Embed Size (px)
Citation preview
J. Duranteau
Department of Anaesthesia and Intensive Care
Hôpitaux universitaires Paris-Sud
A disaster in Paris

2
No conflict of interest

Stade de France
Bataclan
Rue de Charonne
Le Petit Cambodge
Cosa Nostra
Bd Voltaire
On November 13th 2015 in Paris, terrorists used explosives and assault rifles,
both on streets, café terraces, and in a theatre.
The city of Paris was exposed to 3 bomb explosions, 4 shooting scenes and
during 3 hours several hundreds people have been taken hostage
130 deaths and ≥ 540 injured victims

Stade de France
Bataclan
Rue de Charonne
Le Petit Cambodge
Cosa Nostra
Bd Voltaire

Most unstable patients were transferred to the six
trauma centers of the Paris
45 mobile intensive care units (MICU) of the SAMU (Services d’Aide
Médicale Urgente) and Fire-Brigade ambulances EMT with physicians
trained in disaster medicine had been mobilized and dispatched to the
six terrorist attack locations
Casualties were categorized as absolute (AE) or
relative (RE) emergencies
Uncontrolled admissions in closest non
trauma-oriented hospitals
Battle field

Scoop and run - Damage control strategy
Pre-hospital resuscitation procedures were
limited to essential measures
the on-going anti-terrorist action and the prolonged hostage-taking in the Bataclan
complicated access to the casualties, their prehospital care, and evacuation
Thirteen (4%) received orotracheal
intubation and 9 (3%)
catecholamine administration
No security on the battle field
Difficult and dangerous for emergency teams
(terrorist gunshots)
Transportation by ambulance convoys:
waves of patients
Inefficiency of
Advanced Medical Post
Scoop and run - Damage control strategy
Pre-hospital resuscitation procedures were
limited to essential measures
the on-going anti-terrorist action and the prolonged hostage-taking in the Bataclan
complicated access to the casualties, their prehospital care, and evacuation
Thirteen (4%) received orotracheal intubation and 9 (3%)
catecholamine administration
No security on the battle field
Difficult and dangerous for emergency teams
(terrorist gunshots)
Transportation by ambulance convoys: waves of patients
Inefficiency of
Advanced Medical Post

Massive mobilization of everyone, Solidarity and professionalism

What we learned from Paris terrorist attack
Controlled admissions in
trauma-oriented hospitals:
▪ 61 (51%) AE
▪ 94 (43%) RE
Controlled admissions in trauma-oriented
hospitals:
▪ 120 (36%) of absolute emergencies (AE)
▪ 217 (64%) of relatives emergencies (RE)
Uncontrolled admissions in closest
non trauma-oriented hospitals:
▪ 59 (49%) AE
▪ 123 (57%) RE
Hospital
mortality 2.1%
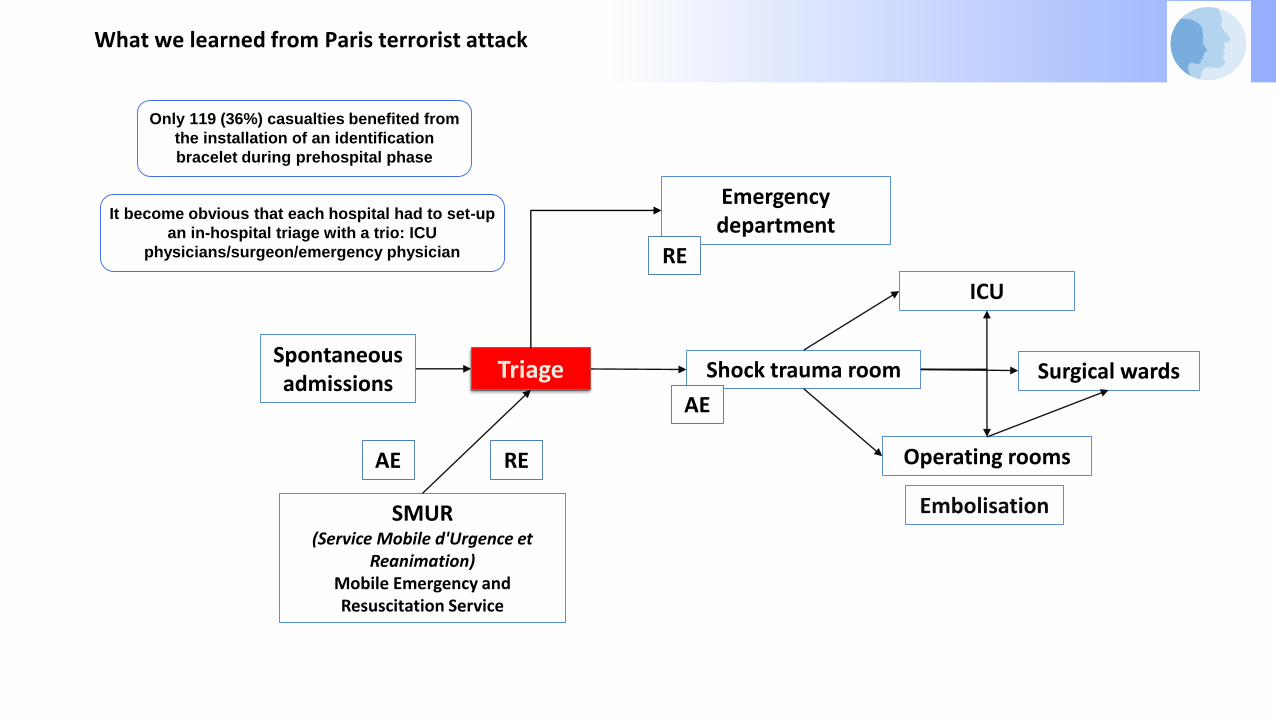
SMUR(Service Mobile d'Urgence et
Reanimation)Mobile Emergency and Resuscitation Service
Shock trauma room
Operating rooms
ICU
Emergency department
RE
AE
RE
Triage
AE
Spontaneousadmissions
Embolisation
Surgical wards
It become obvious that each hospital had to set-up
an in-hospital triage with a trio: ICU
physicians/surgeon/emergency physician
Only 119 (36%) casualties benefited from
the installation of an identification
bracelet during prehospital phase
What we learned from Paris terrorist attack

Rooms and Circuits
TriageEmergency department
Surgical Walls
ICU
Shock trauma room
Operating rooms
PediatricTrauma Room
Forward march
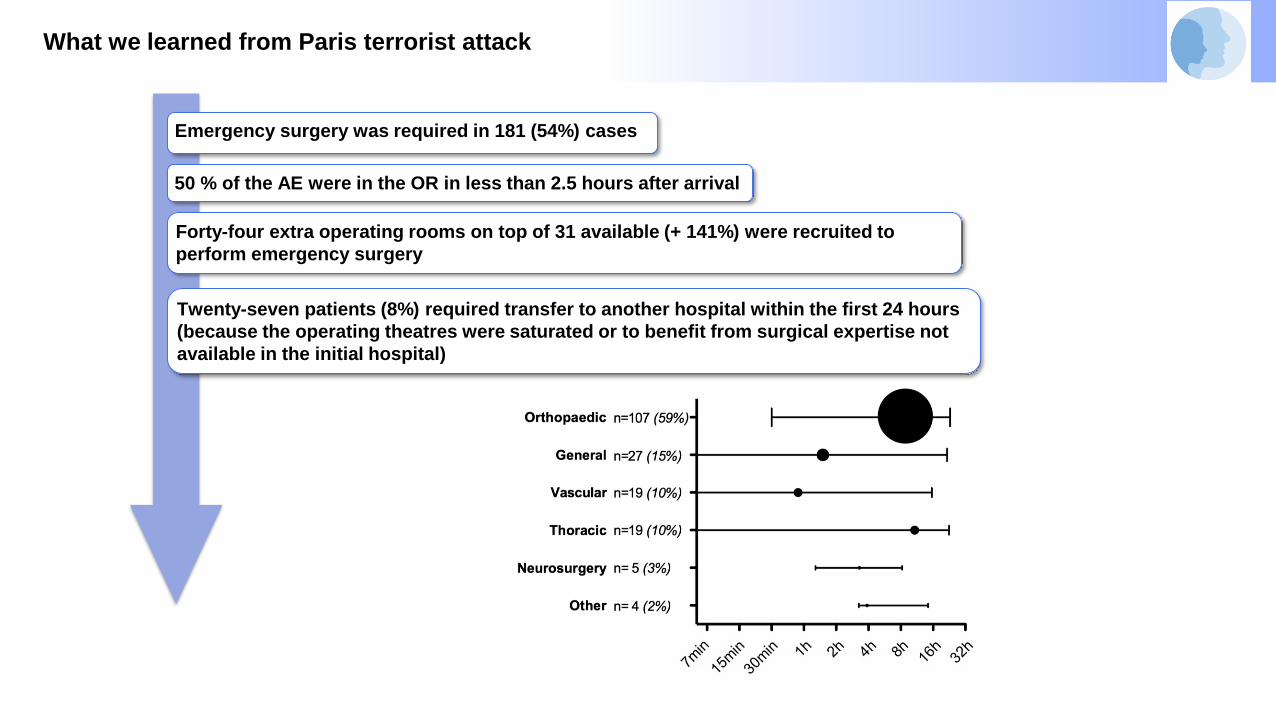
What we learned from Paris terrorist attack
Emergency surgery was required in 181 (54%) cases
50 % of the AE were in the OR in less than 2.5 hours after arrival
Forty-four extra operating rooms on top of 31 available (+ 141%) were recruited to
perform emergency surgery
Twenty-seven patients (8%) required transfer to another hospital within the first 24 hours
(because the operating theatres were saturated or to benefit from surgical expertise not
available in the initial hospital)

What we learned from Paris terrorist attack
Massive mobilization of everyone, Solidarity and professionalism
The recall of medical and nonmedical resources was performed in
collaboration with the crisis teams of hospital administrations
But also spontaneous mobilization of physicians and
nurses that we had to organize
Communications problems between hospital teams and out-
of-hospital emergency services
Thankfully, the Internet played a significant role and contact
was maintained throughout text messaging

Damage control resuscitation
Assessment and initial management
Management of respiratory and
hemodynamic failures
EFAST (extended focused assessment with sonography
for trauma) to augment clinical assessment
Major haemorrhage protocol activation
Peripheral + Central intravenous access + Arterial line
Fluid + Vasopressor resuscitation
Transfusion protocol
whole-body CT
Tourniquet - Pelvic binders

Training to manage successives “waves
of 10 patients”
▪ One team for one patient with an absolute emergency: 1
intensivist senior-1 intensivist junior / 2 nurses
▪ One team from the admission to the operating room
Afflux
Operating roomsICU
Shock Trauma
rooms
What we learned from Paris terrorist attack

Identification of victims
A key source of error and confusion
▪ Pre-admission with a pre-set anonymization
▪ 20 pre-admission nameless identities
▪ Each patient is identified also by a colour code and
the team in charge of the patient has an armband of
the same color
Nom : axbctnoviunPrénom : axbctnoviun
DDN : 01/01/1900

Family
Family area for the family of the victims with psychologists
and medical officers available to assist family and to provide
detailed personalized informations
Bed management
vision of bed capacity available and of the number of patients
that need to be discharged or transferred rapidly

Simulation
The morning of the day of the attacks, a multiple shooting simulation was organized in Paris!

Education
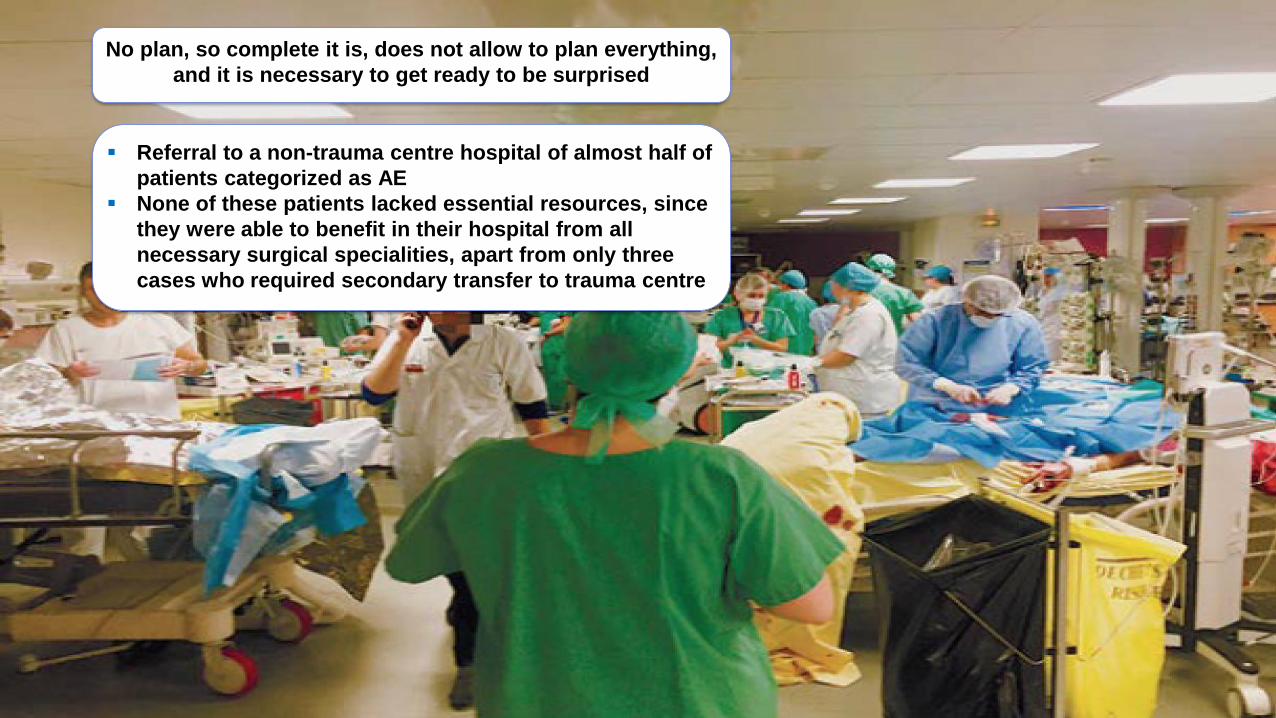
No plan, so complete it is, does not allow to plan everything,
and it is necessary to get ready to be surprised
▪ Referral to a non-trauma centre hospital of almost half of
patients categorized as AE
▪ None of these patients lacked essential resources, since
they were able to benefit in their hospital from all
necessary surgical specialities, apart from only three
cases who required secondary transfer to trauma centre

Hospital mortality <2.1%

What we learned from recent terrorist attacks
We have to be ready to take in charge « waves of patients»
We have to establish intra-hospital cicuits for these patients
We have to improve communications with the police
authorities and out-of-hospital emergency services
We have to be capable to identify patients
We have to train all the teams (simulation)
We have to educate physicians on damage control
B. Vigué
C. Laplace
C. Ract
P.E. Leblanc
G. Cheisson
A. Harrois
S. Figueiredo
S. Hamada
A. Rodrigues
G. Dubreuil
Department of Anaesthesia and Intensive Care
Hôpitaux Universitaires Paris-Sud
Bicêtre Hospital
« Change starts with one person standing up
and saying « no more » »





























