Embed Size (px)
DESCRIPTION
A new approach to Arthrocentesis of the Temporomandibular joint
Citation preview

Technical Note
TMJ Disorders
Int. J. Oral Maxillofac. Surg. 2009; 38: 85–86doi:10.1016/j.ijom.2008.11.005, available online at http://www.sciencedirect.com
A new approach toarthrocentesis of thetemporomandibular joint
A. Alkan, E. Kilic: A new approach to arthrocentesis of the temporomandibular joint.Int. J. Oral Maxillofac. Surg. 2009; 38: 85–86. # 2008 International Association ofOral and Maxillofacial Surgeons. Published by Elsevier Ltd. All rights reserved.0901-5027/01085 + 02 $30.00/0 # 2008 Internat
ional Association of Oral and Maxillofacial SurgeonA. Alkan, E. KilicDepartment of Oral and Maxillofacial Surgery,Faculty of Dentistry, Erciyes University,Kayseri, Turkey
Abstract. We describe a new temporomandibular joint (TMJ) arthrocentesistechnique using the irrigation pump from a surgical and dental implant motor,providing the highest hydraulic pressure reported in the literature for TMJlavage.
Accepted for publication 3 November 2008Arthrocentesis is an easy, minimallyinvasive, highly efficient procedure todecrease joint pain and increase therange of mouth opening in patients withclosed lock of the temporomandibularjoint (TMJ)6. NITZAN et al.2 firstdescribed TMJ arthrocentesis as the sim-plest form of surgery in the TMJ, aimingto release the articular disc and toremove adhesions between the disc sur-face and the mandibular fossa by meansof hydraulic pressure from irrigation ofthe upper chamber of the TMJ. YURA
et al.6 confirmed that adhesions arereleased after irrigation of the upperjoint space under sufficient hydraulicpressure. It is not known whether arthro-centesis performed with higher pressurein a short time period is more effective.The authors describe the use of thesurgical and dental motor as a newdevice to accomplish TMJ arthrocentesiswith higher pressure.
Technique
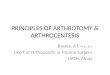
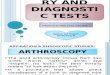
The arthrocentesis technique described byNITZAN et al.2 was used. A line was drawnfrom the corner of the eye to tragus and thefirst mark was made 10 mm from thetragus and 0.5 mm below the line. Thesecond point was marked 20 mm fromthe tragus and 1 mm below the line. A21-gauge needle was inserted into thesuperior joint compartment from the firstpoint and 5 ml saline solution was injectedto widen the upper joint space. A secondneedle, the same diameter as the first, wasinserted from the second point and it wasmanually confirmed that upper joint spacewas irrigated effectively. The silicone tubeof the irrigation pump (KaVo, INTRAsurg300/300 plus, Biberach, Germany) wasconnected to the second needle and auto-matic irrigation under high pressure wasinitiated (Fig. 1). The upper joint spacewas irrigated with 300 ml saline solutionunder pressure in all patients for 2 min
(Fig. 2). This technique was not used wheneffective manual irrigation was impossi-ble.
Discussion
TMJ arthrocentesis is often performed forthe treatment of TMJ dysfunction. NITZAN
et al.3 reported that the efficiency ofarthrocentesis under low pressure, whichwas applied manually using a 10-ml syr-inge, was not successful in patients withsevere adhesions. In contrast, YURA et al.6
reported on the efficacy of arthrocentesisunder high pressure using the infusionaccelerator for blood bag (maximum pres-sure exerted, 40 KPa). Their study showedthat high pressure removes adhesions andwidens joint spaces in patients withchronic closed lock and with adhesionsin the upper joint. They also stated thatpathologic conditions of the TMJ did notinfluence the efficacy of arthrocentesis
s. Published by Elsevier Ltd. All rights reserved.

86 Alkan, and Kilic
Fig. 1. Use of the irrigation pump from the surgical and dental motor for TMJ arthrocentesis.
Fig. 2. Clinical view of TMJ arthrocentesis under high hydraulic pressure.
under sufficient pressure5. This suggeststhat their procedure with sufficient pres-sure has wider applications than arthro-centesis under low pressure. In a similarstudy, SATO et al.4 stated that pumpingwith injection of sodium hyaluronate intothe TMJ is an effective treatment for non-reducing disc displacement of the TMJ.The authors considered whether the out-come of TMJ arthrocentesis would bemore effective when the hydraulic pres-sure was increased. The clinical outcomeof this technique will be published whenthe study population reaches a sufficientnumber.
ZARDENETA et al.7 stated that approxi-mately 100 ml of total arthrocentesisvolume is sufficient for therapeutic lavageof the superior joint space of the human
TMJ. KANEYAMA et al.1 studied the ideallavage volume for removing bradykinin,interleukin-6 and protein from the TMJ.They performed arthrocentesis with dif-ferent lavage volumes and concluded thatthe ideal lavage volume of perfusate forarthrocentesis is between 300 and 400 ml.The authors consider that it is possible toirrigate the upper joint space in 2 min with300 ml saline solution.
Surgical and dental motors are availablein all oral and maxillofacial surgerydepartments, so no additional equipmentis required to use this technique. Theirrigation pump settings are explained inthe instruction booklet. This techniqueshould be performed by surgeons withexperience of TMJ arthrocentesis. If theirrigation pump is connected to the first
needle without manual confirmation withthe second needle, complications mayoccur in the surrounding tissues owingto the high pressure. During the procedure,if the outlet needle suddenly blocks, thesurgeon must discontinue the irrigationimmediately.
References
1. Kaneyama K, Segami N, Nishimura M,Sato J, Fujimura K, Yoshimura H. Theideal lavage volume for removing brady-kinin, interleukin-6, and protein fromtemporomandibular joint by arthrocent-esis. J Oral Maxillofac Surg 2004: 62:657–661.
2. Nitzan DW, Dolwick MF, Martinez
GA. Temporomandibular joint arthrocent-esis: a simplified treatment for severe,limited mouth opening. J Oral MaxillofacSurg 1991: 49: 1163–1167.
3. Nitzan DW, Price A. The use of arthro-centesis for the treatment of osteoarthritictemporomandibular joints. J Oral Maxillo-fac Surg 2001: 59: 1154–1159.
4. Sato S, Goto S, Kasahara T, Kawa-
mura H, Motegi K. Effect of pumpingwith injection of sodium hyaluronate andthe other factors related to outcome inpatients with non reducing disk displace-ment of the temporomandibular joint. Int JOral Maxillofac Surg 2001: 30: 194–198.
5. Yura S, Totsuka Y. Relationshipbetween effectiveness of arthrocentesisunder sufficient pressure and conditionsof the temporomandibular joint. J OralMaxillofac Surg 2005: 63: 225–228.
6. Yura S, Totsuka Y, Yoshikawa T,Inoue N. Can arthrocentesis release intra-capsular adhesions? Arthroscopic findingsbefore and after irrigation under sufficienthydraulic pressure. J Oral Maxillofac Surg2003: 61: 1253–1256.
7. Zardeneta G, Milam SB, Schmitz JP.Elution of proteins by continuous tempor-omandibular joint arthrocentesis. J OralMaxillofac Surg 1997: 55: 709–716.
Address: Alper AlkanErciyes UniversityFaculty of DentistryDepartment of Oral and Maxillofacial Sur-gery38039MelikgaziKayseriTurkeyTel: +90 352 4374937 29177Fax: +90 352 4380657E-mail: [email protected]