Embed Size (px)
Citation preview

A. KazdaA. Kazda

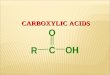
Graph of acidGraph of acid--base regulationbase regulationGraph of acidGraph of acid--base regulationbase regulation
Graf acidobazické regulace (M. Engliš, Prakt. lék. 1972)Graf acidobazické regulace (M. Engliš, Prakt. lék. 1972)

buffersbuffers acid acid basebase % relative% relative present in present in
hydrogenhydrogen--carboniccarbonic HH22COCO33 HCOHCO--33 5151 plasmaplasma
Buffer system in bloodBuffer system in blood
hydrogenhydrogen--carboniccarbonic HH22COCO33 HCOHCO 33 5151 plasmaplasma
hemoglobinhemoglobin oxyhemoglobinoxyhemoglobin deoxyhemoglobindeoxyhemoglobin 3535 erytrocyteserytrocytes
phosphatesphosphates HH22POPO--44 HPOHPO22--
44 77erytrocyteserytrocytes
(plasma)(plasma)
proteinsproteins --COOHCOOH --COOCOO-- 77plasmaplasma
(erytrocytes)(erytrocytes)

HendersonHenderson--HasselbachHasselbach''s equation:s equation:[base][base]
pH = pK + log pH = pK + log
[acid][acid]
HendersonHenderson--HasselbachHasselbach''s equations equation::
[HCO[HCO--33]]
pH = pK + log pH = pK + log
[H[H22COCO33]][H[H22COCO33]]
Carbonic acid concentration can be expressed as a function of pCOCarbonic acid concentration can be expressed as a function of pCO22
[HCO[HCO--33]]
pH = pK + log pH = pK + log
αα . pCO. pCO22
αα = coeficient of solubility of CO= coeficient of solubility of CO22, 0,0306 mol, 0,0306 mol--1111--11torrtorr--11, tj. 0,2295 mol, tj. 0,2295 mol--1111--11kPakPa--11
pK = approximately 6,1 pK = approximately 6,1

tissues COtissues CO22 COCO22 lunglung
COCO22 + H+ H22OO (800)(800)
↕↕
HH22COCO33 (1)(1)
↕↕
HH++ + HCO+ HCO--33 (0,03)(0,03)
Interaction reactionInteraction reaction
HCOHCO--33 HH22COCO33
HH++HH++
Buf HBufBuf HBuf
Retention of CORetention of CO22
HCOHCO--33 HH22COCO33 ← CO← CO22 + H+ H22OO
HH++
Buf HBufBuf HBuf




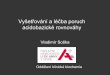
METABOLIC ACID-BASE DISTURBANCES AND THEIR CLINICAL REASONS
AFTER STEWART
Diagnosis Clinical cause
dilutional acidosis
concentrational alkalosis
hyperchloremic acidosis
every cause of hyponatremia
every cause of hypernatremia
infusions rich in chloridediarrheatubular dysfunction during acute or
hypochloremic alkalosis
acidosis from elevation of UA
hyperphosphatemic acidosis
hypoalbuminemic alkalosis
tubular dysfunction during acute orchronic renal failurecompensation of chronic RAL
loss of gastric juicediureticscompensation of chronic RAC
uremia, ketoacidosis, lacticacidosis, intoxications (salicilates,methanol, ethanol)
every cause of hyperphosphatemia(renal failure)
hepatic insufficiency, malnutrition,
nephrotic sd, burns











Thank you for your attentionThank you for your attentionThank you for your attentionThank you for your attention













![ALEXANDR KAZDA, VLADIMIR KOLMOGOROV, …0:2 Alexandr Kazda, Vladimir Kolmogorov, and Michal Rolínek [13]. After 20 years of effort by mathematicians and computer scientists, the dichotomy](https://img.pdfslide.net/doc/110x75/5f70606e1ce6fe2d1f0d3a44/alexandr-kazda-vladimir-kolmogorov-02-alexandr-kazda-vladimir-kolmogorov-and.jpg)