Embed Size (px)
Citation preview

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014
Today we’ll finish the liver diseases. Italic bold font represents the extra information.
Alcoholic liver disease
- It is the most common liver disease in the west- It is the most common cause of cirrhosis and the most common cause of liver cancer in
the west (because alcohol is more prevalent in the west)
The important information about alcoholic liver diseases:
1. Chronicity (time) is more important than the cause or the amount itself (the longer the duration of exposure to alcohol, the higher the probability to get the disease)
I.e: Short term exposure to intake of 80 mg / day (which is considered a high dose) might cause mild and reversible changes
While, chronic intake of 50-60 mg / day can cause severe hepatitis and liver injury
2. It is more important and damage is more severe in females
3. Variation exists between individuals (susceptibility or chance of getting the disease varies)I.e: Some people don’t develop the disease even if they take it for a long time,others might have severe disease upon exposure to a lower dose
4. Type of alcohol and habit of drinking are also important; possibility of liver disease is higher and more severe with beer consumption, compared to wine, and with binge-drinking habit rather than drinking in small sips ( شرب من بدل الشرب في االفراط
صغيرة (رشفات
1

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014
I.e: Wine has higher concentration of alcohol than beer, but still risk of disease in beer is higher because it is related to the amount as a person may consume higher amounts than wine
5. There is no cut-limit (threshold) between safe and dangerous (disease-causing) amount of alcohol consumption - due to the individual variation and susceptibility
→Thisis also applied to the red wine; despite the small doses it may be a risk factor for liver disease occurrence. Although red wine is taken for its protective value against cardiovascular diseases as it reduces lipid concentration in the blood
6. Morphological changes of alcoholic liver diseases:
A. Steatosis (most important feature) - alcohol consumption causes both micro-vesicular and macro-vesicular lipid accumulation in the cytoplasm of hepatocytes through different mechanisms;
1. Byproducts of alcohol metabolism result in fat synthesis inside the hepatocytes;
The two enzymes responsible for alcohol metabolism and degradation are present inside the cytoplasm of the liver cells – alcohol dehydrogenase and acetaldehyde dehydrogenase. A characteristic feature of these enzymes is that they don’t have a plateau level; the more the alcohol dose, the more the concentration and activation of these enzymes
2

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014
2. Alcohol impairs the assembly and secretion of lipoproteins to the blood; so more fat is stored in the hepatocytes
3. Alcohol increases peripheral catabolism of adipose tissue - so more fat is carried to the blood and finally it reaches the liver
B. Inflammation; both alcohol and acetaldehyde can cause physical damage to the cells, whether to the membrane or to the cytoskeleton, leading to cell ballooning, followed by necrosis and inflammation.
7. Histology:
a. Steatosis:
3

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014Most prevalent finding, present in 100% of patients in various degrees according to the amount of alcohol consumptionStarts as micro-vesicular and centri-lobular(reversible), then progress to macro-vesicular(reversible), then finally irreversible fibrosis occurs in association with the damage
b. Hepatitis:The inflammation is present in around 1/3rd of patients – 35%Inflammation signifies more damage, with more progress to fibrosis and less reversibility - even if the patient stops drinking Inflammation is separate and independent of Steatosis; it might appear before Steatosis (not necessarily following Steatosis), it may be predominant more than Steatosis
c. Cirrhosis:20% of cases progress to cirrhosis; which is a high chance compared to viral cirrhosisIn early cirrhosis - the liver is large and we have steatosisIn late cirrhosis – shrinkage, less apparent steatosis (due to shrinkage and more damage to the hepatocytes) and small nodules of maximum 3 mm diameter (in contrast to viral cirrhosis)
d. Hepatocellular carcinoma:The least common complication of around 5% chance of occurrence - but still it is a risk factor for carcinoma
Slide 12: Revision for Alcoholic Liver Disease
4

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014This is normal liver, if patient has chronic exposure to alcohol, he develops steatosis which is the most common and by definition it is reversible upon abstinence (امتناع). In severe exposure cases, hepatitis occurs (inflammation due to direct damage of the hepatocytes by increased concentration of alcohol and acetaldehyde), it has less reversibility upon abstinence. Steatosis and hepatitis are independent, any of them might appear first or they may be combined. Then the final stage is the cirrhosis.
Slide 13:
This is a section of advanced stagealcohol liver disease, stained by the specialMasson tri-chrome stain ( ثالثي which is used to stain the collagen fibers in blue to assess the –(ملونdegree of fibrosis
The hepatic parenchyma appears white due to macro-vesicular steatosis (appears as if it is adipose tissue section not liver). If we look carefully around each individual cell we can see fibrosis, since fibrosis starts peri-cellular and then grows into bands (there are four fibrotic bands apparent in the figure)
The Central Vein (Most Upper Left) appears with fibrosis around it
These areas can be appreciated as the beginning of nodules – therefore, indicating cirrhosis and advanced disease stage
Slide 14:
Hepatitis can occur
a. Hepatitis resembled by a cluster of inflammatory cells, mainly small lymphocytes with dark nuclei surrounding dead hepatocytes (which lack nuclei)
5

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014
b. Mallory bodies; specific to alcohol liver disease – not seen in viral hepatitisThey appear as very dark pink within the cytoplasm due to the degradation of aggregation of the cytokeratin proteins
Slide 15:6

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014A gross picture showing small nodules all over the liver, and sometimes it is greenish
due to accumulation of bile
--------------------------------- End of Alcoholic Liver Disease ----------------------------------
Drug Induced Hepatitis:
We have history of drug intake which causes the clinical morphology, although it resembles the viral hepatitis under the microscope in terms of presence of damage to the hepatocytes, inflammation and even progression to cirrhosis (in cases of chronic exposure) but by definition viral screen is negative
- Very common
- Liver is the main site of metabolism of most drugs – making it more vulnerable to damage due to drugs
- It is important for us to know that there are two types of damage:
1. Predictable (Intrinsic risk) –hepatitis caused as a side effect of the drug, is very common, the % of patients receiving the medication who will develop drug induced hepatitis is known , is dose - dependent
E.g: 7

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014a. Paracetamol (very common analgesic) in high dosesb. Tetracyclin (an antibiotic commonly used in our practice)
2. Unpredictable (Idiosyncratic)- very rare , more dangerous (can be lethal), due to an odd (uncommon) unexpected allergic reaction toward a certain drug
Results from:
a) Autoimmune disease; allergy toward a certain drug
b) Polymorphism; this is not a disease, it is a genetic variation within a small % of the total population resulting in having different proteins and therefore less metabolism of drugs by their bodies - unlike the majority of the population
E.g:
a. Halothane (pre-surgical anesthetic)We mentioned halothane when we talked about fulminant hepatitis; drug is one of the causes of severe liver injury and necrosis
b. Aspirin consumption by children; Rye syndrome – may lead to the same reaction
- Clinically and histologically it resembles viral hepatitis and autoimmune hepatitis; therefore history of any previous drug intake is taken and exclusion of viral hepatitis
8

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014through serologic markers is done to diagnose the disease and distinguish it from the viral or autoimmune hepatitis
- If the drug is stopped – the hepatitis is reversible
------------------------------------ End of Drug-Induced Hepatitis -------------------------------------
Non-Alcoholic Fatty Liver Disease:
- Same symptoms and morphology as Alcoholic Fatty Liver disease, with the only difference that there is no alcohol or drug consumption here
- Develops in patients having chronic diseases of metabolic, the most common being Diabetes Mellitus Type 2
- Diabetes changes all the normal metabolism in the body, most importantly the liver is affected – leading to abnormal metabolism in proteins, carbohydrates and lipidsleading to liver disease identical to alcohol
- Can show only steatosis (named fatty liver) or with additional inflammation (named hepatitis)or only hepatitis (very rarely) or steato-hepatitis (both components)
- The old name is NASH – non-alcoholic steato-hepatitis
9

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014- Causes: Diabetes (most common), obesity (related to diabetes) and hyperlipidemia
- Commonly, diabetes – obesity and hyperlipidemia come together and we call them “metabolic syndrome”.Sometimes they are also associated with hypertension and ischemic heart disease
------------------------------------------------------------------------------------------ Alakyaz Assadorian
Non alcoholic fatty liver disease
-how does NAFLD develop fat storage ?
Tissue in diabetes patient are resistant to imsuline .however; the insulin try to do its job but they don’t respond so its concentration will increase in the blood .
Because the glucose is resistant to insulin this will make insulin work on fat .
The insulin is considered as most potent anabolic hormone in the body (it builds glycogen and fat ) …so it works on fat through :
• (1) impaired oxidation of fatty acids
• (2) increased synthesis and uptake of fatty acids
• (3) decrease hepatic secretion of very-low-density lipoprotein cholesterol (VLDL).
Hepatocyte cells are very sensitive to lipid peroxidation cuz these radicals will take some charges from the fat and cuz severe damage and inflammation then apoptosis .
10

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014
peroxidation : is free radicals toxin molecules they appear in any type of inflammation occur or any minor trauma and they cuz damage to any cell in the body .
The peripheral fat in patient with diabetes increase secretion oF TNF and IL-6 which are inflammatory mediators so the can cuz inflammation in the liver .
the morphology of NAFLD s the same (steatosis ,inflammation cirrhosis ).
Portal tract
There are two main diseases in the portal tract :1)biliarycirrhosis .2)primary sclerosing cholangitis
**biliary cirrhosis
It affect the bile duct in biliary tree.
It is classified to two categories :
i) Primary : it is the main disease and it is an autoimmune disease with NO cuzes occure in the biliary tree ( it’s open ) .
ii) Secondary : the closure of the biliary tree either by stone or destructions is the most common in secondary biliary tree , so the bile will stagnate and make inflammation that make damage to the cells then cirrhosis.
11

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014• Primary biliary cirrhosis is a chronic, progressive, and often fatal cholestatic liver
disease, characterized by the destruction of intrahepatic bile ducts( the extra is
intact ) , portal inflammation and scarring, and the eventual development of cirrhosis and liver failure over years to decades
• PBC is primarily a disease of middle-aged women
• Commonly associated with other autoimmune diseases
• High serum anti-mitochondrial antibodies (?)
• In the early lesions there is a dense lymphocyte/plasma cell infiltrate around small bile ducts in portal tracts, and granulomatous lesions may also appear
• With time, cirrhosis develop, and the liver is very cholestatic
The picture below shows biliary portal area with inflammatory cells ( lymphocyte and plasma cells ) . the hepatitis C & biliary portal area are differentiate to each other ( they are the same morphology ).
12
Primary biliary cirrhosis. A portal tract is markedly expanded by an infiltrate of lymphocytes and plasma cells

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014
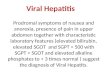
Primary sclerosing cholangitis
Its more sclerosis than inflammation .there is no clear cuzes .it’s a chronic choleastatis disorder .characterized by progressive fibrosis and destruction of EXTRAHEPATIC and larg INTRAHEPATIC bile duct .
it is more common in males and the clinical setting is differ than primary biliary cirrhosis ,there is NO Autoimmune disease ,in contrast they have Inflammatory Bowel Disease .
the extrahepatic and intrahepatic bile duct appear as white skipped region ( normal-diseas-normal-dosease …and so on ) like a beading ( ( المسبحة مثل مقسمينSo, beading appearance is a characteristic for primary sclerosis cholangitis .
Serology : there is no antibodies mitochondrial , there is another antibody called “antinutrophil cytoplasmic antibody “ ANCA .
13

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014
Progress to cirrhosis.
No effective medical therapy.
The picture below related to primary sclerosing cholangitis ,there is significant fibrosis ,but the inflammation is minimal .
fibrosis appear as a cellular segmental .its appeare as onion .
14

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014
Hepatocellular carcinoma
It is a rare and bad disease ,5% of all human cancer.the risk fators : HBV , HCV .ALCOHOL and aflatoxin
Aflatoxin : is a toxin from fungus .if the food is contaminated with it it will make hepatocellular carcinoma .
15
Primary sclerosing cholangitis. A bile duct undergoing degeneration is entrapped in a dense, "onion-skin" concentric scar

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014• HBC & HCV and aflatoxin are most common in the far EAST of ASIA .however , the
alcoholic risk factor that cuz hepatocellular carcinoma are common in west .
May develop without previous cirrhosis
• Highly invasive to the veins, reaching the major vessels and heart
• Poor prognosis with no effevtive treatment
Morphology
• Grossly appears as a large mass or small multiple masses without nodule .
• Microscopically, the architecture is disturbed (however, in cirrhosis there is nodules stable in plates without disturbed , the liver cells arrange in plate ) . Under normal situations, hepatocytes are arranged in plates of 1-2 cell thickness, surrounded by sinusoids. In HCC, there is marked increase in cell layers
16

HibaKhalayleh-Alakyaz Assadourian Pathology – Sheet 14 24/3/2014• Hepatocellular carcinoma. A large neoplasm with extensive areas of necrosis has
replaced most of the right hepatic lobe in this noncirrhotic liver. A satellite tumor nodule is directly adjacent with yellow color related to necrosis.
Hepatocellular carcinoma Carcinoma cells forming trabecular, pseudoacinar architecture. No portal areas are seen , the cells are hazard in arrangement with no normal structure , the nuclri are not in regular arrangement
•
17