Embed Size (px)
Citation preview

A description of an HPLC assay ofcoproporphyrinogen III oxidase activityin mononuclear cellsU. GROSS
1*, R. GERLACH1, A. K�HNEL
2, V. SEIFERT1 and M. O. DOSS
2
1Department of Neurosurgery, Johann Wolfgang Goethe University,Frankfurt/Main; 2Division of Clinical Biochemistry, Philipps UniversityHospital, Marburg, Germany
*Correspondence: Department of Neurosurgery, Johann WolfgangGoethe-University, Schleusenweg 2-16, 60528 Frankfurt/Main, Germany.E-mail:[email protected]
MS received 24.01.03 Accepted 19.05.03
Summary: Coproporphyrinogen III oxidase is de¢cient in hereditarycoproporphyria. An activity assay for this enzyme in mononuclear cells, besidesthe preparation of the substrate, are presented. The separation conditionsfor the product of the test protoporphyrin IX by gradient, reversed-phasehigh-performance liquid chromatography are given. The normal valuefrom mononuclear cells of healthy volunteers was 138� 21 pkat/g totalsoluble protein (mean� SD). The enzyme activity of a family withhereditary coproporphyria was measured. The gene carriers exhibit aspeci¢c coproporphyrinogen III oxidase activity of 61^90 pkat/g total solubleprotein.
Hereditary coproporphyria (McKusick 121300), the third most frequent acutehepatic porphyria among European populations, is a metabolic disorder that isphenotypically characterized by abnormal amounts of coproporphyrin III in faecesand urine. The clinically evaluable symptoms are various neurovisceral, psychiatric,cardiovascular and sometimes also cutaneous manifestations (Martasek 1998)accompanied by increased concentrations of urinary d-aminolevulinic acid,porphobilinogen and porphyrins (Kˇhnel et al 2000).
At the cellular level, a signi¢cant lack of the mitochondrial enzymecoproporphyrinogen III oxidase, catalysing the oxidative decarboxylation step fromcoproporphyrinogen III to protoporphyrinogen IX, has been reported for leukocytesfrom patients with hereditary coproporphyria (Guo et al 1988). In the majority ofcases the enzyme activity is reduced to 50% in heterozygotes. This indicates themutation of one allele of the coproporphyrinogen oxidase gene. In a rare compound
J. Inherit.Metab.Dis. 26 (2003) 565^570# SSIEMandKluwerAcademic Publishers. Printed in theNetherlands
565

heterozygous case of hereditary coproporphyria, the enyme activity amounts to 2%(Doss et al 1999).
Besides the eukaryotic coproporphyrinogen III oxidase, an oxygen-independentenzyme exists in bacteria. It was recently demonstrated that puri¢ed HemNpossesses coproporphyrinogen III oxidase activity (Layer et al. 2002)
In the present study we describe the assay for coproporphyrinogen III oxidase formononuclear cells based on the application of high-performance liquidchromatography for the quantitative measurement of protoporphyrin IXconcentrations.
METHODS
Separation and storage of mononuclear cells from whole blood: Mononuclear cellshave a lower density compared to erythrocytes and granulocytes. Aftercentrifugation of blood cells loaded on a separation £uid of appropriate density,the mononuclear cells remain at the top where they can be collected (BFyum 1984).
Heparinized blood is diluted 1:1 with phosphate-bu¡ered saline. This mixture islayered carefully on a Ficoll solution with a density of 1.077 g/ml in a centrifugetube by keeping the pipette against the tube wall 2^3 cm above the £uid meniscus.The blood should £ow out of the pipette continuously in order to prevent mixingof the phases. After centrifugation at room temperature for 15min at 1250 gmax,the blood cells separate into two fractions: a white layer containing mononuclearcells and a pelleted fraction containing erythrocytes and granulocytes. Themononuclear cells are collected and resuspended in phosphate-bu¡ered salineand centrifuged for 40min at 1250 gmax. The supernatant is discarded. The sedimentis resuspended in phosphate-bu¡ered saline and centrifuged for 10min at 300 gmax.The supernatant is discarded again and the sediment containing the mononuclearcells is resuspended in cold medium consisting of 50% (v/v) tissue culture mediumRPMI 1640, 40% (v/v) fetal calf serum and 10% (v/v) dimethyl sulphoxide. It is¢nally frozen and stored in liquid nitrogen (Gray and Golub 1984).
Principle of the activity assay: Coproporphyrinogen III oxidase converts thesubstrate coproporphyrinogen III to protoporphyrinogen IX. The product isoxidized to protoporphyrin IX and quantitatively estimated using £uorescencehigh-performance liquid chromatography by comparison with known standards.Mesoporphyrin is used as internal standard.
Preparation of the reducing agent sodium amalgam: Weigh out 16 g mercury into aside-armed £ask and £ush it with nitrogen for 5min. Cut a block of 1 cm3 sodium andblot dry. Remove outer darkened areas with a scalpel. Weigh out 0.5 g sodium andcut into small pieces. Add sodium all at once. Agitate the £ask and continue to £ushwith nitrogen. Shake amalgam loose from the sides of the £ask and store in ascrew-top jar under hexane.
Preparation of coproporphyrinogen III substrate: Coproporphyrin III dihydro-chloride is dissolved in a few drops of concentrated ammonia. The solution is diluted
566 Gro5 et al
J. Inherit. Metab. Dis. 26 (2003)

with 0.1mol/L KOH to a concentration of 50 mmol/L coproporphyrin III. Thiscoproporphyrin III solution is reduced with sodium amalgam under nitrogen inthe dark by shaking vigorously until there is no UV £uorescence. Then a 9-fold vol-ume of a solution of 250mmol/LTris-HCl, pH 7, 0.1mmol/LEDTAand 90mmol/Lascorbic acid is added. After mixing, the coproporphyrinogen III solution is rapidlytransferred to another tube on ice, £ushed with nitrogen and stored at � 20�C.
Assay procedure: The suspension of mononuclear cells is frozen and thawed threetimes before assay. The standard assay mixture containing 100 ml of the cell solutionand 100 ml of 250mmol/L Tris-HCl, pH 7, 0.1mmol/L EDTA is preincubated at37�C for 5min. The reaction is started by adding 50 ml freshly thawed, bu¡eredcoproporphyrinogen III solution at a ¢nal concentration of 1 mmol/L. Then theincubation is continued for 90min at 37�C in the dark. The reaction is terminatedby cooling on ice and immediately mixed with 250 ml of 20% (w/v) trichloroaceticacid, 50% (v/v) dimethyl sulphoxide containing 150 pmol mesoporphyrin as aninternal standard. After centrifugation for 10min at 4�C (2100 gmax), thesupernatant is kept on ice in the dark until analysis by high-performance liquidchromatography. A blank is carried out in parallel with a suspension of mononuclearcells deactivated by boiling at 100�C for 10min.
Total soluble protein of mononuclear cells was determined by the Bio-Rad assaywith bovine serum albumin as a standard according to the method of Bradford(1976).
HPLC analysis: The product of the enzyme reaction is protoporphyrinogen IX,which is oxidized to protoporphyrin IX. Protoporphyrin IX is separated fromcoproporphyrin III and is quantitatively analysed by reversed-phase high-performance liquid chromatography. Supernatant (220 ml) is injected by a 200 mlRheodyne injection loop. The separation is performed by a LiChrospher 100RP-18 with a gradient of 88% (v/v) methanol in 1mol/L ammonium acetate bu¡er,pH 5.16, and methanol as eluent. The chromatographic and detection conditionsfor the analyses are presented in Table 1.
Table 1 The chromatographic and detection conditions for analysis of protoporphyrin IX
Injection volume 200 ml sample volume by manual injectionSeparation column LiChrospher 100 RP-18 (5 mm), 4� 75mm (Merck)Pre-column LiChrospher 100 RP-18 (5 mm), 4� 4mm (Merck)Solvent A: 88% methanol (v/v) in 1mol/L ammonium acetate, pH 5.16
B: methanol LiChrosolve (Merck)Gradient Stepwise gradientTime (min) 0 12 13 14 18 20 22Solvent composition A (%) 100 50 25 0 0 100 100Flow rate 1.0ml/minPressure VariableTemperature 29�CStop time 22minFluorimetric detection Excitation 405 nm; emission 620 nmUV detection 406 nm
Measurement of coproporphyrinogen oxidase activity 567
J. Inherit. Metab. Dis. 26 (2003)

RESULTS
Linearity of protoporphyrin IX formation: The volume- and time-dependentlinearity of the activity assay has been tested. Volume-dependent linearity wasobserved for 0.25mg to 1.25mg total soluble protein from mononuclear cells.
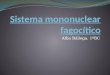
The course of the incubation time is shown in Figure 1. Protoporphyrin IX for-mation grew linearly with time from 15 to 90min when 1mg of total soluble proteinfrom mononuclear cells was the enzyme source.
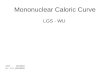
Family study: The speci¢c activity of coproporphyrinogen III oxidase in healthyvolunteers was 138� 21 pkat/g total soluble protein (mean� SD; intra-assayvariation, CV¼ 11%). In a family with hereditary coproporphyria a patient, themother and two sisters of the index patient were determined as gene carriers by theirurinary porphyrin precursors and porphyrins as well as their faecal porphyrins.Furthermore, the inversion of their faecal coproporphyrin isomers I and III wasused as a diagnostic tool. The father was normal in his excretion parameters.Figure 2 shows the coproporphyrinogen III oxidase activities in mononuclear cellsfrom the members of this family compared to the normal range. The father’s speci¢ccoproporphyrinogen III oxidase activity was 129% of the normal range. Themother’s and the patient’s speci¢c activities were 49% and 65%, respectively. Sister1 and sister 2 expressed 44% and 58%, respectively, of the speci¢c copropor-phyrinogen III oxidase activity from healthy controls.
DISCUSSION
An acute crisis of hereditary coproporphyria is triggered by various exogenousfactors such as alcohol, drugs and hormones (Takeuchi et al 2001). It may belife-threatening. Thus, the recognition of gene carriers is important for avoidanceof inducing factors. There are several possibilities for diagnosing an acute hepaticporphyria even in its subclinical state. First, the analysis of the excretion from
Figure 1 Time-dependent linearity of protoporphyrin IX formation by the activity assay(mean; n¼ 3)
568 Gro5 et al
J. Inherit. Metab. Dis. 26 (2003)

urinary porphyrin precursors and urinary as well as faecal porphyrins is important.In most cases these measurements are suf¢cient to detect gene carriers. These personsusually have enhanced excretion even in a subclinical state of the disease. In addition,analyses of haem precursors give information on the clinical expression of the disease(Kˇhnel et al 2000). The inversion of faecal coproporphyrin isomers I and III in genecarriers with hereditary coproporphyria is another diagnostic tool (Kˇhnel et al2000).
The lowered coproporphyrinogen III oxidase activity re£ects the result of themutation on the enzyme protein. This enzyme activity is diminished for the wholeof life in gene carriers of hereditary coproporphyria. Moreover, heterozygousand homozygous or compound heterozygous gene defects di¡er in the level ofthe lowered activity (Doss et al 1999). Thus, an assay of the coproporphyrinogenoxidase activity gives additional information; it is also a second diagnostic toolin patients with hereditary coproporphyria in addition to the excretion parameters.In cases where no products of excretion are available, for example in patients withanuria or obstipation, analyis of the coproporphyrinogen III oxidase activitymay also help to diagnose hereditary coproporphyria. In rare cases of gene carrierswith hereditary coproporphyria, in a¡ected children or those under therapy withhaem arginate (GroM et al 2002b), the excretion of haem precursors may beborderline. However, the coproporphyrinogen III oxidase activity is decreased underthese circumstances. Thus, this activity helps to recognize those persons as at risk.
The detection of enzyme concentration is not suitable for the recognition of genecarriers. Families with hereditary coproporphyria are reported in the literature within one case lowered (GroM et al 2002a) and in another case increased concentration(GroM et al 2002b) of coproporphyrinogen III oxidase.
Figure 2 Coproporphyrinogen III oxidase activity in mononuclear cells of a patient withhereditary coproporphyria and her family
Measurement of coproporphyrinogen oxidase activity 569
J. Inherit. Metab. Dis. 26 (2003)

A recent possibility for detecting gene carriers of hereditary coproporphyria withnormal excretion, for example some family members, is the analysis of the unknownmutation by denaturing gradient gel electrophoresis (GroM et al. 2002b; Petersenet al. 2000).
For a secure diagnosis of hereditary coproporphyria, especially in the subclinicalphase, two or more methods should be combined.
ACKNOWLEDGEMENTS
This study was supported by the German Research Association (grant GR 1363/2-3)and a grant of the Adolf Messer Foundation.
REFERENCES
BFyum A (1984) Separation of lymphocytes, granulocytes, and monocytes from human bloodusing iodinated density gradient media. Methods Enzymol 108: 88^102.
Bradford MM (1976) A rapid and sensitive method for the quantitation of microgram quan-tities of protein utilizing the principle of protein^dye binding. Anal Biochem 72: 248^254.
Doss MO, Gross U, Lamoril J, et al (1999) Compound heterozygous hereditarycoproporphyria with £uorescing teeth. Ann Clin Biochem 36: 680^682.
Gray D, Golub SH (1984) Cryopreservation of lymphoid cells. Methods Enzymol 108:363^367.
GroM U, Puy H, Kˇhnel A, et al (2002a) Molecular, immunological, enzymatic and biochemi-cal studies of coproporphyrinogen oxidase de¢ciency in a family with hereditarycoproporphyria. Cell Mol Biol 48: 49^55.
GroM U, Puy H, Meissauer U, et al (2002b) A molecular, enzymatic and clinical study in afamily with hereditary coproporphyria. J Inherit Metab Dis 25: 279^286.
Guo R, Lim CK, Peters TJ (1988) Accurate and speci¢c HPLC assay of coproporphyrinogenIII oxidase activity in human peripheral leucocytes. Clin Chim Acta 177: 245^252.
Kˇhnel A, GroM U, Doss MO (2000) Hereditary coproporphyria in Germany:clinical-biochemical studies in 53 patients. Clin Biochem 33: 465^473.
Layer G, Verfurth K, Mahlitz E, Jahn D (2002) Oxygen-independent coproporphyrinogen-IIIoxidase HemN from Escherichia coli. J Biol Chem 277: 34136^34142.
Martasek P (1998) Hereditary coproporphyria. Semin Liver Dis 18: 25^32.Petersen NE, KOehne M, Christiansen L, Brock A, Hother-Nielsen O, Rasmussen K (2000)DGGE analysis of the coproporphyrinogen oxidase gene: two new mutations in DNA fromDanish patients with hereditary coproporphyria. Scand J Clin Lab Invest 60: 617^626.
Takeuchi H, Kondo M, Daimon M, et al (2001) Neonatal-onset hereditary coproporphyriawith male pseudohermaphrodism. Blood 98: 3871^3873.
570 Gro5 et al
J. Inherit. Metab. Dis. 26 (2003)