Embed Size (px)
Citation preview

M O L M E D 2 0 : 3 8 1 - 3 8 9 , 2 0 1 4 | H A N S S O N | 3 8 1
INTRODUCTIONMy decision to go to medical school
was based in equal parts on a desire tohelp people, a wish to have a meaning-ful job and the challenge to get into aprogram that was, at the time, the mostcoveted one in the Swedish universitysystem. I had dreams of becoming athoughtful psychiatrist, a decisive cardi-ologist or perhaps a doctor for the poorsomewhere in a developing country. I made it to and through medical school,but I fulfilled none of these dreams.After a short time in internal medicine,the research bug had bitten me and I be-came a physician-scientist, with the em-phasis gradually moving toward the lat-ter part of the term.
I grew up in a small town in the prov-ince of Bohuslän on the Swedish NorthSea coast. My dad ran the local newspa-per of the town, and my mum was anurse at its small hospital. The town ofLysekil was dominated by the sea sur-rounding it. Commercial fishing, her-ring canneries, and a factory producingboat engines were its main activities. Insummer, the coast was invaded bytourists from the big cities—Stockholm,Göteborg and Oslo. When the seawarmed up, we went swimming, canoe-ing and sailing. Life was magical for ateenager—sailing in the day and party-ing at night. Winds from the big worldbrought new influences and newsounds, such as the Beatles, Bob Dylan,
world politics and student protests. The1960s were an exciting time.
MEDICAL SCHOOL AND HOW TOSURVIVE IT
The curriculum in medical schoolstarted with anatomy. It was a night-mare. We were expected to memorizeLatin names for hundreds of structureson bones—fossae, sulci, capita and so on.We were incessantly told that knowledgeof all these anatomical details was ab-solutely necessary for any clinical doctor.When I started working as a clinicianmyself, I found this kind of descriptiveanatomy completely useless. In real life,bones have tendons and muscles at-tached; they are not bare except in thecemetery.
One day, I saw a poster in the corridoroutside the anatomy department. Theneighboring department of histology in-vited students to an evening with infor-mation about medical research. We talkedabout it over a beer in the park when wewere skipping another boring hour ofanatomy, and decided to attend. Thatevening, we met other kinds of teachers.They were scientists and told us about
A Journey in Science: Medical Scientist in Translation
Göran K Hansson
Karolinska Institute, Department of Medicine Solna and Center for Molecular Medicine at Karolinska University Hospital,Stockholm, Sweden
Real innovations in medicine and science are historic and singular; the stories behind each occurrence are precious. At Mo-lecular Medicine we have established the Anthony Cerami Award in Translational Medicine to document and preserve these his-tories. The monographs recount the seminal events as told in the voice of the original investigators who provided the crucial earlyinsight. These essays capture the essence of discovery, chronicling the birth of ideas that created new fields of research; andlaunched trajectories that persisted and ultimately influenced how disease is prevented, diagnosed and treated. In this volume,the Cerami Award Monograph is by Göran K Hansson, MD, PhD, Karolinska Institute. A visionary in the field of cardiovascular re-search, this is the story of Dr. Hansson’s scientific journey.Online address: http://www.molmed.orgdoi: 10.2119/molmed.2014.00092
Address correspondence to Göran K Hansson, Karolinska University Hospital, Center for
Molecular Medicine L8:03, SE-17176 Stockholm, Sweden. E-mail: [email protected];
Phone: +46-8-5177-6222.
Submitted May 1, 2014; Accepted for publication May 1, 2014; Epub (www.molmed.org)
September 5, 2014.
Anthony Cerami Award in Translational Medicine
3 8 2 | H A N S S O N | M O L M E D 2 0 : 3 8 1 - 3 8 9 , 2 0 1 4
A M E D I C A L S C I E N T I S T I N T R A N S L A T I O N
medical problems that needed to besolved, pointing out methods for solvingthem. And they wanted us to join them inthat endeavor. We immediately signed up.
Our first experiment was not a success.My classmate, Per Elias, and I joined aneurobiology project to analyze biochem-ical changes in the cerebellum after alco-hol exposure. Our main finding was thatthe cerebellum is completely devoid ofprotein. Neurobiology was not ready forsuch a paradigm shift, and we decided tomove to other fields.
In the laboratory of Sören Björkerud, Iheard about cardiovascular disease, themajor cause of death in our society. Sörenwas an enthusiastic teacher. It was fasci-nating to hear him explain how the cellsof the blood vessels form a barrier to pre-vent cholesterol from accumulating andhow that barrier could be damaged bythe forces of blood pressure, leading toatherosclerosis and ultimately to myocar-dial infarction.
I was assigned to work with GöranBondjers, a young physician-scientist
who had just finished his PhD in Sören’slab. Göran taught me how to dissect ar-teries, analyze cholesterol in tissues andlabel dividing cells with radioactive iso-topes. I was learning the craft of science(Figure 1).
Life was intense. There were lecturesand classes in physiology, pharmacologyand pathology in the mornings and after-noons, work to do in the research lab inthe evenings, and books to read at night.And there were a thousand things toprotest against in endless demonstra-tions, ranging from the war in Vietnamto the new curricula in universities. Mygirlfriend (and future wife), Margareta,who was studying psychology, and Iwere busy all the time.
And things were to get even busier.Margareta was pregnant, and we hadn’teven finished our educations. Our son,Emil, was born the day I had my majorexam in internal medicine. Axel followed3 years later. Margareta switched frompsychology to physiotherapy when it be-came obvious that job opportunitieswere dwindling in psychology. I contin-ued in medical school and could evencontinue with part-time research, thanksto an understanding wife and a modestneed for sleep.
IMMUNITY IN BLOOD VESSELS?Immunology immediately captivated
me in medical school. I took immunol-ogy courses as part of my PhD programand learned about antibodies, vaccina-tion and memory. I was fascinated by thefact that this powerful defense systemwas patrolling our bodies, next to theblood vessels where atherosclerosis de-veloped. “How would the immune sys-tem react to a pathology that builds upin its immediate vicinity?” I asked my-self. “Someone must know,” I reasoned,and I went to the library and read all thetextbooks and review papers I could findabout cardiovascular pathology. Not aword was said about the immune sys-tem. I asked Göran Bondjers. His answerwas “Go and find out.”
I knocked on the door of the microbiol-ogy department, and they allowed me to
come and learn. The head of the depart-ment was the famous immunologist,Örjan Ouchterlony, who had invented theimmunodiffusion method for analyzingantigens. Much of the work in the depart-ment still dealt with the “Ouchterlonytechnique,” but they were also doing im-munofluorescence microscopy. I stainednormal rabbit arteries for immunoglobu-lins and complement factors and foundnothing. But when I applied the samestaining protocol to atherosclerotic arter-ies of fat-fed rabbits, there were tons ofIgG and C3 in the lesions! Something wasgoing on. There was an immune activityof some kind in the atherosclerotic lesion.For the first time, I had made a discovery.
POSTDOCTORAL STUDY IN A MECCAOF VASCULAR BIOLOGY
I finished my PhD thesis, applied for apostdoctoral fellowship and contactedscientists at the University of Washingtonin Seattle, which was a Mecca for vascu-lar biology and atherosclerosis research. Iwas overwhelmed with joy when I wasawarded a Fogarty International Postdoc-toral Fellowship from the U.S. NationalInstitutes of Health and could move toSeattle with my little family.
Seattle was a fun city and the Univer-sity of Washington was everything a re-search university should be. I workedwith Steve Schwartz, an eccentric, excit-ing and intellectually brilliant scientist inthe pathology department. Steve’s pas-sion was cell kinetics, and he could arguefor hours about cell cycles and popula-tion dynamics in the endothelium. Nextdoor was Earl Benditt, the former chair-man of the department, who had pro-posed that atherosclerosis was a mono-clonal population of smooth muscle cells.The new chairman, Russell Ross, had an-other theory—that atherosclerosis wascaused by the platelet-derived growthfactor, which was released when plateletsaggregated at sites of arterial damage.Earl and Russell would never reach aconsensus, but some kind of working re-lationship developed, with Earl being theking of vascular biology in Seattle andRussell in the rest of the world.
Figure 1. Göran Hansson smashes someglassware while trying to isolate organelles.Caricature by student colleague TomBjörnheden, 1980; reproduced with permis-sion from him.

A N T H O N Y C E R A M I A W A R D I N T R A N S L A T I O N A L M E D I C I N E
M O L M E D 2 0 : 3 8 1 - 3 8 9 , 2 0 1 4 | H A N S S O N | 3 8 3
The young generation of cardiovascu-lar scientists was a great crowd. RonHeimark, a skillful biochemist, patientlytaught me how to run SDS (sodium do-decyl sulfate) gels. Alec Clowes was apromising young vascular surgeon whodid beautiful work on arterial restenosis,together with his wife Monica, and AlanChait, a brilliant endocrinologist study-ing lipoprotein metabolism. I shared anoffice with an expatriate Brit, MichaelReidy, at the time of the Falklands warand was offered advice on military strat-egy every day.
Our family had a good time. We madelots of friends, some with whom we stillkeep in touch. Weekends were spentdoing excursions into the fantastic naturesurrounding Seattle, with the Olympicpeninsula, the Cascade Range and thePacific Ocean. In the summer of 1982, wedrove down the Pacific coast, camping inOregon and California and having awonderful time. I came back to Swedenin 1983 as a full-fledged cell biologist. Iknew how to grow endothelial cells andsmooth muscle cells, how to analyzegrowth factors and how to assess cellproliferation.
WHERE DO THE CELLS IN THE PLAQUECOME FROM?
At this time, the cellular composition ofthe atherosclerotic lesion was still un-known. It was a question everyone in thefield was asking. While most pathologiststhought of it as a smooth muscle lesion,histochemical data pointed to a contribu-tion of macrophages. In the 1950s, JohnPoole and Howard Florey in Oxford hadidentified macrophagelike cells, possiblyemanating from blood monocytes, accu-mulating in the artery wall of fat-fed rab-bits. Twenty-five years later, Ross Gerrityin Cleveland described how monocytesentered the arterial intima of fat-fedswine, and Bob Wissler in Chicago de-tected macrophages in lesions of nonhu-man primates. Russell Ross was settingup a heroic experiment, by using the newmonoclonal antibody technology to makeantibodies against homogenates of le-sions and then identifying what these an-
tibodies recognized to characterize thefeatures of the cells forming the lesion. I thought I had a better idea and startedtesting it as soon as I came back to Göteborg.
My idea was to use well-characterizedantibodies to known cell types, applythem to human atherosclerotic lesionsand find out if they stained any of thecells. From the immunology literature, I knew about the T- and B-cell–specificantibodies, later to be known by their CDnumbers, and my friend Giulio Gabbianiin Geneva sent us antibodies to smoothmuscle cell components. But wherecould we find human arteries? Autopsymaterial was probably too degraded, sowe needed surgical material.
My clinical training helped solve theproblem. As part of my 21-month intern-ship at Sahlgrenska University Hospitalin Göteborg, I worked for 4 months invascular surgery. I was a lousy surgeon,but I learned a lot and had a good time.The chief vascular surgeon, Jan Holm,recommended me to use endarterectomymaterial from the carotid artery. Evenbetter, Jan offered to provide carotid en-darterectomies for our studies. We struckup a collaboration that lasted throughoutmy years in Göteborg and led to a greatfriendship as well as an exciting scien-tific endeavor. We were joined by anMD/PhD student, Lena Jonasson, nowprofessor of cardiology at LinköpingUniversity. Always enthusiastic, Lenaprepared the surgical specimens, cut thesections and did the immunostaining.When I came back to the lab in theevening after a day in the clinic, welooked at the results in the fluorescentmicroscope together.
INFLAMMATION LEAVES HLA TRACKSThe expected suspects were there, but
we were also in for some surprises. Vas-cular smooth muscle and endothelialcells did not account for more than abouthalf of all cells in the lesions. Suspectingthat the rest might be macrophages, weapplied an antibody that was supposedto stain macrophages, OKIa1. But the re-sults were astonishing. This antibody
stained the majority of cells in the plaque(Figure 2) (1).
When looking into the details, wefound that this antibody recognizedHLA-DR, a major histocompatibilitycomplex (MHC) protein that presentsantigen to CD4+ T cells. HLA-DR was ex-pressed not only by macrophages butalso by a significant proportion of thesmooth muscle cells as well as some en-dothelial cells. Therefore, OKIa1 was nota macrophage marker but a marker ofantigen-presenting capacity. But how did
Figure 2. HLA-DR expression in the humanatherosclerotic plaque. HLA-DR protein(green) is expressed by most cells in theatherosclerotic plaque (right side) but notin the normal artery adjacent to it (leftside). This fluorescent micrograph of a sec-tion from a human endarterectomy sam-ple led us to propose that atherosclerosis isan inflammatory disease driven by a localimmune reaction. Reproduced from (42): Hansson GK; Jonasson L. The discovery of cellular
immunity in the atherosclerotic plaque. Arte-
rioscler. Thromb. Vasc. Biol. 2009;29(11):1714–7.
Also, see (1):Expression of class II transplantation antigen on vas-
cular smooth muscle cells in human atherosclerosis.
L Jonasson, J Holm, O Skalli, G Gabbiani, G K Hansson
Published in Volume 76, Issue 1
J Clin Invest. 1985; 76(1):125–131 doi:10.1172/JCI111934

3 8 4 | H A N S S O N | M O L M E D 2 0 : 3 8 1 - 3 8 9 , 2 0 1 4
A M E D I C A L S C I E N T I S T I N T R A N S L A T I O N
HLA-DR end up on smooth muscle cells?We could never detect it in normal arter-ies, only in atherosclerotic plaques. It wasalready known that interferon-γ, a proin-flammatory cytokine produced by acti-vated T cells, could induce HLA-DR oncertain target cells. But T cells, the key ac-tivators and regulators of adaptive im-munity, were not supposed to be in-volved in atherosclerosis. We were,therefore, both surprised and excitedwhen we found that about 10% of allcells in human plaques were positive forthe T-cell marker OKT3 (recognizing CD3protein). And when we stimulatedsmooth muscle cells in culture with inter-feron-γ, they started to express HLA-DR.
The time was ripe for proposing a hypothesis:
1. T cells are recruited to atheroscleroticlesions.
2. They are activated by an (unknown)antigen.
3. When activated, these T cells producethe cytokine interferon-γ that activatesmacrophages and smooth muscle cells.
4. Cytokine-activated cells express im-mune/inflammatory genes includingHLA-DR.
5. Inflammation promotes atherosclerosis.
We thought this was important enoughto justify publication in Nature. Unfortu-nately, the editors of that revered journaldid not agree with us, and the manuscriptcame back by return mail. We had moresuccess with the Journal of Clinical Investi-gation, although their reviewers de-manded one control experiment after an-other, delaying the publication for morethan a year. They also forced us to tonedown our conclusions and hypothesis;therefore, the paper that came out in July1985 was not as exciting as the first ver-sion of the manuscript (1).
A follow-up paper was written, inwhich we provided a map of the cell pop-ulations in the plaque. It was a straight-forward, descriptive paper that was published in Arteriosclerosis (now Arte-riosclerosis, Thrombosis, and Vascular Biology[ATVB]) in March 1986 (2). Because thepaper did not contain the immunopatho-
logical concepts and proposals of thepaper published in the Journal of ClinicalInvestigation, it was more appealing to thecardiovascular community. Our findingswere soon confirmed by the Ross teamand by several other groups. The 1986paper was considered “unpublishable” bymany of our colleagues, but it has nowbeen cited nearly a thousand times. De-scriptive data are helpful; we need mapsto orient ourselves in an unknown terrain.
Some key questions that needed to beaddressed were: what was the specificityof the cellular immune response in ather-osclerosis, and which were the vasculareffects of the immune effector response?How important were the inflammatoryeffects of interferon-γ and other cytokinesin atherosclerosis?
CHASING IMMUNE SPECIFICITYTo determine the immunologic speci-
ficity of T cells resident in atheroscleroticlesions, we needed to clone them. Thisstep was not a trivial exercise, and weneeded to learn from a master. I had fol-lowed the work of Marc Feldmann inLondon on the autoimmune specificity ofGraves’ disease and was impressed, bothby the technology and the biology.Hence, I wrote to Marc and asked if wecould visit his lab to learn T-cell cloning.He kindly invited me and PhD studentSten Stemme to come to his lab, then atthe Charing Cross Sunley Research Insti-tute in West London.
Sten and I went to London in the win-ter of 1990 to spend a couple of weeks inMarc’s lab learning human T-cell cloning.This was at the time when Marc and hiscolleagues made the groundbreaking dis-covery of the role of tumor necrosis factorin rheumatoid arthritis, which led to arevolution in rheumatology. We returnedto Göteborg, inspired by the spirit at theInstitute and equipped with knowhow onhow to clone T cells.
Obtaining arterial T cells from patientsamples was not a trivial problem. Aftera year of methodological development,Sten had produced enough clones, fromsurgical specimens of four patients, tostart an antigen challenge. I assumed
that all humans would be tolerant to na-tive low-density lipoprotein (LDL) andhypothesized that oxidation would breaktolerance. Therefore, we exposed ourT-cell clones to oxidized LDL, in thepresence of antigen-presenting mono-cytes. Some of the T cells reacted andstarted to divide; this response wasblunted when anti–HLA-DR antibodieswere present in the cultures. The inter-pretation was obvious: oxidized LDLwas taken up by antigen-presentingmonocytes, fragments of LDL proteinwere bound to HLA-DR and theLDL–HLA-DR complex was exposed toT cells. T cells carrying TCR antigen re-ceptors that could bind this complexwere activated and mounted an immuneresponse. Our paper presenting thesefindings was published in Proceedings ofNational Academy of Sciences of the UnitedStates of America in 1995 (3).
When we revisited this problem lateron using the more refined tools of T-cellhybridomas, we confirmed that LDL actsas an autoantigen but also found, to oursurprise, that T cells recognize nativerather than oxidized LDL epitopes (4). In-deed, heavy oxidation makes LDL unrec-ognizable by T cells. Mild oxidation mayincrease scavenger receptor–mediateduptake of LDL into antigen-presentingcells, whereas heavy oxidation destroysthe T-cell epitopes. We proposed that awindow of mild oxidation permits bothuptake and recognition and therefore cancause autoimmune reactions to LDL (5).
PHYSICIAN OR SCIENTIST?At this stage, it became necessary to re-
consider my career plans. I had gone intomedicine with the goal of becoming a cli-nician, with an aim to practice internalmedicine or cardiology. Medical researchwas a way to get there and to be able todo it better. But with the discovery of theatherosclerosis-associated immune re-sponse, I found myself in the midst of anextremely exciting research project thatpromised to provide new insights into thepathogenesis of a major lethal disease,and perhaps even offer new therapeuticopportunities. I realized that I did not

A N T H O N Y C E R A M I A W A R D I N T R A N S L A T I O N A L M E D I C I N E
M O L M E D 2 0 : 3 8 1 - 3 8 9 , 2 0 1 4 | H A N S S O N | 3 8 5
have the capacity to simultaneously leadthis line of research, take good care of se-verely ill patients and be a good father tomy children. I had to make a choice.
A patient I met as a resident in internalmedicine helped me solve the problem.He was 40 years old and had been ad-mitted with a major stroke. I saw himwhen he came to the medicine ward andfound that the stroke had had a disas-trous effect. A computed tomographyscan showed a large ischemic lesion inthe left hemisphere. At this time, no ac-tive therapy was available for ischemicstroke. We had nothing to offer thisyoung patient with a devastating cere-brovascular condition.
We requested that the patient be trans-ferred to intensive care and neurorehabil-itation. But the neurologist found thebrain damage too large for meaningfulrehabilitation and said “no.” I was upsetand tried to argue for my patient, but tono avail. The patient’s wife and their twoyoung daughters came to visit and leftcrying. The prognosis was poor, and theman was likely to remain in need of hos-pital care for the rest of his life, with per-sistent paralysis and aphasia. The bestthey could hope for was that the manwould die soon.
Meeting this patient made me realizethe limitations of clinical medicine. As aphysician, you can do a lot for your patient—but not more than the tools ofmedicine available at the time allow. Asa clinician, your hands are tied by thelimitations of medicine. As a physician-scientist, you can help stretch those limitations.
This experience made it easier for meto make the decision to focus on science.I switched residency, from internal med-icine and cardiology to laboratory medi-cine. This turned out to be an ideal com-promise. I could focus on research anddevelopment while maintaining con-tacts with clinical medicine through thelaboratory service. My eccentric boss,Professor Sven Lindstedt, put it bluntly:“The task of the residents is to do re-search and develop new methods thatwe can apply in diagnostics. Don’t run
around in the routine lab disturbing thestaff.”
Once the decision was made, it waseasy to move on. Lots of excitement layahead. Equipped with cell culture sys-tems, human tissue specimens and ani-mal models, and learning the conceptsand technologies of molecular biology,we were ready to make discoveries.
IMMUNOSUPPRESSANTS,INFLAMMATION, AND THE PROBLEM OFBEING TOO EARLY
Encouraged by Per Peterson, then inUppsala and later at Scripps, we testedthe effect of an immunosuppressantdrug, cyclosporin A, on arterial injury.The effect was striking—postinjury le-sions in rat arteries were reduced byabout 80% (6). I immediately saw thepossibility to use immunosuppressantsto prevent restenosis after vascular pro-cedures. With the new stenting techniqueto maintain patency of arteries after in-tervention, it might even be possible tocoat stents with cyclosporin as a slow- release preparation to eliminate resteno-sis altogether.
Unfortunately, the pharmaceutical in-dustry was not as excited as I. At Sandoz(now Novartis), which produced cy-closporin, no one wanted to see me. I got an invitation to Hoffmann-LaRoche, but they all shook their heads,thinking I was a crazy immunologistwho thought I could cure heart diseasewith cyclosporin! We had to give up theproject. A few years later, Andrew Marksand his colleagues in New York discov-ered a similar effect of another immuno-suppressant, rapamycin/sirolimus (7),and were more successful in convincingindustry. The sirolimus-coated stent isnow a multimillion dollar industry.
Our hypothesis that atherosclerosis isan inflammatory disease was met withimmense skepticism, although we andothers made several findings that sup-ported this notion. Michael Gimbrone,Peter Libby, Jordan Pober and their col-leagues in Boston demonstrated, in cellculture systems and transplant models,that vascular cells are important targets
for immune cytokines and that their re-sponse includes expression moleculesthat promote recruitment of immune cellsto lesions (8–10). Our own work showed,for the first time, local production of aproinflammatory cytokine, interferon-γ,in the atherosclerotic lesion (11). GeorgWick and Qingbo Xu in Innsbruck identi-fied heat shock protein-65–reactive T cellsin atherosclerotic lesions of hypercholes-terolemic rabbits (12). Our first reviewpapers started to create some interest inthe topic among cardiovascular scientists(13,14). However, all these findings werenot sufficient to convince our colleaguesthat any other molecules than cholesteroland the platelet-derived growth factorwere worth investigating.
At best, cardiovascular conferenceshad a session on inflammation on thelast day of the meeting, when everybodywas leaving town. The two speakers inthe session were usually my friend PeterLibby and I. Peter chaired when I talkedabout the cellular immunology of athero-sclerotic lesions, and then it was my turnto chair while he spoke about cytokinesignaling in vascular cells. The rest of theaudience consisted of a few energeticpostdoctoral scientists who had not yetleft the conference.
In the mid-1990s, all this changed. Vascular biologists, cardiologists andeven immunologists were getting inter-ested in vascular immunology and itsrole in atherosclerosis. The clinical andepidemiological findings of Atilio Maseri,Mark Pepys and Paul Ridker changed thetide. Maseri and Pepys discovered thatinterleukin-6 and its downstream prod-uct, C-reactive protein (CRP), are ele-vated in patients with unstable coronarydisease (15,16). Ridker, when interrogat-ing large population cohorts, demon-strated that modest CRP elevations pre-dict future coronary events in healthymiddle-aged individuals (17). But CRPdoes not cause the disease, since pureCRP preparations failed to elicit anyatherogenic effects. Therefore, the lesionin the artery wall must “leak” inflamma-tory mediators such as IL-6, which in-duces CRP when reaching the liver.

3 8 6 | H A N S S O N | M O L M E D 2 0 : 3 8 1 - 3 8 9 , 2 0 1 4
A M E D I C A L S C I E N T I S T I N T R A N S L A T I O N
NEW OPPORTUNITIES AT THEKAROLINSKA INSTITUTE
In December 1994, I was appointed to anew chair in cardiovascular research atthe Karolinska Institute in Stockholm. I now had a chance to build up a largerresearch team, set up new technologyand embark on long-term projects. It wasa golden opportunity, and I was excitedto start working in Stockholm. For thefirst 2 years, I worked very hard in Stock-holm Monday through Friday and spentweekends in our home in Göteborg. Twoyears later, when our youngest son hadfinished gymnasium (“high school,” inUS terms), we sold our apartment inGöteborg and moved to Stockholm. Al-though Margareta in particular missedGöteborg, Stockholm is a great city thatwe enjoy living in, a beauty on the water,with a rich history and a great culturallife.
I decided to set up two new technolo-gies. The first one was obvious: to estab-lish a genetic mouse model for atheroscle-rosis. Because all possible immunologicalreagents were available and many mole-cules and genes were identified in themouse, I was convinced that such amodel would make it possible to dissectthe immunopathogenesis of atherosclero-sis to an extent that was unthinkablewhen using other species such as rabbitsor rats. A golden era for experimental ath-erosclerosis dawned when NobuyoMaeda and Jan Breslow knocked out theapoe gene in mice, and the Dallas team ofMike Brown, Joe Goldstein and JoachimHerz made an ldlr–/– mouse (18–20). Weset up an apoe–/– colony at the KarolinskaInstitute, characterized its cellular pathol-ogy and went on to test the effect of im-munomodulation on atherosclerosis.
My second initiative was to team upwith the clinicians. In Göteborg, I hadhad fruitful collaborations with the vas-cular surgeons, and it was natural for meto establish a similar relationship withJesper Swedenborg, Ulf Hedin and theircolleagues at Karolinska Hospital. We setup a pipeline between the cardiovascularsurgery theater and our lab in the Centerfor Molecular Medicine to obtain fresh
human specimens. It has emerged intothe BiKE (Biobank of Karolinska En-darterectomy) biobank with tissue, RNA,DNA, sera, disease history and follow-up, and, I believe, the world’s largestglobal transcriptome database of humanatherosclerosis (21). Collaboration withheart surgeons, cardiologists andrheumatologists has also helped us trans-late findings between experimental mod-els and human disease.
AN ATHEROPROTECTIVE IMMUNERESPONSE
Two brilliant young postdoctoral scien-tists, Antonino (Tony) Nicoletti andGiuseppina (Pina) Caligiuri, both now inParis, had joined the team and led thework on immunomodulation. Tony and Iwere thrilled when we saw that intra-venous immunoglobulin treatment inhib-ited disease progression (22). This and aparallel study by Francois Mach andPeter Libby showing a similar effectwhen blocking the immune costimula-tory factor CD40L (23) were the first stud-ies to demonstrate a therapeutic effect ofimmunotherapy on atherosclerosis.
Pina performed another exciting ex-periment. She splenectomized mice withthe thought that removal of a major im-mune organ might affect atherosclerosis.The effect was remarkable—lesions ofsplenectomized apoe–/– mice were twiceas large as those in intact apoe–/– controls(24). By transfer experiments, we couldshow protective effects of T cells, buteven more so of B cells. The immune re-sponse apparently contained an athero-protective component that resides with apopulation of B cells in the spleen.
While I was busy setting up my newlab in Stockholm, the labs of Joe Witztumand Jan Nilsson published some very ex-citing findings. They reported that im-munization of fat-fed rabbits with oxi-dized LDL reduced rather than increasedatherosclerosis (25,26). Our spleen cellfindings identified a mechanism for thisprotection (24), and I set up the goal todevelop a vaccine against atherosclerosis.Later on, the discovery that regulatoryT cells inhibit atherosclerosis added im-
portantly to our understanding ofatheroprotective immunity (27,28).
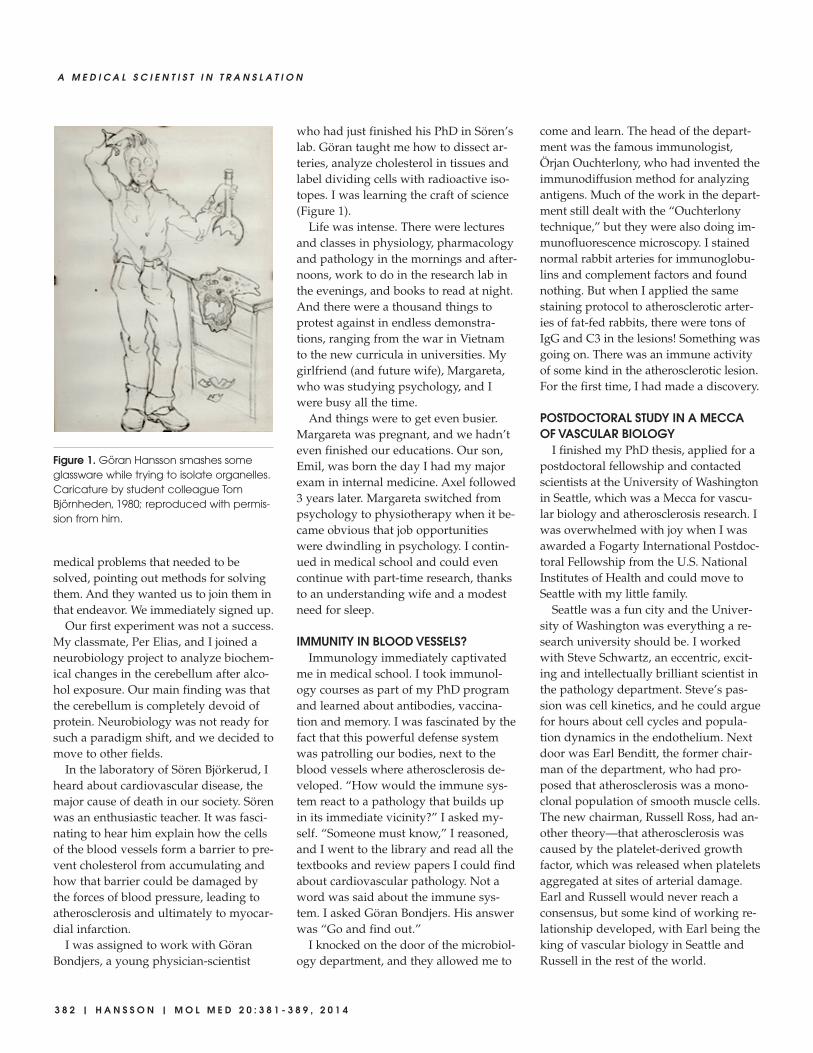
More than 15 years later and thanks tothe work in several labs, we havelearned a lot about the autoimmune re-sponse to LDL and the atheroprotectiveeffector mechanisms it triggers (Figure 3).And although we still do not have a vac-cine or an immunotherapy on the mar-ket, we have come a long way towardthat goal.
VASCULAR INFLAMMATION GETS HOTTwo major themes had emerged in our
lab: the adaptive immunity of atheroscle-rosis and the vascular biology of inflam-mation. While a T cell–focused teamstudies the autoimmune properties ofLDL, the mechanisms of its presentationas antigen and the effects of immuniza-tion on disease, a second team in the labworks on the vascular biology of im-mune inflammation.
The second line of work got a kick-start when Yong-jian Geng joined us asa PhD student in 1990. His cDNAcloning of rat iNOS (NOS2) (29,30)brought us into the core of molecular bi-ology technology, and I learned that aresearch project is an excellent way ofestablishing a new technique. WhenYong-jian moved to the United States,Zhong-qun Yan continued the vascularbiology research and expanded into in-nate immunity (31,32). Zhong-qunmoved with me to Stockholm, and wecontinue to collaborate, 20 years later.At the Karolinska Institute, Guro Valenjoined us as a postdoctoral fellow,learned vascular biology and taught usheart physiology (33). After her postdoc,she set up her own lab in the physiol-ogy department and later moved toOslo to take up a professorship in phys-iology. Another postdoctoral scientist,Gabrielle Paulsson-Berne (34), is nowour lab manager as well as an expert inmolecular biology. A gifted physician-scientist, Magnus Bäck, introduced us toeicosanoid biology and leukotriene sig-naling (35). He now runs his own re-search program on vascular inflamma-tion at our center, while also serving as
A N T H O N Y C E R A M I A W A R D I N T R A N S L A T I O N A L M E D I C I N E
M O L M E D 2 0 : 3 8 1 - 3 8 9 , 2 0 1 4 | H A N S S O N | 3 8 7
a consultant in cardiology at KarolinskaUniversity Hospital.
Our studies of adaptive immunitywere facilitated immensely by the avail-ability of gene-targeted mouse models.A succession of fellows includingXingha Zhou, Anna-Karin Robertson,Ariane Sultan, Daniel Johansson,Roland Klingenberg, Norbert Gerdes,Andreas Hermansson, Daniel Ketelhuth,Anna Lundberg, Olga Ovchinnikova,Daniela Strodthoff, Anton Gisterå andothers addressed these aspects, by using
crossbreeding and transplantation tech-niques. Their work identified immuneresponses that promote vascular inflam-mation and atherosclerosis, but alsoother responses that inhibit lesion de-velopment, modulate lipoprotein metab-olism and cause plaque stabilization(4,28,36–39).
After decades of controversy, it is timeto reconcile the views of atherosclerosisas a metabolic disturbance or a responseto injury. Atherosclerosis is a chronic in-flammatory disease caused by an im-
mune response to LDL accumulation inthe artery wall.
NEW OPPORTUNITIES AND NEWEXCITEMENT
At the moment, we have an exciting setof scientific questions, a great panel oftechniques to address them and a superbteam to solve the problems. We havebeen able to translate many of our find-ings to human pathology and some toclinical development. With the exceptionof the coated stents, vascular immunol-ogy has not reached clinical therapy, butwe remain hopeful that it will do so inthe years to come. Ongoing clinical trialson interleukin-1β blockade andmethotrexate-based immunosuppressionshould be informative, as should clinicalstudies of vaccination. Translational med-icine is a slow but exciting process!
To be a medical scientist is stimulat-ing not only because of the intellectualchallenges you are facing, but also be-cause of the discoveries you may make.Our workplace is global; we addresssimilar problems and methods whereverwe are located and we can easily crossborders created by language, culture orpolitics. Our apprentice system calledthe postdoctoral fellowship createsunique opportunities to live in anothercountry and get to know another cul-ture. I get a kick every morning when Icome to work and meet my colleaguesfrom Asia, Europe and the Americas(Figure 4).
The position at the interface betweenbasic life science and clinical medicine isvery special. You learn from both sidesand appreciate all the various kinds ofexpertise that are needed for a transla-tional research project, from biochem-istry to surgery. I have had the privilegeof working together with a series of out-standing basic and clinical scientists atthe Karolinska’s Center for MolecularMedicine. My lab neighbors include thesurgeon and cell biologist Ulf Hedin, thecardiologist/geneticist Anders Hamsten,the rheumatologists/immunologists Lars Klareskog and Marie Wahren- Herlenius, the neurologist/immunologist
Figure 3. Counterbalancing forces of adaptive immunity in the atherosclerotic plaque:proinflammatory Th1 cells and atheroprotective Treg cells, as proposed in a review article(43). We have since learned that native rather than oxidized LDL serves as a T-cell anti-gen. Reproduced from (43): Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 2005;352(16):
1685–95. Copyright © 2005 Massachusetts Medical Society. Reprinted with permission.

3 8 8 | H A N S S O N | M O L M E D 2 0 : 3 8 1 - 3 8 9 , 2 0 1 4
A M E D I C A L S C I E N T I S T I N T R A N S L A T I O N
Tomas Olsson and the virologist CeciliaSöderberg-Nauclér, to mention a few. Ourresearch network Center of Excellencefor Research on Inflammation and Car-diovascular disease (CERIC) gives all ofus access to unique biobanks and animalmodels of several inflammatory diseases,including atherosclerosis, multiple scle-rosis and rheumatoid arthritis (40). Ourbiochemistry partners Jesper Haeggström,Thomas Renné and Rikard Holmdahladd expertise in fundamental sciences toour network. With support from the Linnaeus program of the Swedish Re-search Council, our vision for a transla-tional research center in inflammationand cardiovascular disease has finallybecome a reality.
Scientific journals, conferences and organizations provide opportunities toextend our networks and to get insights
into many aspects of science. I have hadthe very special privilege of serving onthe Nobel Committee for Physiology orMedicine for 15 years (41). By forcingme to learn about many different areasof life science and medicine, my workwith the Nobel Prize is a continuing sci-entific education and a wonderfulsource of excitement and intellectualstimulation.
Science is a very large part of life forany scientist, and particularly so in trans-lational medicine, since you try to bridgebetween two very dynamic areas: molec-ular life science and clinical medicine. Itis, nevertheless, important to find timefor other activities. Family life has al-ways been a source of joy for me, as hasmusic. I was introduced to classicalmusic as an aspiring pianist with limitedtalent in my teens, and it has remained
with me since then, as an island of es-cape and a sheer pleasure. It remains achallenge to be a reasonably completehuman being, but you must never stoptrying.
ACKNOWLEDGMENTSI am grateful to all present and former
fellows and students in our lab for mak-ing it such a great place to work. I amalso indebted to many colleagues forstimulating discussions and collabora-tion, in the Center for Molecular Medi-cine at Karolinska Institute and all overthe world. I gratefully acknowledge thesupport of the funding agencies thatmade our research possible. Our work iscurrently supported by the Swedish Re-search Council, the Swedish Heart-LungFoundation, the European Commissionand the Foundation for Strategic Re-
Figure 4. Hansson Lab 2014. Upper row: Anton Gisterå, Zhong-qun Yan, Daniel Ketelhuth, Andres Laguna Fernandez, Reiner Mailer, RolandBaumgartner, André Strodthoff, Marcelo Petri, Stephen Malin, Martin Berg. Middle row: John Pirault, Olga Ovchinnikova, Miguel Cao-racedo, Sophie Xintong Jiang, Monica Centa, Linda Haglund, Katrin Habir, Gabrielle Paulsson-Berne, Konstantinos Polyzos. Lower row:Glykeria Karadimou, Maria Klement, Teodora Andonova, Göran Hansson, Ann Hellström, Anneli Olsson.
A N T H O N Y C E R A M I A W A R D I N T R A N S L A T I O N A L M E D I C I N E
M O L M E D 2 0 : 3 8 1 - 3 8 9 , 2 0 1 4 | H A N S S O N | 3 8 9
search. Finally, I thank my wife Mar-gareta and our sons Emil and Axel for awonderful life together.
DISCLOSUREI have no competing interests as de-
fined by Molecular Medicine, or other in-terests that might be perceived to influ-ence the results and discussion reportedin this paper.
REFERENCES1. Jonasson L, Holm J, Skalli O, Gabbiani G, Hans-
son GK. (1985) Expression of class II transplanta-tion antigen on vascular smooth muscle cells inhuman atherosclerosis. J. Clin. Invest. 76:125–31.
2. Jonasson L, Holm J, Skalli O, Bondjers G, Hans-son GK. (1986) Regional accumulations of T cells,macrophages, and smooth muscle cells in thehuman atherosclerotic plaque. Arteriosclerosis.6:131–8.
3. Stemme S, et al. (1995) T lymphocytes fromhuman atherosclerotic plaques recognize oxi-dized low density lipoprotein. Proc. Natl. Acad.Sci. U. S. A. 92:3893–7.
4. Hermansson A, et al. (2010) Inhibition of T cellresponse to native low-density lipoprotein re-duces atherosclerosis. J. Exp. Med. 207:1081–93.
5. Hansson GK, Hermansson A. (2011) The immunesystem in atherosclerosis. Nat. Immunol. 12:204–12.
6. Jonasson L, Holm J, Hansson GK. (1988) Cy-closporin A inhibits smooth muscle proliferationin the vascular response to injury. Proc. Natl.Acad. Sci. U. S. A. 85:2303–6.
7. Marx SO, Jayaraman T, Go LO, Marks AR. (1995)Rapamycin-FKBP inhibits cell cycle regulators ofproliferation in vascular smooth muscle cells.Circ. Res. 76:412–7.
8. Warner S, Auger KR, Libby P. (1987) Interleukin-1 induces interleukin-1. II. Recombinant humaninterleukin-1 induces interleukin-1 production byadult human vascular endothelial cells. J. Im-munol. 139:1911–7.
9. Pober JS, Collins T, Gimbrone MA, Libby P, ReissCS. (1986) Inducible expression of class II majorhistocompatibility complex antigens and the im-munogenicity of vascular endothelium. Trans-plant. 41:141–6.
10. Bevilacqua MP, Pober JS, Mendrick DL, CotranRS, Gimbrone MA. (1987) Identification of an in-ducible endothelial-leukocyte adhesion molecule.Proc. Natl. Acad. Sci. U. S. A. 84:9238–42.
11. Hansson GK, Holm J, Jonasson L. (1989) Detec-tion of activated T lymphocytes in the humanatherosclerotic plaque. Am. J. Pathol. 135:169–75.
12. Xu Q, Kleindienst R, Waitz W, Dietrich H, WickG. (1993) Increased expression of heat shock pro-tein 65 coincides with a population of infiltrat-ing T lymphocytes in atherosclerotic lesions ofrabbits specifically responding to heat shockprotein 65. J. Clin. Invest. 91:2693–702.
13. Hansson GK, Jonasson L, Seifert PS, Stemme S.(1989) Immune mechanisms in atherosclerosis.Arteriosclerosis. 9:567–78.
14. Libby P, Hansson GK. (1991) Involvement of theimmune system in human atherogenesis: currentknowledge and unanswered questions. Lab. In-vest. 64:5–15.
15. Liuzzo G, et al. (1994) The prognostic value of C-reactive protein and serum amyloid a protein insevere unstable angina. N. Engl. J. Med. 331:417–24.
16. Liuzzo G, et al. (1996) Plasma protein acute-phase response in unstable angina is not inducedby ischemic injury. Circulation. 94:2373–80.
17. Ridker PM, Hennekens CH, Buring JE, Rifai N.(2000) C-reactive protein and other markers ofinflammation in the prediction of cardiovasculardisease in women. N. Engl. J. Med. 342:836–43.
18. Piedrahita JA, Zhang SH, Hagaman JR, OliverPM, Maeda N. (1992) Generation of mice carry-ing a mutant apolipoprotein E gene inactivatedby gene targeting in embryonic stem cells. Proc.Natl. Acad. Sci. U. S. A. 89:4471–5.
19. Plump AS, et al. (1992) Severe hypercholesterolemiaand atherosclerosis in apolipoprotein E-deficientmice created by homologous recombination in EScells. Cell. 71:343–53.
20. Ishibashi S, Herz J, Maeda N, Goldstein JL,Brown MS. (1994) The two-receptor model oflipoprotein clearance: tests of the hypothesis in“knockout” mice lacking the low densitylipoprotein receptor, apolipoprotein E, or bothproteins. Proc. Natl. Acad. Sci. U. S. A. 91:4431–5.
21. Folkersen L, et al. (2012) Prediction of ischemicevents on the basis of transcriptomic and ge-nomic profiling in patients undergoing carotidendarterectomy. Mol. Med. 18:669–75.
22. Nicoletti A, Kaveri S, Caligiuri G, Bariety J,Hansson GK. (1998) Immunoglobulin treatmentreduces atherosclerosis in apo E knockout mice.J. Clin. Invest. 102:910–8.
23. Mach F, Schonbeck U, Sukhova GK, Atkinson E,Libby P. (1998) Reduction of atherosclerosis inmice by inhibition of CD40 signalling. Nature.394:200–3.
24. Caligiuri G, Nicoletti A, Poirier B, Hansson GK.(2002) Protective immunity against atherosclero-sis carried by B cells of hypercholesterolemicmice. J. Clin. Invest. 109:745–53.
25. Palinski W, Miller E, Witztum JL. (1995) Immu-nization of low density lipoprotein (LDL) recep-tor-deficient rabbits with homologous malondi-aldehyde-modified LDL reduces atherogenesis.Proc. Natl. Acad. Sci. U. S. A. 92:821–5.
26. Ameli S, et al. (1996) Effect of immunization withhomologous LDL and oxidized LDL on early ath-erosclerosis in hypercholesterolemic rabbits. Ar-terioscler. Thromb. Vasc. Biol. 16:1074–9.
27. Ait-Oufella H, et al. (2006) Natural regulatoryT cells control the development of atherosclerosisin mice. Nat. Med. 12:178–80.
28. Klingenberg R, et al. (2013) Depletion of FOXP3+regulatory T cells promotes hypercholesterolemiaand atherosclerosis. J. Clin. Invest. 123:1323–34.
29. Geng YJ, Almqvist M, Hansson GK. (1994) cDNAcloning and expression of inducible nitric oxidesynthase from rat vascular smooth muscle cells.Biochim. Biophys. Acta. 1218:421–4.
30. Geng YJ, Hansson GK, Holme E. (1992) Inter-feron-γ and tumor necrosis factor synergize to in-duce nitric oxide production and inhibit mito-chondrial respiration in vascular smooth musclecells. Circ. Res. 71:1268–76.
31. Yan Z, Hansson GK. (1998) Overexpression of in-ducible nitric oxide synthase by neointimalsmooth muscle cells. Circ. Res. 82:21–9.
32. Edfeldt K, Swedenborg J, Hansson GK, Yan ZQ.(2002) Expression of toll-like receptors in humanatherosclerotic lesions: a possible pathway forplaque activation. Circulation. 105:1158–61.
33. Valen G, Yan ZQ, Hansson GK. (2001) Nuclearfactor kappa-B and the heart. J. Am. Coll. Cardiol.38:307–14.
34. Paulsson G, Zhou X, Törnquist E, Hansson GK.(2000) Oligoclonal T cell expansions in athero-sclerotic lesions of apoE-deficient mice. Arte-rioscler. Thromb. Vasc. Biol. 20:10–7.
35. Back M, et al. (2005) Leukotriene B4 signalingthrough NF-kappaB-dependent BLT1 receptorson vascular smooth muscle cells in atherosclero-sis and intimal hyperplasia. Proc. Natl. Acad. Sci.U. S. A. 102:17501–6.
36. Zhou X, Paulsson G, Stemme S, Hansson GK.(1998) Hypercholesterolemia is associated with aT helper (Th) 1/Th2 switch of the autoimmuneresponse in atherosclerotic apo E-knockout mice.J. Clin. Invest. 101:1717–25.
37. Robertson AK, et al. (2003) Disruption of TGF-beta signaling in T cells accelerates atherosclero-sis. J. Clin. Invest. 112:1342–50.
38. Hermansson A, et al. (2011) Immunotherapy withtolerogenic apolipoprotein B-100-loaded den-dritic cells attenuates atherosclerosis in hyperc-holesterolemic mice. Circulation. 123:1083–91.
39. Gistera A, et al. (2013) Transforming growth fac-tor-beta signaling in T cells promotes stabiliza-tion of atherosclerotic plaques through an inter-leukin-17-dependent pathway. Sci. Transl. Med.5:196ra100.
40. Center of Excellence for Research on Inflamma-tion and Cardiovascular disease (CERIC). Wel-come to CERIC [Internet]. c2014. Stockholm(Sweden): CERIC; [cited 2014 Jun 26]. Availablefrom: http://www.ceric.se.
41. Nobel Assembly at Karolinska Institutet [Inter-net]. c2014. [cited 2014 Jun 26]. Available from:http://www.nobelprizemedicine.org.
42. Göran K, Jonasson L. (2009) The discovery ofcellular immunity in the atherosclerotic plaque.Arterioscler. Thromb. Vasc. Biol. 29:1714–1717.
43. Hansson GK. (2005) Inflammation, atherosclero-sis, and coronary artery disease. N. Engl. J. Med.352:1685–95.












![EUROPE 2016 - bi-podium.nlbi-podium.nl/mediaFiles/upload/DMzone16/DMZ2016_program.pdf · The Journey from ER Modeler to Data Scientist Asoka Diggs Intel Corp. [United States] smartDATA](https://img.pdfslide.net/doc/110x75/5ec96b6b7beb091b19104915/europe-2016-bi-the-journey-from-er-modeler-to-data-scientist-asoka-diggs-intel.jpg)