-
University of Southern Denmark
Treatment of chronic post-herpetic neuralgia with autologous fat
grafts
a first-in-the-world case reportSollie, Martin; Sørensen, Jens
Ahm
Published in:British Journal of Pain
DOI:10.1177/2049463718817570
Publication date:2019
Document version:Accepted manuscript
Citation for pulished version (APA):Sollie, M., & Sørensen,
J. A. (2019). Treatment of chronic post-herpetic neuralgia with
autologous fat grafts: afirst-in-the-world case report. British
Journal of Pain, 13(4), 239-243.
https://doi.org/10.1177/2049463718817570
Go to publication entry in University of Southern Denmark's
Research Portal
Terms of useThis work is brought to you by the University of
Southern Denmark.Unless otherwise specified it has been shared
according to the terms for self-archiving.If no other license is
stated, these terms apply:
• You may download this work for personal use only. • You may
not further distribute the material or use it for any profit-making
activity or commercial gain • You may freely distribute the URL
identifying this open access versionIf you believe that this
document breaches copyright please contact us providing details and
we will investigate your claim.Please direct all enquiries to
[email protected]
Download date: 03. Jul. 2021
https://doi.org/10.1177/2049463718817570https://doi.org/10.1177/2049463718817570https://portal.findresearcher.sdu.dk/en/publications/695c6119-c8c9-4fab-8ad3-98d6ef8d9f21
-
1
Title
Treatment of Chronic Post-Herpetic Neuralgia with Autologous Fat
Grafts: A first in the world case report
Abstract A 60-year-old woman suffering from severe chronic
post-herpetic neuralgia (PHN) was treated with simple autologous
fat grafting to the affected area of skin. Post-operatively she
reported a great improvement in her symptoms. The effect was stable
throughout the three months follow-up period. This case report
presents a first in the world case of using fat grafting to treat
chronic post-herpetic neuralgia and discusses the future potential
of this as a primary treatment of this syndrome. This report
presents partial data of a pilot study registered at
clinicaltrials.org. (ClinicalTrials.gov Identifier: NCT03584061)
Key points:
- PHN is chronic pain in the skin area of previous outbreak of
Herpes Zoster. - PHN is a common, very painful and exceptionally
drug-resistant condition. - The future prevalence of PHN will most
likely increase as the population ages. - Pharmacological treatment
is often unsuccessful and alternative treatments are not
available. - Autologous fat grafting shows promise in relieving
pain from PHN.
Keywords Post-herpetic neuralgia, neuralgia, fat grafting,
autologous fat grafting, stem cells.
-
2
Introduction Postherpetic neuralgia (PHN) is a neuropathic pain
syndrome occurring after an outbreak herpes zoster (HZ) or
“shingles”. It is caused by a reactivation of varicella zoster
virus (VZV)1,2. The risk of developing PHN after HZ is reported
being between 5% to 30% and the pain can last up to 10 years3.
Clinically, the disease is characterized by a painful, unilateral
vesicular eruption, which usually occurs with limited dermatomal
distribution1. Pain is the predominant symptom in all phases of the
disease and is reported in up to 90% of patients4. Most patients
with PHN describe three types of pain: a constant deep, aching or
burning pain, a paroxysmal, lancinating pain, and allodynia5.
Treatment of PHN is complex and the neuropathic pain is
exceptionally drug-resistant5. Several broad recommendations on
treatment of the neuropathic pain have been published 6–8. There
is, however, currently, no internationally accepted guideline of
treating PHN1. Treatment consists of topically and systemically
administered medication. The present standard of care in not very
effective and new treatments are needed. One such approach is
autologous fat grafting. Fat tissue is abundant in most individuals
and fat grafting is a safe and simple procedure. Fat grafting has
shown potential in treating several painful conditions, such as
post-mastectomy pain and scar-related pain, but it has not
previously been used to treat post-herpetic neuralgia9–11.
Case presentation The patient was a 60-year old woman with pain
in the areas of the previous shingles-rash. The reactivation of VZV
had occurred three years previously. The area of outbreak measured
30 x 10 cm and stretched from the right side of the abdomen
backwards towards the columna. The patient described the pain in
the affected areas as a constant burning, throbbing pain. She had
previously tried several pain medications for her condition without
any effect. The medications tried were paracetamol, ibuprofen,
tramadol, and gabapentin. As she felt they had no effect, she had
stopped taking them prior to beginning our treatment. The affected
area was marked pre-operatively by the surgeon and the patient. The
marked area can be seen in photo 1. The patient was thoroughly
informed of the potential risks of the procedure and signed a
written consent form prior to surgery. [insert PHOTO1]
-
3
Photo 1. The area of pain marked pre-operatively. The area
marked with cross-markings was the area with the most
predominant pain. This was the area where fat-injection
was performed.
Treatment The procedure was performed under general anesthesia.
Liposuction (body-jet; Human med AG, Schwerin, Germany,
http://www.humanmed.com) was performed by harvesting fat from the
abdomen. Prior to harvesting, the area was prepared by installing
ringer-adrenalin solution. 300 cc of fat was harvested. The fat was
then decanted. After 15 minutes 120 cc of fat was injected
sub-dermally in the marked area of pain using 10 ml cannulas. The
patient was then fitted with a compression belt for the area of
liposuction. The patient was discharged the same afternoon.
Investigations Outcomes measured were degree and quality of
neuropathic pain and Quality of Life. Neuropathic pain was measured
using the questionnaire: Neuropathic Pain Symptom Inventory Scale
(NPSI) 12. Quality of Life was measured using the Short Form 36
(SF-36)
-
4
questionnaire 13–15. All questionnaires have validated
translations into Danish12,15. The questionnaire was filled out by
the patient pre-operatively and three months postoperatively.
Effect of treatment A few days after the surgery the patient
reported improvement of her symptoms. This continued throughout the
follow-up period. The patient experienced improvement in all
measured parameters. Quality of life was measured using the SF-36
questionnaire. The patient reported improvement in all Quality of
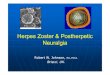
Life-parameters (FIGURE 1). The degree and quality of pain were
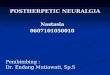
measured using the NPSI. The patient reported improvement in all
types of recorded pain (FIGURE 2). The patient did not report any
disturbances in the sensation of the skin. There was no cosmetic
effect of the treatment and no severe side effects were
observed.
Figure 1. Results of the SF-36 recorded pre-surgery and 3 months
post-surgery. The maximum score of each parameter was 100.
-
5
Figure 2. Results of the NPSI recorded pre-surgery and 3 months
post-surgery. The maximum score of each parameter was 10.
Discussion Relevance of treatment: One in four people will
suffer from HZ in their lifetime and the risk is markedly increased
after the age of 50, with an incidence of almost 50% in elderly
individuals. The prevalence of PHN will likely increase in the
future as the population ages. The resolve of the disease is slow
and the disease has been shown to have a negative impact on Quality
of Life 16–18. Today’s treatment regimen of medications has
potentially serious side effects and the risk of addiction. It is
therefore important that we find an effective way of treating these
patients. Pathophysiology: The pathophysiology behind HZ and PHN is
neural damage to both the peripheral and central nervous system. HZ
also induces neuroinflammation, a process that normally promotes
regeneration and healing. If the resolution of neuroinflammation is
disturbed, the result may
-
6
be chronic pain19,20. The direct damage and continued
inflammation lower the threshold for action potentials, causing the
nerves to fire painful signals, even by non-painful stimuli21. Skin
biopsies of people affected by HZ and PHN have shown a lowered
number of free epidermal nerve endings, with an even lower number
in people with PHN compared to HZ alone 22. The aim of treatment
should, therefore, be to modulate the signaling by the nerve
endings by resolving the neuroinflammation and by repairing the
damage and possibly help increase the number of free epidermal
nerve ending. Fat grafting, safety, and possible effect: Fat
grafting has been used for many years and has proven to be a simple
and safe procedure. The most common side effects such as; numbness,
bruising, pain, swelling, infection, and changes in skin sensation
are usually mild and easily treated. Fat grafting has shown
potential in treating painful conditions such as post-mastectomy
pain syndrome, painful neurinomas, and painful scars9–11,23 The
exact mechanism of fat grafting on painful conditions is not known
and there are several theories being debated. First, fat grafting
has a potential anti-inflammatory effect. In mouse model studies
fat grafting to the sub-dermal tissues has shown an
anti-inflammatory effect, both in the skin and in the spinal cord.
The level of neuropathic pain was also reduced 24. The stem cells
within the fatty tissue could also play a role in the
pain-relieving effect. Adipose Derived Stem Cells (ADSC) have shown
the ability to secrete several different growth factors in vitro,
possibly inducing repair of damaged nerves25. The use of ADSC alone
has also proven to have a pain relieving effect in people affected
by neuropathic trigeminal pain26. The third possible effect could
be the injected fats ability to act as a filler that cushions and
improves chronic pain. In our study, this is unlikely as the amount
of injected fat was very small. Fat grafting is also a relatively
inexpensive treatment. When the liposuction equipment has been
acquired, the cost of each individual treatment is low. Though no
cost-benefit analysis has been performed, we would argue that a
single treatment of fat grafting is preferable compared to a
lifetime of medications. We believe that the method presented could
be a potential treatment for patients affected by PHN. Future
studies are needed to investigate the effect. This case study is a
part of a pilot study currently undergoing at our department. Based
on the promising preclinical and clinical results, we are planning
a phase II study in our department to further test the feasibility
and safety of this procedure (ClinicalTrials.gov Identifier:
NCT03584061) )
References 1. Gan EY, Tian EAL, Tey HL. Management of herpes
zoster and post-herpetic neuralgia. Am J Clin Dermatol 2013; 14:
77–85.
-
7
2. Schutzer-Weissmann J, Farquhar-Smith P. Post-herpetic
neuralgia - a review of current management and future directions.
Expert Opin Pharmacother 2017; 18: 1739–1750. 3. Kawai K,
Gebremeskel BG, Acosta CJ. Systematic review of incidence and
complications of herpes zoster: towards a global perspective. BMJ
Open 2014; 4: e004833. 4. Johnson RW, Bouhassira D, Kassianos G, et
al. The impact of herpes zoster and post-herpetic neuralgia on
quality-of-life. BMC Med 2010; 8: 37. 5. Truini A, Galeotti F,
Haanpaa M, et al. Pathophysiology of pain in postherpetic
neuralgia: a clinical and neurophysiological study. Pain 2008; 140:
405–410. 6. Attal N, Cruccu G, Baron R, et al. EFNS guidelines on
the pharmacological treatment of neuropathic pain: 2010 revision.
Eur J Neurol 2010; 17: 1113-e88. 7. Finnerup NB, Attal N,
Haroutounian S, et al. Pharmacotherapy for neuropathic pain in
adults: systematic review, meta-analysis and updated NeuPSIG
recommendations. Lancet Neurol 2015; 14: 162–173. 8. Moulin D,
Boulanger A, Clark AJ, et al. Pharmacological management of chronic
neuropathic pain: revised consensus statement from the Canadian
Pain Society. Pain Res Manag 2014; 19: 328–335. 9. Caviggioli F,
Maione L, Forcellini D, et al. Autologous fat graft in
postmastectomy pain syndrome. Plast Reconstr Surg 2011; 128:
349–352. 10. Klinger M, Caviggioli F, Klinger FM, et al. Autologous
fat graft in scar treatment. J Craniofac Surg 2013; 24: 1610–1615.
11. Maione L, Vinci V, Caviggioli F, et al. Autologous fat graft in
postmastectomy pain syndrome following breast conservative surgery
and radiotherapy. Aesthetic Plast Surg 2014; 38: 528–532. 12.
Bouhassira D, Attal N, Fermanian J, et al. Development and
validation of the Neuropathic Pain Symptom Inventory. Pain 2004;
108: 248–257. 13. Bjorner JB, Damsgaard MT, Watt T, et al. Tests of
data quality, scaling assumptions, and reliability of the Danish
SF-36. J Clin Epidemiol 1998; 51: 1001–1011. 14. Bjorner JB,
Kreiner S, Ware JE, et al. Differential item functioning in the
Danish translation of the SF-36. J Clin Epidemiol 1998; 51:
1189–1202. 15. Bjorner JB, Thunedborg K, Kristensen TS, et al. The
Danish SF-36 Health Survey: translation and preliminary validity
studies. J Clin Epidemiol 1998; 51: 991–999. 16. Laurent B, Vicaut
E, Leplège A, et al. Prevalence and impact on quality of life of
post-herpetic neuralgia in French medical centers specialized in
chronic pain management: the ZOCAD study. Med Mal Infect 2014; 44:
515–524. 17. Mizukami A, Sato K, Adachi K, et al. Impact of Herpes
Zoster and Post-Herpetic Neuralgia on Health-Related Quality of
Life in Japanese Adults Aged 60 Years or Older: Results from a
Prospective, Observational Cohort Study. Clin Drug Investig 2018;
38: 29–37. 18. Serpell M, Gater A, Carroll S, et al. Burden of
post-herpetic neuralgia in a sample of UK residents aged 50 years
or older: findings from the Zoster Quality of Life (ZQOL) study.
Health Qual Life Outcomes 2014; 12: 92. 19. Sommer C, Leinders M,
Üçeyler N. Inflammation in the pathophysiology of neuropathic pain.
Pain 2018; 159: 595–602. 20. Huh Y, Ji R-R, Chen G.
Neuroinflammation, Bone Marrow Stem Cells, and Chronic Pain. Front
Immunol 2017; 8: 1014. 21. Woolf CJ, Mannion RJ. Neuropathic pain:
aetiology, symptoms, mechanisms, and management. Lancet 1999; 353:
1959–1964. 22. Oaklander AL. The density of remaining nerve endings
in human skin with and without
-
8
postherpetic neuralgia after shingles. Pain 2001; 92: 139–145.
23. Vaienti L, Gazzola R, Villani F, et al. Perineural fat grafting
in the treatment of painful neuromas. Tech Hand Up Extrem Surg
2012; 16: 52–55. 24. Huang S-H, Wu S-H, Lee S-S, et al. Fat
Grafting in Burn Scar Alleviates Neuropathic Pain via
Anti-Inflammation Effect in Scar and Spinal Cord. PLoS One; 10.
Epub ahead of print September 14, 2015. DOI:
10.1371/journal.pone.0137563. 25. Rehman J, Traktuev D, Li J, et
al. Secretion of angiogenic and antiapoptotic factors by human
adipose stromal cells. Circulation 2004; 109: 1292–1298. 26.
Vickers ER, Karsten E, Flood J, et al. A preliminary report on stem
cell therapy for neuropathic pain in humans. J Pain Res 2014; 7:
255–263.