Embed Size (px)
Citation preview

Eating Behaviors 10 (2009) 10–15
Contents lists available at ScienceDirect
Eating Behaviors
A consideration of developmental egocentrism in anorexia nervosa
Andrew Fox a,⁎, Chris Harrop a,b, Peter Trower a,c, Newman Leung a,c
a School of Psychology, University of Birmingham, Edgbaston B15 2TT, UKb West London Mental Health NHS Trust, Lakeside, Isleworth, Middlesex, UKc Birmingham and Solihull Mental Health Trust, Birmingham, UK
⁎ Corresponding author. Tel.: +44 121 414 7124.E-mail address: [email protected] (A. Fox).
1471-0153/$ – see front matter © 2008 Elsevier Ltd. Aldoi:10.1016/j.eatbeh.2008.10.001
a b s t r a c t
a r t i c l e i n f oArticle history:
Recent research has suggeste Received 4 January 2008Received in revised form 8 August 2008Accepted 8 October 2008Keywords:Anorexia nervosaAdolescenceSelfDevelopmental
d that normal adolescent processes are important in understanding psychosis, andthat young adult individuals with psychosis are often struggling to develop an individual and autonomous self(the “fundamental task” of adolescence). The current paper explores the utility of considering normativeadolescent developmental processes in understanding anorexia nervosa. Data were collected from 31 femaleyoung-adultswith symptomsof anorexia nervosa, 26 female comparisonyoung-adults and71 femaleadolescentsonmeasures of adolescent egocentrism. Aone-wayANOVA indicated that individualswith symptoms of anorexianervosa scored more highly than both their peers and the adolescents on several dimensions of egocentricdevelopmental beliefs. Correlations also showed that egocentrismwas positively associated with eating concernin participants with symptoms of anorexia. The results suggest that young-adult women with symptoms ofanorexia nervosa tended to feel physically invulnerable while also feeling both psychologically vulnerable toothers and special or different. Together with the finding of excessive self-consciousness, this supports a notionthat they may be experiencing exaggerated versions of normal self-developmental phenomena. Clinically,offering alternative ways of feeling unique other than dieting may be important in therapeutic approaches toanorexia nervosa. Similarly, strategies aimed at normalisation, such as facilitating healthy attachment to peers,may be useful for individuals with anorexia nervosa.
© 2008 Elsevier Ltd. All rights reserved.
1. Introduction
Adolescence is an important developmental stage, where beliefsabout the self are developed and individual boundaries are negotiatedand expanded (Harter, 1999). Given that several psychopathologiesonset during adolescence and the following period of ‘emerging-adulthood’ (Arnett, 2000), including eating disorders (Fairburn &Harrison, 2003) and psychosis (Hafner, 2003), it is somewhatsurprising that little research has examined the role of adolescentdevelopmental processes in mental health difficulties. Some recentresearch has explicitly considered the importance of adolescentdevelopmental phenomena in the onset of psychosis (Harrop &Trower, 2001, 2003); however, there has been little consideration ofthe role of these same phenomena in other mental health difficulties.This paper aims to consider whether these processes of adolescentdevelopment are relevant to an understanding of anorexia nervosa —
an illness that typically affects adolescents and young people (Fairburn& Harrison, 2003).
l rights reserved.
1.1. Adolescent development
Recent research has considered the role of social factors withinadolescent development, with particular emphasis on the develop-ment of a unique and individual self identity (Lapsley, 1993). Inessence, it seems that adolescents are making their first attempts toprovide an answer to the question ‘who am I?’ (Rosenberg, 1979).Typical adolescent feelings of uniqueness and self-consciousness arethought to reflect the ‘personal fable’ (the belief that one is special orunique) and ‘imaginary audience’ (the belief that others are alwayswatching) (Elkind, 1967).
In order to move beyond this stage of development, it has beenargued that adolescents must meet a variety of psychosocial challenges,such as negotiating increasing independence, developing romanticrelationships, exploring self-identity, and choosing a career (Hendry &Kloep, 2003). In meeting these challenges, adolescents are beginning todevelop a coherent sense of self, and starting a process that continuesinto emerging-adulthood (Arnett, 2000; Frankenberger, 2000). Indeed,Frankenberger (2000) found that personal fable beliefs continuedbeyond adolescence and into early adulthood and concluded thatthese cognitions reflect attempts to maintain a sense of self duringseparation–individuation from parents. More recently, personal fablecognitions have been separated into several distinct dimensions,including beliefs regarding personal uniqueness, invulnerability andomnipotence (Duggan, Lapsley & Norman, 2000; Goosens, Beyers,

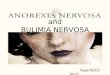
Table 1Comparison of egocentrism scores across the adolescent, anorexia and adult groups
Anorexia Adolescents Comparison F Comparisons
N=31 N=71 N=26 (pb .05)
M (SD) M (SD) M (SD)
Dangerinvulnerability
2.20 (.88) 1.92 (.42) 1.89 (.48) 2.99 –
Psychologicalinvulnerability
1.61 (.57) 2.24 (.59) 2.07 (.44) 13.83⁎ ANbA, A=C, ANbC
Doubts aboutbeing understood
3.53 (.64) 2.53 (.69) 2.07 (.80) 34.08⁎ ANNANC
Doubts aboutbeing the same
3.59 (.57) 2.97 (.53) 2.70 (.52) 21.60⁎ ANNA=C
Public selfconsciousness
3.44 (.64) 2.81 (.70) 2.43 (.81) 15.10⁎ ANNA=C
⁎ pb .001.
11A. Fox et al. / Eating Behaviors 10 (2009) 10–15
Emmen&vanAken, 2002).However, the role that thesebeliefsmay playin adolescent self-development, and whether they are indeed confinedto adolescence as originally suggested by Elkind (1967), has not beenwell explored.
1.2. Self-development and psychopathology
While typical adolescent development is a time of increased self-focus, other research has linked self-focused attention with a varietyofmental health problems (Penn &Witkin,1994). Aalsma, Lapsley, andFlannery (2006) found that personal uniqueness was linked todepression and suicidal ideation in adolescents, and suggest it is arisk-factor for internalising symptomatology. Furthermore, self-con-sciousness is commonly associated with the imaginary audience(Vartanian, 2000) and has been linked with a variety of mental healthissues (see Ruiperez & Belloch, 2003). Several disorders onset duringadolescence, including both anorexia nervosa and psychosis, however,relatively little research has examined the normative adolescentprocesses of self-development in young people with mental healthdifficulties.
There is some previous research that does suggest that individualswith anorexia nervosa are struggling with normal development (e.g.separation–individuation issues, Barth, 2003; self-esteem, Halvorsen& Heyerdahl, 2006; self-consciousness, Rosen, Reiter & Orosan, 1995).Rhodes and Kroger (1992) found that eating disordered young-adultwomen demonstrated particularly high levels of separation anxiety,suggesting that they had failed to resolve the adolescent task ofseparation–individuation. Indeed, traditional eating psychopathologyliterature suggests that individuals with anorexia nervosa struggle toform an identity of their own, and strive to live up to the expectationsof others in order to secure a sense of self (Bruch, 1978). Thisperspective has also been supported in more recent analyses in thecourse of development and recovery in anorexia nervosa (Weaver,Wuest & Ciliska, 2005).
It is possible that people who experience anorexia nervosa duringadolescence may have difficulties with progressing beyond this stageof personal development, in a similar manner to that observed inyoung-adult psychosis (Harrop & Trower, 2001, 2003). If this is thecase, then it would be expected that individuals with symptoms ofanorexia nervosa would demonstrate exaggerated egocentric beliefsand problems with autonomy. One possible explanation could be thatthe difficulties associated with adolescence focus some individualsupon observable aspects of themselves (e.g. Fredrickson & Roberts,1997; Thompson, Dinnel & Dill, 2003), which when combined withperfectionistic and controlling personality characteristics (Bjorck,Clinton, Sohlberg, Hallstrom, & Norring, 2003) leads to symptoms ofanorexia nervosa — a theme common in many of the cognitive–behavioural models of anorexia nervosa (e.g. Fairburn, Cooper &Shafran, 2003; Garner & Bemis, 1982; Slade, 1982).
It is unclear from the literature which egocentric beliefs areassociated with which self-developmental aspects of adolescence,and this makes it problematic to offer precise predictions re-garding the elements of adolescent egocentrism that will be as-sociated with psychopathology. However, it may be speculatedthat adult individuals with symptoms of anorexia nervosa may beexpected to demonstrate egocentric cognitions regarding self-consciousness and the personal fable (the belief that one is uniqueand invulnerable).
1.3. Current aims and hypotheses
The current paper has outlined the possibility that people withsymptoms of anorexia nervosa may also experience exaggeratedadolescent beliefs. Such beliefs, although normative in adolescence,have been associated with negative affect (Penn & Witkin, 1994) andexperiences of psychosis (Harrop & Trower, 2001, 2003). In an effort to
explore this possible relationship further, levels of specific egocentricbeliefs will be measured in adolescent individuals without a history ofmental health problems in order to assess ‘normative’ levels ofegocentrism. These scores will be compared to young adult indivi-duals with anorexia nervosa and a matched non-clinical group. Threehypotheses are made:
1) Non-clinical adolescents will score more highly on measures ofegocentric beliefs (personal uniqueness, adolescent invulnerabilityand public self-consciousness) than non-clinical adults, as sug-gested by the traditional adolescent cognitive developmentaltheory of Elkind (1967).
2) Adult individuals who have experienced symptoms of anorexianervosa will score more highly on measures of egocentric beliefsthan an age-matched comparison group; in effect, they will bemore like adolescents than their contemporaries.
3) There will be significant positive correlations between eatingdisorder symptom severity and levels of egocentricity in adultindividuals with symptoms of anorexia but not in adult individualswithout symptoms of anorexia.
2. Methods
2.1. Participants
31 individuals with symptoms of anorexia nervosa wererecruited through opportunity sampling from eating disordersteams within the local health authority area (Birmingham andSolihull) and from adverts posted out to self-help groups around thecountry, through a UK based charity (‘beat’, formerly known as theEating Disorders Association). Individuals were included if theyindicated that they had experienced symptoms of dietary restriction(with or without bulimic symptoms) in the last 12 months and wereaged between 18 and 30 (M=22.87, SD=2.32). All participants inthis anorexia group were female and of white ethnic background(although neither gender nor ethnic bias was specifically sought). Acomparison group of 26 non-eating-disordered women wasassembled through personal contacts, also aged between 18 and30 (M=22.77 SD=3.53) and was matched as closely as practicable tothe anorexia group for age, educational experiences and ethnicbackground. This group reported no previous history with psychia-tric services. Both groups completed the Eating Disorders Examina-tion Questionnaire (Fairburn & Beglin, 1994; EDE-Q) to help ensurethey matched the recruitment criteria; scores above 3.09 on theglobal subscale of the EDE-Q were taken as an indication of thepresence of eating psychopathology (Mond, Hay, Rodgers, Owen &Beumont, 2004). In the anorexia group, 34 individuals wereoriginally recruited, but 3 were not entered into the final anorexiadata-set due to scores that were below this threshold. In the final

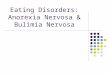
Table 2Test of associations between eating disorder symptom scores and developmental egocentricity in the anorexia group
Eating Disorder ExaminationQuestionnaire Subscale
Public self-consciousness Danger invulnerability Psychological Invulnerability Doubts about being understood Doubts aboutbeing the same
Dietary restriction − .04 − .15 − .03 .10 .06Eating concern .36⁎ .39⁎ .02 .39⁎ − .14Shape concern .17 .10 .12 .17 − .14Weight concern .03 − .10 − .02 .14 − .10
⁎ pb .05.
12 A. Fox et al. / Eating Behaviors 10 (2009) 10–15
analysis, 15 individuals reported at least one episode of binge-eating(bulimic behaviour) in addition to their restrictive symptoms. Anadolescent comparison group of 71 females were recruited from alocal school, aged between 16 and 17 (M=16.87, SD= .34), althoughthey were not screened with the EDE-Q.
2.2. Measures
A version of the Adolescent Invulnerability Scale (AIS; Duggan et al.,2000) was used to measure the invulnerability component of thepersonal fable. It consists of 21 items ratedby theparticipanton a5-pointagreement scale, ranging through: 1. strongly disagree; 2. disagree; 3.neutral; 4. agree; 5. strongly agree. 12 items represent ‘dangerinvulnerability’ (e.g. ‘There are times when I think I am indestructible’),while 9 represent ‘psychological invulnerability’ (e.g. ‘It is just impossiblefor people to hurt my feelings’). The scale has demonstrated acceptableinternal reliability,when administered to a sample of 80 femalefirst-yearUniversity students (mean age=18.53, SD= .95), with the dangerinvulnerability scale yielding a Chronbach's alpha of .82, and thepsychological invulnerability subscale an alpha of .80.
A slightly modified version of the Personal Uniqueness Scale(PUS; Duggan et al., 2000) was used to measure the uniquenesscomponent of the personal fable. The same reliability analysis asused for the AIS suggested that one item in the doubts about beingunderstood subscale (‘There isn't anything special about me’)should not be reversed, despite the wording of the item indicatingthe opposite. Upon closer inspection, the item did not appear toreflect the underlying construct of doubts about being understood,and was deleted from the analysis. The final version consisted of 20items rated on the same 5-point scale as the AIS, with 12 items thatrepresent doubts about ‘being understood’ by others (e.g. ‘No-onereally understands me’), and 8 that represent doubts about ‘beingthe same’ as others (e.g. ‘I am very different from my friends’). Thisversion of the scale yielded a Chronbach's alpha of .92 for thedoubts about being understood subscale, and .70 for the doubtsabout being the same subscale. A copy of both the PUS and the AISused in the current study can be supplied upon request from thefirst author.
The ‘Public’ subscale of the Self Consciousness Scale (SCS;Fenigstein, Scheier & Buss, 1975) was used to assess levels of concernregarding aspects of the self that are on public display. Public self-consciousness has been linked to concerns about the imaginaryaudience (Frankenberger, 2000; Vartanian, 2000) and psychopathol-
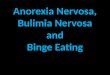
Table 3Test of associations between eating disorder symptom scores and developmental egocentri
Eating Disorder ExaminationQuestionnaire Subscale
Public self-consciousness Danger invulnerability Psycholo
Dietary restriction .14 − .27 − .21Eating concern .18 .02 − .24Shape concern .40⁎ − .05 − .22Weight concern .38⁎ − .10 − .06
⁎ pb .05.
ogy (Ruiperez & Belloch, 2003). It consists of 7 items rated on a 4point scale ranging through: 0, ‘not at all like me’; 1, a little like me; 2,somewhat like me; 3, ‘a lot like me’. The scale has previously shownadequate internal reliability with Chronbach's alpha reported at .79(Britt, 1992).
2.3. Procedure
Individuals completed the questionnaires on their own andreturned them anonymously in the post, whereupon they received£5 for their participation in the study.
Adolescent individuals were recruited from a local school, andasked to complete the questionnaires in a classroom situation insilence. They were not paid for their participation, but were fullydebriefed regarding the nature of the study. All participants gaveinformed consent. The research was approved by both the School ofPsychology Human Research Ethics committee and the Birminghamand Solihull NHS Local Research committee.
3. Results
3.1. Data analysis strategy
Kolmogorov-Smirnov tests demonstrated that the data werenormally distributed, which allowed parametric tests of significantdifference. To test for differences between the groups on measures ofegocentricity, an analysis of variance was conducted. The results ofthis ANOVA are presented in Table 1. To test for associations withingroups, a one-tailed Pearson's R was calculated for the EDE-Qsubscales and the egocentricity scales, the results of which can befound in Tables 2 and 3.
3.2. The group differences
A one-way ANOVA was conducted to examine the differences onscores of egocentricity between the three groups of participants. Dueto differences in the size of the groups and their variances, Games–Howell procedure was used to explore these differences (Table 1). Theresults suggest that individuals with anorexia nervosa symptomsscored significantly more highly than both other groups (adolescentsand young-adults without eating disorder symptoms) on the PUS andthe SCS. However, they scored lower than both other groups on thepsychological invulnerability subscale of the AIS. Out of all the
city in the comparison adult group
gical Invulnerability Doubts about being understood Doubts about being the same
.11 .29
.37⁎ .17
.35⁎ .18
.31 .04

13A. Fox et al. / Eating Behaviors 10 (2009) 10–15
egocentric measures, the adolescent group only scored more highlythan the adult group on the ‘doubts about being understood’ subscaleof the PUS.
3.3. Tests of within-group associations
Pearson's correlations were conducted to test the hypothesis thateating disorder symptom severity would be positively associated withincreased levels of egocentricity in the adult group with symptoms ofanorexia but not the adult groupwithout. Results of these correlationscan be seen in Tables 2 and 3. It appears that in both groups, the‘doubts about being understood’ subscale was moderately associatedwith eating concern, while in the non-anorexia adult group it was alsoassociated with shape concern. Furthermore, in the anorexia group,‘danger invulnerability’ and public self-consciousness were alsoassociated with eating concern, while in the adult non-clinicalgroup, public self-consciousness was associated with shape concernand weight concern.
4. Discussion
This paper set out to explore whether a consideration of normativeadolescent development may be relevant to an understanding ofanorexia nervosa. Following Elkind's (1967) original cognitive theoryof adolescent development, it was hypothesised that non-clinicaladolescent individuals would score more highly on measures ofpersonal uniqueness, adolescent invulnerability and self conscious-ness than non-clinical adult individuals. This hypothesis was onlyminimally supported, as adolescent individuals only demonstratedstatistically significantly higher scores on the ‘doubts about beingunderstood’ subscale of the PUS. Previous literature suggests thatthere may be some form of adolescent disruption in people whoexperience anorexia nervosa and it was therefore also hypothesisedthat young-adult individuals with a recent history of anorexicsymptoms would score more highly on measures of developmentalegocentrism than their non-clinical peers. This hypothesis wasgenerally supported. Lastly, it was hypothesised that eating disordersymptoms would be positively associated with egocentricity in peoplewith symptoms of anorexia but not people without such symptoms.Moderate associations were found between several eating disordersymptom subscales and egocentricity in both groups of participants,although the pattern of the associations differed, which offers somesupport to this hypothesis.
4.1. Adolescence
The current study found that adolescent individuals did not scoremore highly than the non-clinical adult individuals on the majority ofthe egocentrism measures used in the current study. Both the AIS andPUS are designed to measure separate dimensions of the personalfable construct, and traditional adolescent theory suggests thatpersonal fable cognitions decrease in line with cognitive development(Elkind, 1967). If this were indeed the case, then it would be expectedthat young adults would have lower levels of egocentricity thanteenagers due to their more developed cognitive capacity. As such, thecurrent data support more recent alternative suggestions thategocentrism during adolescence is a component of a social self-development process that actually continues past adolescence(Frankenberger, 2000; Lapsley, 1993). From this perspective, personalfable beliefs would only be expected to decrease once the individualhas successfully separated from their parents and developed a new,autonomous self— something that recent considerations suggest doesnot completely happen until the latter period of emerging-adulthood(Arnett, 2000). Furthermore, no difference was found betweenadolescents and young adults on measures of public self-conscious-ness (imaginary audience beliefs), which also suggests that other
dimensions of self-developmental egocentrism besides the personalfable extend into young-adulthood. This finding therefore contradictsthe original Piagetian cognitive developmental theory of Elkind, andoffers support for more recent socially oriented developmentalconsiderations of egocentrism (e.g. Lapsley, 1993; Vartanian, 2000).
Despite no difference between the adults and adolescents on themajority of scales, adolescents were found to score more highly on thedoubts about being understood subscale of the PUS (see Table 1). Suchbeliefs may serve to aid the young person in their individuation fromtheir parents and be an integral factor in the recognition anddevelopment of their own unique self. However, interpersonal experi-ence would likely demonstrate to the young person that although theyare separate from others, they can still be understood by them, and thestrength of such beliefs should diminish. Further research could usefullyexamine the dimensionally distinct components of the personal fableand imaginary audience over a section of age-ranges in an effort toestablish the developmental characteristics of these.
In sum, the data provide some support for more recent social-developmental theories of adolescent egocentrism where suchcognitions are linked to socially mediated processes of self-develop-ment and separation–individuation (see Vartanian, 2000); however itis unclear which dimensions of these are linked to which aspects ofadolescent and young-adult development. Future longitudinalresearch would be essential to clarify such relationships.
4.2. Anorexia nervosa
As predicted, young-adults who had experienced symptoms ofanorexia nervosa scored more highly than adolescents and non-clinical adults onmeasures of both the doubts about being understoodand doubts about being the same. This lends support to the idea thatsuch individuals may have experienced a disruption of the develop-mental processes outlined in the previous section. It is also perhapsnot surprising that individuals with anorexia nervosa symptomsindicated that they also felt more publicly self-conscious than theirpeers, given their self-reported beliefs regarding uniqueness, and theirfixations on body-image and appearance.
Despite these findings of increased personal uniqueness and self-consciousness in the anorexia participants, this group demonstratedsignificantly lower levels of psychological invulnerability (e.g. ‘Myfeelings don't get hurt’, ‘The opinions of others just don't botherme’)—which is another form of adolescent egocentricity (Lapsley & Duggan,2001). It is possible that higher levels of psychological invulnerabilityact as a protective factor in the development of mental healthproblems, as suggested by Goosens et al. (2002), although furtherresearch with other clinical populations would be needed to explorethis. This finding also supports previous research that demonstratesthat individuals with restrictive eating pathology display fears ofnegative evaluation (Gilbert & Meyer, 2005) and are therefore morevulnerable to the opinions of others. Clearly, further research is neededto establish the associations between ‘adolescent’ invulnerability andpsychopathology.
These results suggest that individuals with symptoms of anorexianervosa feel particularly psychologically vulnerable, rather thanphysically vulnerable, despite the fact that they are harmingthemselves through extreme dietary restriction. This psychologicalvulnerability may encourage them to avoid getting close to others andremain aloof and secretive, for fear of getting hurt, as reflected in adismissive attachment style (Ward et al., 2001). Social anxiety isprevalent within the eating disorders, with high internalisedglobal shame scores indicated in individuals with anorexia nervosa(Grabhorn, Stenner, Stangier & Kaufhold, 2006).
Individuals with symptoms of anorexia nervosa also seem tobelieve that they are particularly unique, and this may take the form ofa type of pride — possibly in regard to their achievements in the areaof dietary restraint (Johnson, Sansone & Chewning, 1992). Indeed, it

14 A. Fox et al. / Eating Behaviors 10 (2009) 10–15
has been suggested that the pride that comes from a belief in theuniqueness of the ability to restrict may contribute to resistance tochange found in people with anorexia nervosa (Vitousek, Watson &Wilson, 1998). As such, carefully unpicking this dysfunctional sense ofspecialness may be therapeutically useful, so long as more adaptivemechanisms for feeling special are provided.
The anorexia group in the current study also showed severalassociations between the egocentric measures (doubts about beingunderstood, self-consciousness, and danger invulnerability subscales)and the eating concern subscale of the EDE-Q. This pattern ofassociation appears quite different to that seen in the non-clinicalgroup, and when these measures of egocentricity are consideredtogether, it suggests that there is some form of negative social self-awareness associated with concerns about eating. It may be that theheightened awareness of the social self that is typical duringadolescence has become particularly focused into concerns abouteating. It is possible, however, that an intense eating concern mayserve to distinguish individuals from those around them, includingtheir parents, and thus may represent an attempt to move towardssuccessful separation–individuation.
4.3. Limitations and suggestions for further research
The current study has demonstrated that several aspects of self-developmental beliefs (or egocentrism) appear to be exaggerated inindividuals who have recently experienced symptoms of anorexianervosa. However, there are a number of limitations that need to beborne in mind when considering these results.
The number of participants was small, which limits the generali-sability of the findings, and this should perhaps be seen as a study forexploring the utility of considering normative adolescent develop-ment in anorexia nervosa, rather than as a comprehensive test of amodel. Indeed, had the number of participants been greater, theobserved trend of elevated danger invulnerability in the anorexiagroup may have reached statistical significance — something whichfuture research could explore. Furthermore, because of the smallnumber of participants, it was not possible to compare the twosubgroups of anorexia nervosa symptoms to each other (i.e. bingeversus restrictive). There may be a difference between the two groupsthat is not reflected in the current results, and future research couldaddress this possibility.
Another potential problem is a lack of BMI data for the groups, as itis unclear whether the individuals were below the normal height-for-weight range — information which is needed for eating disorderdiagnosis. However, BMI may not have been a particularly accuratereflection of eating disorder status in these cases, as severalindividuals were in treatment where their weight was managed byothers (e.g. through inpatient treatments, or outpatient monitoring)rather than by themselves. Furthermore, the use of the EDE-Q acted asa general guide to the presence or absence of eating disordersymptoms between the groups and facilitated an exploration of theassociations between eating disorder symptomatology and egocentr-ism — a method that has been used before in populations with eatingdisorder symptoms (e.g. Ross & Wade, 2003). Unfortunately, such ananalysis could not be completed with the adolescent group as EDE-Qdata was unavailable, and as such, it is unclear whether the pattern ofassociation between anorexic symptoms and egocentricity would bethe same as that in adults. This also meant that the eating disorderprofile of the adolescent population used in the current study isunclear, although as they were collected from a local school it wouldbe expected that normal population estimates of prevalence wouldapply (e.g. 0.7%; Fairburn & Harrison, 2003).
It is possible that beliefs regarding uniqueness and self-conscious-ness need not necessarily stem from self-developmental egocentrismas individuals with a mental health conditionmay think of themselvesas different from others due to the stigmatism of diagnosis.
Alternatively, it could be that the differences observed betweengroups reflect psychometric issues with the scales used, as they arecurrently in development, and have been used in a comparativelylimited range of settings so far. Therefore, a study that examined thephenomenology of the egocentrism involved could avoid these issuesand shed light on whether such cognitions are indeed related topsychosocial development, while also exploring their potentialrelevance to anorexia nervosa.
Finally, it is also worth acknowledging that not all aspects of self-development were measured in the current study. In particular,autonomy (e.g. Silverberg & Steinberg, 1987) and attachment (e.g.Bartholomew & Horowitz, 1991) have been explicitly linked with thedevelopment of self, and future research could perhaps examine these.This would also help to validate whether the beliefs measured in thecurrent study are indeed beliefs linked to self-developmental processes.
4.4. Conclusions
The empirical data offer support to the notion explored in thispaper of considering developmental phenomena in an understandingof anorexia nervosa. In particular, it seems that beliefs regardingpersonal uniqueness are highly salient to people with symptoms ofanorexia nervosa. In the context of emerging-adult development, thiswould suggest that although such individuals are aware of their ownindividual sense of self, they are also struggling to appreciate theaspects of themselves that they have in common with others.Interactions with peers are the usual mechanism thought to resultin a reduction of these types of beliefs, but in this clinical group apicture of isolation from others is common, which may havecontributed to the presence of these cognitions.
Clinically, a few suggestions can be offered with regard toworkingwith people with anorexia nervosa. Firstly, the apparent role ofdevelopmental processes supports the notion of involving family inany therapeutic efforts in an attempt to facilitate normal adolescentprocesses, such as dealing with autonomy, control and independenceissues. Secondly, the research also supports the suggestion that socialanxiety may be common in anorexia nervosa (e.g. Grabhorn et al.,2006), which therefore suggests that individuals may benefit fromtreatments that consider such interpersonal difficulties, including,for example, more behavioural exercises that gradually (and care-fully) expose them to their anxieties. Finally, encouraging engage-ment with peers and the development of interpersonal relationshipsmay help to foster an understanding of others, how they function,and what makes them feel special, which could encourage indivi-duals to explore other sources of uniqueness other than extremedietary restriction.
Acknowledgements
The research was supported by a joint School of Psychology andBirmingham and Solihull Mental Health NHS Trust studentship. Wewish to thank all the participants who gave their time to take part inthe research and special mention should go to b-eat (formerly knownas the EatingDisorders Association),who assistedwith data-collection.
References
Aalsma, M. C., Lapsley, D. K., & Flannery, D. J. (2006). Personal fables, narcissism, andadolescent adjustment. Psychology in the Schools, 43, 481−491.
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teensthrough the twenties. American Psychologist, 55, 469−480.
Barth, F. D. (2003). Separate but not alone: Separation–individuation issues in collegestudents with eating disorders. Clincial Social Work Journal, 31, 139−153.
Bartholomew, K., &Horowitz, L.M. (1991). Attachment styles among young adults: A testof a four-category model. Journal of Personality and Social Psychology, 61, 226−244.
Bjorck, C., Clinton, D., Sohlberg, S., Hallstrom, T., & Norring, C. (2003). Interpersonal profilesin eating disorders: Ratings of SASB self-image. Psychology and Psychotherapy: Theory,Research and Practice, 76, 337−349.

15A. Fox et al. / Eating Behaviors 10 (2009) 10–15
Britt, T. W. (1992). The Self-Consciousness Scale — On the stability of the 3-factorstructure. Personality and Social Psychology Bulletin, 18, 748−755.
Bruch, H. (1978). The golden cage: The enigma of anorexia nervosa. London: Open Books.Duggan, P., Lapsley, D.K., & Norman, K. (2000). Adolescent invulnerability and personal
uniqueness: Scale development and initial construct validation. Paperpresentedat theEighth Biennial Meeting of the Society for Research on Adolescence. Chicago, Illinois.
Elkind, D. (1967). Egocentrism in adolescence. Child Development, 38, 1025−1034.Fairburn, C. G., & Beglin, S. J. (1994). Assessment of eating disorders: Interview or self-
report questionnaire? International Journal of Eating Disorders, 16, 363−370.Fairburn, C. G., & Harrison, P. J. (2003). Eating disorders. The Lancet, 361, 407−416.Fairburn, C. G., Cooper, Z., & Shafran, R. (2003). Cognitive behaviour therapy for eating
disorders: A “transdiagnostic” theory and treatment. Behaviour Research andTherapy, 41, 509−528.
Fenigstein, A., Scheier, M. F., & Buss, A. H. (1975). Public and private self-consciousness—Assessment and theory. Journal of Consulting and Clinical Psychology, 43, 522−527.
Frankenberger, K. D. (2000). Adolescent egocentrism: A comparison among adolescentsand adults. Journal of Adolescence, 23, 343−354.
Fredrickson, B. L., & Roberts, T. A. (1997). Objectification theory — Toward under-standing women's lived experiences and mental health risks. Psychology of WomenQuarterly, 21, 173−206.
Garner, D. M., & Bemis, K. M. (1982). A cognitive–behavioural approach to anorexianervosa. Cognitive Therapy and Research, 6, 123−150.
Gilbert, N., &Meyer, C. (2005). Fear of negative evaluation and the development of eatingpsychopathology: A longitudinal study among nonclinical women. InternationalJournal of Eating Disorders, 37, 307−312.
Goosens, L., Beyers,W., Emmen,M., & van Aken, M. A. G. (2002). The imaginary audienceand personal fable: Factor analyses and concurrent validity of the ‘new look’measures. Journal of Research on Adolescence, 12, 193−215.
Grabhorn, M., Stenner, H., Stangier, U., & Kaufhold, A. (2006). Social anxiety in anorexiaand bulimia nervosa: The mediating role of shame. Clinical Psychology &Psychotherapy, 13, 12−19.
Hafner, H. (2003). Gender differences in schizophrenia.Psychoneuroendocrinology,28,17−54.Halvorsen, I., & Heyerdahl, S. (2006). Girls with anorexia nervosa as young adults:
Personality, self-esteem, and life satisfaction. International Journal of EatingDisorders, 39, 285−293.
Harrop, C.,&Trower, P. (2003).Whydoes schizophreniadevelopat late adolescence?A cognitive–developmental approach to psychosis. Chichester, England: JohnWiley and Sons, Ltd.
Harrop, C., & Trower, P. (2001). Why does schizophrenia develop at late adolescence?Clinical Psychology Review, 21, 241−265.
Harter, S. (1999). The construction of the self: A developmental perspective. New York: TheGuilford Press.
Hendry, L. B., & Kloep, M. (2003). Lifespan development: Resources, challenges and risks.London: Thomson learning.
Johnson, C. L., Sansone, R. A., & Chewning, M. (1992). Good reasons why young womenwould develop anorexia nervosa: The adaptive context. Pediatric Annals, 21,731−737.
Lapsley, D. K. (1993). Toward an integrated theory of adolescent ego developement: The“new look” at adolescent egocentrism. American Journal of Orthopsychiatry, 63,562−571.
Lapsley, D.K. & Duggan, P. (2001). The adolescent invulnerability scale: Factor structureand construct validity. Paper presented at the biennial meeting of the Society forResearch on Child Development, Minneapolis.
Mond, J. M., Hay, P. J., Rodgers, B., Owen, C., & Beumont, R. J. V. (2004). Validity of theEating Disorder Examination Questionnaire (EDE-Q) in screening for eatingdisorders in community samples. Behaviour Research and Therapy, 42, 551−567.
Penn, M. L., & Witkin, D. J. (1994). Pathognomic versus developmentally appropriateself-focus during adolescence — Theoretical concerns and clinical implications.Psychotherapy, 31, 368−374.
Rhodes, B., & Kroger, J. (1992). Parental bonding and separation–individuationdifficulties among late adolescent eating disordered women. Child Psychiatry andHuman Development, 22, 249−263.
Rosen, J. C., Reiter, J., & Orosan, P. (1995). Assessment of body-image in eating disorderswith the body dysmorphic disorder examination. Behaviour Research and Therapy,33, 77−84.
Rosenberg, M. (1979). Conceiving the self. New York: Basic Books.Ross, M., & Wade, T. D. (2003). Shape and weight concern and self-esteem as mediators
of externalized self-perception, dietary restraint and uncontrolled eating. EuropeanEating Disorders Review, 12, 129−136.
Ruiperez, M. A., & Belloch, A. (2003). Dimensions of the self-consciousness scale andtheir relationship with psychopathological indicators. Personality and IndividualDifferences, 35, 829−841.
Silverberg, S. B., & Steinberg, L. (1987). Adolescent autonomy, parent adolescent conflict,and parental well-being. Journal of Youth and Adolescence, 16, 293−312.
Slade, P. (1982). Towards a functional analysis of anorexia nervosa and bulimia nervosa.British Journal of Clinical Psychology, 21, 167−179.
Thompson, T., Dinnel, D. L., & Dill, N. J. (2003). Development and validation of a BodyImage Guilt and Shame Scale. Personality and Individual Differences, 34, 59−75.
Vartanian, L. R. (2000). Revisiting the imaginary audience and personal fable constructsof adolescent egocentrism: A conceptual review. Adolescence, 35, 639−661.
Vitousek, K., Watson, S., & Wilson, G. T. (1998). Enhancing motivation for change intreatment-resistant eating disorders. Clinical Psychology Review, 18, 391−420.
Ward, A., Ramsay, R., Turnbull, S., Steele, M., Steele, H., & Treasure, J. (2001). Attachmentin anorexia nervosa: A transgenerational perspective. British Journal of MedicalPsychology, 74, 497−505.
Weaver, K., Wuest, J., & Ciliska, D. (2005). Understanding women's journey of recoveringfrom anorexia nervosa. Qualitative Health Research, 15, 188−206.
![[PPT]Anorexia Nervosa - Mr Sitar's Website - homemrsitarswebsite.wikispaces.com/file/view/Anorexia Nervosa... · Web viewWhat is the definition to this illness? Anorexia nervosa is](https://img.pdfslide.net/doc/110x75/5af162f57f8b9ad0618f592d/pptanorexia-nervosa-mr-sitars-website-nervosaweb-viewwhat-is-the-definition.jpg)