Embed Size (px)
Citation preview
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 1
Opening Remarks
A. Keith Stewart, MBChB, MRCP, FRCPC, MBAVasek and Anna Maria Polak Professor of Cancer Research
Consultant, Division of Hematology/OncologyMayo Clinic
Scottsdale, Arizona
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic Approaches
8:15 AM – 8:20 AM Community Case Part 1 Saad Z. Usmani, MD
8:20 AM – 8:40 AM Translating Molecular and Cytogenetic Profiles Into Precision MedicineSuzanne Trudel, MD
8:40 AM – 9:00 AM Induction Therapy Options for Transplant Eligible and Ineligible PatientsMaría-Victoria Mateos, MD, PhD
9:00 AM – 9:05 AM Panel Discussion
9:05 AM – 9:10 AM Community Case Part 2Saad Z. Usmani, MD
9:10 AM – 9:30 AM Consolidation and Maintenance Therapy OptionsSergio Giralt, MD
9:30 AM – 9:50 AM Updates on Options for Relapsed/Refractory DiseaseSaad Z. Usmani, MD
9:50 AM – 9:55 AM Panel Discussion9:55 AM – 10:00 AM Community Case Part 3
Saad Z. Usmani, MD10:00 AM – 10:20 AM Immunotherapy
Thomas G. Martin, III, MD
10:20 AM – 10:40 AM New Agents in DevelopmentA. Keith Stewart, MBChB
10:40 AM – 10:50 AM Community Case RevisitedA. Keith Stewart, MBChB
10:50 AM – 11:00 AM Question and Answer Session
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 2
Which of the following best represents your professional role?
A. HematologistB. Hematologist-oncologistC. OncologistD. RN/NP/PAE. PharmacistF. Other health care providerG. ResearcherH. PatientI. Other
?
Which of the following best represents the professional setting
in which you currently work?
A. AcademicB. CommunityC. HMOD. HospitalE. PrivateF. OtherG. Does not apply to me
?
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 3
Where do you practice?A. Asia and AustraliaB. CanadaC. Central and South AmericaD. Europe and IsraelE. Middle East and AfricaF. United StatesG. Rest of worldH. Texas
?
Community Case Part 1
Saad Usmani, MD, FACPDirector, Plasma Cell Disorders Program
Director, Clinical Research in Hematologic MalignanciesDepartment of Hematologic Oncology & Blood Disorders
Levine Cancer InstituteCharlotte, North Carolina
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 4
Disclosures
• Consultant/Advisor: Array BioPharma, Bristol-Myers Squibb, Celgene, Janssen, Onyx, an Amgen subsidiary, Sanofi, Takeda Oncology
• Research Grant: Array BioPharma, Janssen, Onyx, an Amgen subsidiary, Sanofi
• Speakers Bureau: Celgene, Onyx, an Amgen subsidiary, Takeda Oncology
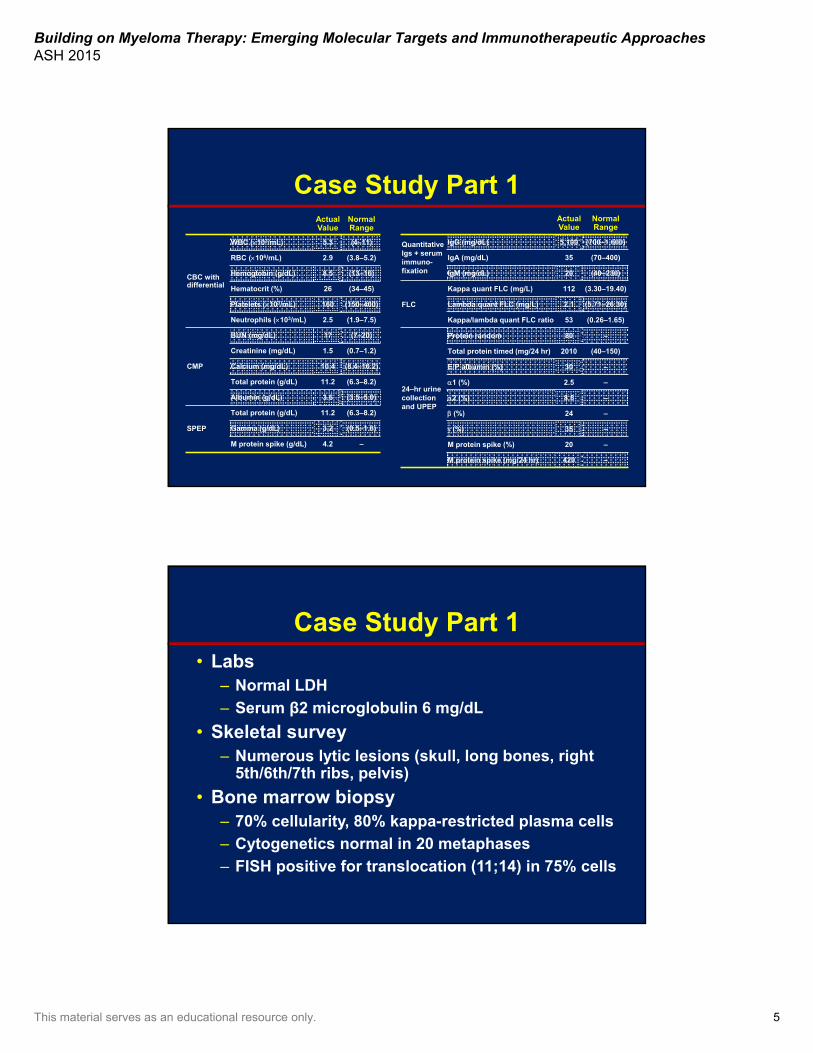
Case Study Part 154-year-old man presents with 6-month history of lower back pain, increasing fatigue, right rib pain.
• Hypertension for 5 years (controlled)
Past medical history
• Right/left arthroscopic surgery
Past surgical history
• Hypertension
• Type 2 diabetes
• No cancers
Familyhistory
• Banker, marathon runner
• Married
• Two kids
Socialhistory
• Pallor, right rib cage tenderness
Physicalexam
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 5
Case Study Part 1ActualValue
Normal Range
CBC withdifferential
WBC (103/mL) 5.3 (4–11)
RBC (106/mL) 2.9 (3.8–5.2)
Hemoglobin (g/dL) 8.5 (13–16)
Hematocrit (%) 26 (34–45)
Platelets (103/mL) 160 (150–400)
Neutrophils (103/mL) 2.5 (1.9–7.5)
CMP
BUN (mg/dL) 17 (7–20)
Creatinine (mg/dL) 1.5 (0.7–1.2)
Calcium (mg/dL) 10.4 (8.4–10.2)
Total protein (g/dL) 11.2 (6.3–8.2)
Albumin (g/dL) 3.6 (3.5–5.0)
SPEP
Total protein (g/dL) 11.2 (6.3–8.2)
Gamma (g/dL) 3.2 (0.5–1.6)
M protein spike (g/dL) 4.2 –
ActualValue
Normal Range
QuantitativeIgs + serum immuno-fixation
IgG (mg/dL) 5,100 (700–1,600)
IgA (mg/dL) 35 (70–400)
IgM (mg/dL) 20 (40–230)
FLC
Kappa quant FLC (mg/L) 112 (3.30–19.40)
Lambda quant FLC (mg/L) 2.1 (5.71–26.30)
Kappa/lambda quant FLC ratio 53 (0.26–1.65)
24–hr urinecollection and UPEP
Protein random 80 –
Total protein timed (mg/24 hr) 2010 (40–150)
E/P albumin (%) 30 –
1 (%) 2.5 –
2 (%) 8.5 –
(%) 24 –
(%) 35 –
M protein spike (%) 20 –
M protein spike (mg/24 hr) 420 –
Case Study Part 1• Labs
– Normal LDH
– Serum β2 microglobulin 6 mg/dL
• Skeletal survey– Numerous lytic lesions (skull, long bones, right
5th/6th/7th ribs, pelvis)
• Bone marrow biopsy– 70% cellularity, 80% kappa-restricted plasma cells
– Cytogenetics normal in 20 metaphases
– FISH positive for translocation (11;14) in 75% cells
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 6
Which one of the methodologies do you currently use most often?
A. Gene expression profilingB. Conventional cytogeneticsC. FISHD. Gene mutation panelE. Flow cytometryF. More than one methodG. None of the above
?
Is this patient considered eligible for stem cell transplantation?
A. YesB. NoC. Not sure
?

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 7
Which factors do you use to decide whether to consider aggressive therapy
such as stem cell transplantation?
A. Age, comorbidity scoreB. Social support and insurance
coverageC. Response to induction therapyD. Risk profileE. All of the aboveF. I don’t do transplants up front
?
What would be your recommendation for initial treatment?
A. Melphalan, prednisone, bortezomib (MPV)B. Bortezomib, thalidomide, dexamethasone (VTD)C. Lenalidomide + low-dose dexamethasone (Ld)D. Lenalidomide, bortezomib, dexamethasone
(RVD)E. Cyclophosphamide, bortezomib,
dexamethasone (CyBorD)F. Carfilzomib, lenalidomide, dexamethasone
(KRD)G. Other
?

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 8
Does your practice routinely test for minimal residual disease (MRD)
following therapy?
A. YesB. NoC. We soon willD. Not sure
?
Translating Molecular and Cytogenetic Profiles Into Precision Medicine:
Identifying Molecularly Defined Subsets
Suzanne Trudel, MDPrincess Margaret Cancer Centre
University Health NetworkToronto, Ontario, Canada

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 9
Disclosures
• Consultancy: Novartis• Honoraria: Celgene, Amgen, BMS,
Novartis• Research funding: GSK, Oncoethix,
Onyx, Trillium, Astellas
Objectives
• Describe oncogenic drivers in MM and their relationship to molecular subsets
• Describe their prognostic implication and integration of cytogenetics and molecular profiles with clinical data as new prognostic tools
• Describe the use of molecular profiling for precision therapeutic strategies in MM

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 10
Multiple Myeloma: Molecular PathogenesisIntrinsic Genetic Background
Figure 3, page 3460
Kuehl WM, Bergsagel PL. Molecular pathogenesis of multiple myeloma and its premalignant precursor. J Clin Invest. 2012;122(10):3456-3463.
Figure 1
Chesi M, Bergsagel PL. Molecular pathogenesis of multiple myeloma: basic and clinical updates. Int J Hematol. 2013 Mar;97(3):313-323.
MM Karyotypes Identify Unique Molecular Subsets
Figure 4A, page 300
Bergsagel PL, et al. CyclinD dysregulation: an early and unifying pathogenic event in multiple myeloma. Blood. 2005;106:296-303.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 11
t(4;14)1
• Translocation between heavy Ig gene locus and MMSET + FGFR3
• Associated with IgA myeloma • Immature morphology • Tendency for less lytic bone disease, younger
age
t(11:14)2
• Translocation between heavy Ig gene locus and cyclinD1
• Associated with IgD, IgM and nonsecretory MM• Lymphoplasmacytoid morphology and B
lineage–Ag (CD20 and CD79a)
1. Jaksic W et al. J Clin Oncol. 2005;23:7069.2. An G et al. Leuk Res. 2013;37:1251.
Cytogenetics: Biologically Defined Unique Clinical Subsets
Figure 2A & 2B, page 2033
Garand R, et al. t(11;14) and t(4;14) translocations correlated with mature lymphoplasmacytoid and immature morphology, respectively, in multiple myeloma. Leukemia. 2003 Oct;17(10):2032-2035.
Karyotypes and Prognostic Implications
Figure 1, page 885
Bergsagel PL, et al. Improving overall survival and overcoming adverse prognosis in the treatment of cytogenetically high-risk multiple myeloma. Blood. 2013 Feb 7;121(6):884-892.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 12
Heterogeneity Within Cytogenetically-Defined Subsets
t(4;14) Subgroup
Figure 3, page 2022
Moreau P, et al. Heterogeneity of t(4;14) in multiple myeloma. Long-term follow-up of 100 cases treated with tandem transplantation in IFM99 trials. Leukemia. 2007 Sep;21(9):2020-2024.
Combined Prognostic ModelsRevised International Staging System (R-ISS)
Table 1
Palumbo A, et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J Clin Oncol. 2015 Sep 10;33(26):2863-2869.
Figure 1A
Palumbo A, et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J Clin Oncol. 2015 Sep 10;33(26):2863-2869.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 13
Revised R-ISS and OS by Type of Treatment
Figure 3, page 2867
Palumbo A, et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J Clin Oncol. 2015 Sep 10;33(26):2863-2869.
Gene Expression Profiling (GEP) for Risk Stratification
Zhou Y et al. Leukemia. 2009; 23: 1941.Shaughnessy JD et al. Blood. 2007;109:2276.
Figure 1, page 2279
Shaughnessy JD, et al. A validated gene expression model of high-risk multiple myeloma is defined by deregulated expression of genes mapping to chromosome 1. Blood. 2007 Mar 15;109(6):2276-2284.
UMAS GEP70• Defined in patients with poor
outcomes with Total Therapy 2 (TT2)
• Present in 15% of newly diagnosed patients
• High-risk signature found in all molecular subsets
• Commercially available
Considerations:• No standardized high risk
GEP signature (UAMS70, EMC-92 and IFM)
• Perception that they are not reproducible
• Difficult to interpret

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 14
Technological Advances in Detecting Biomarkers in MM
Figure 1, page 811
Landgren O, Morgan GJ. Biologic frontiers in multiple myeloma: from biomarker identification to clinical practice. Clin Cancer Res. 2014 Feb 15;20(4):804-813.
NGS Studies Identify Recurrent Mutations in Key Cellular Pathways
Figure 1B, page 93
Lohr JG, et al. Widespread genetic heterogeneity in multiple myeloma: implications for targeted therapy. Cancer Cell. 2014 Jan 13;25(1):91-101.
Mutations accumulate in key pathways:• MAPK signaling• NFkB signaling• Cell cycle• Chromatin-modifying• RNA processing
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 15
NGS Studies Identify Recurrent Mutations in Key Cellular Pathways
Figure 1B, page 93
Lohr JG, et al. Widespread genetic heterogeneity in multiple myeloma: implications for targeted therapy. Cancer Cell. 2014 Jan 13;25(1):91-101.
What are the clinical implications?
Impact of Mutations on Myeloma SurvivalAnalysis of MRC XI Trial (IMiD-based Phase 3 in NDMM)
Figure 3
Walker BA, et al. Mutational spectrum, copy number changes, and outcome: results of a sequencing study of patients with newly diagnosed myeloma. J Clin Oncol. 2015 Nov 20;33(33):3911-3920.
Figure 4D & 4F
Walker BA, et al. Mutational spectrum, copy number changes, and outcome: results of a sequencing study of patients with newly diagnosed myeloma. J Clin Oncol. 2015 Nov 20;33(33):3911-3920.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 16
Impact on Survival of CCND1 Mutations on Whole Cohort and Among t(11;14) Patients
Figure 7B, 7D & 7F
Walker BA, et al. Mutational spectrum, copy number changes, and outcome: results of a sequencing study of patients with newly diagnosed myeloma. J ClinOncol. 2015 Nov 20;33(33):3911-3920.
• Significantly mutated genes occur within cytogenetic subgroups
• Mutations and cytogenetic abnormalities interact to define more homogeneous prognostic groups
Survival Analysis and Cumulative Negative Impact of NGS-Defined
Molecular Abnormalities
Figure 5A, 5B, 5C & 5E
Walker BA, et al. Mutational spectrum, copy number changes, and outcome: results of a sequencing study of patients with newly diagnosed myeloma. J Clin Oncol. 2015 Nov 20;33(33):3911-3920.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 17
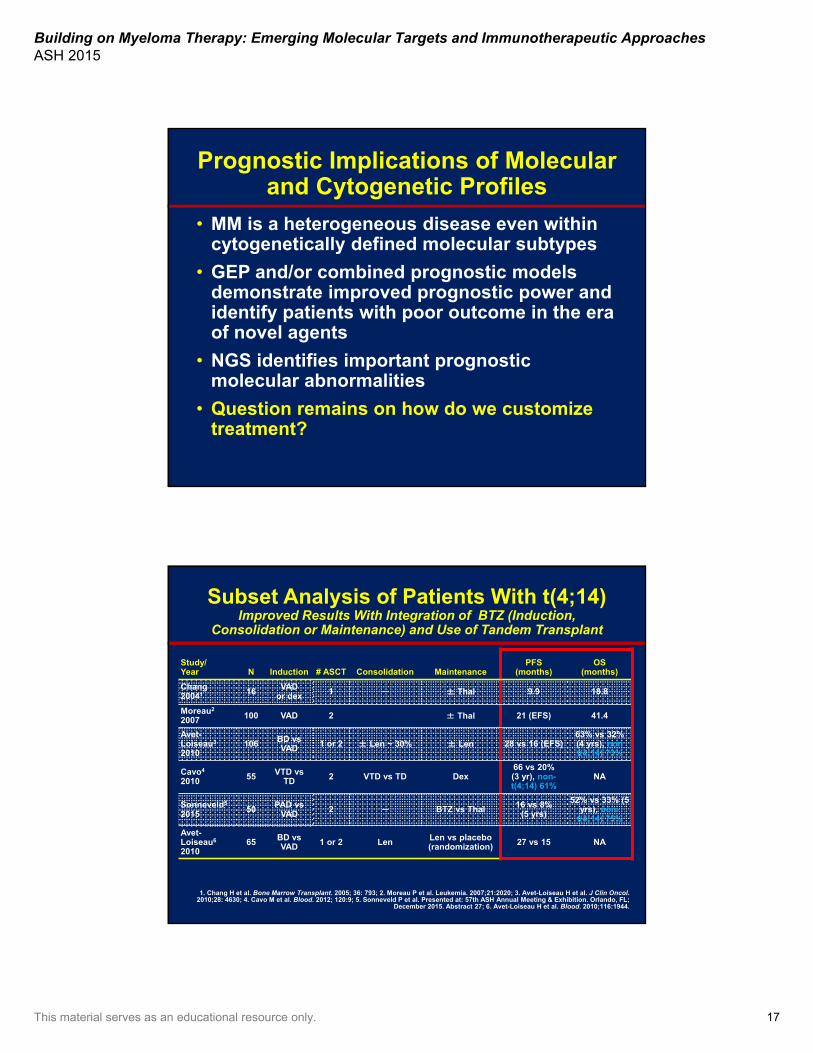
Prognostic Implications of Molecular and Cytogenetic Profiles
• MM is a heterogeneous disease even within cytogenetically defined molecular subtypes
• GEP and/or combined prognostic models demonstrate improved prognostic power and identify patients with poor outcome in the era of novel agents
• NGS identifies important prognostic molecular abnormalities
• Question remains on how do we customize treatment?
Subset Analysis of Patients With t(4;14)Improved Results With Integration of BTZ (Induction,
Consolidation or Maintenance) and Use of Tandem Transplant
Study/Year N Induction # ASCT Consolidation Maintenance
PFS(months)
OS(months)
Chang20041 16 VAD
or dex 1 ─ ± Thal 9.9 18.8
Moreau2
2007 100 VAD 2 ± Thal 21 (EFS) 41.4
Avet-Loiseau3
2010106 BD vs
VAD 1 or 2 ± Len ~ 30% ± Len 28 vs 16 (EFS)63% vs 32% (4 yrs), non t(4;14) 73%
Cavo4
2010 55 VTD vs TD 2 VTD vs TD Dex
66 vs 20% (3 yr), non-t(4;14) 61%
NA
Sonneveld5
2015 50 PAD vs VAD 2 ─ BTZ vs Thal 16 vs 8%
(5 yrs)
52% vs 33% (5 yrs), non-
t(4;14) 75%
Avet-Loiseau6
201065 BD vs
VAD 1 or 2 Len Len vs placebo (randomization) 27 vs 15 NA
1. Chang H et al. Bone Marrow Transplant. 2005; 36: 793; 2. Moreau P et al. Leukemia. 2007;21:2020; 3. Avet-Loiseau H et al. J Clin Oncol. 2010;28: 4630; 4. Cavo M et al. Blood. 2012; 120:9; 5. Sonneveld P et al. Presented at: 57th ASH Annual Meeting & Exhibition. Orlando, FL;
December 2015. Abstract 27; 6. Avet-Loiseau H et al. Blood. 2010;116:1944.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 18
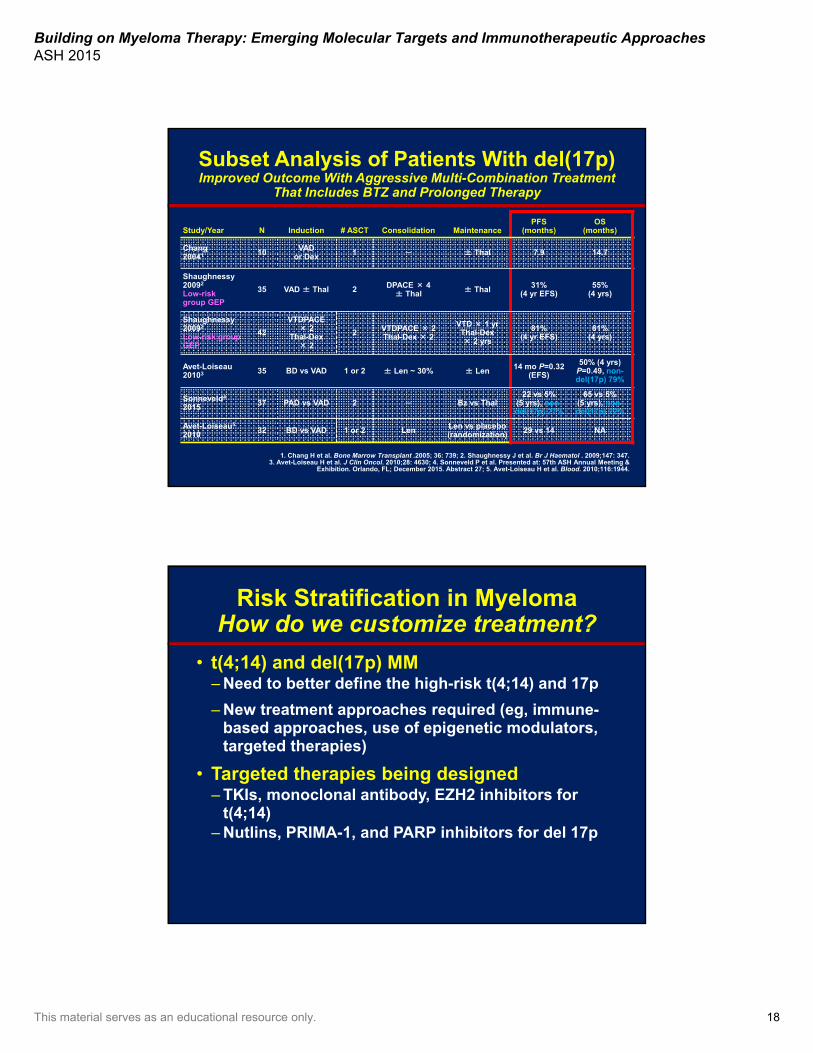
Subset Analysis of Patients With del(17p)Improved Outcome With Aggressive Multi-Combination Treatment
That Includes BTZ and Prolonged Therapy
Study/Year N Induction # ASCT Consolidation MaintenancePFS
(months)OS
(months)
Chang20041 10 VAD
or Dex 1 ─ ± Thal 7.9 14.7
Shaughnessy20092
Low-riskgroup GEP
35 VAD ± Thal 2 DPACE × 4 ± Thal ± Thal 31%
(4 yr EFS)55%
(4 yrs)
Shaughnessy20092
Low-risk group GEP
42
VTDPACE× 2
Thal-Dex× 2
2 VTDPACE × 2Thal-Dex × 2
VTD × 1 yrThal-Dex × 2 yrs
81%(4 yr EFS)
81%(4 yrs)
Avet-Loiseau20103 35 BD vs VAD 1 or 2 ± Len ~ 30% ± Len 14 mo P=0.32
(EFS)
50% (4 yrs)P=0.49, non-del(17p) 79%
Sonneveld4
2015 37 PAD vs VAD 2 ─ Bz vs Thal22 vs 5%
(5 yrs), non-del(17p) 27%
65 vs 5% (5 yrs), non-del(17p) 72%
Avet-Loiseau5
2010 32 BD vs VAD 1 or 2 Len Len vs placebo (randomization) 29 vs 14 NA
1. Chang H et al. Bone Marrow Transplant .2005; 36: 739; 2. Shaughnessy J et al. Br J Haematol . 2009;147: 347.3. Avet-Loiseau H et al. J Clin Oncol. 2010;28: 4630; 4. Sonneveld P et al. Presented at: 57th ASH Annual Meeting &
Exhibition. Orlando, FL; December 2015. Abstract 27; 5. Avet-Loiseau H et al. Blood. 2010;116:1944.
Risk Stratification in MyelomaHow do we customize treatment?
• t(4;14) and del(17p) MM– Need to better define the high-risk t(4;14) and 17p
– New treatment approaches required (eg, immune-based approaches, use of epigenetic modulators, targeted therapies)
• Targeted therapies being designed– TKIs, monoclonal antibody, EZH2 inhibitors for
t(4;14)– Nutlins, PRIMA-1, and PARP inhibitors for del 17p
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 19
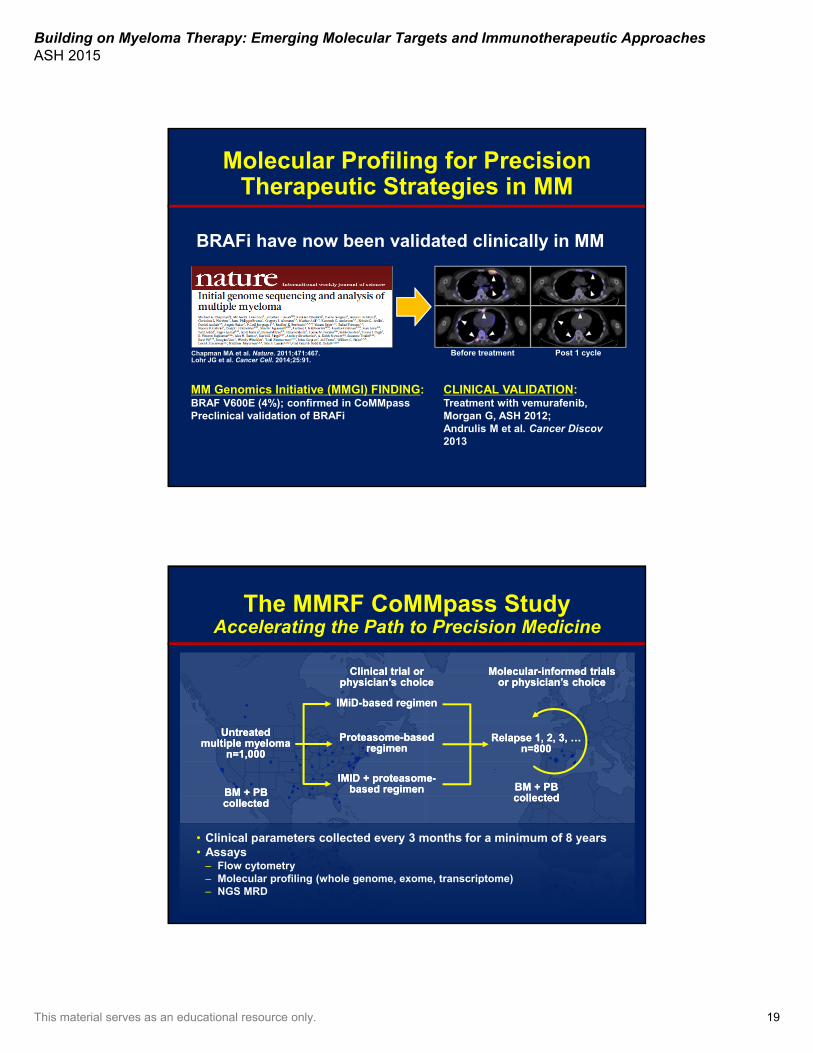
Chapman MA et al. Nature. 2011;471:467. Lohr JG et al. Cancer Cell. 2014;25:91.
CLINICAL VALIDATION:Treatment with vemurafenib, Morgan G, ASH 2012; Andrulis M et al. Cancer Discov2013
Molecular Profiling for Precision Therapeutic Strategies in MM
BRAFi have now been validated clinically in MM
Before treatment Post 1 cycle
MM Genomics Initiative (MMGI) FINDING:BRAF V600E (4%); confirmed in CoMMpassPreclinical validation of BRAFi
The MMRF CoMMpass StudyAccelerating the Path to Precision Medicine
• Clinical parameters collected every 3 months for a minimum of 8 years• Assays
– Flow cytometry– Molecular profiling (whole genome, exome, transcriptome)– NGS MRD
Untreatedmultiple myeloma
n=1,000
Untreatedmultiple myeloma
n=1,000
Clinical trial orphysician’s choice
Clinical trial orphysician’s choice
IMiD-based regimenIMiD-based regimen
Proteasome-basedregimen
Proteasome-basedregimen
IMID + proteasome-based regimen
IMID + proteasome-based regimen
Molecular-informed trialsor physician’s choice
Molecular-informed trialsor physician’s choice
Relapse 1, 2, 3, …n=800
Relapse 1, 2, 3, …n=800
BM + PBcollectedBM + PBcollected
BM + PBcollectedBM + PBcollected

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 20
“Actionable” Alterations in MMMMRF CoMMpass and other efforts have identified “actionable”
molecular alterations in about 60% of relapsed myeloma patients.
KRAS and NRAS(40%)
BRAF(8%)
CDKN2C and CCND1(18%)
PI3K-AKT(5%)
FGFR3(5%)
IGF1R and ALK(5%)
IDH1/2(5%)
MyD88(3%)
Others(11%)
Auclair D, unpublished data.
Selected Academic Molecular Screening Programs
Adapted from Bedard PL et al. Nature 2013; 501:355.
Selected Academic Molecular Screening Programs
Number of Genes
Tumor Types Tissue
MSKCC (IMPACT) 347 All Archival
Dana Farber(PROFILE)
305 (OncoPanel) All Archival
EORTC (SPECTA) ~360 Disease
specific Archival
UCSF(Genomic Medicine)
500 (UCSF 500) All Archival
MD Anderson 50–200 All Archival
Princess Margaret(IMPACT/COMPACT) ~550 All Archival or
fresh
Mayo (MM panel)MP3
~88 (including chromosomal abnormalities)
Myeloma Fresh
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 21
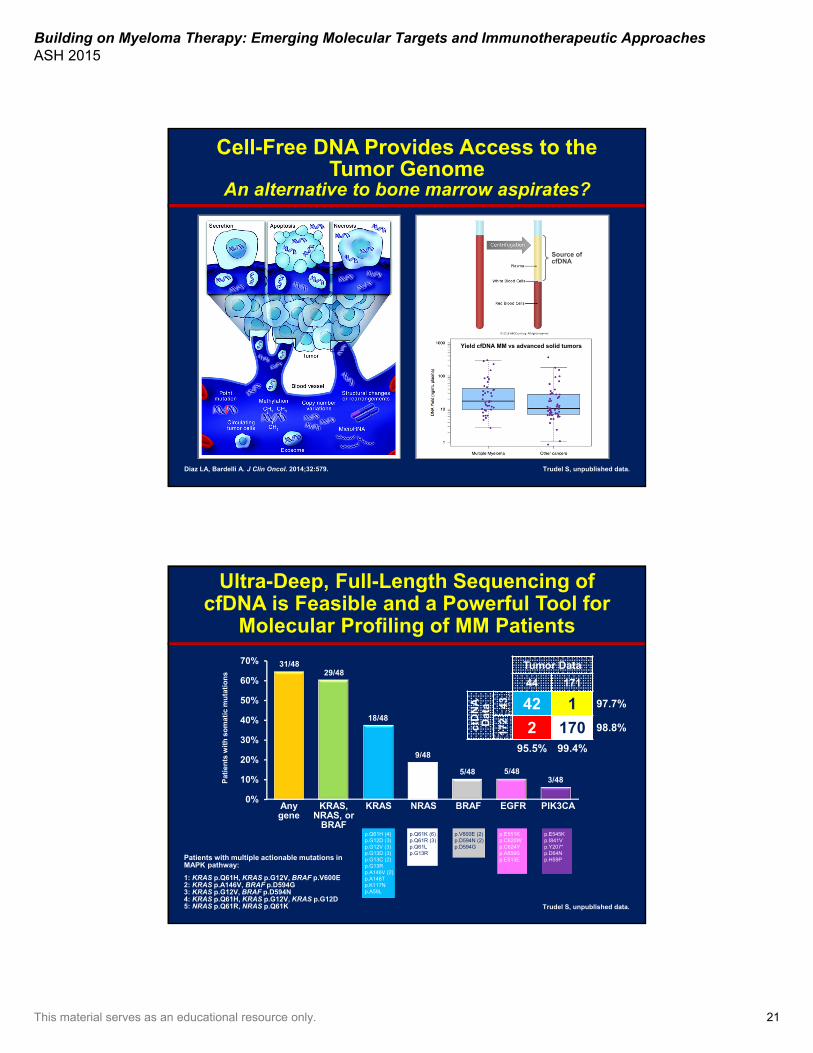
Diaz LA, Bardelli A. J Clin Oncol. 2014;32:579.
Source of cfDNA
Cell-Free DNA Provides Access to the Tumor Genome
An alternative to bone marrow aspirates?
Trudel S, unpublished data.
Yield cfDNA MM vs advanced solid tumors
Ultra-Deep, Full-Length Sequencing of cfDNA is Feasible and a Powerful Tool for
Molecular Profiling of MM Patients
0%
10%
20%
30%
40%
50%
60%
70%
p.E545Kp.I841Vp.Y207*p.D64Np.H59P
p.E551Kp.C620Wp.C624Yp.A859Sp.E513E
p.V600E (2)p.D594N (2)p.D594G
p.Q61K (6)p.Q61R (3)p.Q61L p.G13R
p.Q61H (4)p.G12D (3)p.G12V (3)p.G13D (3)p.G13C (2)p.G13Rp.A146V (2)p.A146Tp.K117Np.A59L
31/4829/48
18/48
9/48
5/48 5/483/48
Patients with multiple actionable mutations in MAPK pathway:
1: KRAS p.Q61H, KRAS p.G12V, BRAF p.V600E2: KRAS p.A146V, BRAF p.D594G3: KRAS p.G12V, BRAF p.D594N4: KRAS p.Q61H, KRAS p.G12V, KRAS p.G12D5: NRAS p.Q61R, NRAS p.Q61K Trudel S, unpublished data.
Any gene
KRAS,NRAS, or
BRAF
KRAS NRAS BRAF EGFR PIK3CA
Tumor Data
44 171
ctD
NA
D
ata 43 42 1 97.7%
172
2 170 98.8%
95.5% 99.4%
Pat
ien
ts w
ith
so
mat
ic m
uta
tio
ns
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 22
Conclusions• Risk stratification should include combination of ISS
(β2M and albumin), LDH, and chromosomal abnormalities: del(17p), t(4;14), t(14;16), and 1q21 by FISH or GEP
• Prognostic implications are now impacting treatment decisions (use of BTZ, tandem transplant, prolonged treatment)
• NGS studies have uncovered novel prognostic biomarkers and actionable mutations and has the potential to replace iFISH
• With the right small-molecule therapeutic tools we should be able to therapeutically manipulate the key deregulated pathways (eg, clinical data now supports the strategy of targeting MAPK signaling)
Induction Therapy Options for Transplant-Eligible and -Ineligible Patients
María-Victoria Mateos, MD, PhDConsultant Physician
Haematology DepartmentUniversity Hospital of Salamanca
Salamanca, Spain
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 23
Disclosures• María-Victoria Mateos, MD, PhD, has
disclosed the following relevant financial relationships:
– Janssen, Celgene, Takeda, Amgen, BMS, Novartis
• Dr. Mateos will discuss the unlabeled or investigational use of a commercial product.
Main Objectives for NDMM Patients
A. CureB. Prolong overall survival (OS)C. Prolong progression-free
survival (PFS)D. Maintain quality of lifeE. Prolong PFS, OS, and ensure good
quality of life
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 24
Maximal Eradication of Tumor Clone Through Achievement of Best Possible
Response
Figure 2, page 532
Martinez-Lopez J, et al. Long-term prognostic significance of response in multiple myeloma after stem cell transplantation. Blood. 2011 Jul; 21;118:529-534.
Main Objectives for NDMM Patients
A. Cure
B. Prolong OS
C. Prolong PFS
D. Maintain quality of life
E. Prolong PFS, OS, and ensure good quality of life

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 25
Main Objectives for NDMM Patients
A. Cure
B. Prolong OS
C. Prolong PFS
D. Maintain quality of life
E. Prolong PFS, OS, and ensure good quality of life
Does quality of the response predict final outcome?
Impact of MRD Detected by Flow Cytometry on Clinical Outcomes
Figure 4A & 4B, page 2544
Rawstron AC, et al. Minimal residual disease assessed by multiparameter flow cytometry in multiple myeloma: impact on outcome in the Medical Research Council Myeloma IX Study. J ClinOncol. 2013 Jul 10;31(20):2540-2547.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 26
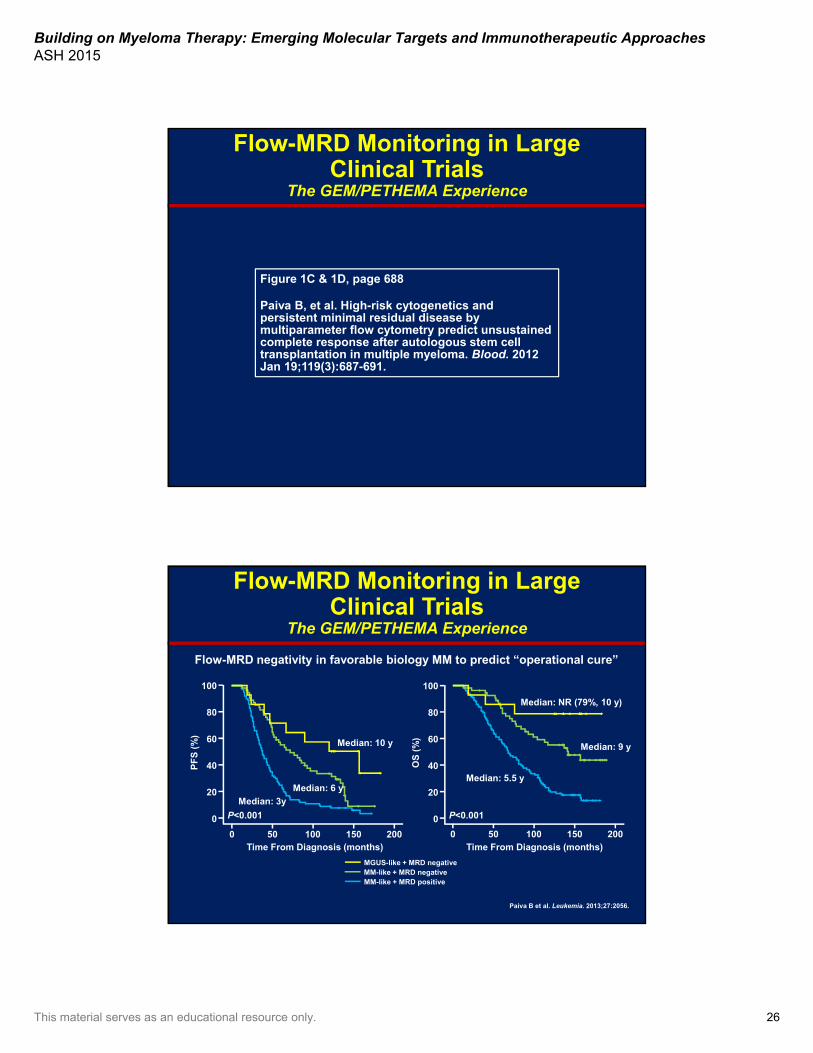
Flow-MRD Monitoring in Large Clinical Trials
The GEM/PETHEMA Experience
Figure 1C & 1D, page 688
Paiva B, et al. High-risk cytogenetics and persistent minimal residual disease by multiparameter flow cytometry predict unsustainedcomplete response after autologous stem cell transplantation in multiple myeloma. Blood. 2012 Jan 19;119(3):687-691.
Flow-MRD negativity in favorable biology MM to predict “operational cure”
Paiva B et al. Leukemia. 2013;27:2056.
Flow-MRD Monitoring in Large Clinical Trials
The GEM/PETHEMA Experience
Time From Diagnosis (months) Time From Diagnosis (months)
Median: 10 y
Median: 6 y
Median: 3y
0
20
40
60
80
100
PF
S (
%)
P<0.001
0 50 100 150 200
0
20
40
60
80
100
OS
(%
)
P<0.001
Median: NR (79%, 10 y)
Median: 9 y
Median: 5.5 y
0 50 100 150 200
MGUS-like + MRD negativeMM-like + MRD negativeMM-like + MRD positive
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 27
8 cycles of CRd lenalidomide (2-year)
• MRD testing was clinically feasible in 55 of 56 (98%) patient samples by MFC (1 patient sample was not processed due to equipment breakdown)
• NGS assay at MRD was technically successful in 45 of 56 (80%) patient samples (8 with undetectable clonotypes; 3 without available sample)
Flow and NGS-MRD Monitoring: The NIH Experience
Figure 3B & 3C, page 752
Korde N, et al. Treatment with carfilzomib-lenalidomide-dexamethasone with lenalidomideextension in patients with smoldering or newlydiagnosed multiple myeloma. JAMA Oncol. 2015 Sep;1(6):746-754.
Important Aim of Treatment
• CR should be an important objective in this patient
• Achievement of high-quality, sustained CR balanced with acceptable toxicity can translate into an “operational cure”
Does imaging assessment matter in this young patient with bone disease?

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 28
Impact of Post-ASCT PET-CT Negativity on Clinical Outcomes
Figure 3, page 5994
Zamagni E, et al. Prognostic relevance of 18-F FDG PET/CT in newly diagnosed multiple myeloma patients treated with up-front autologous transplantation. Blood. 2011 Dec 1;118(23):5989-5995.
Important Aim of Treatment
• CR should be an important objective in this patient
• Achievement of high-quality, sustained CR balanced with acceptable toxicity can translate into an “operational cure”*
What is the best option of therapy for this patient?
*Inside and outside bone marrow

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 29
54-Year-Old Man With Newly Diagnosed MM IgGκ: Anemia, Hypercalcemia, and Bone Lesions
What is the option of therapy proposed?
A. Induction + ASCT + consolidation + maintenance
B. Induction + consolidation and maintenance
C. Induction + ASCTD. Induction + ASCT + maintenance
Is there something better than VAD or thalidomide/dexamethasone?
Modified from Figure 2, page 5438
Stewart AK, et al. How I treat multiple myeloma in younger patients. Blood. 2009 Dec 24;114(27):5436-5443.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 30
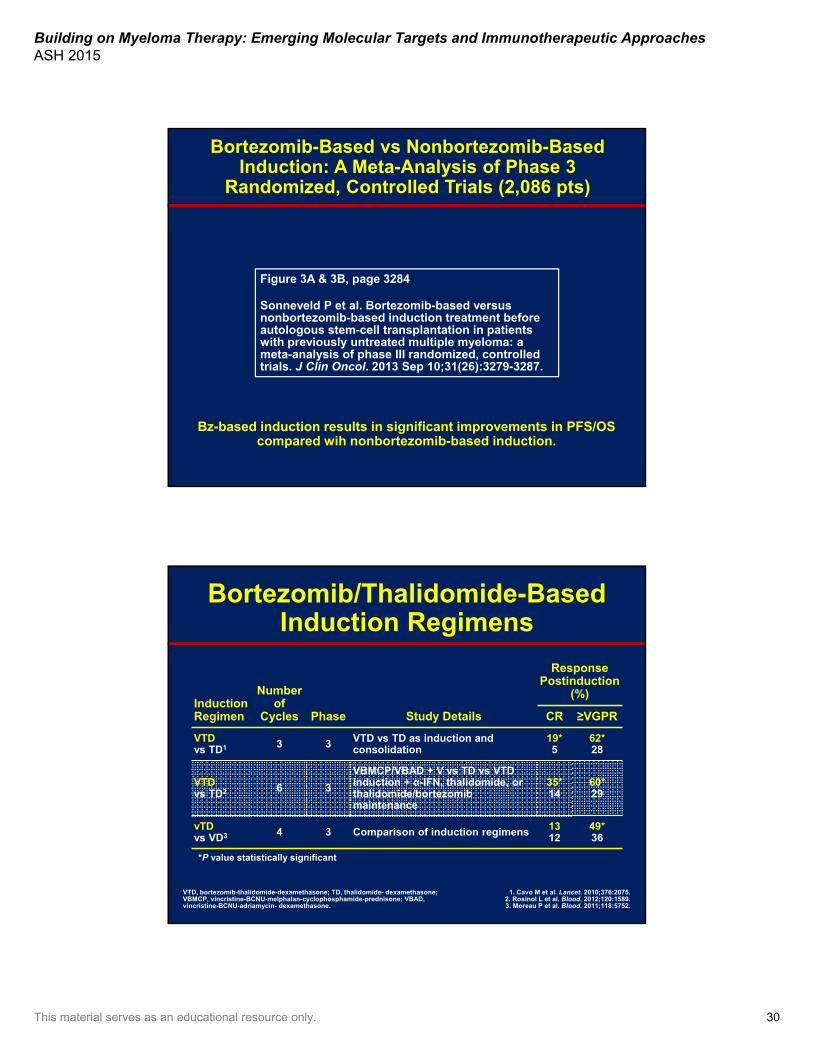
Bortezomib-Based vs Nonbortezomib-BasedInduction: A Meta-Analysis of Phase 3
Randomized, Controlled Trials (2,086 pts)
Bz-based induction results in significant improvements in PFS/OS compared wih nonbortezomib-based induction.
Figure 3A & 3B, page 3284
Sonneveld P et al. Bortezomib-based versus nonbortezomib-based induction treatment beforeautologous stem-cell transplantation in patientswith previously untreated multiple myeloma: a meta-analysis of phase III randomized, controlledtrials. J Clin Oncol. 2013 Sep 10;31(26):3279-3287.
*P value statistically significant
Bortezomib/Thalidomide-Based Induction Regimens
InductionRegimen
Number of
Cycles Phase Study Details
ResponsePostinduction
(%)
CR ≥VGPR
VTD vs TD1 3 3 VTD vs TD as induction and
consolidation19*5
62*28
VTD vs TD2 6 3
VBMCP/VBAD + V vs TD vs VTD induction + α-IFN, thalidomide, or thalidomide/bortezomib maintenance
35*14
60*29
vTD vs VD3 4 3 Comparison of induction regimens 13
1249*36
1. Cavo M et al. Lancet. 2010;376:2075.2. Rosinol L et al. Blood. 2012;120:1589.3. Moreau P et al. Blood. 2011;118:5752.
VTD, bortezomib-thalidomide-dexamethasone; TD, thalidomide- dexamethasone; VBMCP, vincristine-BCNU-melphalan-cyclophosphamide-prednisone; VBAD, vincristine-BCNU-adriamycin- dexamethasone.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 31
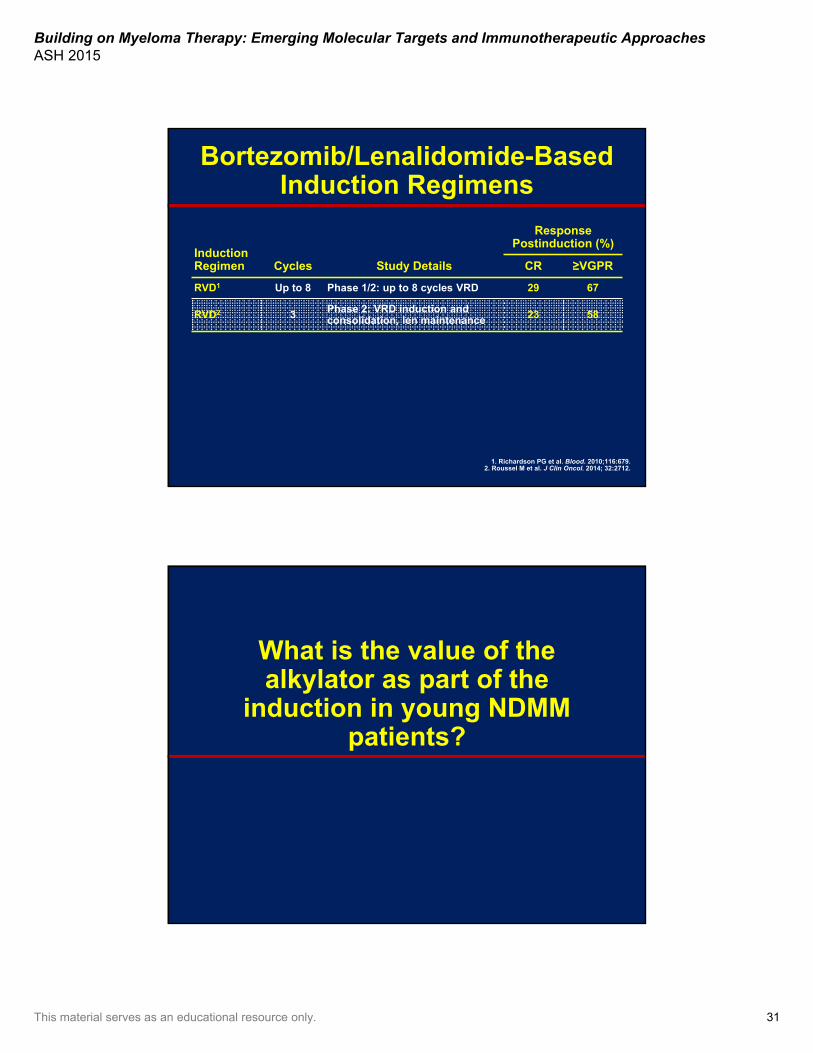
Bortezomib/Lenalidomide-Based Induction Regimens
InductionRegimen Cycles Study Details
ResponsePostinduction (%)
CR ≥VGPR
RVD1 Up to 8 Phase 1/2: up to 8 cycles VRD 29 67
RVD2 3 Phase 2: VRD induction and consolidation, len maintenance 23 58
1. Richardson PG et al. Blood. 2010;116:679.2. Roussel M et al. J Clin Oncol. 2014; 32:2712.
What is the value of thealkylator as part of the
induction in young NDMM patients?

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 32
Retrospective, Case-Matched Analysis: VTD vs VCD Induction
Patients enrolled in GIMEMA MMY-3006 study and EMN-02 study
VTD (n=236)
VCD (n=236) P
Response to induction therapy
CR 19% 6% <0.001
≥ VGPR 64% 37% <0.001
≥ PR 93% 81% <0.001
Toxicity
Any grade 3–4 hematological AE 2% 8% 0.003
Any grade 3–4 PN 7% 2% 0.009
No difference between regimens in terms of efficiency to mobilize PBSC.
Cavo M et al. Leukemia. 2015;Oct 7 [Epub ahead of print].AE, adverse event; PN, peripheral neuropathy; PBSC, peripheral blood stem cell.
What has been the value of addition a fourth drug for induction in young NDMM
patients so far?

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 33
Is the Alkylator Necessary as Part of the Induction?
Phase 2 Randomized European Trial
Ludwig H et al. J Clin Oncol. 2013;31:247.
Response, %VTD
(N=49)VTDCy(N=48)
After induction
CR (%) 27 27
≥VGPR (%) 69 69
ORR (%) 100 96
Post ASCT
CR/nCR (%) 85 77
MRD negative (%) 35 27
3-y OS (%) 80 80
G3–4 AEs/SAEs (%) 47/22 57/41
The addition of the alkylator as fourth drug doesnot add any significant benefit
SAE, serious adverse events.
EVOLUTION Trial: Three- and Four-Drug Combinations for NDMM Patients
Response, n (%)VDCR (n=40)
VDR (n=41)
VDC (n=32)
VDC-mod (n=17)
CR 2 (5) 3 (7) 1 (3) 2 (12)
sCR 1 (3) 1 (2) 0 2 (12)
VGPR 11 (26) 10 (24) 3 (9) 5 (29)
≥ VGPR 13 (33) 13 (32) 4 (13) 7 (41)
≥ nCR 4 (10) 3 (7) 1 (3) 3 (18)
ORR (≥ PR) 32 (80) 30 (73) 20 (63) 14 (82)
Progressive disease 0 0 0 0
Patients categorized as VGPR include those who have no measurable M-protein but have not yet had bone marrow assessments to confirm CR/nCR status.
Kumar S et al. Blood. 2012;119:4375.
No substantial advantage was observed in four- vs three-drug combinations.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 34
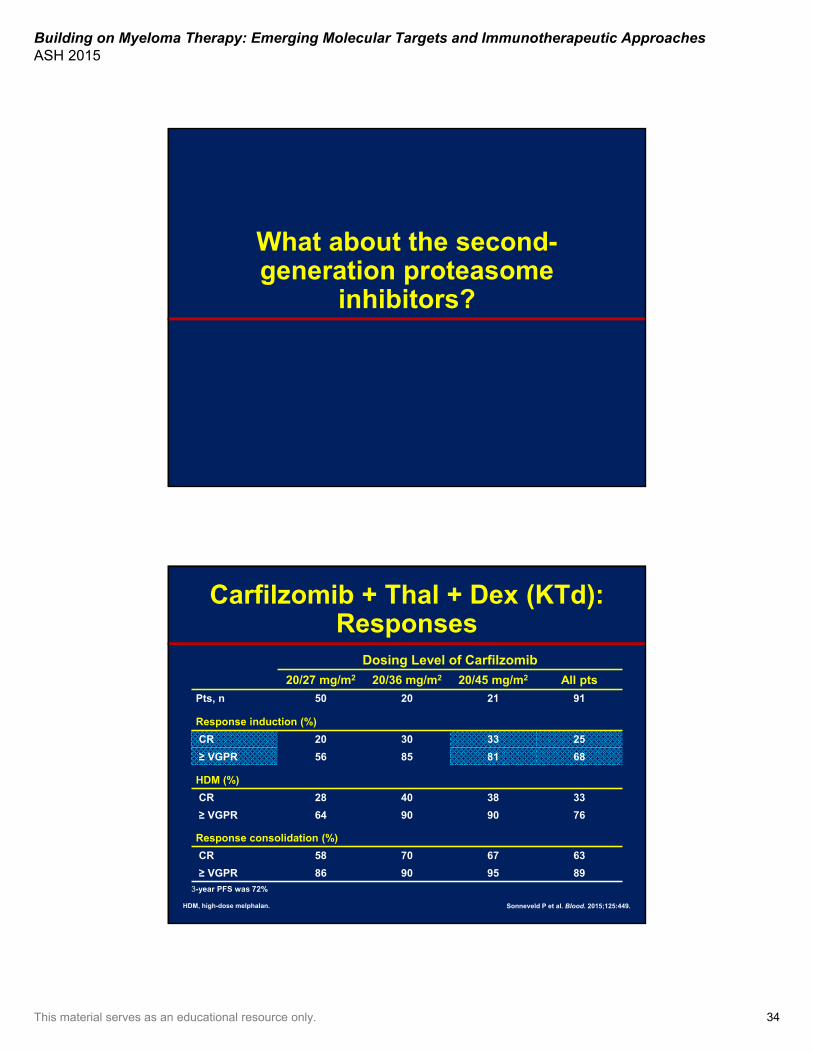
What about the second-generation proteasome
inhibitors?
HDM, high-dose melphalan.
Carfilzomib + Thal + Dex (KTd): Responses
3-year PFS was 72%
Sonneveld P et al. Blood. 2015;125:449.
Dosing Level of Carfilzomib
20/27 mg/m2 20/36 mg/m2 20/45 mg/m2 All pts
Pts, n 50 20 21 91
Response induction (%)
CR 20 30 33 25
≥ VGPR 56 85 81 68
HDM (%)
CR 28 40 38 33
≥ VGPR 64 90 90 76
Response consolidation (%)
CR 58 70 67 63
≥ VGPR 86 90 95 89
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 35
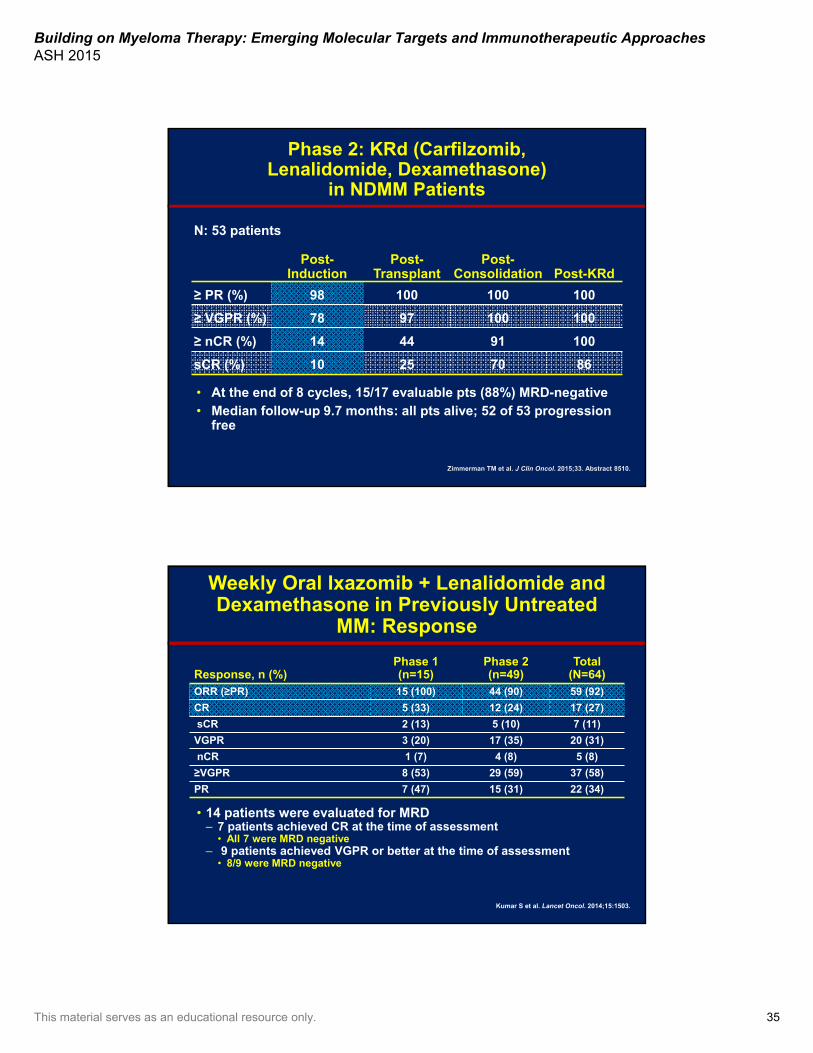
Phase 2: KRd (Carfilzomib, Lenalidomide, Dexamethasone)
in NDMM Patients
N: 53 patients
Post-Induction
Post-Transplant
Post-Consolidation Post-KRd
≥ PR (%) 98 100 100 100
≥ VGPR (%) 78 97 100 100
≥ nCR (%) 14 44 91 100
sCR (%) 10 25 70 86
• At the end of 8 cycles, 15/17 evaluable pts (88%) MRD-negative• Median follow-up 9.7 months: all pts alive; 52 of 53 progression
free
Zimmerman TM et al. J Clin Oncol. 2015;33. Abstract 8510.
Weekly Oral Ixazomib + Lenalidomide and Dexamethasone in Previously Untreated
MM: Response
• 14 patients were evaluated for MRD– 7 patients achieved CR at the time of assessment
• All 7 were MRD negative– 9 patients achieved VGPR or better at the time of assessment
• 8/9 were MRD negative
Kumar S et al. Lancet Oncol. 2014;15:1503.
Response, n (%)Phase 1 (n=15)
Phase 2 (n=49)
Total (N=64)
ORR (≥PR) 15 (100) 44 (90) 59 (92)
CR 5 (33) 12 (24) 17 (27)
sCR 2 (13) 5 (10) 7 (11)
VGPR 3 (20) 17 (35) 20 (31)
nCR 1 (7) 4 (8) 5 (8)
≥VGPR 8 (53) 29 (59) 37 (58)
PR 7 (47) 15 (31) 22 (34)

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 36
What about the addition of “a different fourth drug” in the
near future?
Daratumumab + Bortezomib-Thalidomide-DexElotuzumab + Bortezomib-Lenalidomide-Dex
• Dara-bortezomib (sc)-thalidomide-dexamethasone (VTD)1
– 100% ORR– Daratumumab does not appear to have a negative effect on
stem cell mobilization
• Phase 3 study is ongoing – VTD + daratumumab (induction, MMY3006/IFM-HOVON-
CASSIOPEIA)
• Elo-bortezomib (sc)-lenalidomide-dexamethasone (VRD)*2
– The addition of Elo is feasible with no major additive adverse events
1. Mateos MV et al. Haematologica. 2015;100. Abstract P275.2. Usmani SZ et al. Blood Cancer J. 2015;5:e334.*In high-risk patients

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 37
GEM2005MAS65: VMP/VTP→VT/VPImpact of Response in the Whole Series of Patients
(n=260)
Figure 3A & 3B, page 1891
Mateos MV et al. GEM2005 trial update comparing VMP/VTP as induction in elderly multiple myeloma patients: do we still need alkylators? Blood. 2014 Sep 18;124(12):1887-1893.
GEM2005MAS65: VMP/VTP→VT/VPImpact of Flow-CR in the Whole Series After Induction
(n=153)
Modified from Figure 3C & 3D, page 1891
Mateos MV et al. GEM2005 trial update comparing VMP/VTP as induction in elderly multiple myeloma patients: do we still need alkylators? Blood. 2014 Sep 18;124(12):1887-1893.

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 38
MPT
MP
VMP
Alkylator-based regimens
Alkylator-freeregimens
Len-dex
IMiDs
Six randomized trials:benefit in
PFS & OS...6 m
One randomized trial:benefit in PFS & OS
One randomized trial:benefit in PFS & OS
vs MPT
New Standards of Care for Elderly MM Patients
Figure 1
San Miguel JF et al. Bortezomib plus melphalan and prednisone for initial treatment of multiple myeloma. N Engl J Med. 2008 Aug 28;359(9):906-917.
Figure 2, page 451
San Miguel JF, et al. Persistent overall survival benefit and no increased risk of second malignancies with bortezomib-melphalan-prednisone versus melphalan-prednisone in patients with previously untreated multiple myeloma. J Clin Oncol. 2013 Feb 1;31(4):448-455.
MP + Bortezomib (VMP) vs MP: VISTABortezomib Twice a Week× 4 Cycles + Weekly× 5 Cycles

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 39
Further optimization was done through subcutaneous administration.5
Modified-VISTA Schemes: Weekly Bortezomib
Study Details
Grade 3/4GI
Toxicity (%)
Grade 3/4 Peripheral
Neuropathy (%)
ORR (%)
CR (%)
PFS (mos)
OS (mos)
VISTA1,2: VMP Bortezomib twice weekly (5+4 cycles)
20 14 71 30 21 56
PETHEMA/GEM3: VMP Bortezomib once weekly except 1st cycle (6 cycles)
7 7 80 20 — —
GIMEMA4: VMP Bortezomib once weekly (9 cycles)
— 5 81 24 25 54
1. San Miguel J et al. J Clin Oncol. 2013; 31:448.2. San Miguel J et al. N Engl J Med. 2008;359:906.
3. Mateos MV et al. Lancet Oncol. 2010;11:934.4. Palumbo A et al. J Clin Oncol. 2010;28:5101.
5. Moreau P et al. Lancet Oncol. 2011;12:431.
FIRST Trial: Study Design
1. Benboubker L et al. N Engl J Med. 2014;371:906. 2. Facon T et al. Lancet. 2007;370:1209.
3. Hulin C et al. J Clin Oncol. 2009;27:3664.
Patients >75 yrs: LoDEX 20 mg D1, 8, 15, 22/28; THAL 100 mg D1–42/42; MEL 0.2 mg/kg D1–4.All patients received thromboprophylaxis.
• Stratification: age, country, and ISS stage
RA
ND
OM
IZA
TIO
N 1
:1:1
Arm BRd18
Arm CMPT
LEN + LoDEX 18 Cycles1 (72 wks) LENALIDOMIDE 25 mg D1-21/28LoDEX 40 mg D1,8,15 & 22/28
MEL + PRED + THAL 12 Cycles2,3 (72 wks)MELPHALAN 0.25 mg/kg D1-4/42PREDNISONE 2 mg/kg D1-4/42THALIDOMIDE 200 mg D1-42/42
PD
, OS
, an
d
Su
bse
qu
ent
AM
T
PD
or
Un
acce
pta
ble
To
xici
ty
Active Treatment + PFS Follow-up Phase
LEN + LoDEX Continuously1
LENALIDOMIDE 25 mg D1-21/28LoDEX 40 mg D1,8,15 & 22/28
Arm ARd Continuous
ScreeningLT
Follow-Up
AMT, antimyeloma therapy; ISS, International Staging System; LEN, lenalidomide; LoDEX, low-dose dexamethasone; LT, long-term; MEL, melphalan; PD, progressive disease; PRED, prednisone; THAL, thalidomide.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 40
FIRST Trial: Progression-Free Survival & Overall Survival
Figure 1A & 1B, page 912
Benboubker L, et al. Lenalidomide and dexamethasone in transplant-ineligible patients with myeloma. N Engl J Med. 2014 Sep 4;371(10):906-917.
Severely frail:Dependent on other
people
Elderly MM Patients Are a Heterogeneous Group
Very fit: Active, exercise
regularly
Moderately fit:Not regularly active but
routinely walking
Vulnerable:Can perform limitedactivities; don’t need
help
Mildly frail:Need help for
household tasks
Moderately frail:Need partial help for
personal care
Palumbo A et al. Blood. 2011;118:4519.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 41
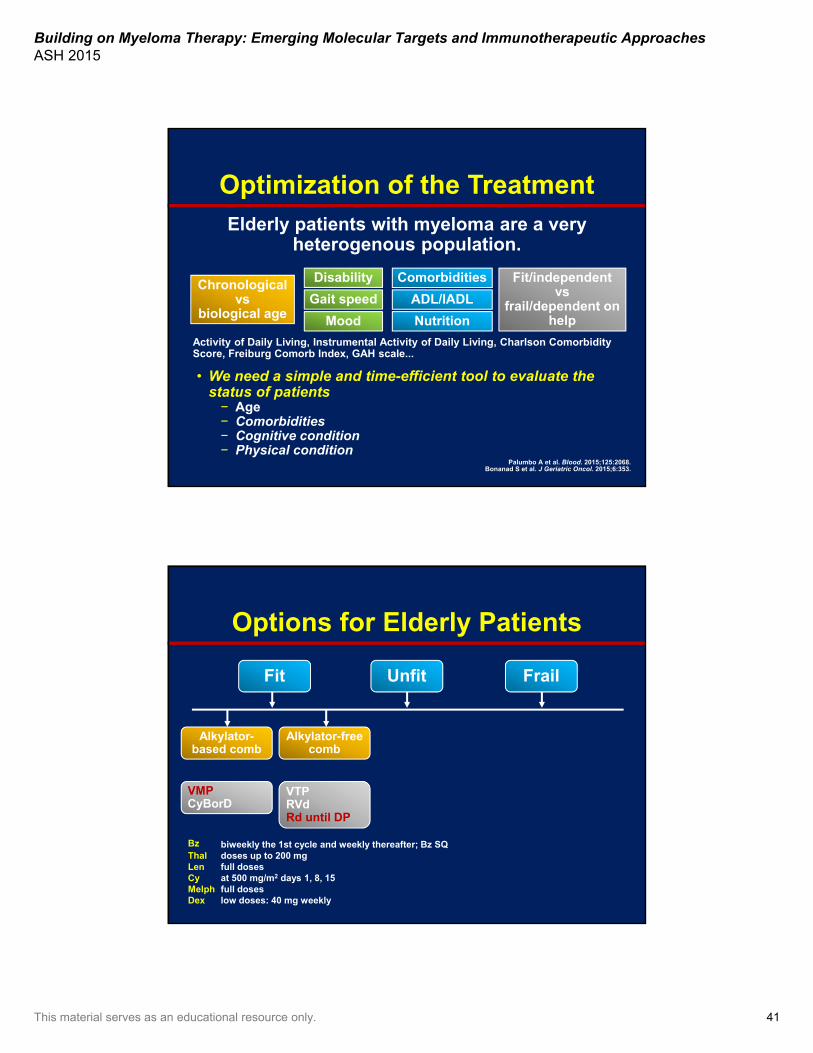
Optimization of the Treatment
Chronological vs
biological age
Fit/independent vs
frail/dependent on help
ComorbiditiesDisability
• We need a simple and time-efficient tool to evaluate the status of patients− Age− Comorbidities− Cognitive condition− Physical condition
Palumbo A et al. Blood. 2015;125:2068.Bonanad S et al. J Geriatric Oncol. 2015;6:353.
Elderly patients with myeloma are a veryheterogenous population.
Activity of Daily Living, Instrumental Activity of Daily Living, Charlson Comorbidity Score, Freiburg Comorb Index, GAH scale...
Gait speed
Mood
ADL/IADL
Nutrition
Options for Elderly Patients
Fit Unfit Frail
Alkylator-based comb
VMPCyBorD
Alkylator-free comb
VTPRVdRd until DP
Bz biweekly the 1st cycle and weekly thereafter; Bz SQThal doses up to 200 mgLen full dosesCy at 500 mg/m2 days 1, 8, 15Melph full dosesDex low doses: 40 mg weekly
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 42
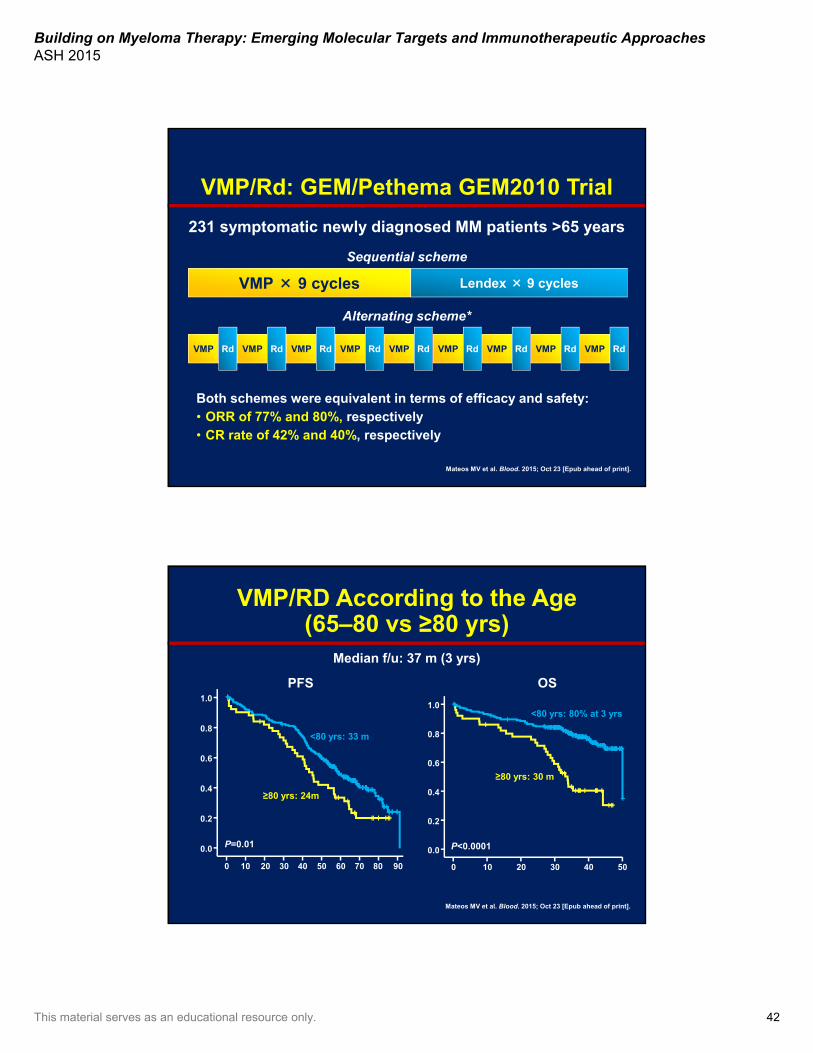
VMP × 9 cycles Lendex × 9 cycles
Sequential scheme
Alternating scheme*
Mateos MV et al. Blood. 2015; Oct 23 [Epub ahead of print].
Both schemes were equivalent in terms of efficacy and safety:• ORR of 77% and 80%, respectively• CR rate of 42% and 40%, respectively
VMP/Rd: GEM/Pethema GEM2010 Trial
VMP Rd VMP Rd VMP Rd VMP Rd VMP Rd VMP Rd VMP Rd VMP Rd VMP Rd
231 symptomatic newly diagnosed MM patients >65 years
VMP/RD According to the Age(65–80 vs ≥80 yrs)
Mateos MV et al. Blood. 2015; Oct 23 [Epub ahead of print].
≥80 yrs: 24m
<80 yrs: 33 m
P=0.01
9080706050403020100
1.0
0.8
0.6
0.4
0.2
0.0
Median f/u: 37 m (3 yrs)
PFS
≥80 yrs: 30 m
<80 yrs: 80% at 3 yrs
P<0.0001
50403020100
1.0
0.8
0.6
0.4
0.2
0.0
OS
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 43
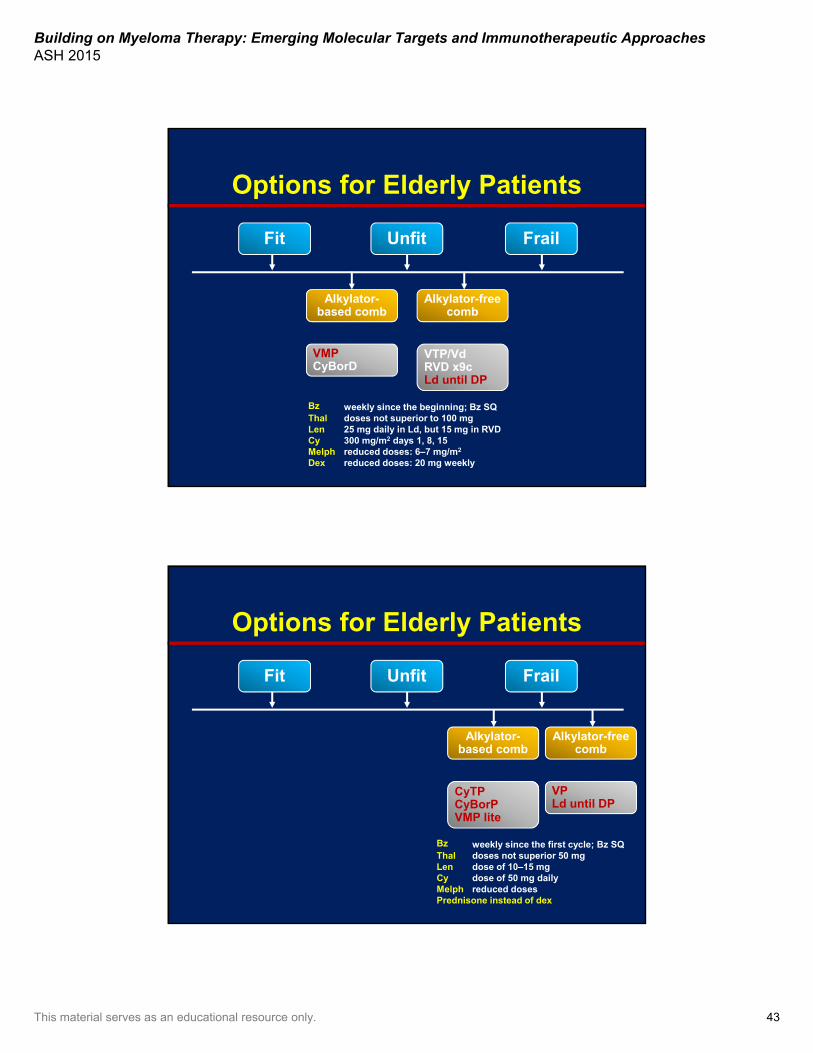
Alkylator-based comb
VMP CyBorD
Alkylator-free comb
VTP/VdRVD x9cLd until DP
Options for Elderly Patients
Bz weekly since the beginning; Bz SQThal doses not superior to 100 mgLen 25 mg daily in Ld, but 15 mg in RVDCy 300 mg/m2 days 1, 8, 15Melph reduced doses: 6–7 mg/m2
Dex reduced doses: 20 mg weekly
Fit Unfit Frail
Options for Elderly Patients
Fit Unfit Frail
Alkylator-based comb
CyTPCyBorPVMP lite
Alkylator-free comb
VPLd until DP
Bz weekly since the first cycle; Bz SQThal doses not superior 50 mgLen dose of 10–15 mgCy dose of 50 mg dailyMelph reduced dosesPrednisone instead of dex
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 44
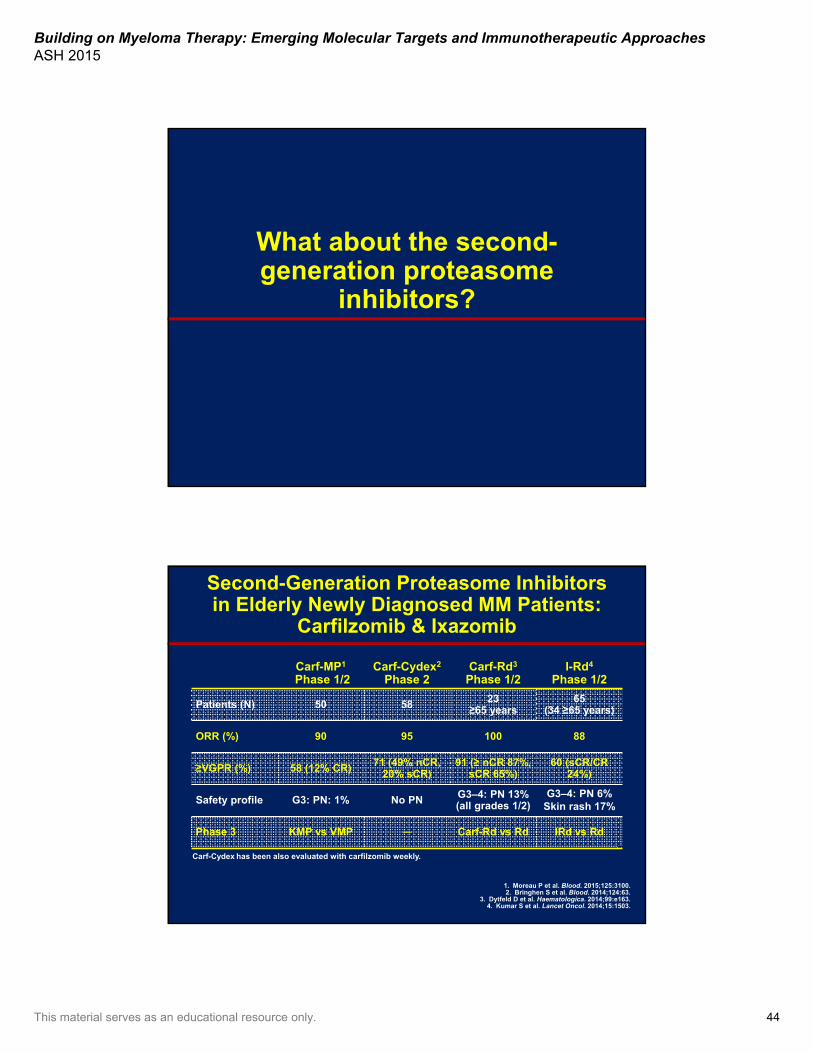
What about the second-generation proteasome
inhibitors?
Second-Generation Proteasome Inhibitorsin Elderly Newly Diagnosed MM Patients:
Carfilzomib & Ixazomib
1. Moreau P et al. Blood. 2015;125:3100.2. Bringhen S et al. Blood. 2014;124:63.
3. Dytfeld D et al. Haematologica. 2014;99:e163.4. Kumar S et al. Lancet Oncol. 2014;15:1503.
Carf-Cydex has been also evaluated with carfilzomib weekly.
Carf-MP1
Phase 1/2Carf-Cydex2
Phase 2Carf-Rd3
Phase 1/2I-Rd4
Phase 1/2
Patients (N) 50 58 23≥65 years
65(34 ≥65 years)
ORR (%) 90 95 100 88
≥VGPR (%) 58 (12% CR) 71 (49% nCR, 20% sCR)
91 (≥ nCR 87%, sCR 65%)
60 (sCR/CR 24%)
Safety profile G3: PN: 1% No PN G3–4: PN 13% (all grades 1/2)
G3–4: PN 6%Skin rash 17%
Phase 3 KMP vs VMP ─ Carf-Rd vs Rd IRd vs Rd

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 45
What will be the addition of “a different fourth drug” in the
near future?
VMP +/- DaratumumabLenalidomide-Dex +/- DaratumumabLenalidomide-Dex +/- Elotuzumab
• Bortezomib (sc)-melphalan and prednisone (VMP) + dara– 100% ORR
• Phase 3 studies are ongoing – VMP +/- Daratumumab (Alcyone trial)– Rd +/- Daratumumab (Maia trial)– Rd +/- Elotuzumab (Eloquent-1 trial):
completed recruitment
Mateos MV et al. Haematologica. 2015;100. Abstract P275.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 46
Conclusions• Highest quality of the response (inside/outside BM)
should be the goal for all MM patients• PI-based combinations plus IMiDs will be the standard of
care as induction for NDMM patients, plus the addition of mAbs
• Number of cycles undecided: – 4–6 for trx-eligible– Fixed vs continuous for non-trx eligible
• Dose adjustments should be considered based on age and comorbidities to enable optimal delivery of effective therapy
• Numerous planned/ongoing studies addressing questions of optimal regimen, schedule, treatment duration...to optimize and individualize induction therapy
Panel Discussion
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 47
Community Case Part 2
Case Study Part 2• Induction chemotherapy: RVd × 4 cycles
– Aspirin and acyclovir prophylaxis
• Bone health: bisphosphonates every month
• Best response: VGPR by IMWG criteria
• Relevant events during induction– Grade II peripheral neuropathy after cycle #2
• Started on gabapentin, symptoms controlled
– Increasing lower back pain during cycle #3• L3 compression fracture, undergoes kyphoplasty with
near complete resolution of back pain

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 48
Based on the patient’s response to induction therapy, you collect stem cells.
What would you consider next ?
A. Continue current regimen
B. Wait to transplant after relapse
C. Proceed to transplant
D. Provide consolidation therapy
?
Case Study Part 2• Transplant eligible• Collects 13.5 million CD34 cells/kg BW in six bags• Mel-200 ASCT with 4.2 million CD34 cells/kg BW in
two bags• Transplant course: grade 3 diarrhea, resolved by Day
+28• Restaging post-ASCT
– M spike 0– Normal k/l ratio– BM biopsy shows no clonal PCs and normal hematopoiesis– sCR by IMWG criteria
• Patient comes to discuss maintenance
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 49
Is now an appropriate time for MRD testing?
A. YesB. NoC. Not sure
?
Do you recommend maintenance?
A. YesB. NoC. Not sure
?
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 50
Would the MRD result affect your decision to use maintenance therapy?
A. YesB. NoC. Not sure
?
Which maintenance treatment do you recommend?
A. LenalidomideB. BortezomibC. Lenalidomide, bortezomibD. ThalidomideE. PrednisoneF. Clinical trialG. I don’t use maintenance
?
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 51
Would your maintenance choice change if the patient had low-risk cytogenetics?
A. YesB. NoC. Not sure
?
High-Dose Therapy and Hematopoietic Cell
Transplantation: Current Status in Myeloma
Sergio A. Giralt, MDMelvin Berlin Family Chair in Myeloma Research
Professor of MedicineWeill Cornell Medical College
Chief, Adult Bone Marrow Transplant ServiceDivision of Hematologic Oncology
Department of MedicineMemorial Sloan Kettering Cancer Center
New York, New York
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 52
Disclosures
• Consultant/Advisor: Celgene, Jazz Pharmaceuticals, Onyx Pharmaceuticals, an Amgen subsidiary, Sanofi, Takeda Oncology
• Research Grant: Celgene, Sanofi, Takeda Oncology
Rationale for High-Dose Therapy
100%
Cures
DoseLethal bone
marrow toxicityLethal toxicity
to other organs
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 53
McElwain et alLancet 1983
McElwain TJ, Powles RL. Lancet. 1983;2:822.Barlogie B et al. Blood. 1987;70:869.
Transplant Eligible vs Transplant Ineligible
Transplant ineligible• Poor performance status
– Elderly and frail– Unable to perform activities of daily living– Decompensated comorbidity
• Congestive heart failure (CHF)• Uncontrolled diabetes• Unstable angina
• Socioeconomic factors– Lack of caregiver– Distance from transplant center– Inability to comply with peritransplant
follow-up care• Patient choice• Very low–risk disease
– Asymptomatic myeloma– Solitary plasmacytoma
• AGE PER SE SHOULD NOT BE CONSIDERED AN ABSOLUTE CONTRAINDICATION FOR STEM CELL COLLECTION AND TRANSPLANTATION
Transplant eligible• Good performance status• Adequate organ function
– Compensated comorbidities• No actve CHF• Patients with renal failure stable on dialysis
are appropriate candidates• No active uncontrolled infections• No acute bleeding or recent thromboembolic
events
• Socioeconomic factors– Adequate caregivers– Adequate support for transport to and
from transplant center– Ability to comply with peritransplant
follow-up care• Willing to proceed
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 54
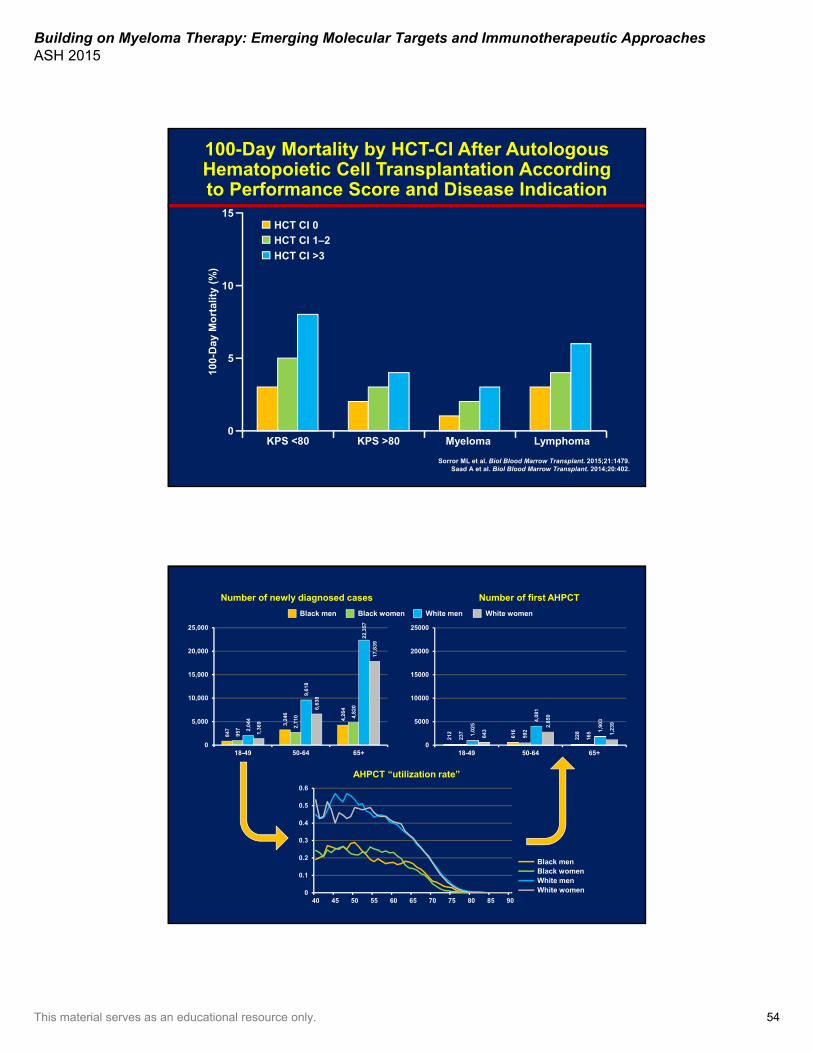
100-Day Mortality by HCT-CI After Autologous Hematopoietic Cell Transplantation According to Performance Score and Disease Indication
100-
Day
Mo
rtal
ity
(%)
0
5
10
15
KPS <80 KPS >80 Myeloma Lymphoma
HCT CI 0
HCT CI 1–2
HCT CI >3
Sorror ML et al. Biol Blood Marrow Transplant. 2015;21:1479.Saad A et al. Biol Blood Marrow Transplant. 2014;20:402.
847
3,24
6
4,26
4
957 2,
710 4,
820
2,04
4
9,61
8
22,3
57
1,36
9
6,63
8
17,8
39
0
5,000
10,000
15,000
20,000
25,000
18-49 50-64 65+
Number of newly diagnosed cases Number of first AHPCT
212
616
228
237
592
1651,02
5
4,08
1
1,90
3
643
2,85
0
1,23
9
0
5000
10000
15000
20000
25000
18-49 50-64 65+
0
0.1
0.2
0.3
0.4
0.5
0.6
40 45 50 55 60 65 70 75 80 85 90
AHPCT “utilization rate”
Black men Black women White men White women
Black menBlack womenWhite menWhite women

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 55
Case Studies Case 1• 55-year-old woman presents
with asymptomatic anemia of 10 gm/dL and total serum protein 10 gm/L
• Workup reveals– 30% plasma cells– Cytogenetic diploid– IgA kappa peak of 3.2– β2M of 3.0
• Receives 4 cycles of Bz/Thal/Dex
• Achieves stringent CR
Case 2• 55-year-old woman presents
with asymptomatic anemia of 10 gm/dL and total serum protein 10 gm/L
• Workup reveals– 30% plasma cells– Cytogenetic t(4;14)– IgA kappa peak of 3.2– β2M of 3.0
• Receives 4 cycles of Bz/Thal/Dex
• Paraprotein peak stays at 2.8 gm/dl
Timing of HCT
• What are the issues?– Early vs late– After fixed number of cycles
• 4–6, 8–10?– After a defined response
• VGPR?• Plateau?• What about the nonresponder?
• NO RANDOMIZED TRIALS BEING PERFORMED
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 56
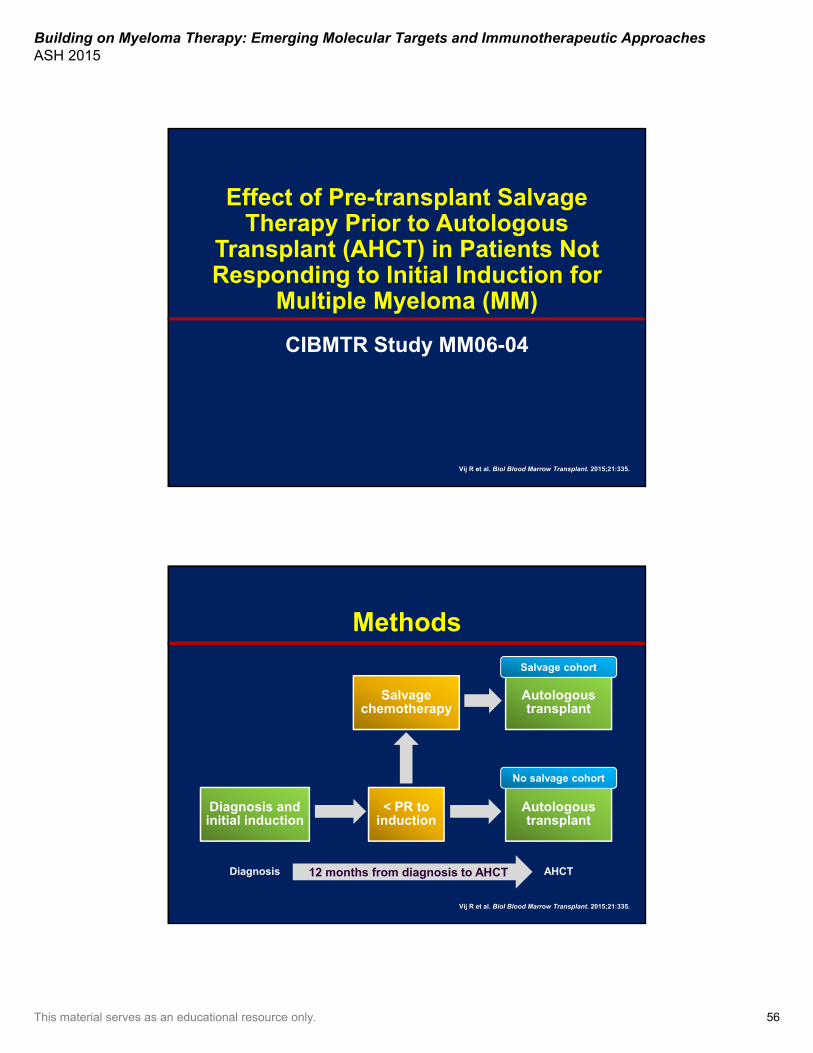
Effect of Pre-transplant Salvage Therapy Prior to Autologous
Transplant (AHCT) in Patients Not Responding to Initial Induction for
Multiple Myeloma (MM)
CIBMTR Study MM06-04
Vij R et al. Biol Blood Marrow Transplant. 2015;21:335.
Methods
< PR toinduction
Salvage chemotherapy
Autologous transplant
Diagnosis and initial induction
Autologous transplant
12 months from diagnosis to AHCT
Salvage cohort
No salvage cohort
AHCTDiagnosis
Vij R et al. Biol Blood Marrow Transplant. 2015;21:335.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 57
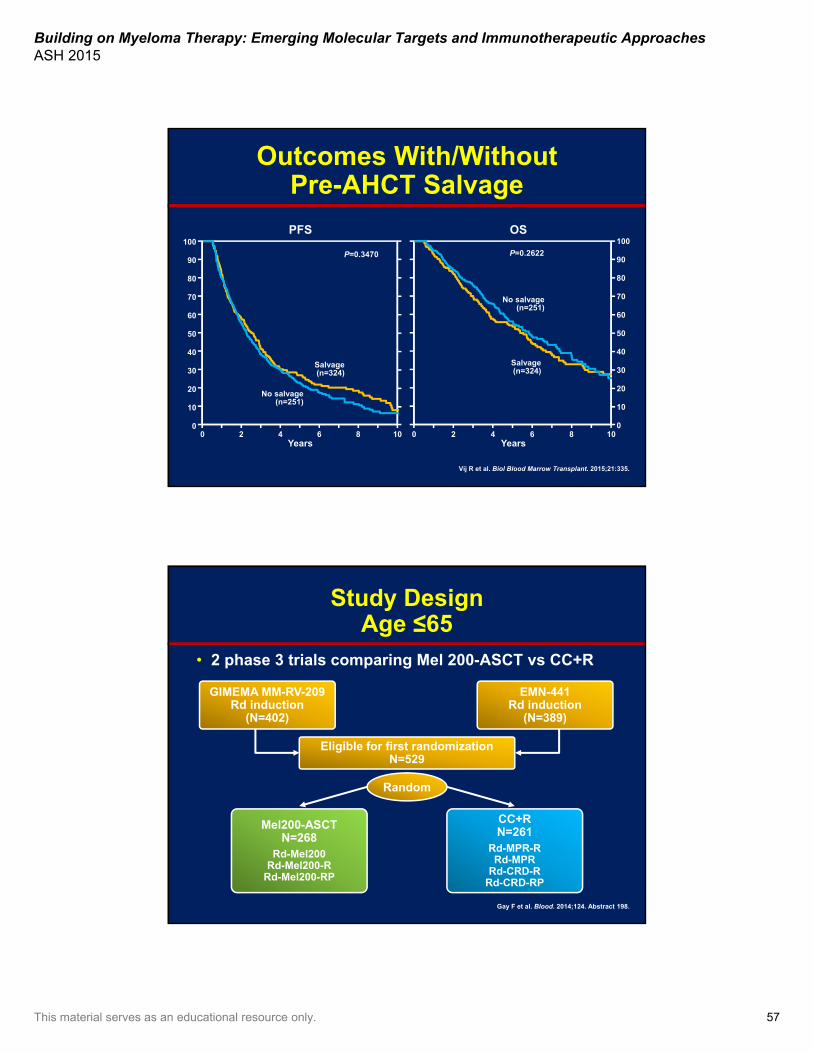
Years Years0 2 4 1086
100
0
20
40
60
80
90
10
30
50
70
No salvage(n=251)
Salvage(n=324)
PFS
0 2 4 10860
100
20
40
60
80
90
10
30
50
70
Salvage(n=324)
No salvage(n=251)
OS
P=0.3470 P=0.2622
Outcomes With/Without Pre-AHCT Salvage
Vij R et al. Biol Blood Marrow Transplant. 2015;21:335.
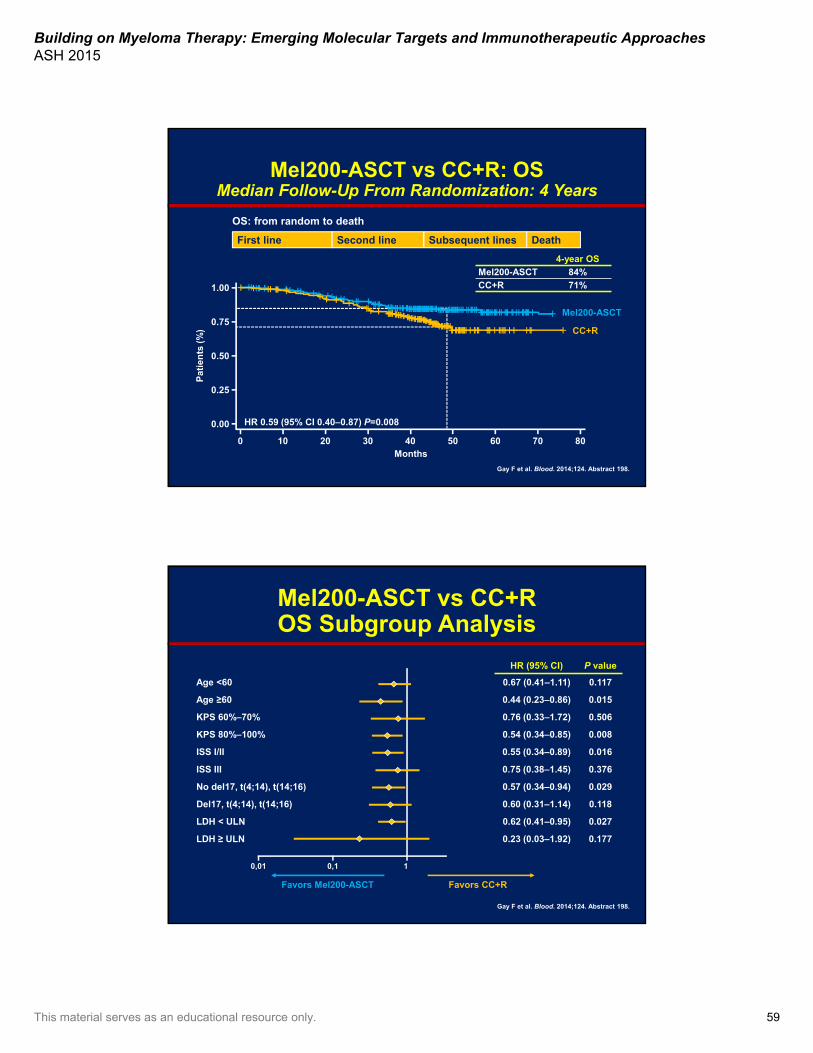
Study DesignAge ≤65
• 2 phase 3 trials comparing Mel 200-ASCT vs CC+R
Gay F et al. Blood. 2014;124. Abstract 198.
GIMEMA MM-RV-209Rd induction
(N=402)
EMN-441Rd induction
(N=389)
Eligible for first randomizationN=529
Mel200-ASCTN=268
Rd-Mel200Rd-Mel200-R
Rd-Mel200-RP
CC+RN=261
Rd-MPR-RRd-MPR
Rd-CRD-RRd-CRD-RP
Random
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 58
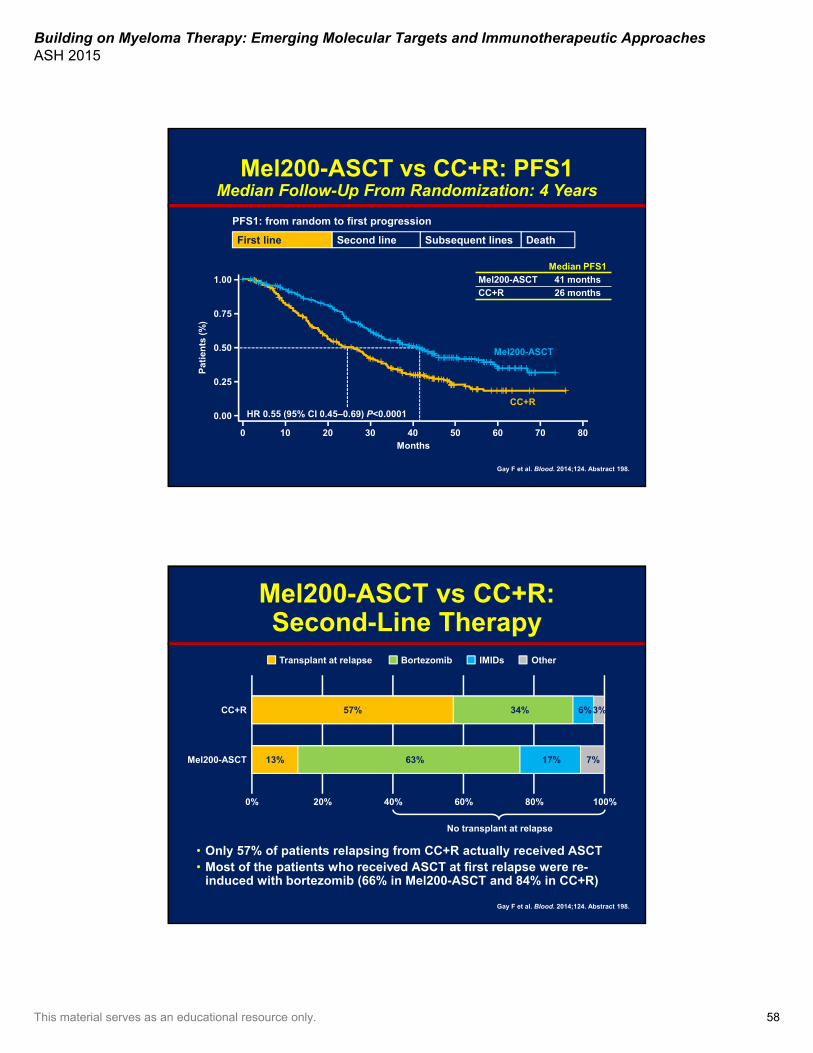
Gay F et al. Blood. 2014;124. Abstract 198.
Mel200-ASCT vs CC+R: PFS1Median Follow-Up From Randomization: 4 Years
First line Second line Subsequent lines Death
PFS1: from random to first progression
Median PFS1
Mel200-ASCT 41 months
CC+R 26 months
1.00
0.00
0.50
0.75
0.25
0 10 20 30 40 50 60 70 80Months
HR 0.55 (95% CI 0.45–0.69) P<0.0001
Mel200-ASCT
CC+R
Pat
ien
ts (
%)
Gay F et al. Blood. 2014;124. Abstract 198.
Mel200-ASCT vs CC+R:Second-Line Therapy
• Only 57% of patients relapsing from CC+R actually received ASCT• Most of the patients who received ASCT at first relapse were re-
induced with bortezomib (66% in Mel200-ASCT and 84% in CC+R)
Mel200-ASCT
CC+R
0% 20% 40% 60% 80% 100%
Transplant at relapse Bortezomib IMIDs Other
No transplant at relapse
57% 34% 6%3%
13% 63% 17% 7%
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 59
Gay F et al. Blood. 2014;124. Abstract 198.
Mel200-ASCT vs CC+R: OSMedian Follow-Up From Randomization: 4 Years
First line Second line Subsequent lines Death
OS: from random to death
4-year OS
Mel200-ASCT 84%
CC+R 71%1.00
0.00
0.50
0.75
0.25
0 10 20 30 40 50 60 70 80Months
HR 0.59 (95% CI 0.40–0.87) P=0.008
Mel200-ASCT
CC+R
Pat
ien
ts (
%)
Gay F et al. Blood. 2014;124. Abstract 198.
Mel200-ASCT vs CC+ROS Subgroup Analysis
HR (95% CI) P value
Age <60 0.67 (0.41–1.11) 0.117
Age ≥60 0.44 (0.23–0.86) 0.015
KPS 60%–70% 0.76 (0.33–1.72) 0.506
KPS 80%–100% 0.54 (0.34–0.85) 0.008
ISS I/II 0.55 (0.34–0.89) 0.016
ISS III 0.75 (0.38–1.45) 0.376
No del17, t(4;14), t(14;16) 0.57 (0.34–0.94) 0.029
Del17, t(4;14), t(14;16) 0.60 (0.31–1.14) 0.118
LDH < ULN 0.62 (0.41–0.95) 0.027
LDH ≥ ULN 0.23 (0.03–1.92) 0.177
0,01 0,1 1
Favors Mel200-ASCT Favors CC+R
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 60
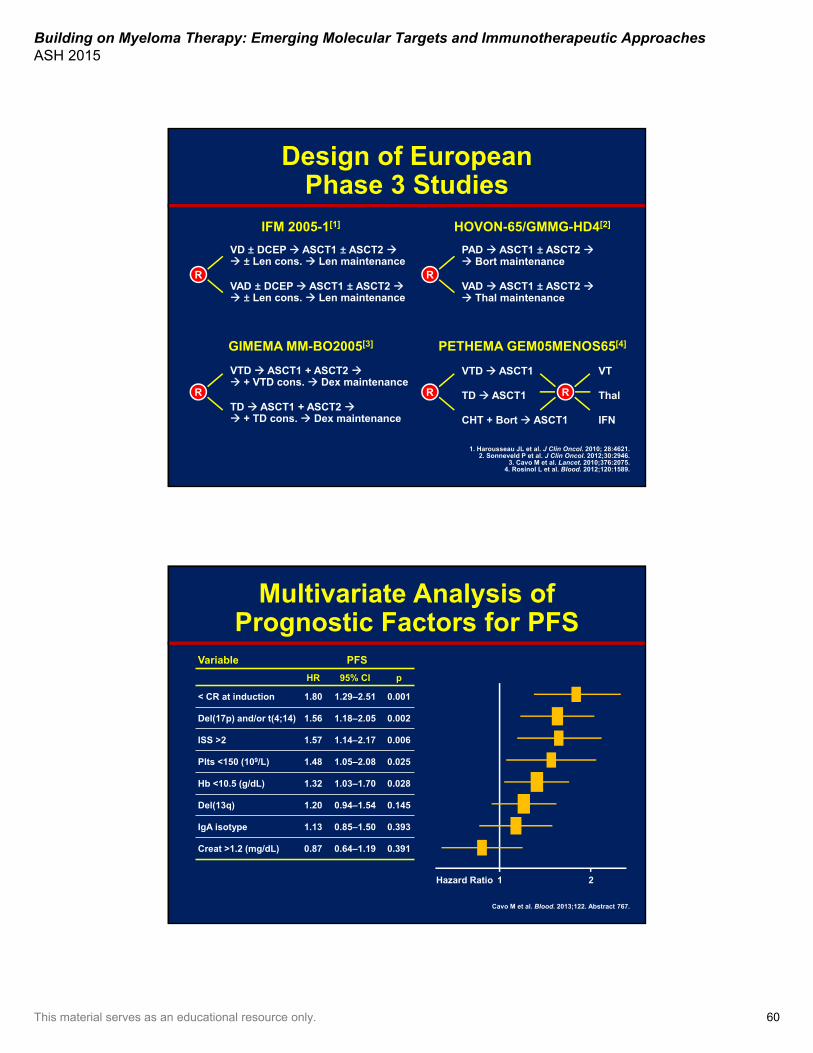
Design of EuropeanPhase 3 Studies
VD ± DCEP ASCT1 ± ASCT2 ± Len cons. Len maintenance
VAD ± DCEP ASCT1 ± ASCT2 ± Len cons. Len maintenance
IFM 2005-1[1]
R
PAD ASCT1 ± ASCT2 Bort maintenance
VAD ASCT1 ± ASCT2 Thal maintenance
HOVON-65/GMMG-HD4[2]
VTD ASCT1 + ASCT2 + VTD cons. Dex maintenance
TD ASCT1 + ASCT2 + TD cons. Dex maintenance
GIMEMA MM-BO2005[3]
VTD ASCT1
CHT + Bort ASCT1
PETHEMA GEM05MENOS65[4]
TD ASCT1 Thal
VT
IFN
1. Harousseau JL et al. J Clin Oncol. 2010; 28:4621.2. Sonneveld P et al. J Clin Oncol. 2012;30:2946.
3. Cavo M et al. Lancet. 2010;376:2075.4. Rosinol L et al. Blood. 2012;120:1589.
R
R R R
Multivariate Analysis of Prognostic Factors for PFS
Variable PFS
HR 95% CI p
< CR at induction 1.80 1.29–2.51 0.001
Del(17p) and/or t(4;14) 1.56 1.18–2.05 0.002
ISS >2 1.57 1.14–2.17 0.006
Plts <150 (109/L) 1.48 1.05–2.08 0.025
Hb <10.5 (g/dL) 1.32 1.03–1.70 0.028
Del(13q) 1.20 0.94–1.54 0.145
IgA isotype 1.13 0.85–1.50 0.393
Creat >1.2 (mg/dL) 0.87 0.64–1.19 0.391
1 2Hazard Ratio
Cavo M et al. Blood. 2013;122. Abstract 767.

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 61
Score System Definition(Assessable Pts = 606)
Score Group
Prognostic variables
ISSCytogenetic
AbnormalitiesResponse at
Induction # of Pts (%)
0 1–2 Del(17p) – t(4;14)- CR 77 (12.71%)
1 Presence of a single adverse variable 369 (60.88%)
1–2 Del(17p) – t(4;14)- < CR 330 (54.45%)
1–2 Del(17p) ± t(4;14) CR 22 (3.63%)
3 Del(17p) – t(4;14)- CR 17 (2.80%)
2 Presence of 2 out of 3 adverse variables 141 (23.27%)
1–2 Del(17p) ± t(4;14) < CR 70 (11.55%)
3 Del(17p) – t(4;14)- < CR 65 (10.73%)
3 Del(17p) ± t(4;14) CR 6 (0.99%)
3 3 Del(17p) ± t(4;14) < CR 19 (3.14%)
Cavo M et al. Blood. 2013;122. Abstract 767.
PFS According to Score Groups
Log-rank test: score 0 vs 1 P=0.0546
P<0.0001 score 1 vs 2 P<0.0001
trend P<0.0001 score 2 vs 3 P=0.0103
1.00
0.75
0.00
0.25
0.50
Months0
Kaplan-Meier survival estimates
12 24 36 48 60
61 mo
score 0
score 1
score 2
score 3
56 mo36 mo26 mo
Cavo M et al. Blood. 2013;122. Abstract 767.

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 62
What is the role of consolidation?
PFS According to Preplanned Number of ASCT(s)
Log-rank test: HR 0.72 (0.60–0.87)
P=0.0005 P<0.001
50 mo2 ASCT
38 mo
1 ASCT
Cavo M et al. Blood. 2013;122. Abstract 767.
Kaplan-Meier survival estimates1.00
0.75
0.00
0.25
0.50
Months0 12 24 36 48 60
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 63
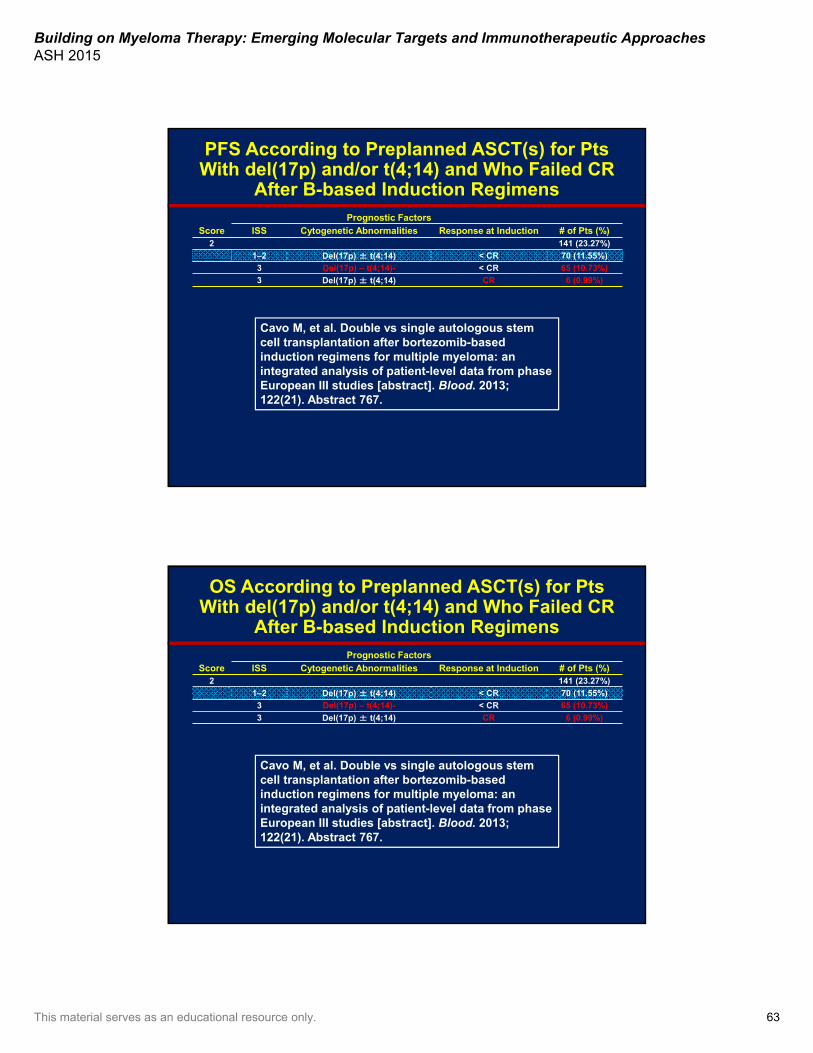
PFS According to Preplanned ASCT(s) for Pts With del(17p) and/or t(4;14) and Who Failed CR
After B-based Induction Regimens
Score
Prognostic Factors
ISS Cytogenetic Abnormalities Response at Induction # of Pts (%)2 141 (23.27%)
1–2 Del(17p) ± t(4;14) < CR 70 (11.55%)
3 Del(17p) – t(4;14)- < CR 65 (10.73%)
3 Del(17p) ± t(4;14) CR 6 (0.99%)
Cavo M, et al. Double vs single autologous stemcell transplantation after bortezomib-basedinduction regimens for multiple myeloma: anintegrated analysis of patient-level data from phaseEuropean III studies [abstract]. Blood. 2013;122(21). Abstract 767.
OS According to Preplanned ASCT(s) for Pts With del(17p) and/or t(4;14) and Who Failed CR
After B-based Induction Regimens
Score
Prognostic Factors
ISS Cytogenetic Abnormalities Response at Induction # of Pts (%)2 141 (23.27%)
1–2 Del(17p) ± t(4;14) < CR 70 (11.55%)
3 Del(17p) – t(4;14)- < CR 65 (10.73%)
3 Del(17p) ± t(4;14) CR 6 (0.99%)
Cavo M, et al. Double vs single autologous stemcell transplantation after bortezomib-basedinduction regimens for multiple myeloma: anintegrated analysis of patient-level data from phaseEuropean III studies [abstract]. Blood. 2013;122(21). Abstract 767.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 64
Lenalidomide maintenance†
Lenalidomide maintenance†
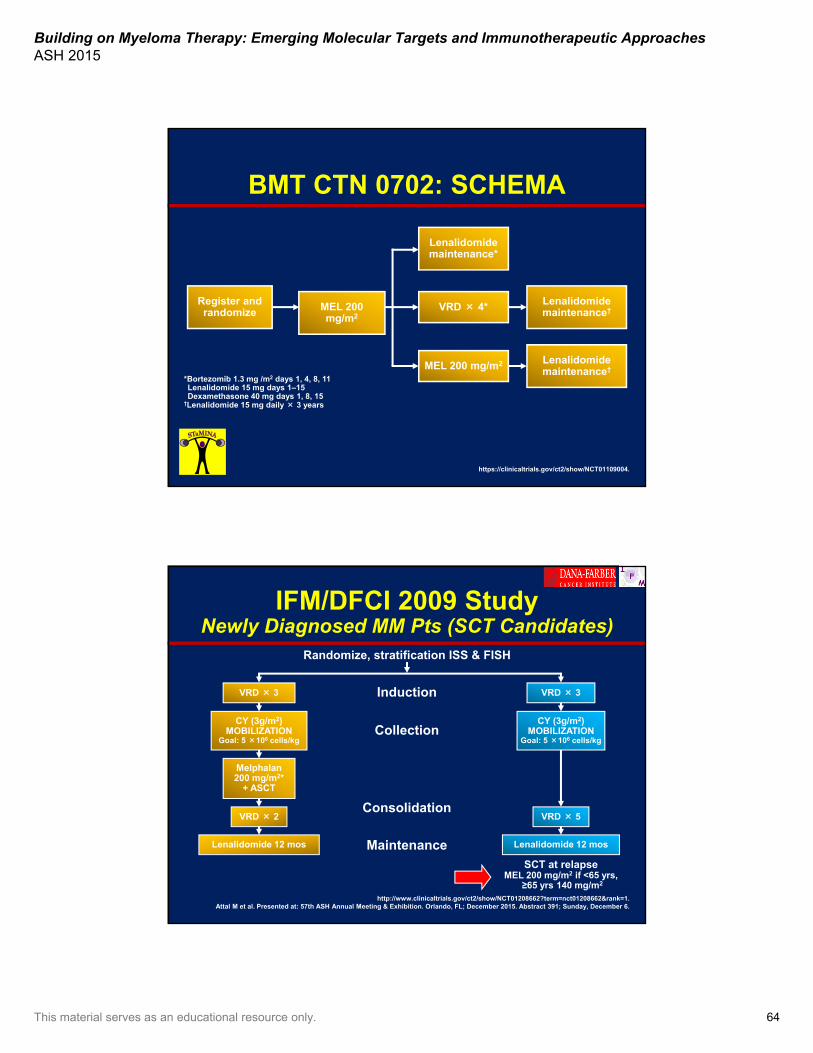
BMT CTN 0702: SCHEMA
Register and randomize MEL 200
mg/m2VRD × 4*
Lenalidomide maintenance*
MEL 200 mg/m2
*Bortezomib 1.3 mg /m2 days 1, 4, 8, 11 Lenalidomide 15 mg days 1–15 Dexamethasone 40 mg days 1, 8, 15
†Lenalidomide 15 mg daily × 3 years
https://clinicaltrials.gov/ct2/show/NCT01109004.
IFM/DFCI 2009 StudyNewly Diagnosed MM Pts (SCT Candidates)
VRD × 3
VRD × 2 VRD × 5
Lenalidomide 12 mos
Melphalan200 mg/m2*
+ ASCT
Induction
Consolidation
Maintenance
CY (3g/m2) MOBILIZATION
Goal: 5 ×106 cells/kg
VRD × 3
CY (3g/m2)MOBILIZATION
Goal: 5 ×106 cells/kg
Randomize, stratification ISS & FISH
Collection
Lenalidomide 12 mos
SCT at relapse MEL 200 mg/m2 if <65 yrs,
≥65 yrs 140 mg/m2
http://www.clinicaltrials.gov/ct2/show/NCT01208662?term=nct01208662&rank=1.Attal M et al. Presented at: 57th ASH Annual Meeting & Exhibition. Orlando, FL; December 2015. Abstract 391; Sunday, December 6.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 65
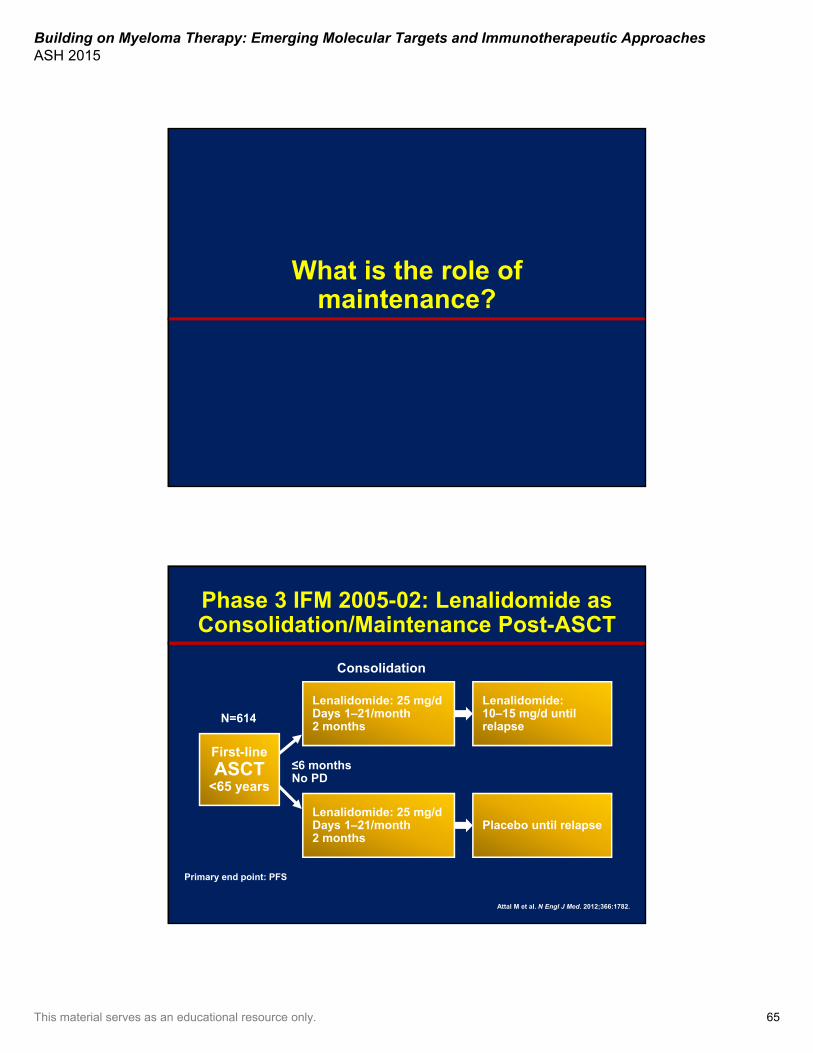
What is the role of maintenance?
Lenalidomide: 10–15 mg/d until relapse
Placebo until relapse
First-line
ASCT<65 years
Lenalidomide: 25 mg/d Days 1–21/month2 months
Primary end point: PFS
≤6 monthsNo PD
N=614
Lenalidomide: 25 mg/d Days 1–21/month2 months
Consolidation
Phase 3 IFM 2005-02: Lenalidomide as Consolidation/Maintenance Post-ASCT
Attal M et al. N Engl J Med. 2012;366:1782.

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 66
HR 0.37 (CI 95% 0.25–0.58) HR 0.54 (CI 95% 0.37–0.78)
Phase 3 IFM 2005-02: PFS According to Response Preconsolidation
Attal M et al. Blood. 2009;114. Abstract 529.Attal M et al. J Clin Oncol. 2010;28. Abstract 8018.
Attal M et al. N Engl J Med. 2012;366:1782.
LEN PLA
PR or SD VGPR or CR
P<10-5 P=0.0010.00
0.25
0.50
0.75
1.00
0 6 12 18 24 30 36
LEN PLA
0.00
0.25
0.50
0.75
1.00
0 6 12 18 24 30 36
Stage 1–3, <70 yearsTherapy at least 2 cycles Stable disease or better≤1 year from Rx initiation2 × 106 CD34 cells/kg
Placebo
Lenalidomide10 mg/d with ↑↓ (5–15 mg)
RestagingDays 90–100
Registration
CRPRSD
Stratification based on diagnostic β2M andIMiD use during induction
Mel 200
ASCT
CALGB 100104 Schema
McCarthy PL et al. N Engl J Med. 2012;366:1770.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 67
CALGB 100104
Figure S2e, supplement to:
McCarthy PL, et al. Lenalidomide after stem-cell transplantation for multiple myeloma. N Engl J Med. 2012 May 10;366(19):1770-1781.
Figure 2A & 2B, page 1776
McCarthy PL, et al. Lenalidomide after stem-cell transplantation for multiple myeloma. N Engl J Med. 2012 May 10;366(19):1770-1781.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 68
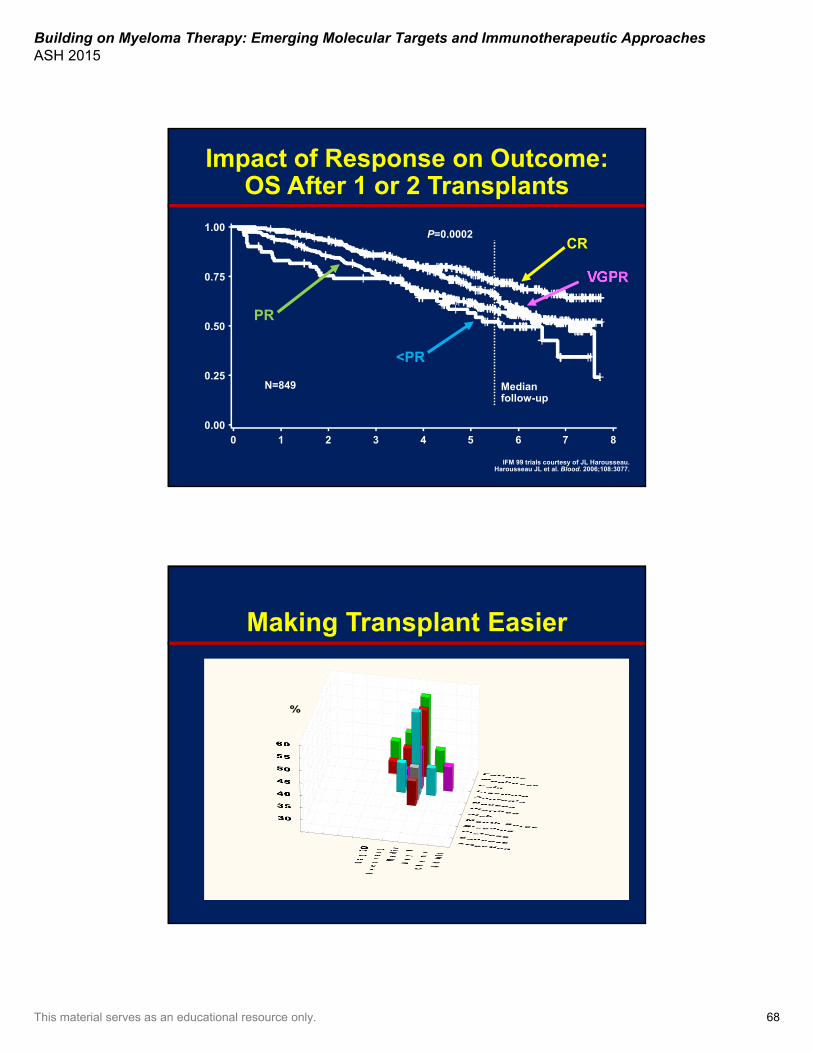
Impact of Response on Outcome: OS After 1 or 2 Transplants
IFM 99 trials courtesy of JL Harousseau.Harousseau JL et al. Blood. 2006;108:3077.
VGPR
N=849
P=0.0002CR
PR
<PR
0 1 2 3 4 5 6 7 80.00
0.25
0.50
0.75
1.00
Median follow-up
Making Transplant Easier
%

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 69
Symptoms, Toxicities, and Cytokines
Wang XS et al. Cancer. 2008;113:2102.
0
6
10
2
Glo
bal
Mea
n S
ymp
tom
Sev
erit
y
8
4
1.1 1.2 1.3 1.4 1.5 1.6 1.7Global Mean (log) Cytokine
0
6
7
2
5
4
1
3
Mea
n M
DA
SI
Sev
erit
y
0
1.5
2
1
0.5
IL-6
(lo
g)IL-6
Symptoms
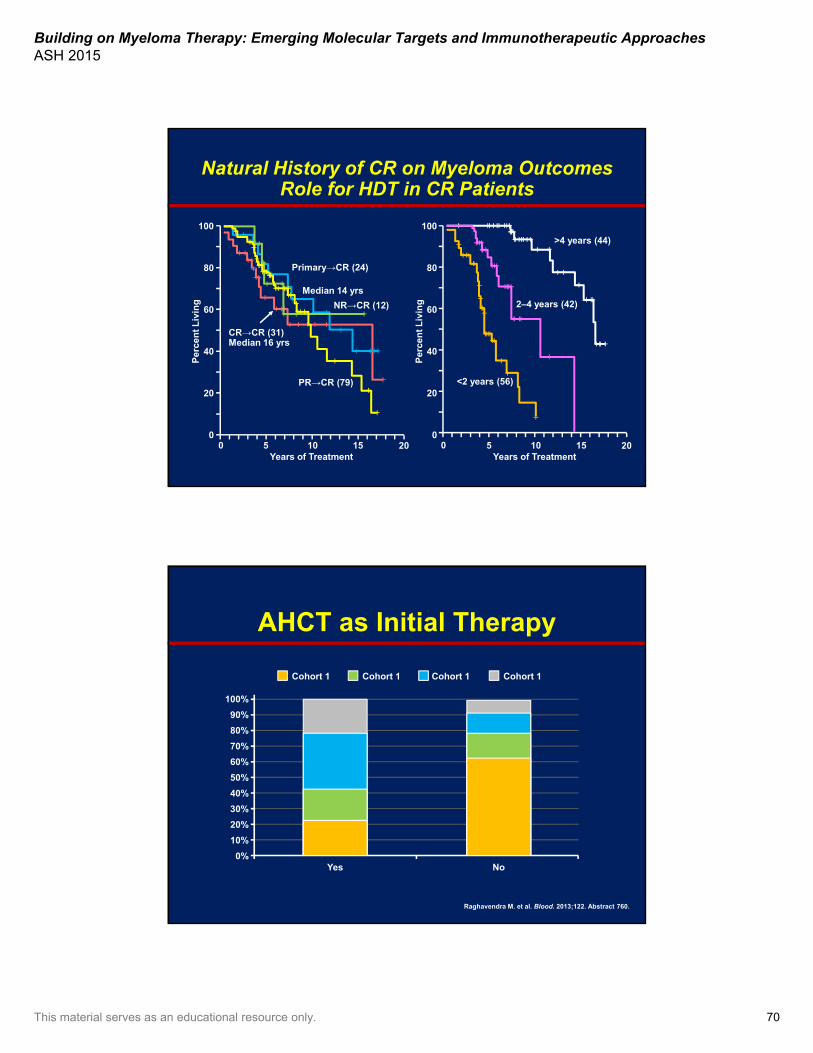
Does high-dose therapy and transplant cure myeloma?
Long-term disease control is possible, and some patients may never have to
deal with their disease again…Are they cured?
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 70
>4 years (44)
<2 years (56)
2–4 years (42)NR→CR (12)
CR→CR (31)Median 16 yrs
PR→CR (79)
Primary→CR (24)
Natural History of CR on Myeloma OutcomesRole for HDT in CR Patients
Years of Treatment
20
40
60
80
100
5 10 15
Per
cen
t L
ivin
g
0
Years of Treatment
20
40
60
80
100
5 10 15
Per
cen
t L
ivin
g
0200200
Median 14 yrs
AHCT as Initial Therapy
Raghavendra M. et al. Blood. 2013;122. Abstract 760.
0%
40%
20%
80%
100%
60%
10%
50%
30%
90%
70%
Yes No
Cohort 1 Cohort 1 Cohort 1 Cohort 1
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 71
CR Definition Does Matter With Regards to Depth of Remission
Figure 1
Poon ML, Chng WJ. Is complete remission an important therapeutic aim in multiple myeloma? Cancer Ther. 2008;6:275-284.
In My Humble Opinion• High-dose melphalan is one of the most active agents in
myeloma today– 30%–40% CR– 24 months median remission duration without maintenance– Name another agent with similar single-agent activity– It is also cost-effective
• With stem cell support it can be given safely to older patients with comorbidities
• Thus, not planning for its use up front is similar to telling a patient, “I am never going to use bortezomib or lenalidomide during your disease course because I don’t like it or I don’t believe in it”
• Early or late or once, twice, or more times, it remains an active agent that can be extremely effective in all stages of the patient’s disease journey
• Continued exploration in clinical trials is essential
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 72
Updates on Options for Relapsed/Refractory Disease
Saad Usmani, MD, FACPDirector, Plasma Cell Disorders Program
Director, Clinical Research in Hematologic MalignanciesDepartment of Hematologic Oncology & Blood Disorders
Levine Cancer InstituteCharlotte, North Carolina
Outline
• Practical considerations in choosing therapy for relapsed and/or refractory MM
• New options for relapsed MM (1–3 prior therapies)
• Role of transplant in relapsed and/or refractory MM

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 73
When to Consider Retreatment in Relapsed/Refractory MM
• Nature of relapse/progression– Slow/biochemical vs rapid/high burden– Renal failure, sPCL, EMD, bone fractures, cytogenetic
abnormalities
• Host factors– Age, comorbidities, performance status, organ failure
• Prior therapies/treatment-related factors– Tolerability, dose reductions, adverse events (AEs)/serious
adverse events (SAEs)– Duration of therapy and durability of previous response
• Socioeconomic aspects– Insurance issues, access to care, adequate social support
• Availability of clinical trials
Treatment Approaches in Relapsed/Refractory MM
Figure 1, page S72
Usmani SZ, Lonial S. Novel drug combinations for the management of relapsed/refractory multiple myeloma. Clin Lymphoma Myeloma Leuk. 2014 Sep;14 Suppl:S71-S77.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 74
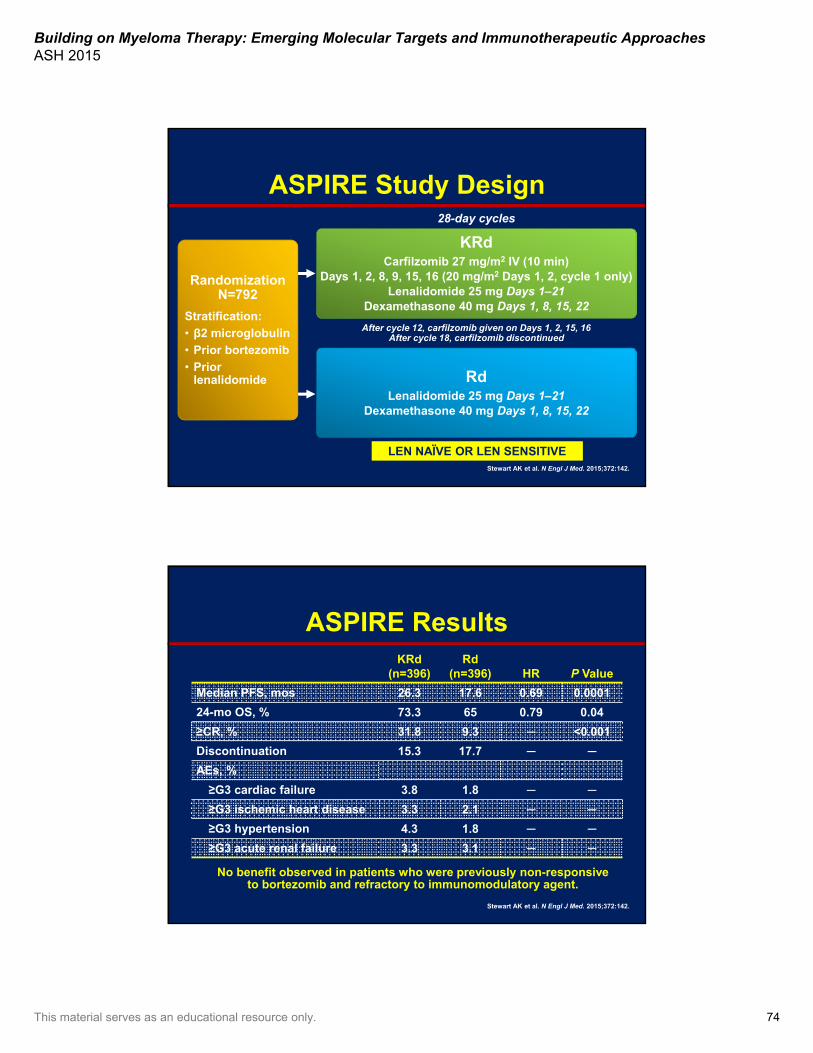
KRdCarfilzomib 27 mg/m2 IV (10 min)
Days 1, 2, 8, 9, 15, 16 (20 mg/m2 Days 1, 2, cycle 1 only) Lenalidomide 25 mg Days 1–21
Dexamethasone 40 mg Days 1, 8, 15, 22
RdLenalidomide 25 mg Days 1–21
Dexamethasone 40 mg Days 1, 8, 15, 22
ASPIRE Study Design
After cycle 12, carfilzomib given on Days 1, 2, 15, 16After cycle 18, carfilzomib discontinued
28-day cycles
Stewart AK et al. N Engl J Med. 2015;372:142.
Randomization N=792
Stratification:
• β2 microglobulin
• Prior bortezomib
• Prior lenalidomide
LEN NAÏVE OR LEN SENSITIVE
ASPIRE ResultsKRd
(n=396)Rd
(n=396) HR P Value
Median PFS, mos 26.3 17.6 0.69 0.0001
24-mo OS, % 73.3 65 0.79 0.04
≥CR, % 31.8 9.3 ─ <0.001
Discontinuation 15.3 17.7 ─ ─
AEs, %
≥G3 cardiac failure 3.8 1.8 ─ ─
≥G3 ischemic heart disease 3.3 2.1 ─ ─
≥G3 hypertension 4.3 1.8 ─ ─
≥G3 acute renal failure 3.3 3.1 ─ ─
Stewart AK et al. N Engl J Med. 2015;372:142.
No benefit observed in patients who were previously non-responsive to bortezomib and refractory to immunomodulatory agent.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 75
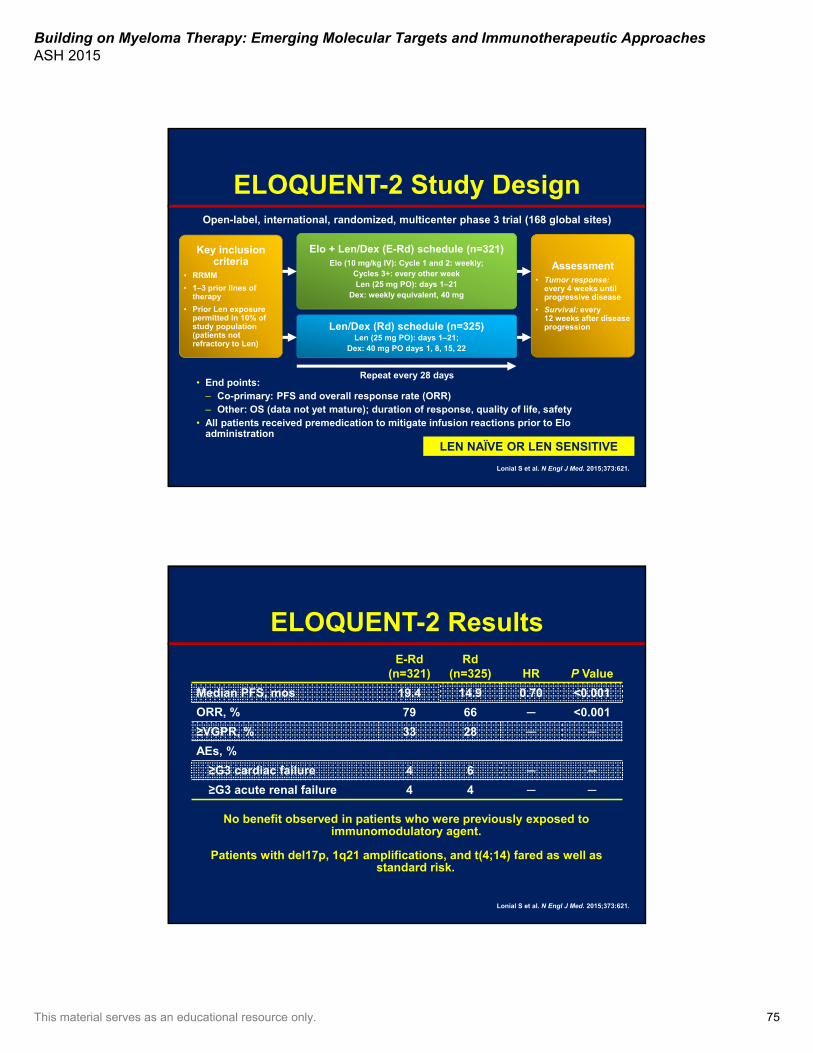
ELOQUENT-2 Study Design Open-label, international, randomized, multicenter phase 3 trial (168 global sites)
Lonial S et al. N Engl J Med. 2015;373:621.
LEN NAÏVE OR LEN SENSITIVE
Elo + Len/Dex (E-Rd) schedule (n=321)Elo (10 mg/kg IV): Cycle 1 and 2: weekly;
Cycles 3+: every other weekLen (25 mg PO): days 1–21
Dex: weekly equivalent, 40 mg
Len/Dex (Rd) schedule (n=325)Len (25 mg PO): days 1–21;
Dex: 40 mg PO days 1, 8, 15, 22
Key inclusion criteria
• RRMM
• 1–3 prior lines of therapy
• Prior Len exposure permitted in 10% of study population (patients not refractory to Len)
Assessment• Tumor response:
every 4 weeks until progressive disease
• Survival: every 12 weeks after disease progression
• End points:– Co-primary: PFS and overall response rate (ORR)– Other: OS (data not yet mature); duration of response, quality of life, safety
• All patients received premedication to mitigate infusion reactions prior to Eloadministration
Repeat every 28 days
ELOQUENT-2 ResultsE-Rd
(n=321)Rd
(n=325) HR P Value
Median PFS, mos 19.4 14.9 0.70 <0.001
ORR, % 79 66 ─ <0.001
≥VGPR, % 33 28 ─ ─
AEs, %
≥G3 cardiac failure 4 6 ─ ─
≥G3 acute renal failure 4 4 ─ ─
Lonial S et al. N Engl J Med. 2015;373:621.
Patients with del17p, 1q21 amplifications, and t(4;14) fared as well as standard risk.
No benefit observed in patients who were previously exposed to immunomodulatory agent.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 76
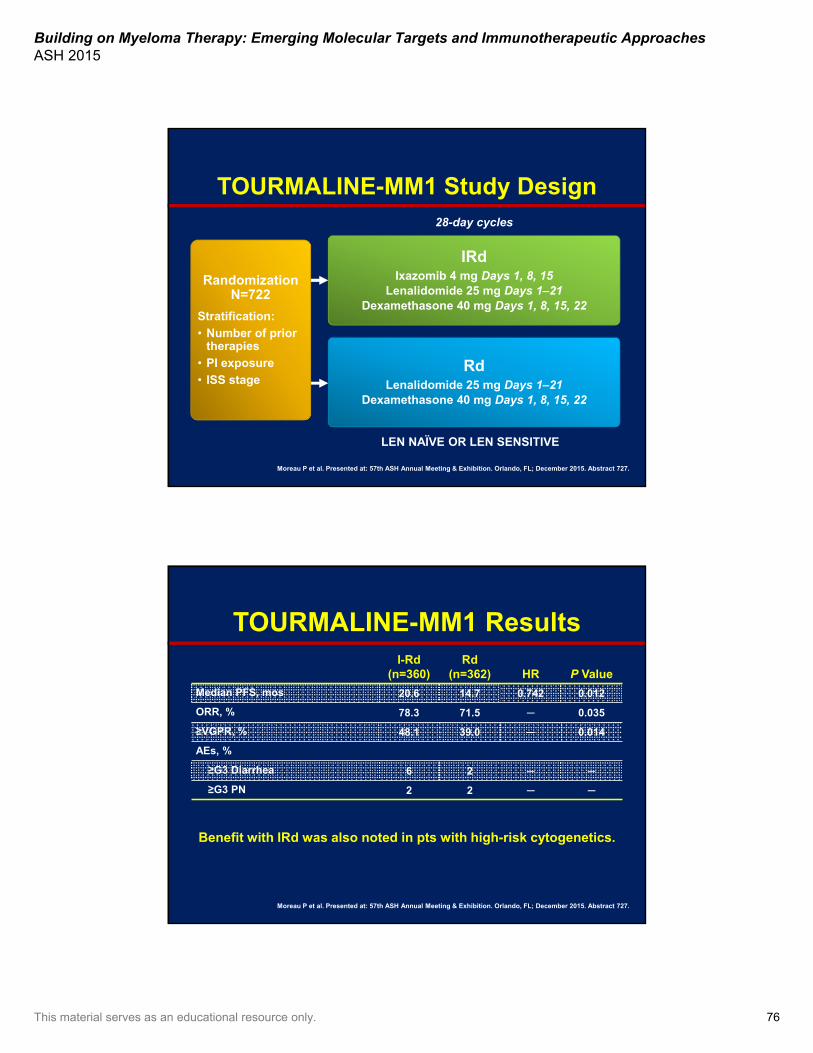
TOURMALINE-MM1 Study Design
Moreau P et al. Presented at: 57th ASH Annual Meeting & Exhibition. Orlando, FL; December 2015. Abstract 727.
IRdIxazomib 4 mg Days 1, 8, 15
Lenalidomide 25 mg Days 1–21Dexamethasone 40 mg Days 1, 8, 15, 22
RdLenalidomide 25 mg Days 1–21
Dexamethasone 40 mg Days 1, 8, 15, 22
28-day cycles
LEN NAÏVE OR LEN SENSITIVE
Randomization N=722
Stratification:
• Number of prior therapies
• PI exposure
• ISS stage
TOURMALINE-MM1 ResultsI-Rd
(n=360)Rd
(n=362) HR P Value
Median PFS, mos 20.6 14.7 0.742 0.012
ORR, % 78.3 71.5 ─ 0.035
≥VGPR, % 48.1 39.0 ─ 0.014
AEs, %
≥G3 Diarrhea 6 2 ─ ─
≥G3 PN 2 2 ─ ─
Benefit with IRd was also noted in pts with high-risk cytogenetics.
Moreau P et al. Presented at: 57th ASH Annual Meeting & Exhibition. Orlando, FL; December 2015. Abstract 727.

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 77
ENDEAVOR Study Design
Dimopoulos MA et al. J Clin Oncol. 2015;33. Abstract 8509.
KdCarfilzomib 56 mg/m2 IV
Days 1, 2, 8, 9, 15, 16 (20 mg/m2 Days 1, 2, cycle 1 only)Infusion duration: 30 minutes for all doses
Dexamethasone 20 mg Days 1, 2, 8, 9, 15, 16, 22, 23
28-day cycles until disease progression or unacceptable toxicity
VdBortezomib 1.3 mg/m2 (3–5 second IV bolus
or subcutaneous injection)Days 1, 4, 8, 11
Dexamethasone 20 mg Days 1, 2, 4, 5, 8, 9, 11, 12
21-day cycles until disease progression or unacceptable toxicity
BOR NAÏVE OR BOR SENSITIVE
Randomization 1:1 N=929
Stratification:
• Prior proteasome inhibitor therapy
• Prior lines of treatment
• ISS stage
• Route of administration
ISS, International Staging System
ENDEAVOR ResultsKd
(n=464)Vd
(n=465) HR P Value
Median PFS, mos 18.7 9.4 0.53 <0.0001
≥CR, % 12.5 6.2 ─ ─
≥VGPR, % 54.3 28.6 ─ ─
Discontinuation 14.0 15.7 ─ ─
AEs, %
≥G3 Hypertension 8.9 2.6 ─ ─
≥G3 Dyspnea 5.6 2.2 ─ ─
≥G3 Cardiac failure 4.8 1.8 ─ ─
≥G3 Acute renal failure 4.1 2.6 ─ ─
≥G2 PN 6.3 32.0 ─ <0.0001
Dimopoulos MA et al. J Clin Oncol. 2015;33. Abstract 8509.
No benefit observed in patients refractory to lenalidomide

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 78
Pano-VdPanobinostat 20 mg Days 1, 3, 5, 8, 10, 12
Bortezomib 1.3 mg/m2 Days 1, 4, 8, 11Dexamethasone 20 mg Days 1, 2, 4, 5, 8, 9, 11, 12
VdBortezomib 1.3 mg/m2mg Days 1, 4, 8, 11
Dexamethasone 20 mg Days 1, 2, 4, 5, 8, 9, 11, 12
RandomizationN=768
Stratification:
• Number of previous treatment lines
• Prior bortezomib
PANORAMA1 Study Design21-day cycles
San Miguel JF et al. Lancet Oncol. 2014;15:1195.
LEN AND BZ EXPOSED
PANORAMA1 ResultsPano-Vd(n=387)
Vd(n=381) HR P Value
Median PFS, mos 12 8.1 0.63 <0.0001
ORR, % 60.7 54.6 ─ 0.09
≥nCR, % 27.6 15.7 ─ <0.001
IMiD + bortezomib, mos 10.6 5.8 -- --
IMiD + bortezomib + ≥2 prior lines, mos
12.5 4.7 -- --
AEs, %
≥G3 Diarrhea 25 7 ─ ─
≥G3 Asthenia 24 12 ─ ─
≥G3 PN 17 15 ─ ─
San Miguel JF et al. Lancet Oncol. 2014;15:1195.
Benefit less pronounced in women and patients > 65 years BUT more evident in patients who with previous exposure to bortezomib and immunomodulatory agent.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 79
Treatment Approaches in Relapsed/Refractory MM
Figure 1, page S72
Usmani SZ, Lonial S. Novel drug combinations for the management of relapsed/refractory multiple myeloma. Clin Lymphoma Myeloma Leuk. 2014 Sep;14 Suppl:S71-S77.
Treatment Approaches in Relapsed/Refractory MM
Figure 1, page S72
Usmani SZ, Lonial S. Novel drug combinations for the management of relapsed/refractory multiple myeloma. Clin Lymphoma Myeloma Leuk. 2014 Sep;14 Suppl:S71-S77.
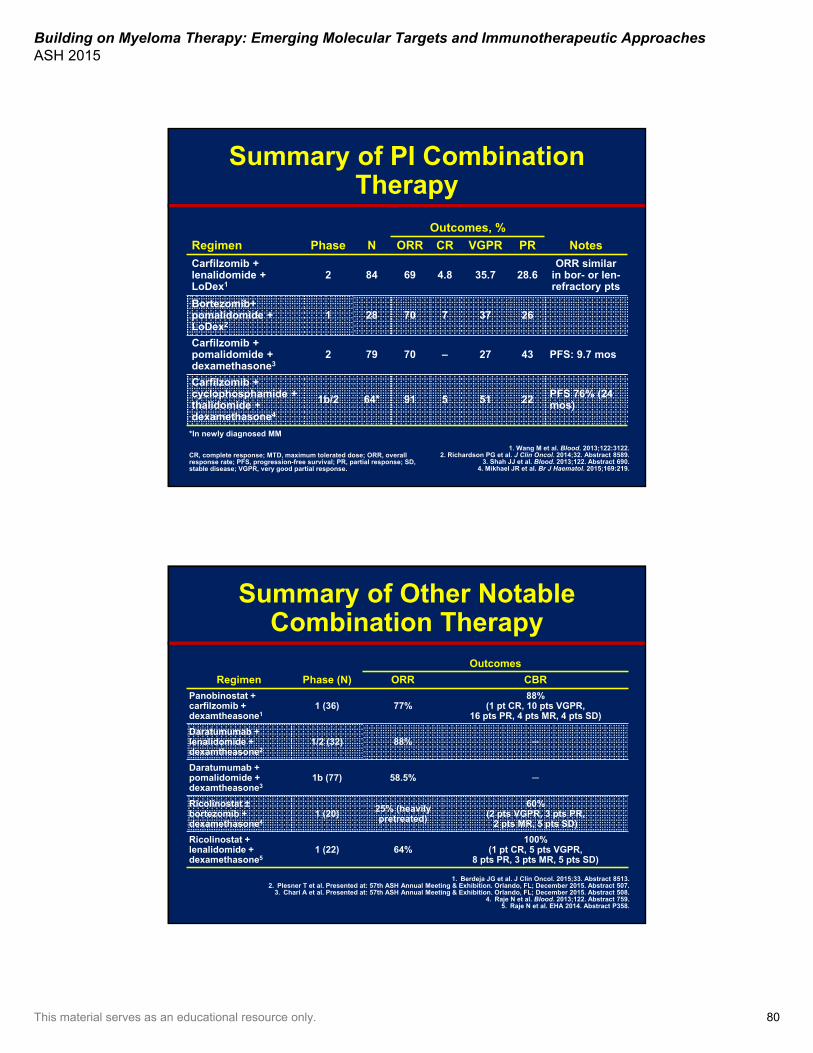
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 80
Summary of PI Combination Therapy
Regimen Phase N
Outcomes, %
NotesORR CR VGPR PR
Carfilzomib + lenalidomide + LoDex1
2 84 69 4.8 35.7 28.6ORR similar
in bor- or len-refractory pts
Bortezomib+ pomalidomide + LoDex2
1 28 70 7 37 26
Carfilzomib + pomalidomide + dexamethasone3
2 79 70 – 27 43 PFS: 9.7 mos
Carfilzomib + cyclophosphamide + thalidomide + dexamethasone4
1b/2 64* 91 5 51 22 PFS 76% (24 mos)
1. Wang M et al. Blood. 2013;122:3122. 2. Richardson PG et al. J Clin Oncol. 2014;32. Abstract 8589.
3. Shah JJ et al. Blood. 2013;122. Abstract 690.4. Mikhael JR et al. Br J Haematol. 2015;169:219.
CR, complete response; MTD, maximum tolerated dose; ORR, overall response rate; PFS, progression-free survival; PR, partial response; SD, stable disease; VGPR, very good partial response.
*In newly diagnosed MM
1. Berdeja JG et al. J Clin Oncol. 2015;33. Abstract 8513. 2. Plesner T et al. Presented at: 57th ASH Annual Meeting & Exhibition. Orlando, FL; December 2015. Abstract 507.
3. Chari A et al. Presented at: 57th ASH Annual Meeting & Exhibition. Orlando, FL; December 2015. Abstract 508.4. Raje N et al. Blood. 2013;122. Abstract 759.
5. Raje N et al. EHA 2014. Abstract P358.
Summary of Other Notable Combination Therapy
Regimen Phase (N)
Outcomes
ORR CBR
Panobinostat + carfilzomib + dexamtheasone1
1 (36) 77%88%
(1 pt CR, 10 pts VGPR, 16 pts PR, 4 pts MR, 4 pts SD)
Daratumumab + lenalidomide + dexamtheasone2
1/2 (32) 88% ─
Daratumumab + pomalidomide + dexamtheasone3
1b (77) 58.5% ─
Ricolinostat ±bortezomib + dexamethasone4
1 (20) 25% (heavily pretreated)
60% (2 pts VGPR, 3 pts PR,
2 pts MR, 5 pts SD)
Ricolinostat + lenalidomide + dexamethasone5
1 (22) 64%100%
(1 pt CR, 5 pts VGPR, 8 pts PR, 3 pts MR, 5 pts SD)
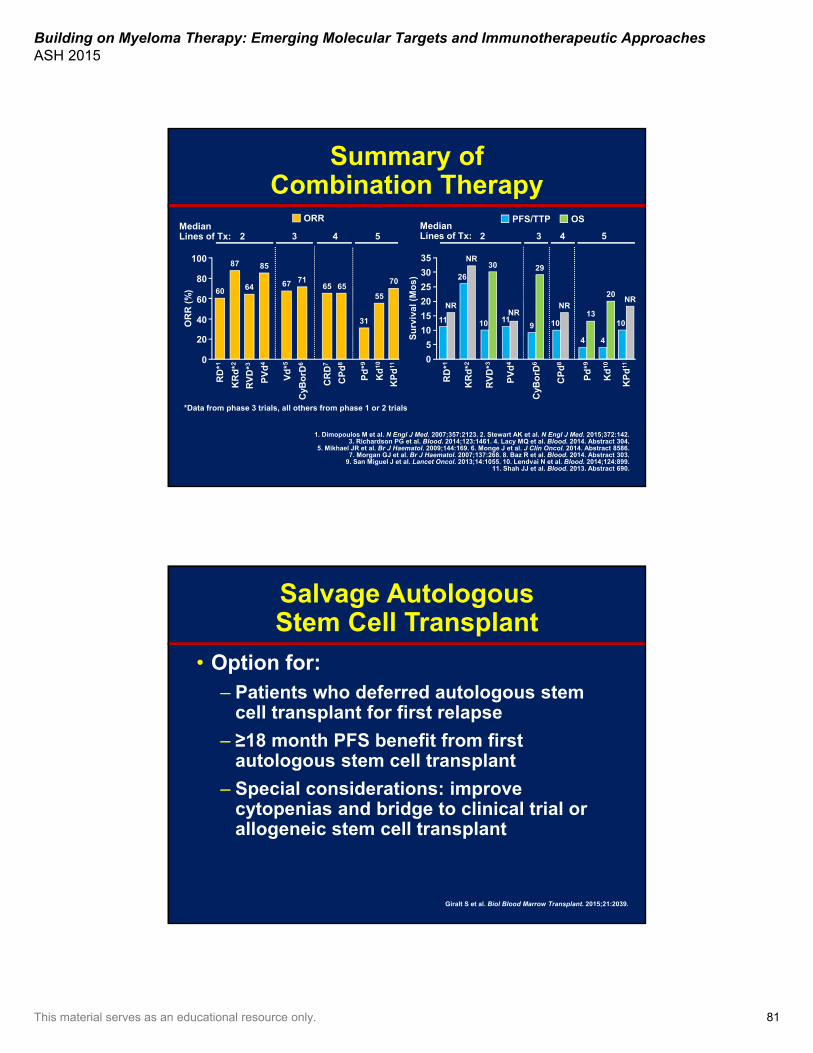
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 81
100
2 4 53
80
60
40
20
0
Summary of Combination Therapy
Median Lines of Tx:
1. Dimopoulos M et al. N Engl J Med. 2007;357:2123. 2. Stewart AK et al. N Engl J Med. 2015;372:142. 3. Richardson PG et al. Blood. 2014;123:1461. 4. Lacy MQ et al. Blood. 2014. Abstract 304.
5. Mikhael JR et al. Br J Haematol. 2009;144:169. 6. Monge J et al. J Clin Oncol. 2014. Abstract 8586. 7. Morgan GJ et al. Br J Haematol. 2007;137:268. 8. Baz R et al. Blood. 2014. Abstract 303.
9. San Miguel J et al. Lancet Oncol. 2013;14:1055. 10. Lendvai N et al. Blood. 2014;124:899. 11. Shah JJ et al. Blood. 2013. Abstract 690.
RD
*1
CR
D7
Pd
*9
CP
d8
Kd
10
KR
d*2
KP
d11
Vd
*5
RV
D*3
PV
d4
CyB
orD
6
RD
*1
Pd
*9
CP
d8
Kd
10
KR
d*2
KP
d11
RV
D*3
PV
d4
CyB
orD
6
OR
R (
%)
Su
rviv
al (
Mo
s)*Data from phase 3 trials, all others from phase 1 or 2 trials
6065
31
6555
87
706764
85
71
35
30
25
20
15
10
5
0
11
NR
4
1310
NR
4
20
NR
26
10
NR
30
10
29
911
NR
2 3 4 5Median Lines of Tx:
ORR OSPFS/TTP
Salvage Autologous Stem Cell Transplant
• Option for:– Patients who deferred autologous stem
cell transplant for first relapse
– ≥18 month PFS benefit from first autologous stem cell transplant
– Special considerations: improve cytopenias and bridge to clinical trial or allogeneic stem cell transplant
Giralt S et al. Biol Blood Marrow Transplant. 2015;21:2039.
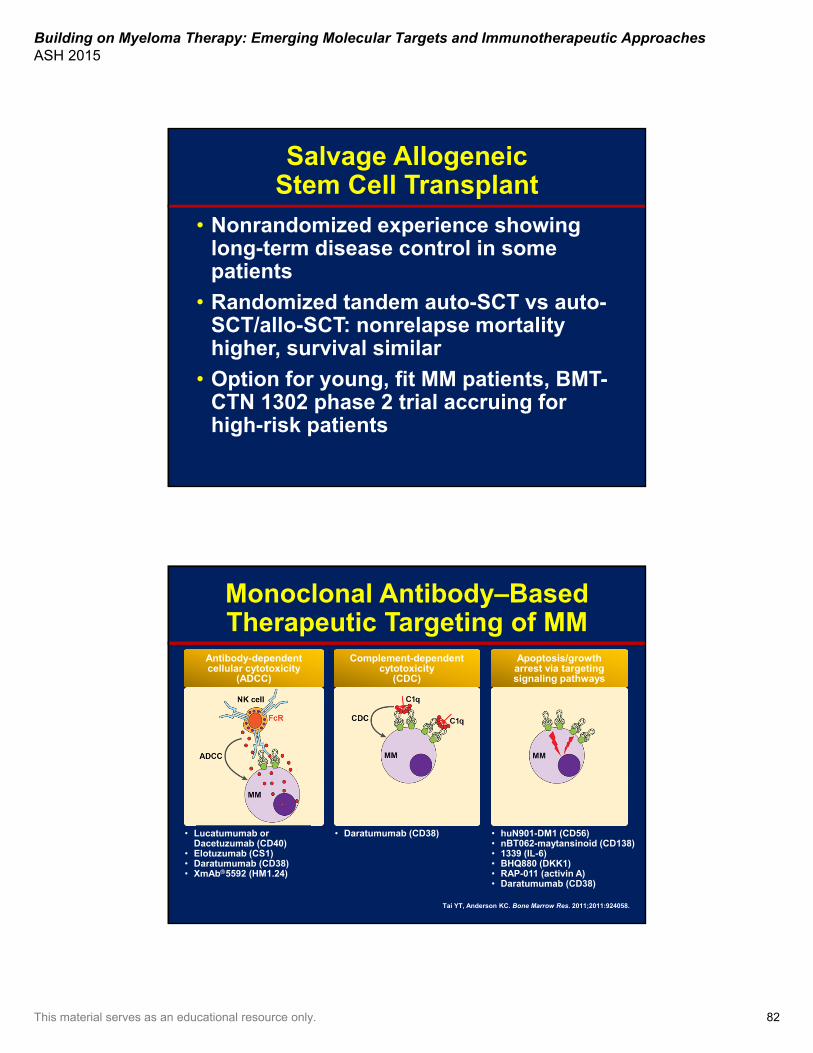
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 82
Salvage Allogeneic Stem Cell Transplant
• Nonrandomized experience showing long-term disease control in some patients
• Randomized tandem auto-SCT vs auto-SCT/allo-SCT: nonrelapse mortality higher, survival similar
• Option for young, fit MM patients, BMT-CTN 1302 phase 2 trial accruing for high-risk patients
Monoclonal Antibody–Based Therapeutic Targeting of MM
Apoptosis/growtharrest via targetingsignaling pathways
Complement-dependentcytotoxicity
(CDC)
Antibody-dependentcellular cytotoxicity
(ADCC)
• Lucatumumab or Dacetuzumab (CD40)
• Elotuzumab (CS1)• Daratumumab (CD38)• XmAb5592 (HM1.24)
• Daratumumab (CD38) • huN901-DM1 (CD56)• nBT062-maytansinoid (CD138)• 1339 (IL-6)• BHQ880 (DKK1)• RAP-011 (activin A)• Daratumumab (CD38)
Tai YT, Anderson KC. Bone Marrow Res. 2011;2011:924058.

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 83
AnMed
Blue Ridge
Cleveland Regional
CMC
LCI-Lincoln
LCI-Mercy
LCI-NortheastLCI-Pineville
LCI-Union
Roper St. FrancisStanly Regional
Thank you for your attention!
LCI-University
LCI-Main
Panel Discussion

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 84
Community Case Part 3
Case Study Part 3• Patient deferred Len maintenance and prefers
close observation
• Traveling for new job, starts to train for half-marathon 6 months post ASCT
• Monthly CBC, CMP, SPEP, FLC; doctor visits every 2–3 months
• Successfully runs half marathon for MMRF and raises $26K 1 year after ASCT
• Returns 2 years post-ASCT with increasing shoulder pain while working out in the gym, increasing fatigue, and urinary frequency with frothiness
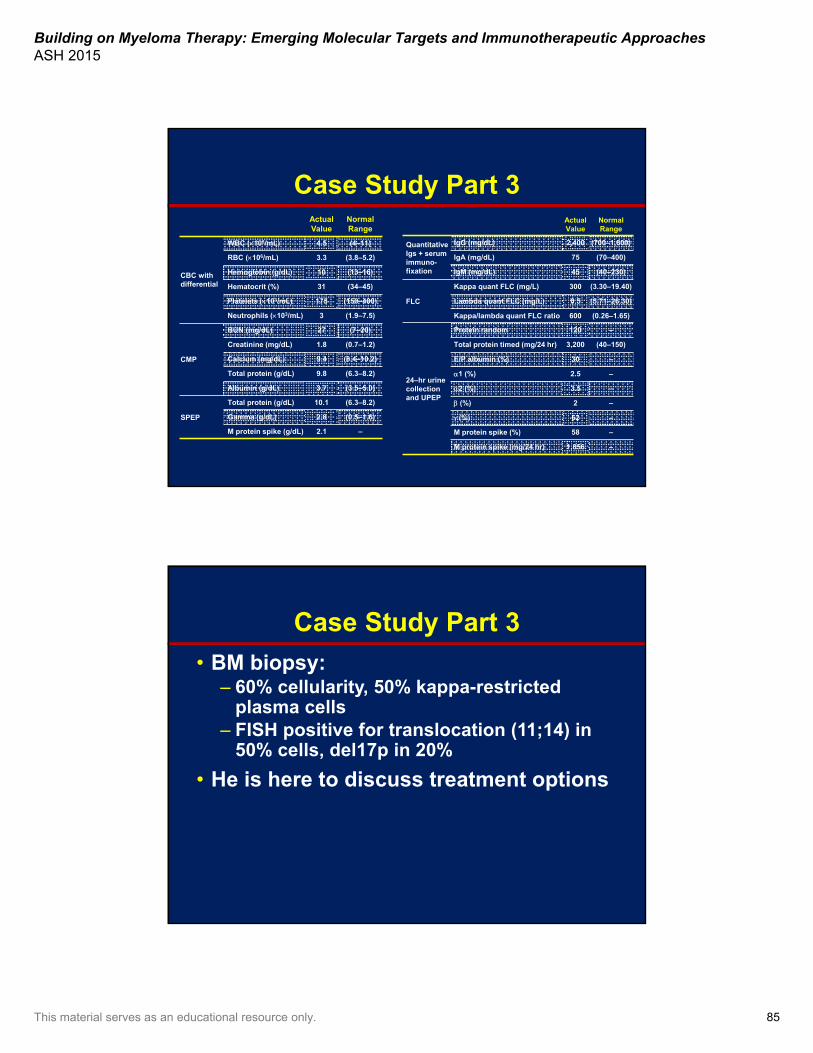
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 85
Case Study Part 3ActualValue
Normal Range
CBC withdifferential
WBC (103/mL) 4.5 (4–11)
RBC (106/mL) 3.3 (3.8–5.2)
Hemoglobin (g/dL) 10 (13–16)
Hematocrit (%) 31 (34–45)
Platelets (103/mL) 175 (150–400)
Neutrophils (103/mL) 3 (1.9–7.5)
CMP
BUN (mg/dL) 27 (7–20)
Creatinine (mg/dL) 1.8 (0.7–1.2)
Calcium (mg/dL) 9.4 (8.4–10.2)
Total protein (g/dL) 9.8 (6.3–8.2)
Albumin (g/dL) 3.7 (3.5–5.0)
SPEP
Total protein (g/dL) 10.1 (6.3–8.2)
Gamma (g/dL) 2.8 (0.5–1.6)
M protein spike (g/dL) 2.1 –
ActualValue
Normal Range
QuantitativeIgs + serum immuno-fixation
IgG (mg/dL) 2,400 (700–1,600)
IgA (mg/dL) 75 (70–400)
IgM (mg/dL) 45 (40–230)
FLC
Kappa quant FLC (mg/L) 300 (3.30–19.40)
Lambda quant FLC (mg/L) 0.5 (5.71–26.30)
Kappa/lambda quant FLC ratio 600 (0.26–1.65)
24–hr urinecollection and UPEP
Protein random 120 –
Total protein timed (mg/24 hr) 3,200 (40–150)
E/P albumin (%) 30 –
1 (%) 2.5 –
2 (%) 3.5 –
(%) 2 –
(%) 62 –
M protein spike (%) 58 –
M protein spike (mg/24 hr) 1,856 –
Case Study Part 3
• BM biopsy:– 60% cellularity, 50% kappa-restricted
plasma cells– FISH positive for translocation (11;14) in
50% cells, del17p in 20%
• He is here to discuss treatment options
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 86
What would you use for treatment of MM in first relapse?
A. Bortezomib + dexamethasone ±cyclophosphamide
B. Lenalidomide + dexamethasoneC. Pomalidomide + dexamethasoneD. Bortezomib, lenalidomide, and
dexamethasoneE. Carfilzomib + dexamethasoneF. Carfilzomib + lenalidomide + dexamethasoneG. Elotuzumab + lenalidomide + dexamethasoneH. Daratumumab
?
2015: Immunotherapy for the Treatment of Multiple Myeloma
Thomas Martin, MDUniversity of California, San Francisco
Medical CenterSan Francisco, California
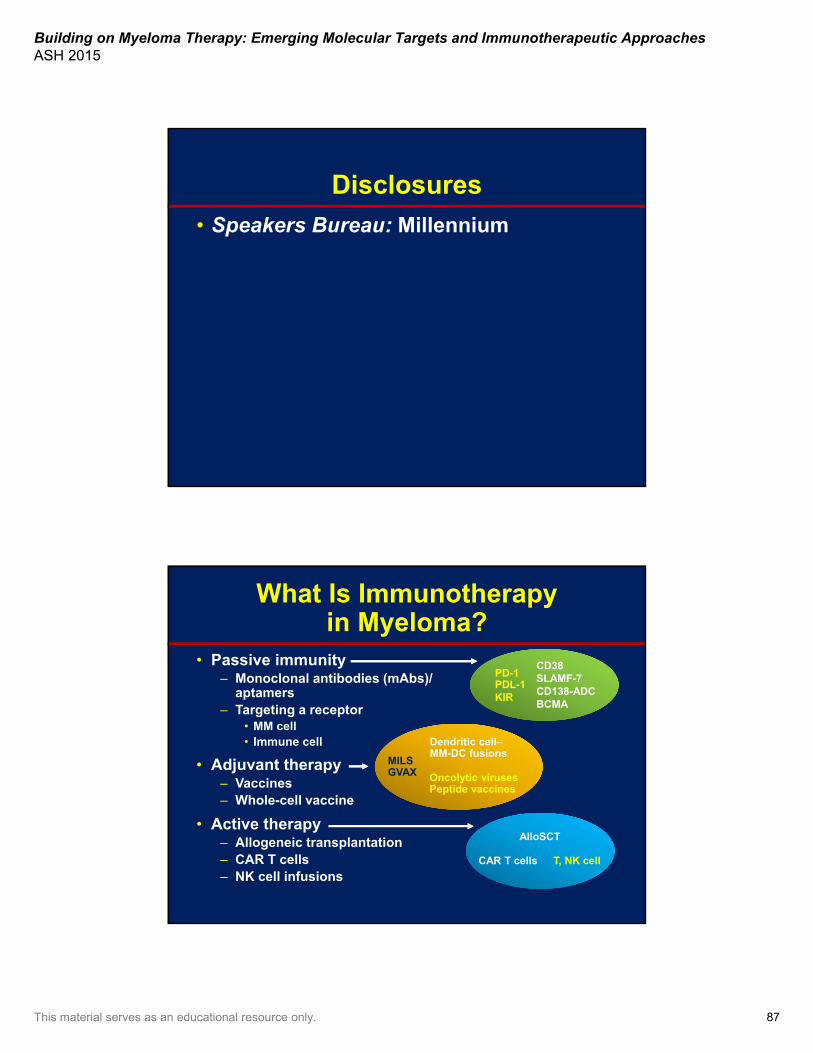
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 87
Disclosures
• Speakers Bureau: Millennium
What Is Immunotherapyin Myeloma?
• Passive immunity – Monoclonal antibodies (mAbs)/
aptamers– Targeting a receptor
• MM cell• Immune cell
• Adjuvant therapy – Vaccines– Whole-cell vaccine
• Active therapy– Allogeneic transplantation– CAR T cells– NK cell infusions
CD38SLAMF-7 CD138-ADCBCMA
CD38SLAMF-7 CD138-ADCBCMA
Dendritic cell–MM-DC fusionsDendritic cell–MM-DC fusions
MILSGVAX Oncolytic viruses
Peptide vaccines
PD-1PDL-1KIR
AlloSCTAlloSCT
CAR T cells T, NK cell
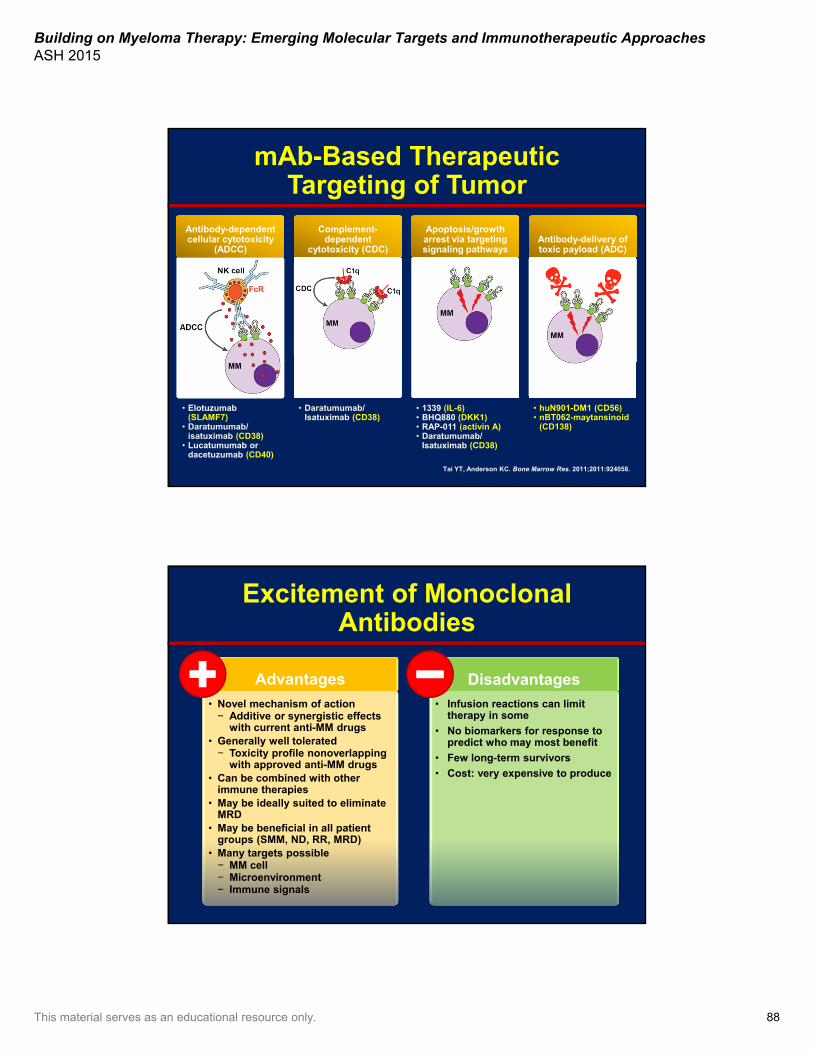
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 88
mAb-Based Therapeutic Targeting of Tumor
Apoptosis/growth arrest via targetingsignaling pathways
Complement-dependent
cytotoxicity (CDC)
Antibody-dependentcellular cytotoxicity
(ADCC)Antibody-delivery oftoxic payload (ADC)
• Elotuzumab (SLAMF7)
• Daratumumab/isatuximab (CD38)
• Lucatumumab or dacetuzumab (CD40)
• Daratumumab/ Isatuximab (CD38)
• 1339 (IL-6)• BHQ880 (DKK1)• RAP-011 (activin A)• Daratumumab/
Isatuximab (CD38)
• huN901-DM1 (CD56)• nBT062-maytansinoid
(CD138)
Tai YT, Anderson KC. Bone Marrow Res. 2011;2011:924058.
Excitement of Monoclonal Antibodies
• Novel mechanism of action− Additive or synergistic effects
with current anti-MM drugs• Generally well tolerated− Toxicity profile nonoverlapping
with approved anti-MM drugs• Can be combined with other
immune therapies• May be ideally suited to eliminate
MRD• May be beneficial in all patient
groups (SMM, ND, RR, MRD)• Many targets possible − MM cell− Microenvironment− Immune signals
Advantages
• Infusion reactions can limit therapy in some
• No biomarkers for response to predict who may most benefit
• Few long-term survivors
• Cost: very expensive to produce
Disadvantages
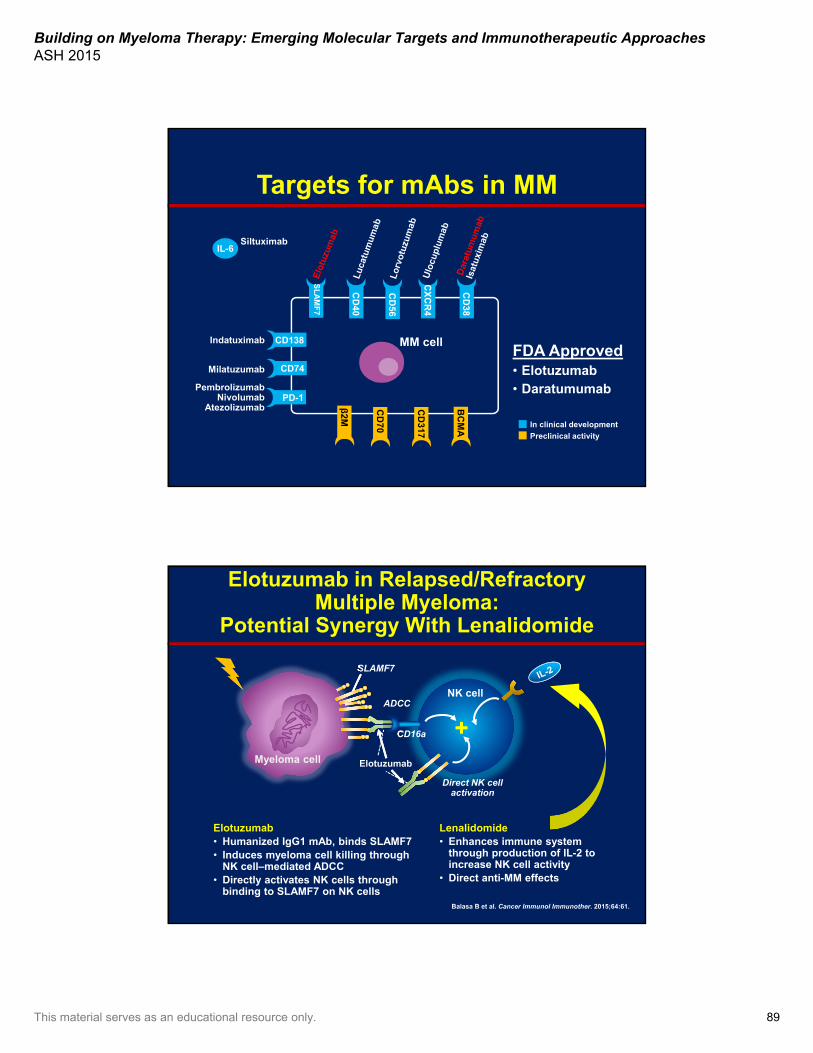
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 89
Targets for mAbs in MM
FDA Approved• Elotuzumab• Daratumumab
IL-6
CD
38
CD
40
CD
56
CX
CR
4
CD74
PD-1
CD138
β2M
MM cell
SL
AM
F7
Milatuzumab
PembrolizumabNivolumab
Atezolizumab
Indatuximab
Siltuximab
In clinical development
Preclinical activity
BC
MA
CD
70
CD
317
Elotuzumab in Relapsed/Refractory Multiple Myeloma:
Potential Synergy With Lenalidomide
Balasa B et al. Cancer Immunol Immunother. 2015;64:61.
Direct NK cell activation
NK cell
Elotuzumab
SLAMF7
ADCC
CD16a +Myeloma cell
Elotuzumab• Humanized IgG1 mAb, binds SLAMF7• Induces myeloma cell killing through
NK cell–mediated ADCC• Directly activates NK cells through
binding to SLAMF7 on NK cells
Lenalidomide• Enhances immune system
through production of IL-2 to increase NK cell activity
• Direct anti-MM effects

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 90
Elotuzumab in Relapsed/Refractory Multiple Myeloma:
Clinical Synergy With Lenalidomide• Elotuzumab in combination with lenalidomide and dexamethasone (E-Ld)
demonstrated a high response rate and progression-free survival (PFS) benefits in an open-label phase 1b/2 study1 in patients with MM
• Elotuzumab has FDA breakthrough therapy designation in MM
1. Richardson PG et al. Blood. 2014;124. Abstract 302.
6050403020100
-10-20-30-40-50-60-70-80-90
-100
10 mg/kg elotuzumab (n=36)
Per
cen
tag
e C
han
ge
Fro
m B
asel
ine
Maximum Percent Reduction in Serum M Protein in Multiple Myeloma – Study 17036050403020100
-10-20-30-40-50-60-70-80-90
-100
20 mg/kg elotuzumab (n=29)*
Per
cen
tag
e C
han
ge
Fro
m B
asel
ine
*Eight patients without measurable disease (baseline and all on-study M-protein levels <0.5 g/dL) were not included.
Repeat every 28 days
ELOQUENT-2 Study Design • Open-label, international, randomized, multicenter, phase 3 trial
(168 global sites)
Of note: ELOQUENT-1 Study: similar design in newly diagnosed MM; ongoing Lonial S et al. N Engl J Med. 2015;373:621.
• End points:– Co-primary: PFS and overall response rate (ORR)– Other: overall survival (data not yet mature); duration of response, quality of
life, safety
• All patients received premedication to mitigate infusion reactions prior to Elo administration
Key inclusion criteria• RRMM
• 1–3 prior lines of therapy
• Prior Len exposure permitted in 10% of study population (patients not refractory to Len)
Elo + Len/Dex (E-Ld) schedule (n=321)Elo (10 mg/kg IV): cycle 1 and 2: weekly;
cycles 3+: every other weekLen (25 mg PO): days 1–21
Dex: weekly equivalent, 40 mg
Len/Dex (Ld) schedule (n=325)Len (25 mg PO): days 1–21
Dex: 40 mg PO days 1, 8, 15, 22
Assessment• Tumor response:
every 4 weeks until progressive disease
• Survival: every 12 weeks after disease progression
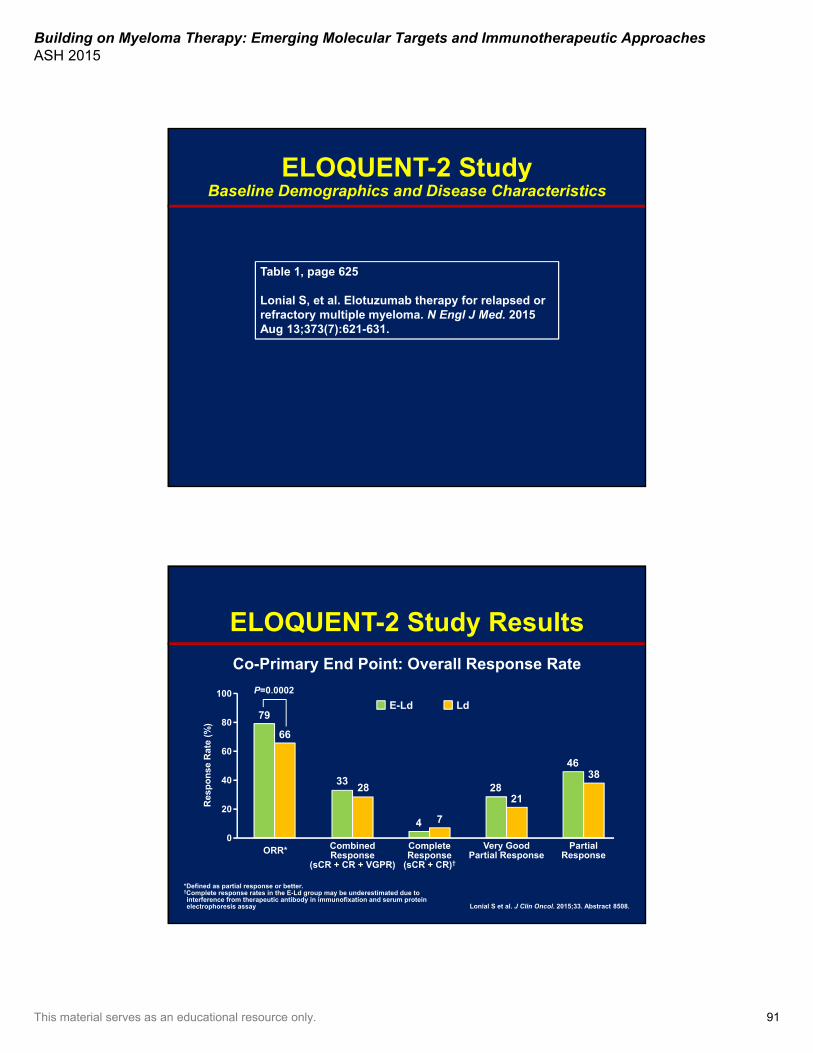
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 91
ELOQUENT-2 StudyBaseline Demographics and Disease Characteristics
Table 1, page 625
Lonial S, et al. Elotuzumab therapy for relapsed or refractory multiple myeloma. N Engl J Med. 2015 Aug 13;373(7):621-631.
ELOQUENT-2 Study Results
Co-Primary End Point: Overall Response Rate
Lonial S et al. J Clin Oncol. 2015;33. Abstract 8508.
*Defined as partial response or better.†Complete response rates in the E-Ld group may be underestimated due to interference from therapeutic antibody in immunofixation and serum protein electrophoresis assay
100
80
60
40
20
0
Res
po
nse
Rat
e (%
)
ORR* CombinedResponse
(sCR + CR + VGPR)
CompleteResponse
(sCR + CR)†
Very GoodPartial Response
PartialResponse
E-Ld Ld79
66
3328
4 7
2821
4638
P=0.0002
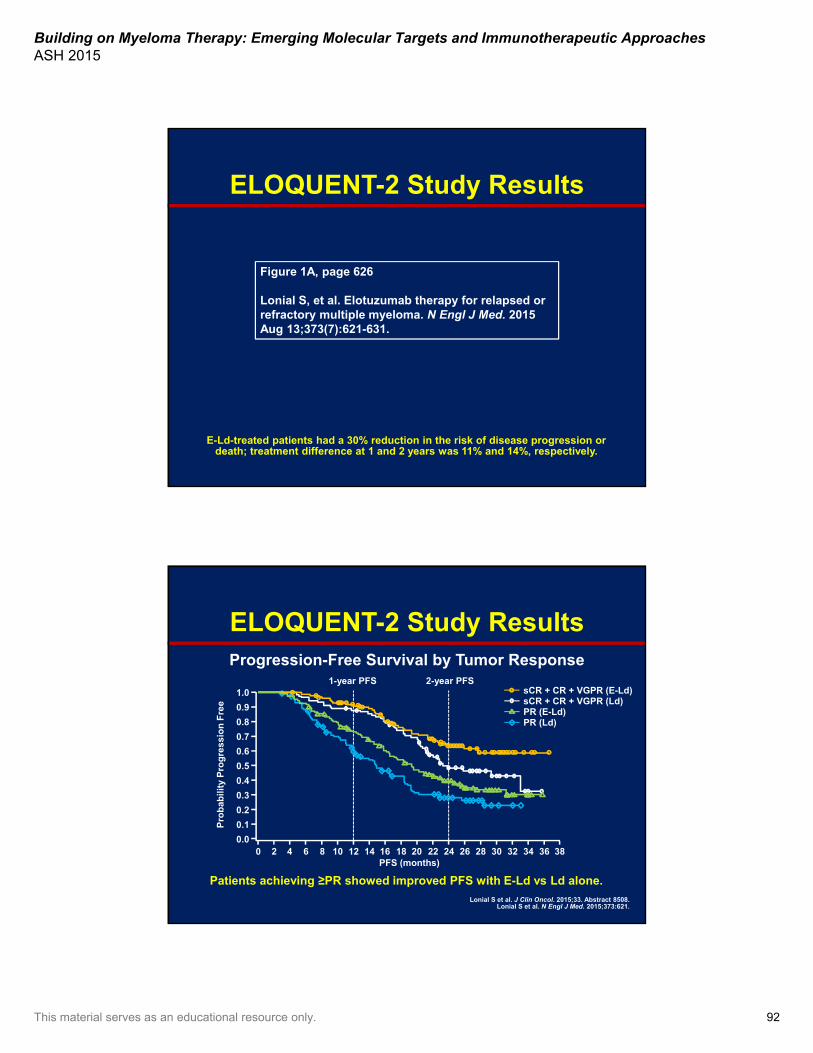
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 92
ELOQUENT-2 Study Results
E-Ld-treated patients had a 30% reduction in the risk of disease progression or death; treatment difference at 1 and 2 years was 11% and 14%, respectively.
Figure 1A, page 626
Lonial S, et al. Elotuzumab therapy for relapsed or refractory multiple myeloma. N Engl J Med. 2015 Aug 13;373(7):621-631.
ELOQUENT-2 Study ResultsProgression-Free Survival by Tumor Response
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38PFS (months)
Patients achieving ≥PR showed improved PFS with E-Ld vs Ld alone.
1.0
0.8
0.6
0.4
0.2
0.0
Pro
bab
ilit
y P
rog
ress
ion
Fre
e 0.9
0.7
0.5
0.3
0.1
1-year PFS 2-year PFSsCR + CR + VGPR (E-Ld)sCR + CR + VGPR (Ld)PR (E-Ld)PR (Ld)
Lonial S et al. J Clin Oncol. 2015;33. Abstract 8508.Lonial S et al. N Engl J Med. 2015;373:621.

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 93
24
ELOQUENT-2 Study ResultsProgression-Free Survival According to Age
Lonial S et al. J Clin Oncol. 2015;33. Abstract 8508.
100
80
60
40
20
0
Pro
gre
ssio
n-F
ree
Pat
ien
ts (
%)
90
70
50
30
10
0 2 4 6 8 101214161820222426283032343638
Time (months)
100
80
60
40
20
0
Pro
gre
ssio
n-F
ree
Pat
ien
ts (
%)
90
70
50
30
10
0 2 4 6 8 10121416182022 26283032343638
Time (months)
2-year PFS2-year PFS
≥65 years<65 years
Hazard ratio: 0.75(95% CI, 0.551.02)
Hazard ratio: 0.65(95% CI, 0.500.85)
40%
30%
E-Ld
Ld
42%
25%
E-Ld
Ld
1.0
0.8
0.6
0.4
0.2
0.0
Pro
bab
ilit
y P
rog
ress
ion
Fre
e
0.9
0.7
0.5
0.3
0.1
0 2 4 6 8 10 121416 18 20 2224 2628 3032 3436 38
PFS (months)
ELOQUENT-2 Study Results
Lonial S et al. J Clin Oncol. 2015;33. Abstract 8508.
Progression-Free Survival of Patients With del(17p) and t(4;14) Translocation
1.0
0.8
0.6
0.4
0.2
0.0
Pro
bab
ilit
y P
rog
ress
ion
Fre
e
0.9
0.7
0.5
0.3
0.1
0 2 4 6 8 10 121416 18 20 2224 26 28 3032 3436 38
PFS (months)
t(4;14)+del(17p)+
Hazard ratio: 0.65(95% CI, 0.450.94)
Hazard ratio: 0.53(95% CI, 0.290.95)
E-Ld
Ld E-Ld
Ld
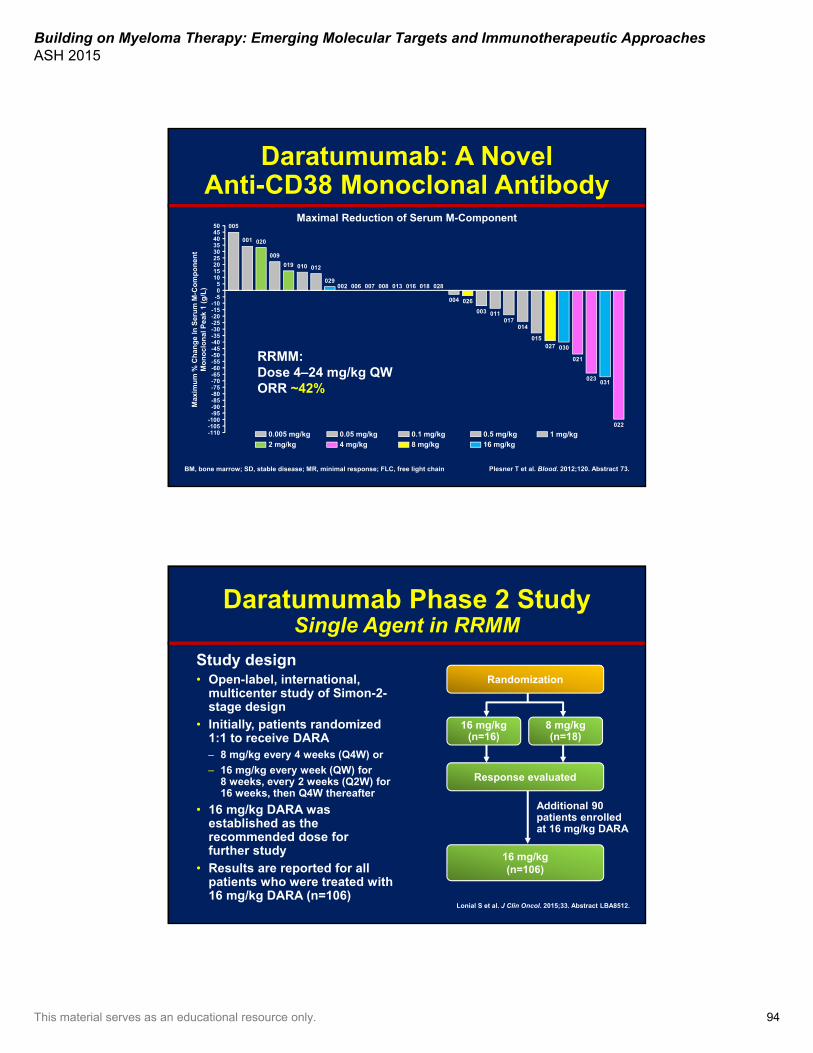
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 94
Maximal Reduction of Serum M-Component
RRMM:Dose 4–24 mg/kg QW ORR ~42%
Plesner T et al. Blood. 2012;120. Abstract 73.
Daratumumab: A Novel Anti-CD38 Monoclonal Antibody
504540353025201510
50
-5-10-15-20-25-30-35-40-45-50-55-60-65-70-75-80-85-90-95
-100-105-110
Max
imu
m %
Ch
ang
e In
Ser
um
M-C
om
po
nen
t M
on
ocl
on
al P
eak
1 (g
/L)
005
001 020
009
019 010
029
012
002 006 007 008 013 016 018 028
004 026
003 011017
014
015027 030
021
023031
022
0.005 mg/kg
2 mg/kg
0.05 mg/kg
4 mg/kg
0.1 mg/kg
8 mg/kg
0.5 mg/kg
16 mg/kg1 mg/kg
BM, bone marrow; SD, stable disease; MR, minimal response; FLC, free light chain
Daratumumab Phase 2 StudySingle Agent in RRMM
Study design• Open-label, international,
multicenter study of Simon-2-stage design
• Initially, patients randomized 1:1 to receive DARA– 8 mg/kg every 4 weeks (Q4W) or
– 16 mg/kg every week (QW) for 8 weeks, every 2 weeks (Q2W) for 16 weeks, then Q4W thereafter
• 16 mg/kg DARA was established as the recommended dose for further study
• Results are reported for all patients who were treated with 16 mg/kg DARA (n=106)
Lonial S et al. J Clin Oncol. 2015;33. Abstract LBA8512.
Randomization
16 mg/kg(n=16)
8 mg/kg(n=18)
Response evaluated
16 mg/kg(n=106)
Additional 90 patients enrolled at 16 mg/kg DARA
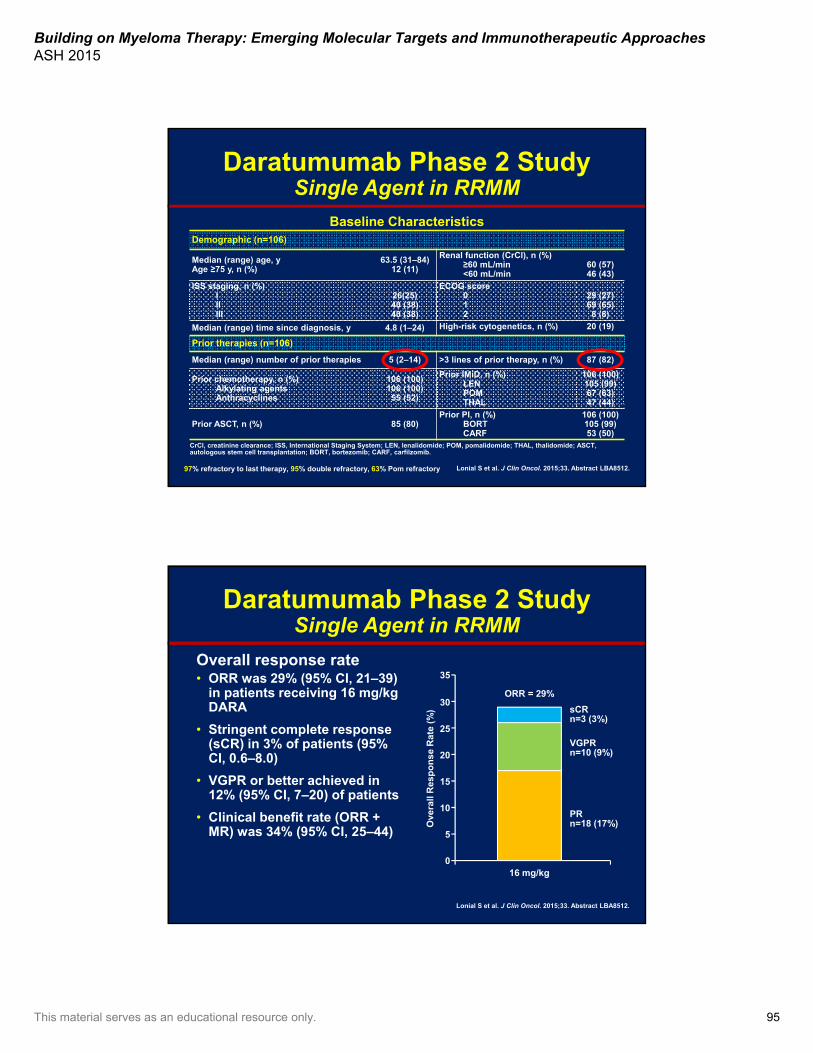
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 95
Daratumumab Phase 2 StudySingle Agent in RRMM
97% refractory to last therapy, 95% double refractory, 63% Pom refractory Lonial S et al. J Clin Oncol. 2015;33. Abstract LBA8512.
Baseline CharacteristicsDemographic (n=106)
Median (range) age, yAge ≥75 y, n (%)
63.5 (31–84)12 (11)
Renal function (CrCl), n (%)≥60 mL/min<60 mL/min
60 (57)46 (43)
ISS staging, n (%)IIIIII
26(25)40 (38)40 (38)
ECOG score012
29 (27)69 (65)8 (8)
Median (range) time since diagnosis, y 4.8 (1–24) High-risk cytogenetics, n (%) 20 (19)
Prior therapies (n=106)
Median (range) number of prior therapies 5 (2–14) >3 lines of prior therapy, n (%) 87 (82)
Prior chemotherapy, n (%)Alkylating agentsAnthracyclines
106 (100)106 (100)55 (52)
Prior IMiD, n (%)LENPOMTHAL
106 (100)105 (99)67 (63)47 (44)
Prior ASCT, n (%) 85 (80)Prior PI, n (%)
BORTCARF
106 (100)105 (99)53 (50)
CrCl, creatinine clearance; ISS, International Staging System; LEN, lenalidomide; POM, pomalidomide; THAL, thalidomide; ASCT,autologous stem cell transplantation; BORT, bortezomib; CARF, carfilzomib.
Daratumumab Phase 2 StudySingle Agent in RRMM
Overall response rate• ORR was 29% (95% CI, 21–39)
in patients receiving 16 mg/kg DARA
• Stringent complete response (sCR) in 3% of patients (95% CI, 0.6–8.0)
• VGPR or better achieved in 12% (95% CI, 7–20) of patients
• Clinical benefit rate (ORR + MR) was 34% (95% CI, 25–44)
Lonial S et al. J Clin Oncol. 2015;33. Abstract LBA8512.
35
25
15
5
0
Ove
rall
Res
po
nse
Rat
e (%
)
30
20
10
16 mg/kg
ORR = 29%
sCRn=3 (3%)
VGPRn=10 (9%)
PRn=18 (17%)

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 96
Daratumumab Phase 2 StudySingle Agent in RRMM
Change in Paraprotein From Baseline
Lonial S et al. J Clin Oncol. 2015;33. Abstract LBA8512.
100
50
0
-75
-100
Max
imu
m C
han
ge
Fro
m
Bas
elin
e (%
)
75
25
-25
-50
-90
• The majority of patients had reductions in paraprotein from baseline– 40 patients (38%) had reductions >50%– 17 patients (16%) had reductions >90%
20
35
5
OR
R, %
10
25
15
0
Lonial S et al. J Clin Oncol. 2015;33. Abstract LBA8512.
40
30
Daratumumab Phase 2 StudySingle Agent in RRMM
33 3330
21 20
30 29 28 2826
21
ORR by Subgroup
Refractory to

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 97
Daratumumab Phase 2 StudySingle Agent in RRMM
Lonial S et al. J Clin Oncol. 2015;33. Abstract LBA8512.
Progression-Free and Overall Survival
20
80
Pat
ien
ts P
rog
ress
ion
-Fre
e an
d A
live
(%
)
40
0
100
60
0 2 4 6 8 10 12 14 16
Months From Start of Treatment
Median PFS = 3.7 months(95% CI, 2.8–4.6)
20
80
Pat
ien
ts A
live
(%)
40
0
100
60
0 2 4 6 8 10 12 14 16
Months From Start of Treatment
Median OS = NE(95% CI, 13.7–NE)
• 29 of 31 responders are still alive• The 1-year survival rate was 65% (95% CI, 51.2–75.5)
Phase 1 Isatuximab Monotherapy Study: Results High-Risk Cohort
Key eligibility criteria• 17 p del, t(4;14), t(14;16), t(14;20), or
>3 copies of 1q21• Relapsed <6 months of autologous
transplantation• A high-risk GEP signature Patient characteristics• Median prior lines of treatment: 4.5
(range 2–8)• All patients received IMiD and
proteasome inhibitor• Majority (72.2%) received
pomalidomide or carfilzomib
Overall response rate
# Responder features1 t(4;14)2 17p and 1q gains3 t(4;14)4 HR GEP
22.2
0
10
20
30
40
50
60
10mg/kg Q2W (HR)(N=18)
ORR = 22% (4/18)
Presented by Tom Martin at IMW Rome, Italy 2015
High-risk criteria N=1817p 4 (22.2%)
17p and 1q gains 4 (22.2%)
1q 4 (22.2%)
1q and t(4;14) 2 (11.1%)
t(4;14) 2 (11.1%)
HR GEP 1 (5.6%)
Transplant relapse 1 (5.6%)
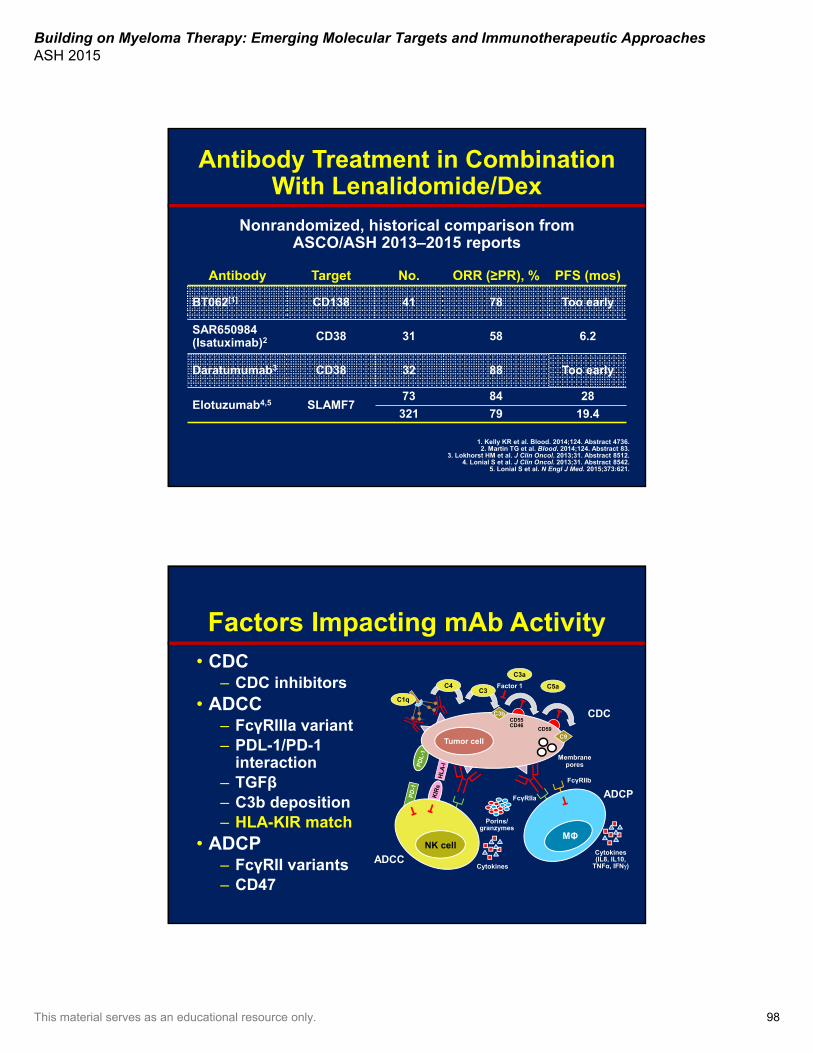
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 98
Antibody Treatment in Combination With Lenalidomide/Dex
Antibody Target No. ORR (≥PR), % PFS (mos)
BT062[1] CD138 41 78 Too early
SAR650984 (Isatuximab)2 CD38 31 58 6.2
Daratumumab3 CD38 32 88 Too early
Elotuzumab4,5 SLAMF773 84 28
321 79 19.4
Nonrandomized, historical comparison from ASCO/ASH 2013–2015 reports
1. Kelly KR et al. Blood. 2014;124. Abstract 4736.2. Martin TG et al. Blood. 2014;124. Abstract 83.
3. Lokhorst HM et al. J Clin Oncol. 2013;31. Abstract 8512.4. Lonial S et al. J Clin Oncol. 2013;31. Abstract 8542.
5. Lonial S et al. N Engl J Med. 2015;373:621.
Factors Impacting mAb Activity• CDC
– CDC inhibitors• ADCC
– FcγRIIIa variant – PDL-1/PD-1
interaction– TGFβ – C3b deposition– HLA-KIR match
• ADCP– FcγRII variants– CD47
C3a
C5aC3
C4
C1q
Tumor cell
C3b
Factor 1
CDC
C9
CD55CD46
CD59
Membranepores
ADCC
ADCP
FcγRIIb
FcγRIIa
Porins/granzymes
Cytokines
Cytokines(IL8, IL10,
TNFα, IFN)
NK cellMΦ
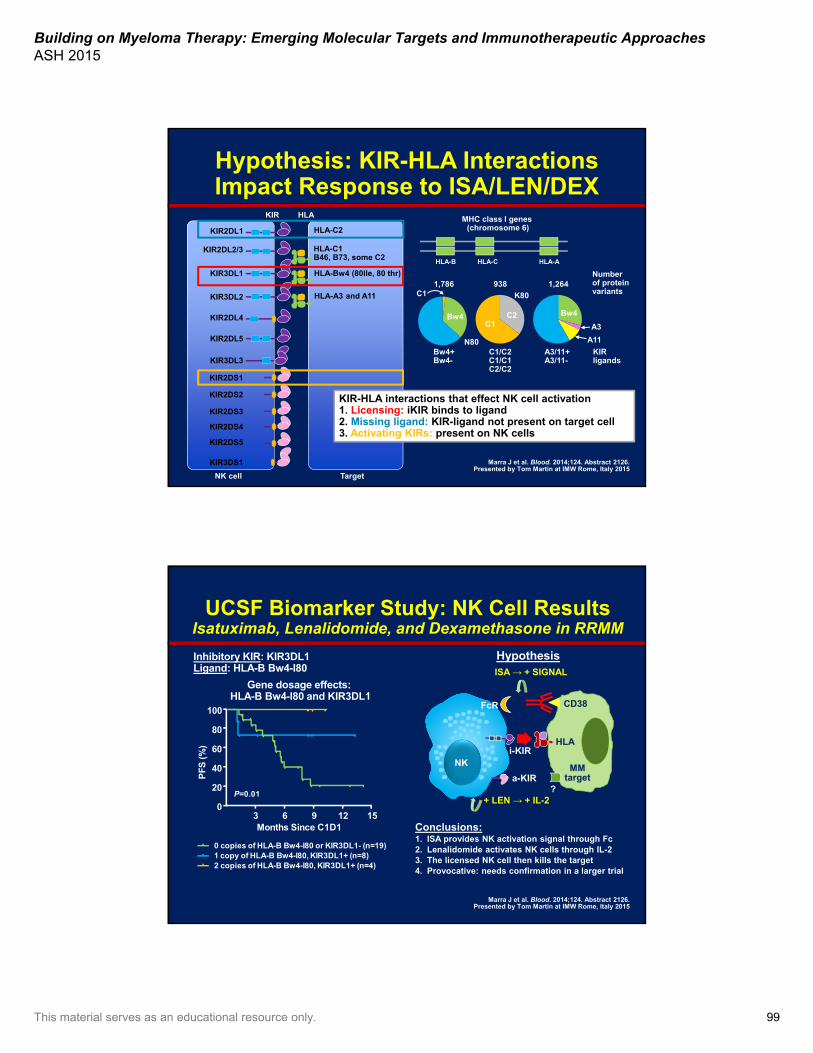
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 99
Target
HLA
HLA-A3 and A11
HLA-Bw4 (80lle, 80 thr)
HLA-C1B46, B73, some C2
HLA-C2
HLA-CHLA-B HLA-A
1,786 938 1,264
MHC class I genes (chromosome 6)
Number of proteinvariants
KIRligands
Bw4+Bw4-
C1/C2C1/C1C2/C2
A3/11+A3/11-
Bw4
C1
C1C2 Bw4
A11
A3
N80
K80
NK cell
KIR3DL2
KIR3DL1
KIR3DS1
KIR2DS5
KIR2DS4
KIR2DS3
KIR2DS2
KIR2DS1
KIR2DL2/3
KIR3DL3
KIR2DL5
KIR2DL4
KIR2DL1
KIR
KIR-HLA interactions that effect NK cell activation1. Licensing: iKIR binds to ligand2. Missing ligand: KIR-ligand not present on target cell3. Activating KIRs: present on NK cells
Hypothesis: KIR-HLA Interactions Impact Response to ISA/LEN/DEX
Marra J et al. Blood. 2014;124. Abstract 2126.Presented by Tom Martin at IMW Rome, Italy 2015
UCSF Biomarker Study: NK Cell ResultsIsatuximab, Lenalidomide, and Dexamethasone in RRMM
Months Since C1D1
PF
S(%
)
3 12 15
20
0 copies of HLA-B Bw4-I80 or KIR3DL1- (n=19) 1 copy of HLA-B Bw4-I80, KIR3DL1+ (n=8)2 copies of HLA-B Bw4-I80, KIR3DL1+ (n=4)
P=0.01
Conclusions: 1. ISA provides NK activation signal through Fc2. Lenalidomide activates NK cells through IL-2 3. The licensed NK cell then kills the target4. Provocative: needs confirmation in a larger trial
Hypothesis
NK i-KIR
a-KIR
FcR
HLA
CD38
?
MMtarget
ISA → + SIGNAL
+ LEN → + IL-2
80
60
40
100
06 9
Gene dosage effects: HLA-B Bw4-I80 and KIR3DL1
Inhibitory KIR: KIR3DL1Ligand: HLA-B Bw4-I80
Marra J et al. Blood. 2014;124. Abstract 2126.Presented by Tom Martin at IMW Rome, Italy 2015
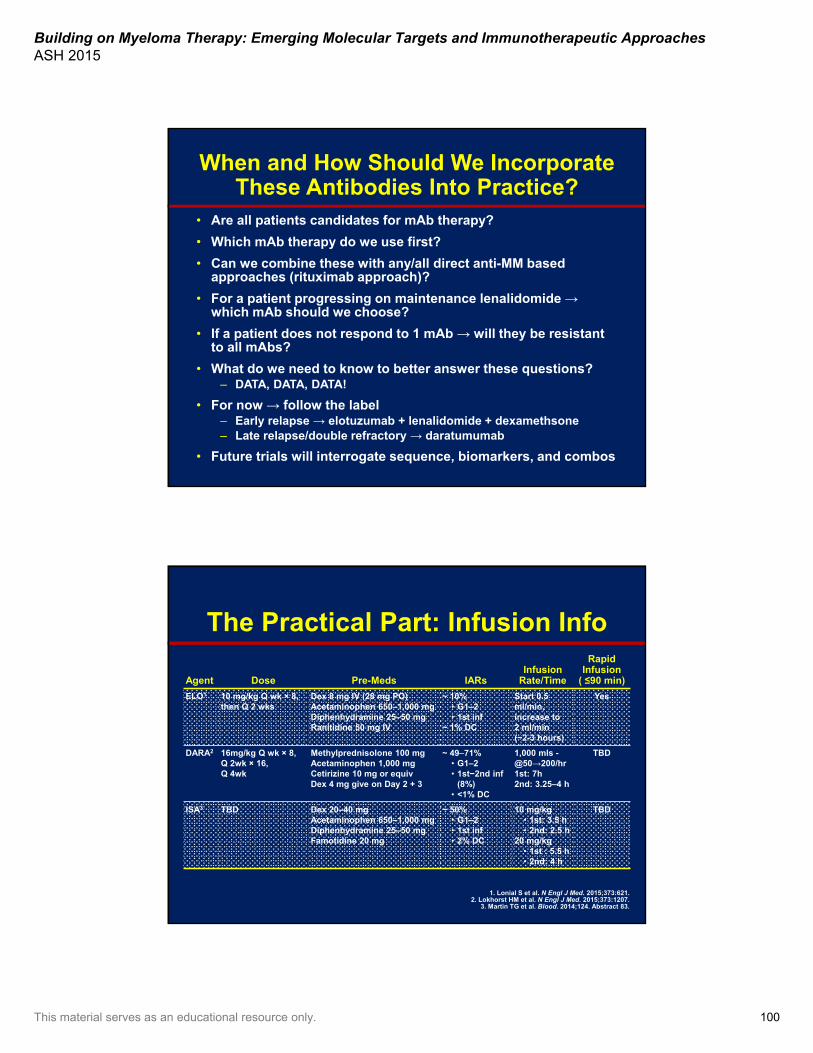
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 100
When and How Should We Incorporate These Antibodies Into Practice?
• Are all patients candidates for mAb therapy?
• Which mAb therapy do we use first?
• Can we combine these with any/all direct anti-MM based approaches (rituximab approach)?
• For a patient progressing on maintenance lenalidomide →which mAb should we choose?
• If a patient does not respond to 1 mAb → will they be resistant to all mAbs?
• What do we need to know to better answer these questions?– DATA, DATA, DATA!
• For now → follow the label– Early relapse → elotuzumab + lenalidomide + dexamethsone– Late relapse/double refractory → daratumumab
• Future trials will interrogate sequence, biomarkers, and combos
The Practical Part: Infusion Info
Agent Dose Pre-Meds IARsInfusion
Rate/Time
Rapid Infusion
( ≤90 min)
ELO1 10 mg/kg Q wk × 8, then Q 2 wks
Dex 8 mg IV (28 mg PO)Acetaminophen 650–1,000 mgDiphenhydramine 25–50 mgRanitidine 50 mg IV
~ 10%• G1–2• 1st inf
~ 1% DC
Start 0.5 ml/min, increase to 2 ml/min(~2-3 hours)
Yes
DARA2 16mg/kg Q wk × 8, Q 2wk × 16, Q 4wk
Methylprednisolone 100 mgAcetaminophen 1,000 mgCetirizine 10 mg or equivDex 4 mg give on Day 2 + 3
~ 4971%• G1–2• 1st−2nd inf
(8%)• <1% DC
1,000 mls -@50→200/hr1st: 7h2nd: 3.25–4 h
TBD
ISA3 TBD Dex 20–40 mgAcetaminophen 650–1,000 mgDiphenhydramine 25–50 mgFamotidine 20 mg
~ 50%• G1–2• 1st inf• 2% DC
10 mg/kg• 1st: 3.5 h• 2nd: 2.5 h
20 mg/kg• 1st : 5.5 h• 2nd: 4 h
TBD
1. Lonial S et al. N Engl J Med. 2015;373:621. 2. Lokhorst HM et al. N Engl J Med. 2015;373:1207.
3. Martin TG et al. Blood. 2014;124. Abstract 83.
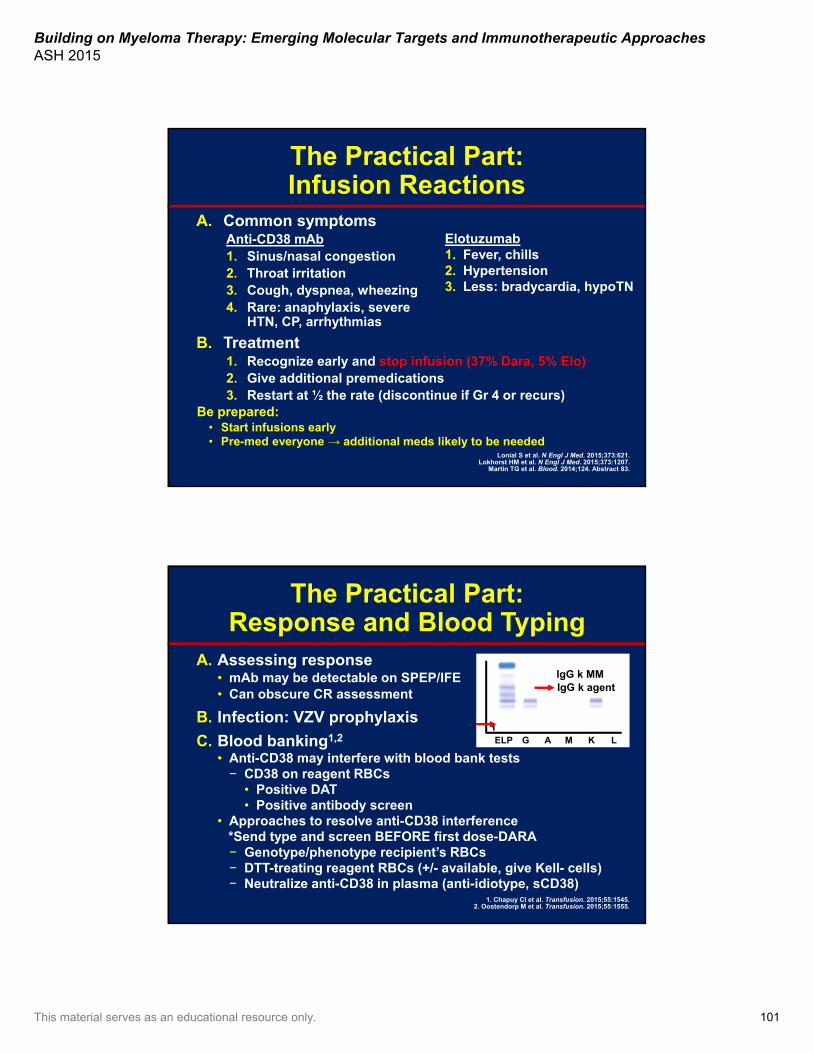
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 101
The Practical Part: Infusion Reactions
A. Common symptomsAnti-CD38 mAb1. Sinus/nasal congestion2. Throat irritation3. Cough, dyspnea, wheezing4. Rare: anaphylaxis, severe
HTN, CP, arrhythmias
B. Treatment1. Recognize early and stop infusion (37% Dara, 5% Elo)2. Give additional premedications3. Restart at ½ the rate (discontinue if Gr 4 or recurs)
Be prepared: • Start infusions early• Pre-med everyone → additional meds likely to be needed
Lonial S et al. N Engl J Med. 2015;373:621. Lokhorst HM et al. N Engl J Med. 2015;373:1207.
Martin TG et al. Blood. 2014;124. Abstract 83.
Elotuzumab1. Fever, chills2. Hypertension3. Less: bradycardia, hypoTN
The Practical Part:Response and Blood Typing
A. Assessing response• mAb may be detectable on SPEP/IFE• Can obscure CR assessment
B. Infection: VZV prophylaxis
C. Blood banking1,2
• Anti-CD38 may interfere with blood bank tests− CD38 on reagent RBCs
• Positive DAT• Positive antibody screen
• Approaches to resolve anti-CD38 interference*Send type and screen BEFORE first dose-DARA− Genotype/phenotype recipient’s RBCs− DTT-treating reagent RBCs (+/- available, give Kell- cells)− Neutralize anti-CD38 in plasma (anti-idiotype, sCD38)
1. Chapuy CI et al. Transfusion. 2015;55:1545.2. Oostendorp M et al. Transfusion. 2015;55:1555.
IgG k MMIgG k agent
ELP G A M K L1
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 102
FUTURE: Where do we go from here?
• Novel antibodies– More specific targets– Checkpoint inhibitors (PD-1, PDL-1)– Stromal compartment/ cell-cell interactions
• Antibody-drug conjugates– BT-062 (anti-CD138)– GSK2857916 (anti-BCMA)
• Can we combine mAbs with ?– Novel drugs– ELO + anti-KIR, ELO + CD137– Vaccines + antibodies
Conclusions• Antibody therapy has “come of age”
– ELO with Len/Dex for early relapse in Len sensitive– DARA for double refractory
• Combinations actively be tested– Frontline, early relapse, and refractory – Proteasome inhibitors, pomalidomide, other mAbs
• Future efforts need to focus on:– Identifying biomarkers for response/relapse– Optimizing the combinations and dosing strategies– Potentially using genomic data to help select patients
• All patients are appropriate for clinical trials
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 103
Novel Therapeutics in Myeloma: Update
A. Keith Stewart, MBChB, MRCP, FRCPC, MBAVasek and Anna Maria Polak Professor of Cancer Research
Consultant, Division of Hematology/OncologyMayo Clinic
Scottsdale, Arizona
Disclosures
• Consultant/Advisor: Bristol-Myers Squibb, Celgene, Janssen, MedImmune, Novartis, Takeda Oncology

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 104
Progression-Free Survival in Late-Stage Disease
Figure 2A, page 1059
San Miguel J, et al. Pomalidomide plus low-dose dexamethasone versus high-dose dexamethasone alone for patients with relapsed and refractory multiple myeloma (MM-003): a randomised, open-label, phase 3 trial. Lancet Oncol. 2013 Oct;14(11):1055-1066.
What’s New in MM Therapeutics?
• Ixazomib
• Oprozomib
Oral proteasome
inhibitors
• Elotuzumab
• Daratumumab
• Isatuximab
Monoclonal antibodies
• Afuresertib
• Dinaciclib
• PIM (LGH447)
• Trametinib
Kinase inhibitors
• Panobinostat
• Ricolinostat
HDACs
• ABT-199
• Selinexor
Novel mechanisms
• CAR-T
• BITE
• PDL-1/PD-1
Immuno-therapies
HDAC, histone deacetylase.

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 105
Profile of Single-Agent Oprozomib in Patients With Multiple Myeloma:
Updated Results From a Multicenter, Open-Label, Dose-
Escalation Phase 1b/2 Study
Ravi Vij,1 Michael Savona,2 David Siegel,3 Jonathan Kaufman,4Ashraf Badros,5 Irene Ghobrial,6 Agne Paner,7
Sundar Jagannath,8 Andrzej Jakubowiak,9 Joseph Mikhael,10
Prashant Kapoor,11 Linda Neuman,12 Jesus Berdeja13
1Washington University, St. Louis, MO; 2Vanderbilt University, Nashville, TN; 3John Theurer Cancer Center at Hackensack University Medical Center, Hackensack, NJ; 4Winship Cancer Institute, Emory University, Atlanta, GA; 5University of Maryland, Baltimore, MD; 6Dana-Farber Cancer Institute, Boston, MA; 7Rush University, Chicago, IL;
8Mt. Sinai Hospital, New York, NY; 9University of Chicago Medical Center, Chicago, IL; 10Mayo Clinic, Scottsdale, AZ; 11Mayo Clinic, Rochester, MN; 12Onyx Pharmaceuticals, Inc., an Amgen subsidiary, South San Francisco, CA;
13Sarah Cannon Research Institute, Nashville, TN
Phase 1b/2 Study of Single-Agent Oprozomib in MM: Efficacy
9 42
44
9
19
9
19
12
13
2
0 20 40 60 80 100
Phase 1b + 2 150–270 mg/d
(n=43)
Phase 1b 150–330 mg/d
(n=16)
PD
SD
MR
PR
VGPR
CR
5/14
Sch
edu
le2
2/7
Sch
edu
le1
Patients, %
CBR 50%
CBR 32.6%
ORR 31.3%
ORR 23.3%3
1 2/7 schedule: 1 patient (6%) was not evaluable.2 5/14 schedule: 5 patients (12%) were not evaluable and 2 patients (5%) were off study before response assessment.
3 ORR in 11 CFZ-refractory patients (phase 2): 18.2%. Vij R et al. Blood. 2014;124. Abstract 34.

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 106
Phase 1b/2 Study of Single-Agent Oprozomib in MM
Vij R et al. Blood. 2014;124. Abstract 34.
Authors’ Conclusions
The most common grade ≥3 nonhematologic AEs were diarrhea, nausea, and vomiting; rates of treatment-emergent PN and rash were low.
Recommended phase 2 dose and schedule: 240/300 mg/day in the 2/7 step-up schedule and 150/180 mg/day in the 5/14 step-up schedule.
Preliminary data suggest that step-up dosing is associated with improved tolerability.
Enrollment of patients with MM continues both schedules in the phase 2 study with a target of 94 patients; all patients are now receiving a new (extended-release) formulation of oprozomib.
Single-agent oprozomib has promising antitumor activity, with responses observed in patients who had carfilzomib-refractory MM.
Phase 1b Study of Ricolinostat (ACY-1215) + LEN-DEX in Patients With RRMM: Efficacy
and Authors’ Conclusions
1625
32
42
24
88
0
25
50
75
100
All Evaluable(n=25)
LEN Refractory(n=12)
Pat
ien
ts (
%)
MR PR VGPR sCR
ORR: 64%ORR: 50%
Yee AJ et al. Blood. 2014;124. Abstract 4772.
Ricolinostat is well tolerated when combined with LenDex at doses up to 160 mg bid; most AEs were low-grade and manageable.
Continuous bid treatment for 21 days is ongoing.
ORR was 64% and CBR was 80%; response rate was 85% in LEN-sensitive and -naive patients, and 50% in LEN-refractory patients.

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 107
Phase 1b Study of Ricolinostat (ACY-1215) and BTZ-DEX in Patients With RRMM
Vogl DT et al. Blood. 2014;124. Abstract 4764.
Ricolinostat is tolerable with clinical benefit in combination with bortezomib/dexamethasone.
No differences in PK were observed for the strength formulations.
Toxicities were generally manageable.
Responses were observed in this heavily pretreated population.
An expansion cohort at 160 mg QD is ongoing to better define a recommended phase 2 dose.
Authors’ Conclusions
A Phase 1/2 Trial of Dinaciclib, a Small Molecule Inhibitor of Cyclin-Dependent
Kinase 5 (CDK5)
• 29 patients were accrued (19 phase 1, 9 phase 2)
• Median time from diagnosis to registration was 3.5 years
• Median follow-up for patients still alive is 3.2 months (range: 0.7–20.8)
• Toxicity profile was hematological, fatigue, nausea, and mucositis
• Preclinical work indicates high synergy with bortezomib phase 1b trials now under way
Kumar SK et al. Blood. 2015;125:443.
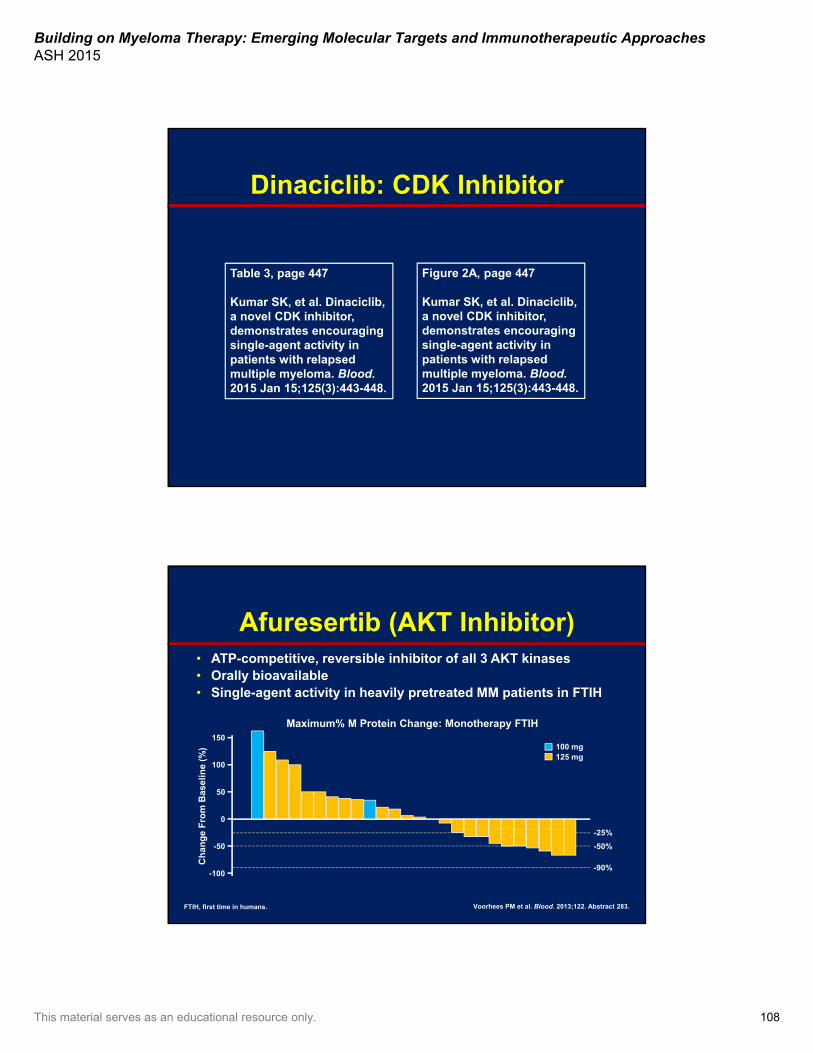
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 108
Table 3, page 447
Kumar SK, et al. Dinaciclib, a novel CDK inhibitor, demonstrates encouraging single-agent activity in patients with relapsed multiple myeloma. Blood. 2015 Jan 15;125(3):443-448.
Figure 2A, page 447
Kumar SK, et al. Dinaciclib, a novel CDK inhibitor, demonstrates encouraging single-agent activity in patients with relapsed multiple myeloma. Blood. 2015 Jan 15;125(3):443-448.
Dinaciclib: CDK Inhibitor
Afuresertib (AKT Inhibitor)• ATP-competitive, reversible inhibitor of all 3 AKT kinases• Orally bioavailable• Single-agent activity in heavily pretreated MM patients in FTIH
Voorhees PM et al. Blood. 2013;122. Abstract 283.
Maximum% M Protein Change: Monotherapy FTIH150
50
0
-100
100
-50
-25%
-90%
-50%
100 mg125 mg
FTIH, first time in humans.
Ch
ang
e F
rom
Bas
elin
e (%
)
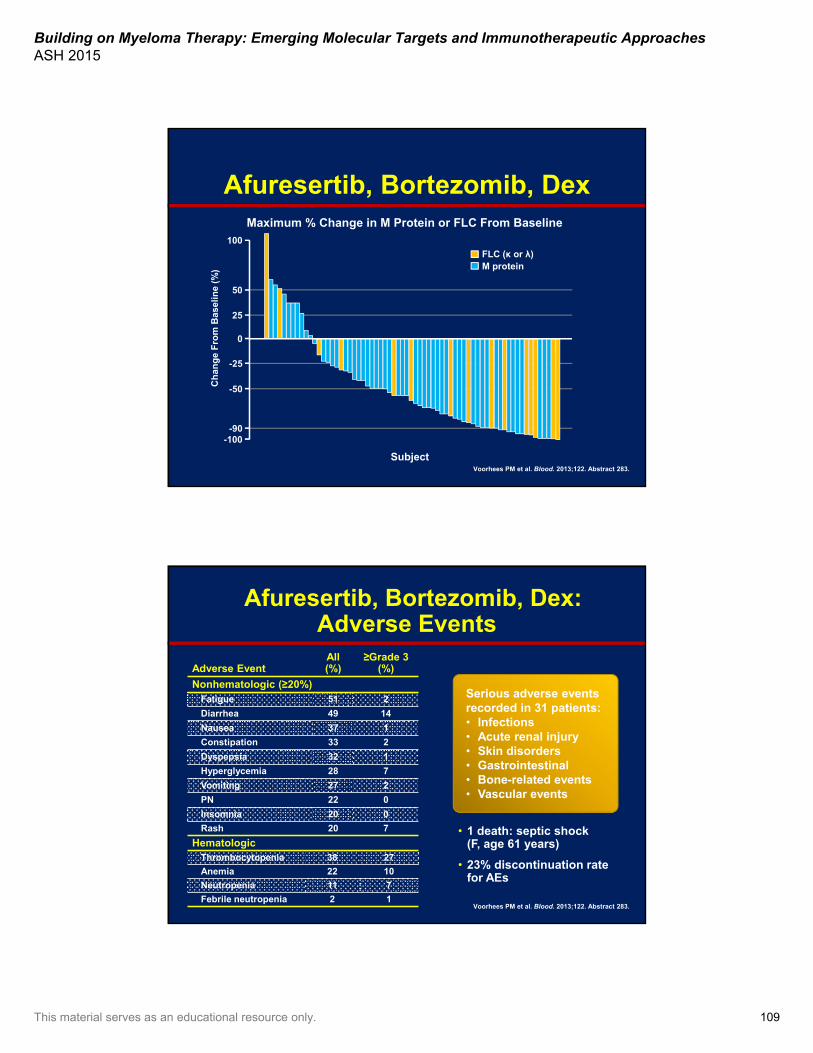
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 109
Afuresertib, Bortezomib, Dex
Voorhees PM et al. Blood. 2013;122. Abstract 283.
100
25
0
-50
50
-25
FLC (κ or λ)M protein
Subject
-100-90
Maximum % Change in M Protein or FLC From BaselineC
han
ge
Fro
m B
asel
ine
(%)
Afuresertib, Bortezomib, Dex: Adverse Events
Adverse Event All (%)
≥Grade 3(%)
Nonhematologic (≥20%)Fatigue 51 2
Diarrhea 49 14
Nausea 37 1
Constipation 33 2
Dyspepsia 32 1
Hyperglycemia 28 7
Vomiting 27 2
PN 22 0
Insomnia 20 0
Rash 20 7
HematologicThrombocytopenia 38 27
Anemia 22 10
Neutropenia 11 7
Febrile neutropenia 2 1
• 1 death: septic shock (F, age 61 years)
• 23% discontinuation rate for AEs
Voorhees PM et al. Blood. 2013;122. Abstract 283.
Serious adverse eventsrecorded in 31 patients:• Infections • Acute renal injury• Skin disorders• Gastrointestinal• Bone-related events• Vascular events
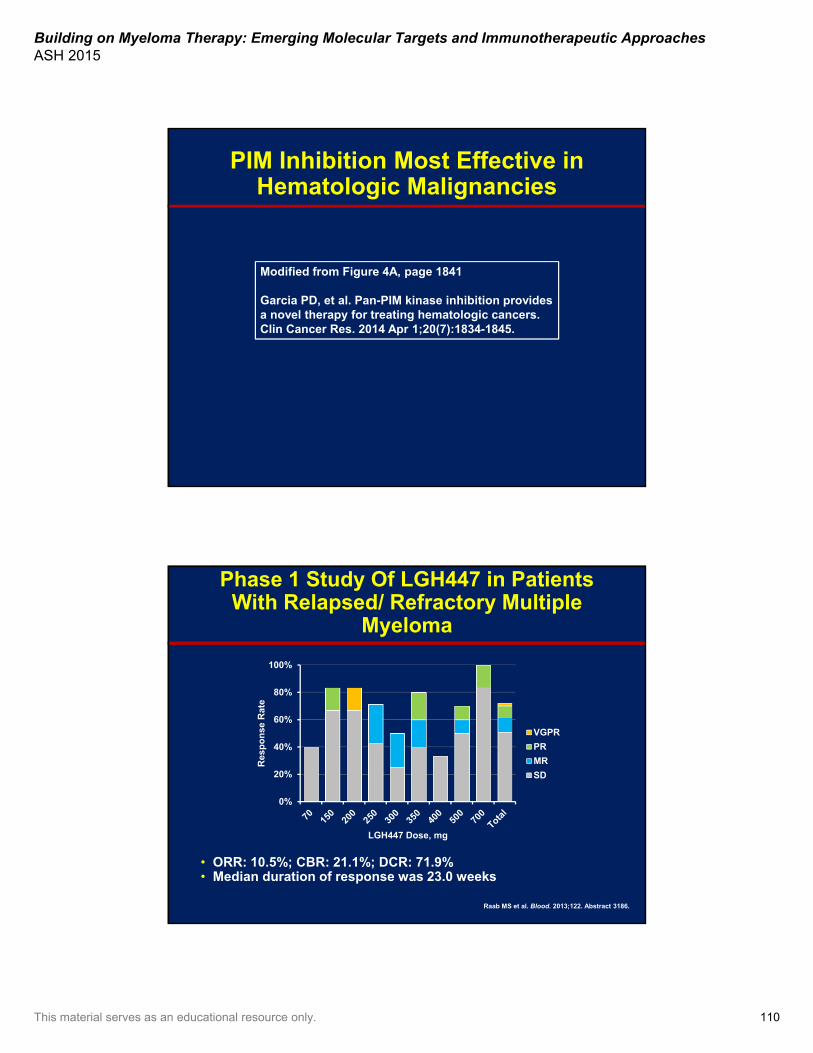
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 110
PIM Inhibition Most Effective in Hematologic Malignancies
Modified from Figure 4A, page 1841
Garcia PD, et al. Pan-PIM kinase inhibition provides a novel therapy for treating hematologic cancers. Clin Cancer Res. 2014 Apr 1;20(7):1834-1845.
Phase 1 Study Of LGH447 in Patients With Relapsed/ Refractory Multiple
Myeloma
• ORR: 10.5%; CBR: 21.1%; DCR: 71.9%• Median duration of response was 23.0 weeks
Raab MS et al. Blood. 2013;122. Abstract 3186.
0%
20%
40%
60%
80%
100%
Res
po
nse
Rat
e
LGH447 Dose, mg
VGPR
PR
MR
SD
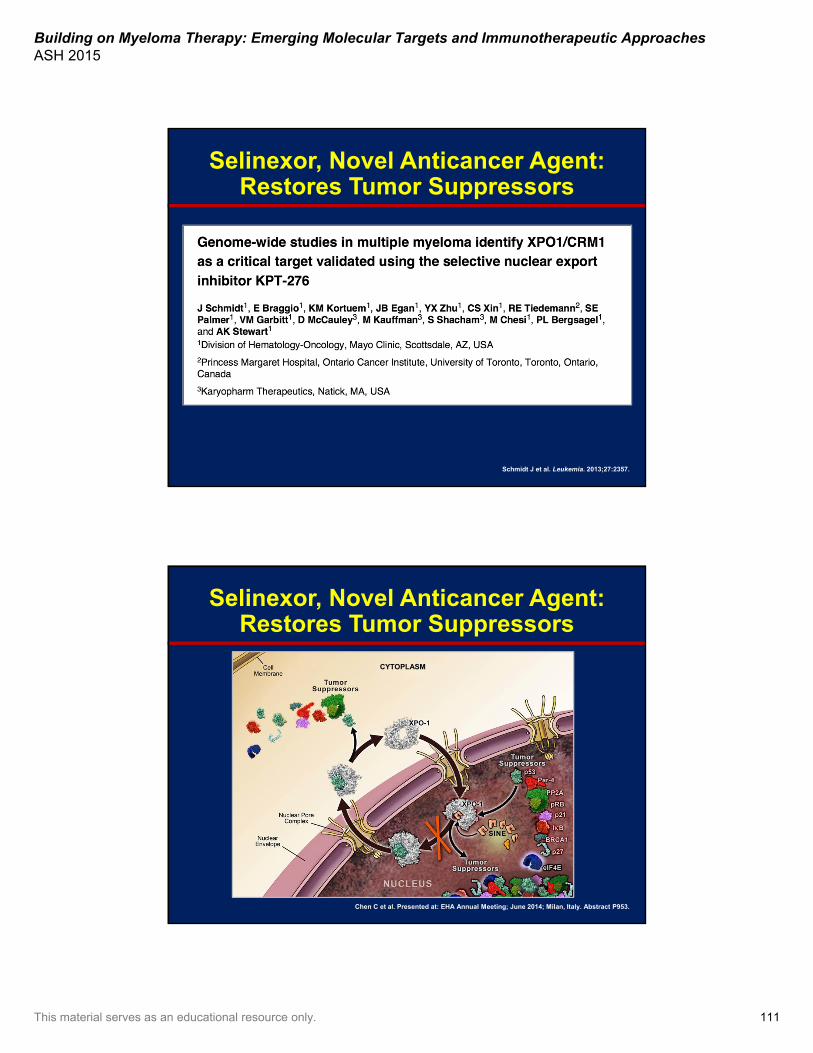
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 111
Selinexor, Novel Anticancer Agent: Restores Tumor Suppressors
Schmidt J et al. Leukemia. 2013;27:2357.
Selinexor, Novel Anticancer Agent: Restores Tumor Suppressors
Chen C et al. Presented at: EHA Annual Meeting; June 2014; Milan, Italy. Abstract P953.
CYTOPLASM
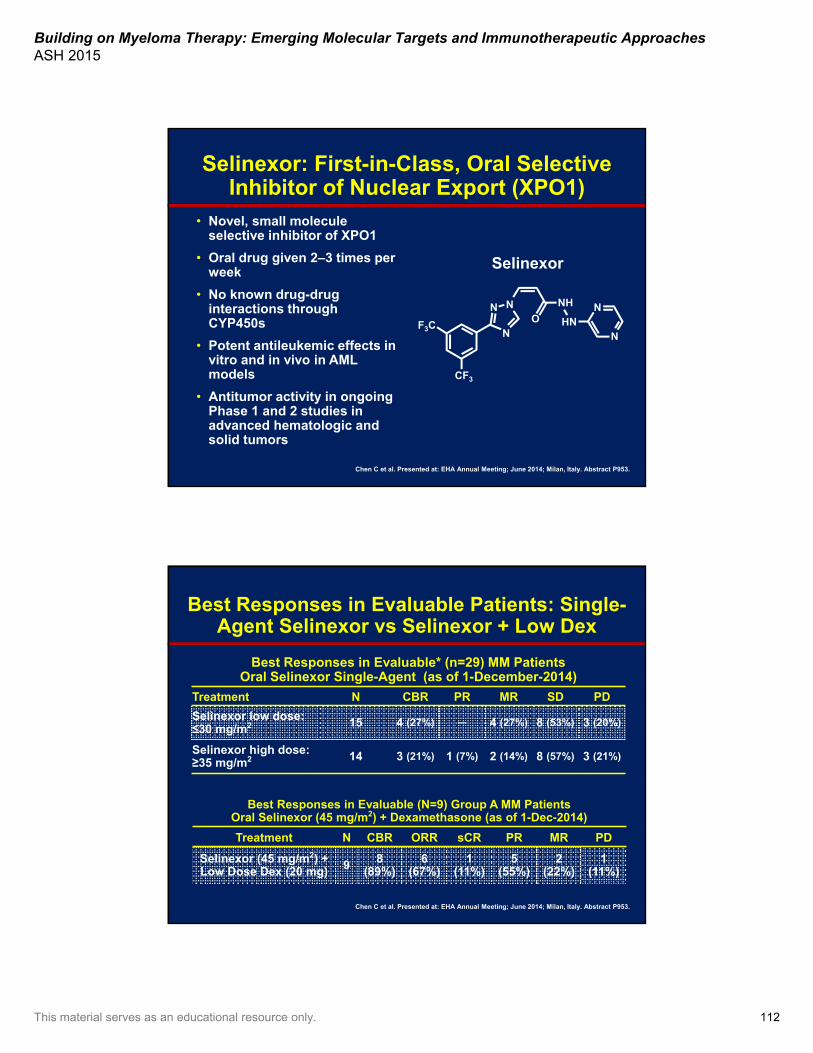
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 112
Selinexor: First-in-Class, Oral Selective Inhibitor of Nuclear Export (XPO1)
• Novel, small molecule selective inhibitor of XPO1
• Oral drug given 2–3 times per week
• No known drug-drug interactions through CYP450s
• Potent antileukemic effects in vitro and in vivo in AML models
• Antitumor activity in ongoing Phase 1 and 2 studies in advanced hematologic and solid tumors
Selinexor
Chen C et al. Presented at: EHA Annual Meeting; June 2014; Milan, Italy. Abstract P953.
CF3
F3C N
N NO
NH
HNN
N
Best Responses in Evaluable Patients: Single-Agent Selinexor vs Selinexor + Low Dex
Best Responses in Evaluable* (n=29) MM PatientsOral Selinexor Single-Agent (as of 1-December-2014)
Treatment N CBR PR MR SD PD
Selinexor low dose: ≤30 mg/m2 15 4 (27%) ─ 4 (27%) 8 (53%) 3 (20%)
Selinexor high dose: ≥35 mg/m2 14 3 (21%) 1 (7%) 2 (14%) 8 (57%) 3 (21%)
Chen C et al. Presented at: EHA Annual Meeting; June 2014; Milan, Italy. Abstract P953.
Best Responses in Evaluable (N=9) Group A MM PatientsOral Selinexor (45 mg/m2) + Dexamethasone (as of 1-Dec-2014)
Treatment N CBR ORR sCR PR MR PD
Selinexor (45 mg/m2) + Low Dose Dex (20 mg) 9 8
(89%)6
(67%)1
(11%)5
(55%)2
(22%)1
(11%)
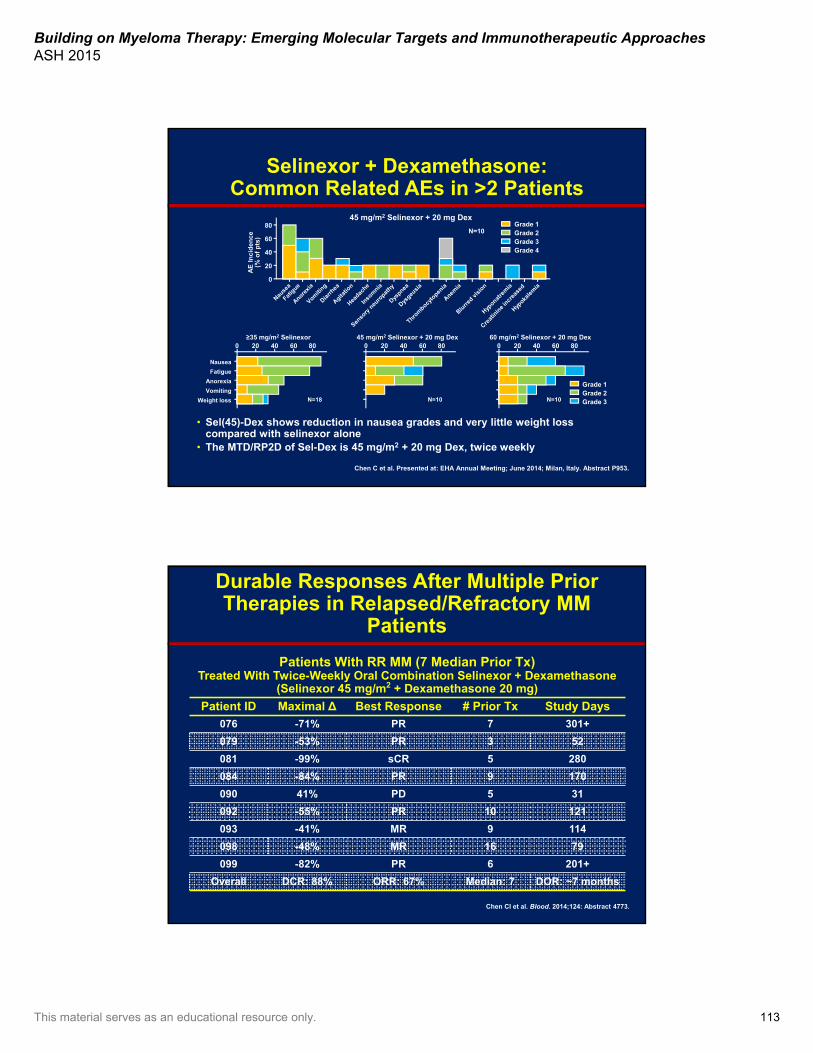
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 113
Selinexor + Dexamethasone: Common Related AEs in >2 Patients
• Sel(45)-Dex shows reduction in nausea grades and very little weight loss compared with selinexor alone
• The MTD/RP2D of Sel-Dex is 45 mg/m2 + 20 mg Dex, twice weekly
Chen C et al. Presented at: EHA Annual Meeting; June 2014; Milan, Italy. Abstract P953.
45 mg/m2 Selinexor + 20 mg Dex80
60
40
20
0
AE
In
cid
ence
(% o
f p
ts)
N=10Grade 1Grade 2Grade 3Grade 4
Grade 1Grade 2Grade 3
806040200
Nausea
Fatigue
Anorexia
Vomiting
Weight loss N=18
≥35 mg/m2 Selinexor806040200
45 mg/m2 Selinexor + 20 mg Dex
N=10
80604020060 mg/m2 Selinexor + 20 mg Dex
N=10
Durable Responses After Multiple Prior Therapies in Relapsed/Refractory MM
Patients
Patients With RR MM (7 Median Prior Tx)Treated With Twice-Weekly Oral Combination Selinexor + Dexamethasone
(Selinexor 45 mg/m2 + Dexamethasone 20 mg)
Patient ID Maximal ∆ Best Response # Prior Tx Study Days
076 -71% PR 7 301+
079 -53% PR 3 52
081 -99% sCR 5 280
084 -84% PR 9 170
090 41% PD 5 31
092 -55% PR 10 121
093 -41% MR 9 114
098 -48% MR 16 79
099 -82% PR 6 201+
Overall DCR: 88% ORR: 67% Median: 7 DOR: ~7 months
Chen CI et al. Blood. 2014;124: Abstract 4773.
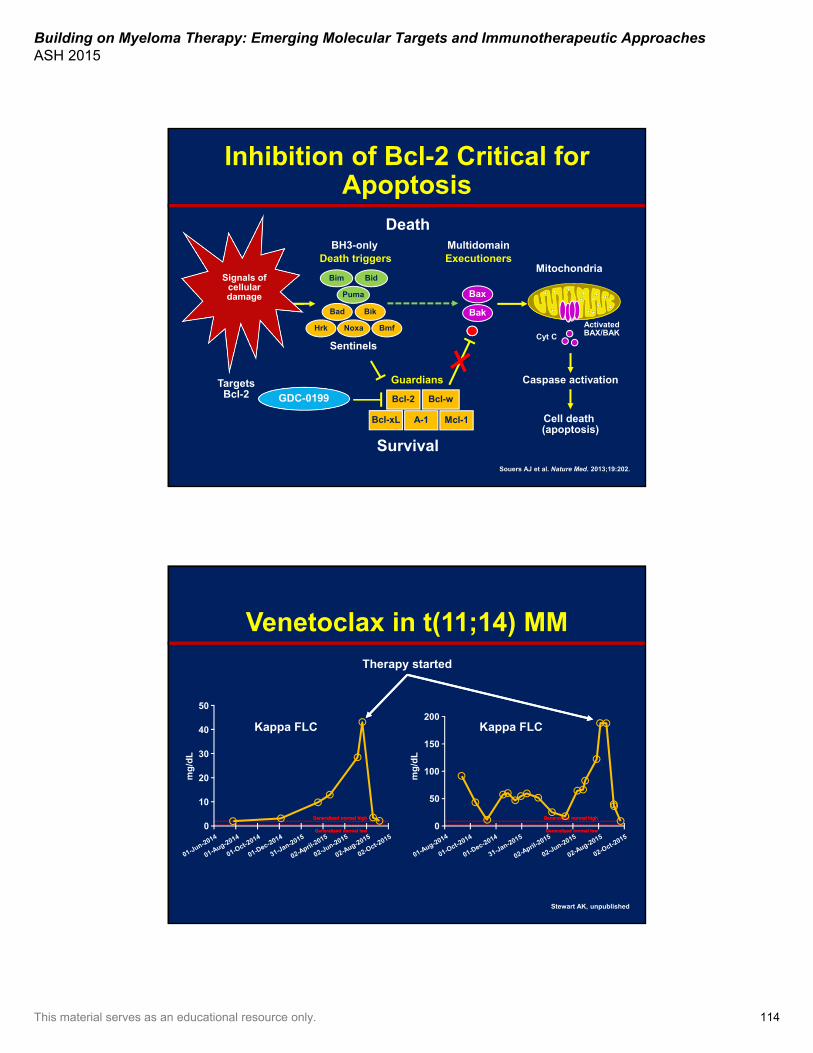
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 114
Cell death (apoptosis)
Inhibition of Bcl-2 Critical for Apoptosis
DeathBH3-only
Bim Bid
Puma
Bak
Bax
MultidomainDeath triggers Executioners
Caspase activation
ActivatedBAX/BAK
Mitochondria
Cyt C
Bik
Bmf
Bad
NoxaHrk
Bcl-2 Bcl-w
Bcl-xL Mcl-1A-1
Survival
Guardians
Sentinels
Signals ofcellulardamage
Targets Bcl-2 GDC-0199
Souers AJ et al. Nature Med. 2013;19:202.
Venetoclax in t(11;14) MMTherapy started
50
40
30
20mg
/dL
0
10
Generalized normal highGeneralized normal high
Generalized normal lowGeneralized normal low
200
150
100
mg
/dL
0
50
Generalized normal highGeneralized normal high
Generalized normal lowGeneralized normal low
Kappa FLC Kappa FLC
Stewart AK, unpublished

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 115
Chimeric Antigen Receptor (CAR) T Cells Against CD19 for Multiple Myeloma
Figure 1A-C, page 1042
Garfall AL, et al. Chimeric antigen receptor T cells against CD19 for multiple myeloma. N Engl J Med. 2015 Sep 10;373(11):1040-1047.
B-Cell Maturation Antigen (BCMA) CAR-T
Remissions of Multiple Myeloma during a First-in-Humans Clinical Trial of T Cells Expressing
an Anti-BCMA Chimeric Antigen Receptor
• BCMA targeted CAR-T cells infused after 3 days of cyclophosphamide and fludarabine
• Highest dose level in 2 patients– severe cytokine release syndrome
• 90-100% clearance of bone marrow plasma cells
Ali SA et al. Presented at: 57th ASH Annual Meeting & Exhibition. Orlando, FL; December 2015. Late-breaking abstract 1.
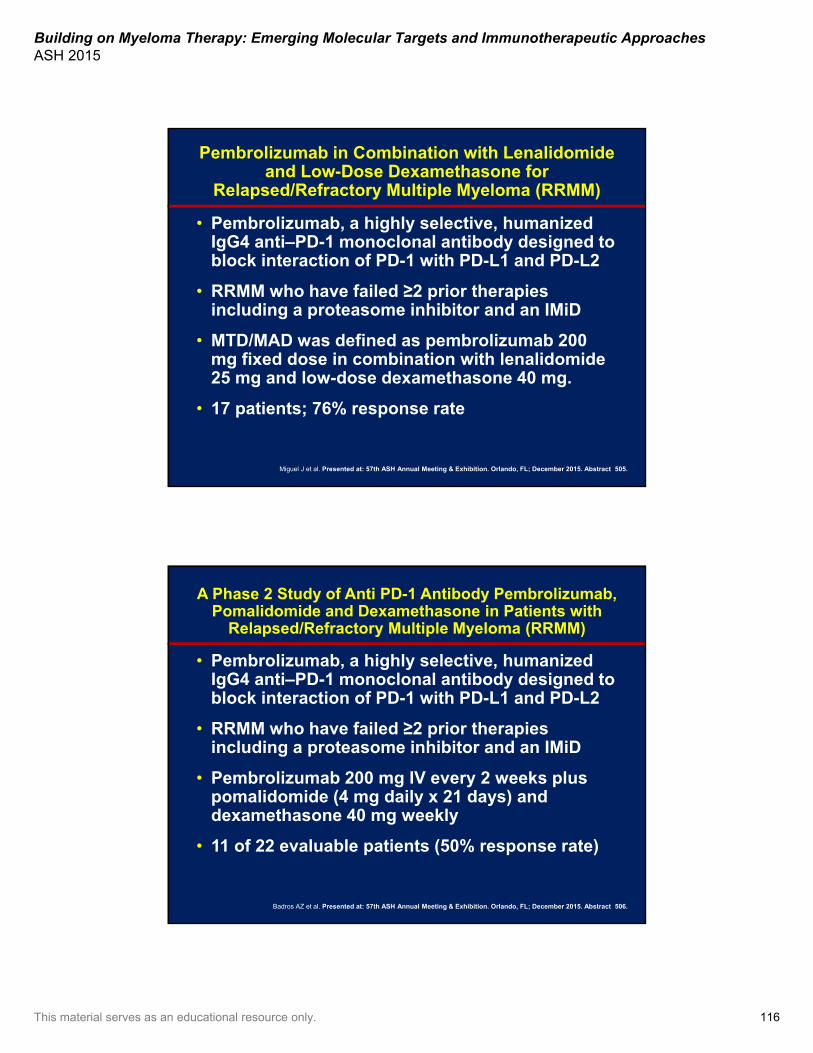
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 116
Pembrolizumab in Combination with Lenalidomideand Low-Dose Dexamethasone for
Relapsed/Refractory Multiple Myeloma (RRMM)
• Pembrolizumab, a highly selective, humanized IgG4 anti–PD-1 monoclonal antibody designed to block interaction of PD-1 with PD-L1 and PD-L2
• RRMM who have failed ≥2 prior therapies including a proteasome inhibitor and an IMiD
• MTD/MAD was defined as pembrolizumab 200 mg fixed dose in combination with lenalidomide25 mg and low-dose dexamethasone 40 mg.
• 17 patients; 76% response rate
Miguel J et al. Presented at: 57th ASH Annual Meeting & Exhibition. Orlando, FL; December 2015. Abstract 505.
A Phase 2 Study of Anti PD-1 Antibody Pembrolizumab, Pomalidomide and Dexamethasone in Patients with
Relapsed/Refractory Multiple Myeloma (RRMM)
• Pembrolizumab, a highly selective, humanized IgG4 anti–PD-1 monoclonal antibody designed to block interaction of PD-1 with PD-L1 and PD-L2
• RRMM who have failed ≥2 prior therapies including a proteasome inhibitor and an IMiD
• Pembrolizumab 200 mg IV every 2 weeks plus pomalidomide (4 mg daily x 21 days) and dexamethasone 40 mg weekly
• 11 of 22 evaluable patients (50% response rate)
Badros AZ et al. Presented at: 57th ASH Annual Meeting & Exhibition. Orlando, FL; December 2015. Abstract 506.
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 117
Summary• Oral proteasome inhibitors seem active; likely
approval(s)
• Monoclonal antibodies: likely to be approved elotuzumab, daratumumab, isatuximab
• Kinase inhibitors dinaciclib (CDK5), afuresertib (AKT), PIM kinase have some single-agent activity and now in combination
• HDACs: ricolinostat too soon to say
• Selinexor, ABT-199 t(11;14) also promising
• Checkpoint inhibitors and CAR-T: too soon to say but potential paradigm shift
Community Case Revisited
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 118
Case Study Part 1• 54-year-old man presents with 6-month history of
lower back pain, increasing fatigue, right rib pain.
• Labs– Normal LDH
– Serum β2 microglobulin 6 mg/dL
• Skeletal survey– Numerous lytic lesions (skull, long bones, right 5th/6th/7th
ribs, pelvis)
• Bone marrow biopsy:– 70% cellularity, 80% kappa-restricted plasma cells
– Cytogenetics normal in 20 metaphases
– FISH positive for translocation (11;14) in 75% cells
Having completed this program, which one of the methodologies do
you plan to use most often?
A. Gene expression profilingB. Conventional cytogeneticsC. FISHD. Gene mutation panelE. More than one methodF. None of the above
?
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 119
Is this patient considered eligible for stem cell transplantation?
A. YesB. NoC. Not sure
?
Having completed this program, which factors do you plan to use to decide whether to consider
aggressive therapy such as stem cell transplantation?
A. Age, comorbidity scoreB. Social support and insurance
coverageC. Response to induction therapyD. Risk profileE. All of the aboveF. I don’t do transplants up front
?
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 120
What would be your recommendation for initial treatment?
A. Melphalan, prednisone, bortezomib (MPV)B. Bortezomib, thalidomide, dexamethasone (VTD)C. Lenalidomide + low-dose dexamethasone (Ld)D. Lenalidomide, bortezomib, dexamethasone
(RVD)E. Cyclophosphamide, bortezomib,
dexamethasone (CyBorD)F. Carfilzomib, lenalidomide, dexamethasone
(KRD)G. Other
?
Having completed this program, will your practice plan to routinely test for minimal residual disease (MRD) following therapy?
A. YesB. NoC. Not sure
?

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 121
Case Study Part 2• Induction chemotherapy: RVd × 4 cycles
• Bone health: bisphosphonates every month
• Best response: VGPR by IMWG criteria
• Relevant events during induction– Grade II peripheral neuropathy after cycle #2
– Increasing lower back pain during cycle #3
Based on the patient’s response to induction therapy, you collect stem cells.
What would you consider next?
A. Continue current regimen
B. Wait to transplant after relapse
C. Proceed to transplant
D. Provide consolidation therapy
?
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 122
Case Study Part 2• Transplant eligible• Restaging post-ASCT: sCR by IMWG criteria
• Patient comes to discuss maintenance
Is now an appropriate time for MRD testing?
A. YesB. NoC. Not sure
?
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 123
Do you recommend maintenance?
A. YesB. NoC. Not sure
?
Would the MRD result affect your decision to use maintenance therapy?
A. YesB. NoC. Not sure
?
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 124
Which maintenance treatment do you recommend?
A. LenalidomideB. BortezomibC. Lenalidomide, bortezomibD. ThalidomideE. PrednisoneF. Clinical trialG. I don’t use maintenance
?
Would your maintenance choice change if the patient had low-risk cytogenetics?
A. YesB. NoC. Not sure
?
Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 125
Case Study Part 3• Patient deferred Len maintenance and prefers
close observation
• Returns 2 years post-ASCT with increasing shoulder pain while working out in the gym, increasing fatigue, and urinary frequency with frothiness
• BM biopsy:– 60% cellularity, 50% kappa-restricted plasma cells– FISH positive for translocation (11;14) in 50%
cells, del17p in 20%
• He is here to discuss treatment options
What would you use for treatment of MM in first relapse?
A. Bortezomib + dexamethasone ±cyclophosphamide
B. Lenalidomide + dexamethasoneC. Pomalidomide + dexamethasoneD. Bortezomib, lenalidomide, and
dexamethasoneE. Carfilzomib + dexamethasoneF. Carfilzomib + lenalidomide + dexamethasoneG. Elotuzumab + lenalidomide + dexamethasoneH. Daratumumab
?

Building on Myeloma Therapy: Emerging Molecular Targets and Immunotherapeutic ApproachesASH 2015
This material serves as an educational resource only. 126
Questions and Answers
Active now:YouKnowIt!—Round 2
and Evaluation