Embed Size (px)
Citation preview
Pediatric Transplantation. 2019;00:e13528. wileyonlinelibrary.com/journal/petr | 1 of 8https://doi.org/10.1111/petr.13528
© 2019 Wiley Periodicals, Inc.
Received:1March2019 | Revised:25April2019 | Accepted:25May2019DOI: 10.1111/petr.13528
O R I G I N A L A R T I C L E
A learning health network for pediatric liver transplantation: Inaugural meeting report from the Starzl Network for Excellence in Pediatric Transplantation
James E. Squires1 | Beth Logan2 | Angela Lorts3 | Henrisa Haskell4 | Kristen Sisaithong4 | Tony Pillari5 | Jonathan Szolna6 | Darcy Dodd7 | Regino P. Gonzalez‐Peralta8 | Evelyn Hsu9 | Beau Kelly10 | Beverly Kosmach‐Park7 | Steven Lobritto11 | Vicky L. Ng12 | Emily Perito13,14 | Sara Rasmussen15 | Rene Romero16 | Eyal Shemesh17 | Hannah Karolak2 | George V. Mazariegos2
1Division of Gastroenterology and Hepatology, UPMC Children’s Hospital of Pittsburgh, Pittsburgh, Pennsylvania2Hillman Center for Pediatric Transplantation, UPMC Children’s Hospital of Pittsburgh, Pittsburgh, Pennsylvania3Department of Pediatrics, Cincinnati Children's Hospital Medical Center, The Heart Institute, University of Cincinnati College of Medicine, Cincinnati, Ohio4Department of Organizational Excellence and Member Quality, United Network for Organ Sharing, Richmond, Virginia5Excelis Consulting Founder, New York, New York6Licensed Social Worker, UPMC Children's Hospital of Pittsburgh, Pittsburgh, Pennsylvania7Department of Transplant Surgery, UPMC Children’s Hospital of Pittsburgh, Pittsburgh, Pennsylvania8PediatricGastroenterology,HepatologyandLiverTransplant,AdventHealthforChildren,Orlando,Florida9Division of Gastroenterology and Hepatology, Seattle Children’s Hospital, Seattle, Washington10DCI Donor Services, Sacramento, California11Division of Gastroenterology and Hepatology, CUIMC – Children’s Hospital of New York, New York, New York12Division of Pediatric Gastroenterology, Hepatology and Nutrition, Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada13Department of Pediatrics, University of California San Francisco, San Francisco, California14Department of Epidemiology and Biostatistics, University of California San Francisco, San Francisco, California15Division of Pediatric Surgery, University of Virginia, Charlottesville, Virginia16DivisionofPediatricGastroenterology,HepatologyandNutrition,Children’sHealthcareofAtlantaandEmoryUniversitySchoolofMedicine,Atlanta,Georgia17Department of Psychiatry and Pediatrics, Icahn School of Medicine at Mount Sinai, New York, New York
Abbreviations:ACTION,AdvancedCardiacTherapiesImprovingOutcomesNetwork;COIIN,CollaborativeInnovationandImprovementNetwork;KDPI,KidneyDonorProfileIndex;LHN, Learning Health Network; LT, Liver transplantation; OPO, Organ Procurement Organizations; OPTN, Organ Procurement and Transplantation Network; PCO, Patient‐centered outcomes; PRECIS, Pragmatic Explanatory Continuum Indicator Summary; QI, Quality improvement; SNEPT, Starzl Network for Excellence in Pediatric Transplantation; SPLIT, Society of PediatricLiverTransplantation;UNOS,UnitedNetworkforOrganSharing;VAD,Ventricularassistdevice.
CorrespondenceGeorge V. Mazariegos, Hillman Center for Pediatric Transplantation, UPMC Children’s HospitalofPittsburgh,4401PennAvenue,FP 6thFloor,6141,Pittsburgh15224,PA.Email: [email protected]
AbstractLearning Health Networks (LHN) improve the well‐being of populations by aligning clinical care specialists, technology experts, patients and patient advocates, and other thoughtleadersforcontinuousimprovementandseamlesscaredelivery.AnovelLHNfocused on pediatric transplantation, the Starzl Network for Excellence in Pediatric Transplantation (SNEPT), convened its inaugural meeting in September 2018. Clinical care team representatives, patients, and patient families/advocates partnered to take
2 of 8 | SQUIRES Et al.
1 | INTRODUC TION
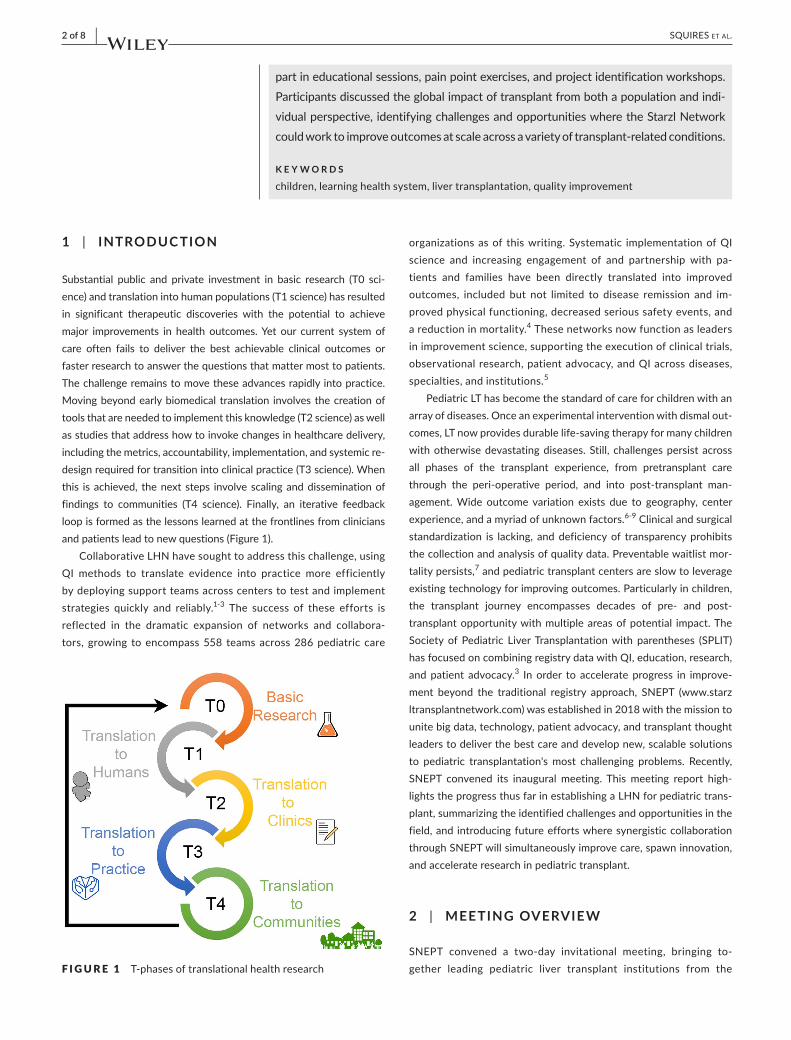
Substantial public and private investment in basic research (T0 sci‐ence) and translation into human populations (T1 science) has resulted in significant therapeutic discoveries with the potential to achieve major improvements in health outcomes. Yet our current system of care often fails to deliver the best achievable clinical outcomes or faster research to answer the questions that matter most to patients. The challenge remains to move these advances rapidly into practice. Moving beyond early biomedical translation involves the creation of tools that are needed to implement this knowledge (T2 science) as well as studies that address how to invoke changes in healthcare delivery, including the metrics, accountability, implementation, and systemic re‐design required for transition into clinical practice (T3 science). When this is achieved, the next steps involve scaling and dissemination of findings to communities (T4 science). Finally, an iterative feedback loop is formed as the lessons learned at the frontlines from clinicians and patients lead to new questions (Figure 1).
Collaborative LHN have sought to address this challenge, using QI methods to translate evidence into practice more efficiently by deploying support teams across centers to test and implement strategies quickly and reliably.1‐3 The success of these efforts is reflected in the dramatic expansion of networks and collabora‐tors, growing to encompass 558 teams across 286 pediatric care
organizations as of this writing. Systematic implementation of QI science and increasing engagement of and partnership with pa‐tients and families have been directly translated into improved outcomes, included but not limited to disease remission and im‐proved physical functioning, decreased serious safety events, and a reduction in mortality.4 These networks now function as leaders in improvement science, supporting the execution of clinical trials, observational research, patient advocacy, and QI across diseases, specialties, and institutions.5
Pediatric LT has become the standard of care for children with an array of diseases. Once an experimental intervention with dismal out‐comes, LT now provides durable life‐saving therapy for many children with otherwise devastating diseases. Still, challenges persist across all phases of the transplant experience, from pretransplant care through the peri‐operative period, and into post‐transplant man‐agement. Wide outcome variation exists due to geography, center experience, and a myriad of unknown factors.6‐9 Clinical and surgical standardization is lacking, and deficiency of transparency prohibits the collection and analysis of quality data. Preventable waitlist mor‐tality persists,7 and pediatric transplant centers are slow to leverage existing technology for improving outcomes. Particularly in children, the transplant journey encompasses decades of pre‐ and post‐transplant opportunity with multiple areas of potential impact. The Society of Pediatric Liver Transplantation with parentheses (SPLIT) has focused on combining registry data with QI, education, research, and patient advocacy.3 In order to accelerate progress in improve‐ment beyond the traditional registry approach, SNEPT (www.starz ltran splan tnetw ork.com) was established in 2018 with the mission to unite big data, technology, patient advocacy, and transplant thought leaders to deliver the best care and develop new, scalable solutions to pediatric transplantation's most challenging problems. Recently, SNEPT convened its inaugural meeting. This meeting report high‐lights the progress thus far in establishing a LHN for pediatric trans‐plant, summarizing the identified challenges and opportunities in the field, and introducing future efforts where synergistic collaboration through SNEPT will simultaneously improve care, spawn innovation, and accelerate research in pediatric transplant.
2 | MEETING OVERVIE W
SNEPT convened a two‐day invitational meeting, bringing to‐gether leading pediatric liver transplant institutions from the
part in educational sessions, pain point exercises, and project identification workshops. Participants discussed the global impact of transplant from both a population and indi‐vidual perspective, identifying challenges and opportunities where the Starzl Network could work to improve outcomes at scale across a variety of transplant‐related conditions.
K E Y W O R D S
children, learning health system, liver transplantation, quality improvement
F I G U R E 1 T‐phases of translational health research

| 3 of 8SQUIRES Et al.
SPLIT consortium, academic and transplant organizations, tech‐nology innovators, and patient voices to identify fundamental challenges and future opportunities able to be addressed by a pediatric liver transplant‐specific LHN. The meeting was planned by a seven‐member committee and ultimately engaged 59 rep‐resentatives from multifaceted transplant‐related domains over twodaysinAtlanta,Georgia,onSeptember14‐15,2018.(Table1)Premeeting surveys were circulated to both center representa‐tives and patient/family representatives to identify common
themes and challenges. Following introductions, a LHN primer education series and input on improvement exercises, patient and family representatives undertook independent exercises aimed at identifying patient‐driven targets for the LHN. Separately, the other network partners, collaborators, and data management ad‐visors discussed mechanisms for infrastructure establishment. After re‐convening,attendeesparticipated inexercises focusingon the four phases of transplant: (a) pretransplant, (b) peri‐opera‐tive, (c) early post‐transplant (0‐3 years) and (d) late post‐trans‐plant (>3 years). Exercise objectives were (a) to categorize provider‐ and family/patient‐specific pain points in pediatric liver transplant and (b) to facilitate the identification and prioritization of future SNEPT project(s). Following the meeting, the planning committee compiled, refined, and organized the results of each exercise. Projects were scored by SNEPT participants using an ad‐aptation of the PRECIS tool.10
3 | THE CHALLENGES AND OPPORTUNITIES
3.1 | A LHN experience
In the spirit of sharing and learning from others, SNEPT sought guidance from other well‐functioning learning networks with simi‐lar focus. ACTION is focused on improving outcomes in patients with end‐stage heart failure. This network is currently focused on thecareandpatient/familyexperiencearoundVADsupportofpa‐tients awaiting a suitable organ. The ACTION network had under‐gone a similar exercise as the inaugural SNEPT meeting and agreed on a common “burning platform” on which to focus initial efforts. AllresourceswereinitiallyallocatedtoreducingthestrokerateinchildrensupportedwithVADs.Examplesofchangesintherapythatspread quickly throughout the network were reviewed. These exam‐ples clarified the differences between dissemination via a learning networkvstraditionalacademicmethods.Anexampleofhowfasta change can spread is evident in the anticoagulation interventions that have occurred across the 25 ACTION centers. Participants’ agreement upon anticoagulation protocol adaptations has ena‐bled the stroke rates in children supported onVADs to decreasedramatically among participating centers (Personal Communication Angela Lorts). ACTION also shared the importance of inclusivity and dispersed leadership throughout the network in order to accelerate QI work.
3.2 | Lessons from transplant QI and relational coordination expertise
Projects that incorporate the broad concepts of collaboration, innova‐tion, and improvement within the field of transplant have been shown to be successful, with some work utilizing the theory of relational coor‐dination to achieve results. Relational coordination is a mutually rein‐forcing process of communicating and relating for the purpose of task integration.11 It is comprised of three relational dimensions—shared
TA B L E 1 SNEPT meeting participants
Center representative Milken institute
UPMC Children's Hospital of Pittsburgh
TonyPillari(Advisor)
George Mazariegos MD LHS consultant
KyleSoltysMD AngelaLortsMD
James E Squires MD,MS SPLIT
Jonathan Szolna MSW BeauKellyMD
Beth Logan PhD Steve Lobritto MD
Molly Vogel Data management advisor
Douglas Landsittel Emmes
Darcy Dodd RavinderAnand
BeverlyKosmach‐Park,ANP,FAAN
Jeff Mitchell
AsadZaman Transplant QI and relational coordination expertise
AlanAbraham KristenSisaithongMA
Seattle Children's Hospital Henrisa Haskell
Simon Horslen MD Sarah Taranto
Evelyn Hsu MD Michelle Rabold
University of Virginia Industry
Sara Rasmussen MD, PhD Health tech solutions
SickKids(Toronto) Eric Pahl PhD
Vicky Ng MD Matthew Miller
Blossom Dharmaraj Family/patient representatives: city (number of participants)
Children'sHealthcareofAtlanta Pittsburgh (8)
Rene Romero MD New York City (4)
Nitika Gupta MD Atlanta(4)
University of California, San Francisco
Toronto (1)
Emily Perito MD Chicago (1)
Sue Rhee MD New Orleans (1)
Mt. Sinai NY KansasCity(1)
Eyal Shemesh MD Cincinnati (1)
John Bucuvalas MD Seattle (1)
Megan Czurda
AdventHealthforChildren
Regino Gonzalez‐Peralta MD
Barry Friedman

4 of 8 | SQUIRES Et al.
goals, shared knowledge, and mutual respect—and four communica‐tion dimensions—frequent, timely, accurate, and problem solving—that together drive the effective coordination of work.11 In an effort to educate the Network on how concepts of improvement and relational coordination can be used in the field of transplant, expert representa‐tives were invited to speak about their experiences.
Members of the Department of Organizational Excellence and Member Quality at the UNOS presented their work. Supported by the OPTN, the group participated in a 3‐year collaborative im‐provement project to increase the utilization of moderate‐to‐high (50%‐100%) KDPI kidneys by focusing on process improvementsthat drive higher utilization.12 The objectives of the COIIN were to use a trusted collaborative improvement framework to engage transplant hospitals and their partner OPOs in discovering effective practicestoutilizemoremoderate‐to‐highKDPIkidneys.
Recently published, the preliminary findings show an increase intransplantrateandutilizationofmoderate‐to‐highKDPIkidneyswas achieved in many participating organizations following the de‐velopment of a change package of key interventions for three dis‐tinct areas: waitlist management, organ‐offer acceptance, and care coordination. These COIIN project results suggest that an improve‐ment approach that supports collaboration can be effective in the transplant community.12
3.3 | SNEPT meeting work process
3.3.1 | Precirculated surveys
In an effort to organize the network as “actor‐oriented,” that is ar‐ranging itself to avoid a more hierarchical structure and to promote equal distribution of resources and efforts across the people, or‐ganizations, databases, and registries that comprise the network,13 premeeting surveys were completed in order to begin the process of self‐organization and enable identification of problems that are im‐portant to the participants who make up the network.
Center representatives: In addition to the identification of per‐sonnel and technology resources (electronic medical record, in‐stitutional transplant‐specific database, etc) available at each institution, center representatives were asked to identify three key areas that could be addressed through participation in SNEPT. A summary of the center representative responses is shown inFigure 2. Examples of technology innovations included pathology digitalization, the ability to digitally record and distribute both sur‐gical (biliary anastomosis, technical variant graft preparation, etc) and process (evaluation, consent, education, etc) content, and the use of novel tools to more accurately capture a patients’ exposure to immunosuppression. Universal among all participating centers was the need to identify variability in practice, to standardize best practices, and to leverage SNEPT as a patient and family transplant‐specific resource.
Patient/family representatives: Prior to the meeting, patient and family representatives completed a separate survey containing a range of open‐ended questions designed to elicit their passion and
priorities related to LT care. Responses generally fell into four main categories: (a) medication, (b) transition to adult providers, (c) psy‐chosocial support, and (d) general aspects of care (eg, time spent with providers, communication with providers, and patient engagement in care). Participants were asked to endorse which aspects of care they felt most strongly a LHN such as SNEPT could problem‐solve. Patients and families overwhelmingly endorsed psychosocial support as the area most in need of project development, with 100% of re‐spondents (n = 11) endorsing post‐transplant psychological function‐ing as a pain point, 92% endorsing family and sibling support as needs, and 62% citing access to resources as a project target. Transition to adult providers (72% endorsed) and patient self‐advocacy (62%) were also identified as areas of need. In addition, respondents were asked to identify needs unique to the four phases of transplant. Patients and families most frequently reported a desire to be connected with other patients and families who have experienced LT, citing potential ben‐efits of social support, mentorship, and linkage to helpful resources as the drivers for project development in this area. Respondents also commonly reported emotional support for patients and families as a need during all phases of LT. Survey results were further reviewed during the patient and family breakout session.
3.3.2 | Summary of patient and family breakout session
Patients and families attended a half‐day breakout session. The aim was to allow patients and families an opportunity to further discuss premeeting survey results and propose project ideas for the LHN that would directly impact patient and family care. The results of the premeeting survey were reviewed. Participants were then divided into working groups based on the transplant phase about which they
F I G U R E 2 Premeeting survey center responses
| 5 of 8SQUIRES Et al.
self‐identified as being most passionate about creating change. Group members were asked to propose 1‐2 potential projects to reflect the identified needs within each phase of LT. Each small group then shared their project ideas with the larger patient and family group to solicit feedback and further refine their proposals. The proposed projects were summarized in real time to create a patient and family work prod‐uct which was presented to the LHN the following day.
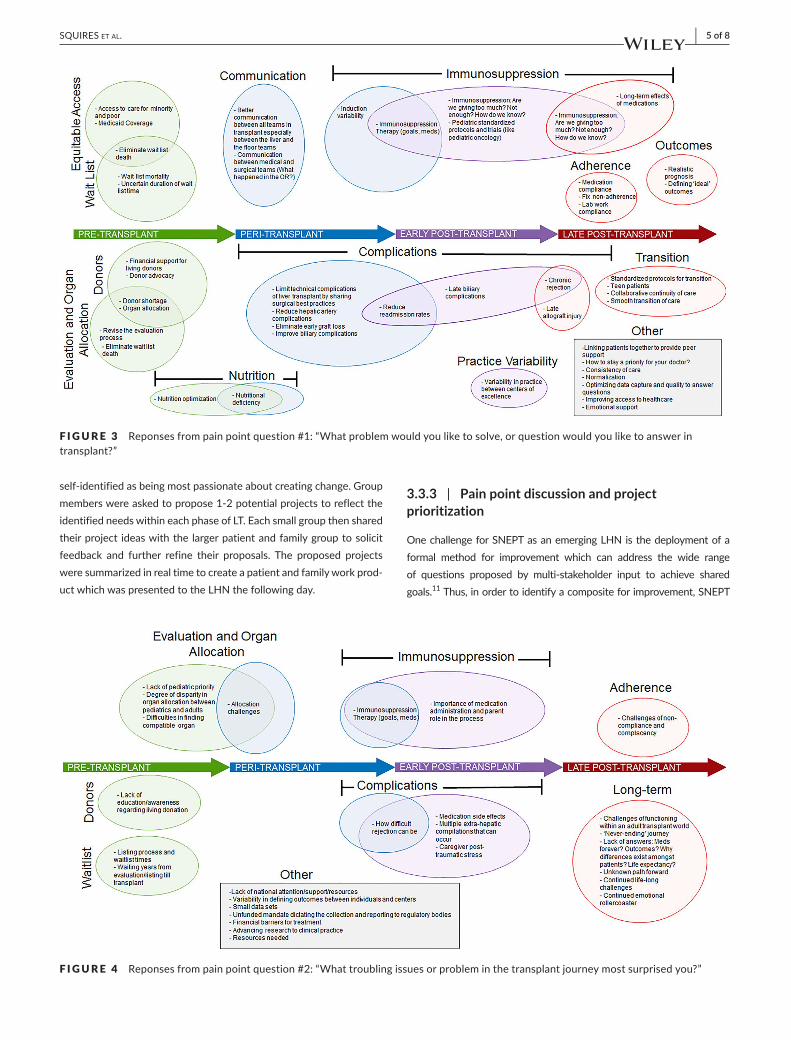
3.3.3 | Pain point discussion and project prioritization
One challenge for SNEPT as an emerging LHN is the deployment of a formal method for improvement which can address the wide range of questions proposed by multi‐stakeholder input to achieve shared goals.11 Thus, in order to identify a composite for improvement, SNEPT
F I G U R E 3 Reponses from pain point question #1: “What problem would you like to solve, or question would you like to answer in transplant?”
F I G U R E 4 Reponses from pain point question #2: “What troubling issues or problem in the transplant journey most surprised you?”
6 of 8 | SQUIRES Et al.
participants were asked to answer two critical questions related to the transplant journey: (a) “What problem would you like to solve, or question would you like to answer in transplant?” and (b) “What troubling issues or probleminthetransplantjourneymostsurprisedyou?”Answerstothesequestions were initially written on index cards by each participant, col‐lected, and then openly organized under “General Themes” and arranged along the transplant journey. (Figures 3 and 4) Based on these pain point
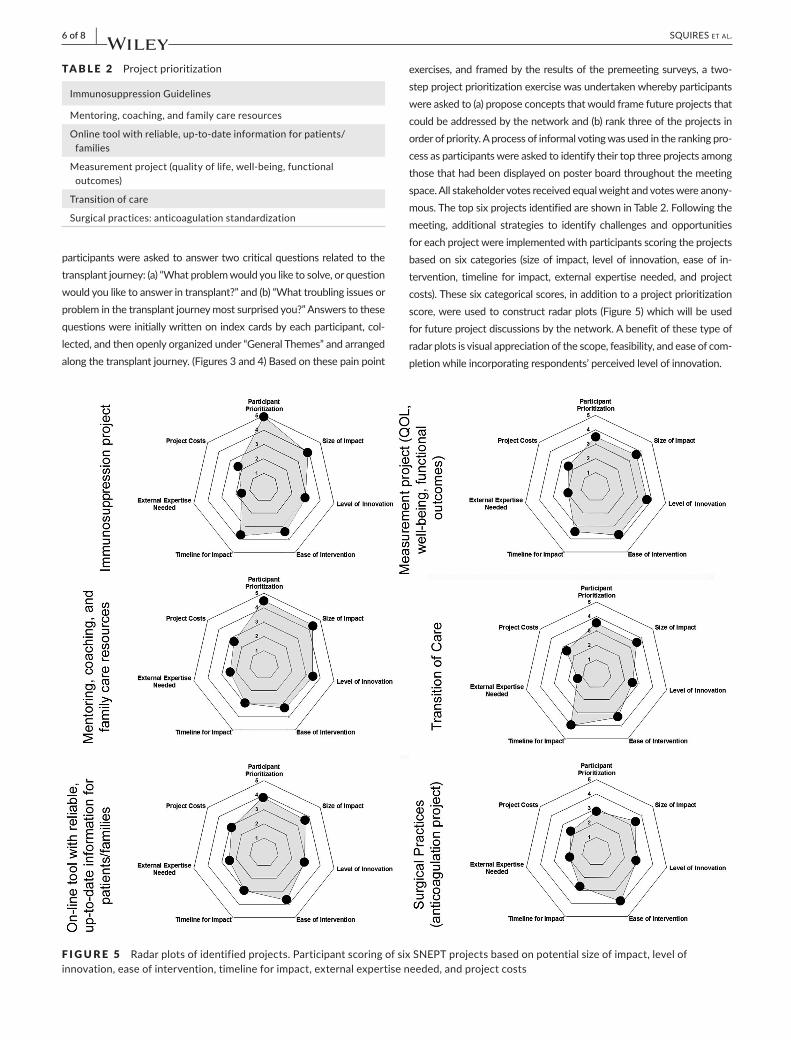
exercises, and framed by the results of the premeeting surveys, a two‐step project prioritization exercise was undertaken whereby participants were asked to (a) propose concepts that would frame future projects that could be addressed by the network and (b) rank three of the projects in orderofpriority.Aprocessofinformalvotingwasusedintherankingpro‐cess as participants were asked to identify their top three projects among those that had been displayed on poster board throughout the meeting space.Allstakeholdervotesreceivedequalweightandvoteswereanony‐mous. The top six projects identified are shown in Table 2. Following the meeting, additional strategies to identify challenges and opportunities for each project were implemented with participants scoring the projects based on six categories (size of impact, level of innovation, ease of in‐tervention, timeline for impact, external expertise needed, and project costs). These six categorical scores, in addition to a project prioritization score, were used to construct radar plots (Figure 5) which will be used forfutureprojectdiscussionsbythenetwork.Abenefitofthesetypeofradar plots is visual appreciation of the scope, feasibility, and ease of com‐pletion while incorporating respondents’ perceived level of innovation.
TA B L E 2 Project prioritization
Immunosuppression Guidelines
Mentoring, coaching, and family care resources
Online tool with reliable, up‐to‐date information for patients/families
Measurement project (quality of life, well‐being, functional outcomes)
Transition of care
Surgical practices: anticoagulation standardization
F I G U R E 5 Radar plots of identified projects. Participant scoring of six SNEPT projects based on potential size of impact, level of innovation, ease of intervention, timeline for impact, external expertise needed, and project costs

| 7 of 8SQUIRES Et al.
4 | SUMMARY, CHALLENGES, AND FUTURE DIREC TIONS
Improvements in pediatric transplantation quality and outcome pre‐sent challenges not easily addressed by traditional research efforts. Broad areas of interest for future improvement identified by meet‐ing participants included (a) variability in care, (b) educational and social networking tools, (c) quality of life, and (d) transition of care. The solicitation and incorporation of expertise and input from pa‐tients and families to identify important and impactful interventions thatwillenableidealPCOsarecritical.Atthismeeting,stakeholdersacross the transplant community, QI thought leaders, and LHN ex‐perts discussed how a novel, LHN approach may be used to enhance future efforts.
We recognize that a crucial component of continued growth for the network will be demonstrating generalizability and value in a resource‐constrained environment. The Starzl Network addresses these issues by focusing on synergy and collaboration and utilizing sharing of tools and expertise across the transplant community more seamlesslythanhasbeendonebefore.Also,currentworkisbeingdone to ultimately reduce unnecessary or duplicative data entry re‐lated to improvement processes and transplant follow‐up.
Finally, a critical component of SNEPT is the establishment of community‐healthcare team reciprocity. Historically, there has not been a strong, collective patient/family voice in designing or prior‐itizing efforts in pediatric transplant. Moving forward, we intend to directly address this by leveraging SNEPT efforts to continually increase engagement and partnership with families and providers to identify key gaps in knowledge, strategize for improvement, and categorize meaningful outcome metrics to measure success. Through structured engagement, development, and co‐creation, we anticipate the establishment of a supportive infrastructure for PCO research in pediatric transplant. We envision a collaborative partnership (patients, providers, and stakeholders) functioning within a system designed to support and adjust based on relational interactions.Additionalavenuesofpursuitwillalsolooktoexpandexisting relationships with digital health leaders and experts in patient‐centered research to accelerate learning and increase ef‐fectiveness and generalizability. Ultimately, we hope to (a) ingrain critical skills, shared priorities, and feasible plans for authentic PCO research within the SNEPT community, (b) shift from tradi‐tional investigator‐driven study to a patient and family‐centered approach, and (c) improve outcomes and quality of life for pediat‐ric transplant patients.
ACKNOWLEDG MENTS
The Starzl Network gratefully acknowledges the Citrone Family and the Citrone 33 Foundation for the transformative gift that estab‐lished this network and the passion of Joy Starzl who carries on the vision of Dr Thomas Starzl to “save the children.” The Starzl Network is thankful for the question sourcing ideas stimulated by Dr John S. Maier, University of Pittsburgh
AUTHOR CONTRIBUTIONS
James E Squires: Conceived and designed the analysis, collected the data, contributed data or analysis tools, performed the analysis, wrote the paper; Beth Logan: Conceived and designed the analysis and col‐lected thedata;AngelaLorts:Substantialcontributions toconceptionand design, acquisition of data, or analysis and interpretation of data, and final approval of the version to be published; Henrisa Haskell: Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, and final approval of the version to bepublished;Kristen Sisaithong: Substantial contributions to con‐ception and design, acquisition of data, or analysis and interpretation of data, and final approval of the version to be published; Tony Pillari: Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, and final approval of the version to be published; Jonathan Szolna: Conceived and designed the analysis and collected the data; Darcy Dodd: Contributed data or analysis tools; Regino P. Gonzalez‐Peralta: Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, and final approval of the version to be published; Evelyn Hsu: Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, and final approval of the version to be pub‐lished;BeauKelly:Substantialcontributionstoconceptionanddesign,acquisition of data, or analysis and interpretation of data, and final ap‐provaloftheversiontobepublished;BeverlyKosmach‐Park:Substantialcontributions to conception and design, acquisition of data, or analysis and interpretation of data, and final approval of the version to be pub‐lished; Steven Lobritto: Substantial contributions to conception and de‐sign, acquisition of data, or analysis and interpretation of data, and final approval of the version to be published; Vicky L Ng: Substantial contri‐butions to conception and design, acquisition of data, or analysis and interpretation of data, and final approval of the version to be published; Emily Perito: Substantial contributions to conception and design, acqui‐sition of data, or analysis and interpretation of data, and final approval of the version to be published; Sara Rasmussen: Substantial contributions to conception and design, acquisition of data, or analysis and interpre‐tation of data, and final approval of the version to be published; Rene Romero: Substantial contributions to conception and design, acquisi‐tion of data, or analysis and interpretation of data, and final approval of the version to be published; Eyal Shemesh: Substantial contributions to conception and design, acquisition of data, or analysis and interpreta‐tion of data, and final approval of the version to be published; Hannah Karolak:Draftingthearticleorrevisingitcriticallyforimportantintellec‐tual content, and final approval of the version to be published; George V. Mazariegos: Conceived and designed the analysis, collected the data, contributed data or analysis tools, performed the analysis, edited the paper, and final approval of the version to be published.
ORCID
James E. Squires https://orcid.org/0000‐0001‐6979‐8987
Angela Lorts https://orcid.org/0000‐0003‐1447‐5456
Evelyn Hsu https://orcid.org/0000‐0003‐4359‐7102

8 of 8 | SQUIRES Et al.
Steven Lobritto https://orcid.org/0000‐0003‐1482‐1128
Vicky L. Ng https://orcid.org/0000‐0002‐9998‐5692
Emily Perito https://orcid.org/0000‐0002‐2911‐9684
Rene Romero https://orcid.org/0000‐0002‐1566‐2280
Eyal Shemesh https://orcid.org/0000‐0003‐2508‐3423
George V. Mazariegos https://orcid.org/0000‐0002‐2624‐8632
R E FE R E N C E S
1. ClancyCM,MargolisPA,MillerM.Collaborativenetworksforbothimprovement and research. Pediatrics. 2013;131(Suppl 4):S210‐214.
2. Morrow WR, Naftel D, Chinnock R, et al. Outcome of listing for heart transplantation in infants younger than six months: predictors of death and interval to transplantation. The Pediatric Heart Transplantation Study Group. J Heart Lung Transplant. 1997;16:1255‐1266.
3. KellyB,SquiresJE,FeingoldB,HooperDK,MazariegosGV.Qualityinitiatives in pediatric transplantation. Curr Opin Organ Transplant. 2019;24:64‐72.
4. CincinnatiChildren'sHospitalMedicalCenter:JamesM.AndersonCenter for Health Systems Excellence. In. https ://www.cinci nnati child rens.org/servi ce/j/ander son‐cente r/learn ing‐netwo rks/active‐emerging.
5. Forrest CB, Margolis P, Seid M, Colletti RB. PEDSnet: how a prototype pediatric learning health system is being expanded into a national network. Health Aff (Millwood). 2014;33:1171‐1177.
6. Hsu EK, Shaffer M, Bradford M, Mayer‐Hamblett N, Horslen S.Heterogeneity and disparities in the use of exception scores in pediatric liver allocation. Am J Transplant. 2015;15:436‐444.
7. Hsu EK, ShafferML, Gao L, et al. Analysis of liver offers to pe‐diatric candidates on the transplant wait list. Gastroenterology. 2017;153:988‐995.
8. MinnemanJA,GrijalvaJL,LaQuagliaMJ,KimHB,RangelSJ,VakiliK.Variationinresourceutilizationin livertransplantationatfree‐standing children's hospitals. Pediatr Transplant. 2016;20:921‐925.
9. Cramm SL,Waits SA, EnglesbeMJ, et al. Failure to rescue as aquality improvement approach in transplantation: a first effort to evaluate this tool in pediatric liver transplantation. Transplantation. 2016;100:801‐807.
10. ThorpeKE,ZwarensteinM,OxmanAD,etal.Apragmatic‐explan‐atory continuum indicator summary (PRECIS): a tool to help trial designers. J Clin Epidemiol. 2009;62:464‐475.
11. Friedman C, Rubin J, Brown J, et al. Toward a science of learning systems: a research agenda for the high‐functioning learning health system. J Am Med Inform Assoc. 2015;22:43‐50.
12. Tosoc‐Haskell H, Sisaithong K, Carrico R. The collaborative im‐provement and innovation network project to drive quality im‐provement. Curr Opin Organ Transplant. 2019;24:73‐81.
13. BrittoMT,FullerSC,KaplanHC,etal.Usinganetworkorganisa‐tional architecture to support the development of learning health‐care systems. BMJ Qual Saf. 2018;27:937‐946.
How to cite this article:SquiresJE,LoganB,LortsA,etal.Alearning health network for pediatric liver transplantation: Inaugural meeting report from the Starzl Network for Excellence in Pediatric Transplantation. Pediatr Transplant. 2019;00:e13528. https ://doi.org/10.1111/petr.13528