Embed Size (px)
Citation preview


A daily dose of 400 mg efavirenz (EFV) is non-inferior to the standard 600 mg dose: week 48 data from the ENCORE1 study, a
randomised, double-blind, placebo controlled, non-inferiority trial
Rebekah Puls for the ENCORE1 Study Group
Reduced dose antiretroviral drugs (ARV)
GFATM/WHO/PEPFAR plans to expand treatment to 15 million people by 2015 will come at significant cost
Although reduced, the cost of ARV remains substantial
Dose reduction may be a means to reduce drug costs
Efavirenz (EFV) is a globally important ARV
WHO guidelines recommend EFV for first line
Phase II trial and observational cohort data suggest comparable performance at lower daily doses

Encore1 study designA randomized, double-blind, placebo-controlled, non-inferiority clinical trial to compare the safety and efficacy of reduced dose EFV with standard dose EFV plus 2N(t)RTI in ART-naïve HIV-infected individuals over 96 weeks
Patient populationART-naïve HIV-infected adults with no prior AIDS, plasma HIV-1 RNA (pVL) >1,000 copies/mL, 50 <CD4+ T cells/µL <500, creatinine clearance ≥50 mL/min, no pregnancy or nursing mothers
RandomisationI. TDF/FTC + 400 mg EFV qd
(2 x 200 mg EFV + 1 x 200 mg matched placebo)
II. TDF/FTC + 600 mg EFV qd (3 x 200 mg EFV)
1:1 (400mg:600mg), stratified by clinical site and screening pVL

MethodsPrimary endpointProportion of participants with pVL <200 copies/mL at 48 weeks
in the intention to treat (ITT, M=F) population, using a non-inferiority margin of 10%
pVL determined retrospectively at a single, central laboratory<50, <400 copies/mL
Sample size630 patients to demonstrate non-inferiority of 400 mg EFV
assuming 85% participants taking 600 mg have <200 copies/mL, at least 90% power for both ITT and PP analyses
Safety dataAdverse event (AE) summaries, cessation of study drugsChanges from baseline in laboratory results

Participant disposition
Withdrew consentN=9
RandomizedN=636
EFV 400mg, N=324
Withdrew prior to commencing randomized therapy N=3
ITT and NC=F, N=321
PP, N=293
EFV 600mg, N=312
Withdrew prior to commencing randomized therapy N=3
ITT and NC=F, N=309
PP, N=271
Total screenedN=768
Total ineligible N=123
SingaporeMalaysia
Australia
Israel
United Kingdom
Germany
Nigeria
South Africa
Mexico
Chile
Argentina
Thailand
Hong Kong
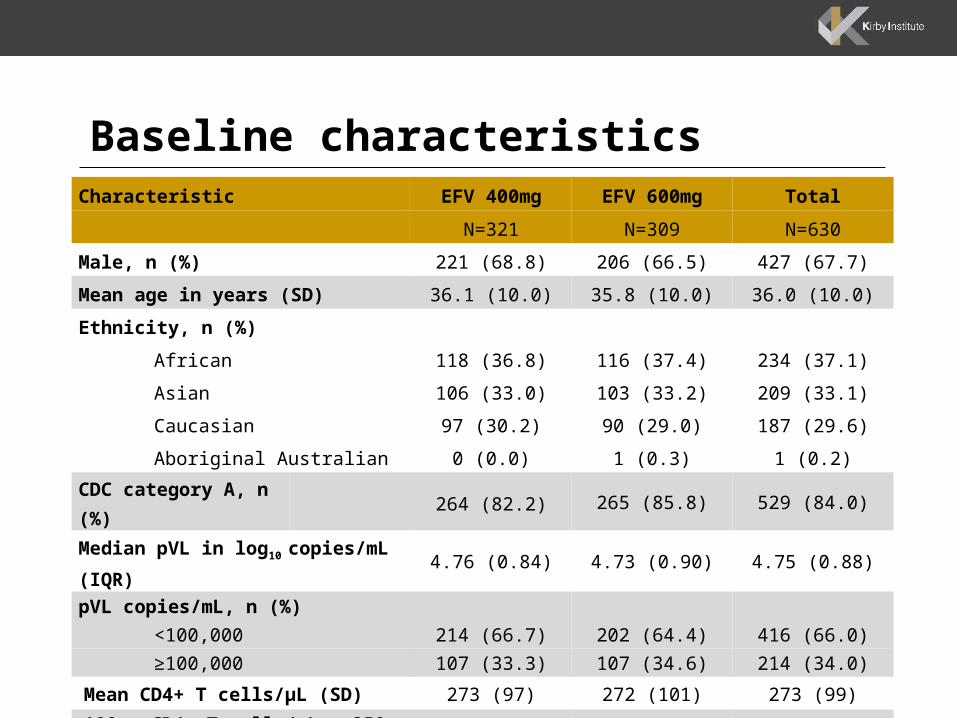
Baseline characteristics Characteristic EFV 400mg EFV 600mg Total
N=321 N=309 N=630
Male, n (%) 221 (68.8) 206 (66.5) 427 (67.7)
Mean age in years (SD) 36.1 (10.0) 35.8 (10.0) 36.0 (10.0)
Ethnicity, n (%)
African 118 (36.8) 116 (37.4) 234 (37.1)
Asian 106 (33.0) 103 (33.2) 209 (33.1)
Caucasian 97 (30.2) 90 (29.0) 187 (29.6)
Aboriginal Australian 0 (0.0) 1 (0.3) 1 (0.2)
CDC category A, n (%) 264 (82.2) 265 (85.8) 529 (84.0)
Median pVL in log10 copies/mL (IQR) 4.76 (0.84) 4.73 (0.90) 4.75 (0.88)
pVL copies/mL, n (%)
<100,000 214 (66.7) 202 (64.4) 416 (66.0)
≥100,000 107 (33.3) 107 (34.6) 214 (34.0)
Mean CD4+ T cells/µL (SD) 273 (97) 272 (101) 273 (99)
100 < CD4+ T cells/µL ≤ 350, n (%) 244 (76) 224 (72) 468 (74)

Primary endpoint: non inferiority at week 48
EFV400
%
EFV600 % Difference (95%CI) p
ITT 94.1 92.2 1.8 (-2.1, 5.8) 0.36
NC=F 90.0 85.8 4.3 (-0.8, 9.4) 0.10
PP 98.3 97.4 0.9 (-1.5, 3.3) 0.47
-15 -10 -5 0 5 10 15
Difference in percentage of participants with pVL <200 copies/mL
favours EFV400
favours EFV600

Primary endpoint: non inferiority at week 48
EFV400
%
EFV600 % Difference (95%CI) p
ITT 94.1 92.2 1.8 (-2.1, 5.8) 0.36
<105 strata 94.9 92.9 2.0 (-2.7, 6.8) 0.40
≥105 92.7 91.1 1.7 (-5.3, 8.6) 0.64
NC=F 90.0 85.8 4.3 (-0.8, 9.4) 0.10
<105 strata 90.4 84.8 5.6 (-0.9, 12.1) 0.09
≥105 89.5 87.5 2.0 (-6.1, 10.2) 0.63
PP 98.3 97.4 0.9 (-1.5, 3.3) 0.47
<105 strata 98.9 97.6 1.2 (-1.5, 4.0) 0.70
≥105 97.4 97.0 0.3 (-4.1, 4.8) 1.00
-15 -10 -5 0 5 10 15favours EFV600
favours EFV400
Difference in percentage of participants with pVL <200 copies/mL

Distribution of participants : NC=F <200 copies/mL
EFV 400 mg EFV 600 mg Total
N=321 N=309 N=630
n (%) n (%) n (%)
Failures 32 (10.0) 44 (14.2) 79 (12.5)
pVL >200 copies/mL 5 (1.6) 7 (2.3) 12 (1.9)
Death 2 (0.6) 3 (1.0) 5 (0.8)
Withdrew consent 3 (0.9) 3 (1.0) 6 (1.0)
Lost to follow up 4 (1.2) 3 (1.0) 7 (1.1)
Missing data @ week 48 1 (0.3) 5 (1.6) 6 (1.0)
Stopped EFV due to VF 1 (0.3) 2 (0.6) 3 (0.5)
Stopped EFV for other reason 16 (5.0) 21 (6.8) 40 (6.4)
pVL <200 copies/mL 289 (90.0) 265 (85.8) 554 (87.9)

Mean change from baseline to week 48 pVL
mean difference (95%CI) -0.06 log10 copies/mL (-0.19, 0.07), p=0.350
0 4 8 12 16 20 24 28 32 36 40 44 48-5
-4
-3
-2
-1
0
1
EFV 400 mgEFV 600 mg
pV
L l
og
10
co
pie
s/m
L

Mean change from baseline to week 48 CD4+ T cells
Time (weeks)
mean difference (SD) 25 cells (6, 44) p=0.009*
0 4 8 12 16 20 24 28 32 36 40 44 48-50
0
50
100
150
200
250
300
EFV 400 mg EFV 600 mg
CD
4+
T c
ell
s/µ
L

Adverse events - overall
Adverse eventsEFV400
n (%)EFV600n (%)
Total n (%)
Number of AEs 1,173 (49.8) 1,182 (50.2) 2,355 (100)
Grade 1/2 1,119 (47.5) 1,118 (47.4) 2,237 (95.0)
Grade 3/4 54 (2.3) 65 (2.7) 117 (5.0)
Serious adverse events
EFV400 N=321n (%)
EFV600 N=309n (%)
Difference (95%CI)
p
Total numbers of SAEs 31 (46.2) 36 (53.7)
Number with SAE 23 (7.17) 22 (7.12) 0.05% (-3.98, 4.07) 0.980
Number with SAE related to study drug
3 (0.93) 4 (1.29) 0.36% (-1.98, 1.27) 0.670
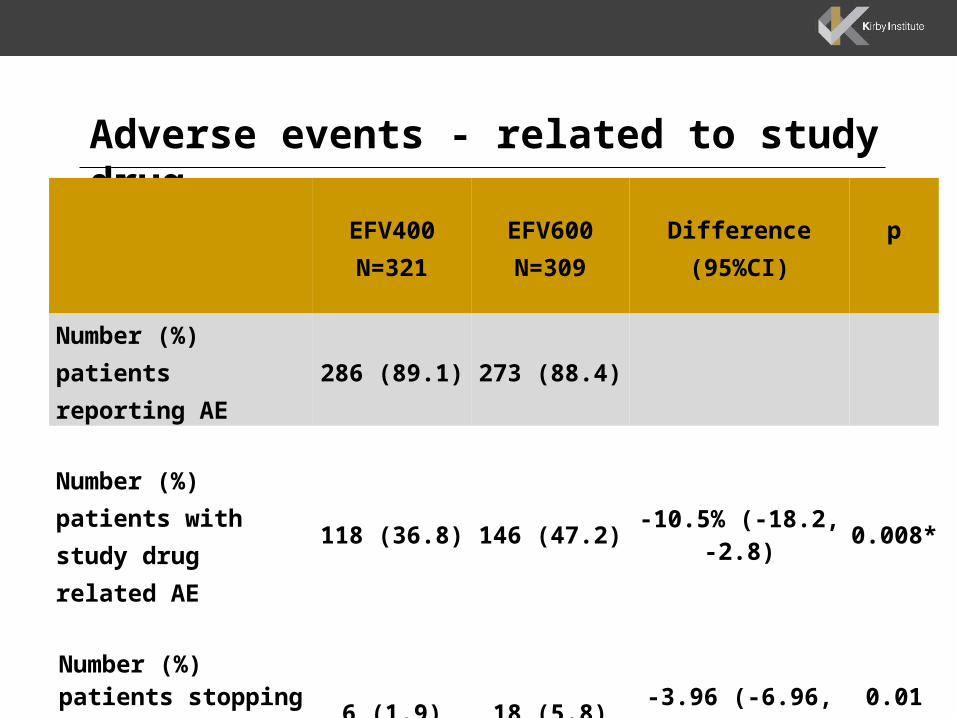
Adverse events - related to study drug
EFV400N=321
EFV600N=309
Difference (95%CI)
p
Number (%) patients reporting AE
286 (89.1) 273 (88.4)
Number (%) patients with study drug related AE
118 (36.8) 146 (47.2) -10.5% (-18.2, -2.8) 0.008*
Number (%) patients stopping drug due to related AE
6 (1.9) 18 (5.8) -3.96 (-6.96, -0.95) 0.010*

Efavirenz adverse events*
CNS Psychiatric Rash Gastrointestinal Respiratory Hepatotoxicity0
10
20
30
40
50
60
Pro
po
rtio
n o
f p
art
icip
an
ts (
%)
231
272
13 12
68
105
62
21 221 0
EFV400
EFV600
78
*categorised according to the EFV Product Information

Conclusions
400 mg EFV was non-inferior to 600 mg EFV when combined with Truvada in a treatment-naive, HIV-infected adult population over 48 weeks
Evidence of reduced EFV-related side effects with lower dose
400 mg EFV should be considered for initial ARV treatment.
AcknowledgmentsWe extend our grateful thanks to all the volunteers who have been participating in this study. The study was funded from the following sources: an unrestricted grant from the Bill & Melinda Gates Foundation (Grant ID 51040); the Australian Government Department of Health and Ageing; the University of New South Wales. We thank Gilead Sciences Inc for their very kind donation of Truvada™ to undertake this project and Matrix Laboratories (Mylan Inc.) for their supply of efavirenz and matched placebo. The Kirby Institute is affiliated with the Faculty of Medicine, University of New South Wales, Australia.
Protocol Steering Committee – Waldo Belloso, Marta Boffito, David Cooper, Chris Duncombe, Sean Emery, Sharne Foulkes, Andrew Hill, Heiko Jessen, Suresh Kumar, Man Po Lee, Brenda Crabtree-Ramirez, Marcelo Losso, Praphan Phanupak, Rebekah Puls, Jim Rooney, Eduardo Shahar, Alan Winston, Marcelo Wolff, Barnaby Young
DSMB – Matthew Dolan, David Dunn, Roy Gulick
Sydney coordinating team – Sean Emery, Rebekah Puls, Dianne Carey, Carlo Dazo, Anna Donaldson, Mark Boyd, Kymme Courtney-Vega, Janaki Amin, Sarah Pett, Jessica Taylor, Enmoore Lin, Tanya Johannesen, Tony Kelleher, Philip Cunningham, Kate Merlin, Julie Yeung, Ansari Shaik, Bertha Fsadni, Alex Carrera, Melanie Lograsso Buenos Aires coordinating team – Marcelo Losso, Waldo Belloso, Cecilia Abela, Marina Delfino, Lucas Roby, Alejandra Moricz, Silvia Pizzuto, Silvana Marangón Bangkok coordinating team – Praphan Phanupak, Amanda Clarke, Kanitta Pussadee, Louise Tomkins, Parinya Sutheerasak, Peeraporn Kaew-on, Sasiwimol Ubolyam

AcknowledgmentsAustralia: Alfred Hospital – Julian Elliot, Michelle Boglis, Janine Roney. Melbourne Sexual Health Centre – Tim Read, Helen Kent, Julie Silvers. Northside Clinic – Richard Moore, Thai Lim, Jeff Wilcox. AIDS Medical Unit – Mark Kelly, Abby Gibson, Lucy Bird. Royal Perth Hospital – David Nolan, Julie Robinson, Laura Barba. Albion St Centre: Don Smith, Jega Sarangapany, Denise Smith. Burwood Road General Practice: Nicholas Doong, Nam Phan, Jeff Hudson. Taylor Square Private Clinic: Emanuel Vlahakis, Amrita Patel, Isobel Prone. St Vincent’s Hospital: David Cooper, Sarah Pett, Karen MacRae. Argentina: CAICI - Sergio Lupo, Liliana Trape, Luciana Peroni. Hospital Italiano - Waldo Belloso, Marisa Sanchez, Mariana de Paz Sierra. Hospital Ramos Mejia - Marcelo Losso, Mariana Kundro, Patricia Burgoa. Hospital Posadas - Hector Laplume Lucia Daciuk. Hospital Rawson - Norma Luna, Daniel David, Laura Nieto. FUNCEI - Valeria Confalonieri, Emiliano Bissio, Pablo Luchetti. CEADI - Oscar Garcia Messina, Olivia Gear, Adrian Rodriguez. CEIN - Liliana Calanni, Susana Calanni, Daniel Clafunao. Chile: – Hospital San Borja-Arriaran - Marcelo Wolff, Claudia Cortes, Gladys Allendes. Hospital de la Universidad Catolica Pontificia - Carlos Perez, Jimena Flores. Germany: Medical Group Practice Berlin – Heiko Jessen, Arne Jessen, Luca Stein, Carmen Zedlack, Maria Koch. Bonn University – Jurgen Rockstroh, Brigitta Späth, Christoph Boesecke. Israel: Rambam Medical Centre – Eduardo Shahar, Eynat Kedem, Garmal Hassoun. Hong Kong: Queen Elizabeth Hospital - Man-Po Lee, Patrick CK Li, Pansy PC Yu. Malaysia: UMMC - Raja Iskandar Shah Raja Azwa, Sharifah Faridah Syed Omar, Sasheela Sri La Sri Ponnampalavanar. Hospital Sungai Buloh - Suresh Kumar, Yasmin Gani, Henry Chang. Mexico: Hospital General de Guadalajara - Jaime Andrade Villanueva, Angeles Gonzalez, Lucero Gonzalez. INCMNSZ- Brenda Crabtree Ramirez, Juan Sierra Madero, Maru Zghaib. Singapore: Tan Tock Seng Hospital - Barnaby Young, Evelyn Chia, Andy Loh. South Africa: Desmond Tutu HIV Centre - Catherine Orrell, Richard Kaplan, Robin Wood. Josha Research - Sharne Foulkes, Neo Tsikoane, Nadia Grace. Chris Hani Baragwanath Hospital - Lerato Mohapi, Maureen Mohata, Ashaan Naidoo. Nigeria: BUTH - Chidi Nwizu, George Chima, Vera Labesa. PSSH - Chidi Nwizu, Henriatta Selle Tiri, Jonathan Bulu. Thailand: HIV-NAT - Praphan Phanuphak, Amanda Clarke, Anchalee Avihingsanon. Khon Kaen University - Ploenchan Chetchotisakd, Siriluck Anunnatsiri, Parichat Seawsirikul. RIHES - Khuanchai Supparatpinyo, Patcharaphan Sugandhavesa, Patchanee Samutarlai. United Kingdom: St. Mary’s Hospital – Alan Winston, Borja Mora-Peris, Siobhan McKenna. Chelsea and Westminster Hospital –Brian Gazzard, Marta Boffito, Chris Higgs.