
clearly warranted to elucidate the effect of coffee consumption on bone health. 385
Finally, for all other categories of health outcomes identified, results are equivocal and 386
therefore conclusions on the benefit, risk, or null effect of coffee consumption cannot be 387
determined based on the current literature. 388
389
3.9. Additional risks 390
Additional risks of coffee consumption were apparent for pregnant women (for example 391
relative to pregnancy complications, birth outcomes, or the health of the infant). Although 392
these risks were noted in 26 out of the 50 studies, many were linked with higher coffee 393
consumption (Olsen and others 1991; Armstrong and others 1992; Parazzini and others 1998; 394
Bech and others 2005; Parazzini and others 2005; Werler and others 2015) and approximately 395
the same number of studies (22 out of 50) also reported null (no) effects on such adverse 396
events of pregnancy (Borlee and others 1978; Zhang and others 2010; Conde and others 397
2011; Alonso and others 2012; Conde and others 2010). Indeed, some studies did report 398
positive (beneficial) effects on certain pregnancy/infant health outcomes, such as the risk of 399
pre-term delivery (Petridou and others 1996) or childhood acute leukemia (Clavel and others 400
2005). Many of these studies state caffeine as responsible for the adverse events noted. 401
However, in support of those that have shown null effects, the European Food Safety Authority 402
(EFSA) recently concluded that habitual caffeine consumption (200 mg/d) does not give rise 403
to safety concerns for the fetus (EFSA 2015). 404
16
Finally, a number of other studies (n=45) were identified by the literature search that 405
highlighted coffee as a potential source of certain unwanted/toxic constituents, such as 406
ochratoxin A (StuderRohr and others 1994, 1995), furan (Crews and others 2009; Altaki and 407
others 2011), heavy metals (Taylor and others 2013; Nedzarek and others 2013) and 408
acrylamide (Bjellaas and others 2007; Eerola and others 2007). For the most part, however, 409
such studies did report that measured/estimated intake levels were well below estimated daily 410
acceptable intakes or that coffee was not a major source, therefore deemed safe (Perez de 411
Obanos and others 2005; Akdemir and others 2010; Guenther and others 2010; Ates and 412
others 2011; Coronel and others 2012). Moreover, the beneficial effects of other ‘bioactive’ 413
components, such as chlorogenic acids, phenolic acids and melanoids, add further support to 414
the beneficial effect of coffee as a beverage (Olthof and others 2001; Borrelli and others 2002; 415
Monteiro and others 2007; Rufian-Henares and de la Cueva 2009; Fumeaux and others 2010; 416
Fogliano and Morales 2011; Farrell and others 2012; Lardeau and Poquet 2013). 417
418
4. Conclusions 419
Overall, results of this comprehensive review show that the health benefits (or null effects) 420
clearly outweigh the risks of moderate coffee consumption in adult consumers for the majority 421
of health outcomes considered. This finding is largely based on observational data and, 422
moreover, major interactions were noted between coffee consumption and other lifestyle 423
habits (such as smoking/alcohol/HRT). 424
Additional randomized clinical trials are warranted, particularly in relation to cardiovascular 425
risk factors or endpoints and gastrointestinal disorders. This research should distinguish 426
effects of coffee consumption as a beverage, rather than quantify effects of caffeine intake per 427
se, adequately quantify/define coffee consumption and take account of all potential 428
confounding factors. Consideration should also be given to the type of coffee preparation or 429
brewing method, any potential influences of relevant genetic polymorphisms (for example, 430
CYP2A1), as well as the population group of interest (for example, healthy individuals vs. 431
patient groups and habitual vs. non habitual coffee drinkers). 432
17
433
5. Future work 434
Results from this research may aid further qualitative and quantitative risk-benefit 435
assessments of coffee consumption, using published approaches (Hoekstra and others 2012; 436
Verhagen and others 2012; Boobis and others 2013; Vidry and others 2013; Hart and others 437
2013) and further activities emphasizing the potential benefits should be pursued. As such, 438
the potential benefits for public health of consuming coffee or not consuming coffee could be 439
calculated for the most convincing benefits (for example, type 2 diabetes and neurological 440
and/or hepatic disorders). The potential public health benefits can be quantified in terms of 441
more Quality Adjusted Life Years (QALYs) or less Disability Adjusted Life Years (DALYs) (Hart 442
and others 2013) for countries and population groups of interest, depending on the availability 443
of population level dietary consumption data. 444
445
6. Acknowledgements 446
Professor Hans Verhagen is acknowledged for his introduction to risk-benefit assessment. 447
Thanks also go to illycaffè s.p.a. for funding this research. Disclosure statement: Even though 448
some financial support for this study was provided by the company (illycaffè s.p.a.), the 449
authors declare no conflict of interest regarding this objective search and summary of the 450
published literature. 451
452
7. Author contributions 453
LKP was responsible for study design, searching the literature, interpreting, results and 454
preparing the manuscript; LN, MP, and JJS were responsible for study design and drafting the 455
final manuscript. All authors reviewed the final manuscript before submission. 456
457
458
459
460
18
8. References 461
Abel EL, Hendrix SO, McNeeley SG, Johnson KC, Rosenberg CA, Mossavar-Rahmani Y, 462
Vitolins M, Kruger M. 2007. Daily coffee consumption and prevalence of nonmelanoma skin 463
cancer in Caucasian women. Eur J Cancer Prev 16:446-52. 464
Aeschbacher HU, Chappuis C. 1981. Non-mutagenicity of urine from coffee drinkers 465
compared with that from cigarette smokers. Mutat Res 89:161-77. 466
Ahola I, Jauhiainen M, Aro A. 1991. The hypercholesterolemic factor in boiled coffee is 467
retained by a paper filter. J Intern Med 230:293-7. 468
Akdas A, Kirkali Z, Bilir N. 1990. Epidemiological case-control study on the etiology of bladder 469
cancer in Turkey. Eur Urol 17:23-6. 470
Akdemir C, Ulker OC, Basaran A, Ozkaya S, Karakaya A. 2010. Estimation of ochratoxin A in 471
some Turkish populations: an analysis in urine as a simple, sensitive and reliable 472
biomarker. Food Chem Toxicol 48:877-82. 473
Alonso J, Sosa C, Verde ME, Balsamo A, Moraes M, Zolessi M, Bertolino L, Amaral J, Di 474
Giovanni JP. 2012. Risk factors for term small for gestational age. A case-control study in 475
an Uruguayan population. Int J Gynecol Obst 119:S276. 476
Altaki MS, Santos FJ, Galceran MT. 2011. Occurrence of furan in coffee from Spanish market: 477
Contribution of brewing and roasting. Food Chem 126:1527-32. 478
Ammon HPT, Bieck PR, Mandalaz D, Verspohl EJ. 1983. Adaptation of blood pressure to 479
continuous heavy coffee drinking in young volunteers. A double-blind crossover study. Br 480
J Clin Pharmacol 15:701-6. 481
Arab L, Biggs ML, O'Meara ES, Longstreth WT, Crane PK, Fitzpatrick AL. 2011. Gender 482
differences in tea, coffee, and cognitive decline in the elderly: The cardiovascular health 483
study. J Alzheimer's Dis 27:553-66. 484
Armstrong BG, McDonald AD, Sloan M. 1992. Cigarette, alcohol, and coffee consumption and 485
spontaneous abortion. Am J Public Health 82:85-7. 486
Aro A, Teirila J, Gref C. 1990. Dose-dependent effect on serum cholesterol and apoprotein B 487
concentrations by consumption of boiled, non-filtered coffee. Atherosclerosis 83:257-61. 488
19
Arsenault BJ, Earnest CP, Despres J-, Blair SN, Church TS. 2009. Obesity, coffee 489
consumption and CRP levels in postmenopausal overweight/obese women: Importance of 490
hormone replacement therapy use. Eur J Clin Nutr 63:1419-24. 491
Ascherio A, Zhang SM, Hernan MA, Kawachi I, Colditz GA, Speizer FE, Willett WC. 2001. 492
Prospective study of caffeine consumption and risk of Parkinson's disease in men and 493
women. Ann Neurol 50:56-63. 494
Ascherio A, Chen H, Schwarzschild MA, Zhang SM, Colditz GA, Speizer FE. 2003. Caffeine, 495
postmenopausal estrogen, and risk of Parkinson's disease. Neurology 60:790-5. 496
Ascherio A, Weisskopf MG, O'Reilly EJ, McCullough ML, Calle EE, Rodriguez C, Thun MJ. 497
2004. Coffee consumption, gender, and Parkinson's disease mortality in the Cancer 498
Prevention Study II cohort: The modifying effects of estrogen. Am J Epidemiol 160:977-84. 499
Ates I, Ulker OC, Akdemir C, Karakaya A. 2011. Correlation of ochratoxin A exposure to 500
urinary levels of 8-hydroxydeoxyguanosine and malondialdehyde in a Turkish population. 501
Bull Environ Contam Toxicol 86:258-62. 502
Awaad AS, Soliman GA, Al-Outhman MR, Al-Shdoukhi IF, Al-Nafisah RS, Al-Shamery J, Al-503
Samkhan R, Baqer M, Al-Jaber NA. 2011. The effect of four coffee types on normotensive 504
rats and normal/hypertensive human volunteers. Phytotherapy Res 25:803-8. 505
Ayari I, Fedeli U, Saguem S, Hidar S, Khlifi S, Pavanello S. 2013. Role of CYP1A2 506
polymorphisms in breast cancer risk in women. Molecular Medicine Reports 7:280-6. 507
Azevedo A, Barros H. 2006. Coffee and myocardial infarction: Heterogeneity of an association 508
in Portuguese men. Eur J Cardiovas Prev Rehab 13:268-73. 509
Bageman E, Ingvar C, Rose C, Jernstrom H. 2008. Coffee consumption and CYP1A2*1F 510
genotype modify age at breast cancer diagnosis and estrogen receptor status. Cancer 511
Epidemiol Biomarkers Prev 17:895-901. 512
Bak AAA, Grobbee DE. 1989. The effect on serum cholesterol levels of coffee brewed by 513
filtering or boiling. N Engl J Med 321:1432-7. 514
Bak AAA, Grobbee DE. 1990. A randomized study on coffee and blood pressure. J Hum 515
Hypertens 4:259-64. 516
20
Baker JA, McCann SE, Reid ME, Nowell S, Beehler GP, Moysich KB. 2005. Associations 517
between black tea and coffee consumption and risk of lung cancer among current and 518
former smokers. Nutr Cancer 52:15-21. 519
Baker JA, Boakye K, McCann SE, Beehler GP, Rodabaugh KJ, Villella JA, Moysich KB. 2007. 520
Consumption of black tea or coffee and risk of ovarian cancer. Int J Gynecol Cancer 17:50-521
4. 522
Bakuradze T, Boehm N, Janzowski C, Lang R, Hofmann T, Stockis J-, Albert FW, Stiebitz H, 523
Bytof G, Lantz I, Baum M, Eisenbrand G. 2011. Antioxidant-rich coffee reduces DNA 524
damage, elevates glutathione status and contributes to weight control: Results from an 525
intervention study. Mol Nutr Food Res 55:793-7. 526
Bakuradze T, Parra GAM, Riedel A, Somoza V, Lang R, Dieminger N, Hofmann T, Winkler S, 527
Hassmann U, Marko D, Schipp D, Raedle J, Bytof G, Lantz I, Stiebitz H, Richling E. 2014. 528
Four-week coffee consumption affects energy intake, satiety regulation, body fat, and 529
protects DNA integrity. Food Res Int 63:420-7. 530
Bakuradze T, Lang R, Hofmann T, Eisenbrand G, Schipp D, Galan J, Richling E. 2015. 531
Consumption of a dark roast coffee decreases the level of spontaneous DNA strand breaks: 532
a randomized controlled trial. Eur J Nutr 54:149-56. 533
Barrett-Connor E, Chang JC, Edelstein SL. 1994. Coffee-associated osteoporosis offset by 534
daily milk consumption: The Rancho Bernardo study. J Am Med Assoc 271:280-3. 535
Basile J. 2002. Coffee intake over 33 years is not associated with developing hypertension. J 536
Clin Hypertens 4:434. 537
Bech BH, Nohr EA, Vaeth M, Henriksen TB, Olsen J. 2005. Coffee and fetal death: A cohort 538
study with prospective data. Am J Epidemiol 162:983-90. 539
Berndt B, Mensink GBM, Kohlmeier M, Kohlmeier L, Kottgen E. 1993. Lipoprotein metabolism 540
and coffee intake - Who is at risk?. Z Ernahrungswiss 32:163-75. 541
Bhatia SJ, Reddy DN, Ghoshal UC, Jayanthi V, Abraham P, Choudhuri G, Broor SL, Ahuja V, 542
Augustine P, Balakrishnan V, Bhasin DK, Bhat N, Chacko A, Dadhich S, Dhali GK, Dhawan 543
PS, Dwivedi M, Goenka MK, Koshy A, Kumar A, Misra SP, Mukewar S, Raju EP, Shenoy 544
21
KT, Singh SP, Sood A, Srinivasan R. 2011. Epidemiology and symptom profile of 545
gastroesophageal reflux in the Indian population: Report of the Indian Society of 546
Gastroenterology Task Force. Indian J Gastroenterol 30:118-27. 547
Bhoo-Pathy N, Peeters PHM, Uiterwaal CSPM, Bueno-de-Mesquita HB, Bulgiba AM, Bech 548
BH, Overvad K, Tjonneland A, Olsen A, Clavel-Chapelon F, Fagherazzi G, Perquier F, 549
Teucher B, Kaaks R, Schutze M, Boeing H, Lagiou P, Orfanos P, Trichopoulou A, Agnoli 550
C, Mattiello A, Palli D, Tumino R, Sacerdote C, Van Duijnhoven FJB, Braaten T, Lund E, 551
Skeie G, Redondo M-, Buckland G, Perez MJS, Chirlaque M, Ardanaz E, Amiano P, Wirfalt 552
E, Wallstrom P, Johansson I, Nilsson LM, Khaw K, Wareham N, Allen NE, Key TJ, Rinaldi 553
S, Romieu I, Gallo V, Riboli E, Van Gils CH. 2015. Coffee and tea consumption and risk of 554
pre- and postmenopausal breast cancer in the European Prospective Investigation into 555
Cancer and Nutrition (EPIC) cohort study. Breast Cancer Res 17. 556
Bissonauth V, Shatenstein B, Fafard E, Maugard C, Robidoux A, Narod S, Ghadirian P. 2009. 557
Risk of breast cancer among French-Canadian women, noncarriers of more frequent 558
BRCA1/2 mutations and consumption of total energy, coffee, and alcohol. Breast J 15 559
Suppl 1:S63-71. 560
Bjellaas T, Stolen LH, Haugen M, Paulsen JE, Alexander J, Lundanes E, Becher G. 2007. 561
Urinary acrylamide metabolites as biomarkers for short-term dietary exposure to 562
acrylamide. Food Chem Toxicol 45:1020-6. 563
Boekema PJ, Samsom M, Roelofs JM, Smout AJ. 2001. Effect of coffee on motor and sensory 564
function of proximal stomach. Dig Dis Sci 46:945-51. 565
Boekschoten MV, Schouten EG, Katan MB. 2004. Coffee bean extracts rich and poor in 566
kahweol both give rise to elevation of liver enzymes in healthy volunteers. Nutr J 3:. 567
Bonaa K, Arnesen E, Thelle DS, Forde OH. 1988. Coffee and cholesterol: is it all in the 568
brewing? The Tromso study. Br Med J 297:1103-4. 569
Boobis A, Chiodini A, Hoekstra J, Lagiou P, Przyrembel H, Schlatter J, Schutte K, Verhagen 570
H, Watzl B. 2013. Critical appraisal of the assessment of benefits and risks for foods, 571
'BRAFO Consensus Working Group'. Food Chem Toxicol 55:659-75. 572
22
Borlee I, Bouckaert A, Lechat MF, Misson CB. 1978. Smoking patterns during and before 573
pregnancy: weight, length and head circumference of progeny. Eur J Obst Gynecol Reprod 574
Biol 8:171-7. 575
Borrelli RC, Visconti A, Mennella C, Anese M, Fogliano V. 2002. Chemical characterization 576
and antioxidant properties of coffee melanoidins. J Agric Food Chem 50:6527-33. 577
Boutron-Ruault M, Senesse P, Faivre J, Chatelain N, Belghiti C, Meance S. 1999. Foods as 578
risk factors for colorectal cancer: a case-control study in Burgundy (France). Eur J Cancer 579
Prev 8:229-35. 580
Buscemi S, Verga S, Batsis JA, Donatelli M, Tranchina MR, Belmonte S, Mattina A, Re A, 581
Cerasola G. 2010. Acute effects of coffee on endothelial function in healthy subjects. Eur J 582
Clin Nutr 64:483-9. 583
Camfield DA, Silber BY, Scholey AB, Nolidin K, Goh A, Stough C. 2013. A randomised 584
placebo-controlled trial to differentiate the acute cognitive and mood effects of chlorogenic 585
acid from decaffeinated coffee. Plos One 8:e82897. 586
Cano-Marquina A, Tarin JJ, Cano A. 2013. The impact of coffee on health. Maturitas 75:7-21. 587
Carson CA, Caggiula AW, Meilahn EN, Matthews KA, Kuller LH. 1994. Coffee consumption: 588
Relationship to blood lipids in middle-aged women. Int J Epidemiol 23:523-7. 589
Catalano D, Trovato GM, Spadaro D, Martines GF, Garufi G, Tonzuso A, Grasso D, 590
Sciacchitano SG. 2008. Insulin resistance in postmenopausal women: Concurrent effects 591
of hormone replacement therapy and coffee. Climacteric 11:373-82. 592
Chacon MR. 2014. Serum sCD163 levels are associated with type 2 diabetes mellitus and are 593
influenced by coffee and wine consumption: results of the [email protected] study. PloS one 594
9:e101250. 595
Christensen B, Mosdol A, Retterstol L, Landaas S, Thelle DS. 2001. Abstention from filtered 596
coffee reduces the concentrations of plasma homocysteine and serum cholesterol--a 597
randomized controlled trial. Am J Clin Nutr 74:302-7. 598
Chung SJ, Armasu SM, Anderson KJ, Biernacka JM, Lesnick TG, Rider DN, Cunningham JM, 599
Ahlskog JE, Frigerio R, Maraganore DM. Jun 2013. Genetic susceptibility loci, 600
23
environmental exposures, and Parkinson's disease: A case-control study of gene-601
environment interactions. Parkinsonism Relat Disord 19:595-9. 602
Clavel F, Benhamou E, Auquier A, Tarayre M, Flamant R. 1989. Coffee, alcohol, smoking and 603
cancer of the pancreas: A case-control study. Int J Cancer 43:17-21. 604
Clavel J, Bellec S, Rebouissou S, Menegaux F, Feunteun J, Bonaiti-Pellie C, Baruchel A, 605
Kebaili K, Lambilliotte A, Leverger G, Sommelet D, Lescoeur B, Beaune P, Hemon D, Loriot 606
M. 2005. Childhood leukaemia, polymorphisms of metabolism enzyme genes, and 607
interactions with maternal tobacco, coffee and alcohol consumption during pregnancy. Eur 608
J Cancer Prev 14:531-40. 609
Clavel J, Cordier S. 1991. Coffee consumption and bladder cancer risk. Int J Cancer 47:207-610
12. 611
Coffey RJ, Go VL, Zinsmeister AR, DiMagno EP. 1986. The acute effects of coffee and 612
caffeine on human interdigestive exocrine pancreatic secretion. Pancreas 1:55-61. 613
Cohen S. 1980. Pathogenesis of coffee-induced gastrointestinal symptoms. N Engl J Med 614
303:122-4. 615
Conde A, Figueiredo B, Tendais I, Teixeira C, Costa R, Pacheco A, Rodrigues MC, Nogueira 616
R. 2010. Mother's anxiety and depression and associated risk factors during early 617
pregnancy: Effects on fetal growth and activity at 20-22 weeks of gestation. J Psych Obst 618
Gynecol 31:70-82. 619
Conde A, Teves C, Figueiredo B. 2011. Maternal coffee intake and associated risk factors: 620
Effects on fetal growth and activity. Acta Med Port 24:241-8. 621
Cornelis MC, El-Sohemy A, Kabagambe EK, Campos H. 2006. Coffee, CYP1A2 genotype, 622
and risk of myocardial infarction. J Am Med Assoc 295:1135-41. 623
Coronel MB, Marin S, Cano-Sancho G, Ramos AJ, Sanchis V. 2012. Exposure assessment 624
to ochratoxin A in Catalonia (Spain) based on the consumption of cereals, nuts, coffee, 625
wine, and beer. Food Additives and Contaminants Part A-Chemistry Analysis Control 626
Exposure & Risk Assessment 29:979-93. 627
24
Corrao G, Lepore AR, Torchio P, Valenti M, Galatola G, D'Amicis A, Arico S, di Orio F. 1994. 628
The effect of drinking coffee and smoking cigarettes on the risk of cirrhosis associated with 629
alcohol consumption. A case-control study. Provincial Group for the Study of Chronic Liver 630
Disease. Eur J Epidemiol 10:657-64. 631
Corrao G, Zambon A, Bagnardi V, D'Amicis A, Klatsky A. 2001. Coffee, caffeine, and the risk 632
of liver cirrhosis. Ann Epidemiol 11:458-65. 633
Corti R, Binggeli C, Sudano I, Spieker L, Hanseler E, Ruschitzka F, Chaplin WF, Luscher TF, 634
Noll G. 2002. Coffee acutely increases sympathetic nerve activity and blood pressure 635
independently of caffeine content role of habitual versus nonhabitual drinking. Circulation 636
106:2935-40. 637
Crews C, Roberts D, Lauryssen S, Kramer G. 2009. Survey of furan in foods and coffees from 638
five European Union countries. Food Additives and Contaminants: Part B -- Surveillance 639
Communications 2:95-8. 640
D'Amelio M, Ragonese P, Callari G, Di Benedetto N, Palmeri B, Terruso V, Salemi G, Famoso 641
G, Aridon P, Savettieri G. 2009. Diabetes preceding Parkinson's disease onset. A case-642
control study. Parkinson Rel Dis 15:660-4. 643
Danielsson J, Kangastupa P, Laatikainen T, Aalto M, Niemela O. May-Jun 2013. Dose- and 644
gender-dependent interactions between coffee consumption and serum GGT activity in 645
alcohol consumers. Alcohol and Alcoholism 48:303-7. 646
D'Avanzo B, La Vecchia C, Franceschi S, Negri E, Talamini R, Buttino I. 1992. Coffee 647
consumption and bladder cancer risk. Eur J Cancer 28A:1480-4. 648
D'Avanzo B, Santoro L, Nobili A, La Vecchia C. 1993. Coffee consumption and serum 649
cholesterol. Prev Med 22:219-24. 650
De Roos B, Van Tol A, Urgert R, Scheek L, Van Gent T, Buytenhek R, Princen H, Katan M. 651
2000. Consumption of French-press coffee raises cholesteryl ester transfer protein activity 652
levels before LDL cholesterol in normolipidaemic subjects. J Intern Med 248:211-6. 653
deGroot J, vanStaveren W, Dirren H, Hautvast J. 1996. Consumption of unfiltered coffee 654
brews in elderly Europeans. Eur J Clin Nutr 50:S101-4. 655
25
DiBaise JK. 2003. A randomized, double-blind comparison of two different coffee-roasting 656
processes on development of heartburn and dyspepsia in coffee-sensitive individuals. Dig 657
Dis Sci 48:652-6. 658
Donato F, Boffetta P, Fazioli R, Aulenti V, Gelatti U, Porru S. 1997. Bladder cancer, tobacco 659
smoking, coffee and alcohol drinking in Brescia, northern Italy. Eur J Epidemiol 13:795-660
800. 661
Eerola S, Hollebekkers K, Hallikainen A, Peltonen K. 2007. Acrylamide levels in Finnish 662
foodstuffs analysed with liquid chromatography tandem mass spectrometry. Mol Nutr Food 663
Res 51:239-47. 664
Efird JT, Friedman GD, Sidney S, Klatsky A, Habel LA, Udaltsova NV, Van Den Eeden S, 665
Nelson LM. 2004. The risk for malignant primary adult-onset glioma in a large, multiethnic, 666
managed-care cohort: Cigarette smoking and other lifestyle behaviors. J Neurooncol 68:57-667
69. 668
Eggertsen R, Andreasson A, Hedner T, Karlberg BE, Hansson L. 1993. Effect of coffee on 669
ambulatory blood pressure in patients with treated hypertension. J Intern Med 233:351-5. 670
Eisig JN, Zaterka S, Massuda HK, Bettarello A. 1989. Coffee drinking in patients with duodenal 671
ulcer and a control population. Scand J Gastroenterol 24:796-8. 672
El Maghraoui A, Ghazi M, Gassim S, Ghozlani I, Mounach A, Rezqi A, Dehhaoui M. 2010. 673
Risk factors of osteoporosis in healthy Moroccan men. BMC Musculoskeletal Disorders 674
11:148. 675
el Shabrawy Ali M, Felimban FM. 1993. A study of the impact of Arabic coffee consumption 676
on serum cholesterol. J R Soc Health 113:288-91. 677
Enga KF, Braekkan SK, Hansen-Krone IJ, Wilsgaard T, Hansen J-. 2011. Coffee consumption 678
and the risk of venous thromboembolism: The Tromso study. J Thromb Haem 9:1334-9. 679
European Food Safety Authority (EFSA). 2015. Scientific opinion on the safety of caffeine. 680
EFSA Journal 13:4102. 681
26
Facheris MF, Schneider NK, Lesnick TG, de Andrade M, Cunningham JM, Rocca WA, 682
Maraganore DM. 2008. Coffee, caffeine-related genes, and Parkinson's disease: A case-683
control study. Move Dis 23:2033-40. 684
Fardet A, Boirie Y. 2014. Associations between food and beverage groups and major diet-685
related chronic diseases: an exhaustive review of pooled/meta-analyses and systematic 686
reviews. Nutr Rev 72:741-62. 687
Farrell TL, Gomez-Juaristi M, Poquet L, Redeuil K, Nagy K, Renouf M, Williamson G. 2012. 688
Absorption of dimethoxycinnamic acid derivatives in vitro and pharmacokinetic profile in 689
human plasma following coffee consumption. Mol Nutr Food Res 56:1413-23. 690
Fogliano V, Morales FJ. 2011. Estimation of dietary intake of melanoidins from coffee and 691
bread. Food Funct 2:117-23. 692
Forde OH, Knutsen SF, Arnesen E, Thelle DS. 1985. The Tromso heart study: Coffee 693
consumption and serum lipid concentrations in men with hypercholesterolaemia: A 694
randomised intervention study. Br Med J 290:893-5. 695
Fortes C, Mastroeni S, Melchi F, Anzidei P, Innocenzi L, Raffaella G, Antonelli GM, Pasquini 696
P, Venanzetti F. 2009. Polymorphisms in GSTM1 and GSTT1, Coffee consumption, and 697
cutaneous melanoma risk. J Nutrigenetics Nutrigenomics 2:211-2. 698
Fortes C, Mastroeni S, Boffetta P, Antonelli G, Pilla MA, Botta G, Anzidei P, Venanzetti F. 699
2013. The protective effect of coffee consumption on cutaneous melanoma risk and the 700
role of GSTM1 and GSTT1 polymorphisms. Cancer Caus Cont 24:1779-87. 701
Fried RE, Levine DM, Kwiterovich PO, Diamond EL, Wilder LB, Moy TF, Pearson TA. 1992. 702
The effect of filtered-coffee consumption on plasma lipid levels: Results of a randomized 703
clinical trial. J Am Med Assoc 267:811-5. 704
Fumeaux R, Menozzi-Smarrito C, Stalmach A, Munari C, Kraehenbuehl K, Steiling H, Crozier 705
A, Williamson G, Barron D. 2010. First synthesis, characterization, and evidence for the 706
presence of hydroxycinnamic acid sulfate and glucuronide conjugates in human biological 707
fluids as a result of coffee consumption. Org Biomol Chem 8:5199-211. 708
27
Galanis DJ, Kolonel LN, Lee J, Nomura A. 1998. Intakes of selected foods and beverages and 709
the incidence of gastric cancer among the Japanese residents of Hawaii: A prospective 710
study. Int J Epidemiol 27:173-80. 711
Gallus S, Foschi R, Talamini R, Altieri A, Negri E, Franceschi S, Montella M, Dal Maso L, 712
Ramazzotti V, La Vecchia C. 2007. Risk factors for prostate cancer in men aged less than 713
60 years: A case-control study from Italy. Urology 70:1121-6. 714
George SE, Ramalakshmi K, Rao LJM. 2008. A perception on health benefits of coffee. Crit 715
Rev Food Sci Nutr 48:464-86. 716
Goodman MT, Tung K-, McDuffie K, Wilkens LR, Donlon TA. 2003. Association of caffeine 717
intake and CYP1A2 genotype with ovarian cancer. Nutr Cancer 46:23-9. 718
Gorham ED, Garland CF, Garland FC, Benenson AS, Cottrell L. 1988. Coffee and pancreatic 719
cancer in a rural California county. West J Med 148:48-53. 720
Goto A, Song Y, Chen BH, Manson JE, Buring JE, Liu S. 2011. Coffee and caffeine 721
consumption in relation to sex hormone-binding globulin and risk of type 2 diabetes in 722
postmenopausal women. Diabetes 60:269-75. 723
Goto A, Chen BH, Song Y, Cauley J, Cummings SR, Farhat GN, Gunter M, Horn LV, Howard 724
BV, Jackson R, Lee J, Rexrode KM, Liu S. 2014. Age, body mass, usage of exogenous 725
estrogen, and lifestyle factors in relation to circulating sex hormone-binding globulin 726
concentrations in postmenopausal women. Clin Chem 60:174-85. 727
Grandinetti A, Morens DM, Reed D, MacEachern D. 1994. Prospective study of cigarette 728
smoking and the risk of developing idiopathic Parkinson's disease. Am J Epidemiol 729
139:1129-38. 730
Green CJ, de Dauwe P, Boyle T, Tabatabaei SM, Fritschi L, Heyworth JS. 2014. Tea, coffee, 731
and milk consumption and colorectal cancer risk. Journal of Epidemiology 24:146-53. 732
Gross G, Jaccaud E, Huggett A. 1997. Analysis of the content of the diterpenes cafestol and 733
kahweol in coffee brews. Food Chem Toxicol 35:547-54. 734
Guenther H, Hoenicke K, Biesterveld S, GerhardRieben E, Lantz I. 2010. Furan in coffee: pilot 735
studies on formation during roasting and losses during production steps and consumer 736
28
handling. Food Additives and Contaminants: Part A -- Chemistry, Analysis, Control, 737
Exposure and Risk Assessment 27:283-90. 738
Gullo L, Pezzilli R, Morselli-Labate AM, Malesci A, Zerbi A, Andriulli A, Acquadro P, D'Ambrosi 739
A, Alvisi V, Montalto G, Carroccio A, De Conca V, Mesiti S, Mansi C, Campione O, Casadei 740
R, Brambati M, Lesi C, Battistini C. 1995. Coffee and cancer of the pancreas: An Italian 741
multicenter study. Pancreas 11:223-9. 742
Gutierrez-Grobe Y, Chavez-Tapia N, Sanchez-Valle V, Gavilanes-Espinar JG, Ponciano-743
Rodriguez G, Uribe M, Mendez-Sanchez N. 2012. High coffee intake is associated with 744
lower grade nonalcoholic fatty liver disease: The role of peripheral antioxidant activity. Ann 745
Hepatol 11:350-5. 746
Hallstrom H, Melhus H, Glynn A, Lind L, Syvanen A-, Michalsson K. 2010. Coffee consumption 747
and CYP1A2 genotype in relation to bone mineral density of the proximal femur in elderly 748
men and women: A cohort study. Nutr Metab 7:. 749
Hallstrom H, Byberg L, Glynn A, Lemming EW, Wolk A, Michaelsson K. 2013. Long-term 750
coffee consumption in relation to fracture risk and bone mineral density in women. Am J 751
Epidemiol 178:898-909. 752
Hammar N, Andersson T, Alfredsson L, Reuterwall C, Nilsson T, Hallqvist J, Knutsson A, 753
Ahlbom A. 2003. Association of boiled and filtered coffee with incidence of first nonfatal 754
myocardial infarction: The SHEEP and the VHEEP study. J Intern Med 253:653-9. 755
Harnack LJ, Anderson KE, Zheng W, Folsom AR, Sellers TA, Kushi LH. 1997. Smoking, 756
alcohol, coffee, and tea intake and incidence of cancer of the exocrine pancreas: The Iowa 757
women's health study. Cancer Epidemiol Biomarkers Prev 6:1081-6. 758
Hart A, Hoekstra J, Owen H, Kennedy M, Zeilmaker MJ, de Jong N, Gunnlaugsdottir H. 2013. 759
Qalibra: a general model for food risk-benefit assessment that quantifies variability and 760
uncertainty. Food Chem Toxicol 54:4-17. 761
Hartge P, Hoover R, West DW, Lyon JL. 1983. Coffee drinking and risk of bladder cancer. J 762
Natl Cancer Inst 70:1021-6. 763
29
Hemminki E, Pesonen T. 1977. Regional coffee consumption and mortality from ischemic 764
heart disease in Finland. Acta Med Scand 201:127-30. 765
Hennekens CH, Drolette ME, Jesse MJ, Davies JE, Hutchison GB. 1976. Coffee drinking and 766
death due to coronary heart disease. N Engl J Med 294:633-6. 767
Herraiz T, Chaparro C. 2006. Human monoamine oxidase enzyme inhibition by coffee and 768
beta-carbolines norharman and harman isolated from coffee. Life Sci 78:795-802. 769
Heyden S, Tyroler HA, Cassel JC, Hames CG, Becker C, Heiss G. 1976. Coffee consumption 770
and mortality in a community study--Evans Co., Ga. Z Ernahrungswiss 15:143-50. 771
Hoekstra J, Hart A, Boobis A, Claupein E, Cockburn A, Hunt A, Knudsen I, Richardson D, 772
Schilter B, Schutte K, Torgerson PR, Verhagen H, Watzl B, Chiodini A. 2012. BRAFO tiered 773
approach for Benefit-Risk Assessment of Foods. Food Chem Toxicol 50 Suppl 4:S684-98. 774
Hoelzl C, Knasmuller S, Wagner K, Elbling L, Huber W, Kager N, Ferk F, Ehrlich V, Nersesyan 775
A, Neubauer O, Desmarchelier A, Marin-Kuan M, Delatour T, Verguet C, Bezencon C, 776
Besson A, Grathwohl D, Simic T, Kundi M, Schilter B, Cavin C. 2010. Instant coffee with 777
high chlorogenic acid levels protects humans against oxidative damage of 778
macromolecules. Mol Nutr Food Res 54:1722-33. 779
Honjo S, Kono S, Coleman MP, Shinchi K, Sakurai Y, Todoroki I, Umeda T, Wakabayashi K, 780
Imanishi K, Nishikawa H, Ogawa S, Katsurada M, Nakagawa K, Yoshizawa N. 2001. Coffee 781
consumption and serum aminotransferases in middle-aged Japanese men. J Clin 782
Epidemiol 54:823-9. 783
Hori A, Kasai H, Kawai K, Nanri A, Sato M, Ohta M, Mizoue T. 2014. Coffee intake is 784
associated with lower levels of oxidative DNA damage and decreasing body iron storage 785
in healthy women. Nutr Cancer 66:964-9. 786
Hosseini Tabatabaei N, Babakhani B, Hosseini Tabatabaei A, Vahabi Z, Soltanzadeh A. 2013. 787
Non-genetic factors associated with the risk of Parkinson's disease in Iranian patients. 788
Funct Neurol 28:107-13. 789
Ikeda M, Maki T, Yin G, Kawate H, Adachi M, Ohnaka K, Takayanagi R, Kono S. 2010. 790
Relation of coffee consumption and serum liver enzymes in Japanese men and women 791
30
with reference to effect modification of alcohol use and body mass index. Scand J Clin Lab 792
Invest 70:171-9. 793
Jaquet M, Rochat I, Moulin J, Cavin C, Bibiloni R. 2009. Impact of coffee consumption on the 794
gut microbiota: a human volunteer study. Int J Food Microbiol 130:117-21. 795
Jazbec A, Simic D, Corovic N, Durakovic Z, Pavlovic M. 2003. Impact of coffee and other 796
selected factors on general mortality and mortality due to cardiovascular disease in Croatia. 797
J Health Pop Nutr 21:332-40. 798
Johnson-Kozlow M, Kritz-Silverstein D, Barrett-Connor E, Morton D. 2002. Coffee 799
consumption and cognitive function among older adults. Am J Epidemiol 156:842-50. 800
Johnston KL, Clifford MN, Morgan LM. 2003. Coffee acutely modifies gastrointestinal hormone 801
secretion and glucose tolerance in humans: glycemic effects of chlorogenic acid and 802
caffeine. Am J Clin Nutr 78:728-33. 803
Luo J, Inoue M, Iwasaki M, Sasazuki S, Otani T, Ye W, Tsugane S; JPHC Study Group. 2007. 804
Green tea and coffee intake and risk of pancreatic cancer in a large-scale, population-805
based cohort study in Japan (JPHC study). Eur J Cancer Prev 16:542-8. 806
Kim HJ, Cho S, Jacobs DR Jr, Park K. 2014. Instant coffee consumption may be associated 807
with higher risk of metabolic syndrome in Korean adults. Diab Res Clin Prac 106:145-53. 808
Klatsky AL, Armstrong MA, Friedman GD. 1993. Coffee, tea, and mortality. Ann Epidemiol 809
3:375-81. 810
Klatsky AL, Morton C, Udaltsova N, Friedman GD. 2006. Coffee, cirrhosis, and transaminase 811
enzymes. Arch Intern Med 166:1190-5. 812
Koizumi T, Nakaya N, Okamura C, Sato Y, Shimazu T, Nagase S, Niikura H, Kuriyama S, 813
Tase T, Ito K, Tsubono Y, Okamura K, Yaegashi N, Tsuji I. 2008. Case-control study of 814
coffee consumption and the risk of endometrial endometrioid adenocarcinoma. Eur J 815
Cancer Prev 17:358-63. 816
Kokic NZ, Adanja JB, Vlajinac DH, Marinkovic PJ, Colovic BR, Jarebinski SM. 1996. Case-817
control study of pancreatic cancer in Serbia, Yugoslavia. Neoplasma 43:353-6. 818
31
Kono S, Shinchi K, Imanishi K, Todoroki I, Hatsuse K. 1994. Coffee and serum gamma-819
glutamyltransferase: A study of self-defense officials in Japan. Am J Epidemiol 139:723-7. 820
Korpelainen R, Korpelainen J, Heikkinen J, Vaananen K, Keinanen-Kiukaanniemi S. 2003. 821
Lifestyle factors are associated with osteoporosis in lean women but not in normal and 822
overweight women: A population-based cohort study of 1222 women. Osteoporosis Int 823
14:34-43. 824
Kotsopoulos J, Ghadirian P, El-Sohemy A, Lynch HT, Snyder C, Daly M, Domchek S, Randall 825
S, Karlan B, Zhang P, Zhang S, Sun P, Narod SA. 2007. The CYP1A2 genotype modifies 826
the association between coffee consumption and breast cancer risk among BRCA1 827
mutation carriers. Cancer Epidemiol Biomarkers Prev 16:912-6. 828
Kotyczka C, Boettler U, Lang R, Stiebitz H, Bytof G, Lantz I, Hofmann T, Marko D, Somoza V. 829
2011. Dark roast coffee is more effective than light roast coffee in reducing body weight, 830
and in restoring red blood cell vitamin E and glutathione concentrations in healthy 831
volunteers. Mol Nutr Food Res 55:1582-6. 832
Kumao T, Fujii S. 2006. Mannooligosaccharides blended coffee beverage intake increases 833
the fat level in feces. J Health Sci 52:329-32. 834
Kuper H, Titus-Ernstoff L, Harlow BL, Cramer DW. 2000. Population based study of coffee, 835
alcohol and tobacco use and risk of ovarian cancer. Int J Cancer 88:313-8. 836
Lancaster T, Muir J, Silagy C. 1994. The effects of coffee on serum lipids and blood pressure 837
in a UK population. J R Soc Med 87:506-7. 838
Lardeau A, Poquet L. 2013. Phenolic acid metabolites derived from coffee consumption are 839
unlikely to cross the blood-brain barrier. J Pharm Biomed Anal 76:134-8. 840
Lee KJ, Inoue M, Otani T, Iwasaki M, Sasazuki S, Tsugane S, JPHC Study Group. 2007. 841
Coffee consumption and risk of colorectal cancer in a population-based prospective cohort 842
of Japanese men and women. Int J Cancer 121:1312-8. 843
LeGrady D, Dyer AR, Shekelle RB, Stamler J, Liu K, Paul O, Lepper M, Mac Millan Shryock 844
A. 1987. Coffee consumption and mortality in the Chicago Western Electric Company 845
study. Am J Epidemiol 126:803-12. 846
32
Leurs LJ, Schouten LJ, Goldbohm RA, Van Den Brandt PA. 2010. Total fluid and specific 847
beverage intake and mortality due to IHD and stroke in the Netherlands Cohort Study. Br J 848
Nutr 104:1212-21. 849
Lindahl B, Johansson I, Huhtasaari F, Hallmans G, Asplund K. 1991. Coffee drinking and 850
blood cholesterol - Effects of brewing method, food intake and life style. J Intern Med 851
230:299-305. 852
Liu J, Sui X, Lavie CJ, Hebert JR, Earnest CP, Zhang J, Blair SN. 2013. Association of coffee 853
consumption with all-cause and cardiovascular disease mortality. Mayo Clin Proc 88:1066-854
74. 855
Lueth NA, Anderson KE, Harnack LJ, Fulkerson JA, Robien K. 2008. Coffee and caffeine 856
intake and the risk of ovarian cancer: The Iowa Women's Health Study. Cancer Caus Cont 857
19:1365-72. 858
Maki T, Pham NM, Yoshida D, Yin G, Ohnaka K, Takayanagi R, Kono S. 2010. The 859
relationship of coffee and green tea consumption with high-sensitivity C-reactive protein in 860
Japanese men and women. Clin Chem Lab Med 48:849-54. 861
van der Mark M, Nijssen PC, Vlaanderen J, Huss A, Mulleners WM, Sas AM, van Laar T, 862
Kromhout H, Vermeulen R. 2014. A case-control study of the protective effect of alcohol, 863
coffee, and cigarette consumption on Parkinson disease risk: time-since-cessation modifies 864
the effect of tobacco smoking. PLoS ONE 9, (4): e95297. 865
Marotta T, Liccardo M, Ferrara LA. 2013. Intake of coffee and metabolic profile in an outpatient 866
population. High Blood Pres Cardiovas Prev 20:204. 867
Marrett LD, Walter SD, Meigs JW. 1983. Coffee drinking and bladder cancer in Connecticut. 868
Am J Epidemiol 117:113-27. 869
McCulloch CC, Kay DM, Factor SA, Samii A, Nutt JG, Higgins DS, Griffith A, Roberts JW, Leis 870
BC, Montimurro JS, Zabetian CP, Payami H. 2008. Exploring gene-environment 871
interactions in Parkinson's disease. Hum Genet 123:257-65. 872
Meyer HE, Pedersen JI, Loken EB, Tverdal A. 1997. Dietary factors and the incidence of hip 873
fracture in middle-aged Norwegians: A prospective study. Am J Epidemiol 145:117-23. 874
33
Michels KB, Willett WC, Fuchs CS, Giovannucci E. 2005. Coffee, tea, and caffeine 875
consumption and incidence of colon and rectal cancer. J Natl Cancer Inst 97:282-92. 876
Misik M, Hoelzl C, Wagner K-, Cavin C, Moser B, Kundi M, Simic T, Elbling L, Kager N, Ferk 877
F, Ehrlich V, Nersesyan A, Dusinska M, Schilter B, Knasmuller S. 2010. Impact of paper 878
filtered coffee on oxidative DNA-damage: Results of a clinical trial. Mut Res 692:42-8. 879
Miyake Y, Kono S, Nishiwaki M, Hamada H, Nishikawa H, Koga H, Ogawa S. 1999. 880
Relationship of coffee consumption with serum lipids and lipoproteins in Japanese men. 881
Ann Epidemiol 9:121-6. 882
Monteiro M, Farah A, Perrone D, Trugo LC, Donangelo C. 2007. Chlorogenic acid compounds 883
from coffee are differentially absorbed and metabolized in humans. J Nutr 137:2196-201. 884
Naidoo N, Chen C, Rebello SA, Speer K, Tai ES, Lee J, Buchmann S, Koelling-Speer I, van 885
Dam RM. 2011. Cholesterol-raising diterpenes in types of coffee commonly consumed in 886
Singapore, Indonesia and India and associations with blood lipids: a survey and cross 887
sectional study. Nutr J 10:48. 888
Natu MV, Agarwal AK. 1997. Testing of stimulant effects of coffee on the psychomotor 889
performance: An exercise in clinical pharmacology. Indian J Pharmacol 29:11-4. 890
Nedzarek A, Torz A, Karakiewicz B, Clark JS, Laszczynska M, Kaleta A, Adler G. 2013. 891
Concentrations of heavy metals (Mn, Co, Ni, Cr, Ag, Pb) in coffee. Acta Biochim Pol 60:623-892
7. 893
Nilsson LM, Johansson I, Lenner P, Lindahl B, Van Guelpen B. 2010. Consumption of filtered 894
and boiled coffee and the risk of incident cancer: A prospective cohort study. Cancer Caus 895
Cont 21:1533-44. 896
Ochiai R, Sugiura Y, Shioya Y, Otsuka K, Katsuragi Y, Hashiguchi T. 2014. Coffee 897
polyphenols improve peripheral endothelial function after glucose loading in healthy male 898
adults. Nutr Res 34:155-9. 899
Odegaard AO, Koh WP, Yuan JM, Pereira MA. 2015. Beverage habits and mortality in 900
Chinese adults. J Nutr 145:595-604. 901
34
O'Keefe JH, Bhatti SK, Patil HR, Dinicolantonio JJ, Lucan SC, Lavie CJ. 2013. Effects of 902
habitual coffee consumption on cardiometabolic disease, cardiovascular health, and all-903
cause mortality. J Am Coll Cardiol 62:1043-51. 904
Olsen J, Overvad K, Frische G. 1991. Coffee consumption, birthweight, and reproductive 905
failures. Epidemiol 2:370-4. 906
Olthof MR, Hollman PCH, Katan MB. 2001. Chlorogenic acid and caffeic acid are absorbed in 907
humans. J Nutr 131:66-71. 908
Ostensen H, Gudmundsen TE, Ostensen M. 1985. Smoking, alcohol, coffee, and familial 909
factors: Any associations with peptic ulcer disease? A clinically and radiologically 910
prospective study. Scand J Gastroenterol 20:1227-35. 911
Otake T, Fukumoto J, Abe M, Takemura S, Mihn PN, Mizoue T, Kiyohara C. 2014. Linking 912
lifestyle factors and insulin resistance, based on fasting plasma insulin and HOMA-IR in 913
middle-aged Japanese men: A cross-sectional study. Scand J Clin Lab Invest 74:536-45. 914
Palatini P, Ceolotto G, Ragazzo F, Dorigatti F, Saladini F, Papparella I, Mos L, Zanata G, 915
Santonastaso M. 2009. CYP1A2 genotype modifies the association between coffee intake 916
and the risk of hypertension. J Hypertens 27:1594-601. 917
Panagiotakos DB, Pitsavos C, Chrysohoou C, Kokkinos P, Toutouzas P, Stefanadis C. 2003. 918
The J-shaped effect of coffee consumption on the risk of developing acute coronary 919
syndromes: the CARDIO2000 case-control study. J Nutr 133:3228-32. 920
Parazzini F, Chatenoud L, Di Cintio E, Mezzopane R, Surace M, Zanconato G, Fedele L, Benzi 921
G. 1998. Coffee consumption and risk of hospitalized miscarriage before 12 weeks of 922
gestation. Hum Reprod 13:2286-91. 923
Parazzini F, Chiaffarino F, Chatenoud L, Tozzi L, Cipriani S, Chiantera V, Fedele L. 2005. 924
Maternal coffee drinking in pregnancy and risk of small for gestational age birth. Eur J Clin 925
Nutr 59:299-301. 926
Pavanello S, Mastrangelo G, Placidi D, Campagna M, Pulliero A, Carta A, Arici C, Porru S. 927
2010. CYP1A2 polymorphisms, occupational and environmental exposures and risk of 928
bladder cancer. Eur J Epidemiol 25:491-500. 929
35
Perez de Obanos A, GonzalesPenas E, Lopez de Cerain A. 2005. Influence of roasting and 930
brew preparation on the ochratoxin A content in coffee infusion. Food Addit Contam 22:463-931
71. 932
Petridou E, Trichopoulos D, Tong D, Revinthi K, Tsitsika A, Papathoma E, Aravantinos D. 933
1996. Modulators of length of gestation: a study in Greece. Eur J Public Health 6:159-65. 934
Pietinen P, Aro A, Tuomilehto J, Uusitalo U, Korhonen H. 1990. Consumption of boiled coffee 935
is correlated with serum cholesterol in Finland. Int J Epidemiol 19:586-90. 936
Pintus F, Mascia P. 1996. Distribution and population determinants of gamma-937
glutamyltransferase in a random sample of Sardinian inhabitants. Eur J Epidemiol 12:71-938
6. 939
Piters KM, Colombo A, Olson HG, Butman SM. 1985. Effect of coffee on exercise-induced 940
angina pectoris due to coronary artery disease in habitual coffee drinkers. Am J Cardiol 941
55:277-80. 942
Popat RA, Van Den Eeden, S. K, Tanner CM, Kamel F, Umbach DM, Marder K, Mayeux R, 943
Ritz B, Ross GW, Petrovitch H, Topol B, McGuire V, Costello S, Manthripragada AD, 944
Southwick A, Myers RM, Nelson LM. 2011. Coffee, ADORA2A, and CYP1A2: The caffeine 945
connection in Parkinson's disease. Eur J Neurol 18:756-65. 946
Powers KM, Kay DM, Factor SA, Zabetian CP, Higgins DS, Samii A, Nutt JG, Griffith A, Leis 947
B, Roberts JW, Martinez ED, Montimurro JS, Checkoway H, Payami H. 2008. Combined 948
effects of smoking, coffee, and NSAIDs on Parkinson's disease risk. Move Dis 23:88-95. 949
Pujolar AE, Gonzalez CA, Lopez-Abente G, Errezola M, Izarzugaza I, Nebot M, Riboli E. 1993. 950
Bladder cancer and coffee consumption in smokers and non-smokers in Spain. Int J 951
Epidemiol 22:38-44. 952
Rosengren A, Wilhelmsen L. 1991. Coffee, coronary heart disease and mortality in middle-953
aged Swedish men: Findings from the Primary Prevention Study. J Intern Med 230:67-71. 954
Ross WG, Abbott RD, Petrovitch H, Morens DM, Grandinetti A, KoHui Tung TCM, Masaki KH, 955
Blanchette PL, Curb JD, Popper JS, White LR. 2000. Association of coffee and caffeine 956
intake with the risk of Parkinson disease. J Am Med Assoc 283:2674-9. 957
36
Rubach M, Lang R, Bytof G, Stiebitz H, Lantz I, Hofmann T, Somoza V. 2014. A dark brown 958
roast coffee blend is less effective at stimulating gastric acid secretion in healthy volunteers 959
compared to a medium roast market blend. Mol Nutr Food Res 58:1370-3. 960
Rufian-Henares JA, de la Cueva SP. 2009. Antimicrobial Activity of Coffee Melanoidins-A 961
Study of Their Metal-Chelating Properties. J Agric Food Chem 57:432-8. 962
Sanikini H, Dik VK, Siersema PD, Bhoo-Pathy N, Uiterwaal CSPM, Peeters PHM, Gonzalez 963
CA, Zamora-Ros R, Overvad K, Tjonneland A, Roswall N, Boutron-Ruault M-, Fagherazzi 964
G, Racine A, Kuhn T, Katzke V, Boeing H, Trichopoulou A, Trichopoulos D, Lagiou P, Palli 965
D, Grioni S, Vineis P, Tumino R, Panico S, Weiderpass E, Skeie G, Braaten T, Huerta JM, 966
Sanchez-Cantalejo E, Barricarte A, Sonestedt E, Wallstrom P, Nilsson LM, Johansson I, 967
Bradbury KE, Khaw K-, Wareham N, Huybrechts I, Freisling H, Cross AJ, Riboli E, Bueno-968
de-Mesquita HB. 2015. Total, caffeinated and decaffeinated coffee and tea intake and 969
gastric cancer risk: Results from the EPIC cohort study. Int J Cancer 136:E720-30. 970
Savica R, Grossardt BR, Bower JH, Ahlskog JE, Rocca WA. 2013. Risk factors for Parkinson's 971
disease may differ in men and women: An exploratory study. Horm Behav 63:308-14. 972
Scazzina F, Del Rio D, Pucci T, Campanini E, Brighenti F. 2011. Coffee polyphenols and 973
colonic fermentation: An in vivo study. Ann Nutr Metab 58:86-7. 974
Schlemper RJ, Van Der Werf SDJ, Vandenbroucke JP, Biemond I, Lamers CBHW. 1996. Risk 975
factors of peptic ulcer disease: Different impact of Helicobacter pylori in Dutch and 976
Japanese populations? J Gastroenterol Hepatol 11:825-31. 977
Sihvo S, Hemminki E. 1999. Self medication and health habits in the management of upper 978
gastrointestinal symptoms. Patient Educ Couns 37:55-63. 979
Simon D, Yen S, Cole P. 1975. Coffee drinking and cancer of the lower urinary tract. J Natl 980
Cancer Inst 54:587-91. 981
Slattery ML, West DW, Robison LM. 1988. Fluid intake and bladder cancer in Utah. Int J 982
Cancer 42:17-22. 983
37
Slattery ML, West DW, Robison LM, French TK, Ford MH, Schuman KL, Sorenson AW. 1990. 984
Tobacco, alcohol, coffee, and caffeine as risk factors for colon cancer in a low-risk 985
population. Epidemiol 1:141-5. 986
Slow S, Miller WE, McGregor DO, Lee MB, Lever M, George PM, Chambers ST. 2004. 987
Trigonelline is not responsible for the acute increase in plasma homocysteine following 988
ingestion of instant coffee. Eur J Clin Nutr 58:1253-6. 989
Smits P, Pieters G, Thien T. 1986a. The role of epinephrine in the circulatory effects of coffee. 990
Clin Pharmacol Ther 40:431-7. 991
Smits P, Thien T, van 't Laar A. 1986b. Influence of slow calcium-channel blockade on the 992
cardiovascular effects of coffee. Eur J Clin Pharmacol 30:171-5. 993
Soga S, Ota N, Shimotoyodome A. 2013. Stimulation of postprandial fat utilization in healthy 994
humans by daily consumption of chlorogenic acids. Biosci Biotech Biochem 77:1633-6. 995
Steinkellner H, Hoelzl C, Uhl M, Cavin C, Haidinger G, Gsur A, Schmid R, Kundi M, Bichler J, 996
Knasmuller S. 2005. Coffee consumption induces GSTP in plasma and protects 997
lymphocytes against (+/-)-anti-benzo[a]pyrene-7,8-dihydrodiol-9,10-epoxide induced DNA-998
damage: Results of controlled human intervention trials. Mut Res 591:264-75. 999
Strandhagen E, Landaas S, Thelle DS. 2003. Folic acid supplement decreases the 1000
homocysteine increasing effect of filtered coffee. A randomised placebo-controlled study. 1001
Eur J Clin Nutr 57:1411-7. 1002
Strandhagen E, Zetterberg H, Aires N, Palmer M, Rymo L, Blennow K, Landaas S, Thelle DS. 1003
2004. The methylenetetrahydrofolate reductase C677T polymorphism is a major 1004
determinant of coffee-induced increase of plasma homocysteine: a randomized placebo 1005
controlled study. Int J Mol Med 13:811-5. 1006
StuderRohr I, Dietrich DR, Schlatter J, Schlatter C. 1994. Ochratoxin A and coffee. 1007
Mitteilungen aus dem Gebiete der Lebensmitteluntersuchung und Hygiene 85:719-27. 1008
StuderRohr I, Dietrich DR, Schlatter J, Schlatter C. 1995. The occurrence of ochratoxin A in 1009
coffee. Food Chem Toxicol 33:341-55. 1010
38
Tan EK, Tan C, Fook-Chong SM, Lum SY, Chai A, Chung H, Shen H, Zhao Y, Teoh ML, Yih 1011
Y, Pavanni R, Chandran VR, Wong MC. 2003. Dose-dependent protective effect of coffee, 1012
tea, and smoking in Parkinson's disease: a study in ethnic Chinese. J Neurol Sci 216:163-1013
7. 1014
Tan EK, Lu ZY, Fook-Chong SMC, Tan E, Shen H, Chua E, Yih Y, Teo YY, Zhao Y. 2006. 1015
Exploring an interaction of adenosine A2A receptor variability with coffee and tea intake in 1016
Parkinson's disease. Am J Med Gen 141B:634-6. 1017
Tanaka K, Tokunaga S, Kono S, Tokudome S, Akamatsu T, Moriyama T, Zakouji H. 1998. 1018
Coffee consumption and decreased serum gamma-glutamyltransferase and 1019
aminotransferase activities among male alcohol drinkers. Int J Epidemiol 27:438-43. 1020
Taylor CM, Golding J, Hibbeln J, Emond AM. 2013. Environmental factors predicting blood 1021
lead levels in pregnant women in the UK: the ALSPAC study. PLoS ONE 8:e72371. 1022
Trimpou P, Landin-Wilhelmsen K, Oden A, Rosengren A, Wilhelmsen L. 2010. Male risk 1023
factors for hip fracture-a 30-year follow-up study in 7,495 men. Osteoporosis Int 21:409-16. 1024
Tverdal A, Stensvold I, Solvoll K, Foss OP, Lund-Larsen P, Bjartveit K. 1990. Coffee 1025
consumption and death from coronary heart disease in middle-aged Norwegian men and 1026
women. Br Med J 300:566-9. 1027
Tverdal A. 2015. Boiled coffee consumption and the risk of prostate cancer: Follow-up of 1028
224,234 Norwegian men 20-69 years. Br J Cancer 112:576-9. 1029
Umemura M, Fujii S, Asano I, Hoshino H, Lino H. 2004. Effect of "coffee mix drink" containing 1030
mannooligosaccharides from coffee mannan on defecation and fecal microbiota in healthy 1031
volunteers. Food Sci Tech Res 10:195-8. 1032
Urgert R, Weusten-van Der Wouw MPME, Hovenier R, Meyboom S, Beynen AC, Katan MB. 1033
1997. Diterpenes from coffee beans decrease serum levels of lipoprotein(a) in humans: 1034
Results from four randomised controlled trials. Eur J Clin Nutr 51:431-6. 1035
Urgert R, Vanderweg G, Kosmeijerschuil T, Vandebovenkamp P, Hovenier R, Katan M. 1995. 1036
Levels of the cholesterol-elevating diterpenes cafestol and kahweol in various coffee brews. 1037
J Agric Food Chem 43:2167-72. 1038
39
Urgert R, Meyboom S, Kuilman M, Rexwinkel H, Vissers M, Klerk M, Katan M. 1996. 1039
Comparison of effect of cafetiere and filtered coffee on serum concentrations of liver 1040
aminotransferases and lipids: Six month randomised controlled trial. Br Med J 313:1362-6. 1041
Uzcudun A, Retolaza I, Grande A, Olivar L, Garcia A, Baron M, Bouzas J. 2002. Pharyngeal 1042
cancer prevention: evidence from a case-control study involving 232 consecutive patients. 1043
J Laryngol Otol 116:523-31. 1044
Van Deventer G, Kamemoto E, Kuznicki JT, Heckert DC, Schulte MC. 1992. Lower 1045
esophageal sphincter pressure, acid secretion, and blood gastrin after coffee consumption. 1046
Dig Dis Sci 37:558-69. 1047
Van Dusseldorp M, Katan MB, Van Vliet T, Demacker PNM, Stalenhoef AFH. 1991. 1048
Cholesterol-raising factor from boiled coffee does not pass a paper filter. Arterio Thromb 1049
11:586-93. 1050
Verhagen H, Andersen R, Antoine JM, Finglas P, Hoekstra J, Kardinaal A, Nordmann H, 1051
Pekcan G, Pentieva K, Sanders TA, van den Berg H, van Kranen H, Chiodini A. 2012. 1052
Application of the BRAFO tiered approach for benefit-risk assessment to case studies on 1053
dietary interventions. Food Chem Toxicol 50 Suppl 4:S710-23. 1054
Vidry S, Hoekstra J, Hart A, Watzl B, Verhagen H, Schütte K, Boobis A, Chiodini A. 2013. 1055
Benefit-risk analysis for foods (BRAFO) - Executive project summary. Eur J Nutr Food Saf 1056
3:146-53. 1057
Walton GE, Rastall RA, Martini MC, Williams CE, Jeffries RL, Gibson GR. 2010. A double-1058
blind, placebo-controlled human study investigating the effects of coffee derived manno-1059
oligosaccharides on the faecal microbiota of a healthy adult population. Int J Pro Pre 5:75-1060
83. 1061
Werler MM, Yazdy MM, Kasser JR, Mahan ST, Meyer RE, Anderka M, Druschel CM, Mitchell 1062
AA. 2015. Maternal cigarette, alcohol, and coffee consumption in relation to risk of clubfoot. 1063
Paediatr Perinat Epidemiol 29:3-10. 1064
40
Xiao Q, Sinha R, Graubard BI, Freedman ND. 2014. Inverse associations of total and 1065
decaffeinated coffee with liver enzyme levels in National Health and Nutrition Examination 1066
Survey 1999-2010. Hepatology 60:2091-8. 1067
Yamada H, Kawado M, Aoyama N, Hashimoto S, Suzuki K, Wakai K, Suzuki S, Watanabe Y, 1068
Tamakoshi A, JACC Study Group. 2014. Coffee consumption and risk of colorectal cancer: 1069
the Japan Collaborative Cohort Study. J Epidemiol 24:370-8. 1070
Zeegers MPA, Tan FES, Goldbohm RA, Van Den Brandt PA. 2001. Are coffee and tea 1071
consumption associated with urinary tract cancer risk? A systematic review and meta-1072
analysis. Int J Epidemiol 30:353-62. 1073
Zhang B, Wei Y, Niu J, Li Y, Miao Z, Wang Z. 2010. Risk factors for unexplained recurrent 1074
spontaneous abortion in a population from southern China. Int J Gyn Obst 108:135-8. 1075
41
Table 1 Study inclusion/exclusion criteria 1076
INCLUSION CRITERIA EXCLUSION CRITERIA
Human observational and intervention original
research studies
Examined coffee consumption and reported
health outcome(s)
English
Published 1970 - 30th June 2015
In vitro or animal studies, systematic reviews or
meta-analyses
No health outcome
No original data (e.g. letters/editorials)
Not available in English
Published before 1970
1077
1078
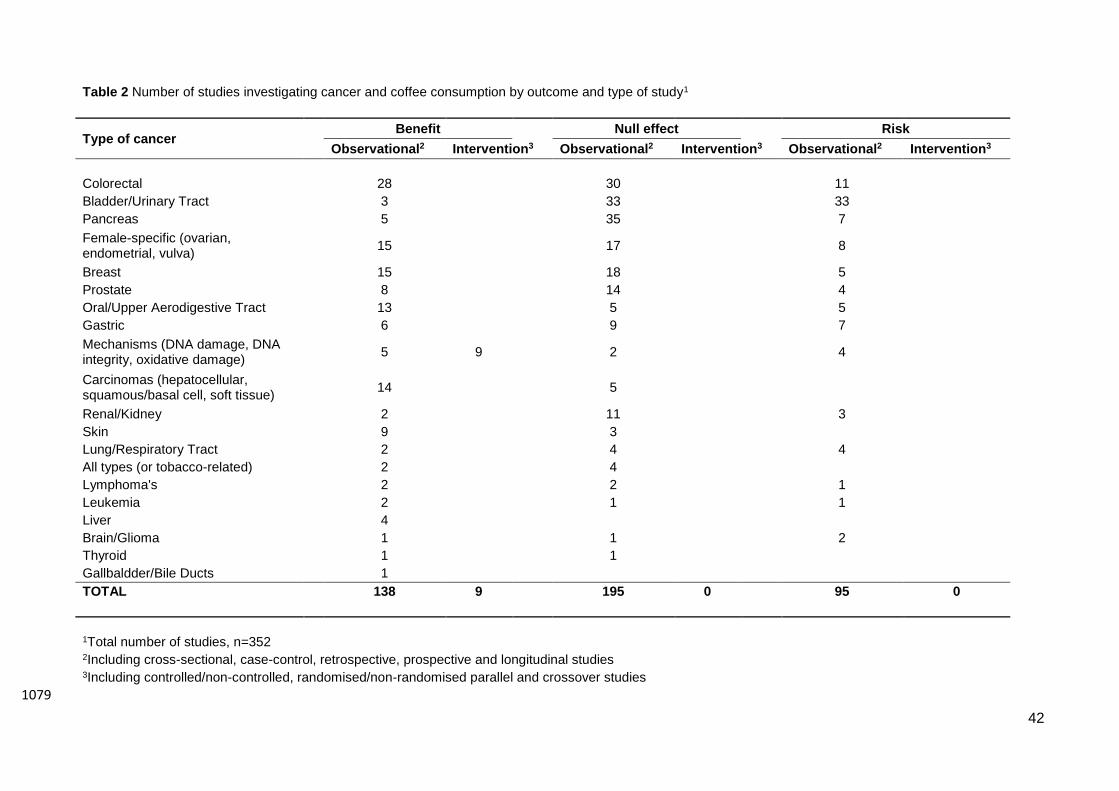
42
Table 2 Number of studies investigating cancer and coffee consumption by outcome and type of study1
Type of cancer Benefit Null effect Risk
Observational2 Intervention3 Observational2 Intervention3 Observational2 Intervention3
Colorectal 28 30 11
Bladder/Urinary Tract 3 33 33
Pancreas 5 35 7
Female-specific (ovarian, endometrial, vulva)
15 17 8
Breast 15 18 5
Prostate 8 14 4
Oral/Upper Aerodigestive Tract 13 5 5
Gastric 6 9 7
Mechanisms (DNA damage, DNA integrity, oxidative damage)
5 9 2 4
Carcinomas (hepatocellular, squamous/basal cell, soft tissue)
14 5
Renal/Kidney 2 11 3
Skin 9 3
Lung/Respiratory Tract 2 4 4
All types (or tobacco-related) 2 4
Lymphoma's 2 2 1
Leukemia 2 1 1
Liver 4
Brain/Glioma 1 1 2
Thyroid 1 1
Gallbaldder/Bile Ducts 1
TOTAL 138 9 195 0 95 0
1Total number of studies, n=352 2Including cross-sectional, case-control, retrospective, prospective and longitudinal studies 3Including controlled/non-controlled, randomised/non-randomised parallel and crossover studies
1079
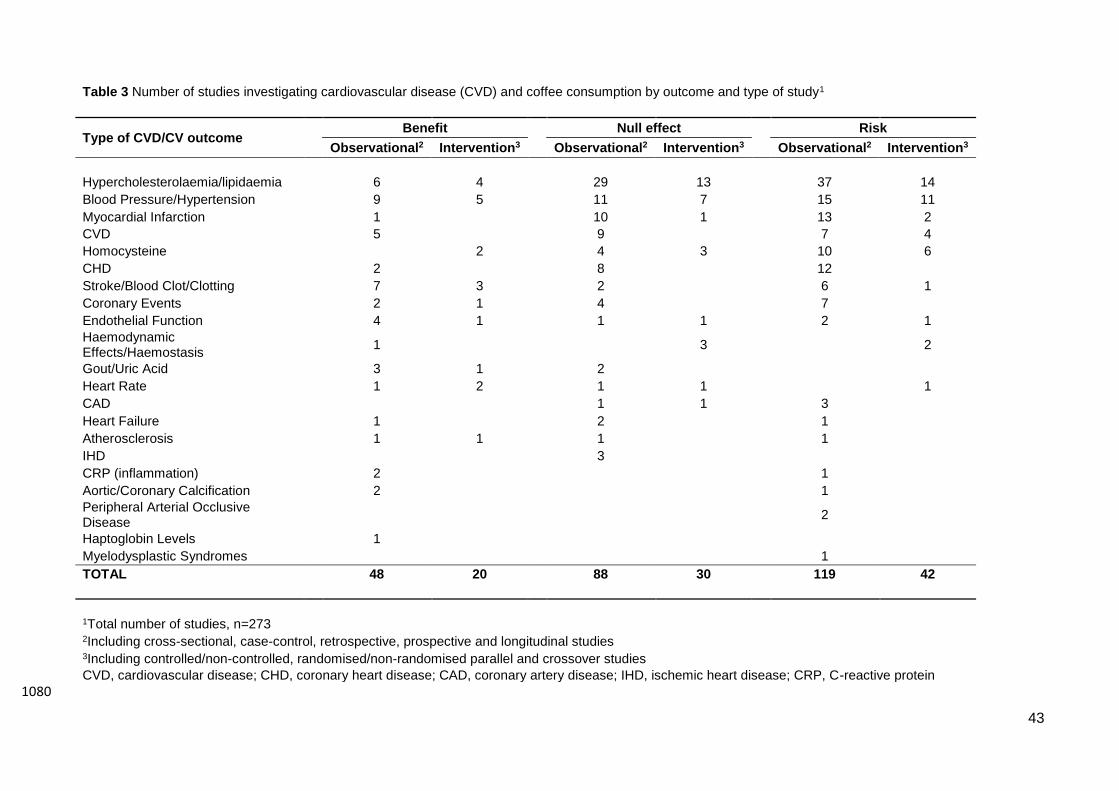
43
Table 3 Number of studies investigating cardiovascular disease (CVD) and coffee consumption by outcome and type of study1
Type of CVD/CV outcome Benefit Null effect Risk
Observational2 Intervention3 Observational2 Intervention3 Observational2 Intervention3
Hypercholesterolaemia/lipidaemia 6 4 29 13 37 14
Blood Pressure/Hypertension 9 5 11 7 15 11
Myocardial Infarction 1 10 1 13 2
CVD 5 9 7 4
Homocysteine 2 4 3 10 6
CHD 2 8 12
Stroke/Blood Clot/Clotting 7 3 2 6 1
Coronary Events 2 1 4 7
Endothelial Function 4 1 1 1 2 1
Haemodynamic Effects/Haemostasis
1 3 2
Gout/Uric Acid 3 1 2
Heart Rate 1 2 1 1 1
CAD 1 1 3
Heart Failure 1 2 1
Atherosclerosis 1 1 1 1
IHD 3
CRP (inflammation) 2 1
Aortic/Coronary Calcification 2 1
Peripheral Arterial Occlusive Disease
2
Haptoglobin Levels 1
Myelodysplastic Syndromes 1
TOTAL 48 20 88 30 119 42
1Total number of studies, n=273 2Including cross-sectional, case-control, retrospective, prospective and longitudinal studies 3Including controlled/non-controlled, randomised/non-randomised parallel and crossover studies
CVD, cardiovascular disease; CHD, coronary heart disease; CAD, coronary artery disease; IHD, ischemic heart disease; CRP, C-reactive protein
1080
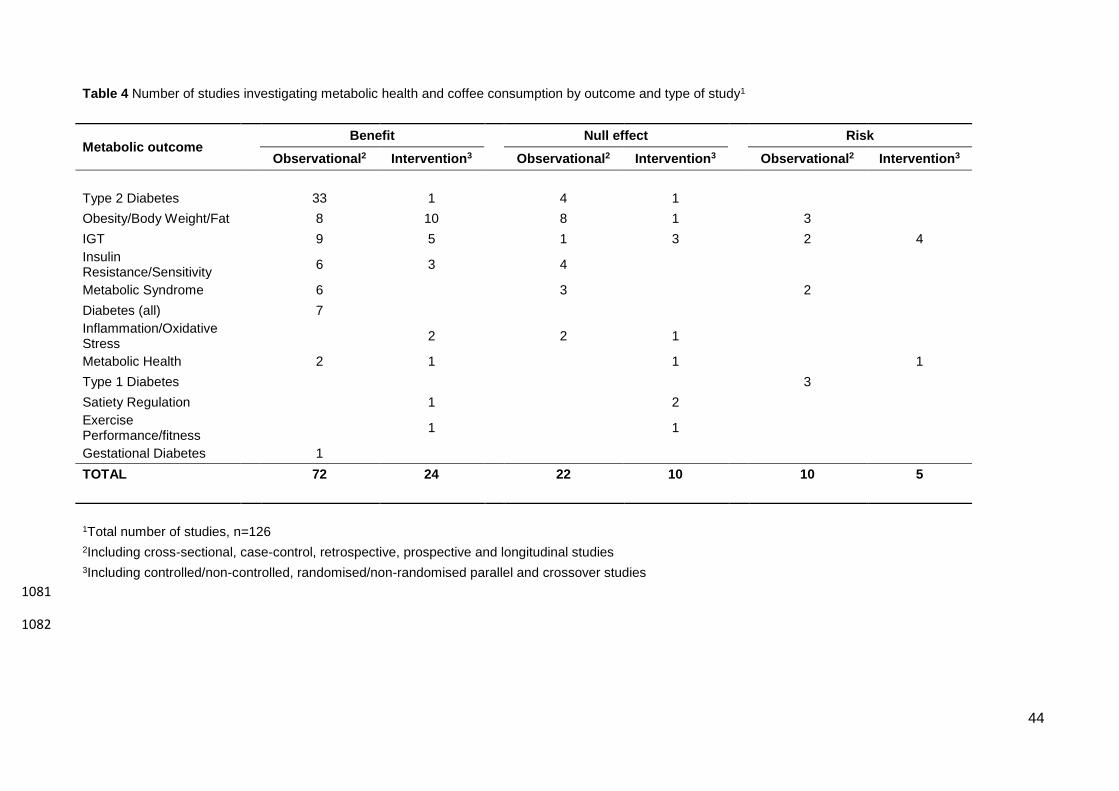
44
Table 4 Number of studies investigating metabolic health and coffee consumption by outcome and type of study1
Metabolic outcome Benefit Null effect Risk
Observational2 Intervention3 Observational2 Intervention3 Observational2 Intervention3
Type 2 Diabetes 33 1 4 1
Obesity/Body Weight/Fat 8 10 8 1 3
IGT 9 5 1 3 2 4
Insulin Resistance/Sensitivity
6 3 4
Metabolic Syndrome 6 3 2
Diabetes (all) 7
Inflammation/Oxidative Stress
2 2 1
Metabolic Health 2 1 1 1
Type 1 Diabetes 3
Satiety Regulation 1 2
Exercise Performance/fitness
1 1
Gestational Diabetes 1
TOTAL 72 24 22 10 10 5
1Total number of studies, n=126
2Including cross-sectional, case-control, retrospective, prospective and longitudinal studies
3Including controlled/non-controlled, randomised/non-randomised parallel and crossover studies
1081
1082
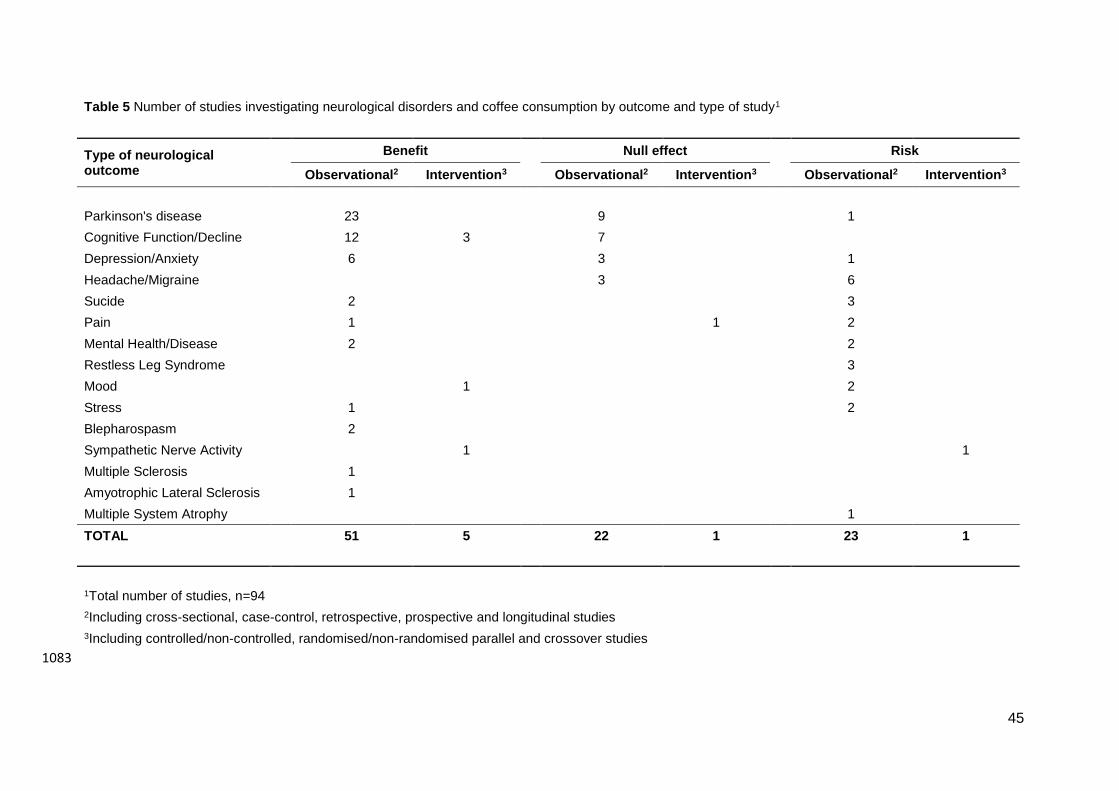
45
Table 5 Number of studies investigating neurological disorders and coffee consumption by outcome and type of study1
Type of neurological outcome
Benefit Null effect Risk
Observational2 Intervention3 Observational2 Intervention3 Observational2 Intervention3
Parkinson's disease 23 9 1
Cognitive Function/Decline 12 3 7
Depression/Anxiety 6 3 1
Headache/Migraine 3 6
Sucide 2 3
Pain 1 1 2
Mental Health/Disease 2 2
Restless Leg Syndrome 3
Mood 1 2
Stress 1 2
Blepharospasm 2
Sympathetic Nerve Activity 1 1
Multiple Sclerosis 1
Amyotrophic Lateral Sclerosis 1
Multiple System Atrophy 1
TOTAL 51 5 22 1 23 1
1Total number of studies, n=94
2Including cross-sectional, case-control, retrospective, prospective and longitudinal studies
3Including controlled/non-controlled, randomised/non-randomised parallel and crossover studies
1083
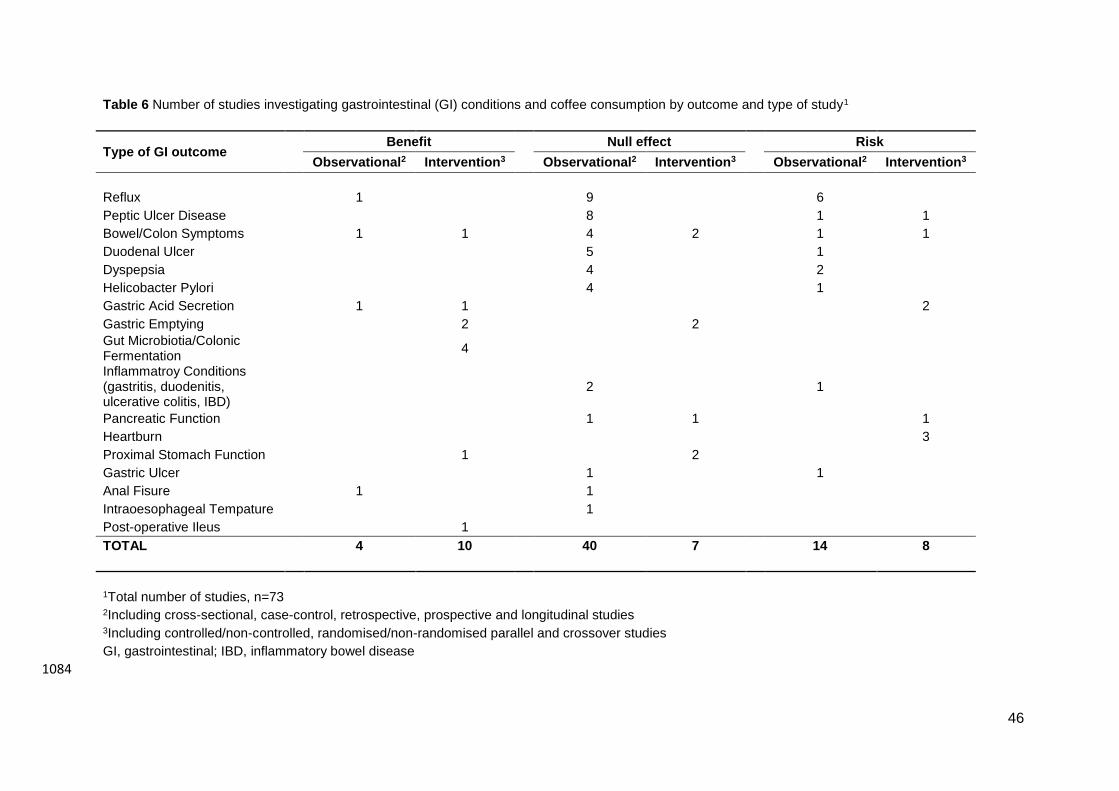
46
Table 6 Number of studies investigating gastrointestinal (GI) conditions and coffee consumption by outcome and type of study1
Type of GI outcome Benefit Null effect Risk
Observational2 Intervention3 Observational2 Intervention3 Observational2 Intervention3
Reflux 1 9 6
Peptic Ulcer Disease 8 1 1
Bowel/Colon Symptoms 1 1 4 2 1 1
Duodenal Ulcer 5 1
Dyspepsia 4 2
Helicobacter Pylori 4 1
Gastric Acid Secretion 1 1 2
Gastric Emptying 2 2
Gut Microbiotia/Colonic Fermentation
4
Inflammatroy Conditions (gastritis, duodenitis, ulcerative colitis, IBD)
2 1
Pancreatic Function 1 1 1
Heartburn 3
Proximal Stomach Function 1 2
Gastric Ulcer 1 1
Anal Fisure 1 1
Intraoesophageal Tempature 1
Post-operative Ileus 1
TOTAL 4 10 40 7 14 8
1Total number of studies, n=73 2Including cross-sectional, case-control, retrospective, prospective and longitudinal studies 3Including controlled/non-controlled, randomised/non-randomised parallel and crossover studies
GI, gastrointestinal; IBD, inflammatory bowel disease
1084
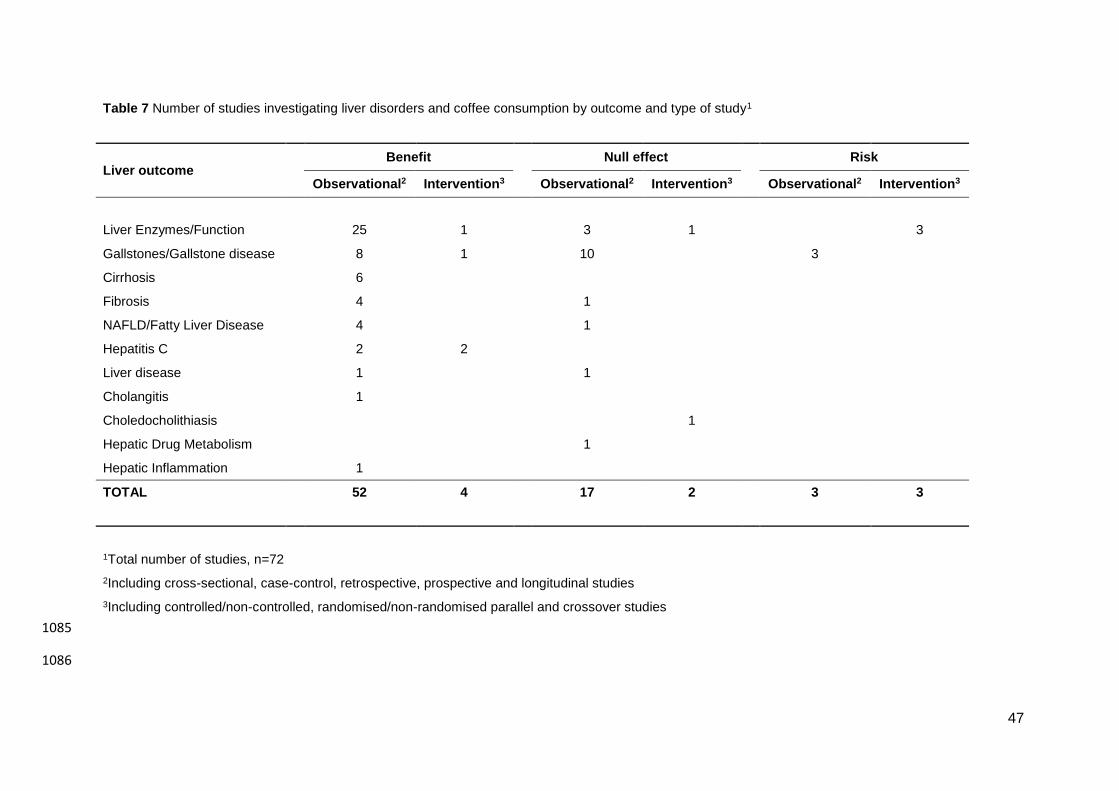
47
Table 7 Number of studies investigating liver disorders and coffee consumption by outcome and type of study1
Liver outcome Benefit Null effect Risk
Observational2 Intervention3 Observational2 Intervention3 Observational2 Intervention3
Liver Enzymes/Function 25 1 3 1 3
Gallstones/Gallstone disease 8 1 10 3
Cirrhosis 6
Fibrosis 4 1
NAFLD/Fatty Liver Disease 4 1
Hepatitis C 2 2
Liver disease 1 1
Cholangitis 1
Choledocholithiasis 1
Hepatic Drug Metabolism 1
Hepatic Inflammation 1
TOTAL 52 4 17 2 3 3
1Total number of studies, n=72
2Including cross-sectional, case-control, retrospective, prospective and longitudinal studies
3Including controlled/non-controlled, randomised/non-randomised parallel and crossover studies
1085
1086
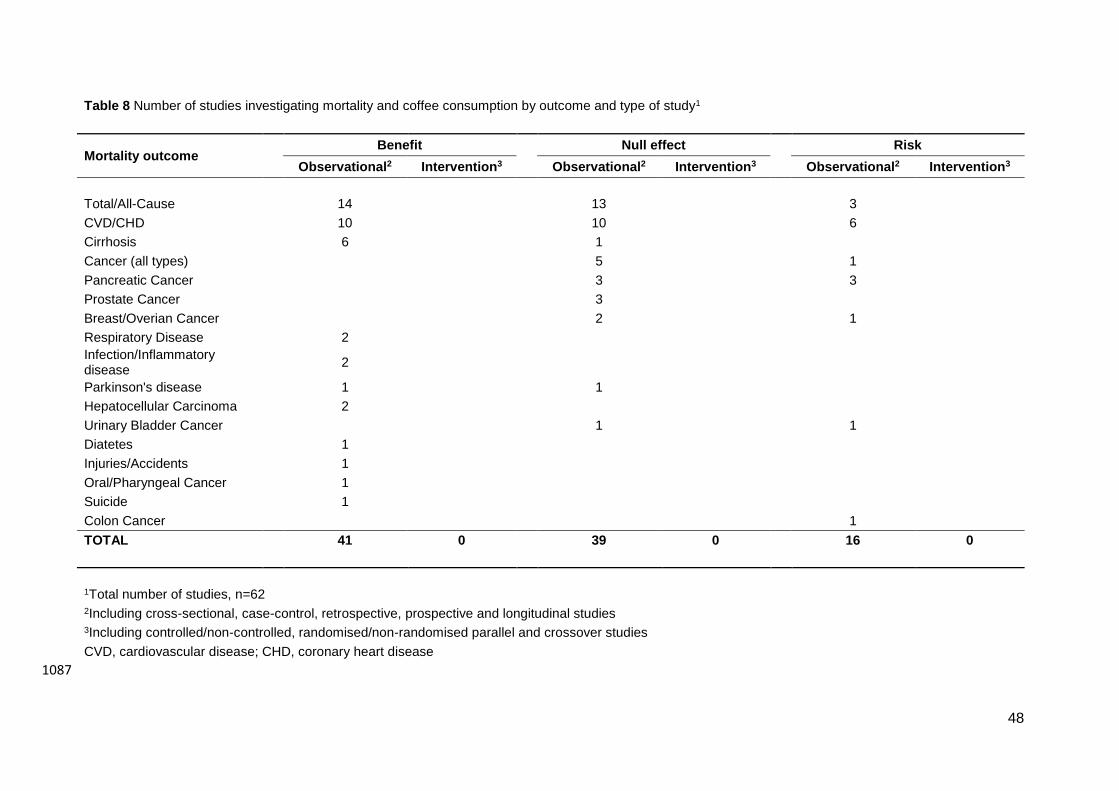
48
Table 8 Number of studies investigating mortality and coffee consumption by outcome and type of study1
Mortality outcome Benefit Null effect Risk
Observational2 Intervention3 Observational2 Intervention3 Observational2 Intervention3
Total/All-Cause 14 13 3
CVD/CHD 10 10 6
Cirrhosis 6 1
Cancer (all types) 5 1
Pancreatic Cancer 3 3
Prostate Cancer 3
Breast/Overian Cancer 2 1
Respiratory Disease 2
Infection/Inflammatory disease
2
Parkinson's disease 1 1
Hepatocellular Carcinoma 2
Urinary Bladder Cancer 1 1
Diatetes 1
Injuries/Accidents 1
Oral/Pharyngeal Cancer 1
Suicide 1
Colon Cancer 1
TOTAL 41 0 39 0 16 0
1Total number of studies, n=62 2Including cross-sectional, case-control, retrospective, prospective and longitudinal studies 3Including controlled/non-controlled, randomised/non-randomised parallel and crossover studies
CVD, cardiovascular disease; CHD, coronary heart disease
1087
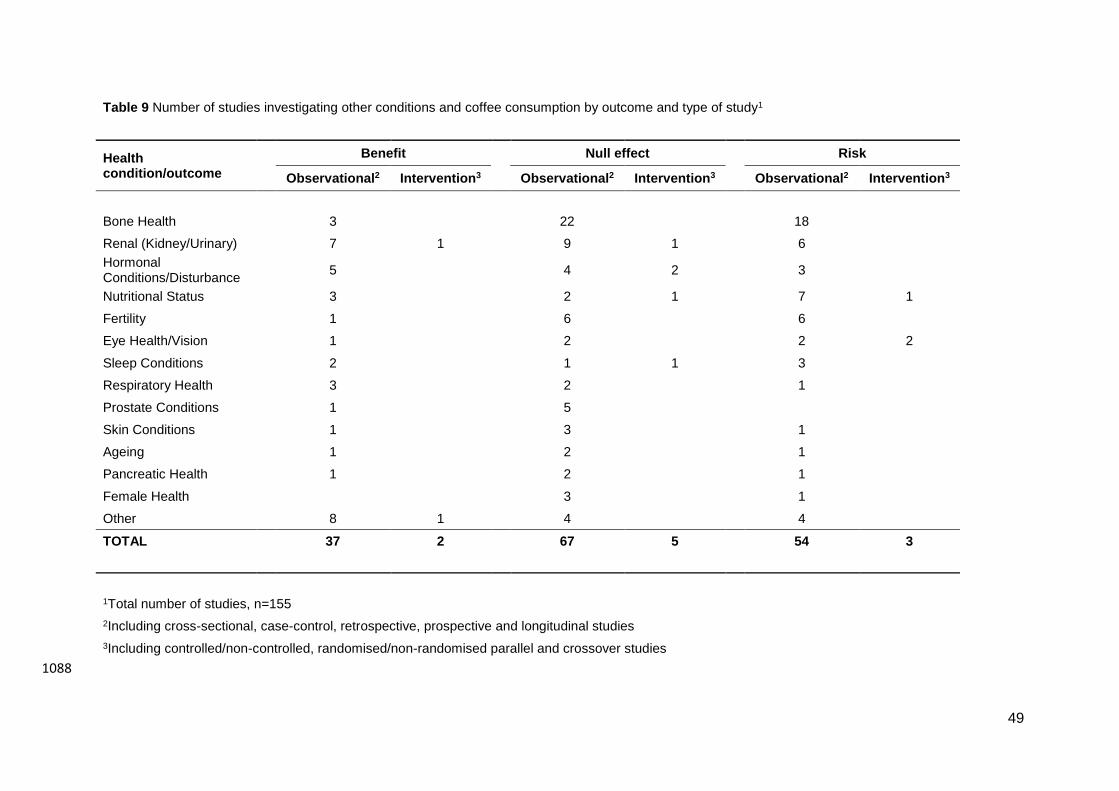
49
Table 9 Number of studies investigating other conditions and coffee consumption by outcome and type of study1
Health condition/outcome
Benefit Null effect Risk
Observational2 Intervention3 Observational2 Intervention3 Observational2 Intervention3
Bone Health 3 22 18
Renal (Kidney/Urinary) 7 1 9 1 6
Hormonal Conditions/Disturbance
5 4 2 3
Nutritional Status 3 2 1 7 1
Fertility 1 6 6
Eye Health/Vision 1 2 2 2
Sleep Conditions 2 1 1 3
Respiratory Health 3 2 1
Prostate Conditions 1 5
Skin Conditions 1 3 1
Ageing 1 2 1
Pancreatic Health 1 2 1
Female Health 3 1
Other 8 1 4 4
TOTAL 37 2 67 5 54 3
1Total number of studies, n=155
2Including cross-sectional, case-control, retrospective, prospective and longitudinal studies
3Including controlled/non-controlled, randomised/non-randomised parallel and crossover studies
1088
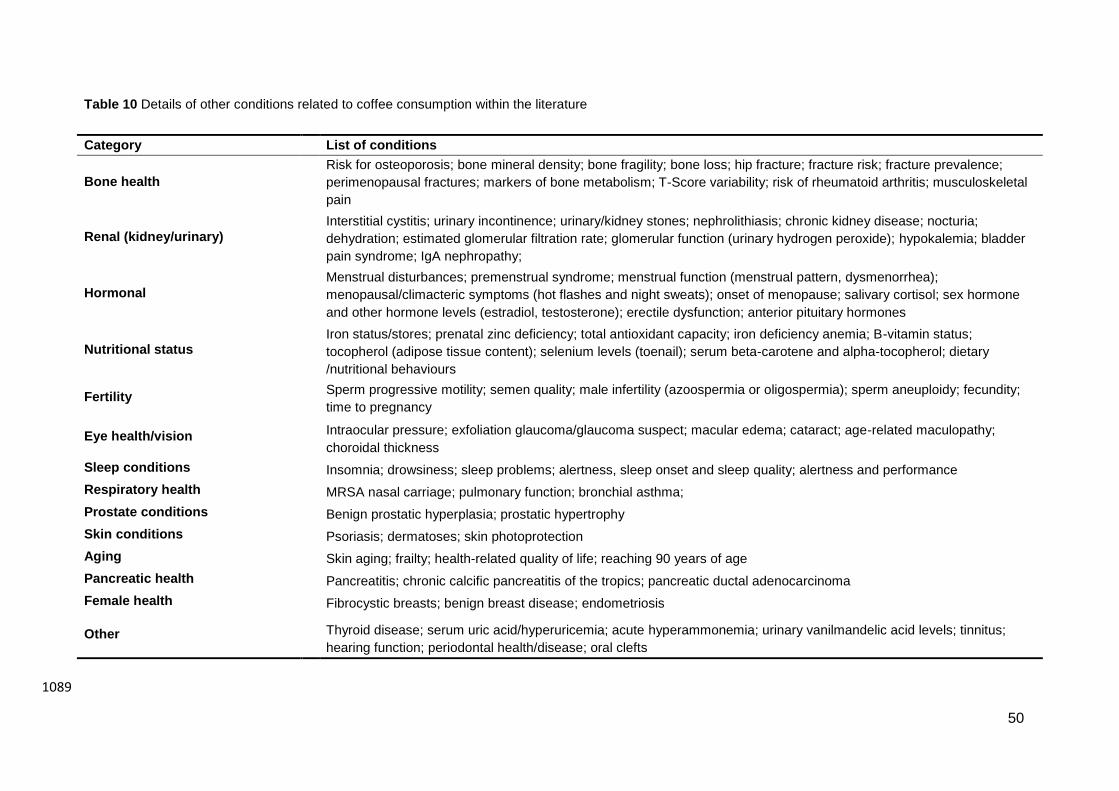
50
Table 10 Details of other conditions related to coffee consumption within the literature
Category List of conditions
Bone health
Risk for osteoporosis; bone mineral density; bone fragility; bone loss; hip fracture; fracture risk; fracture prevalence;
perimenopausal fractures; markers of bone metabolism; T-Score variability; risk of rheumatoid arthritis; musculoskeletal
pain
Renal (kidney/urinary)
Interstitial cystitis; urinary incontinence; urinary/kidney stones; nephrolithiasis; chronic kidney disease; nocturia;
dehydration; estimated glomerular filtration rate; glomerular function (urinary hydrogen peroxide); hypokalemia; bladder
pain syndrome; IgA nephropathy;
Hormonal
Menstrual disturbances; premenstrual syndrome; menstrual function (menstrual pattern, dysmenorrhea);
menopausal/climacteric symptoms (hot flashes and night sweats); onset of menopause; salivary cortisol; sex hormone
and other hormone levels (estradiol, testosterone); erectile dysfunction; anterior pituitary hormones
Nutritional status
Iron status/stores; prenatal zinc deficiency; total antioxidant capacity; iron deficiency anemia; B-vitamin status;
tocopherol (adipose tissue content); selenium levels (toenail); serum beta-carotene and alpha-tocopherol; dietary
/nutritional behaviours
Fertility
Sperm progressive motility; semen quality; male infertility (azoospermia or oligospermia); sperm aneuploidy; fecundity;
time to pregnancy
Eye health/vision
Intraocular pressure; exfoliation glaucoma/glaucoma suspect; macular edema; cataract; age-related maculopathy;
choroidal thickness
Sleep conditions Insomnia; drowsiness; sleep problems; alertness, sleep onset and sleep quality; alertness and performance
Respiratory health MRSA nasal carriage; pulmonary function; bronchial asthma;
Prostate conditions Benign prostatic hyperplasia; prostatic hypertrophy
Skin conditions Psoriasis; dermatoses; skin photoprotection
Aging Skin aging; frailty; health-related quality of life; reaching 90 years of age
Pancreatic health Pancreatitis; chronic calcific pancreatitis of the tropics; pancreatic ductal adenocarcinoma
Female health Fibrocystic breasts; benign breast disease; endometriosis
Other
Thyroid disease; serum uric acid/hyperuricemia; acute hyperammonemia; urinary vanilmandelic acid levels; tinnitus;
hearing function; periodontal health/disease; oral clefts
1089
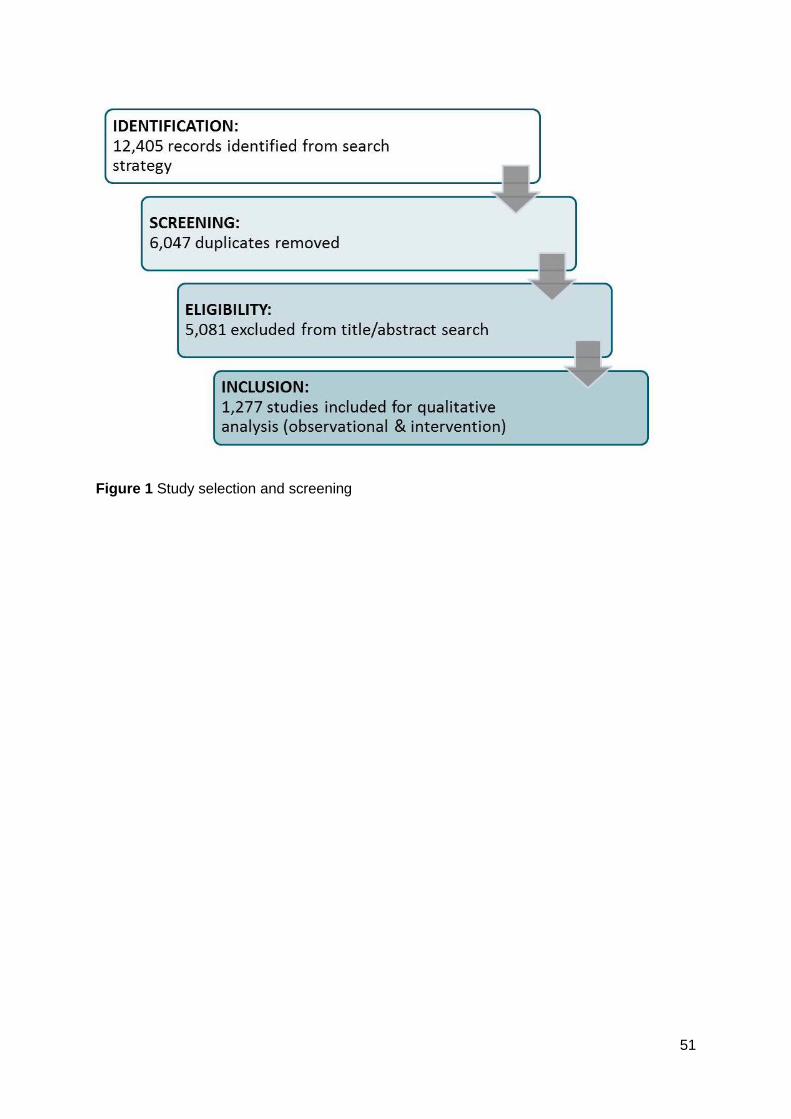
51
Figure 1 Study selection and screening





























