Embed Size (px)
Citation preview

Council of Governors Meeting 4.00 – 6.00pm on 24 July 2017
The Education Centre, Birmingham Heartlands Hospital
A G E N D A
Presenter
1. Apologies
Jacqui Smith
2. Declarations of Interest 2.1 Governors 2.2 Directors
Jacqui Smith (Enclosure) (Enclosure)
3. Minutes of previous meetings – 3.1 17 May 2017 3.2 26 June 2017
Jacqui Smith
(Enclosure) (Enclosure)
4. Matters arising
Jacqui Smith (Oral)
5. Chair’s Update – Emerging Issues
Jacqui Smith (Oral )
6. Performance Report
Kevin Bolger (Enclosure)
7. Clinical Quality Report Q1
David Rosser (Enclosure)
8. Care Quality Report Q1 8.1 Annual Infection Prevention and Control Report
Sam Foster (Enclosure) (Enclosure)
9. Finance Report Q1
Julian Miller (Enclosure)
10. Quality Report update Q1 David Rosser (Enclosure)
11. Compliance & Assurance Report Q1 David Burbridge (Enclosure)
12. Health & Safety Annual Report David Burbridge (Enclosure)
13. Any Other Business Previously Advised to the Chair

COUNCIL OF GOVERNORS
REGISTER OF INTERESTS
NAME INTEREST DECLARED DATE DECLARED
DATE CEASED
Stan Baldwin
1. Joint Vice Chair – Solihull College & University Centre
2. Member of the Institute of Sport and Physical Activity
3. Fellow of The Chartered Management Institute
17 Aug 2016
Kath Bell Company Secretary – Succeed Services Ltd 21 Nov 2011
Nicola Burgess Assistant Professor of Operations Management, Warwick Business School, Warwick University and honorary contract with HEFT to conduct research.
2 Jun 2015
Tony Cannon No relevant of material interests 7 Sep 2016
Carol Doyle Awaiting information
Sarah Edwards Awaiting information
Keith Fielding 1) Fellow & Guest Lecturer – Cranfield University 2) Consultant & Guest Lecturer – Business
Development Midlands Ltd 3) Member - Institute of Leadership & Management 4) Member - British Chamber of Commerce in
Lithuania 5) Guest Lecturer - International School of Law
(Vilnius) 6) Member - Latvian Chamber of Commerce 7) Speaker - Latvian School of Political Sciences 8) Member - North Midlands Society of Rugby
Football Referees 9) Treasurer - Castle Bromwich Cricket & Sports
Club 10) Member & Taster - Order of the Froth Blowers 11) Consultant - Lagos Business School 12) Consultant - Nigerian Business Improvement
School 13) Lecturer - Ikorodu College 14) Member - Lekki Business School 15) Member - Stuttgart Chamber of Commerce 16) Member - IHK Frankfurt
Oct 2005 Sept 2007 Sept 2007 Mar 2016 Mar 2016 Nov 2015 Nov 2015 1990 1968 2013 2009 2009 2009 2009 2002 2003
Albert Fletcher Director – Aquarius (unpaid). A charity that specialises in helping and treating those with drink and/or drug issues.
28 May 2013
Derek Hoey 1. Member of Advisory Board / Volunteer - Healthwatch, Staffordshire
2. Committee Member – Tamworth and District Civic Society
3. Magistrate – South East Staffordshire Magistrates Bench
22 Aug 2016

4. District Patient Group Member – South East
Staffs and Seisdon Peninsula CCG
Sue Hutchings Shareholder in Lloyds TSB 19 Sept 2013
Phillip Johnson Nothing to declare 21 Nov 2011
Attiqa Khan Nothing to declare 16 Aug 2013
Anne McGeever 1. Registered with Therapy Bank in Worcestershire to provide services to BMI Droitwich Spa Hospital.
2. Unite Professionals Limited (Occupational Therapists) – ad hoc employment.
12 Sep 2014
14 Apr 2015
Veronica Morgan 1. Magistrate in criminal and family courts 2. Shareholder in Halifax, Millwall FC and Lloyds
TSB 3. Member (patient rep) of West Midlands Breast
Expert Advisory Committee 4. Member of West Midlands Cancer patient
&public engagement expert advisory group 5. Expert member on Solihull Research Ethics
Committee 6. HEFT Employee
07 Jan 2016 07 Jan 2016 07 Jan 2016 07 Jan 2016 07 Jan 2016 07 Jan 2016
Gerry Moynihan Nothing to declare
31 Jan 2017
Barry Orriss Member of Project Management Team, Warwick Medical School, University of Warwick
7 Apr 2016
Louise Passey Conservative Town Councillor – Royal Sutton Coldfield Town Council
16 Aug 2016
Mike Robinson 1. Solihull MBC – Health & Adult Social Care SB 2. Hampton-in-Arden Surgery – PPG Member
03 July 2017
Jane Teall Awaiting information
Jean Thomas Nothing to declare 30 Sep 2014
David Treadwell 1. Shareholder – Lloyds TSB 2. Shareholder – STW 3. Shareholder – National Grid
21 Nov 2011
Matthew Trotter
1. HEFT Employee 2. Director Specialist Health Partnership 3. Director Specialist ENT Care Ltd
12 Sep 13 15 Dec 14
David Wallis 1. Knowle, Dorridge & Bentley Heath Neighbourhood Plan Ltd – Director
2. Prospect (Trade Union) – Member 3. Member – Steering Group of Healthwatch Solihull
16 Sept 2015 16 Sept 2015 24 Apr 2017.
Tom Webster
Awaiting information
Lee Williams
Awaiting information

REGISTER OF DIRECTORS and REGISTER OF DIRECTORS’ INTERESTS
VOTING DIRECTORS
NAME DATE OF
APPOINTMENT INTEREST (if any)
DATE OF NOTIFICATION
DATE OF TERMINATION OF INTEREST
Mr Jonathan Brotherton 04.03.15 Nothing to declare 04.03.15
Mr Andrew Edwards 01.10.14 1. Couch Perry & Wilkes - in receipt of annuity following business sale until May 2019.
2. Voluntary role as a business mentor for the Prince's Trust.
01.10.14
26.04.16
Mrs Sam Foster 01.09.13 Nothing to declare. 01.09.13
Prof Jon Glasby 01.10.15 1. Professor / Head of School, University
of Birmingham
2. Senior Fellow, NIHR School for Social
Care Research
3. Member of Birmingham Health
Partners Executive Group
4. Works with Birmingham Safeguarding
Children’s Board from time to time.
3. Fellow of Royal Society of Arts
4. Board Member – Campaign for Social
Services
01.10.15
01.10.15
01.10.15
06.01.16
14.02.17
14.02.17
Ms Hazel Gunter 04.03.15
Nothing to declare. 04.03.15
Mrs Jackie Hendley 13.06.16 1. Director - SC Advisory Services Ltd
2. Director - Smith Cooper - IT Services
Ltd
3. Director – Smith Cooper Ltd
4. Partner/Member – SHH 101 LLP
13.05.13
13.05.13
13.05.13
01.04.14
Dr Michael Kinski 13.06.16 1. NED - Infinis Capital Limited (UK)
2. NED - Trireme Holdings Ltd (USA)
3. Senior Independent Director - AWAS
Aviation Capital Ltd (Dublin)
4. NED - Lake Woods Holding Pty
(Australia)
5. Prof of Business Change – Middlesex
University.
6. NED – Bristol City Council Holding
Company
7. NED – Forest Coachlines Pty Ltd
(Australia)
Jan 2016
01.08.15
01.08.15
01.08.15
01.09.15
06.06.16
01.10.2016
31/10/2016 31/10/2016
31/10/2016
31/10/2016
Mrs Karen Kneller 01.10.14 1. CEO of Criminal Cases Review Commission
2. Fee paid judge Social Entitlement Chamber
3. Fitness to Practise Member for General Dental Council
4. Director (unremunerated) of BRAP, an equalities think tank.
01.10.14
01.10.14
01.10.14 01.10.14

Miss Mehrunnisa Lalani 01/02.2017 1. Member – Doctors and Dentists Pay
Review Body (DDRB)
2. Lay Adjudicator/Member - British
Association of Counselling and
Psychotherapy
3. Director - Sara (Leicester) Ltd
Sept 2015
Jan 2015
Feb 2016
Mr Julian Miller 03.02.16 Director of Finance (non-voting) – University Hospitals Birmingham NHS Foundation Trust
03.02.16
Dame Julie Moore 26.10.2015 1. Birmingham Systems Ltd 2. Director of Innovating Global Health
China Ltd (registered in Hong Kong) 3. Member of Birmingham Business
School Advisory Board 4. Court of the University of Birmingham 5. Governor – Birmingham City University 6. Non-Executive Director – Precision
Medicine Catapult (PMC) 7. CEO – University Hospitals
Birmingham NHS Foundation Trust 8. Trustee – Prince of Wales Charitable
Foundation
26.10.15 26.10.15 26.10.15
26.10.15 26.10.15 26.10.15
26.10.15
Sept 16
Dr David Rosser 01.03.15 Medical Director – University Hospitals Birmingham NHS Foundation Trust
01.03.16
Prof Michael Sheppard 13.06.16 1. Chair – West Midlands Academic Health Sciences Network
2. NED – University Hospital Birmingham NHS FT
Octr 2013
Dec 2010
31 Jul 2016
Rt Hon Jacqui Smith 01.12.15 1. Chair – The Precious Trust
2. Chair – Public Affairs Practice for Westbourne Communications
3. Associate – Cumberledge Eden & Partners
4. Associate – Global Partners Governance
5. Chair – University Hospitals Birmingham NHS Foundation Trust
6. Trustee – The Kings Fund
01.12.15
01.12.15
01.12.15
01.12.15
01.12.15 01.02.17
30.03.2017

Council of Governors
Minutes of a meeting of the Council of Governors of Heart of England NHS Foundation Trust held
on 17 May 2017 at 4.00pm in the Education Centre, Birmingham Heartlands Hospital
PRESENT: Rt Hon. J Smith (Chair)
Mrs K Bell Mr A Cannon Mr K Fielding Mr A Fletcher Mr D Hoey Mrs S Hutchings Mr P Johnson Mrs V Morgan
Mr G Moynihan Mr B Orriss Mrs J Thomas Mr D Treadwell Dr M Trotter Mr D Wallis Mr T Webster
IN ATTENDANCE:
Ms F Alexander Mr K Bolger Mr J Brotherton Mr D Burbridge Mr A Edwards Mrs S Foster Mrs K Kneller
Miss M Lalani Mr J Miller Dame J Moore Dr D Rosser Prof M Sheppard Mrs C Walker (Minutes) Mrs H Wyton
17.039 WELCOME and APOLOGIES for ABSENCE
The Chair welcomed all to the meeting. Apologies for Governors were received from Mr Baldwin, Cllr Cotton, Mrs Doyle, Mrs Nicholl, Mrs Passey and Mrs Teall. Apologies for Directors were received from Prof Glasby, Mrs Hendley and Dr Kinski.
17.040 MINUTES OF PREVIOUS MEETINGS
The minutes of the meeting held on 27 March 2017 were approved as a true record.
17.041 MATTERS ARISING
17.019.1 – The Chair of HEFT’s Donated Funds Committee reiterated his support of the transfer of HEFT charitable funds and asked that proper consideration should be given to the governors when appointing future trustees. The interim Director of Communications assured that a skills analysis for future trustees would be undertaken. All trustees would be appointed independently by the charity. In addition, it was clarified that Brian Hanson, the Chair of UHB Charities Limited was not retiring. Rather, the Vice Chair would working with Mike Hammond, the Chief Executive of UHB Charities Limited, would be taking a more active role, especially in relation to the HEFT Charity.

P a g e | 2
The Chair asked the interim Medical Director to give an update on the cyber-attack and its effect at this Trust. He reported that the attack had been a virus was set to activate on a specific date. . HEFT currently had no 24 hour technical cover. Additional resources to respond to the incident had been provided by UHB. A great deal of work had taken place over the weekend and all systems were now patched. The Council of Governors formally recorded thanks to the interim Director of ICT and the IT Team for all their hard work, most of which had taken place over the weekend.
17.042 PERFORMANCE POSITION REPORT
The Council of Governors considered the update given by the interim Deputy Chief Executive – Improvement on the Trust’s performance against local and national indicators and targets. Performance against the A&E 4 hour wait target had improved in April but had deteriorated again in May. Increased attendances had been seen but the reason for the increase was unclear. Delayed transfers of care continued to contribute to pressures. The diagnostics and cancer targets had been achieved. There had been deterioration in performance against March’s ambulance handover data. A full review would take place to establish the reasons. A number of mixed sex breaches were reported, these had been as a result of capacity and flow issues on the sites. Focus would be placed on monitoring performance on dementia screening, a slight improvement had been seen in month but the Trust failed to meet the target. It was confirmed that the Trust had achieved the VTE assessment target and it was therefore not noted within the report. Targets were being achieved within workforce. Appraisals were above the contractual target and as a result the Trust had increased its own internal target. It was confirmed that the high level of compliance last year against information governance (IG) training was linked to an advice note distributed on pay slips. For 2017/18 IG training could also be completed by via Moodle, which can be assessed off-site. The update was received and no further questions were raised.
17.043 FINANCIAL POSITION REPORT
The interim Director of Finance gave an update on the current position and the agreed planned deficit of £7.5m for 2017/18 was in line with the control total. The Trust had reported an actual deficit of £4.3m against a plan of £2.4m in month 1 with the main components being healthcare income (£1.2m) below the seasonal plan and CIP slippage. The Trust’s cash balance was £23.3m and it was forecast that the Trust would not

P a g e | 3
need to access funding until September. In summary the Trust was £1.9m off plan, resulting in a difficult start to the financial year, with a need to focus on delivery of CIP to get back on track. The Chair opened the floor to questions and discussion. It was felt that the CIP target remained an uphill struggle and that last year had seen many quick wins. The meeting was assured of a good level of confidence in the delivery of CIP targets that included plans to cover the majority of schemes. The update was received and no further questions were raised.
17.044 PATERSON UPDATE
The Chair gave a verbal update on the Ian Paterson case and reported that, on Friday 28 April 2017, breast surgeon Paterson was found guilty of 17 counts of wounding with intent and providing procedures that were unjustified and not needed. He was due to be sentenced on Tuesday 30 May and a custodial sentence was expected. It was hoped that it would bring some closure to those treated. The Trust would continue to ensure that those affected were offered on-going care and support. The vast majority of NHS patients seeking compensation had received it. No private patients had yet been compensated. On 30 October 2017, the High Court would determine if the Trust had a legal duty of care to those patients cared for in the independent sector. Spire Healthcare was alleging that the Trust was responsible for Paterson’s private practice and that their role was to provide facilities from which doctors could practise. In recent weeks, the announcement from Secretary of State for Health had stated that, if the Conservatives remained in government, a full inquiry would be held. The focus of the new management team had been the care of his patients and, during 2016, work had continued to contact and support the 532 patients who had received the cleavage sparing mastectomy procedure. 201 patients had attended face-to-face reviews, many of those contacted had declined to attend. The Trust would continue to contact those who had not responded. The review was being written up by an independent panel and key findings would be shared with the Board and Council of Governors in June 2017. No omissions of care had been identified with patients who underwent wide local excision. The Trust intended to write to all 695 patients to offer reassurance and information of compliance with guidelines. The Trust would also continue to provide a venue and on-going support for the Breast Patient Support Group. In response to a question regarding ensuring similar issues did not happen in the future, assurance was given that processes were more robust and staff were able to report concerns and given support by the corporate teams. It was felt that the ‘softer cultural issues’ would minimise any future risk. The emphasis and processes in place would encourage people to report concerns eg at corporate induction for new staff that included nursing, administration and doctors, the Executive Team actively encouraged staff to report any concerns. In addition, it was confirmed that the ‘complete/full report’ referred to in a TV

P a g e | 4
Programme that was allegedly written by Dr Richard Brown did not exist, the organisation had conducted many searches, contacted the author and had contacted the Information Commissioner’s Office and had concluded that no such report existed. It was concluded that further information would be shared in June 2017 and that any remaining patients were given the opportunity for a review. The update was received and no further questions were raised.
17.045 HEFT / UHB JOINT WORKING GROUP OUTCOMES
The interim Director of Corporate Affairs gave an overview of the work of the HEFT/UHB Joint Working Group. A full report would be presented to the whole Council of Governors to consider the proposals for the combined CoG. The Joint Working Group (JWG) had, with the support of the Good Governance Institute, considered how it could take advantage of the opportunity to build a new CoG, what it would look like and what the gaps were with the Current CoG. It had considered how it could improve the important overarching trust wide body and ensure governors could have a focus and input into the services offered by the trusts that were important to them. The JWG had reviewed the constitution of the membership, including public and staff constituencies. HEFT did not have patient constituencies whereas UHB did. It had concluded that patient and public governor roles were the same. The membership constituency recommendations were presented. Statutory requirements stated that at least half of the public governors should be be elected and it was proposed that: • 1 public Governor per 5% of patient population (20)
– 3 for Rest of England & Wales – 3 for Solihull & Meriden – 14 other areas
• 6 Staff Governors – 2 nursing/midwifery – 2 Corporate & Support Services – 1 Medical – 1 AHP
• 3 Stakeholder – Local Authority – Birmingham City Council, Solihull MBC, Lichfield & Tamworth (joint)
• 1 Stakeholder – University of Birmingham • 1 Stakeholder – Birmingham City University • 1 Stakeholder – Ministry of Defence
This bought the overall size of the Council to 32 governors and would ensure that the CoG was a manageable size and based on local authority boundaries. The JWG had considered the working of the CoG. It was proposed that there would be 6 formal meetings in a year and up to 6 seminars. There would be two meetings per year where Governors had the opportunity to hold NEDs to account. There would be a number of sub groups including hospital level environment and patient, care quality group and community panels. The Chair opened the floor to questions.

P a g e | 5
All governors needed to be made aware of their commitment to attend and that attendance would be recorded and non-attendance dealt with. There was a discussion on the change to some of the boundaries and the impact for governor representation and it was confirmed that the JWG had spent considerable time discussing how it would work. In response to a suggestion, the Chair agreed to consider a proposal that the Lead Governor was invited to attend and contribute to a public Board meeting. There were no fundamental issues with constituency and governor representation proposals. There was a discussion on the process to be followed for existing HEFT governors following the acquisition. The JWG would be considering this transaction in a subsequent meeting. The Chair thanked everyone who had been involved with the Joint Working Group. Resolved: The CoG agreed to the proposals set out within the presentation.
17.046 CHAIR OF COG SUB-GROUP REPORTS
17.046.1
Hospital Environment Group Mrs Hutchings, Chair, gave an update on the Hospital Environment Group. It was reported that a visit and taste test had taken place at the CPU which provided patient meals, being one of very few Trusts that provide its own food it was felt that the Trust should be very proud of the quality of food it produced. It was confirmed that the CPU did have the capacity to also provide provisions for UHB.
17.046.2
Membership and Community Engagement Group Mr Fletcher, Chair, reported on the recent meeting of the Membership & Community Engagement Group. All governors were encouraged to engage with members and the group had considered different ways of facilitating this. The monthly membership health seminars continued to be well attended. Resolved :the update was received and no questions were raised.
17.046.3 Patient Experience Group Mr Cannon, Chair, reported that there had been two meetings held this year. The minutes had not been included in the pack as they had not been approved, once approved they would be circulated. The group had refocused and considered its future work programme. In addition, the group had felt that chairs of the PCP’s should be invited to attend future meetings in order to develop links and form new ways of working. The chairs would not become members of the group. Resolved – the update was received and no questions were raised.

P a g e | 6
17.047 ANY OTHER BUSINESS
Feedback on the recent quality of the recent International Nurse Day event was received and would be passed on to the Chief Nurse.
17.048 DATE OF THE NEXT MEETING
The next meeting (Focus) was scheduled for Monday 26 June 2017 in the Harry
Hollier Lecture Theatre, Partnership Learning Centre, Good Hope Hospital
There being no further business the meeting closed.
...................................... Chair

Council of Governors
Minutes of a meeting of the
Council of Governors of Heart of England NHS Foundation Trust held on 26 June 2017 at 4.00pm
in Room 2, Education Centre, Birmingham Heartlands Hospital
PRESENT: Rt Hon. J Smith (Chair) Mr S Baldwin Mrs K Bell Mr J Cotton Ms S Edwards Mr K Fielding Mr A Fletcher Mr D Hoey Mrs S Hutchings Mr G Moynihan
Mr B Orriss Mrs L Passey Mrs J Thomas Mr D Treadwell Dr M Trotter Mr D Wallis Mr T Webster Mr L Williams
IN ATTENDANCE:
Mrs F Alexander Mr A Bostock, KPMG Mr D Burbridge Mr A Edwards Mrs Hendley Mrs A Hudson (Minutes) Mrs K Kneller
Miss M Lalani Mr J Miller Dame J Moore Mr T Tandy, KPMG Mrs H Wyton
Member of the Public
17.049 WELCOME and APOLOGIES for ABSENCE
Apologies for Governors had been received from Mr A Cannon, Mr P Johnson, Mrs McGeever, Mrs Morgan and Mrs Nicholl. Apologies for Directors had been received from Prof Glasby and Dr Kinski. The Chair began the meeting by congratulating David Treadwell on his recent award of an MBE in the Queen’s Birthday Honours List, for voluntary service to the community in Acocks Green. Mr Treadwell thanked the Chair and members of the CoG for all the kind words and congratulations he had received.
17.050 MINUTES OF PREVIOUS MEETINGS
24 April 2017
The minutes of the meeting held on 24 April 2017 were considered and approved
as a true record.
17.051 MATTERS ARISING
There were none

P a g e | 2
17.052 CHAIRS REPORT
The Chair reported that the private meeting of the Board of Directors, held earlier that day, had discussed and approved the submission of the full business case to NHSI. The pre-notification document had been submitted to the CMA in April and they had now confirmed that they had received all the information they required to review the case. Phase one of the review would commence on 3 July and would take up to 40 days after which the CMA would give a decision as to whether the proposed acquisition had been cleared. The NHSI review process would take 2 – 3 months from the submission of the business case after which it would advise the Trust of the risk rating for the transaction, which was RAG rated. The Trust would be holding stakeholder events with councillors, MPs, Healthwatch and other organisations at the end of July in order to brief them on the progress. A Seminar had been arranged for Governors to go through the full business case on the 4 August. The Chair reported on the recent press release about the changes to maternity services at Good Hope Hospital. In order to provide the safest possible treatment for mothers and babies, all elective C-sections would now be undertaken on the Heartlands site. The decision had been taken following recent changes in staffing levels following resignations and recruitment issues. There were no plans for any further changes to the maternity provision at Good Hope. In response to an observation from the Lead Governor, that the story had been as a result of contact from a member of staff, the interim Deputy CEO –Improvement reported that staff had been made aware that the changes to the service were as a result of unsafe staffing levels and the decision had been in response to issues raised by staff at Good Hope. It was reported that the Trust had received the first draft of the CCG report and had been invited to comment upon the factual accuracy. The report had not contained any content that had not been previously shared immediately following the visit. The Chair had recently attended the 3rd Annual Carers Conference held at the Renewal Centre in Solihull. The event had been a very positive event. The Chair had recently invited and met with Birmingham Councillors in order to give an update on a range of issues that included the proposed ACAD work. Of the 30 councillors invited 7 had accepted. Meetings with councillors for Sutton, South Staffordshire and Solihull constituencies were also being arranged.
17.053 PERFORMANCE & FINANCIAL POSITION REPORT
17.053.1
Performance The Council of Governors considered the update given by the interim Deputy Chief Executive – Improvement, on the Trust’s performance. NHS Improvement

P a g e | 3
(NHSI) had introduced a Single Oversight Framework (SOF) which had replaced the Risk Assessment Framework (RAF). The framework looked at 5 themes and a set of measures and triggers which determined the level of support required. Of the 5 indicators in the Single Oversight Framework, 4 were on target. Performance for the A&E 4 hour wait target had deteriorated in May to 83.2% compared to April at 86.73%. The 18 week Referral to Treatment incomplete pathway performance had been achieved in May at 92.67%. The Trust had met the unvalidated 62 day cancer target in May. There had been three patients that had their operations cancelled twice in May and one patient had been cancelled three times. Following a meeting with the Division, a process had been put in place to ensure appropriate escalation of such cases. A total of 491 patients waited over 30 minutes and 6 had waited over 60 minutes for ambulance handover. This was deterioration against April’s performance. The Trust was working with the ambulance service to review and validate data. The Trust had failed to meet the DTOC target in May. The Trust was working with UHB to ensure there was a consistent process in place for measuring DTOC performance. It appeared unlikely that the position would improve in June as Birmingham City Council had advised that it had temporality suspended any referrals that required enhanced assessment beds. Performance against dementia screening had deteriorated in month. Meetings had been held with the Divisions setting out expectations for the delivery of the indictor. Revised targets for appraisals, time to hire and exit interviews had been introduced. Voluntary turnover had shown an increase for a number of months with the biggest increase seen in corporate service. The Trust was focussing on new strategies for retention. There had been one Never Event in May relating to a drug administration error in a non-cancer patient at GHH. An investigation was underway. The Chair opened the floor to questions from Governors. In response to a question about recruitment, the Chief Nurse advised that recruitment had remained static as the Trust was seeing as many leavers as starters. Work to improve retention was underway. The Trust had held several open days. The University of Birmingham had increased the number of nursing places it offered. In response to a question regarding the breakdown between the number of long term and short term sickness rates, the Director of Workforce reported that long term sickness was activated after a period of 3 weeks. The Trust had several initiatives in place to keep people at work, including the availability of information on well-being through trust wide communications and Team briefs. Resolved: the report was received.

P a g e | 4
17.053.2
2
Finance The Committee considered the paper presented by the interim Director of Finance and noted the agreed planned deficit of (£7.5m) for 2017/18 was in line with the control total. The plan included £21.3m of STF income subject to financial performance. The Trust had reported an actual deficit of £4.5m against a plan of £2.4m in month 2 with the main components being healthcare income (£4.0m) below the seasonal plan and CIP slippage. A full report would be presented to the next meeting. The Trust’s cash balance was £19.7m against a plan of £13.5m a favourable movement of £6.2m. The Chair invited questions. With regard to how the Trust monitored furniture and equipment it loaned out to patients, the Deputy CEO advised that Community Services were responsible for all community based equipment eg commodes, beds etc. Patients who were lent equipment, such as walking sticks and crutches, were encouraged to return them when they were no longer required. The Trust often held equipment amnesty days in order to encourage members of the public to return unwanted items. Patients were also required to sign for expensive items of equipment which were loaned out. The interim Director of Finance advised that further discretionary spend restrictions had been put in place on such items as stationery, magazine subscriptions, hospitality etc. The Trust also sourced products for the best possible price. The Chair reported that, following a request by a Governor as to whether Governors could to have access to the HSJ, enquiries had been made and the cost of an annual subscription would be circa £3,000. Given the discretionary restrictions in place this would not be possible. In response to a question, the interim CEO advised that UHB were on plan at month one. Resolved: the report was received.
17.054 EXTERNAL AUDIT REPORT ON GOVERNOR QUALITY ACCOUNTS
INDICATORS
Mr Bostock, Partner at KPMG, the Trust’s External Auditors, presented an overview of the role of external audit. As part of the Quality Account audit process, the auditors were required to test two mandated indicators, as per national guidance, and a locally selected indicator chosen by the CoG – ‘Stat Dose of Prescribed Antibiotics Administered Within An Hour’. The approach followed was to confirm the definition and guidance used by the trust to calculator the indicator and then document and walk through the Trust systems used to produce the indicator and undertake testing on the underlying data against six specified data quality dimensions. The work on the indicator revealed that the External Auditors had been unable to issue a clean limited assurance opinion on the presentation and recording of this.

P a g e | 5
The audit was able to successfully reconcile the data reported directly back to raw downloaded date from the e-prescribing system but it struggled to gain evidence of cases where the prescribed and administered times were the same. This was due to no documentation or explanations within the system for such scenarios. The Audit of the Quality Report also considered the content to ensure it addresses the requirements as set out by NHSI. The Trust had achieved a clean limited assurance opinion on the content of the Quality Report, that it was accurately reported and in line with regulations set out by NHSI.
The Chair invited questions.
In response to a question around ambulance handover, Mr Bostock reported that, the Trust started the clock for ambulance arrivals from when the arrival was registered and did not refer to the ambulance arrival time, as per national guidance. The Trust Board had previously agreed this practice as it was considered to be in the best interest of patients. Resolved: the report was received.
17.055 COG SUB-GROUP REPORTS
17.055.1
17.055.2
The chairs of the Sub-Groups gave a verbal update on the discussions held at recent meetings and the final minutes for the meetings were received. Hospital Environment Group (SH) The Chair reported that the group had met on 25 May 2017 and had received an update on the site strategy, including the phasing of works around ACAD. Phase 1 of the ACAD was underway. The meeting had discussed patient and visitor bedside phone charges and the PCP’s had agreed to include a question on phone charges on visit questionnaires. The state of some of the guttering on estate buildings had been discussed and a report was to be presented to the next meeting. In response to a question, the Vice-chair confirmed that feedback from PLACE visits would be received. The approved minutes for the meeting held on 30 March 2017 were received. Membership and Community Engagement Group (AF)
The Chair reported that the group had met on19 May 2017 and had agreed the schedule for the Governor Drop-in Sessions that were being held to give members of the public the chance to meet with local governors, with a view to increasing membership. All Governors were encouraged to take part. Briefings, FAQ and leaflets were being produced and would be circulated. The recent membership seminar was given by Dr Mark Gannon had been excellent and well attended and a video was available on the Trust website. The approved minutes for the meeting held on 17 February 2017 were received.

P a g e | 6
17.055.3.
Patient Experience Group (TC) The Vice-chair reported that the group had met on 19 May 2017. The aims of the group had been reviewed and it had been agreed to put in place KPIs for the Group to measure their performance against. A sub-group had been formed to look at how the Trust supported vulnerable patient groups. There was a discussion on the protocols in place to record how vulnerable patients were fed. It was reported that any issues would form part of staff handover meetings. Information was available on the Trust website and it was important that the guidance was followed. The approved minutes for the meeting held on 20 January and 17 March 2017 were received. Resolved: The reports were received.
17.056 ANY OTHER BUSINESS
The interim CEO reported that, following the Grenfell Tower fire tragedy, all trusts had been contacted by NHSI in order to complete a questionnaire detailing the state of its buildings. Late on 24 June, a further email had been received that advised that the estate had to be inspected by the Fire Service by the end of the 25 June. The Trust in partnership with the Fire Service undertook an annual fire service review of the estate which included all sites. The Chief Fire Officer for Birmingham had convened a meeting for later that week to look at the programme for any additional works across the Birmingham area that may be required. The Trust AGM would take place in September. The date would be advertised once it had been agreed. Paterson. There was a discussion on the latest position and the Chair reported that a high court judge was to consider where responsibility for Duty of Care lay - the NHS or the private sector. No terms of reference had yet been set for the Secretary of State’s Enquiry into Paterson. It was the responsibility of the government to determine whether the enquiry was public or not. It was agreed to have a focus meeting to discuss Recruitment and Staff Retention. In response to a request, it was agreed to receive an update on the proposed Charity Panel membership to the next meeting.
17.057 DATE OF THE NEXT MEETING
The next meeting (focus) was scheduled for 24 July 2017, to be held in Rooms 2
and 3, the Education Centre, Birmingham Heartlands Hospital
......................................
Chair

HEART OF ENGLAND NHS FOUNDATION TRUST
COUNCIL OF GOVERNORS
MONDAY 24 JULY 2017
Title: Performance Indicators Report
Responsible Director
:
Kevin Bolger – Interim Deputy CEO - Improvement
Contact Kevin Bolger, Interim Deputy CEO – Improvement
Purpose To update the Council of Governors on the Trust’s performance against targets and indicators in the Single Oversight Framework, contractual targets and internal targets
Confidentiality Level & Reason
Annual Plan Ref
Not applicable
Key Issues Summary:
Exception reports have been provided where there are current or future risks to performance for targets and indicators included in the Single Oversight, national and contractual targets and internal indicators. A&E 4 hour performance remains a risk for the Trust.
Recommendations The Council of Governors is requested to: Accept the report on progress made towards achieving performance targets and associated actions and risks.

Page 2 of 14
HEART OF ENGLAND NHS FOUNDATION TRUST
COUNCIL OF GOVERNORS
MONDAY 24 JULY 2017
PERFORMANCE INDICATORS REPORT PRESENTED BY THE INTERIM DEPUTY CEO - IMPROVEMENT
1. Purpose
This paper summarises the Trust’s performance against national indicators and targets, including those in the NHSI Single Oversight Framework 6, as well as local priorities. Material risks to the Trust’s Provider Licence, reputation or clinical quality resulting from performance against indicators are detailed below.
2. HEFT Performance Framework
The Trust has a suite of Key Performance Indicators that includes national targets set by NHS Improvement and the Department of Health (DH) and local indicators selected by the Trust as priority areas, some of which are jointly agreed with the Trust’s commissioners. This report is intended to give a view of overall performance of the organisation in a concise format and highlight key risks particularly around national and contractual targets.
3. Material Risks
The DH sets out a number of national targets for the NHS each year which are priorities to improve quality and access to healthcare. NHS Improvement (NHSI) tracks the Trust’s performance against a subset of these targets, enabling Trusts to access the Sustainability and Transformation Fund as long as agreed trajectories are achieved. Table 1: Performance against National Contractual Requirements
Indicator Threshold Current
Data Period
Performance
Single Oversight Framework
18 week RTT - incomplete 92% June 92.34%
A&E 4 hour access 95% June 83.54%
Cancer 62 day - GP urgent referral 85% May 86.1%
Cancer 62 day - national screening 90% May 100.0%
6 weeks diagnostic test 99% June 99.22%

Page 3 of 14
Indicator Threshold Current
Data Period
Performance
Other National Targets
Cancer 2 week 93% May 94.9%
Cancer breast - 2 week 93% May 93.2%
Cancer 31 days- first treatment 96% May 98.7%
Cancer 31 days- subsequent treatment -surgery
94% May 97.8%
Cancer 31 days - subsequent treatment - drugs
98% May 100%
Ambulance Handover > 30 minutes >0 June 156
Ambulance Handover > 60 minutes >0 June 6
12 hour Trolley waits A&E 0 June 0
52 week waits 0 June 0
Cancelled Ops rearranged 28 days 0 June 0
Urgent operation cancelled x2 0 June 0
Sleeping Accommodation Breach 0 June 0
MRSA 0 June 0
C.difficile - (post 48 hours)) 6 June 5
VTE risk assessment 95% June 97.32%
Duty of Candour (2 months in arrears) 0 April 0
NHS Number acute 99% June 99.64%
NHS Number A&E 95% June 98.43%
3.1 Single Oversight Framework
3.1.1 A&E 4 Hour Waits
Performance for the A&E 4 hour wait target was slightly improved in June at 83.54 % compared with 83.3% in May. Table 2: A&E Performance by Site June 2017
Site Performance Attendances Daily Av
Heartlands 83.23% 11,550 385
Good Hope 76.13% 7,410 247
Solihull 99.27% 3,715 124
Trust 83.54% 22,675 756
Table 3: A&E Performance by Site June 2016
Site Performance Attendances Daily Av
Heartlands 83.61% 11,368 379
Good Hope 90.70% 7,451 248
Solihull 98.50% 3,669 122
Trust 88.39% 22,488 750

Page 4 of 14
There were 22,675 attendances in June 2017 (an average of 756 patients per day). This compares to 22,488 attendances in June 2016 (an average of 750 patients per day). The data demonstrates the decline in performance is predominantly at the Good Hope Hospital site.
3.1.2 18 Week Referral to Treatment (Incomplete Pathways)
Incomplete pathway performance was achieved at aggregate level in June with a performance of 92.34%. The only specialty failing to meet the target in month was Trauma and Orthopaedics who achieved 85.88%. Within the category “other” a number of specialties have failed to meet the target, where applicable this performance was discussed at the Divisional Review meetings and rectification plans are being developed Table 4: 18 week RTT performance – category “other”
Specialty Description Apr May Jun
Breast Surgery 81.52% 85.85% 83.52%
Colorectal Surgery 83.33% 95.59% 91.21%
Interventional Radiology
76.40% 83.43% 88.37%
Pain Relief 90.32% 92.46% 90.62%
Upper GI Surgery 64.55% 65.95% 61.90%
Trauma and Orthopaedics -. A business case is being developed to recruit an additional upper limb consultant to address capacity issues in the longer term and, in the interim, a locum has been brought in. The service has also implemented learned procedure times for elective lists and is working with booking staff to ensure these are fully implemented. Increased demand on trauma has had a knock-on effect on theatre capacity and outpatient activity and the service is in the process of developing a plan for virtual fracture clinics in order to alleviate demand pressure in this area. IR – There remain significant workforce shortages in Interventional Radiology, the service saw an overall RRT improvement of 5% in June. Additional sessions are being put in place with the existing consultants to cover the position in the short term.
Pain Relief – Additional clinics have been put in place to improve the position.

Page 5 of 14
Breast – The service is exploring extended theatre capacity subject to adequate theatre staffing for a three session day.
Colorectal – Performance deteriorated due to cancellations, plans are in place to ensure that future cancellations are dated within month.
Upper GI – Underperformance predominantly relates to the admitted pathway, with gallbladder surgery being the main driver for the current position. Pathway work is being undertaken to scope a ‘hot’ gall bladder service and the service is also exploring weekend day case capacity for gall bladders, which will improve the position, whilst the pathway work is being progressed.
3.1.3 62 day cancer
The Trust met both the 62 day cancer targets (referral from GP and referral from screening service) achieving 86.10% and 100%, respectively, in May. The unvalidated June position shows that these indicators should be met in month.
3.1.4. Cancer Long Waits – Latest Guidance
A letter from NHSI and NHSE Midlands and East was sent to Trusts and CCGs in May 2017 regarding public reporting and quality review of cancer long waits. It set out two national objectives to increase the number of providers delivering the 85% cancer 62 day standard to over 70% and for all Trusts to achieve the standard from September 2017. In addition the following action is required of Trusts and CCGs by end of June 2017.
Routinely report the number of <62 day and <104 day breaches, plus outcomes and learning from RCAs to Public Board meetings.
Routinely report themes, outcomes and learning from long waits to local quality steering groups.
Local quality steering groups to agree further action and escalation to regional quality steering groups.
Develop a plan, for improving monthly trajectory to clear long waits where there are patients waiting over 104 days.
As at 30th June, the Trust had 3 patients over 104 days on a cancer pathway. The reasons for their extended wait were as follows; 1 x Lung (compliance issues with patient cancelling and failing to attend for multiple appointments and requesting surgery in July), 2 x Urology (1 patient incurring diagnostics delay of over two months at UCHW, 1 patient with complex treatment plan between Endocrinology, Cardiology and Urology).

Page 6 of 14
This compares to May where the Trust treated 3.5 cases for patients waiting > 104 days (the 0.5 shared breach was a late referral from Walsall to HEFT at day 128).
3.1.5 % patients waiting 6 weeks for 15 key diagnostic tests
The Trust has provisionally met the target in June with un-validated performance at 99.2% against the 99% target.
3.2 National Targets Monitored Locally Through CCG Contract
Of the 18 national targets that are not included as Operational Performance Metrics in the new Single Oversight Framework but are included in the CCG contract the Trust is on target for 16.
3.2.1 C.difficile
There have been 5 cases of post 48 hour toxin positive Clostridium difficile cases in the Trust during June 2017 which falls within the monthly trajectory of 6 cases per month. The total number of post 48 hour C.diff cases for the year is 10 compared to the trajectory 64 cases.
3.2.2 Ambulance Handover
The Trust met the CCG target of 95% of patients waiting less than 30 mins (97.19%) and 60 mins (99.91%) in month. There were 156 patients who waited over 30 minutes and 6 patients who waited over 60 mins for ambulance handover. This performance is a significant improvement on May, as is shown in the table below, however Good Hope remains the poorest performer against this indicator. The Trust has implemented a new agreed joint validation process for ambulance delays which has been in operation since late May. This has been supported by dedicated HALO presence on all three sites, combined with a daily validation process between the Trust and WMAS. Division 3 will analyse confirmed breach data to identify themes and any associated action requirements. Table 5: Ambulance handover 30 minute breaches by site
Site Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17
BHH 141 253 116 99 173 237 61
GHH 223 295 200 200 185 233 92
SH 15 14 5 7 16 21 3
Trust 379 562 321 306 374 491 156

Page 7 of 14
4. Local Indicators – acute contract
There are 67 local contractual indicators that the Trust’s performance is measured against (31 are reported monthly, 32 of these are reported quarterly and the others either bi-annually or bi-monthly).
4.1 Delayed Transfers of Care (DTOC) for health and joint delays
The Trust failed to meet this target in month, achieving 2.70% against a target of 1.4%, performance by site and patient numbers waiting are shown in the tables below.
Table 6: DTOC HEFT and external NHS joint health delays
Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17
BHH 2.00% 1.78% 2.36% 2.64% 2.48% 2.73% 2.80%
GHH 0.29% 0.70% 0.85% 0.94% 0.80% 1.02% 1.95%
SH 2.78% 1.99% 1.62% 4.11% 4.72% 3.20% 4.03%
TRUST 1.58% 1.50% 1.77% 2.29% 2.27% 2.24% 2.70%
Table 7: DTOC HEFT and external NHS joint health delays – bed days occupied
Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17
BHH 474 422 506 627 538 613 608
GHH 42 101 111 136 108 142 263
SH 169 121 89 250 293 205 250
TRUST 685 644 706 1013 939 960 1121
The tables below show performance for all delayed transfers of care and actual numbers i.e. those that are health and social delays. Table 8: All DTOC delays
Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17
Jun-17
BHH 4.35% 3.93% 4.02% 4.76% 4.05% 4.14% 6.01%
GHH 1.63% 2.20% 3.21% 2.66% 3.20% 3.06% 5.20%
SH 4.08% 5.31% 6.33% 6.61% 8.18% 8.19% 8.43%
TRUST 3.53% 3.56% 3.94% 3.68% 4.39% 4.39% 6.11%
Table 9: All DTOC delays - bed days occupied
Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17
Jun-17
BHH 1032 932 861 1129 879 930 1306
GHH 236 318 419 384 433 427 703

Page 8 of 14
SH 248 323 348 402 508 525 523
TRUST 1516 1573 1628 1915 1820 1882 2532
4.2 Compliance with Nursing Care Indicators - Tissue Viability metric
(Repositioning frequency adhered to 3 days) Performance against this indicator remains below target at 89% in
June, just below the 90%. Further information on this can be found in the Care Quality Report.
4.3 Pressure Ulcer Reduction
The Trust had no patients with a grade 4 pressure ulcer in this quarter and 3 patients with grade 3 pressure ulcers (2 in April, 1 in May and 0 in June). The target is zero tolerance for grade 4 pressure ulcers and an annual target of 36 grade 3 pressure ulcers. Year to date we have had 0 grade 4 and 3 grade 3 pressure ulcers. Further detail can be found in the Care Quality Report.
4.4 Quarterly Maternity Screening Indicators
There are 14 maternity screening indicators, all reported a quarter in arrears, and therefore the current performance reported this quarter relates to Q4 (2016/17). Of the 14 indicators, the Trust has failed to meet 4, with final validated results for one metric outstanding. These are:
Proportion of laboratory request forms submitted to 10+0 to 20+0 weeks gestation
Proportion of babies requiring repeat blood sample due to an avoidable failure in the sampling process
Proportion of referred babies receiving hearing assessment in 4 weeks of decision that assessment is required by 44 weeks gestational age
Proportion of babies who, as a result of possible hip abnormality detected at the new-born physical examination, have ultrasound assessment within 2 weeks of birth.
These 4 indicators are reported through a combination of Birmingham Women’s and Children’s Hospital, Sandwell and West Birmingham NHS Trust and national (NIPE) systems quarterly in arrears, which makes management of performance a challenge as performance data is always out of date.
The Head of Operations for Division 2 is meeting with BCWH, SWBT and the national ‘NIPE’ system representatives in an effort to move to monthly reporting.

Page 9 of 14
Whilst these discussions are underway the division are working on internal mechanisms to identify current performance in month where possible, all performance data is discussed with the relevant directorate management teams at their monthly confirm and challenge meetings with the Divisional Director and Head of Operations, with actions are tracked at the weekly management team meeting.
4.5 Medicines Management (1b) Reducing inappropriate use of piperacillin with tazobactam (“piptaz”) - 70 % have stop date/specified duration
This is a bi-annual metric with a target to have achieved 70% by March 2018. March 17 performance was 76.7%. Q1 and Q2 will be reported at the December Board.
4.6 Medicines Management (4) The number of discharges that include medication changes and explanations for changes or state “no change” where appropriate. This is a bi-annual metric with a target of 90%. Year-end position for 2016/17 was 88.9%
4.7 Stroke: 80% of patients spending ≥90% of their stay on a stroke unit The Trust has met this target in May achieving 86.9% against an 80% target.
4.8 TIA – proportion of patients who present at A&E and are discharged with a TIA that are scanned and treated within 24 hours – target 60% The Trust has failed the target in May at 45.0% within 24 hours. This is the first time this indicator has not been met in 12 months. The service has reported that 90% were within 30 hours and initial review of breach reasons has identified some delays with access to CT scanning and discharge process from Hyper Acute Stroke Unit. Improved identification of patients arriving in ED and captured in MMS is being reviewed as previous performance has been consistent.
5. Local Indicators – community contract
The Trust has a number of community contracts, many of the indicators against these contracts are reported quarterly. In Q4 2016/17 the designated doctor KPI was not met at 82.29% (target 85%). However, Q1 2017/18 has seen the indicator achieved at 91.67%. All other indicators in this contract have been met.

Page 10 of 14
6. Internal Indicators – Performance
6.1 Dementia Screening
The Trust’s performance against the dementia screening ‘FIND’ element of this metric has improved from May’s position (86.98%) to 88.03% in June, but still failing to meet the 90% target, as shown in the table below. Actions to improve the Trust position were discussed at the Performance Review meeting for Divisions 3 and 5 in June 2017.
Table 10: Dementia Screening Performance ytd
Table 11: Dementia Screening Performance by Division
Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17
Div 1 100.00% 100.00% 66.67% 100.00% 90.19% 100.00%
Div 2 N/A N/A N/A 500.00% N/A 100.00%
Div 3 86.61% 91.31% 88.90% 89.97% 87.36% 88.48%
Div 4 87.37% 92.94% 93.67% 88.79% 92.11% 94.12%
Div 5 76.86% 77.47% 79.64% 86.73% 82.38% 82.55%
TRUST 85.36% 89.64% 87.93% 89.31% 86.98% 88.03%
6.2 Information Governance Training
Performance against the Information Governance Mandatory Training target of 95% has continued to improve in month, with performance at 83.38% in June. Table12: Information Governance Training - Cumulative performance
85.36%
89.64%
87.93% 88.42%
86.98%
88.03%
Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17

Page 11 of 14
Division Mar-17 Apr-17 May-17 Jun-17
Corporate 83.1% 86.2% 84.9% 87.5%
Facilities 63.7% 72.3% 84.1% 87.7%
Education Services 92.9% 93.3% 94.0% 93.2%
Research Management 95.7% 97.9% 93.5% 93.5%
Division 1 84.1% 85.8% 88.1% 89.7%
Division 2 74.9% 75.5% 77.6% 81.6%
Division 3 72.8% 74.9% 78.6% 80.2%
Division 4 74.8% 78.0% 79.7% 82.8%
Division 5 64.5% 67.9% 70.7% 72.9%
Trustwide 75.44% 78.13% 80.9% 83.38%
7. Local Indicators - Workforce
7.1 Mandatory Training
Mandatory Training performance remains above target at 92.05% for June.
7.2 Appraisal
Appraisal completion rates continue to remain above target at 88.55% for June.
7.3 Recruitment
Time to Hire (recruitment) performance is now 6.57 weeks against a target of 6 weeks.
7.4 Voluntary Turnover
Retention of staff remains a key workforce objective with Trust turnover rates now at 11% which is an increase from 10.98% last month. On-line exit interview completion rates and reasons for leaving are expected to improve with our use of a new exit interview monitoring tool.
The table below shows the trend for 2017. Table 13 : – Voluntary Turnover 2017

Page 12 of 14
The new on line exit monitoring tool is set to launch in July as part of a trial in conjunction with our partner the Pickers institute, who also administer the national staff survey on our behalf. In the meantime our existing exit monitoring arrangements have been prioritised and performance has risen in the last few months to over 35% from circa 11%, so intelligence on why staff leave the Trust is improving. Targets have been set for completion rates on exit interviews which rise throughout the year and are reported through Divisional performance reviews.
7.5 Sickness Absence
Sickness absence rates have increased very slightly in May to 4.31% in month and to 4.36% moving annual average against a target of 4.00%. This is compared to 4.00% (in month) and 4.31% (moving annual average) at the same point last year.
8. CQUIN Update Quarter 4 2016-17
With the exception of the CQUINs reference 2a & 2b, Timely identification and treatment for Sepsis in emergency departments and inpatient settings, the Trust fully achieved all CQUIN milestones in quarter 4 for the Acute, Specialised Services and Public Health Contracts. The target for both emergency and inpatient sepsis screening was 90%. The Trust out turned at 56% and 56.8% respectively. A partial payment of 5% of the maximum 25% available was achieved for the quarter.

Page 13 of 14
9. Recommendations
The Council of Governors is requested to: 10.1 Receive the report on progress made towards achieving performance
targets and associated actions and risks. Kevin Bolger Interim Deputy Chief Executive - Improvement

Page 14 of 14
Appendix 1
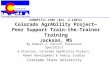
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
86.62% 83.21% 83.54%
90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 95.00%
4 Hour Performance
STF Trajectory
Emergency DepartmentSustainability and Transformation Fund (STF)
2017/18
Quarter 1 Quarter 2 Quarter 3 Quarter 4
86.62%
83.21% 83.54%
76%
78%
80%
82%
84%
86%
88%
90%
92%
94%
96%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% 4
Ho
ur
Pe
rfo
rman
ce
4 Hour Performance STF Trajectory

1
HEART OF ENGLAND NHS FOUNDATION TRUST
COUNCIL OF GOVERNORS
MONDAY 24th JULY 2017
Title: Clinical Quality Monitoring Report
Responsible
Director :
Dr David Rosser, Interim Executive Medical Director
Contact Amy Fowlie, Project Assistant
Mariola Smallman, Head of Quality Management
Purpose To provide assurance on clinical quality to the Council of Governors and detail the actions being taken following the Joint Clinical Quality Monitoring Group (JCQMG) 28th June 2017 and the HEFT Clinical Quality Monitoring Group (CQMG) 4th July 2017.
Confidentiality
Level & Reason
N/a
Annual Plan Ref
N/a
Key Issues
Summary:
The Council of Governors will consider:
Investigations into Doctors’ performance currently underway
Mortality indicators: CUSUM, SHMI, CRAB and HSMR
Board of Directors’ Unannounced Governance Visits
Recommendations The Council of Governors is asked to receive the information set out in this report and accept the actions identified.
Approved by: Dr David Rosser, Interim Executive Medical
Director
13th July 2017

2
1. Introduction
1.1 The aim of this paper is to provide assurance on clinical quality to the Board of
Directors, detailing the actions being taken following the JCQMG and CQMG meetings. The Council of Governors is requested to discuss the contents of this report and accept the actions identified.
2. Update On Medical Staff Within The Remit Of Maintaining High Professional
Standards (MHPS) 2.1 There are currently six Doctors subject to MHPS investigation. The investigations
relate to four Consultant Grade Doctors and two specialty doctors. One doctor has
been excluded and two of these doctors have restrictions placed on their
practice. Since the last report the employment contract of one Doctor has been
terminated.
3. Mortality – CUSUM
3.1 Mortality is reviewed in a number of ways including the ‘CUSUM’ (cumulative sum) Hospital Standardised Mortality Ratio (HSMR) methodology which is used by the Care Quality Commission (CQC).
3.2 Two CCS (Clinical Classification System) had higher than expected mortalities and
was a potential mortality threshold trigger in March 2017: ‘Cardiac arrest and ventricular fibrillation (107)’ and ‘Other gastrointestinal disorders (155)’.
3.3 The case lists for the CCS groups were reviewed at the JCQMG 28th June 2017 and the CQMG 4th July 2017. The case lists have been sent to Clive Ryder, Deputy Medical Director who will report any concerns to the JCQMG and CQMG. Please see Figure 1 on the next page.

3
Figure 1: HEFT CUSUM in March 2017 for HSMR CCS Groups

4
3.4 The Trust’s overall mortality rate as measured by the CUSUM for March 2017 is within acceptable limits as shown in Figure 2 below.
Figure 2: HEFT CUSUM in March 2017 at Trust level1
1 University Hospitals Birmingham NHS Foundation Trust (UHB) CUSUM data has been included to enable
benchmarking.

5
4. Mortality – SHMI (Summary Hospital-Level Mortality Indicator)
4.1 The Trust’s SHMI performance for April 2016 to February 2017 was 96.72. The Trust has had 4,132 deaths compared with 4,272 expected. The Trust is within the acceptable limits as shown in Figure 3 below.
Figure 3: HEFT SHMI April 2016 to February 20172
2 UHB SHMI data has been included to enable benchmarking.

6
5. Mortality – HSMR (Hospital Standardised Mortality Radio)
5.1 The Trust’s HSMR for the period April 2016 to March 2017 was 95.85 which is within acceptable limits. The Trust had 2,690 deaths compared with 2803 expected (see Figure 4 below).
Figure 4: HEFT HSMR April 2016 to March 20173
3 UHB HSMR data has been included to enable benchmarking.

7
6. CRAB (Copeland Risk Adjusted Barometer) surgical 30 day risk adjusted mortality
ratio to October 2016. 6.1 The Trust’s CRAB 30 day surgical mortality O/E (outcome versus expected) ratio is
within the normal range and either below or equal to the average of 1 (see Figure 5 below).
Figure 5: CRAB 30 day surgical mortality O/E ratio April 2017
7. Board of Directors’ Unannounced Governance Visits
7.1 Ward 3 (Renal) at Birmingham Heartlands Hospital was visited 20th June 2017.
Patients and relatives expressed some concerns around discharge plans and
hygiene. The visit was largely positive from a staff perspective and the visit team
noted the positive culture on the ward. A number of the ward staff are long serving
and agency has not been used in 2017. The Divisional Management Team are
progressing a plan for the refurbishment of the Renal Unit utilising £500k of
charitable monies granted from GLAXO. There are a number of areas that require
improvements to ensure that Trust standards are upheld in relation to information
governance and the storage of drugs. The action plan has been sent to the Divisional
Management Team for completion.
8. Recommendations
The Council of Governors is asked to:
The Council of Governors is asked to receive the information set out in this report and accept the actions identified.
Dr David Rosser Interim Executive Medical Director 17th July 2017

8

HEART OF ENGLAND NHS FOUNDATION TRUST
COUNCIL OF GOVERNORS
MONDAY 24TH JULY 2017
Title: Care Quality Board Report Responsible Director
:
Sam Foster, Chief Nurse
Contact Sam Foster, Chief Nurse
Purpose The purpose of this report is to provide an exception report of performance against the key performance indicators in the Single Oversight Framework, in addition to contractual and internal targets delivered in June 2017.
Annual Plan Ref
N/A
Key Issues Summary: Exception reports have been provided where there are current or future risks to performance against targets and indicators included in the Single Oversight Framework, national and contractual indicators and internal targets. Infection Control - There are no post 48 hour MRSA bacteraemia reported in June 2017. Two cases of pre- 48 hour MRSA bacteraemia have been reported and following a joint review with the CCG have both been attributed to third party. There were no lapses in practice identified from either the Trust or the community. Five cases of post 48 hour Clostridium difficile have been reported in June 2017. This is within the Trust monthly trajectory of five. The total number of cases this year is 10 against a year to date trajectory of 15 cases and an annual trajectory of 64 cases. Vancomycin-Resistant Enterococci (VRE) An outbreak of VRE was declared on ward 19 at Birmingham Heartlands Hospital in June 2107 with three patients identified as having VRE bacteraemia of the same strain. Screening of inpatients on the ward has revealed a high proportion of inpatients as being colonised with VRE and there is an ongoing action plan, which is being implemented. Tissue Viability - The number of avoidable grade 2 pressure ulcers was a total of two in June 2017. There were no reported hospital acquired pressure ulcers (grade 3) in June 2017.

Dementia Screening - It is an expectation of the Trust that all patients over the age of 75 are screened for dementia. The Trust target for this indicator is 90% and performance for June 2017 is at 88.03%. Parkinson’s Medication - It is an expectation that 90% of all Parkinson’s medication is administered within 30 minutes. The percentage of medication delivered within 30 minutes is at 82% in June 2017. Admissions, Discharges and Transfers (ADT) - Performance in June 2017 was at 88.87%. This has improved in month due to focused work in divisions with regards to the timely logging of deceased patients. A revised Standard Operating Procedure has been launched to guide this practice. Nurse Staffing - There are no areas of concern for June 2017.The Hot spot areas are Intensive Care Unit BHH, Neonatal Unit, and Ward 4 HDU and assurance has been given by Head Nurses that staffing maintained at levels suitable for acuity of patients with no shortfalls. Trainee Nursing Associates - The Trust is the lead partner in the Birmingham and Solihull Partnership that forms one of the national pilot sites for the Nursing Associate programme. There were a total of 41 Nurse Associate Trainees commenced the training programme in April 2017 and there have been no leavers from the programme to date. Complaints - The response rate for May 2017 is currently at 57.3%. This performance figure is not validated and is expected improve on validation (19th July 2017). The 85% target will not be achieved although May performance is currently 16.8% above the required trajectory for improvement towards achieving compliance with target. Friends and Family Test (FFT) - During May 2017, the percentage of positive responders was 95% for inpatient, this was the same as the previous month’s score. For the Emergency Department it was at 84% which is a decrease of 3% on the previous month. Response rates remain at a representative level (39% in patient, 11% ED).
Recommendations The Group is asked to consider the information set out in this report.

HEART OF ENGLAND NHS FOUNDATION TRUST
COUNCIL OF GOVERNORS
MONDAY 24TH JULY 2017 1. Purpose
This paper summarises the Trust’s performance against national indicators and targets, including those in the new Single Oversight Framework which commenced on 1st October 2016 as well as local priorities.
2. Single Oversight Framework
NHS Improvement (NHSI) has introduced a new Single Oversight Framework (SOF) for both NHS Trusts and Foundation Trusts which replaced Monitor’s Risk Assessment Framework (RAF) for Foundation Trusts on 1st October 2016. There are five themes within the framework as follows:
Quality of Care: The CQCs rating for the Safe, Caring, Effective and Responsive domains, delivery of the four priority 7-day standards and in-year information.
Finance and use of Resources: Financial efficiency and progress in meeting the financial control total.
Operational Performance: Progress with improving and sustaining performance against NHS Constitution and other standards.
Strategic Change: How well providers are delivering the strategic changes set out in the Five Year Forward View.
Leadership and Improvement Capability: A shares system view with CQC on what good governance and leadership looks like, including organisations’ ability to learn and improve, building on the joint CQC and NHSI well-led framework.
NHSI will use the information they collect on provider performance to identify where providers need support across these five themes. NHSI have identified an initial set of measures and triggers which will assist them to determine the level of support required and this report will focus on one of the five themes that is Quality of Care. Specifically NHSI will use the quality indicators outlined in table 1 to supplement CQC information in order to identify where providers may need support under the theme of quality:

Table 1 : Quality Performance Metrics
Measure Frequency Target
Mixed sex accommodation breaches Monthly 0
Inpatient scores from Friends & Family Test - % positive
Monthly ≥95%
A&E scores from Friends and Family Test - % positive
Monthly ≥95%
Emergency C-Section Rate Monthly
Maternity scores from Friends & Family Test - % positive
Monthly ≥95%
VTE Risk Assessment Quarterly ≥95%
Clostridium difficile - variance from plan Monthly ≤5
Clostridium difficile - infection rate Monthly
MRSA bacteraemia Monthly 0
Quality of Care 3. Infection Control
3.1 MRSA Bacteraemia
There have been no post-48 hour MRSA bacteraemia reported in June 2017. Two cases of pre-48 hour MRSA bacteraemia have been reported and following a joint review with the CCG have both been attributed to third party. There were no lapses in practice identified from either the Trust or the community.
3.2 Clostridium Difficile
Five cases of post 48 hour Clostridium difficile have been reported in June 2017. This is within the Trust monthly trajectory of five. The total number of cases this year is 10 against a YTD trajectory of 15 cases and an annual trajectory of 64 cases.
The reduction plan for 2017-18 is currently being developed and current planned interventions include:-
Introduction of RAG rating for newly identified cases, red cases will be reviewed twice weekly by the Infection Prevention Control Team (IPCT) to ensure the correct treatment and management.
Early identification of previously positive patients with those at risk of reoccurrence reviewed weekly by the IPCT in order that early isolation and stool sampling is implemented.
Post infection review tool to be issued to all clinicians responsible for patients who develop post 48 hour infections. Any gaps in care will be escalated to the division and managed through the local governance process.
Implementation of a revised clostridium difficile treatment algorithm.

Divisional RAPS have been introduced to ensure local ownership and improve overall performance. Each division will be expected to present performance against the RAP at the Divisional Scrutiny Meeting in April Chaired by the Chief Nurse and attended by an infection control specialist from NHSi.
3.3 Vancomycin-Resistant Enterococci (VRE)
An outbreak of VRE was declared on ward 19 at Birmingham Heartlands Hospital in June 2107 with three patients identified as having VRE bacteraemia of the same strain. Screening of inpatients on the ward has revealed a high proportion of inpatients as being colonised with VRE and there is an ongoing action plan, which is being implemented. The ongoing actions include:-
Deep cleaning of ward and day unit including use of Bioquell HPV for pressurises side rooms.
Removal of carpet from clinic rooms.
Washing of patients with Octenisan antimicrobial hair and body wash.
Weekly hand hygiene activity with clinical and non-clinical staff.
Antibiotic regime review.
Scoping peer review.
There has been one newly identified CPE patient in May 2017 from a routine screen of a patient who had been hospitalised abroad.
4. Tissue Viability
4.1 Avoidable Grade 2 Pressure Ulcers
The number of avoidable grade 2 pressure ulcers was a total of two in June 2017.
4.2 Avoidable Grade 3 Pressure Ulcers
There were no reported hospital acquired pressure ulcers (grade 3) in June 2017.
4.3 Care Quality Metrics - Tissue Viability Assessment
Tissue viability metrics were compliant at 98% in May 2017 with repositioning frequency adhered to non-compliant at 89%. Those wards that have not achieved performance above 85% for repositioning frequency adhered to will be attending the Chief Executive RCA performance meeting to present their rectification plans during May and June 2017.

5. Dementia Screening
It is an expectation of the Trust that all patients over the age of 75 are screened for dementia. The Trust target for this indicator is 90% and performance for June 2017 is at 88.03%. Divisional Directors have reminded all medical staff to ensure that Junior Doctors are completing the screening tool.
6. Parkinson’s Medication
It is an expectation that 90% of all Parkinson’s medication is administered within 30 minutes and compliance against this in June 2017 and is at 82%. This performance has risen slightly is an overall improving trend in performance and the programme of works across the trust needs to be developed and embedded.
7. Admissions, Discharges and Transfers (ADT)
Compliance against this standard is at 88.87% June 2017. This has improved in month due to focused work in divisions with regards to the timely logging of deceased patients. A revised Standard Operating Procedure has been launched to guide this practice.
8. Nurse Staffing
8.1 Compliance with Unify - The following table outlines compliance with Unify
for June 2017.
Divisional Area Qualified compliance HCA compliance Division 1 wards 100% 112% Division 1 critical care 90% 131% Division 2 Paeds 95% 96% Division 2 O&G 95% 97% Division 3 98% 111% Division 4 101% 112% Division 5 97% 105% Trust Overall 97% 109%
The Hot spot areas are Intensive Care Unit BHH, Neonatal Unit, and Ward 4 HDU and assurance has been given by Head Nurses that staffing maintained at levels suitable for acuity of patients with no shortfalls.
8.2 Vacancy Position
There are 298wte qualified nursing/midwifery vacancies in June 2017 which is an increase of 4wte in month. Division Three continues to have the highest vacancy rate (136wte). There are 153 planned Band 5 starters between July and September and an advert currently running to attract nurses from overseas who have had 6 months experience in the UK.

8.3 Trainee Nursing Associates
The Trust is the lead partner in the Birmingham and Solihull Partnership that forms one of the national pilot sites for the Nursing Associate programme. There were a total of 41 Nurse Associate Trainees commenced the training programme in April 2017 and there have been no leavers from the programme to date. A total of 79% of the trainees were established trust employees working in the Trust as HCA’s and this has offered a valued career pathway for these staff. Early feedback is positive and the potential for the role is becoming clear across all clinical areas and specialties. A scoping paper is being prepared to review the options to upscale future cohorts of trainees.
9. Friends and Family Test
During May 2017, the percentage of positive responders was 95% for inpatient; this was the same as the previous month’s score. For the Emergency Department it was at 84% which is a decrease of 3% on the previous month. Response rates remain at a representative level (39% in patient, 11% ED).
Patient comments received via FFT are shared with Divisions and the themes evident for improvement are analysed and presented in a quarterly patient experience for the Board.
10. Complaints
The response rate for May 2017 is currently at 57.3%. This performance figure is not validated and is expected improve on validation (19th July 2017). The 85% target will not be achieved although May performance is currently 16.8% above the required trajectory for improvement towards achieving compliance with target.
The invalidated May Divisional performance is currently:-
Division 1 - 100%,
Division 2 - 40%,
Division 3 - 54.2%,
Division 4 - 70%,
Division 5 - 76.9%.
The total number of complaints received during May was 110; the total number closed was 133. The total number of complaints received during June was 99; the total number closed was 117.
The live complaints caseload is currently at a total of 167. This is the lowest number of live cases recorded and at the start of 2017 this number was 290. Cases exceeding 50 working days from the Trust’s most recent response have decreased from 67 to 22 over the last 4 months.

Divisions are provided with a weekly real time summary of all complaints within the 30 working days and their older complaints. The stage each complaint is at in the process is, also provided.
In addition each division is provided with a weekly position of the numbers of live complaints they have within the 30 working day period and the number they need to resolve to achieve the target. If this target cannot be achieved, the highest possible response rate, which can be achieved within the month, is communicated.
In terms of actions taken as a result of complaints all divisions were provided with a log of actions, which were pledged following complaint investigations closed during quarter 4. Divisions have been asked to use these action log reports to gain assurance of learning from complaints and consequent completion of actions from within their Division. The Complaints team is currently arranging the Quarter 1 action logs for Divisions. Further action planning workshops took place in June 2017 with Supervisory Ward Sisters Matrons and Band 6 Sisters to discuss complaints and patient experience feedback. A report of these sessions will be produced in July 2017 and a Trust wide action plan will be developed. Themes for improvement have been identified and will be disseminated through divisions to allow teams to devise action plans from within their areas.

Appendix - Dashboard






Infection Prevention &
Control
Annual Report 2016-17
Dr Abid Hussain
Consultant Microbiologist
Associate Medical Director
Director, Infection Prevention & Control
July 2017

0
5
10
15
20
25
30
35
40
45
11/12 12/13 13/14 14/15 15/16 16/17
Ca
se
s p
er
10
00
be
d d
ays
Trust apportioned Clostridium difficile
infection rates
HEFT
UHB
UHCW
UHNM
SWBH
WAH
TRW
GEH
NUH
UHL

0
1
2
3
11/12 12/13 13/14 14/15 15/16 16/17
Ca
se
s p
er
10
00
be
d d
ays
Trust apportioned MRSA bacteraemia rates
HEFT
UHB
UHCW
UHNM
SWBH
WAH
TRW
GEH
NUH
UHL

0
5
10
15
20
25
11/12 12/13 13/14 14/15 15/16 16/17
Ra
te p
er
10
00
be
d d
ays
Trust Apportioned MSSA bacteraemia rates
HEFT
UHB
UHCW
UHNM
SWBH
WAH
TRW
GEH
NUH
UHL

0
20
40
60
80
100
120
140
160
12/13 13/14 14/15 15/16 16/17
Ra
te p
er
10
00
be
d d
ays
Total E coli bacteraemia rates
HEFT
UHB
UHCW
UHNM
SWBH
WAH
TRW
GEH
NUH
UHL

0
1
2
3
4
5
6
7
8
9
10
Nu
mb
ers
of
ba
ca
tera
em
ias
MRSA bacteraemia cumulative data
Pre 48hr
Post 48hr
Attrib
Post 48hr Trajectory




41
48
40 40 42 42 38
44
35 40
45
36
5
9
10 11 11
6
2
6
7
8
7
8
0
10
20
30
40
50
60
E. coli bacteraemia cases
Post 48hr
Pre 48 hr



0
1
2
3
Apr May Jun Jul Oct Nov Dec Jan Feb Mar
2016 2017
STrategic Executive Information System (STEIS) notifications
C diff death
C diff outbreak
Flu Outbreak
GAS Outbreak
MRSA Outbreak
Neonatal Outbreak
Norovirus outbreak
Post 48hr MRSA Bacteraemia
Pre 48hr MRSA Bacteraemia

NHS England CQUIN
Delivery
• 2016/17 CQUIN included a national indicator
on antimicrobial resistance
CQUIN 4a Target reduction
Position at end of Q4
All antibiotic
consumption – DDD’s per 1000 admissions
-1% -3.5%
Pip/taz consumption -
DDD’s per 1000 admissions
-1% -1.5%
Carbapenem
consumption - DDD’s per 1000 admissions
-1% -9.7%

2016/17 Key points
•7 MRSA Bacteraemia attributed to the organisation
•Over-performance of C. difficile infection against
trajectory
•Clustering of multiple outbreaks in Q4 2016/17
•Organisation pressures, in terms of patient flow
and footfall
•Some failure of IPC procedure – refreshing needed
•Fabric of the wards
•Lack of effective isolation facilities

Corrective actions to
2016/17
•Review of Clostridium difficile diagnosis and
treatment
•Reinforcement of Trust cleaning strategies
•Deployment of new modalities
•Re-investment in patient bathing products
•Refurbishment of key clinical areas

Review of 2017/18
Q1 data
•2 post 48 hr MRSA
bacteraemias
•Successfully defended
•Current attributable = ZERO
•VRE Outbreak in Ward 19



Looking forward to
2017/18 • Joint working with UHB IPCT
• Alignment of policies and practice
• Review of internal governance structures
• Aim for IPC delivery across all sites and
trajectories

HEART OF ENGLAND NHS FOUNDATION TRUST
COUNCIL OF GOVERNORS
MONDAY 24 JULY 2017 Title: Finance Report to 30 June 2017
Responsible
Director :
Julian Miller, Interim Director of Finance
Contact Ext. 40411
Purpose To provide an update on the Trust’s finances for the period ending 30 June 2017 (Month 3 2017/18).
Confidentiality Level & Reason
Confidential
Annual Plan Ref
Key Issues Summary:
The Trust agreed a planned deficit of (£28.8m) pre Sustainability and Transformation Funding (STF) for the 2017/18 financial year.
The full STF allocation for the Trust is £21.3m subject to financial performance. Of this 30% (£6.4m) is also dependant on delivery against the A&E access target improvement trajectory.
Including full allocation of STF, the Trust has a planned deficit of (£7.5m) in line with the control total required by NHS Improvement.
The in month position for month 3 is a deficit of (£4.7m) against a planned deficit pre STF of (£2.4m), an adverse variance of (£2.3m).
The year to date position at Q1 is a deficit of (£13.5m) against a planned deficit pre STF of (£7.2m), an adverse variance of (£6.3m).
The reported position excludes the allocation of STF for the year to date so far due to the adverse financial position against the plan.
The cash balance is £21.7m at 30 June 2017.
The Use of Resources Metric (UoR) is a 3.
Recommendations The Council of Governors is requested to:
Receive the contents of this report.
Approved by: Julian Miller 19 July 2017

2
HEART OF ENGLAND NHS FOUNDATION TRUST
COUNCIL OF GOVERNORS
MONDAY 24 JULY 2017
FINANCE REPORT FOR THE PERIOD ENDING 30 JUNE 2017
PRESENTED BY THE INTERIM DIRECTOR OF FINANCE
1. Introduction
This report covers the first three months of the 2017/18 financial year, for April to June 2017. The report summarises the Trust’s financial performance and includes information on healthcare activity, expenditure variances and Cost Improvement Programme (CIP) delivery.
The Financial Plan agreed by the Board of Directors on 23 January 2017 included a pre Sustainability and Transformation Fund (STF) deficit of (£28.8m) for 2017/18. The Trust’s STF allocation is £21.3m which if received in full would reduce the Trust’s plan deficit to (£7.5m) in line with the control total mandated by NHS Improvement (NHSI).
The Trust has reported an actual deficit of (£4.7m) for June 2017 (month 3) compared to a pre STF planned deficit of (£2.4m), an adverse variance of (£2.3m). This moves the year to date deficit to (£13.5m) against a planned deficit pre STF of (£7.2m), an adverse variance of (£6.3m).
Key variances against the plan year to date include:
Under-performance against clinical income targets (£1.8m);
Under-delivery against CIP targets (£2.0m) – of which (£0.6m) is a gap in the programme, (£0.6m) relates to phasing and (£0.8m) relates to slippage against planned delivery; and
Under-delivery against FRP/stretch savings target (£2.5m) – of which (£1.6m) is a gap in the programme, (£0.7m) relates to phasing and (£0.2m) relates to slippage.
As a result of the adverse financial performance, the allocation of STF of £1.1m per month in quarter 1, £3.2m in total, has not been assumed to be received and this forms part of the (£13.5m) overall deficit.
The cash balance at the end of June is £21.7m against the plan of £10.3m at this point, a favourable movement of £11.4m.

3
2. Income & Expenditure
2.1 Summary Position
The Trust’s income and expenditure position as at the end of June is a (£13.5m) deficit against the planned deficit pre STF of (£7.2m).
Table 1 below details the actual income and expenditure deficit compared to the planned trajectory submitted to NHS Improvement both pre and post STF allocation.
Table 1: I&E – Actual vs Plan
(30.00)
(25.00)
(20.00)
(15.00)
(10.00)
(5.00)
0.00
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
£m
's
2017/18 I&E (pre-impairments) - Cumulative Actual vs Plan
Cumulative Actual pre STF Cumulative Actual including Anticipated STF
Original NHSI Control Total Trajectory pre STF Original NHSI Control Total Trajectory post STF
Table 2 below summarises the Trust’s income and expenditure position at the end of May with analysis of expenditure from section 2.2 and operating revenue from section 2.6 below.

4
Table 2: Income and Expenditure Plan vs Actual
In Month In Month In Month YTD Plan YTD Actual Variance
Plan Actual Variance June June
£m £m £m £m £m £m
Control Total Items
Operating Revenue (excluding STF) 58.5 57.5 (0.9) 175.4 171.3 (4.0)
Operating Expenses (58.9) (60.4) (1.5) (176.8) (179.3) (2.4)
EBITDA (0.5) (2.9) (2.4) (1.5) (7.9) (6.5)
Depreciation (1.3) (1.3) 0.0 (4.0) (4.0) 0.0
Interest Receivable 0.0 0.0 0.0 0.0 0.0 0.0
Interest Payable (0.0) (0.0) 0.0 (0.1) (0.0) 0.0
PDC Dividend (0.5) (0.5) 0.0 (1.6) (1.6) 0.0
Other Finance Costs (0.1) 0.0 0.1 (0.2) 0.0 0.2
Control Total Surplus/(Deficit) (pre STF) (2.4) (4.7) (2.3) (7.2) (13.5) (6.3)
STF Income 1.1 0.0 (1.1) 3.2 0.0 (3.2)
Control Total Surplus/(Deficit) (post STF) (1.3) (4.7) (3.4) (4.0) (13.5) (9.5)
Gain/(Loss) on Asset Disposal 0.0 0.0 0.0 0.0 0.0 0.0
Donations and Grants Received 0.0 0.0 0.0 0.0 0.0 0.0
Depreciation on Donated Assets 0.0 0.0 0.0 0.0 0.0 0.0
Total Surplus/(Deficit) Before Impairments (1.3) (4.7) (3.4) (4.0) (13.5) (9.5)
Impairment (Losses) / Reversals 0.0 0.0 0.0 0.0 0.0 0.0
Surplus / (Deficit) After Impairments (1.3) (4.7) (3.4) (4.0) (13.5) (9.5)
2.2 Operating Expenditure Analysis
The adverse operating expenditure variance of (£1.5m) in month and (£2.4m) year to date can be broken down as detailed in table 3 below.
Table 3: Breakdown of Variance against Plan
In Mth Plan In Mth Actual Variance YTD Plan YTD Actual Variance
£m £m £m £m £m £m
PAY
Medical Staff 10.4 11.0 (0.6) 31.6 32.8 (1.3)
Nursing 14.9 15.2 (0.2) 44.3 46.4 (2.1)
Other 12.1 11.7 0.5 36.5 34.8 1.7
Total Pay 37.5 37.9 (0.4) 112.4 114.1 (1.7)
NON PAY
Drugs 6.2 6.8 (0.5) 18.6 18.5 0.1
Clinical Supplies & Services 6.0 6.3 (0.3) 18.0 18.1 (0.1)
Other 9.3 9.5 (0.2) 27.9 28.6 (0.8)
Total Non Pay 21.5 22.5 (1.1) 64.5 65.2 (0.7)
GRAND TOTAL 58.9 60.4 (1.5) 176.8 179.3 (2.4)
The main areas of pay and non-pay variance are explored further in sections 2.3 and 2.4 below.
2.3 Pay Analysis
Table 4 below details the average monthly pay expenditure each quarter through 2016/17 (adjusted for 2017/18 pay inflation) in comparison to the quarter 1 average in 2017/18.

5
Table 4: Quarterly Average Monthly Pay Expenditure
2017/18
Qtr 1 Avg Qtr 2 Avg Qtr 3 Avg Qtr 4 Avg Qtr 1 Avg
MEDICAL & DENTAL 10.5 10.5 11.0 11.0 10.9
NURSING & MIDWIFERY 15.3 14.9 15.1 15.5 15.5
OTHER SUPPORT STAFF 4.8 5.0 4.8 4.8 4.8
PAMS 2.2 2.2 2.2 2.2 2.2
PROFESSIONAL & TECHNICAL (PTB) 2.3 2.2 2.3 2.3 2.4
SCIENTIFIC & PROFESSIONAL 0.6 0.7 0.6 0.6 0.6
TRUST BOARD 1.8 1.7 1.6 1.5 1.6
Pay Total 37.4 37.3 37.7 37.9 38.0
2016/17
Overall the monthly average pay costs have increased by £0.6m, after inflation adjustment, compared to the quarter 1 average in 2016/17. The main areas of increase relate to Medical staffing (increase of £0.4m) and Nurse staffing (increase of £0.2m).
2.3.1 Medical Staffing
Tables 5.1 and 5.2 below detail the monthly expenditure for medical staff split between consultant and non-consultant posts respectively.
Total medical expenditure was £11.0m in June, which is (£0.2m) higher than the expenditure in May and is (£0.2m) higher than the rolling twelve month average (adjusted for pay inflation) overall.
The June expenditure on consultant medical staff was £6.4m which is (£0.1m) higher than in May. June expenditure on non-consultant staff was £4.6m which is broadly in line with the expenditure in May.
Table 5.1: Senior Medical Expenditure per Month
4,000.0
4,500.0
5,000.0
5,500.0
6,000.0
6,500.0
7,000.0
Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17
£0
00
's
Month
Senior Medical Expenditure per Month against Budget
Substantive WLIs Agency Locum Rolling 12 Month Average Budget

6
Table 5.2: Non-Consultant Medical Expenditure per Month
3,000.0
3,500.0
4,000.0
4,500.0
5,000.0
5,500.0
Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17
£0
00
's
Month
Non Consultant Expenditure per Month against Budget
Substantive Agency Locum Rolling 12 Month Average Budget
2.3.2 Nursing
Table 6 below details the monthly expenditure on nursing compared to the previous twelve months (adjusted for pay inflation).
Table 6: Monthly Nursing Expenditure
11,000.0
12,000.0
13,000.0
14,000.0
15,000.0
16,000.0
17,000.0
Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17
£0
00
's
Month
Nursing Expenditure per Month against Budget
Substantive Expenditure Bank Expenditure Agency Expenditure 12 Month Rolling Average Budget

7
Total nursing expenditure in June was £15.2m which is £0.5m lower than the expenditure in May and £0.1m lower than the rolling 12 month average (adjusted for pay inflation).
2.4 Non Pay Expenditure
Table 7 below details the average monthly non pay spend each quarter by expenditure group through 2016/17 in comparison to the quarter 1 average expenditure in 2017/18.
Table 7: Non Pay Spend by Expenditure Group
2017/18
Qtr 1 Avg Qtr 2 Avg Qtr 3 Avg Qtr 4 Avg Qtr 1 Avg
Clinical Supplies 5.8 5.7 5.9 6.2 6.0
Drugs 5.8 6.1 6.0 6.3 6.2
Less: Pass Through Items (5.9) (6.5) (6.5) (6.6) (6.2)
Clinical Supplies and Drugs Subtotal 5.6 5.4 5.5 5.8 6.0
Non-Clinical Supplies 1.6 1.6 1.6 1.7 1.6
Premises 2.5 2.5 2.6 2.8 2.6
Purchase of Healthcare Services NHS 0.7 0.7 0.6 0.5 0.6
Purchase of Healthcare Services Non NHS 0.6 0.6 0.4 0.4 0.6
Other 5.2 3.7 3.1 3.4 4.2
Grand Total 16.2 14.5 13.8 14.7 15.5
2016/17
2.4.1 Drugs and Clinical Supplies and Services
The expenditure on drugs and clinical supplies is £13.1m in June, which is an adverse variance of (£0.8m) against the plan for the month. However, the in month expenditure on excluded drugs and devices over-performed by £0.8m in the month explaining the increased expenditure in these areas. This increased expenditure is offset by an improved performance against the healthcare income plan for excluded drugs and devices.
The quarterly averages in table 7 above indicates that there is a continuation of an upward trend in the costs of clinical supplies and drugs which are within tariff with expenditure in quarter 1 of 2017/18 being (£0.4m) higher than the average incurred in quarter 1 of 2016/17 and June expenditure of (£6.1m) being (£0.1m) higher than that incurred in May.
2.4.2 Other Non-Pay
The adverse variance in other non-pay is primarily driven by slippage on the new financial years cost improvement schemes including the Financial Recovery Programme and the stretch savings target.
The key movements in the actuals detailed in the quarterly averages between quarter 4 of 2016/17 and quarter 1 of 2017/18 in table 7 are:
Education and training expense (incl. apprenticeship levy) - (£0.1m)
Increased CNST premium - (£0.2m)
Increased movement on bad debt provision - (£0.4m)
Other miscellaneous non pay - (£0.1m)
2.5 Divisional Performance
Table 8 below details the budgetary variance by Division split by expense type. The “Income” expense type refers to Category C income such as SLA

8
income from other organisations; it does not refer to NHS Clinical Income, which is detailed in section 2.6 below.
Table 8: Variance Breakdown by Division
Division ExpenseGroupDesc In Month
Budget -
£000's
In Month
Actual - £000's
In Month
Variance -
£000's
YTD Budget -
£000's
YTD Actual -
£000's
YTD Variance -
£000's
D1 INCOME (398.1) (379.0) (19.2) (1,325.8) (1,345.8) 20.0
NON PAY EXPENDITURE 2,449.5 2,846.1 (396.7) 7,083.7 8,327.3 (1,243.7)
PAY EXPENDITURE 7,897.2 7,940.3 (43.1) 23,679.2 23,906.9 (227.7)
D1 Total 9,948.6 10,407.5 (458.9) 29,437.1 30,888.4 (1,451.3)
D2 INCOME (436.2) (447.6) 11.4 (1,308.5) (1,280.0) (28.4)
NON PAY EXPENDITURE 1,085.6 1,278.3 (192.6) 3,063.3 3,450.8 (387.5)
PAY EXPENDITURE 4,838.2 4,808.8 29.4 14,529.2 14,411.9 117.3
D2 Total 5,487.7 5,639.4 (151.8) 16,284.0 16,582.7 (298.7)
D3 INCOME (315.2) (492.1) 176.9 (945.6) (929.2) (16.4)
NON PAY EXPENDITURE 2,638.3 2,888.4 (250.1) 7,532.5 8,369.0 (836.5)
PAY EXPENDITURE 7,469.2 7,800.3 (331.1) 22,371.7 23,714.0 (1,342.2)
D3 Total 9,792.3 10,196.6 (404.3) 28,958.6 31,153.8 (2,195.2)
D4 INCOME (188.5) (201.5) 13.1 (562.2) (687.8) 125.5
NON PAY EXPENDITURE 4,592.3 4,944.2 (352.0) 12,677.2 14,021.1 (1,343.9)
PAY EXPENDITURE 6,414.7 6,599.9 (185.2) 19,280.1 20,022.8 (742.6)
D4 Total 10,818.5 11,342.6 (524.1) 31,395.0 33,356.1 (1,961.0)
D5 INCOME (83.3) (127.4) 44.1 (417.5) (500.0) 82.5
NON PAY EXPENDITURE 3,887.5 3,713.8 173.7 10,742.5 10,329.3 413.2
PAY EXPENDITURE 5,721.9 5,982.9 (261.0) 16,348.5 17,810.3 (1,461.8)
D5 Total 9,526.1 9,569.3 (43.2) 26,673.6 27,639.7 (966.1)
Grand Total 45,573.1 47,155.4 (1,582.3) 132,748.3 139,620.6 (6,872.3)
The main areas of variance in month for each Division are as follows:
Division 1 (CSS) - Radiology (£133k) non pay predominantly on clinical supplies and outsourcing of reporting, (£146k) pay primarily on Radiographer bank and agency premium rate cover. Laboratory Medicine (£39k) non pay on external testing and reagents. Theatres (£41k) non pay on medical equipment maintenance and unmet CIP target.
Division 2 (W&C) - Obstetrics (£131k) non pay and Paediatrics (£53k) non pay primarily due to unmet CIP targets.
Division 3 (Emergency) - Nursing overspends of (£249k) across the division with (£102k) in Acute Medicine and (£34k) in Accident and Emergency. Medics overspend of (£93k) across the division with Accident and Emergency presenting the biggest pressure at (£113k). Over-recovery of £172k on cat C income related to increased RTA income. Unmet CIP targets across the division of (£165k) in non-pay with Acute Medicine and Respiratory being the biggest pressure points in this area.
Division 4 (Medicine) - Unmet CIP targets in non-pay of (£162k) across the division with Elderly Care and Therapies presented the biggest pressures in this area. Drug overspends of (£193k) driven by Clinical Haematology and Oncology (£158k). Nursing overspends of (£66k) driven by Elderly Care (£45k). Medic overspends of (£105k) with the biggest pressures in Elderly Care (£52k) and Clinical Haematology and Oncology (£38k).

9
Division 5 (Surgery) - Medical overspends of (£376k) with the biggest pressures in Trauma and Orthopaedics (£122k) and Gastroenterology (£153k).
2.6 Income Analysis
2.6.1 Total Operating Income
Total operating income (excluding STF) is (£0.9m) below plan in June taking the year to date under-performance to (£4.0m) as shown in table 9 below.
Table 9 – Income against Plan
In Mth Plan In Mth Actual Variance YTD Plan YTD Actual Variance
June June June June
£m £m £m £m £m £m
Clinical - NHS (52.7) (52.5) (0.2) (158.2) (156.6) (1.5)
Clinical - Non NHS (0.7) (1.0) 0.2 (2.2) (2.3) 0.1
Other (5.0) (4.1) (1.0) (15.0) (12.5) (2.6)
TOTAL (58.5) (57.5) (0.9) (175.4) (171.3) (4.0)
NHS Clinical Income is (£0.2m) below plan in June moving the year to date under-performance to (£1.5m). Excluded drugs and devices improved further in June, with over-performance of £0.9m bringing the year to date performance to a favourable variance of £0.4m. The remaining variance of (£1.1m) under-performance in June relates to a variance against the seasonal healthcare income related to activity moving the year to date under-performance to (£1.9m).
The main areas of variance during June and year to date are detailed in table 10 below:
Table 10 – Healthcare Income Variances by Point of Delivery
In Month
Variance
YTD Variance
Maternity Spells/Pathways (0.7) (1.6)
Emergency Activity 0.0 0.2
Accident and Emergency 0.1 0.2
Elective/Daycase Spells (0.1) (0.1)
Outpatients (0.3) (0.4)
Other (0.1) (0.2)
Grand Total (1.1) (1.9)
2.6.2 NHS Clinical Income/Activity - Inpatients
Table 11.1 below details the monthly admitted patient care (APC) spells against the seasonally phased targets in June.

10
Table 11.1: Trust Inpatient Activity
5,000
6,000
7,000
8,000
9,000
10,000
11,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Sp
ell
s
Month
Admitted Patient Care 2017/18 - Actual vs Target (PbR)
Emergency Spells - Actual Emergency Spells - Phased Target Daycase & Elective Spells - Actual Daycase & Elective Spells - Phased Target
The June in-month activity position reflects an (0.7%) under-performance in emergency pathways (60 spells) against the seasonally phased plan, resulting in year to date over-performance against the seasonal plan of 2.8% (749 spells). Emergency ambulatory work continues to over-perform by 277 spells whilst emergency inpatient admissions have this month under-performed by (108) spells.
A&E activity has shown a (2.2%) under-performance in June (507 attendances) taking the year to date under-performance to (0.6%), (418 attendances).
The elective and daycase activity was 3.2% above plan in June (251 cases) taking the year to date over-performance to 5.5% (1,189 cases).
2.6.3 NHS Clinical Income/Activity – Outpatients
Table 11.2 below details the monthly outpatient attendances compared to the seasonally phased targets in June.

11
Table 11.2: Trust Outpatient Activity
60,000
62,000
64,000
66,000
68,000
70,000
72,000
74,000
76,000
78,000
80,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Att
en
da
nc
es
Month
Outpatients 2017/18 - Actual vs Target
Outpatient Attendances - Actual Outpatient Attendances - Phased Target
Outpatient activity in month has under-performed by (0.5%) in June (357 attendances) taking the year to date position to over-performance of 1.0% (2,158 attendances). The largest areas of over-performance in the month relate to Gynaecology (291 attendances, 9.4%) and Respiratory Medicine (224 attendances, 9.3%). Largest areas of under-performance in the month relate to Paediatrics (585 attendances, 25.8%) and Vascular Surgery (135 attendances, 18.3%).
2.6.4 Divisional Performance
Table 12 below details the variance against the year to date seasonally phased plan, split by Division and point of delivery but excluding performance on Excluded Drugs and Devices.

12
Table 12: Healthcare Income Variance vs Seasonally Phased Plan
Division IP - £000's OP - £000's Other - £000's Total - £000's
1 - CSS 358 15 (333) 39
2 - W&C (59) (39) (2,037) (2,134)
3 - Emergency 338 191 (408) 121
4 - Medicine (874) (604) (321) (1,799)
5 - Surgery 478 108 (288) 298
Central Risks 0 0 1,622 1,622
Total 242 (330) (1,765) (1,853)
Point of Delivery
2.6.5 Other Miscellaneous Operating Revenue
The adverse variance of (£1.0m) against the planned other operating revenue in June is driven by slippage on income cost improvement schemes of (£0.5m) built into the plan, reduction in non-patient care income (£0.1m) and reduction in other income (£0.1m).
3. Efficiency Savings
3.1 Cost Improvement Programme
The 2017/18 identified schemes by Division, together with delivery against them both in June and year to date, is detailed in table 13 below.
Table 13: CIP Delivery by Division
DivisionIn Month 12ths
TargetIn Month Delivery In Month Variance YTD 12ths Target YTD Delivery YTD Variance Annual Target
Annual Target
Identified
CORPORATE 130.8 145.5 14.7 392.4 306.9 (85.5) 1,569.6 1,203.0
FACILITIES 146.4 111.0 (35.4) 439.2 305.2 (134.0) 1,756.7 1,259.3
TRUSTWIDE EDUCATION SERVICES 33.6 0.0 (33.6) 100.9 0.0 (100.9) 403.5 0.1
RESEARCH & INNOVATION 8.1 0.0 (8.1) 24.2 0.0 (24.2) 96.9 0.0
CSS 209.7 96.0 (113.7) 629.2 307.0 (322.2) 2,516.7 2,067.6
WOMENS & CHILDRENS 106.3 44.0 (62.3) 318.8 134.0 (184.8) 1,275.3 945.8
EMERGENCY CARE 185.3 72.0 (113.3) 555.8 176.0 (379.8) 2,223.3 2,312.3
MEDICINE 202.9 69.5 (133.4) 608.7 258.3 (350.4) 2,434.8 1,711.5
SURGERY 171.5 16.6 (154.9) 514.5 140.8 (373.7) 2,058.0 2,245.9
TOTAL 1,194.6 554.6 (639.9) 3,583.7 1,628.2 (1,955.5) 14,334.8 11,745.6
The variance against the year to date target of (£2.0m) reflects a combination of slippage on schemes initially identified to deliver year to date (£0.8m), planned phasing adjustments (£0.6m) and target with schemes unidentified (£0.6m).
3.2 Financial Recovery Plan
Year 2 of the Trust’s Financial Recovery Plan for 2017/18 included agreed cross cutting schemes with saving opportunities of £4.7m, the delivery against which is detailed in table 14 below.

13
Table 14: Year 2 Cross Cutting Schemes
Workstream / Project Scheme StartIn Year Benefit
2017/18In Mth Target In Mth Actual YTD Target YTD Actual
Length of Stay Jun-17 1,042 104 0 104 0
Theatre Productivity Apr-17 524 44 44 125 125
Diagnostics Apr-17 100 8 0 25 0
Procurement: National & Local
StandardisationApr-17 41 6 6 19 19
Procurement: UHB Alignment Aug-17 544 0 3 0 6
Procurement: Direct Source Pricing Aug-17 133 0 0 0 0
Procurement: GHX Renewal Oct-17 114 0 0 0 0
Procurement: Review 111 Other
ContractsOct-17 114 0 0 0 0
Procurement: Mobile Phones Apr-17 22 2 2 5 5
Medical: International Fellows Apr-17 0 0 0 0 0
Medical: Business Case Pipeline Jun-17 272 68 0 68 0
Medical: E-rostering & Compliance
with PoliciesJul-17 0 0 0 0 0
Nursing: Matron Review Apr-17 111 9 9 28 28
Nursing: E-rostering & Compliance
with PoliciesJun-17 755 5 0 5 0
Nursing: ACP Sep-17 426 5 5 15 15
Corporate: Updated
CommunicationsApr-17 25 2 2 6 6
A&C: Balance to full year effect of
restructuresApr-17 698 59 59 167 167
Grand Total 4,921 313 131 567 371
Balance to find from original FRP
following validation1,315
Balance to find from stretch targets 4,900
Total FRP/Stretch Target 11,136
Month 3
As with the CIP targets the total FRP/stretch savings target has been posted in the ledger in 12ths. Overall there is circa (£0.2m) slippage on the planned delivery, (£0.7m) of under-delivery in the position which relates to the planned phasing of the schemes with a further (£1.6m) which relates to the slippage associated with the unidentified stretch savings target. Work continues to try and identify programmes to close this gap.
4. Statement of Financial Position
The Statement of Financial Position (Balance Sheet) shows the value of the Trust’s assets and liabilities. The upper part of the statement shows the net assets after deducting short and long term liabilities with the lower part identifying sources of finance. Table 15 below summarises the Trust’s Statement of Financial Position as at 30 June 2017.

14
Table 15: Statement of Financial Position
Actual Actual Plan Annual Plan
Mar-17 Jun-17 Jun-17 Mar-18
£m £m £m £m
Non Current Assets:
Property, Plant and Equipment 248.1 245.3 256.5 259.8
Intangible Assets 2.0 1.7 9.7 9.1
Trade and Other Receivables 1.0 1.1 1.6 1.6
Other Assets 3.8 3.8 3.7 3.6
Total Non Current Assets 254.8 251.9 271.5 274.0
Current Assets:
Inventories 10.7 10.7 11.0 10.0
Trade and Other Receivables 32.2 99.1 47.3 43.8
Cash 19.2 21.7 10.3 3.0
Total Current Assets 62.2 131.5 68.6 56.8
Current Liabilities:
Trade and Other Payables (102.4) (121.9) (108.5) (98.8)
Borrowings (0.5) (0.5) (0.5) (4.0)
Provisions (3.2) (3.5) (3.1) (2.4)
Tax Payable 0.0 0.0 0.0 0.0
Other Liabilities (6.3) (58.5) (6.5) (6.5)
Total Current Liabilities (112.4) (184.4) (118.6) (111.6)
Non Current Liabilities:
Borrowings (3.3) (3.2) (3.2) (6.0)
Provisions (6.2) (5.9) (5.8) (5.8)
Other Liabilities 0.0 0.0 (1.6) 0.0
Total Non Current Liabilities (9.5) (9.1) (10.6) (11.8)
TOTAL ASSETS EMPLOYED 195.1 190.0 210.8 207.3
Financed by:
Public Dividend Capital 196.7 196.7 196.7 196.7
Income and Expenditure Reserve (45.9) (59.2) (40.1) (42.7)
Donated Asset Reserve (0.2) (0.2) (0.2) (0.2)
Revaluation Reserve 52.9 52.6 54.4 53.5
Merger Reserve 0.0 0.0 0.0 0.0
TOTAL TAXPAYERS EQUITY 203.5 190.0 210.8 207.3
5. Capital Expenditure (Non-Current Assets)
The initial capital programme for 2017/18 initially totalled £18.1m, this included £16.0m of internally funded schemes and £2.1m of costs associated with the enabling works for ACAD for which a DH loan has been approved. This programme was subsequently uplifted to £20.1m as a result of anticipated slippage of £1.0m on 2016/17 schemes and £1.0m slippage on the costs of ACAD. This is the value at which the final plan was submitted to NHSI.
Table 16 below details the planned trajectory of the £20.1m together with the actual spend from April to June.

15
Table 16: Capital Programme Trajectory vs Actuals
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
22.0
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
£m
's
Capital Programme versus Actual Expenditure
Cumulative Capex Plan Cumulative Actual
Expenditure to date is £1.0m against a plan at this point of £5.4m, slippage of (£4.4m) against the plan. The most notable items of slippage are within ICT (£0.7m) (orders have been raised but the asset has not been received) and enabling works costs associated with ACAD of (£1.5m).
6. Current Assets
The Trust’s total current assets (excluding cash and inventories) amount to £99.1m at 30 June 2017 an increase of (£3.0m) during June and (£51.8m) higher than plan. The balance is broken down as detailed in table 17 below.

16
Table 17: Analysis of Current Assets (excluding Inventories and Cash)
YTD Actual YTD Plan
June 2017 June 2017
£m £m
Trade Receivables 89.7 45.8
Bad Debt Provision (10.3) (11.9)
Other Receivables 2.8 2.4
Trade and Other Receivables 82.3 36.3
Accrued Income 3.0 3.5
Other Financial Assets 3.0 3.5
Prepayments 13.9 7.5
Other Current Assets 13.9 7.5
TOTAL 99.1 47.3
The main movement against the plan is as a result of billing commissioners earlier for the mandate payment, resulting in increased trade receivables offset by increased deferred income (within Other Liabilities), in order to ensure the cash is received into the Trust in a timely manner.
Analysis of the age profile of Trade Receivables (unpaid invoices issued by the Trust) is summarised in table 18 below.
Table 18: Aged Debt Analysis
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
0-30 30-60 60-365 1 Year+
£0
00
's
Aged Trade and Other Receivables for June 2017
Overdue debt now stands at £18.5m of which £11.5m relates to CCG/NHS England healthcare income contracts. This represents an overall increase of (£9.0m) on the position at the end of May 2017, predominantly within these healthcare income contracts. The top 3 balances (outside of CCG/NHS England Healthcare Income contracts) are:
Burton Hospitals Foundation Trust (£0.8m > 30 days, £1.1m total) – this is a decrease of £0.4m on both the greater than 30 days and the total debt from

17
the position at the end of May 2017. A write off of disputed debt relating to 2013 to 2015 of £0.4m has been finalised during the month. Some queries around the 2016/17 contract remain under discussion.
University Hospitals Birmingham (£0.7m > 30 days, £0.8m total) – this has not moved from the position at the end of May 2017. The overdue debt predominantly relates to the Maxillofacial services where agreement has been reached and invoices paid to March 2015, but further discussion is needed for the remaining years.
Sandwell and West Birmingham Trust (SWBH) (£0.6m > 30 days, £0.8m total) – this is an increase of (£0.1m) on both the overdue and total debt compared to May 2017. The majority of the overdue debt relates to prior year surgical SLA provision, the queries from which are currently being followed up.
7. Cash Flow
The cash balance at the end of June 2017 was £21.7m, an increase of £2.0m during June and a positive variance of £11.4m against the planned balance of £10.3m.
Table 19 below details the anticipated cash balances to the end of the 2017/18 financial year. Table 19: Daily Cashflow Forecasting as at 10 July
(40.0)
(20.0)
0.0
20.0
40.0
60.0
80.0
01
/04
/201
7
15
/04
/201
7
29
/04
/201
7
13
/05
/201
7
27
/05
/201
7
10
/06
/201
7
24
/06
/201
7
08
/07
/201
7
22
/07
/201
7
05
/08
/201
7
19
/08
/201
7
02
/09
/201
7
16
/09
/201
7
30
/09
/201
7
14
/10
/201
7
28
/10
/201
7
11
/11
/201
7
25
/11
/201
7
09
/12
/201
7
23
/12
/201
7
06
/01
/201
8
20
/01
/201
8
03
/02
/201
8
17
/02
/201
8
03
/03
/201
8
17
/03
/201
8
31
/03
/201
8
£m
Date
Daily Cashflow to end of 2017/18 - as at 10 July 2017
Actual Closing Balance - £m Forecast Closing Balance - £m Drawdown of Borrowing Point - £m
Table 19 demonstrates that whilst the Trust is anticipated to move below the borrowing point briefly towards the end of August, a more prolonged requirement is expected in September. This includes the receipt of the quarter 4 2016/17 STF of £7.7m in July, as confirmed by NHS Improvement (NHSI).

18
The Trust has started the process of setting up the borrowing facility with NHSI with the view to draw cash in the middle of August if required.
8. NHS Improvement Finance and Use of Resources Metric
8.1 Finance and Use of Resource Metrics
The Finance and Use of Resource (UoR) metric has replaced the previous Financial Sustainability Risk rating (FSRR). Each metric is scored between 1 (best) and 4 (worst) and then an average is calculated to derive the overall UoR score for the provider. Where providers have an overall score of 3 or 4 for finance and use of resources, this will identify a potential support need under this theme, as will providers scoring a 4 against any of the individual metrics. Providers in financial special measures will default to an overall score of 4 on this theme.
The individual metrics scored against are detailed in table 20 below.
Table 20: Scoring Mechanism for Finance and Use of Resources Metric
Area Metric Weight Definition 1 2 3 4
Capital Service
Capacity
20% Degree to which the provider's
generated income cover its
financial obligations
>2.5x 1.75-2.5 1.25-1.75 <1.25
Liquidity (days) 20% Days of operating costs held in
cash or cash-equivalent forms,
including wholly committed lines
of credit available for drawdown
>0 (7)-0 (14)-(7) <(14)
Financial EfficiencyI&E Margin 20% I&E surplus or deficit / total
revenue
>1% 1%-0% 0%-(1%) <(1%)
Distance from Finance
Plan
20% Year-to-date actual I&E
surplus/deficit in comparison to
year-to-date plan I&E
surplus/deficit
≥0% (1%)-0% (2%)-(1%) ≤(2%)
Agency Spend 20% Distance from provider's cap ≤0% 0%-25% 25%-50% ≥50%
Use of Resource Metrics
Financial Sustainability
Financial Controls
8.2 Trust Performance
The Trust has been put into segment 3 as was anticipated. This means mandated support must be complied with to address specific issues and help move the Trust into segment 2.
With regards the Finance and Use of Resource Metric, the June year to date metric scoring is detailed in table 21 below.
Table 21: Trust Scoring Year to Date
Area Metric Weight Actual Score
Capital Service
Capacity
20% (4.60) 4
Liquidity (days) 20% (32.24) 4
Financial Efficiency I&E Margin 20% (7.80%) 4
Distance from Finance
Plan
20% (5.50%) 4
Agency Spend 20% (10.10%) 1
Use of Resource Metrics
Financial Sustainability
Financial Controls

19
This rating is anticipated to continue throughout the financial year but is only being maintained through the Trust’s delivery against the agency ceiling.
9. Conclusion
The Trust has delivered an overall deficit of (£4.7m) for month 3 of the 2017/18 financial year, an adverse variance of (£2.3m) against the planned deficit of (£2.4m) pre STF. This moves the year to date deficit to (£13.5m) an adverse variance of (£6.3m) against the planned deficit pre STF of (£7.2m). As a result of under-delivering against the financial plan, the year to date allocation of £3.2m of STF has not been assumed.
The Trust’s cash balance as at 30 June 2017 was £21.7m which is £11.4m above the planned cash of £10.3m at this point in the year.
10. Recommendations
The Council of Governors is requested to:
Receive the contents of this report
Julian Miller Interim Director of Finance 19 July 2017

HEART OF ENGLAND NHS FOUNDATION TRUST
COUNCIL OF GOVERNORS
Monday 24th July 2017
Title: Quality Account Update for Quarter 1 2017/18 (April –
June 2017)
Responsible
Director :
From: Dr David Rosser, Interim Executive Medical Director
Contact Amy Fowlie, Project Assistant – Mariola Smallman, Head of Quality Management – Mark Garrick, Director of Medical Directors’ Services
Purpose To provide an update on the Quality Account for Quarter 1 2017/18 (April – June 2017). To receive and note the contents of this report
Confidentiality Level & Reason
Annual Plan Ref
Key Issues Summary:
Trust Quality Improvement Priorities 2017/18
Mortality (SHMI, HSMR and Crude Mortality)
Patient safety indicators Clinical effectiveness indicators
Recommendations The Council of Governors is asked to receive the information set out in this report and accept the actions identified.
Approved by:

2
Quality Account Update for Quarter 1 2017/18 (April – June 2017)
Contents
Introduction
Quality Improvement Priorities
Priority 1: Reduce avoidable harm to patients from omission and delay in receiving Parkinson’s disease medication
4
Priority 2: Improve early recognition of sepsis and reduce hospital acquired sepsis
7
Priority 3: Reducing surgical site infection after major surgery 12
Priority 4: Improve infection rates for Clostridium Difficile (C Diff) and MRSA
14
Mortality 16
Selected Metrics
Patient safety indicators 18
Clinical effectiveness indicators 22

3
Quality Account Update for Quarter 1 2017/18 (April – June 2017)
Introduction The Trust published its eighth Quality Account Report in June 2017 as part of the Annual Report and Accounts. The report contained an overview of the quality initiatives undertaken in 2016/17, performance data for selected metrics and set out five priorities for improvement during 2017/18: Priority 1: Reduce avoidable harm to patients from omission and delay in receiving
Parkinson’s disease medication Priority 2: Improve early recognition of sepsis and reduce hospital acquired sepsis Priority 3: Reducing surgical site infection after major surgery Priority 4: Improve infection rates for Clostridium Difficile (C Diff) and MRSA This report provides an update on the progress made for the period April to June 2017 towards meeting these priorities and updated performance data for the selected metrics. This update report should be read alongside the Trust’s Quality Account Report for 2016/17.

4
Quality Improvement Priorities
Priority 1: Reduce avoidable harm to patients from omission and delay in receiving Parkinson’s disease medication Background Since June 2015 the Trust has focused on reducing the number of omitted and delayed doses of Parkinson’s disease (PD) medication. PD medications are time critical. If medications are delayed or omitted, patients rapidly deteriorate in terms of their ability to move, speak and swallow. When this happens, patients are at risk of falls, pressure ulcers, aspiration pneumonia and neuroleptic malignant syndrome. This can be fatal. There is also evidence showing that PD patients in whom medication has been delayed or missed have an increased length of stay (Martinez-Ramirez et al, Movement disorders 2015). The importance of timely PD medication in hospital is recognised nationally in the Parkinson’s UK “Get it on time” campaign. Baseline data (2015) at HEFT showed 14,000 delayed doses and 3,500 missed doses of PD medication annually across the three Trust sites. The data also identified that only 53% of inpatients were receiving their PD medication within 30 minutes of the prescribed time. This data, combined with several clinical incidents, formed the impetus for the development of a Quality Improvement (QI) team to address this issue. The Trust aim is for 90% of PD medication to be administered within 30 minutes. Performance Overall performance has continued to improve across the three hospital sites and is 81% for Quarter 1 2017/18. This is an improvement on the same period 2016/17 and 2015/16 – see Table 1 below for detail. It is expected that performance will continue to improve as the nurse responder bleep system is more widely utilised across all wards. In addition, the stocks of emergency PD medication have increased and have been added to the pharmacy out of hours cupboard to support timely administration.
Table 1
Q1 – 2015/16
Q1- 2016/17
Q1 – 2017/18
Overall Trust % (Target 90% PD medication administered within 30 minutes)
51%
71%
81%
Total doses prescribed 9,106 9,689 12,784
Total doses administered late
3,499
2,268 1,969
Total doses non-administered (omitted)
926
572 471

5
Q1 – 2017/18 PD medication performance by Hospital site
Initiatives to be implemented in 2017/18:
A review of Trust-wide reasons for omissions and delays in the administration of PD medication will be undertaken by the PD Quality Improvement team to identify and target any specific areas for further improvement.
An audit of omissions and delays in PD medication will be undertaken in Emergency Department (ED) BHH which is a non -Electronic Prescribing (EP) area. This will identify how further improvements can be made to support timely administration of PD medication in the ED and non EP areas.
The project’s educational film has won an award at the Haelo film festival in the category ‘my story’. More recently it has also won the Parkinson’s Excellence Network award which recognises and celebrates outstanding services that make a difference to people in the UK affected by PD. The Parkinson project has been shortlisted as finalists for the HSJ Patient safety Awards which will be held on 4th July 2017.
83%
76%
83% 83%
75%
88% 85%
76%
92%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
BHH GHH SH
PD drugs administered within 1/2 hour
April
May
June

6
How progress will be monitored, measured and reported
Progress will continue to be measured at ward, speciality, divisional and Trust levels via the live electronic medication dashboard which links directly to the Trust’s EP system. This dashboard provides historical and ‘live’ data to ward areas, allowing ward and divisional review of performance and reasons for delays and non-administration of PD medications.
Ward and divisional performance will continue to be monitored via the Nursing and Midwifery Care Quality Dashboard. Progress will be reported monthly to the Chief Executive’s Group (CEG) by the Chief Nurse.
The Parkinson’s Quality Improvement project team will continue to meet monthly to monitor progress and report to the Safer Medicines Practice Group (SMPG), which is chaired by the Clinical Director of Pharmacy.
Progress will be publicly reported in the quarterly Quality Report updates.

7
Priority 2: Improve early recognition of sepsis and reduce hospital acquired sepsis Background Sepsis is defined as “life threatening organ dysfunction caused by a dysregulated response to infection”. It is a syndrome, described by a set of clinical criteria and not truly a diagnosis in and of itself. This makes recognising it complicated. Previous definitions were based on the systemic inflammatory response (SIRS) criteria. In 2016 these were replaced as they were felt to be insufficiently sensitive. The NICE guidance published that year defined sepsis using broader clinical criteria. An audit at Birmingham Heartlands Hospital (BHH) indicated that these new standards have the potential to increase the proportion of medical admissions classed as septic by 50% (i.e. to one third of the medical take). The Trust has had well publicised clinical pathways for sepsis management in place for several years. These have been updated and now take account of the NICE guidance changes. We have taken this opportunity to launch a number of other changes which are detailed below. This is with the aim of improving:
Reliable recognition and screening of sepsis;
Timely and reliable escalation and sepsis treatment;
Reviewing and de-escalating antibiotics where possible

8
Performance
Indicator 2a Timely identification of sepsis in emergency departments and acute inpatient settings
2016/17 Apr-17 May-17 Total (2017/18 to date)
Total number of patients eligible for screening and received screening
390 56 46 102
Total number of patients eligible for screening but did not receive
screening
296 24 21 45
CQUIN achievement 57%1 70% 69% 69%
Indicator 2b Timely treatment of sepsis in emergency departments and acute inpatient settings 2016/17 Apr-17
May-17
2b Current Total for
Q1 Acute
Inpatient Emergency
Acute Inpatient
Emergency Total Acute
Inpatient Emergency Total
Patient was diagnosed with sepsis and
received IV antibiotics within 1 hour of
diagnosis
25 162 18 2 20 13 2 15 35
Patient was diagnosed with sepsis and did not receive IV antibiotics
within 1 hour of diagnosis
20 158 7 8 15 3 9 12 27
Percentage 56%2 51% 72% 20% 51% 81% 18% 57% 57%
1 2016/17 Quality Account data presented as separate results for ED and inpatients
2 Q2 data 2016/17 only

9
Initiatives to be implemented 2017/18 Admitting areas and inpatient wards
The adult Modified Early Warning Score (MEWS) chart has been updated and relaunched with new sepsis screening prompts and check boxes.
The new Trust adult sepsis screening tool has been launched. This includes a quick screen to identify the sickest patients who are most likely to require critical care involvement.
Education teams went to all wards and admitting areas in all 3 hospital sites providing education sessions and educational material in the week before the launch.
A sepsis power point presentation is available on the intranet along with all the resources for sepsis.
Rolling training is delivered to all new nurses at Trust induction, via the new Acute Illness Management (AIM) course and to junior doctor risky business forums.
The divisional leads have been informed of all these changes and training has been offered to all clinical departments.
Training is being specifically delivered to the Emergency Department to raise awareness of the sepsis requirements.
Rather than limit the Trust to the minimum CQUIN requirement, the sepsis team have identified those factors which we feel will most improve the clinical care of patients with sepsis and will include these in CQUIN data collection. This includes whether blood cultures were taken, the time band of antibiotic administration if beyond 1 hour, and whether patients fell into the sickest group. This will enable us to understand the potential clinical impact of improvement work, beyond CQUIN achievement.
The CQUIN requires a 24-72h antibiotic review by ST3 or above. The aim is presumably to reduce unnecessary antibiotic use. The team felt that this is unlikely to be achieved by ST3 doctors whom rarely stop or de-escalate antibiotics. Septic patients warrant a Consultant review and therefore within the Trust this is the promoted standard. It will be coupled with training on the importance of antibiotic stewardship.
Sepsis screening will form part of the nursing metric audits from August 2017. Paediatrics
Sepsis teaching sessions have been delivered to 108 of the paediatric staff (total 120), this includes qualified nurses (hospital and community based), health care assistants (HCA) & nursery nurses. Plans are underway to train all new starters as they arrive and training dates have been set to capture the remaining staff members. In July 2017 drop in sessions have been increased to facilitate wider teaching.
Doctors are attending ward based scenario sessions and Birmingham Children’s Hospital is delivering RAPT training at the Good Hope Hospital (GHH) site for the multidisciplinary team.
Sepsis scenarios continue to be included on the paediatric recognition & management of the deteriorating child study day which occurs monthly.
The new Sepsis 6 form is currently with the printers, the patient safety team will assist with trust wide communication about the launch of the new form. Staff within paediatrics will receive face to face communication about the new form.

10
The new version of the Paediatric Early Warning Score (PEWS) is now in place, this includes a prompt box on the right hand side to remind staff to consider sepsis. The introduction of a carer/nurse concern box allows staff to record parental concerns regarding subtle signs of deterioration.
A paediatric sepsis tool has been developed and piloted and the plan is to launch in this quarter.
The patient safety team will be supporting the paediatric directorate with communication and raising awareness with the revised PEWS and new sepsis pathway.
The training programme to support the launch will include the lessons learned from serious incidents.
Maternity
A new maternity specific sepsis screening tool and deteriorating patient pathway has been designed along with an updated Modified Early Obstetric Warning Score (MEOWS) chart. Maternity sepsis training continues as part of the multidisciplinary mandatory Obstetric Emergency Day and since 2016 this has included scenario based sepsis sessions.
A new maternity sepsis tool and the updated MEOWS chart will be launched in August 2017 with support of midwifery trainers.
A new 1 day AIMS course for midwives was commenced in June 2017.
Series of audits into compliance with NICE Surgical Site Infection prevention quality standards including: chlorhexidine abdominal prep, prophylactic antibiotic administration, intraoperative hypothermia, antibiotic prescribing, and investigation and management of severe sepsis.
Rewriting of Caesarean section leaflet to include correct information about pre-operative hair removal and advice to patients about post-operative wound care.
Introduction of regular vaginal preparation with chlorhexidine.
Education and training on sepsis and the new pathway will be provided to new doctors at Trust induction.
Infection prevention measures including introduction of triclorsan impregnanted sutures and annual assessment of surgical scrub and gowning technique.
Results of SSI audit from Infection Control expected. How will progress be monitored, measured and reported
The national sepsis CQUIN promotes timely identification and treatment for sepsis in both admitting areas (e.g. ED, AMU) and inpatient areas. This is monitored by the Trust’s Performance team. The CQUIN has 3 key elements for audit and ultimately we need to achieve 90% in each area.
The percentage of patients who meet the criteria for sepsis screening and are screened for sepsis using the Trust recognised screening tool.
The percentage of patients defined as septic who receive their IV antibiotics within 1 hour.
The percentage of patients having a documented antibiotic review within 24-72h by a senior decision maker.
In previous years CQUIN audit data and sepsis improvement work was conducted by a dedicated sepsis nurse and associated team. Following organisational changes this

11
responsibility has passed to the individual divisions. It is worth noting that meetings have taken place between the sepsis groups at HEFT and our University Hospitals Birmingham partners. There are differences in how the organisations have defined sepsis screening and how the cohorts for audit are identified. It is unlikely that this will change in the short term and will limit the extent to which audit data can be compared. The transition from a dedicated audit team to devolved auditing by divisions has seen teething issues – some divisions have audited less than half the notes required, and overall performance is around 51% of notes reviewed. The divisional leads have been informed.
The Performance team identify the notes that require auditing. The management of notes that require auditing is by Matron for BHH Discharge Lounge in conjunction with Medical Records. The audit for part 2a and 2b is conducted by divisional nurses with the load split between them roughly proportional to patient throughput. Part 2c is overseen by the Senior Pharmacist.

12
Priority 3: Reducing surgical site infection after major surgery Background Surgical Site Infections (SSI) comprise up to 20% of all of healthcare-associated infections. At least 5% of patients undergoing a surgical procedure develop a SSI and they represent the second most common hospital acquired infection (after UTI). SSI range in severity from a spontaneously limited wound discharge within a few days of an operation to a life-threatening postoperative complication. Most surgical site infections are caused by contamination of an incision with microorganisms from the patient's own body during surgery and NICE state that the majority of SSI are preventable.3 SSI can severely affect the patient’s experience after surgery and quality of life; they are costly and are associated with considerable morbidity, extended hospital stays and increased rates of readmission. A care bundle is a small set of evidence-based practices that can be delivered together to improve patient outcomes. Based on NICE and WHO guidelines4, a SSI Bundle was established and introduced to Theatre 1 and 3 at BHH for a trial period in 2016. 170 patients undergoing major abdominal surgery were evaluated and a dedicated, independent nurse evaluated the patients for SSI. The overall SSI rate at 30 days was 29% and 28% in the standard group and the bundle group respectively. However, surgical readmissions within 30 days were 6% in the bundle group compared to 20% in the standard care group. This suggests that the trialled bundle needs to be used 7 times to prevent one readmission. A revised bundle has been developed and will be introduced with additional efforts made to ensure compliance. Performance No performance data is available for Q1 2017/18. The first audit will be undertaken in September 2017 and data will be available in Q2 following the implementation of the SSI care bundle in August 2017. Initiatives to be implemented 2017/18 An evidence-based, revised SSI Care Bundle (see Table 2 on the next page) has been developed by a multidisciplinary panel of surgeons, doctors and nurses at BHH and will be implemented into Theatre 1 and 3. Dissemination of the aims and scope of the project to stakeholders (Theatre nurses and ODPs, anaesthetists and surgeons) is underway and the SSI Care Bundle project will be implemented into Theatre 1 and 3 at BHH in August 2017.
3 https://www.nice.org.uk/guidance/cg74/chapter/introduction
4 http://www.who.int/gpsc/ssi-prevention-guidelines/en/

13
Table 2: SSI Care Bundle
PREOPERATIVE INTRAOPERATIVE POSTOPERATIVE
Pre-op attention to optimise control of Diabetes Mellitus
80% inspired O2 during surgery and, if feasible, in the immediate postoperative period for 2–6 h using a non-rebreath mask
Prophylactic topical negative pressure wound therapy should be used on primarily closed surgical incisions in highest-risk Wounds: consider prophylactic TNP therapy when the patient has BMI >35, contaminated or dirty surgery, operation duration > 3 hours
Inform elective patients to wash night before surgery
Skin clipper for body hair, rather than shave, then on table ‘social wash’ of surgical site & surrounding area prior to skin prep
Monitoring to ensure maintenance of normothermia & normal blood sugar (implementation of treatment if BM ≥10mmol/l)
Standardised wound dressing and wound care advice Protocolised treatment of SSI
Surgical Antibiotic Prophylaxis within 60 minutes prior to incision Surgical Antibiotic Prophylaxis should not be prolonged after completion of operation
Chloraprep skin prep & Plus Sutures (antiseptic coated) for torso surgery
Adult patients undergoing elective colorectal surgery should receive mechanical bowel preparation (MBP) combined with preoperative oral antibiotics. MBP should not be used alone (without antibiotics)
Surgical discipline:
Meticulous sterile technique
Consider glove & drape change at end of contaminated or dirty component of operation
Minimise traffic through theatre during surgery (lock doors from inside during surgery, use cordless phone or re-route phone line)
Enhanced patient information Continued SSI surveillance

14
How progress will be monitored, measured and reported The Trust captures data on morbidity after surgery, including readmission rates. The Trust contributes to the National Emergency Laparotomy Audit Project (which captures and openly publishes mortality figures for individual Trusts for patients undergoing emergency major abdominal surgery). The Infection Prevention and Control (IPC) team will undertake regular audit of SSI as part of the Trust-wide rolling SSI audit.

15
Priority 4: Improve infection rates for Clostridium Difficile (C Diff) and MRSA Performance MRSA Bacteraemia The national objective for all Trusts in England in 2017/18 is to have zero avoidable MRSA bacteraemia. During Quarter 1 2017/18, there have been no MRSA bacteraemias apportioned to HEFT. All MRSA bacteraemias are subject to a post infection review (PIR) by the Trust in conjunction with the Clinical Commissioning Group (CCG). MRSA bacteraemias are then apportioned to HEFT, the CCG or a third party organisation, based on where the main lapses in care occurred. The table below shows the Trust-apportioned cases reported to Public Health England for the past three financial years:
Time Period 2015/16 2016/17 2017/18 Q1
HEFT Apportioned 4 7 0
Agreed trajectory 0 0 0
Clostridium difficile Infection (CDI) The Trust’s annual agreed trajectory is a total of 64 cases during 2017/18. Each case is also reviewed to see whether there were any lapses in care – a lapse in care means that correct processes were not fully adhered to, therefore the Trust did not do everything it could to try to prevent a CDI. During Quarter 1 2017/18 HEFT reported 10 cases in total, of which 25 had lapses in care. The Trust uses a post infection review (PIR) tool with the local CCG to identify whether there were any lapses in care which the Trust can learn from. The table below shows the total Trust-apportioned cases reported to Public Health England for the past three financial years:
Time Period 2015/16 2016/17 2017/18 Q1
Lapses in care 14 18 2*
Trust-apportioned cases 61 76 10
Agreed trajectory 64 64 64
5 * At the time of reporting, the cases for June 2017 had not been reviewed for potential lapses in care

16
Initiatives being implemented in 2017/18 A robust action plan has been developed to tackle Trust-apportioned MRSA bacteraemias and CDI:
Strict attention to hand hygiene and the use of PPE (Personal Protective Equipment). Ensuring all staff are compliant in performing hand hygiene and adhere to PPE policy.
Ensuring all relevant staff understand the correct procedure for screening patients for MRSA before admission, on admission and the screening of long stay patients.
Ensuring the optimal management of all patients with MRSA colonisation and infection, including decolonisation treatment, prophylaxis during procedures, and treatment of established infections.
Ensure appropriate antimicrobial use including use of Octenisan hair and body wash.
Optimise patient outcomes and to reduce the risk of adverse events and antimicrobial resistance through prudent antimicrobial prescribing and stewardship.
Careful attention to the care and documentation of any devices, ensuring all procedures are being followed as per Trust policy.
Ensure all relevant staff are performing Saving Lives and Essential Steps (infection prevention and control) audits and acting on the results.
Providing and maintaining a clean environment throughout the Trust including the implementation of the deep cleaning programme.
Ensure all staff are aware of their responsibility for preventing and controlling infection through mandatory training attendance.
Ensure post infection review investigations are completed and lessons learnt are fed back throughout the Trust.
Continuation of the reviews by the Infection Prevention and Control team of any area reporting two or more cases of CDI.
How progress will be monitored, measured and reported
The number of cases of MRSA bacteraemia and CDI will be submitted monthly to Public Health England and measured against the 2017/18 trajectories.
Performance will be monitored via the Clinical Dashboard. Performance data will be discussed at the Care Quality Group and Infection Prevention and Control Group meetings.
Any death where an MRSA bacteraemia or CDI is recorded on part one of the death certificate will continue to be reported as serious incidents (SIs) to Birmingham CrossCity Clinical Commissioning Group (CCG).
PIR and root cause analysis will continue to be undertaken for all MRSA bacteraemia and CDI cases.
Progress against the Trust Infection Prevention and Control annual programme of work will be monitored by the Infection Prevention and Control strategic management group and reported to the Board of Directors via the Infection Prevention and Control quarterly and annual reports. Progress will also be shared with Commissioners.

17
Mortality The Trust continues to monitor mortality as close to real-time as possible with senior managers receiving daily emails detailing mortality information and on a longer term comparative basis via the Trust’s Clinical Quality Monitoring Group. Any anomalies or unexpected deaths are promptly investigated with thorough clinical engagement. The Trust has not included comparative information due to concerns about the validity of single measures used to compare trusts. Summary Hospital-level Mortality Indicator (SHMI) The NHS Digital first published data for the Summary Hospital-level Mortality Indicator (SHMI) in October 2011. This is the national hospital mortality indicator which replaced previous measures such as the Hospital Standardised Mortality Ratio (HSMR). The SHMI is a ratio of observed deaths in a trust over a period time divided by the expected number based on the characteristics of the patients treated by the trust. A key difference between the SHMI and previous measures is that it includes deaths which occur within 30 days of discharge, including those which occur outside hospital. The SHMI should be interpreted with caution as no single measure can be used to identify whether hospitals are providing good or poor quality care6. An average hospital will have a SHMI around 100; a SHMI greater than 100 implies more deaths occurred than predicted by the model but may still be within the control limits. A SHMI above the control limits should be used as a trigger for further investigation. The Trust’s latest SHMI is 96.72 for the period April 2016 – February 2017 which is within tolerance. The latest SHMI value for the Trust, which is available on the HSCIC website, is 96.58 for the period July 2015 – June 2016. This is within tolerance. The Trust has concerns about the validity of the Hospital Standardised Mortality Ratio (HSMR) which was superseded by the SHMI but it is included here for completeness. HEFT’s HSMR value is 96.31 for the period February 2017 – March 2017 as calculated by Health Informatics The validity and appropriateness of the HSMR methodology used to calculate the expected range has however been the subject of much national debate and is largely discredited78. The Trust is continuing to robustly monitor mortality in a variety of ways as detailed above.
6 Freemantle N, Richardson M, Wood J, Ray D, Khosla S, Sun P, Pagano, D. Can we update the
Summary Hospital Mortality Index (SHMI) to make a useful measure of the quality of hospital care? An observational study. BMJ Open. 31 January 2013. 7 Hogan H, Healey F, Neale G, Thomson R, Vincent C, Black, N. Preventable deaths due to problems
in care in English acute hospitals: a retrospective case record review. BMJ Quality & Safety. Online First. 7 July 2012. 3 Lilford R, Mohammed M, Spiegelhalter D, Thomson R. Use and misuse
of process and outcome data
in managing performance of acute and medical care: Avoiding institutional stigma. The Lancet. 3 April 2004.

18
Crude Mortality The first graph shows the Trust’s crude mortality rates for emergency and non-emergency (planned) patients. The second graph below shows the Trust’s overall crude mortality rate against activity (patient discharges) by quarter for the past two calendar years. The crude mortality rate is calculated by dividing the total number of deaths by the total number of patients discharged from hospital in any given time period. The crude mortality rate does not take into account complexity, case mix (types of patients) or seasonal variation.
The Trust’s overall crude mortality rate for Quarter 1 2017/18 is 1.06%, this is a slight increase on Quarter 1 2016/17 (1.01%) and Quarter 1 2015/16 (1.04%). Emergency and Non-emergency Mortality Graph
Overall Crude Mortality Graph
0
0.005
0.01
0.015
0.02
0.025
0.03
0.035
2014/15 2015/16 2016/17 2017/18 Q1
Emergency Elective

19
Selected Metrics Patient safety indicators
Indicator Data source 2015/16 2016/17 2017/18 Q1 Peer Group Average
(where available)
1a. Patients with MRSA infection/
100,000 bed days (includes all bed days from all specialties) Lower rate indicates better performance
Trust MRSA data reported to PHE, HES data (bed
days)
0.9 1.9 Not yet available
0.58 April 2016 – March
2017 Acute trusts in West
Midlands
1b. Patients with MRSA infection/
100,000 bed days (aged >15, excluding
Obstetrics, Gynaecology and
elective Orthopaedics)
Lower rate indicates better performance
Trust MRSA data reported to PHE, HES data (bed
days)
0.4 0.4 Not yet available
0.64 April 2016 – March
2017 Acute trusts in West
Midlands
2a. Patients with C. difficile infection /100,000 bed days
(includes all bed days from all specialties) Lower rate indicates better performance
Trust CDI data reported to PHE, HES data (bed
days)
13.5 16.0 Not yet available
13.77 April 2016 – March
2017 Acute trusts in West
Midlands

20
Indicator Data source 2015/16 2016/17 2017/18 Q1 Peer Group Average
(where available)
2b. Patients with C. difficile infection /100,000 bed days
(aged >15, excluding Obstetrics,
Gynaecology and elective Orthopaedics) Lower rate indicates better performance
Trust CDI data reported to PHE, HES data (bed
days)
5.9 6.8 Not yet available
15.27 April 2016 – March
2017 Acute trusts in West
Midlands
3a. Patient safety incidents
(reporting rate per 1000 bed days)
Higher rate indicates better reporting
Provisional Datix and Trust
admissions data (not validated)
349 3410
52.01
58.7 April – September
2016 Acute (non specialist)
hospitals NRLS website
(Organisational Patient Safety Incidents
Workbook)
3b. Never Events Lower number indicates better
performance
Datix 6 2 2
Not available
9 NRLS data
10 NRLS data April – September 2016

21
Indicator Data source 2015/16 2016/17 2017/18 Q1 Peer Group Average
(where available)
4a. Percentage of patient safety
incidents which are no harm incidents Higher % indicates better performance
Provisional Datix 73%11 75%12 69%
76% April – September
2016 Acute (non specialist)
hospitals NRLS website
(Organisational Patient Safety Incidents
Workbook)
4b. Percentage of patient safety
incidents reported to the National
Reporting and Learning System
(NRLS) resulting in severe harm or
death Lower % indicates better performance
Provisional Datix 0.65%13 0.614
0.6%
0.30% April – September
2016 Acute (non specialist)
hospitals NRLS website
(Organisational Patient Safety Incidents
Workbook)
11
NRLS data 12
NRLS data April – September 2016 13
NRLS Data 14
NRLS data April – September 2016

22
Indicator Data source 2015/16 2016/17 2017/18 Q1 Peer Group Average
(where available)
4c. Number of patient safety
incidents reported to the National
Reporting and Learning System
(NRLS)
Provisional Datix 15,44915 7,89916 4,394
11,155 (6 months)
April – September 2016
Acute (non specialist) hospitals
NRLS website (Organisational Patient
Safety Incidents Workbook)
15
NRLS Data 16
NRLS data April – September 2016

23
Clinical effectiveness indicators
Indicator Data Source 2014/15 2015/16 2016/17 Peer Group Average
(where available)
5a. Emergency readmissions within
28 days (%) (Medical and surgical
specialties - elective
and emergency
admissions aged >15)
%
Lower % indicates
better performance
HED data
8.07%
7.63%
7.88%17
England: 8.86%18
5b. Emergency readmissions within
28 days (%) (all specialties)
Lower % indicates
better performance
HED data
8.40%
7.99% 8.21%19 England: 7.38%20
17
April 2016 – February 2017 18
April 2016 – February 2017 19
April 2016 – February 2017 20
April 2016 – February 2017

24
Indicator Data Source 2014/15 2015/16 2016/17 Peer Group Average
(where available)
5c. Emergency
readmissions within
28 days of discharge
(%)
Lower % indicates
better performance
PMS 2 14.01% 15.15% 15.09%
Not available
This is the information
used in the Trusts LOS
Board reporting.
Latest Position:
14.82%21
6. Falls (incidents reported as % of patient episodes)
Lower % indicates
better performance
Datix and Trust admission
data
Not available 0.98% 1.23% Not available
7. Stroke in-hospital mortality
Lower % indicates
better performance
SSNAP data 13.01% 11.64% 14.16%22
Not available
21
April 2017 – May 2017 22
SSNAP data is currently being validated

25
Notes on patient safety & clinical effectiveness indicators The data shown is subject to standard national definitions where appropriate. 1a, 1b, 2a, 2b, 5a, 5b: Receipt of HES data from the national team always happens two to three months later, these indicators will be updated in the next quarterly report. 3a: The NHS England definition of a bed day (“KH03”). For further information, please see this link: http://www.england.nhs.uk/statistics/statistical-work-areas/bed-availability-and-occupancy/ 4c: The number of incidents shown only includes those classed as patient safety incidents and reported to the National Reporting and Learning System. 5a, 5b: The methodology has been updated to reflect the latest guidance from the Health and Social Care Information Centre. The key change is that day cases and regular day case patients, all cancer patients or patients coded with cancer in the previous 365 days are now excluded from the denominator. This indicator includes patients readmitted as emergencies to the Trust or any other provider within 28 days of discharge. Further details can be found on the Health and Social Care Information Centre website. Any changes in data since the previous Quality Report and due to updates made to the national HES data. 5c: This indicator only includes patients readmitted as emergencies to the Trust within 28 days of discharge and excludes cancer patients. The data source is the PMS 2 system. The data for previous years has been updated to include readmissions from 0 to 27 days and exclude readmissions on day 28 in line with the national methodology. Any changes in previously reported data are due to long-stay patients being discharged after the previous years’ data was analysed.

HEART OF ENGLAND NHS FOUNDATION TRUST
COUNCIL OF GOVERNORS
24th July 2017
Title: QUARTER 1 COMPLIANCE AND ASSURANCE REPORT
From: David Burbridge, Interim Director of Corporate Affairs
To: Council of Governors
The Report is being provided for:
Decision Y/N Discussion Y/N Assurance Y Endorsement Y/N
Purpose: To present an update to the Council of Governors of the internal and external assurance processes around compliance with NICE and local guidelines, National and local clinical audits, NCEPOD and Novel Techniques.
Key points/Summary:
Draft CQC report was received in June and draft factual accuracy check
undertaken and returned to CQC. Final report awaited
Quarterly Divisional Quality Governance reports now include newly published
NICE guidance or updates
63 National Audits have been identified as applicable for 2017/18 and currently
the Trust is participating in 60
Recommendation(s):
The Trust Board is asked to consider the information set out in this report
Assurance Implications:
Board Assurance Framework
Y BAF Risk Reference No.
Performance KPIs year to date
N Resource/Assurance Implications (e.g. Financial/HR)
N
Information Exempt from Disclosure
N If yes, reason why.
Identify any Equality & Diversity issues
Which Committees has this paper been to? (e.g. AC, QC, etc.)
Audit Committee

Page 2 of 6
HEART OF ENGLAND NHS FOUNDATION TRUST
COUNCIL OF GOVERNORS
24th July 2017
COMPLIANCE AND ASSURANCE REPORT
PRESENTED BY THE INTERIM DIRECTOR OF CORPORATE AFFAIRS 1. Purpose
The purpose of this paper is to provide the Council of Governors with information regarding internal and external compliance.
2. Trust Compliance with Regulatory Requirements
2.1 Care Quality Commission (CQC)
The Trust has received the draft CQC Inspection report. Factual accuracy checks have been completed and returned to the CQC.
The publication date of the final report is not currently known.
2.2 NICE GUIDANCE
Q1 Position In Q1 2017 the new Quarterly Divisional Quality Governance Reports have included all of the NICE guidance published or updated during the quarter. This has provided the Divisional Management Teams with an updated position in relation to their NICE guidance and will enable them to take appropriate actions to ensure compliance. A baseline has been produced by the Clinical Audit Team detailing the status of all NICE guidance published prior to April 2017. The baseline will be distributed to Divisions to enable updates on outstanding actions and further assurance of implementation to be reported. The Clinical Audit Team has reviewed the process for dissemination of NICE Guidelines to strengthen assurance gained in relation to implementation of newly published and updated guidance.
The Clinical Audit Team will communicate newly published/updated NICE
Guidance via email to Divisional Directors within 5 working days of publication by
NICE
The Divisional Directors will be responsible for cascading the guidance to the
relevant directorate leads for local dissemination within 10 working days of
publication

Page 3 of 6
Directorate leads will review the guidance and respond via email to
[email protected] within 30 working days of publication. Information
required in the response includes:
Status
Completed NICE Baseline Assessment Tool
A completed risk assessment if the guidance will not be implemented.
It is proposed that the Clinical Audit Team will report divisional NICE guidance status monthly via the Divisional Governance Meetings where directorate level data will be provided and assurance will be sought in relation to implementation.
NICE Guidance published/updated between 01/04/17 and 30/06/17
CG
(C
lin
ical
gu
ideli
ne
s)
DG
(D
iag
no
sti
cs
gu
ida
nce)
ES
(E
vid
en
ce
su
mm
ary
)
HS
T (
Hig
hly
sp
ecia
lised
tech
no
log
ies
gu
ida
nce)
IPG
(In
terv
en
tio
n
al
pro
ced
ure
s
gu
ida
nce)
MIB
(Me
dte
ch
inn
ov
ati
on
b
riefi
ng
)
MT
G
(Me
dic
al
tech
no
log
ies
gu
ida
nce)
NG
(N
ICE
Gu
ideli
ne
s)
QS
(Q
uali
ty
Sta
nd
ard
s)
TA
(Te
ch
no
log
y
ap
pra
isal
gu
ida
nce)
Grand Total
Apr-17
2 1 2 1 1 2 4 13
May-17
2 2 3 1 2 10
Jun-17
1 1 2 1 4 3 1 1 8 12 34
Grand Total
5 1 3 1 8 4 1 5 11 18 57
*June guidance was issued 03/07/17
3. Trust Compliance with External Visits/Peer Reviews
The External Agencies Policy was presented at June’s Policy review Group following alignment with UHB’s policy. Following minor changes this will be presented to July Board for ratification. A full summary of 2017 Q1 and Q2 external visits will be provided at the next Audit Committee in October.
4. Clinical Audits
4.1 National Audits:
The 2017/18 national audit programme has been incorporated into the trust wide forward audit programme (FAP). There are 63 national audits included in the FAP. The process for monitoring participation and implementation of actions is detailed in the additional agenda item relating to the Forward Audit Programme to be presented to this committee today.
At the time of this report, the Safety and Governance Department have been notified that the following national audits, reportable within the 2017/18 Quality Accounts, will not be participated in due to lack of capacity within the associated directorates:

Page 4 of 6
- NJR – Data Quality Audit
- National Comparative Audit – Red Cells in Platelet Transfusion (Adult Haematology
Patients)
- National Diabetes Audit (Core Audit)
Directorates who are unable to participate in national audits have been requested to record this on their risk registers and escalate and discuss with their Divisional Management Team.
4.2 Local Audits:
A total of 74 audits, with proposed start dates between 01 April 2017 and 30 June 2017, were logged on the clinical audit database. A divisional summary is given below:
Divisional Summary - Audits logged on the Clinical Audit Database with proposed start dates between 01/04/17 and 30/06/17:
Approved Declined Open/
submitted Signed-Off Grand Total
Division 1 11 1 3 1 16
Division 2 11
5
16
Division 3 8 1 5
14
Division 4 2
4
6
Division 5 10
12
22
Grand Total 42 2 29 1 74
Work has been completed to close clinical audits dated pre 2014 that were logged on the clinical audit database. There are a number of pre-2014 audits requiring further discussion with directorate audit leads prior to closure.
5. National Confidential Enquiry into Patient Outcome and Death (NCEPOD)
The assurance process in relation to participation in NCEPOD studies and implementation of associated recommendations is currently being reviewed by the NCEPOD Ambassador and Clinical Audit Team. This will be reviewed alongside UHB processes and procedures and incorporated into an overarching National Guidance and Recommendations Policy. There have been no new NCEPOD reports published in Q1 2017/18.
6. Novel Techniques and Interventional Procedures (NTIPs)
The policy for the introduction and development of novel techniques and interventional procedures has been reviewed. Following review, the policy was approved by Chief Executive’s Group on 16 May 2017.
The table below shows the approval status of all NTIPs that have been reviewed by the Trust since December 2004.

Page 5 of 6
Approval status
Division Directorate Application form needs to
be signed. Proposer did not wish to
continue with application.
Disbanded No Under review
by NTIP Group
Yes Grand Total
Div 1
Anaesthetics
1
1 2
Microbiology & Bacteriology
1 1
Radiology
1
7 8
Total
2
9 11
Div 2 Obstetrics & Gynaecology
1
1
2
Total
1
1 2
Div 3
Cardiology
1 1
Respiratory Medicine
2 2
Total
3 3
Div 4
Diabetes
1 1
Elderly care
1 1
Haematology
1 1
Therapies
1 1
Total
4 4
Div 5
Colorectal surgery
1 1
ENT
1 1
Gastroenterology
2 2
General Surgery 1 1
7 9
Ophthalmology
3 3
Thoracic Surgery
8 8
Trauma & Orthopaedics
1 1 2
Urology
7 7
Urology & Obs and Gynae
1 1
Vascular
1
5 6
Total
1 2
1 36 40
Trust Total
1 2 3 1 53 60
7. Clinical Guideline Compliance
A review of all the guidelines currently available on the Trust’s SharePoint site has identified that there are some specialities that contain uploaded ‘Guidelines’ which are documents with links to external sites containing a list of new/updated/overdue guidelines that may potentially have not been through the trust approved ratification process.
A scoping exercise is currently being undertaken to identify these specialities, which of these guidelines are appropriate, due to be reviewed and to be held locally if necessary. Those guidelines with individual links have been omitted from this report.

Page 6 of 6
Divisional Overview
Division WITHIN DATE UPCOMING OVERDUE Grand Total
Clinical Support Services 17 0 6 23
Emergency Care 29 0 20 49
Medical Specialties 40 0 32 72
Surgery 2 0 14 16
Women's & Children's 65 0 49 114
Grand Total 153 0 121 274
Directorate level information in relation to guideline compliance is provided to divisions and directorates via Quality Governance Reports on a quarterly basis.
8. Recommendation
The Council of Governors is asked to accept this report.
David Burbridge July 2017 Interim Director of Corporate Affairs

1
COUNCIL OF GOVERNORS
MONDAY 24 JULY 2017
Title: HEALTH AND SAFETY REPORT – Annual Report 2016/2017
Responsible Director:
David Burbridge, Director of Corporate Affairs
Contact: Sara Sharratt, Lead - Health And Safety
Purpose: This report provides an update with the management of health and safety for the period April 2016 – March 2017
Confidentiality Level & Reason:
None
Key Issues Summary:
Compliance against key requirements the Trust’s Health And Safety Policy remains robust, with all areas covered by a nominated manager and a risk register.
The focus for the health and safety team over the reporting period has been:
Continued support to operational colleagues in providing health and safety training, advice, inspection and audit;
Preparation for external visits (as required) including HSE inspection;
Ensuring compliance with Trust Health And Safety Policy;
Increased support to investigating managers and handlers in order to improve learning from incidents;
Recommendations: The Council of Governors are asked to:
note the contents of the report and associated actions.
Approved by: David Burbridge, Director of Corporate Affairs

2
1 Introduction
This report provides analysis of the Trust health and safety programme for 2016-2017.
The Health and Safety at Work etc Act 1974 provides a legislative framework to promote, stimulate and encourage high standards of health and safety at work. In particular it requires organisations to provide and maintain:
A Health and Safety Policy
Systems to manage and control risks in connection with the use, handling storage and transport of articles and substances
A safe secure working environment, including maintenance of access to and egress from premises
Safe and suitable plant, work equipment and systems of work
Information, instruction, training and supervision
Adequate welfare facilities
The underpinning legislation is enforced by the Health and Safety Executive (HSE) who ensure health and safety in organisations is regulated. The Trust fulfils its legal responsibility for health and safety by:
Employing a team of professionals to provide advice and support to managers and staff
Offering and facilitating a range of work based health and safety training in a variety of different ways
Measuring compliance with health and safety policies through health and safety support visits, safety reports, inspections and audits
Consulting, in various ways, with the workforce in relation to health, safety and welfare.
The Health and Safety team establishment consists of
A Lead for Health and Safety,
A Health and Safety Advisor
A Lead Local Security Management Specialist
2 Health and Safety Officers
The aim of the team is to embed a health and safety framework across the Trust and they are responsible for: a. Advising managers, safety representatives and staff on matters of health and safety at work;
b. Developing, implementing health and safety policies and procedures to improve the management of health and safety across the Trust;

3
c. Developing and delivering bespoke health and safety training courses as appropriate
d. Providing information and corporate data analysis in respect of Trust-wide health and safety compliance.
The Health and Safety Team report to the Health & Safety Group.
The reduction in team resources during the period October – December 2016 has had an impact on the service that the team has been able to provide. The annual work plan and several work-streams were adjusted to mitigate the resource risks detailed above.
2. Provision of advice and support Members of the team have utilised a variety of forums to raise the profile of health and safety, which include:-
Actively participating in a wide range of operational safety groups, in clinical and non clinical directorates
Representation at the Trust Safety Group
As requested, by the project design teams, attending project group meetings to ensure that safety and security risk management is incorporated at the planning stages
Working with managers to address specific safety hazard/risk issues identified pro-actively, via local health and safety visits, or as a result of incidents.
Utilising informal discussions to provide advice to resolve local issues
Responding to requests via telephone or email to problem solve in a timely manner.
Responding to safety concerns raised during training sessions
3. Education
The health and safety training programme, developed and facilitated by the team does not form part of the mandatory training set. The programme includes:-
Managers health and safety responsibilities (short awareness course)
Risk Assessment Workshops
Security awareness sessions
Participation in the delivery of PREVENT training
COSHH (Control of Substances Hazardous to Health) risk assessment workshops
DSE (Display Screen Equipment) risk assessment workshops In November 2016 the Conflict Resolution Training (both initial course and refresher course) became part of the mandatory training set. Moodle packages have been developed and staff are encouraged to complete the on-line moodle training as part of their mandatory training. In addition, face-to-face sessions still continue to be delivered by the team.
In addition to the programmes advertised, the team have:-
Facilitated health and safety sessions on the Health Care Assistant induction programme on a regular basis throughout the year.
Routinely facilitated a health, safety and security awareness lecture on the Student

4
Nurse Induction programme.
Participated in the Volunteers Induction programme Two further on line training modules have been developed in year:
Conflict Resolution Refresher Training
COSHH awareness training There are two further training modules currently being developed:
DSE awareness
Managing health and safety Training figures are incorporated into the report presented to the Trust Health and Safety Group.
The completion of Moodle Packages for the Trust as a whole in the subjects supported by H&S are below:
Compliance with the mandatory training for the year 2016/2017 is as follows:
Health and Safety Training 80.52%
Conflict Resolution Training (initial and refresher sessions) 59.21%
4. Risk assessment The team has continued to provide advice and support managers to complete risk assessments during 2016/17. Similar risks to previous years have been identified, including:
Work stations not meeting the minimum requirements of the Display Screen Regulations.
Risks associated with the potential to expose staff, visitors and patients to hazardous substances.
Unsuitable working environment due to lack of available space.
5. Investigations
The team has continued to follow up incidents reported under the health and safety and security categories. Overall trends are incorporated into the regular report that is presented to the Trust
Course Name YTD Total Category Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Conflict Resolution - Initial Training 4622 MANDATORY 51 28 48 41 15 26 207 1744 692 774 499 548
Conflict Resolution - Refresher 1515 MANDATORY 8 76 603 220 259 170 179
CoSHH Awareness - 2017 228 D6 90 47 18 15 17 8 5 12 5 11
Health & Safety Awareness 2017 2332 MANDATORY 166 106 123 74 40 59 173 638 238 320 282 2794 8697 217 134 261 162 73 108 473 2993 1155 1365 956 1017

5
Safety Group. Incidents reported under the security category are reported to the Security Group.
6. Projects/initiatives
The team has attended project meetings for refurbishment and new build programmes within the acute settings during the period.
7. Raising awareness
Due to the limited resources within the team, it has not been possible to undertake dedicated campaigns this year. However, a variety of communication methods have been used to raise awareness about safety which include:-
Articles within the monthly Trust Newsletter.
Communication during visits to local areas to raise awareness of the importance of safety and training available.
8. Policy review
The policies owned by the team have been reviewed in line with the schedule, to ensure that they remain valid and fit for purpose.
9. Environmental hazard spotting
Team inspections
The programme of environmental health and safety inspections has continued during 2016/17. Environmental hazards identified during the visits are reported back to local managers and trends are incorporated into the quarterly health and safety report to Health and Safety Group.
As a result of the decrease in resources available within the team, the schedule was adjusted in November 2015:-
The programme was extended to an 18 month rolling programme
The standard security risk assessment questions have been incorporated into the inspection pro-forma. This has enabled the Lead Local Security Management Specialist (LSMS) to participate in the inspection programme. It has also ensured that the security element is maintained for clinical areas.
The LSMS has visited several wards with the Head Nurses to assess the security arrangements for patient property and medication.
A total of 84 areas were visited across the Trust during the year and the inspection programme was completed as planned.

6
10. Local inspections Completing regular local environmental health and safety inspections promotes timely management of hazards, which in turn promotes a safe, healthy environment for staff and patients. Managers are requested to forward the completed inspection tool to the health and safety team so that themes and cross site issues can be identified. A number of areas regularly complete and return the inspection forms however, compliance in other areas continues to be poor. Regular reminders are sent to Safety Champions and Ward Managers. The Corporate Nursing team are also provided with details of areas that have not returned. To help support the teams in delivering their responsibilities under health and safety, a revised self-assessment form was introduced with from April 2017. The focus is more on the management of health and safety as well as the environmental issues ensuring that a robust system will be implemented to support the managers of areas in understanding their roles and responsibilities within the safety sphere. 11. Compliance
Compliance against health and safety legislation is monitored through day to day activities. Risks identified are reported to the appropriate groups in line with the Risk Management Policy.
The security self assessment to NHS Protect was completed on schedule. Actions identified as a result of the assessment were incorporated into the team annual work plan. The assessment provided assurance of compliance with the standard.
The Lead for Health and Safety is the single point of contact to receive all Safety Alerts received via the Department of Health Central Alert System (CAS):-
CAS has been updated in accordance with the Trust policy
Monthly status reports are circulated in line with policy to, the Executive Directors, Operational Managers, Head Nurses, Matrons and Heads of Departments, to ensure that they are kept informed of the status of alerts that are open and being managed.
The Lead for Health and Safety continues to liaise with alert managers and escalate potential delays.
A total of 129 safety alerts were issued via the CAS from 1st April 2016– 31st March 2017. In addition to the new alerts received during the year, a total of 5 have been carried forward to 2017/2018. Out of the 129 alerts, 124 were managed and closed within the deadline for completion dates. 5 have been carried forward to 2017/2018 remain open but are within the deadline for completion dates.

7
Reference Alert Title Deadline
NHS/PSA/RE/2016/006
Nasogastric tube misplacement; continuing risk of death and severe harm
COMPLETE
NHS/PSA/D/2016/009 Reducing The Risk Of Oxygen Tubing Being Connected To Air Flow meters
4 July 2017
NHS/PSA/RE/2017/001 Resources to support safer care for full-term babies
23 August 2017
MDA/2017/003 Alaris® Syringe Pumps (Gh, Cc, Tiva &Amp; Pk Models) ? Risk Of Uncontrolled Bolus Of Medicine
23 April 2017
MDA 2017/04
Cardiosave Hybrid intra-aortic balloon pump (IABP) and Cardiosave Rescue IABP – damaged lithium ion batteries may give off smoke, a bad smell or produce sparks
7 June 2017
12. Reports to Health & Safety Executive (HSE)
The Trust reported 54 incidents to the Health and Safety Executive (HSE) in accordance with the Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 2013 (RIDDOR) during the reporting period. The chart below represents the amount of RIDDOR reports for the period with the reason for the report.
The highest reported incidents were, 31.48% musculoskeletal injuries, 24.07% for slips, trips and falls with inoculation/sharp injuries at 22%.
RIDDOR reportable incidents continue to be closely monitored within DATIX and any trends identified for action. All reportable incidents complete a local investigation and monitored through the divisional groups and reported through to Health and Safety Group.
Two of the RIDDOR reports in relation to Occupational Dermatitis have resulted in the Health and Safety Executive requesting a visit to look in more detail at the occupational health, health surveillance and monitoring of health and safety within the Trust. This visit will take place in July.
0
1
2
3
4
5
6
7
8
Q1
Q2
Q3
Q4

8
13. External visits by the (HSE)
The HSE made a visit to the Trust in June 2016: investigation a fall from height at the Solihull hospital site by an employees of the Facilities/Estates team. Following their investigation a notice of contravention was served in relation to breach of HSAW Section 2(1) and the Working at Height Regulations 4(1). An action plan was implemented and the review visit in August 2017 saw the contravention being discharged. No further action was taken.
14. Incidents – Most Reported
The table below shows that the three most frequently reported health and safety incidents and the three most frequently reported security incidents. The number of health and safety incidents reported in each of these categories has generally remained constant.
Category – Health and Safety Number of recorded incidents April 2016-March 2017
Slips trips and falls 253
Impact/struck by moving object 124
Sharps inoculation injuries 169
Category - Security
Aggressive and verbal abuse – staff 356
Physical assault – staff 283
Absconded patients 178
Actions: Inoculation
The Sharps Group (SG) was set-up in 2015 to: monitor and evaluate divisional and local initiatives to reduce the number of inoculation incidents; share best practice; improve data quality; review the information available (via DATIX); implement staff engagement initiatives to benchmark levels of understanding and; review training provision. The SG also led on compliance with the Health and Safety (Sharps Instruments In Healthcare) Regulations 2013 and the introduction of safer sharps throughout the Trust. It meets bi monthly and is chaired by the Head of Risk and Compliance who then reports to Trust Infection and Prevention Committee.
All inoculation incidents are reviewed by the H&S Team and contact made with the investigating managers/handler regarding investigations where appropriate. A sharps investigation tool is now requested to look at root causes and is attached to the Datix form. This is monitored by the Health and Safety Team and reported to Health and Safety Group.
Actions: Impact
Impact incidents include the subcategories; struck against something e.g. furniture, fittings etc; struck by moving/flying object and; struck by moving vehicle. All impact incidents are reviewed by the H&S Team and contact made with the investigating managers/handler regarding investigations where appropriate.

9
Actions: Slips/Trips
Slips/trips are considered a priority for the health and safety team and a schedule of environmental inspections was implemented throughout 2016/12017. This supports the quarterly environmental self assessments undertaken by the wards/departments. All incidents are reviewed by the health and safety team and local investigations are undertaken with/by the manager/handler where appropriate.
Actions: Physical and non-physical V&A incidents All incidents are reviewed and monitored by the Local Security Management Specialist and the Health and Safety Team. All staff involved in incidents receives a support letter outlining actions which can be taken, what support and policies are available to support them. There is a system in place to warn patients and relatives about their behaviour (yellow cards) or if required to exclude (red cards) trust wide patients/relatives who are constantly exhibiting threatening or unacceptable behaviour to staff. During 2016/2017 there were 6 Red cards issued and 24 yellow cards. 15. The Way Forward for 2017/18
The health and safety team have developed a work plan for 2017/18.
The plan will be reviewed at regular intervals during the year to take into account recent changes to the organisational structure and local changes within the directorate as they occur.
The introduction and implementation of a training programme for line managers to ensure roles and responsibilities in relation to health, safety and welfare are robust across the sites will be rolled out.
Focus on security inspections in conjunction with the Head Nurses will continue to be implemented to help focus on specific security issues.
16. Recommendation
The Council of Governors is asked to note the contents of this report and associated actions.
David Burbridge Director of Corporate Affairs