Embed Size (px)
Citation preview

86 Taiwanese Journal of Orthodontics. 2019, Vol. 31. No. 210.30036/TJO.201906_31(2).0003
Case Report
This case report describes the management of an adult patient presenting with a skeletal Class III
malocclusion, mandibular protrusion, upper incisor proclination and mandibular arch spacing by a modified
surgery-first approach. A 26-year-old man had skeletal Class III and dental Class III malocclusion with
concave facial profile, midface deficiency and mandibular prognathism with chin deviation to left. His dental
manifestation presented anterior crossbite, upper incisors proclination and spacing in his mandibular arch.
Treatment was performed with a modified surgery-first approach, which included a short presurgical alignment
phase. In the maxilla, the significant maxillary crowding was relieved by 14 and 24 extractions while partially
retracting the maxillary incisors to reduce the incisal proclination. Then, the upper incisors inclination was
furtherly corrected more by a 2-pieces LeFort I osteotomy and closure of the 14, 24 residual dental space
during surgery. In the mandible, the lower dental spacing was caused by general tooth size/ jaw bone
discrepancy with relative upright incisal inclination. The presurgical preparation included consolidation the
dental space distal to the bilateral mandibular canines. The bilateral sagittal split osteotomies were conducted
for mandible setback and asymmetry correction. Additionally, the subapical osteotomy with Köle procedure
was applied to close the dental space in the mandibular arch while keeping the anterior teeth in relative
normal inclination. The excessive chin prominence caused by the Köle procedure was reduced by reduction
genioplasty and surface contouring. Post-operative orthodontic treatment included overbite control and
detailing of the occlusion. After treatment, the maxillary incisors proclination was corrected and all the dental
spaces were closed. Patient’s profile was dramatically improved with well teeth alignment, angulation and
interdigitation. The 2-pieces LeFort I and Köle osteotomy are the surgical procedures to address the correction
in the dentoalveolar portion for efficiently control the inclination of the anterior teeth. Moreover, it also provides
benefits for patients who require large amount of jaw setback with minimal effect at the posterior airway space.
The treatment goals of the dentoalveolar portion and facial proportion should be contemplated for the staged
procedures to improve the efficiency and effectiveness of the treatment outcome. (Taiwanese Journal of Orthodontics. 31(2): 86-94, 2019)
Keywords: orthognathic surgery; modified surgery-first approach; skeletal Class III malocclusion; mandibular prognathism; segmental osteotomy.
A Modified Surgery-firSt ApproAch for MAndibulAr prognAthiSM with proclined MAxillAry inciSor And MAndibulAr SpAcing
Jutharath Chanruangvanich,1,2
Ellen Wen-Ching Ko,1,2,3
Ying-An Chen3,4
1Department of Craniofacial Orthodontics, Chang Gung Memorial Hospital, Taipei, Taiwan
2Graduate Institute of Dental and Craniofacial science, Chang Gung University, Taoyuan, Taiwan
3Craniofacial Research Center, Chang Gung University, Taoyuan, Taiwan
4Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, Taoyuan, Taiwan
Received: February 26, 2019 Accepted: March 5, 2019Reprints and correspondence to: Dr. Ellen Wen-Ching Ko, Department of Craniofacial Orthodontics, Chang Gung Memorial Hospital, Taipei, Taiwan. 6F, 199, Tung Hwa North Road, Taipei 105, Taiwan Tel: +886-2-27135211 ext.3533 Fax: +886-2-25148246 E-mail: [email protected]

87Taiwanese Journal of Orthodontics. 2019, Vol. 31. No. 210.30036/TJO.201906_31(2).0003
INTRODUCTION
A Class I I I ske le ta l pa t t e rn cou ld l ead to
malocclusion and disharmony facial profile. From the
systematic review and meta-analysis of Hardy et al. in
2012, the Angle Class III malocclusion had been found
in Southeast Asian population with the highest rate of
15.80% compare to other population.1 As well as the
study from Soha et al. in 2005, the relationships of Class
III incisor in Asian male army were 22.4% and Class III
molar relationship were 24.2 % at right side and 21.2%
at left side.2 Tang also reported the prevalence of Class
III malocclusion which was 14.8% in male dental student
in Hong Kong.3 Most of the Class III malocclusion also
presented a skeletal discrepancy (75.4%).4
Although mild skeletal discrepancy can be treated
by camouflage orthodontic treatment. To improve facial
profile and dental occlusion in severe skeletal relationship,
the treatment usually leads to orthognathic surgery.
For conventional orthognathic surgery, the presurgical
orthodontic treatment is needed to decompensate teeth
alignment before surgery which provides benefits of
changing the amount of surgical reposition procedure and
gives the best surgical results.5 However, patients who
received presurgical orthodontic treatment were found to
have negative impact on their quality of life.6
The surgery- first approach was introduced in 1988
by Behrman and Behrman with the advantages of short
treatment period due to no presurgical orthodontics
treatment stage.7 Patients also reported the improvement
of quality of life immediately after surgery in surgery-
first approach group.6 Yet in some cases, the degree
of complexity exceeds the limitation for surgery-first
approach.
A modified surgery-first approach has an advantage
of using short period of presurgical orthodontic
preparation simply for minor teeth adjustment. The aim
of dental correction prior the surgery is to decrease the
Mandibular Prognathism with Atypical Dental Pattern
amount of severe dental discrepancy such as excessive or
recessive inclination and major dental interference which
could impact the setting of surgical occlusion, still there
are some correction needed for postsurgical orthodontic
treatment to be done.
Furthermore, surgical techniques to enhance
dental correction can be benefit for patients who have
atypical skeletal and dental pattern. Segmental osteotomy
can be used to improve surgical outcome and help
occlusal set up instead of strictly relying on orthodontic
tooth movement. In the maxilla, the maxillary segmental
osteotomy provided stable outcomes in sagittal plane.8
With the rigid fixation and interpositional bone grafting,
the stability in horizontal plane of maxilla advancement
in segmental group is the same as one-piece group and
shows less relapse rate in vertical plane.9
For mandible, main reason of skeletal Class III
comes from mandibular prognathism (47.4%) or excessive
growth, meanwhile the maxilla found to be retrognathism
(10.5%) or micrognathia (8.8%).4 To deal with the
excessive mandible, mandibular setback by bilateral
sagittal split osteotomies (BSSO) is usually performed in
our centre. Still the large amount of setback could affect
the posterior airway space10,11
or could not fully correct
patient’s problem. The mandibular anterior segmental
subapical osteotomy was first introduced by Hullihen in
1849.8 After that many modification procedures by Köle
was introduced in 1959.12
The subapical osteotomy at
the anterior part of mandible provide more modification
on lower jaw such as adjusting incisal position, incisal
inclination and arch length.13,14
Therefore, this case report describes the management
of an adult patient presenting with a skeletal Class
III malocclusion with mandibular protrusion, upper
incisor proclination and mandibular arch spacing by a
modified surgery-first approach. The surgical technique
included segmental LeFort I osteotomy in maxilla and
BSSO combined with subapical osteotomy in mandible.

88 Taiwanese Journal of Orthodontics. 2019, Vol. 31. No. 210.30036/TJO.201906_31(2).0003
Chanruangvanich J, Ko EWC, Chen YA
CASE REPORT
A 26-year-old man had chief complaint of a long
lower jaw. He denied any major systemic diseases or drug
allergies.
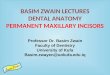
Clinical FindingsThe clinical examination presented skeletal Class III
relationship, retrognathic maxilla, excessive lower facial
height and prognathic mandible with chin deviation to
the left 3 mm. He had non-consonant smile arch without
gummy smile. His lateral facial profile was concave with
paranasal depression, acute nasolabial angle and shallow
mentolabial fold (Figure 1).
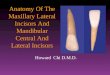
His dental manifestat ion presented Angle’s
Classification III malocclusion with a negative overjet of
-2 mm and overbite of 2.5 mm. The upper dental midline
was 2 mm right to facial midline while the lower dental
midline was 2 mm left to facial midline. For the maxilla,
upper incisors were proclined (U1/SN=128.5°), mild
crowding and right-side up occlusal plane canting. In
contrast, the mandible presented spacing between canine
and first premolar at both side with slightly retroclined
lower incisors (L1/MP=85°) (Figure 2, Table 1).
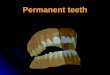
From radiographic examination, all permanent teeth
were erupted with 24 endodontically treatment. Average
retropalatal and retroglossal and airway space, which was
9 mm and 12 mm respectively, were observed (Figure 3).
Figure 1. Pre-treatment facial photographs.
Figure 2. Pre-treatment intraoral photographs.

89Taiwanese Journal of Orthodontics. 2019, Vol. 31. No. 210.30036/TJO.201906_31(2).0003
Mandibular Prognathism with Atypical Dental Pattern
Treatment Goals
Soft Tissue• Correct facial proportion• Correct lip posture• Improve smile arch
Skeletal• Correct midface deficiency and mandibular prognathism• Correct maxilla canting• Correct chin deviation
Dental • Correct dental inclination and relationship • Achieve Class I canine and Class II molar relationship
Figure 3. Pre-treatment radiographs.
Treatment goals and treatment plan
From the examination, the treatment goals were set.
From the diagnosis and treatment goals together with
patient’s expectation, the treatment plan was performed
with a modified surgery-first approach as following steps.
1. General dental care: Full mouth scaling and polishing
2. Presurgical orthodontic treatment: 14, 24 extraction for
reducing incisal proclination, alignment and levelling.
3. Orthognathic surgery:
Maxilla: 2-pieces LeFort I osteotomy
Mandible: Köle procedure and BSSO for mandible
setback and asymmetry correction.
Genioplasty: chin contouring
4. Post-surgical orthodontic treatment
5. Retention

90 Taiwanese Journal of Orthodontics. 2019, Vol. 31. No. 210.30036/TJO.201906_31(2).0003
Treatment ProgressIn the maxilla, the significant maxillary crowding
was relieved by 14 and 24 extractions while partially
retracting the maxillary incisors to reduce the incisal
proclination. Then, the upper incisors inclination was
furtherly corrected more by a 2-pieces LeFort I osteotomy
and closure of the 14, 24 residual dental space during
surgery.
In the mandible, the lower dental spacing was
caused by general tooth size and jaw bone discrepancy
with relative upright incisal inclination. The presurgical
preparation included consolidation the dental space distal
to the bilateral mandibular canines. The presurgical
orthodontics preparation took 7 months before surgery.
Then, the pre-operative records were taken included
dental radiographs, cone beam computed tomography
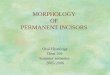
(CBCT) and surgical models. For surgical plan, a 2-pieces
LeFort I osteotomy were performed which was cut at the
area between 13-15 and 23-25. Anterior maxilla portion
Figure 4. The surgical planning.
was clockwise rotated which resulted in upper incisor
setback 4 mm, downward 1 mm and decreasing their
inclination. The posterior portion of maxilla was moved
forward for space closure and posterior impacted for
further dental occlusion.
The bilateral sagittal split osteotomies (BSSO)
were conducted for mandible setback and asymmetry
correction. The mandible was set back 8mm at the
right side and 5mm at the left side. Additionally, the
subapical osteotomy with Köle procedure was applied
with 2mm setback at the right side and 4mm setback at
the left side. This procedure helped closing the dental
space in the mandibular arch while keeping the anterior
teeth in relative normal inclination. The excessive chin
prominence caused by the Köle procedure was reduced by
reduction genioplasty and surface contouring (Figure 4).
Post-operative orthodontic treatment took about 19
months included overbite control and detailing of the
occlusion and interdigitation.
Chanruangvanich J, Ko EWC, Chen YA

91Taiwanese Journal of Orthodontics. 2019, Vol. 31. No. 210.30036/TJO.201906_31(2).0003
Treatment ResultsAfter treatment, patient’s profile was improved
to straight facial profile, symmetry and good facial
proportion. All surgical segments were stable. Class I
canine relationship and Class II molar relationship were
achieved with 2 mm overjet and 2 mm overbite. The
maxillary incisors proclination were improved, all the
dental spaces were closed and well interdigitation (Figure
5, Table 1).
From the superimposition, the mandible was setback
and the maxilla was clockwise rotated by impaction of
posterior segment upward 3 mm. The pogonion point was
moved backward by 7 mm along with posterior airway
reduction to 8 mm at retropalatal and retroglossal area
(Figure 6).
This case report was approved by the Institutional
Review Board and Medical Ethics Committee of Chang
Gung Memorial Hospital (No. 201900284B0).
Figure 5. Post-treatment photographs at the time of debond (19 months after surgery).
Mandibular Prognathism with Atypical Dental Pattern

92 Taiwanese Journal of Orthodontics. 2019, Vol. 31. No. 210.30036/TJO.201906_31(2).0003
Figure 6. 2D and 3D Superimposition of before and after treatment. InitialDebond
Table 1. The cephalometric analysis in before and after treatment.
Skeletal
Pretreatment Debond Norm
SNA 85.0 84.0 79.4 - 82.5
SNB 92.0 84.0 74.6 - 77.8
ANB 7.0 0.0 4.1 - 5.7
SND-MP 30.5 35.0 34.2 - 38.6
Dental Analysis
Upper-NA (mm) 13.0 8.5 3.8-7.2
U1/SN⁰ 128.5 114.0 103.5-109.1
L1-NB (mm) 28.0 27.0 6.1-9.5
L1/MP⁰ (Me-Go) 85.0 87.5 91.1-98.3
Facial Analysis
E-line (mm)Upper 0.5 1.0 0.8-3.2
Lower 6.0 1.0 1.2-4.4
Retropalatal Airway 12.0 8.0
Retroglossal Airway 9.0 8.0
Chanruangvanich J, Ko EWC, Chen YA

93Taiwanese Journal of Orthodontics. 2019, Vol. 31. No. 210.30036/TJO.201906_31(2).0003
technique alone. They generate a better result with less
effect on posterior airway space and provided good
skeletal stability.9,17
Although, upper anterior incisors showed severe
proclination, an excessive amount of rotation at anterior
segment of maxilla could not be done. The large bony
step between anterior and posterior segment should be
considered. It also could cause the periodontal problem
at distal of canine where the surgical cut and extraction
space closure take place which could lead to periodontal
problem such as gingival recession (1.5%).18
Therefore,
with the limitation above, the upper incisors still show
some proclination at the end of the treatment (U1/SN =
114⁰), but no periodontal problem was founded. The side
effect of Köle osteotomy set back is bony prominence
and excessive chin contour.19
The genioplasty could help
contouring the bony prominence and correct remaining
asymmetry.
Finally, a proper surgical result not only concern
about facial profile and dental occlusion, but also airway
space should be appropriate considered. Some maxillary
incisors proclination and minor reduction of airway space
were observed, however, patient reports no change in
sleep quality and feels pleasing with the treatment result.
CONCLUSION
The treatment goals of the dentoalveolar portion and
facial proportion should be contemplated for the staged
procedures to improve the efficiency and effectiveness of
the treatment outcome. Soft tissue including airway space
also should be carefully evaluated to avoid the unwanted
side effects and provided the most suitable treatment for
patient.
REFERENCE
1. Hardy D, Cubas Y, Orellana M. Prevalence of angle
class III malocclusion: A systematic review and meta-
DISCUSSION
With the modified surgery-first technique, the
presurgical orthodontic treatment was performed to reduce
severe incisal inclination, minor levelling and alignment
but didn’t aim for fully dental alignment, space closure
or occlusal interdigitation. Thus, this patient took only 7
months for presurgical orthodontic treatment preparation.
The 2-pieces LeFort I and Köle osteotomy then addressed
the correction in the dentoalveolar portion for efficiently
control the inclination of the anterior teeth.12
For the surgical design, the clockwise rotation of
maxilla could help reducing the incisal inclination.5
From the study of Gandedkar et al., the range of 4-8 mm
setback surgery in bimaxillary surgery showed no change
in risk factors scores for obstructive sleep apnea (OSA).15
However, for this patient, a big amount of rotation was
needed for fully correction which could affect the amount
of bone reduction and could affect the posterior airway
space.10,11
On the other hand, the discrepancy between tooth-
size and arch length in this patient resulted in large
amount of spacing in mandibular arch especially at distal
of lower canine at both sides. If the spacing would be
closed by only orthodontic movement before surgery, a
large amount of incisors retraction or molar protraction
were needed which could lengthening the presurgical
orthodontics treatment. On the contrary, if spacing were
kept for prostheses or planned for space closure after
surgery, the large amount of mandibular setback more
than 8 mm could not be avoided.
Therefore, the combination of the clockwise rotation
of maxillary anterior segment from 2-pieces LeFort I
osteotomy and Köle osteotomy combined with BSSO was
chosen to reduce incisors angulation and space closure.16
The posterior segment of maxilla was moved forward to
close extraction space and Köle osteotomy was helped to
close the excessive mandibular spacing which resulted in
less amount of total mandibular set back by just BSSO
Mandibular Prognathism with Atypical Dental Pattern

94 Taiwanese Journal of Orthodontics. 2019, Vol. 31. No. 210.30036/TJO.201906_31(2).0003
13. Sahin T, Garreau E, Komakli Y, et al. Mandibular
anterior segmental subapical osteotomy for incisor
axis correction. J Stomatol Oral Maxillofac Surg
2017;118(5):271-278.
14. Bell WH. Subapical osteotomy to increase mandibular
arch length. Am J Orthod 1978;74(3):276–285.
15. Gandedkar NH, Chng CK, Por YC, et al. Influence
of Bimaxillary Surgery on Pharyngeal Airway in
Class III Deformities and Effect on Sleep Apnea:
A STOP-BANG Questionnaire and Cone-Beam
Computed Tomography Study. J Oral Maxillofac Surg
2017;75(11):2411-2421.
16. Baek SH, Kim K, Choi, JY. Evaluation of Treatment
Modality for Skeletal Class III Malocclusion with
Labioversed Upper Incisors and/or Protrusive Maxilla.
J Craniomaxillofac Surg 2009;20(6):2049–2054.
17. Chow J, Hägg U, Tiedeman H. The stability of
segmentalized Le Fort I osteotomies with miniplate
fixation in patients with maxillary hypoplasia. J Oral
Maxillofac Surg 1995;53:1407–12.
18. Posnick JC, Adachie A, Choi E. (2016). Segmental
Maxi l lary Osteotomies in Conjunct ion with
Bimaxillary Orthognathic Surgery: Indications
– Safety – Outcome. J Oral Maxillofac Surg
2016;74(7):1422–1440.
19. Choi BK, Lee W, Lo LJ, Yang EJ. Modified Rotational
Anterior Segmental Osteotomy for Prevention
of Common Complication (Aged Appearance).
J Craniofac Surg. 2018;29(5):e517-e518.
analysis. Open J Epidemiol 2012;2:75-82.
2. Soha J, Sandham A, Chan YH. Occlusal Status in
Asian Male Adults: Prevalence and Ethnic Variation.
Angle Orthod 2005;75:814–820.
3. Tang ELK. The Prevalence of Malocclusion Amongst
Hong Kong Male Dental Students. Br J Orthod
1994;21(1),57–63.
4. Staudt CB, Kiliaridis S. Different skeletal types
underlying Class III malocclusion in a random
population. Am J Orthod Dentofacial Orthop
2009:136(5):715–721.
5. Worms FW, Isaacson RJ, Speidel TM. Surgical
orthodontic treatment planning: profile analysis and
mandibular surgery. Angle Orthod 1976;46:1–25.
6. Pelo S, Gasparini G, Garagiola U, et al. Surgery-first
orthognathic approach vs traditional orthognathic
approach: Oral health-related quality of life assessed
with 2 questionnaires. Am J Orthod Dentofacial
Orthop. 2017;152(2):250-254.
7 . Behrman SJ , Behrman, DA. Ora l surgeons’
considerations in surgical orthodontic treatment. Dent
Clin North Am 1988;32:481-507.
8. Hullihen SP. Case of elongation of the underjaw and
distortion of the face and neck, caused by a burn,
successfully treated. Am J Dent Sci 1849;9:157.
9 . Arpornmaeklong P, Heggie AA, Shand JM.
A comparison of the stability of single piece and
segmental Le Fort I maxillary advancements.
J Craniofac Surg 2003;14: 3–9.
10. Hai HK, Egyedi P. Preserving the pterygoid plates in
posterior repositioning of the Le Fort I osteotomy.
J Craniomaxillofac Surg 1989;17(5):219–221.
11. Park JE, Bae SH, Choi YJ, et al. The structural
changes of pharyngeal airway contributing to snoring
after orthognathic surgery in skeletal class III patients.
Maxillofac Plast Reconstr Surg 2017;39(1):22.
12. Köle H. Surgical operations on the alveolar ridge to
correct occlusal abnormalities. Oral Surg Oral Med
Oral Pathol 1959;12(4):413-420.
Chanruangvanich J, Ko EWC, Chen YA