Embed Size (px)
Citation preview

VIEWS amp REVIEWS OPEN ACCESS
A new way to estimate neurologic diseaseprevalence in the United StatesIllustrated with MS
Lorene M Nelson PhD MS Mitchell T Wallin MD MPH Ruth Ann Marrie MD PhD WJ Culpepper PhD
Annette Langer-Gould MD PhD Jon Campbell PhD Stephen Buka ScD Helen Tremlett PhD
Gary Cutter PhD Wendy Kaye PhD Laurie Wagner MPH and Nicholas G Larocca PhD
for the United States Multiple Sclerosis Prevalence Workgroup
Neurologyreg 201992469-480 doi101212WNL0000000000007044
Correspondence
Dr Nelson
lnelsonstanfordedu
AbstractObjectiveConsiderable gaps exist in knowledge regarding the prevalence of neurologic diseases such asmultiple sclerosis (MS) in the United States Therefore the MS Prevalence Working Groupsought to review and evaluate alternative methods for obtaining a scientifically valid estimate ofnational MS prevalence in the current health care era
MethodsWe carried out a strengths weaknesses opportunities and threats (SWOT) analysis for 3approaches to estimate MS prevalence population-based MS registries national probabilityhealth surveys and analysis of administrative health claims databases We reviewed MS prev-alence studies conducted in the United States and critically examined possible methods forestimating national MS prevalence
ResultsWe developed a new 4-step approach for estimating MS prevalence in the United States Firstidentify administrative health claim databases covering publicly and privately insured pop-ulations in the United States Second develop and validate a highly accurate MS case-findingalgorithm that can be standardly applied in all databases Third apply a case definition algo-rithm to estimate MS prevalence in each population Fourth combineMS prevalence estimatesinto a single estimate of US prevalence weighted according to the number of insured persons ineach health insurance segment
ConclusionsBy addressing methodologic challenges and proposing a new approach for measuring theprevalence of MS in the United States we hope that our work will benefit scientists who studyneurologic and other chronic conditions for which national prevalence estimates do not exist
RELATED ARTICLES
Validation of an algorithmfor identifying MS cases inadministrative healthclaims datasets
Page 456
The prevalence of MS inthe United States Apopulation-based estimateusing health claims data
Page 457
From the Division of Epidemiology Department of Health Research and Policy (LMN) Stanford University School of Medicine Stanford CA Department of Veterans AffairsMultiple Sclerosis Center of Excellence (VA MSCoE) and Georgetown University School of Medicine (MTW) Washington DC Department of Internal Medicine (RAM) Max RadyCollege of Medicine Rady Faculty of Health Sciences University of Manitoba Winnipeg Canada VA MS Center of Excellence and University of Maryland (WJC) BaltimoreNeurology Department (AL-G) Kaiser Permanente Southern California Los Angeles University of Colorado (JC) Denver Brown University (SB) Providence RI University ofBritish Columbia (HT) Vancouver Canada University of Alabama at Birmingham (GC) McKing Consulting Corporation (WK LW) Atlanta GA and National Multiple SclerosisSociety (NGL) New York NY
Go to NeurologyorgN for full disclosures Funding information and disclosures deemed relevant by the authors if any are provided at the end of the article
The Article Processing Charge was funded by National Multiple Sclerosis Society
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License 40 (CC BY-NC-ND) which permits downloadingand sharing the work provided it is properly cited The work cannot be changed in any way or used commercially without permission from the journal
Copyright copy 2019 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the American Academy of Neurology 469
Multiple sclerosis (MS) is the most common chronic pro-gressive neurologic disease of young adults12 affecting indi-viduals in their most productive years and placing a heavyburden on affected persons their family members and thehealth care system Unlike some other world regions con-siderable gaps exist in knowledge regarding the incidence andprevalence of MS in the United States because there is norobust method for estimating either epidemiologic statistic ona national basis The only population-based estimates of MSincidence (the number of new cases of MS in a population)have been obtained in the population of Rochester Minne-sota where the presence of the Mayo Clinic enables rigorousperiodic studies of MS incidence and prevalence3 The ab-sence of a unified single health care system in the US does notenable robust estimates of MS incidence on a national leveltherefore our focus is on estimating national MS prevalencein the United States
Obtaining an accurate estimate of MS prevalence in the UnitedStates is critical because prevalence supports comparisons ofMS burden across demographic subgroups geographic regionsand time periods Health care providers and policymakers relyon prevalence estimates to make decisions about future healthservice needs Researchers studying MS need information ondisease prevalence for evaluating changes in disease frequencyin relation to changing population demographics
MS is not a reportable condition and there is no nationalpopulation-based registry for MS Although many studiesexamining the prevalence of MS in select US communitieshave been conducted in the past 25 years4 the variablemethodology and quality of these studies prevent the datafrom being aggregated into a single robust national estimate ofMS in the United States
In 2014 the National Multiple Sclerosis Society establishedthe MS Prevalence Working Group a group composed ofscientists (neurologists epidemiologists statisticians) andpolicy advocates from the United States and Canada to ob-tain a valid estimate of MS prevalence in the United StatesWe sought to evaluate possible methods for estimating MSprevalence in the current health care era with the ultimate goalof providing a scientifically sound estimate of the overallprevalence of MS in the United States
We review MS prevalence studies conducted in the UnitedStates critically examine possible methods for estimatingnational MS prevalence and use this information to develop
a rationale for a new 4-step paradigm for estimating MSprevalence in the United States
Previous estimates of MS prevalencein the United StatesRegional MS prevalence studiesA recent systematic review4 identified 9 population-based MSprevalence studies conducted in small regions of the UnitedStates between 1985 and 2011 (table e-1 httpsdoiorg105061dryadt1k42p8) MS point prevalence was lowest in the19 counties surrounding Lubbock Texas (age-standardizedprevalence 399100000 95 confidence interval [CI]340ndash457)5 and highest in Olmstead County Minnesota(age-standardized prevalence 1912100000 95 CI1656ndash2168)3 A noteworthy advantage of such regionalstudies is that the relatively small population size enablesinvestigators to use many overlapping methods to ascertainpossible MS cases in the study population (case ascertain-ment) and apply standardized criteria to determine whichcases have MS (case definition) Regional MS prevalencestudies have used a variety of methods to maximize thecompleteness of case ascertainment with the most commonsources being specialty clinics or academic MS centerscommunity neurologists or other physicians patient serviceassociations nursing homes or long-term care facilities anddeath certificates4 Case definitions are usually establishedusing medical chart reviews abstracted to apply standard di-agnostic criteria6 However because MS prevalence can haveconsiderable geographic variation4 projecting estimates fromone or a few regions to the entire United States is of uncertainvalidity
National MS prevalence studies in theUnited StatesFor a country the size of the United States (310 millionpopulation in 2010) it is not feasible to use the intensive caseascertainment methods that are routine in smaller geographicregions In the last 4 decades 4 studies have estimated theprevalence of MS in the United States by using methodsintended to provide representative samples of the US pop-ulation (table 1) The first study was conducted in 1976 usinga probability sample of 725 acute short-term general hospitalsand 8800 physicians in the contiguous United States andsurveying them to estimate the number of persons with MSwith whom they had contact7 MS prevalence was estimatedto be 58 per 100000 population corresponding to 123000
GlossaryAHC = administrative health claims BRFSS = Behavioral Risk Factor Surveillance Survey CI = confidence interval DMT =disease-modifying treatment DOD = Department of Defense ICD-9 = International Classification of Diseasesndash9 MEPS-HC = Household Component of the Medical Expenditure Panel Survey MS = multiple sclerosis NHIS = National HealthInterview Survey SWOT = strengths weaknesses opportunities and threats VHA = Veterans Health Administration
470 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
cases in the United States but Anderson et al8 believed thatthe prevalence of MS was underestimated due to severalmethodologic factors A primary source of underascertain-ment was relying on physician recall to identify MS cases as atthe time these studies were conducted computerized medicalrecords systems were rare Another source of under-ascertainment was the single-year surveillance window whichwould havemissed patients withMSwho did not seekmedicalattention for MS during that year Evidence for a third sourceof underascertainment came from a prevalence survey con-ducted in the Weld and Larimer Counties of northern Col-orado9 which used multiple case ascertainment methods andfound that 21 of all prevalent cases identified came exclu-sively from the records of 3 MS service organizations inColorado a source that was not used in the 1976 study7
Anderson et al8 used several adjustments for these sources ofunderascertainment to provide an updated estimate of MSprevalence in the United States in 1990 ranging from 250000to 350000 persons
The next 2 national MS prevalence studies were conductedusing the National Health Interview Survey (NHIS) an annualprobability sample of the noninstitutionalized US populationDuring 1982ndash1996 one-sixth of the NHIS sample was sur-veyed about MS and other health conditions resulting in lim-itation of activity Collins10 used NHIS data for a 3-year period(1990ndash1992) to estimate national MS prevalence becausea single year of data did not yield enough persons with MS forstable estimation MS prevalence was estimated to be 70 per100000 corresponding to an estimated count of 180000 casesA second study also used NHIS data over 1982ndash199611 MSprevalence was estimated to be 85 per 100000 populationcorresponding to an estimated count of 211000 cases in theUnited States (95 CI 191000ndash231000) A major weaknessof the NHIS studies is that survey data were collected from onefamily member within each sampled household who reportedthe medical conditions for the entire household This method
would underestimate MS prevalence if household membersunderreport the condition but could also overestimate MSprevalence if self-reported data resulted in the inclusion ofprovisional cases (or noncases) who would not meet formalcase definition criteria
More recently a national MS prevalence study was carried outusing the Household Component of the Medical ExpenditurePanel Survey (MEPS-HC) a nationally representative surveyof the US civilian noninstitutionalized population drawn fromNHIS that collects data on health status health utilizationhealth costs and health insurance coverage12 MS cases wereidentified on the basis of having one or more medically codeddiagnoses of MS (ICD-9 code 340) Between 1998 and 2009526 MEPS-HC participants met this criterion and the annualaverage number of persons with MS was estimated to be572312 (95 CI 397004ndash747619) Requiring only 1 ICD-9code during the study year could have overestimated MSprevalence if false-positives were included because individualswho had a single ICD-9 340 code were ultimately not di-agnosed with MS or the code was entered erroneously TheMEPS-HC probability sample only captured non-institutionalized persons with MS which could have resultedin underascertainment because it excludes the estimated5ndash10 of persons with MS residing in nursing homes1314
Two studies have used administrative health claims (AHC)data to estimate the number of persons with MS Both studiesassessed subpopulations of the United States and then usedthis information to estimate the total number of persons withMS in the United States as a whole (table 2) Pope et al15
obtained administrative claims data from privately insuredindividuals those aged into Medicare and Medicaid blind ordisabled populations to determine the prevalence of MS in 6states for 1991ndash1997 MS prevalence (per 100000 pop-ulation) was estimated to be 240 in the privately insured 180among Medicare age 65 and above and 710 among Medicaid
Table 1 Epidemiologic studies ofmultiple sclerosis (MS) prevalence in theUnited States using probability sample surveys
ReferenceAuthors(year)
Studyyears Case definition Population
National MSprevalence per100000population
Number of personswith MS in theUnited States (95CI)
Baum andRothschild(1981)7
1976 Survey of physicians and hospitalsasked to report patients meetinguniform criteria for probable andpossible MS
National sample of 8800physicians and 725 hospitalsa probability sample of the 1976 USpopulation
58 per 100000(all ages)
123000
Collins(1997)10
1990ndash1992 Patients or family members reportingphysician-diagnosed MS
NHIS a household probabilitysample of US population
70 per 100000(all ages)
180000
Noonanet al (2002)11
1982ndash1996 Patients or family members reportingphysician-diagnosed MS
NHIS a household probabilitysample of US population
85 per 100000(all ages)
211000(191000ndash231000)
Campbellet al (2014)12
2008ndash2009 Patients having 1 or more medicalclaims with MS diagnostic code 340during a single year
MEPS-HC a household probabilitysample of US population
191 per 100000(ge18 years)
572312(397004ndash747619)
Abbreviations CI = confidence intervalMEPS-HC =Household Component of theMedical Expenditure Panel Survey NHIS =National Health Interview Survey
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 471
disabled populations These estimates are not strictly com-parable due to the different age distributions and the expec-tation that MS prevalence would be much higher in theMedicaid disabled population In addition no algorithm wasdeveloped or used for MS cases Dilokthornsakul et al16 es-timatedMS prevalence for 2008ndash2012 in the privately insuredUS population by applying a case definition algorithm usingthe PharMetrics Plus Health Plan Claims data a large USprivate insurance claims database that contained claims datafor approximately 42 million enrollees in 2011 The casedefinition algorithm required at least 2 inpatient claims withICD-9 code 340 at least 3 ICD-9 code 340 outpatient claimsor at least one MS-specific disease-modifying treatment(DMT) claim The estimated MS prevalence for 2012 was149 per 100000 (95 CI 1476ndash1509) and when extrapo-lated to the United States as a whole yielded an estimate of403630 individual cases (95 CI 387445ndash419833)
Methods for conducting a nationalstudy of MS prevalence in thecurrent eraBefore designing our study to estimate the US prevalenceof MS the working group members carried out a strengthsweaknesses opportunities and threats (SWOT) analysis for 3approaches to estimate MS prevalence (1) population-basedMS registries (table 3) (2) national probability health surveys(table 4) and (3) analysis of AHC databases (table 5) Studiesof each type were evaluated as potential sources for estimatingthe national prevalence ofMS based on the populations studied
Population-based MS registriesLongstanding MS registries have been successfully used toestimate MS prevalence in 4 countries Denmark1718 Swe-den19 Norway20 and Poland21 However a similar USpopulation-based MS registry does not exist In the UnitedStates there are several voluntary MS registries for conduct-ing outcomes research however none of these registriesattempts the near-complete case ascertainment in a definedgeographic region that would enable the estimation of MSprevalence The benefits and pitfalls of population-baseddisease registries were recently reviewed22 and are summa-rized in table 3 A nationwide population-based registry wouldbe costly to implement however it is possible that a geo-graphically representative system of regional registries couldbe implemented similar to the approach used for cancersurveillance23 In the United States only one neurologic dis-ease registry has been implemented The National Amyo-trophic Lateral Sclerosis Registry was established bya Congressional mandate and began estimating nationalamyotrophic lateral sclerosis prevalence in 20102425
National probability health surveysThe primary method used to estimate national MS prevalencein the past has been probability health surveys Howeveralmost none of the national probability surveys conducted bythe US government are sufficiently large enough to containenough people with MS to enable precise estimation of MSprevalence much less prevalence within demographic or re-gional subgroups Moreover the national survey that onceallowed an overall estimate of MS prevalence (NHIS) nolonger includes questions about MS and other disablingconditions National probability survey data rely on patient or
Table 2 Epidemiologic studies of multiple sclerosis (MS) prevalence in large regions of the United States usingadministrative health claims databases
ReferenceAuthors (year)
Studyyears Case definition Population
National MSprevalence per100000 population(95 CI)
Number ofpersons with MSin the UnitedStates (95 CI)
Popeet al (2002)15 1994ndash1997 One ormore ICD-9 codes for MS(diagnosis code 340)
Nationally representative samplesof administrative claims from 6states (California ColoradoGeorgia Michigan MissouriTennessee)
Privately insured (MedstatMarketScan database)
240 per 100000(95 CI NR) (all ages)
NR
Medicare age 65 and above 180 per 100000(95 CI NR) (age ge65)
NR
Medicaid disabled population allages
710 per 10000 (95CI NR) (all ages)
NR
Dilokthornsakulet al (2016)16
2012 At least 2 inpatient claims withICD-9 code 340 at least 3 ICD-9code 340 outpatient claims orat least 1 MS-indicated DMT
Commercially insured population(Truven Market-Scan)
149 per 100000(1475ndash1508) (allages age-adjustedto US 2012population)
403630(387445ndash419833)
Abbreviations CI = confidence interval DMT = disease-modifying treatment ICD-9 = International Classification of Diseasesndash9 NR = not reported
472 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
family member reports of physician-diagnosed MS1012 risk-ing the inclusion of false-positive MS cases or provisionalcases that would not meet formal case definition criteria Onlyone national survey the Behavioral Risk Factor SurveillanceSurvey (BRFSS) which surveys more than 500000 individ-uals each year has a sample size that would potentially yieldprecise estimates of MS prevalence Feasibility work would beneeded to determine if this BRFSS could be used for thispurpose
Administrative health claims dataIn other countries with universally funded health care systemssuch as Canada and many European nations AHC databaseshave been used to provide a population-based alternative to thetraditional intensive methods of case ascertainment used inregional studies1 In the United States AHC data are main-tained by government (public) insurance programs includingMedicare andMedicaid and by private (commercial) insuranceproviders AHC databases are a tremendous resource forstudying neurologic disease incidence and prevalence becauseof their rich prospective data on patients from defined pop-ulations and their use of the standardized international disease-coding framework (using the ICD system)26 However AHCdatabases are not created for research purposes making it
necessary to demonstrate the validity and the accuracy of caseascertainment algorithm prior to using them for estimatingdisease prevalence These challenges exist for estimating prev-alence of all other common chronic neurologic conditions26
AHC data sources have potential strengths and limitationswhen applied for the purpose of estimating disease prevalence(table 5) The information from AHC databases begins withenrollment into health insurance plans and provides a stan-dardized source of longitudinal patient health care utilizationThese data contain near complete capture of demographic in-formation (sex date of birth raceethnicity zip code or state ofresidence) and health care utilization data including diagnosticcodes and pharmacy records They can be used for researchwithout specific consent because the databases are de-identified Identifying persons with MS through pharmacyrecords is an excellent case ascertainment strategy given thatmany of the DMTs are prescribed only for MS thus the per-sons withMS using suchmedications are highly likely to be trueMS cases However over 40 of persons withMS in theUnitedStates do not take DMTs necessitating additional case-findingmethods Because clinical details are often not available such aswhether a diagnostic code was entered by a neurologist phy-sician or nonphysicianmost claims database studies have reliedon case-finding algorithms that have not been judged against
Table 3 Strengths weaknesses opportunities and threats (SWOT) analysis using population-based multiple sclerosis(MS) registries to estimate national MS prevalence in the US
Strengths Weaknesses Opportunities Threats
Multiple overlapping caseascertainment methods areused to yield a high degree ofcase ascertainment
Organizational demands makea nationwide registry infeasible in theUnited States with rare exceptions(National Amyotrophic LateralSclerosis Registry2425)
A systematic approach could bedeveloped to extrapolate results frommultiple regional registries to nationalMS prevalence howevera geographically valid sample of selectstates would need to be selected torepresent the nation
If registry relies on patientvolunteers or requires consenta large degree of nonresponse canseriously affect the validity of theregistry
Data are rigorously collected forresearch purposes according tostandard protocols
Very high cost to implement inpopulation-based regions possiblyinfeasible for nationwideimplementation in the United States
For regions where registryparticipation is high can obtain validand precise estimates of MSprevalence
Confirming clinician diagnoses iscostly and impractical for largenumbers of patients
Some US registries rely in parton case ascertainment throughneurologists primary carephysicians and hospitals
In the United States registries oftenalso rely on MS diagnosis reported bypatient or family member whichmight be misreported medical chartsmay be requested for verification ofcase definition but may be difficult toobtain for all patients in a population-based registry
Need to collect patient identifiers toidentify duplicates identified bymore than one case ascertainmentmethod (risks HIPAAnoncompliance)
Data can be collected on raceethnicity and othersociodemographiccharacteristics
Registries often contain moreclinical details (eg initialsymptomatology clinicalcourse disability status) than doother sources
Abbreviation HIPAA = Health Insurance Portability and Accountability ActWith the exception of studies conducted by Mayo Clinic researchers in Rochester Minnesota17 population-based MS registries do not exist in the UnitedStates However there are several notable population-basedMS registries in Europe that enable ongoing estimation of nationalMS incidence andprevalenceincluding in Denmark1718 Sweden19 Norway20 and Poland21 Such studies often rely on case ascertainment through multiple data sources includingneurologists primary care physicians and hospitals
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 473
case definitions or even neurologist diagnoses for accuracyTwo studies used a case definition that required only a singlehealth care encounter for MS1215 which is likely to be highlynonspecific risking an unknown number of false-positives Thestudy by Dilokthornsakul et al16 that used private insuranceclaims data was strengthened by conducting sensitivity analysesthat examined the performance of 2 alternative algorithms oneof which produced estimates very similar to the primaryalgorithm
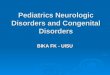
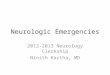
Developing a new approach forestimating MS prevalence in theUnited StatesBased on the SWOT analysis and through discussion andconsensus we concluded that AHC data would provide themost cost-effective method to develop a national prevalenceestimate for MS Collectively government and private healthclaims databases represent a very large proportion of the USpopulation (84 in 2010)28 which together enables preciseestimates of MS prevalence The data are sufficiently distrib-uted geographically and socioeconomically to be representa-tive of the entire US population Figure 1 illustrates a new4-step approach we devised for estimating the prevalence ofMS for the United States as a whole using a segmental
approach for each insurance source and then combining theminto a national estimate
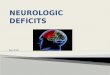
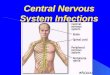
Step 1 Identify datasets covering US publicly and privatelyinsured populations figure 2 illustrates the fragmented natureof insurance coverage of the US population which doesnot enable a single health care source for estimating MSprevalence as is often available in Scandinavian countries withnational unified health care systems Nevertheless AHC dataare available for almost all of the insurance segments of theUS population allowing the estimation of MS prevalenceseparately for each insurance segment which can then beaggregated into an overall national estimate ofMS prevalenceFigure 2 shows US Census Current Population Survey datafor 2008ndash2010 presented separately for individuals under age65 vs those ages 65 and older because the sources of insurancecoverage vary considerably for these 2 age groups In 2010 forindividuals below age 65 private insurance comprised thelargest segment of insurance coverage 65 when employer-purchased and self-purchased private insurance were consid-ered together The next largest segment of insurance coveragein 2010 for individuals under age 65 is Medicaid (17)a government insurance program that provides free medicalinsurance to low-income people Smaller percentages ofindividuals under age 65 in 2010 were covered by a militarysource such as Department of Defense (DOD) or Veterans
Table 4 Strengths weaknesses opportunities and threats (SWOT) analysis using national probability survey samples toestimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can be obtained from existinggovernment surveys
Dedicated MS-specific patientsurveys are costly to carry out andinfeasible for national scope
This method can be feasible ifmultiple years of survey data can beaggregated
Existing national probabilitysamples usually comprise onlysegments of the US population(ie noninstitutionalized)
Sampling designs are rigorous(probability samples) of the USpopulation rigorously collected forresearch purposes according tostandard protocols
Survey participation rates are athistorically low levels
Successful application would requireaccess to a very large survey samplesuch as the BRFSS conducted annuallyby the CDC however a geographicallyvalid sample of select states wouldneed to be selected to represent thenation
Survey questions for patients andfamily members have not beenvalidated for accuracy againsta gold standard (neurologistdiagnosis)
Data are accessible and either cost-free or low-cost
Surveys rely on MS diagnosisreported by patient or a familymember which are susceptible toboth underreporting and false-positive reports
If survey questions were validatedagainst a gold standard (neurologistdiagnosis) this method could befeasibly implemented in a subset ofUS states
Restrictions on number ofquestions limits collection ofclinical details (eg clinicalcourse disability status)
Data are available on age sex raceethnicity broad geographic locationand other sociodemographiccharacteristics
Count ofMS patients in single yearsof data are often too small forprecise estimation
Some surveys collect self-reporteddata that can inform other analyseseg prevalence of comorbidity healthcare utilization and cost DMT uselifestyle risk factors
Overall prevalence might beestimable but data are often toosparse for getting breakdowns bysex age race or geographic region
Abbreviations BRFSS = Behavioral Risk Factor Surveillance Survey CDC = Centers for Disease Control and Prevention DMT = disease-modifying treatmentIn the United States national probability survey samples include the National Health Interview Survey Medical Expenditure Panel Survey HouseholdComponent National Nursing Home Survey and the BRFSS (a probability survey completed by500000 Americans per year and for which disease-specificquestions can be added on a state-by-state basis)
474 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Health Administration (VHA) (4) or by anothergovernment-provided insurance plan (Medicare 3) In2010 18 of individuals under age 65 had no insurancecoverage In 2010 for individuals ages 65 and abovegovernment insurance provided by Medicare covered 93of the population and was often supplemented by privatecoinsurance (33 employer-provided 29 self-purchased)Medicaid either alone or in combination with Medicarecovered 9 of those age 65 and above In 2010 8 ofindividuals age 65 and above were covered by amilitary source(DOD or VHA) and only 2 of the elderly were uninsuredThus despite the fragmentation of the US health care systemAHC databases for all of the insured segments of the USpopulation are available and can be used to estimate MSprevalence in each dataset separately before combining theestimates into a whole (step 4)Step 2 Develop and validate a highly accurate MS case-finding algorithm that can be standardly applied in all AHCdatabases Our approach requires a highly accurate casedefinition to identify MS cases that performs consistently
across AHC databases with differing characteristics so thatit can be applied even in datasets where formal validationis not possible Notably no MS prevalence studies in theUnited States have used validated algorithms for identifyingpersons with MS yet having a validated algorithm for thispurpose is a necessary step for carrying out valid prevalenceestimation26 Culpepper et al27 recently conducted a multi-site validation study to develop a valid and reliable algorithmfor identifying MS cases using AHC data with excellentsensitivity specificity and positive predictive value For thefirst time ever this provides a high-performing algorithmthat performs consistently well across datasets and can beapplied across all AHC databases Similar methodologycould be employed for other chronic neurologic diseasesusing existing literature to provide a starting point for thedevelopment of such case definitions26
Step 3 Apply the case definition algorithm to estimate thenumber of MS cases and prevalence estimates separately foreach database The third step of this approach is simply touse the validated algorithm (step 2) within each of the
Table 5 Strengths weaknesses opportunities and threats (SWOT) analysis using administrative health claims databasesto estimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can develop systematic approachthat could be repeatedly utilizedover time to obtain estimates nowand in the future
Lack of universal health care in theUnited States therefore not allpatients are identifiable throughadministrative data
Can develop a systematic approachthat can be repeatedly utilized overtime to obtain estimates now and inthe future
Lack of certainty whether casedefinitions developed in one datasetwill have same performancecharacteristics in other datasets
Data are accessible and relativelylow-cost
Must accessmultiple administrativedatasets
A case definition can be validated in2 or 3 different administrativedatasets to show consistency offindings across datasets thenapplied even in datasets wherevalidation is not possible4
No easily accessible national sourceof data for uninsured or self-paypopulations
Consistent capture of sex and dateof birth supports calculation of age-and sex-specific prevalenceestimates
Data are collected for health systemmanagement therefore theirvalidity for research must becarefully assessed
If a careful analytic approach is usedcan minimize overlap betweendatasets and avoid duplicatecounting
No easily accessible data forincarcerated or aboriginalpopulations
Data often include zip code whichcan be geocoded to determinesocioeconomic status and establishregion of residence
Lack of identified data to enableidentification of duplicates createsdifficulty identifying the sameindividuals in overlapping datasets
Would ideally include collection ofpatient identifiers to identifyduplicates present inmore than onedatabase howevernongovernment researchers arenot allowed access to suchidentifiers
These databases often haveadditional information that couldinform other analyses egprevalence of comorbidity healthcare utilization and disease-modifying treatment use
Some datasets lack informationregarding raceethnicity or havepoor geographic resolution
Representativeness cannot accessall administrative health databasesin United States must select few toestimate MS prevalence andextrapolate to all
Issue of misdiagnosis as a source oferror lack of clinical detail makes itdifficult to distinguish inaccuratelycoded diagnoses from clinicianmisdiagnosis
In the United States administrative health claims databases include Medicare (a government insurance program covering 93 of US residents age 65 andabove) Medicaid (a government insurance program for low-income parents and children and disabled persons in the United States) the Minimum Data Set(administrative data onMedicare- or Medicaid-certified nursing facilities) the Veterans Health Administration (health care program for veterans of US wars)commercial health insurance claims data (for employer-paid or self-paid insurance) and health maintenance organization health records
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 475
databases (step 1) to obtain valid MS prevalence estimates(overall and specific with respect to age sex raceethnicityand geographic location)Step 4 CombineMSprevalence estimates into a single estimateof the prevalence of MS for the United States weightedaccording to the number of insured persons in each healthinsurance segment after obtaining MS prevalence estimatesseparately for each of the US health insurance segments theycan be combined into a single national prevalence estimateInformation from theCurrent Population Survey can be used toobtain the necessary weights by determining the number of USresidents with each type of insurance coverage stratified by sexage group race and geographic region The total estimatednumber of MS cases for each age sex race and geographicregionndashspecific category can then be summed to estimatethe total number ofMS cases in the United States For exampleMS prevalence for the private insurance segment can beestimated by accessing AHC data for Optum (Eden PrairieMN) and Truven Health (Ann Arbor MI) which in 2010together comprise approximately 68 million individuals or 35of the 2010 privately insured US population MS prevalence inthe government-insured segment of the population can bedirectly and completely estimated for 100 of people coveredby using administrative claims data for Medicaid and MedicareMS prevalence in the military population which is pre-dominantly male can be estimated used the Veterans HealthAdministration database A limitation of this method is that noclaims data exist for persons without health insurance estimatedat 163 in 201028 however for this uninsured group MSprevalence estimates from the Medicaid health care claims datacould be applied because the 2 groups have similar sociodemo-graphic characteristics
Our new approach cannot be applied to estimate the in-cidence of MS in the United States Incidencemdashthe number
of new MS cases per year in a populationmdashis an importantmeasure of disease frequency However it can only be derivedfor countries that have single uniform health care systemswhere longitudinal AHC records for each person enable rel-atively precise indicators of the onset of new MS diagnosisand the exclusion of existing prevalent cases The lack ofa single payer health care system or national tracking systemin the United States does not allow reliable estimates of MSincidence because some individuals may change health carecoverage over time and it is not possible to link patientrecords across insurance sources to provide a single longi-tudinal record within which newly diagnosed persons withMS may be ascertained This creates short periods of ob-servation which do not allow accurate estimates of incidencefor conditions such as MS and cancer due to the inability todefinitively determine which individuals are truly newlydiagnosed29
DiscussionWe have proposed a new approach for applying validatedcase-finding algorithms to AHC data from both governmentand private sources to produce robust estimates of MSprevalence in the United States In a companion article weapplied this approach to estimate the total number of MScases in the United States30 This approach could be appliedto estimate prevalence of other neurologic disorders andchronic conditions that face similar methodologic challengessuch as Parkinson disease dementia and epilepsy
There are several reasons why our new approach is a valuablemethodologic development to estimate the national MSprevalence First this paradigm offers the potential to useexisting AHC data for case ascertainment across the UnitedStates without requiring the cost and effort involved in re-gional MS prevalence studies which typically employ in-tensive case ascertainment methods The data are sufficientlydistributed both geographically and socioeconomically tobe representative of the entire US population and do notrequire consent because the databases are de-identifiedSecond our method is efficient and cost-effective and can beapplied repeatedly with datasets that represent a large pro-portion of the country enabling updates to population-based estimates of MS prevalence over time Third applyingthis approach with data that represent the entire UnitedStates allows us to obtain more stable and precise prevalenceestimates and to fill in knowledge gaps regarding the prev-alence of MS in many regions for which we have never hadestimates Once AHC data are able to accurately and com-pletely capture race and ethnicity this approach could beapplied to racial and ethnic minorities that have receivedlittle study in the past Fourth the use of a highly accuratecase-finding algorithm4 ensures that there will be greatercomparability between estimates derived from these sourcesin the future By adopting a standard paradigm for ascer-taining MS cases and applying validated case definition
Figure 1 Stepwise process for determining the prevalenceof multiple sclerosis (MS) in the United States
476 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
criteria we will be better able to monitor and comparespatial differences in MS prevalence and to examine changesin disease prevalence over time without the variation in-troduced by differing methodologic approaches
Despite many strengths our new approach is limited in thatthe case ascertainment methods do not cover all segments ofthe US population It excludes native American residents whochoose to receive care through the Indian Health Service
Figure 2 Source of health insurance by age (estimates from the current population survey 2008ndash2010)
(A) Population younger than 65 years (B) Population 65 years of age and older
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 477
(06 of the US population in 2010)31 and US residents whoare incarcerated (approximately 05 of the US population in2010)32 If health care databases existed for these populationswe could similarly apply an MS algorithm to estimate MSprevalence and incorporate them into the overall nationalestimate Our approach also cannot distinguish between dif-ferent racial and ethnic groups thus we cannot address towhat extent variations in prevalence by geography or otherfactors may be better explained by racialethnic differences inprevalence33
Our work has important implications for the new era of MSepidemiologic research that will be possible through the 21stCentury Cures Act legislation enacted in December 2016which authorized the establishment of a federally fundedneurologic disorders surveillance system34 A national registryfor MS could be implemented similar to the NationalAmyotrophic Lateral Sclerosis Registry with AHC data asa primary method for case ascertainment and a web portalavailable for all persons with MS to register242535 Withoutaccess to a national registry in the intermediate term wepropose that our approach will deliver the most current andscientifically sound US estimate of the number of personswith MS By addressing methodologic challenges and pro-posing a new paradigm for measuring the prevalence of MS inthe United States we hope that our work will benefit scientistswho study all chronic conditions for which national preva-lence estimates do not currently exist
AcknowledgmentThe authors thank the following members of the US MultipleSclerosis Prevalence Workgroup for their contributionsAlbert Lo Robert McBurney Oleg Muravov Bari Talenteand Leslie Ritter The authors also thank the following keystaff members at the National Multiple Sclerosis Society fortheir contributions to this project Cathy Carlson TimCoetzee Sherri Giger Weyman Johnson Eileen MadrayGraham McReynolds and Cyndi Zagieboylo
Study fundingThe study was funded by contracts from the National Mul-tiple Sclerosis Society to the principal investigators in the MSPrevalence Working Group (HC-1508-05693) The ArticleProcessing Charge was funded by the National MultipleSclerosis Society
DisclosureL Nelson receives grants from the Centers for DiseaseControl and Prevention NIH and National Multiple Scle-rosis Society and contracts from the Agency for Toxic Sub-stances and Diseases Registry She receives compensation forserving as a consultant to Acumen Inc and is on the DataMonitoring Committee of Neuropace M Wallin has servedon data safety monitoring boards for the National Institutes ofNeurological Disease and StrokendashNIH has been an associateeditor for the Encyclopedia of the Neurological Sciences andreceived funding support from the National Multiple Sclerosis
Society and the Department of Veterans Affairs Merit ReviewResearch Program R Marrie is supported by the WaughFamily Chair in Multiple Sclerosis receives research fundingfrom Canadian Institutes of Health Research ResearchManitoba Multiple Sclerosis Society of Canada MultipleSclerosis Scientific Foundation National Multiple SclerosisSociety and Rx amp D Health Research Foundation and hasconducted clinical trials funded by Sanofi-Aventis She alsoserves on the Editorial Board ofNeurologyregW Culpepper hasadditional research funding from the National MultipleSclerosis Society receives support from the VHA MS Centerof Excellence and is a member of the National MultipleSclerosis Society Health Care Delivery and Policy Researchstudy section A Langer-Gould is site principal investigatorfor 2 industry-sponsored phase 3 clinical trials (BiogenIdec Hoffman-LaRoche) and was site PI for one industry-sponsored observation study (Biogen Idec) She receivesgrant support from the NIH National Institute of Neuro-logical Disorders and Stroke Patient-Centered OutcomesResearch Institute and the National Multiple Sclerosis Soci-ety J Campbell has consultancy or research grants over thelast 5 years with Agency for Healthcare Research and QualityALSAM Foundation Amgen AstraZeneca Bayer BiogenIdec Boehringer Ingelheim Centers for Disease Control andPrevention Colorado Medicaid Enterprise CommunityPartners Inc Institute for Clinical and Economic ReviewMallinckrodt NIH National Multiple Sclerosis Society Kai-ser Permanente PhRMA Foundation Teva Research in RealLife Ltd Respiratory Effectiveness Group and Zogenix IncS Buka receives research funding from the NIH and theNational Multiple Sclerosis Society H Tremlett is theCanada Research Chair for Neuroepidemiology and MultipleSclerosis She receives research support from the NationalMultiple Sclerosis Society the Canadian Institutes of HealthResearch the Multiple Sclerosis Society of Canada and theMultiple Sclerosis Scientific Research Foundation In addi-tion in the last 5 years she has received research support fromthe Multiple Sclerosis Society of Canada the Michael SmithFoundation for Health Research and the UK MS Trust andspeaker honoraria andor travel expenses to attend confer-ences G Cutter is a member of Data and Safety MonitoringBoards for AMO Pharmaceuticals Apotek Horizon Phar-maceuticals ModigenetechProlor Merck MerckPfizerOpko Biologics Neurim Sanofi-Aventis Reata Pharmaceut-icals ReceptosCelgene Teva pharmaceuticals NHLBI(Protocol Review Committee) and NICHD (OPRU over-sight committee) and is on the Consulting or AdvisoryBoards for Atara Biotherapeutics Argenix Bioeq GmbHConsortium of MS Centers (grant) Genzyme GenentechInnate Therapeutics Klein-Buendel Incorporated Medi-mmune Medday Novartis Opexa Therapeutics RocheSavara Inc Somahlution Teva Pharmaceuticals Trans-parency Life Sciences and TGTherapeutics W Kaye receivesfunding from the Agency for Toxic Substances and DiseaseRegistry the National Multiple Sclerosis Society and theAssociation for the Accreditation of Human ResearchProtection Programs L Wagner receives funding from the
478 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Agency for Toxic Substances and Disease Registry and Na-tional Multiple Sclerosis Society N LaRocca is employed fulltime by the National Multiple Sclerosis Society and has noother disclosures to report Statistical analysis conducted byDr Gary Cutter PhD University of Alabama at BirminghamGo to NeurologyorgN for full disclosures
Publication historyReceived byNeurology July 17 2018 Accepted in final form October 222018
References1 Wallin MT Kurtzke JF Neuroepidemiology In Bradley WG Daroff RB Fenichel
GM Jankovic J editors Neurology in Clinical Practice Philadelphia Butterworth-Heinemann 2008762ndash780
2 Browne P Chandraratna D Angood C et al Atlas of multiple sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
3 Mayr WT Pittock SJ McClelland RL Jorgensen NW Noseworthy JH Rodriguez MIncidence and prevalence of multiple sclerosis in Olmsted County Minnesota 1985-2000 Neurology 2003611373ndash1377
4 Evans C Beland SG Kulaga S et al Incidence and prevalence of multiple sclerosis inthe Americas a systematic review Neuroepidemiology 201340195ndash210
5 Noonan CW Williamson DM Henry JP et al The prevalence of multiple sclerosis in3 US communities Prev Chronic Dis 20107A1
6 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
7 Baum HM Rothschild BB The incidence and prevalence of reported multiple scle-rosis Ann Neurol 198110420ndash428
8 Anderson DW Ellenberg JH Leventhal CM Reingold SC Rodriguez M SilberbergDH Revised estimate of the prevalence of multiple sclerosis in the United States AnnNeurol 199231333ndash336
9 Nelson LM Hamman RF Thompson DS et al Higher than expected prevalence ofmultiple sclerosis in Northern Colorado dependence on methodological issuesNeuroepidemiology 1986517ndash28
10 Collins JG Prevalence of selected chronic conditions United States 1990-1992 VitalHealth Stat 10 19971941ndash89
Appendix 1 Authors
Name Location Role Contribution
Lorene MNelsonMS PhD
Stanford UniversityCA
Author Study concept anddesign preparation ofdraft manuscriptrevision of themanuscript forcontent approval offinal manuscript
Mitchell TWallin MDMPH
Veterans HealthAdministrationGeorgetownUniversityWashington DC
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
Ruth AnnMarrieMD PhD
University ofManitoba WinnipegCanada
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
William JCulpepperPhD MA
Veterans HealthAdministrationWashington DCUniversity ofMaryland Baltimore
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
AnnetteLanger-GouldMD PhD
Kaiser PermanenteSouthern CaliforniaLos Angeles
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
JonathanCampbellPhD
University of DenverCO
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
StephenBuka PhD
Brown UniversityProvidence RI
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
HelenTremlettPhD
University of BritishColumbia VancouverCanada
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
GaryCutterPhD
University ofAlabamaBirmingham
Author Study concept anddesign critical reviewof the manuscript forcontent
Appendix 1 (continued)
Name Location Role Contribution
WendyKaye PhD
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
LaurieWagnerMPH
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Nicholas GLaRoccaPhD
National MultipleSclerosis Society NewYork NY
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Appendix 2 Coinvestigators and members of the USMultiple Sclerosis Prevalence Workgroup
Name Location Role Contribution
Albert LoMD PhD
Brown UniversityProvidence RI
Coinvestigator Studyconcept anddesign
RobertMcBurneyPhD
Accelerated CureProject Boston MA
Coinvestigator Studyconcept anddesign
OlegMuravovPhD
Agency for ToxicSubstances andDisease RegistryDivision of HealthStudies Atlanta GA
Coinvestigator Studyconcept anddesign
BariTalenteEsq
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
LeslieRitter
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 479
11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Multiple sclerosis (MS) is the most common chronic pro-gressive neurologic disease of young adults12 affecting indi-viduals in their most productive years and placing a heavyburden on affected persons their family members and thehealth care system Unlike some other world regions con-siderable gaps exist in knowledge regarding the incidence andprevalence of MS in the United States because there is norobust method for estimating either epidemiologic statistic ona national basis The only population-based estimates of MSincidence (the number of new cases of MS in a population)have been obtained in the population of Rochester Minne-sota where the presence of the Mayo Clinic enables rigorousperiodic studies of MS incidence and prevalence3 The ab-sence of a unified single health care system in the US does notenable robust estimates of MS incidence on a national leveltherefore our focus is on estimating national MS prevalencein the United States
Obtaining an accurate estimate of MS prevalence in the UnitedStates is critical because prevalence supports comparisons ofMS burden across demographic subgroups geographic regionsand time periods Health care providers and policymakers relyon prevalence estimates to make decisions about future healthservice needs Researchers studying MS need information ondisease prevalence for evaluating changes in disease frequencyin relation to changing population demographics
MS is not a reportable condition and there is no nationalpopulation-based registry for MS Although many studiesexamining the prevalence of MS in select US communitieshave been conducted in the past 25 years4 the variablemethodology and quality of these studies prevent the datafrom being aggregated into a single robust national estimate ofMS in the United States
In 2014 the National Multiple Sclerosis Society establishedthe MS Prevalence Working Group a group composed ofscientists (neurologists epidemiologists statisticians) andpolicy advocates from the United States and Canada to ob-tain a valid estimate of MS prevalence in the United StatesWe sought to evaluate possible methods for estimating MSprevalence in the current health care era with the ultimate goalof providing a scientifically sound estimate of the overallprevalence of MS in the United States
We review MS prevalence studies conducted in the UnitedStates critically examine possible methods for estimatingnational MS prevalence and use this information to develop
a rationale for a new 4-step paradigm for estimating MSprevalence in the United States
Previous estimates of MS prevalencein the United StatesRegional MS prevalence studiesA recent systematic review4 identified 9 population-based MSprevalence studies conducted in small regions of the UnitedStates between 1985 and 2011 (table e-1 httpsdoiorg105061dryadt1k42p8) MS point prevalence was lowest in the19 counties surrounding Lubbock Texas (age-standardizedprevalence 399100000 95 confidence interval [CI]340ndash457)5 and highest in Olmstead County Minnesota(age-standardized prevalence 1912100000 95 CI1656ndash2168)3 A noteworthy advantage of such regionalstudies is that the relatively small population size enablesinvestigators to use many overlapping methods to ascertainpossible MS cases in the study population (case ascertain-ment) and apply standardized criteria to determine whichcases have MS (case definition) Regional MS prevalencestudies have used a variety of methods to maximize thecompleteness of case ascertainment with the most commonsources being specialty clinics or academic MS centerscommunity neurologists or other physicians patient serviceassociations nursing homes or long-term care facilities anddeath certificates4 Case definitions are usually establishedusing medical chart reviews abstracted to apply standard di-agnostic criteria6 However because MS prevalence can haveconsiderable geographic variation4 projecting estimates fromone or a few regions to the entire United States is of uncertainvalidity
National MS prevalence studies in theUnited StatesFor a country the size of the United States (310 millionpopulation in 2010) it is not feasible to use the intensive caseascertainment methods that are routine in smaller geographicregions In the last 4 decades 4 studies have estimated theprevalence of MS in the United States by using methodsintended to provide representative samples of the US pop-ulation (table 1) The first study was conducted in 1976 usinga probability sample of 725 acute short-term general hospitalsand 8800 physicians in the contiguous United States andsurveying them to estimate the number of persons with MSwith whom they had contact7 MS prevalence was estimatedto be 58 per 100000 population corresponding to 123000
GlossaryAHC = administrative health claims BRFSS = Behavioral Risk Factor Surveillance Survey CI = confidence interval DMT =disease-modifying treatment DOD = Department of Defense ICD-9 = International Classification of Diseasesndash9 MEPS-HC = Household Component of the Medical Expenditure Panel Survey MS = multiple sclerosis NHIS = National HealthInterview Survey SWOT = strengths weaknesses opportunities and threats VHA = Veterans Health Administration
470 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
cases in the United States but Anderson et al8 believed thatthe prevalence of MS was underestimated due to severalmethodologic factors A primary source of underascertain-ment was relying on physician recall to identify MS cases as atthe time these studies were conducted computerized medicalrecords systems were rare Another source of under-ascertainment was the single-year surveillance window whichwould havemissed patients withMSwho did not seekmedicalattention for MS during that year Evidence for a third sourceof underascertainment came from a prevalence survey con-ducted in the Weld and Larimer Counties of northern Col-orado9 which used multiple case ascertainment methods andfound that 21 of all prevalent cases identified came exclu-sively from the records of 3 MS service organizations inColorado a source that was not used in the 1976 study7
Anderson et al8 used several adjustments for these sources ofunderascertainment to provide an updated estimate of MSprevalence in the United States in 1990 ranging from 250000to 350000 persons
The next 2 national MS prevalence studies were conductedusing the National Health Interview Survey (NHIS) an annualprobability sample of the noninstitutionalized US populationDuring 1982ndash1996 one-sixth of the NHIS sample was sur-veyed about MS and other health conditions resulting in lim-itation of activity Collins10 used NHIS data for a 3-year period(1990ndash1992) to estimate national MS prevalence becausea single year of data did not yield enough persons with MS forstable estimation MS prevalence was estimated to be 70 per100000 corresponding to an estimated count of 180000 casesA second study also used NHIS data over 1982ndash199611 MSprevalence was estimated to be 85 per 100000 populationcorresponding to an estimated count of 211000 cases in theUnited States (95 CI 191000ndash231000) A major weaknessof the NHIS studies is that survey data were collected from onefamily member within each sampled household who reportedthe medical conditions for the entire household This method
would underestimate MS prevalence if household membersunderreport the condition but could also overestimate MSprevalence if self-reported data resulted in the inclusion ofprovisional cases (or noncases) who would not meet formalcase definition criteria
More recently a national MS prevalence study was carried outusing the Household Component of the Medical ExpenditurePanel Survey (MEPS-HC) a nationally representative surveyof the US civilian noninstitutionalized population drawn fromNHIS that collects data on health status health utilizationhealth costs and health insurance coverage12 MS cases wereidentified on the basis of having one or more medically codeddiagnoses of MS (ICD-9 code 340) Between 1998 and 2009526 MEPS-HC participants met this criterion and the annualaverage number of persons with MS was estimated to be572312 (95 CI 397004ndash747619) Requiring only 1 ICD-9code during the study year could have overestimated MSprevalence if false-positives were included because individualswho had a single ICD-9 340 code were ultimately not di-agnosed with MS or the code was entered erroneously TheMEPS-HC probability sample only captured non-institutionalized persons with MS which could have resultedin underascertainment because it excludes the estimated5ndash10 of persons with MS residing in nursing homes1314
Two studies have used administrative health claims (AHC)data to estimate the number of persons with MS Both studiesassessed subpopulations of the United States and then usedthis information to estimate the total number of persons withMS in the United States as a whole (table 2) Pope et al15
obtained administrative claims data from privately insuredindividuals those aged into Medicare and Medicaid blind ordisabled populations to determine the prevalence of MS in 6states for 1991ndash1997 MS prevalence (per 100000 pop-ulation) was estimated to be 240 in the privately insured 180among Medicare age 65 and above and 710 among Medicaid
Table 1 Epidemiologic studies ofmultiple sclerosis (MS) prevalence in theUnited States using probability sample surveys
ReferenceAuthors(year)
Studyyears Case definition Population
National MSprevalence per100000population
Number of personswith MS in theUnited States (95CI)
Baum andRothschild(1981)7
1976 Survey of physicians and hospitalsasked to report patients meetinguniform criteria for probable andpossible MS
National sample of 8800physicians and 725 hospitalsa probability sample of the 1976 USpopulation
58 per 100000(all ages)
123000
Collins(1997)10
1990ndash1992 Patients or family members reportingphysician-diagnosed MS
NHIS a household probabilitysample of US population
70 per 100000(all ages)
180000
Noonanet al (2002)11
1982ndash1996 Patients or family members reportingphysician-diagnosed MS
NHIS a household probabilitysample of US population
85 per 100000(all ages)
211000(191000ndash231000)
Campbellet al (2014)12
2008ndash2009 Patients having 1 or more medicalclaims with MS diagnostic code 340during a single year
MEPS-HC a household probabilitysample of US population
191 per 100000(ge18 years)
572312(397004ndash747619)
Abbreviations CI = confidence intervalMEPS-HC =Household Component of theMedical Expenditure Panel Survey NHIS =National Health Interview Survey
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 471
disabled populations These estimates are not strictly com-parable due to the different age distributions and the expec-tation that MS prevalence would be much higher in theMedicaid disabled population In addition no algorithm wasdeveloped or used for MS cases Dilokthornsakul et al16 es-timatedMS prevalence for 2008ndash2012 in the privately insuredUS population by applying a case definition algorithm usingthe PharMetrics Plus Health Plan Claims data a large USprivate insurance claims database that contained claims datafor approximately 42 million enrollees in 2011 The casedefinition algorithm required at least 2 inpatient claims withICD-9 code 340 at least 3 ICD-9 code 340 outpatient claimsor at least one MS-specific disease-modifying treatment(DMT) claim The estimated MS prevalence for 2012 was149 per 100000 (95 CI 1476ndash1509) and when extrapo-lated to the United States as a whole yielded an estimate of403630 individual cases (95 CI 387445ndash419833)
Methods for conducting a nationalstudy of MS prevalence in thecurrent eraBefore designing our study to estimate the US prevalenceof MS the working group members carried out a strengthsweaknesses opportunities and threats (SWOT) analysis for 3approaches to estimate MS prevalence (1) population-basedMS registries (table 3) (2) national probability health surveys(table 4) and (3) analysis of AHC databases (table 5) Studiesof each type were evaluated as potential sources for estimatingthe national prevalence ofMS based on the populations studied
Population-based MS registriesLongstanding MS registries have been successfully used toestimate MS prevalence in 4 countries Denmark1718 Swe-den19 Norway20 and Poland21 However a similar USpopulation-based MS registry does not exist In the UnitedStates there are several voluntary MS registries for conduct-ing outcomes research however none of these registriesattempts the near-complete case ascertainment in a definedgeographic region that would enable the estimation of MSprevalence The benefits and pitfalls of population-baseddisease registries were recently reviewed22 and are summa-rized in table 3 A nationwide population-based registry wouldbe costly to implement however it is possible that a geo-graphically representative system of regional registries couldbe implemented similar to the approach used for cancersurveillance23 In the United States only one neurologic dis-ease registry has been implemented The National Amyo-trophic Lateral Sclerosis Registry was established bya Congressional mandate and began estimating nationalamyotrophic lateral sclerosis prevalence in 20102425
National probability health surveysThe primary method used to estimate national MS prevalencein the past has been probability health surveys Howeveralmost none of the national probability surveys conducted bythe US government are sufficiently large enough to containenough people with MS to enable precise estimation of MSprevalence much less prevalence within demographic or re-gional subgroups Moreover the national survey that onceallowed an overall estimate of MS prevalence (NHIS) nolonger includes questions about MS and other disablingconditions National probability survey data rely on patient or
Table 2 Epidemiologic studies of multiple sclerosis (MS) prevalence in large regions of the United States usingadministrative health claims databases
ReferenceAuthors (year)
Studyyears Case definition Population
National MSprevalence per100000 population(95 CI)
Number ofpersons with MSin the UnitedStates (95 CI)
Popeet al (2002)15 1994ndash1997 One ormore ICD-9 codes for MS(diagnosis code 340)
Nationally representative samplesof administrative claims from 6states (California ColoradoGeorgia Michigan MissouriTennessee)
Privately insured (MedstatMarketScan database)
240 per 100000(95 CI NR) (all ages)
NR
Medicare age 65 and above 180 per 100000(95 CI NR) (age ge65)
NR
Medicaid disabled population allages
710 per 10000 (95CI NR) (all ages)
NR
Dilokthornsakulet al (2016)16
2012 At least 2 inpatient claims withICD-9 code 340 at least 3 ICD-9code 340 outpatient claims orat least 1 MS-indicated DMT
Commercially insured population(Truven Market-Scan)
149 per 100000(1475ndash1508) (allages age-adjustedto US 2012population)
403630(387445ndash419833)
Abbreviations CI = confidence interval DMT = disease-modifying treatment ICD-9 = International Classification of Diseasesndash9 NR = not reported
472 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
family member reports of physician-diagnosed MS1012 risk-ing the inclusion of false-positive MS cases or provisionalcases that would not meet formal case definition criteria Onlyone national survey the Behavioral Risk Factor SurveillanceSurvey (BRFSS) which surveys more than 500000 individ-uals each year has a sample size that would potentially yieldprecise estimates of MS prevalence Feasibility work would beneeded to determine if this BRFSS could be used for thispurpose
Administrative health claims dataIn other countries with universally funded health care systemssuch as Canada and many European nations AHC databaseshave been used to provide a population-based alternative to thetraditional intensive methods of case ascertainment used inregional studies1 In the United States AHC data are main-tained by government (public) insurance programs includingMedicare andMedicaid and by private (commercial) insuranceproviders AHC databases are a tremendous resource forstudying neurologic disease incidence and prevalence becauseof their rich prospective data on patients from defined pop-ulations and their use of the standardized international disease-coding framework (using the ICD system)26 However AHCdatabases are not created for research purposes making it
necessary to demonstrate the validity and the accuracy of caseascertainment algorithm prior to using them for estimatingdisease prevalence These challenges exist for estimating prev-alence of all other common chronic neurologic conditions26
AHC data sources have potential strengths and limitationswhen applied for the purpose of estimating disease prevalence(table 5) The information from AHC databases begins withenrollment into health insurance plans and provides a stan-dardized source of longitudinal patient health care utilizationThese data contain near complete capture of demographic in-formation (sex date of birth raceethnicity zip code or state ofresidence) and health care utilization data including diagnosticcodes and pharmacy records They can be used for researchwithout specific consent because the databases are de-identified Identifying persons with MS through pharmacyrecords is an excellent case ascertainment strategy given thatmany of the DMTs are prescribed only for MS thus the per-sons withMS using suchmedications are highly likely to be trueMS cases However over 40 of persons withMS in theUnitedStates do not take DMTs necessitating additional case-findingmethods Because clinical details are often not available such aswhether a diagnostic code was entered by a neurologist phy-sician or nonphysicianmost claims database studies have reliedon case-finding algorithms that have not been judged against
Table 3 Strengths weaknesses opportunities and threats (SWOT) analysis using population-based multiple sclerosis(MS) registries to estimate national MS prevalence in the US
Strengths Weaknesses Opportunities Threats
Multiple overlapping caseascertainment methods areused to yield a high degree ofcase ascertainment
Organizational demands makea nationwide registry infeasible in theUnited States with rare exceptions(National Amyotrophic LateralSclerosis Registry2425)
A systematic approach could bedeveloped to extrapolate results frommultiple regional registries to nationalMS prevalence howevera geographically valid sample of selectstates would need to be selected torepresent the nation
If registry relies on patientvolunteers or requires consenta large degree of nonresponse canseriously affect the validity of theregistry
Data are rigorously collected forresearch purposes according tostandard protocols
Very high cost to implement inpopulation-based regions possiblyinfeasible for nationwideimplementation in the United States
For regions where registryparticipation is high can obtain validand precise estimates of MSprevalence
Confirming clinician diagnoses iscostly and impractical for largenumbers of patients
Some US registries rely in parton case ascertainment throughneurologists primary carephysicians and hospitals
In the United States registries oftenalso rely on MS diagnosis reported bypatient or family member whichmight be misreported medical chartsmay be requested for verification ofcase definition but may be difficult toobtain for all patients in a population-based registry
Need to collect patient identifiers toidentify duplicates identified bymore than one case ascertainmentmethod (risks HIPAAnoncompliance)
Data can be collected on raceethnicity and othersociodemographiccharacteristics
Registries often contain moreclinical details (eg initialsymptomatology clinicalcourse disability status) than doother sources
Abbreviation HIPAA = Health Insurance Portability and Accountability ActWith the exception of studies conducted by Mayo Clinic researchers in Rochester Minnesota17 population-based MS registries do not exist in the UnitedStates However there are several notable population-basedMS registries in Europe that enable ongoing estimation of nationalMS incidence andprevalenceincluding in Denmark1718 Sweden19 Norway20 and Poland21 Such studies often rely on case ascertainment through multiple data sources includingneurologists primary care physicians and hospitals
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 473
case definitions or even neurologist diagnoses for accuracyTwo studies used a case definition that required only a singlehealth care encounter for MS1215 which is likely to be highlynonspecific risking an unknown number of false-positives Thestudy by Dilokthornsakul et al16 that used private insuranceclaims data was strengthened by conducting sensitivity analysesthat examined the performance of 2 alternative algorithms oneof which produced estimates very similar to the primaryalgorithm
Developing a new approach forestimating MS prevalence in theUnited StatesBased on the SWOT analysis and through discussion andconsensus we concluded that AHC data would provide themost cost-effective method to develop a national prevalenceestimate for MS Collectively government and private healthclaims databases represent a very large proportion of the USpopulation (84 in 2010)28 which together enables preciseestimates of MS prevalence The data are sufficiently distrib-uted geographically and socioeconomically to be representa-tive of the entire US population Figure 1 illustrates a new4-step approach we devised for estimating the prevalence ofMS for the United States as a whole using a segmental
approach for each insurance source and then combining theminto a national estimate
Step 1 Identify datasets covering US publicly and privatelyinsured populations figure 2 illustrates the fragmented natureof insurance coverage of the US population which doesnot enable a single health care source for estimating MSprevalence as is often available in Scandinavian countries withnational unified health care systems Nevertheless AHC dataare available for almost all of the insurance segments of theUS population allowing the estimation of MS prevalenceseparately for each insurance segment which can then beaggregated into an overall national estimate ofMS prevalenceFigure 2 shows US Census Current Population Survey datafor 2008ndash2010 presented separately for individuals under age65 vs those ages 65 and older because the sources of insurancecoverage vary considerably for these 2 age groups In 2010 forindividuals below age 65 private insurance comprised thelargest segment of insurance coverage 65 when employer-purchased and self-purchased private insurance were consid-ered together The next largest segment of insurance coveragein 2010 for individuals under age 65 is Medicaid (17)a government insurance program that provides free medicalinsurance to low-income people Smaller percentages ofindividuals under age 65 in 2010 were covered by a militarysource such as Department of Defense (DOD) or Veterans
Table 4 Strengths weaknesses opportunities and threats (SWOT) analysis using national probability survey samples toestimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can be obtained from existinggovernment surveys
Dedicated MS-specific patientsurveys are costly to carry out andinfeasible for national scope
This method can be feasible ifmultiple years of survey data can beaggregated
Existing national probabilitysamples usually comprise onlysegments of the US population(ie noninstitutionalized)
Sampling designs are rigorous(probability samples) of the USpopulation rigorously collected forresearch purposes according tostandard protocols
Survey participation rates are athistorically low levels
Successful application would requireaccess to a very large survey samplesuch as the BRFSS conducted annuallyby the CDC however a geographicallyvalid sample of select states wouldneed to be selected to represent thenation
Survey questions for patients andfamily members have not beenvalidated for accuracy againsta gold standard (neurologistdiagnosis)
Data are accessible and either cost-free or low-cost
Surveys rely on MS diagnosisreported by patient or a familymember which are susceptible toboth underreporting and false-positive reports
If survey questions were validatedagainst a gold standard (neurologistdiagnosis) this method could befeasibly implemented in a subset ofUS states
Restrictions on number ofquestions limits collection ofclinical details (eg clinicalcourse disability status)
Data are available on age sex raceethnicity broad geographic locationand other sociodemographiccharacteristics
Count ofMS patients in single yearsof data are often too small forprecise estimation
Some surveys collect self-reporteddata that can inform other analyseseg prevalence of comorbidity healthcare utilization and cost DMT uselifestyle risk factors
Overall prevalence might beestimable but data are often toosparse for getting breakdowns bysex age race or geographic region
Abbreviations BRFSS = Behavioral Risk Factor Surveillance Survey CDC = Centers for Disease Control and Prevention DMT = disease-modifying treatmentIn the United States national probability survey samples include the National Health Interview Survey Medical Expenditure Panel Survey HouseholdComponent National Nursing Home Survey and the BRFSS (a probability survey completed by500000 Americans per year and for which disease-specificquestions can be added on a state-by-state basis)
474 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Health Administration (VHA) (4) or by anothergovernment-provided insurance plan (Medicare 3) In2010 18 of individuals under age 65 had no insurancecoverage In 2010 for individuals ages 65 and abovegovernment insurance provided by Medicare covered 93of the population and was often supplemented by privatecoinsurance (33 employer-provided 29 self-purchased)Medicaid either alone or in combination with Medicarecovered 9 of those age 65 and above In 2010 8 ofindividuals age 65 and above were covered by amilitary source(DOD or VHA) and only 2 of the elderly were uninsuredThus despite the fragmentation of the US health care systemAHC databases for all of the insured segments of the USpopulation are available and can be used to estimate MSprevalence in each dataset separately before combining theestimates into a whole (step 4)Step 2 Develop and validate a highly accurate MS case-finding algorithm that can be standardly applied in all AHCdatabases Our approach requires a highly accurate casedefinition to identify MS cases that performs consistently
across AHC databases with differing characteristics so thatit can be applied even in datasets where formal validationis not possible Notably no MS prevalence studies in theUnited States have used validated algorithms for identifyingpersons with MS yet having a validated algorithm for thispurpose is a necessary step for carrying out valid prevalenceestimation26 Culpepper et al27 recently conducted a multi-site validation study to develop a valid and reliable algorithmfor identifying MS cases using AHC data with excellentsensitivity specificity and positive predictive value For thefirst time ever this provides a high-performing algorithmthat performs consistently well across datasets and can beapplied across all AHC databases Similar methodologycould be employed for other chronic neurologic diseasesusing existing literature to provide a starting point for thedevelopment of such case definitions26
Step 3 Apply the case definition algorithm to estimate thenumber of MS cases and prevalence estimates separately foreach database The third step of this approach is simply touse the validated algorithm (step 2) within each of the
Table 5 Strengths weaknesses opportunities and threats (SWOT) analysis using administrative health claims databasesto estimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can develop systematic approachthat could be repeatedly utilizedover time to obtain estimates nowand in the future
Lack of universal health care in theUnited States therefore not allpatients are identifiable throughadministrative data
Can develop a systematic approachthat can be repeatedly utilized overtime to obtain estimates now and inthe future
Lack of certainty whether casedefinitions developed in one datasetwill have same performancecharacteristics in other datasets
Data are accessible and relativelylow-cost
Must accessmultiple administrativedatasets
A case definition can be validated in2 or 3 different administrativedatasets to show consistency offindings across datasets thenapplied even in datasets wherevalidation is not possible4
No easily accessible national sourceof data for uninsured or self-paypopulations
Consistent capture of sex and dateof birth supports calculation of age-and sex-specific prevalenceestimates
Data are collected for health systemmanagement therefore theirvalidity for research must becarefully assessed
If a careful analytic approach is usedcan minimize overlap betweendatasets and avoid duplicatecounting
No easily accessible data forincarcerated or aboriginalpopulations
Data often include zip code whichcan be geocoded to determinesocioeconomic status and establishregion of residence
Lack of identified data to enableidentification of duplicates createsdifficulty identifying the sameindividuals in overlapping datasets
Would ideally include collection ofpatient identifiers to identifyduplicates present inmore than onedatabase howevernongovernment researchers arenot allowed access to suchidentifiers
These databases often haveadditional information that couldinform other analyses egprevalence of comorbidity healthcare utilization and disease-modifying treatment use
Some datasets lack informationregarding raceethnicity or havepoor geographic resolution
Representativeness cannot accessall administrative health databasesin United States must select few toestimate MS prevalence andextrapolate to all
Issue of misdiagnosis as a source oferror lack of clinical detail makes itdifficult to distinguish inaccuratelycoded diagnoses from clinicianmisdiagnosis
In the United States administrative health claims databases include Medicare (a government insurance program covering 93 of US residents age 65 andabove) Medicaid (a government insurance program for low-income parents and children and disabled persons in the United States) the Minimum Data Set(administrative data onMedicare- or Medicaid-certified nursing facilities) the Veterans Health Administration (health care program for veterans of US wars)commercial health insurance claims data (for employer-paid or self-paid insurance) and health maintenance organization health records
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 475
databases (step 1) to obtain valid MS prevalence estimates(overall and specific with respect to age sex raceethnicityand geographic location)Step 4 CombineMSprevalence estimates into a single estimateof the prevalence of MS for the United States weightedaccording to the number of insured persons in each healthinsurance segment after obtaining MS prevalence estimatesseparately for each of the US health insurance segments theycan be combined into a single national prevalence estimateInformation from theCurrent Population Survey can be used toobtain the necessary weights by determining the number of USresidents with each type of insurance coverage stratified by sexage group race and geographic region The total estimatednumber of MS cases for each age sex race and geographicregionndashspecific category can then be summed to estimatethe total number ofMS cases in the United States For exampleMS prevalence for the private insurance segment can beestimated by accessing AHC data for Optum (Eden PrairieMN) and Truven Health (Ann Arbor MI) which in 2010together comprise approximately 68 million individuals or 35of the 2010 privately insured US population MS prevalence inthe government-insured segment of the population can bedirectly and completely estimated for 100 of people coveredby using administrative claims data for Medicaid and MedicareMS prevalence in the military population which is pre-dominantly male can be estimated used the Veterans HealthAdministration database A limitation of this method is that noclaims data exist for persons without health insurance estimatedat 163 in 201028 however for this uninsured group MSprevalence estimates from the Medicaid health care claims datacould be applied because the 2 groups have similar sociodemo-graphic characteristics
Our new approach cannot be applied to estimate the in-cidence of MS in the United States Incidencemdashthe number
of new MS cases per year in a populationmdashis an importantmeasure of disease frequency However it can only be derivedfor countries that have single uniform health care systemswhere longitudinal AHC records for each person enable rel-atively precise indicators of the onset of new MS diagnosisand the exclusion of existing prevalent cases The lack ofa single payer health care system or national tracking systemin the United States does not allow reliable estimates of MSincidence because some individuals may change health carecoverage over time and it is not possible to link patientrecords across insurance sources to provide a single longi-tudinal record within which newly diagnosed persons withMS may be ascertained This creates short periods of ob-servation which do not allow accurate estimates of incidencefor conditions such as MS and cancer due to the inability todefinitively determine which individuals are truly newlydiagnosed29
DiscussionWe have proposed a new approach for applying validatedcase-finding algorithms to AHC data from both governmentand private sources to produce robust estimates of MSprevalence in the United States In a companion article weapplied this approach to estimate the total number of MScases in the United States30 This approach could be appliedto estimate prevalence of other neurologic disorders andchronic conditions that face similar methodologic challengessuch as Parkinson disease dementia and epilepsy
There are several reasons why our new approach is a valuablemethodologic development to estimate the national MSprevalence First this paradigm offers the potential to useexisting AHC data for case ascertainment across the UnitedStates without requiring the cost and effort involved in re-gional MS prevalence studies which typically employ in-tensive case ascertainment methods The data are sufficientlydistributed both geographically and socioeconomically tobe representative of the entire US population and do notrequire consent because the databases are de-identifiedSecond our method is efficient and cost-effective and can beapplied repeatedly with datasets that represent a large pro-portion of the country enabling updates to population-based estimates of MS prevalence over time Third applyingthis approach with data that represent the entire UnitedStates allows us to obtain more stable and precise prevalenceestimates and to fill in knowledge gaps regarding the prev-alence of MS in many regions for which we have never hadestimates Once AHC data are able to accurately and com-pletely capture race and ethnicity this approach could beapplied to racial and ethnic minorities that have receivedlittle study in the past Fourth the use of a highly accuratecase-finding algorithm4 ensures that there will be greatercomparability between estimates derived from these sourcesin the future By adopting a standard paradigm for ascer-taining MS cases and applying validated case definition
Figure 1 Stepwise process for determining the prevalenceof multiple sclerosis (MS) in the United States
476 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
criteria we will be better able to monitor and comparespatial differences in MS prevalence and to examine changesin disease prevalence over time without the variation in-troduced by differing methodologic approaches
Despite many strengths our new approach is limited in thatthe case ascertainment methods do not cover all segments ofthe US population It excludes native American residents whochoose to receive care through the Indian Health Service
Figure 2 Source of health insurance by age (estimates from the current population survey 2008ndash2010)
(A) Population younger than 65 years (B) Population 65 years of age and older
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 477
(06 of the US population in 2010)31 and US residents whoare incarcerated (approximately 05 of the US population in2010)32 If health care databases existed for these populationswe could similarly apply an MS algorithm to estimate MSprevalence and incorporate them into the overall nationalestimate Our approach also cannot distinguish between dif-ferent racial and ethnic groups thus we cannot address towhat extent variations in prevalence by geography or otherfactors may be better explained by racialethnic differences inprevalence33
Our work has important implications for the new era of MSepidemiologic research that will be possible through the 21stCentury Cures Act legislation enacted in December 2016which authorized the establishment of a federally fundedneurologic disorders surveillance system34 A national registryfor MS could be implemented similar to the NationalAmyotrophic Lateral Sclerosis Registry with AHC data asa primary method for case ascertainment and a web portalavailable for all persons with MS to register242535 Withoutaccess to a national registry in the intermediate term wepropose that our approach will deliver the most current andscientifically sound US estimate of the number of personswith MS By addressing methodologic challenges and pro-posing a new paradigm for measuring the prevalence of MS inthe United States we hope that our work will benefit scientistswho study all chronic conditions for which national preva-lence estimates do not currently exist
AcknowledgmentThe authors thank the following members of the US MultipleSclerosis Prevalence Workgroup for their contributionsAlbert Lo Robert McBurney Oleg Muravov Bari Talenteand Leslie Ritter The authors also thank the following keystaff members at the National Multiple Sclerosis Society fortheir contributions to this project Cathy Carlson TimCoetzee Sherri Giger Weyman Johnson Eileen MadrayGraham McReynolds and Cyndi Zagieboylo
Study fundingThe study was funded by contracts from the National Mul-tiple Sclerosis Society to the principal investigators in the MSPrevalence Working Group (HC-1508-05693) The ArticleProcessing Charge was funded by the National MultipleSclerosis Society
DisclosureL Nelson receives grants from the Centers for DiseaseControl and Prevention NIH and National Multiple Scle-rosis Society and contracts from the Agency for Toxic Sub-stances and Diseases Registry She receives compensation forserving as a consultant to Acumen Inc and is on the DataMonitoring Committee of Neuropace M Wallin has servedon data safety monitoring boards for the National Institutes ofNeurological Disease and StrokendashNIH has been an associateeditor for the Encyclopedia of the Neurological Sciences andreceived funding support from the National Multiple Sclerosis
Society and the Department of Veterans Affairs Merit ReviewResearch Program R Marrie is supported by the WaughFamily Chair in Multiple Sclerosis receives research fundingfrom Canadian Institutes of Health Research ResearchManitoba Multiple Sclerosis Society of Canada MultipleSclerosis Scientific Foundation National Multiple SclerosisSociety and Rx amp D Health Research Foundation and hasconducted clinical trials funded by Sanofi-Aventis She alsoserves on the Editorial Board ofNeurologyregW Culpepper hasadditional research funding from the National MultipleSclerosis Society receives support from the VHA MS Centerof Excellence and is a member of the National MultipleSclerosis Society Health Care Delivery and Policy Researchstudy section A Langer-Gould is site principal investigatorfor 2 industry-sponsored phase 3 clinical trials (BiogenIdec Hoffman-LaRoche) and was site PI for one industry-sponsored observation study (Biogen Idec) She receivesgrant support from the NIH National Institute of Neuro-logical Disorders and Stroke Patient-Centered OutcomesResearch Institute and the National Multiple Sclerosis Soci-ety J Campbell has consultancy or research grants over thelast 5 years with Agency for Healthcare Research and QualityALSAM Foundation Amgen AstraZeneca Bayer BiogenIdec Boehringer Ingelheim Centers for Disease Control andPrevention Colorado Medicaid Enterprise CommunityPartners Inc Institute for Clinical and Economic ReviewMallinckrodt NIH National Multiple Sclerosis Society Kai-ser Permanente PhRMA Foundation Teva Research in RealLife Ltd Respiratory Effectiveness Group and Zogenix IncS Buka receives research funding from the NIH and theNational Multiple Sclerosis Society H Tremlett is theCanada Research Chair for Neuroepidemiology and MultipleSclerosis She receives research support from the NationalMultiple Sclerosis Society the Canadian Institutes of HealthResearch the Multiple Sclerosis Society of Canada and theMultiple Sclerosis Scientific Research Foundation In addi-tion in the last 5 years she has received research support fromthe Multiple Sclerosis Society of Canada the Michael SmithFoundation for Health Research and the UK MS Trust andspeaker honoraria andor travel expenses to attend confer-ences G Cutter is a member of Data and Safety MonitoringBoards for AMO Pharmaceuticals Apotek Horizon Phar-maceuticals ModigenetechProlor Merck MerckPfizerOpko Biologics Neurim Sanofi-Aventis Reata Pharmaceut-icals ReceptosCelgene Teva pharmaceuticals NHLBI(Protocol Review Committee) and NICHD (OPRU over-sight committee) and is on the Consulting or AdvisoryBoards for Atara Biotherapeutics Argenix Bioeq GmbHConsortium of MS Centers (grant) Genzyme GenentechInnate Therapeutics Klein-Buendel Incorporated Medi-mmune Medday Novartis Opexa Therapeutics RocheSavara Inc Somahlution Teva Pharmaceuticals Trans-parency Life Sciences and TGTherapeutics W Kaye receivesfunding from the Agency for Toxic Substances and DiseaseRegistry the National Multiple Sclerosis Society and theAssociation for the Accreditation of Human ResearchProtection Programs L Wagner receives funding from the
478 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Agency for Toxic Substances and Disease Registry and Na-tional Multiple Sclerosis Society N LaRocca is employed fulltime by the National Multiple Sclerosis Society and has noother disclosures to report Statistical analysis conducted byDr Gary Cutter PhD University of Alabama at BirminghamGo to NeurologyorgN for full disclosures
Publication historyReceived byNeurology July 17 2018 Accepted in final form October 222018
References1 Wallin MT Kurtzke JF Neuroepidemiology In Bradley WG Daroff RB Fenichel
GM Jankovic J editors Neurology in Clinical Practice Philadelphia Butterworth-Heinemann 2008762ndash780
2 Browne P Chandraratna D Angood C et al Atlas of multiple sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
3 Mayr WT Pittock SJ McClelland RL Jorgensen NW Noseworthy JH Rodriguez MIncidence and prevalence of multiple sclerosis in Olmsted County Minnesota 1985-2000 Neurology 2003611373ndash1377
4 Evans C Beland SG Kulaga S et al Incidence and prevalence of multiple sclerosis inthe Americas a systematic review Neuroepidemiology 201340195ndash210
5 Noonan CW Williamson DM Henry JP et al The prevalence of multiple sclerosis in3 US communities Prev Chronic Dis 20107A1
6 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
7 Baum HM Rothschild BB The incidence and prevalence of reported multiple scle-rosis Ann Neurol 198110420ndash428
8 Anderson DW Ellenberg JH Leventhal CM Reingold SC Rodriguez M SilberbergDH Revised estimate of the prevalence of multiple sclerosis in the United States AnnNeurol 199231333ndash336
9 Nelson LM Hamman RF Thompson DS et al Higher than expected prevalence ofmultiple sclerosis in Northern Colorado dependence on methodological issuesNeuroepidemiology 1986517ndash28
10 Collins JG Prevalence of selected chronic conditions United States 1990-1992 VitalHealth Stat 10 19971941ndash89
Appendix 1 Authors
Name Location Role Contribution
Lorene MNelsonMS PhD
Stanford UniversityCA
Author Study concept anddesign preparation ofdraft manuscriptrevision of themanuscript forcontent approval offinal manuscript
Mitchell TWallin MDMPH
Veterans HealthAdministrationGeorgetownUniversityWashington DC
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
Ruth AnnMarrieMD PhD
University ofManitoba WinnipegCanada
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
William JCulpepperPhD MA
Veterans HealthAdministrationWashington DCUniversity ofMaryland Baltimore
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
AnnetteLanger-GouldMD PhD
Kaiser PermanenteSouthern CaliforniaLos Angeles
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
JonathanCampbellPhD
University of DenverCO
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
StephenBuka PhD
Brown UniversityProvidence RI
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
HelenTremlettPhD
University of BritishColumbia VancouverCanada
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
GaryCutterPhD
University ofAlabamaBirmingham
Author Study concept anddesign critical reviewof the manuscript forcontent
Appendix 1 (continued)
Name Location Role Contribution
WendyKaye PhD
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
LaurieWagnerMPH
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Nicholas GLaRoccaPhD
National MultipleSclerosis Society NewYork NY
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Appendix 2 Coinvestigators and members of the USMultiple Sclerosis Prevalence Workgroup
Name Location Role Contribution
Albert LoMD PhD
Brown UniversityProvidence RI
Coinvestigator Studyconcept anddesign
RobertMcBurneyPhD
Accelerated CureProject Boston MA
Coinvestigator Studyconcept anddesign
OlegMuravovPhD
Agency for ToxicSubstances andDisease RegistryDivision of HealthStudies Atlanta GA
Coinvestigator Studyconcept anddesign
BariTalenteEsq
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
LeslieRitter
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 479
11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

cases in the United States but Anderson et al8 believed thatthe prevalence of MS was underestimated due to severalmethodologic factors A primary source of underascertain-ment was relying on physician recall to identify MS cases as atthe time these studies were conducted computerized medicalrecords systems were rare Another source of under-ascertainment was the single-year surveillance window whichwould havemissed patients withMSwho did not seekmedicalattention for MS during that year Evidence for a third sourceof underascertainment came from a prevalence survey con-ducted in the Weld and Larimer Counties of northern Col-orado9 which used multiple case ascertainment methods andfound that 21 of all prevalent cases identified came exclu-sively from the records of 3 MS service organizations inColorado a source that was not used in the 1976 study7
Anderson et al8 used several adjustments for these sources ofunderascertainment to provide an updated estimate of MSprevalence in the United States in 1990 ranging from 250000to 350000 persons
The next 2 national MS prevalence studies were conductedusing the National Health Interview Survey (NHIS) an annualprobability sample of the noninstitutionalized US populationDuring 1982ndash1996 one-sixth of the NHIS sample was sur-veyed about MS and other health conditions resulting in lim-itation of activity Collins10 used NHIS data for a 3-year period(1990ndash1992) to estimate national MS prevalence becausea single year of data did not yield enough persons with MS forstable estimation MS prevalence was estimated to be 70 per100000 corresponding to an estimated count of 180000 casesA second study also used NHIS data over 1982ndash199611 MSprevalence was estimated to be 85 per 100000 populationcorresponding to an estimated count of 211000 cases in theUnited States (95 CI 191000ndash231000) A major weaknessof the NHIS studies is that survey data were collected from onefamily member within each sampled household who reportedthe medical conditions for the entire household This method
would underestimate MS prevalence if household membersunderreport the condition but could also overestimate MSprevalence if self-reported data resulted in the inclusion ofprovisional cases (or noncases) who would not meet formalcase definition criteria
More recently a national MS prevalence study was carried outusing the Household Component of the Medical ExpenditurePanel Survey (MEPS-HC) a nationally representative surveyof the US civilian noninstitutionalized population drawn fromNHIS that collects data on health status health utilizationhealth costs and health insurance coverage12 MS cases wereidentified on the basis of having one or more medically codeddiagnoses of MS (ICD-9 code 340) Between 1998 and 2009526 MEPS-HC participants met this criterion and the annualaverage number of persons with MS was estimated to be572312 (95 CI 397004ndash747619) Requiring only 1 ICD-9code during the study year could have overestimated MSprevalence if false-positives were included because individualswho had a single ICD-9 340 code were ultimately not di-agnosed with MS or the code was entered erroneously TheMEPS-HC probability sample only captured non-institutionalized persons with MS which could have resultedin underascertainment because it excludes the estimated5ndash10 of persons with MS residing in nursing homes1314
Two studies have used administrative health claims (AHC)data to estimate the number of persons with MS Both studiesassessed subpopulations of the United States and then usedthis information to estimate the total number of persons withMS in the United States as a whole (table 2) Pope et al15
obtained administrative claims data from privately insuredindividuals those aged into Medicare and Medicaid blind ordisabled populations to determine the prevalence of MS in 6states for 1991ndash1997 MS prevalence (per 100000 pop-ulation) was estimated to be 240 in the privately insured 180among Medicare age 65 and above and 710 among Medicaid
Table 1 Epidemiologic studies ofmultiple sclerosis (MS) prevalence in theUnited States using probability sample surveys
ReferenceAuthors(year)
Studyyears Case definition Population
National MSprevalence per100000population
Number of personswith MS in theUnited States (95CI)
Baum andRothschild(1981)7
1976 Survey of physicians and hospitalsasked to report patients meetinguniform criteria for probable andpossible MS
National sample of 8800physicians and 725 hospitalsa probability sample of the 1976 USpopulation
58 per 100000(all ages)
123000
Collins(1997)10
1990ndash1992 Patients or family members reportingphysician-diagnosed MS
NHIS a household probabilitysample of US population
70 per 100000(all ages)
180000
Noonanet al (2002)11
1982ndash1996 Patients or family members reportingphysician-diagnosed MS
NHIS a household probabilitysample of US population
85 per 100000(all ages)
211000(191000ndash231000)
Campbellet al (2014)12
2008ndash2009 Patients having 1 or more medicalclaims with MS diagnostic code 340during a single year
MEPS-HC a household probabilitysample of US population
191 per 100000(ge18 years)
572312(397004ndash747619)
Abbreviations CI = confidence intervalMEPS-HC =Household Component of theMedical Expenditure Panel Survey NHIS =National Health Interview Survey
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 471
disabled populations These estimates are not strictly com-parable due to the different age distributions and the expec-tation that MS prevalence would be much higher in theMedicaid disabled population In addition no algorithm wasdeveloped or used for MS cases Dilokthornsakul et al16 es-timatedMS prevalence for 2008ndash2012 in the privately insuredUS population by applying a case definition algorithm usingthe PharMetrics Plus Health Plan Claims data a large USprivate insurance claims database that contained claims datafor approximately 42 million enrollees in 2011 The casedefinition algorithm required at least 2 inpatient claims withICD-9 code 340 at least 3 ICD-9 code 340 outpatient claimsor at least one MS-specific disease-modifying treatment(DMT) claim The estimated MS prevalence for 2012 was149 per 100000 (95 CI 1476ndash1509) and when extrapo-lated to the United States as a whole yielded an estimate of403630 individual cases (95 CI 387445ndash419833)
Methods for conducting a nationalstudy of MS prevalence in thecurrent eraBefore designing our study to estimate the US prevalenceof MS the working group members carried out a strengthsweaknesses opportunities and threats (SWOT) analysis for 3approaches to estimate MS prevalence (1) population-basedMS registries (table 3) (2) national probability health surveys(table 4) and (3) analysis of AHC databases (table 5) Studiesof each type were evaluated as potential sources for estimatingthe national prevalence ofMS based on the populations studied
Population-based MS registriesLongstanding MS registries have been successfully used toestimate MS prevalence in 4 countries Denmark1718 Swe-den19 Norway20 and Poland21 However a similar USpopulation-based MS registry does not exist In the UnitedStates there are several voluntary MS registries for conduct-ing outcomes research however none of these registriesattempts the near-complete case ascertainment in a definedgeographic region that would enable the estimation of MSprevalence The benefits and pitfalls of population-baseddisease registries were recently reviewed22 and are summa-rized in table 3 A nationwide population-based registry wouldbe costly to implement however it is possible that a geo-graphically representative system of regional registries couldbe implemented similar to the approach used for cancersurveillance23 In the United States only one neurologic dis-ease registry has been implemented The National Amyo-trophic Lateral Sclerosis Registry was established bya Congressional mandate and began estimating nationalamyotrophic lateral sclerosis prevalence in 20102425
National probability health surveysThe primary method used to estimate national MS prevalencein the past has been probability health surveys Howeveralmost none of the national probability surveys conducted bythe US government are sufficiently large enough to containenough people with MS to enable precise estimation of MSprevalence much less prevalence within demographic or re-gional subgroups Moreover the national survey that onceallowed an overall estimate of MS prevalence (NHIS) nolonger includes questions about MS and other disablingconditions National probability survey data rely on patient or
Table 2 Epidemiologic studies of multiple sclerosis (MS) prevalence in large regions of the United States usingadministrative health claims databases
ReferenceAuthors (year)
Studyyears Case definition Population
National MSprevalence per100000 population(95 CI)
Number ofpersons with MSin the UnitedStates (95 CI)
Popeet al (2002)15 1994ndash1997 One ormore ICD-9 codes for MS(diagnosis code 340)
Nationally representative samplesof administrative claims from 6states (California ColoradoGeorgia Michigan MissouriTennessee)
Privately insured (MedstatMarketScan database)
240 per 100000(95 CI NR) (all ages)
NR
Medicare age 65 and above 180 per 100000(95 CI NR) (age ge65)
NR
Medicaid disabled population allages
710 per 10000 (95CI NR) (all ages)
NR
Dilokthornsakulet al (2016)16
2012 At least 2 inpatient claims withICD-9 code 340 at least 3 ICD-9code 340 outpatient claims orat least 1 MS-indicated DMT
Commercially insured population(Truven Market-Scan)
149 per 100000(1475ndash1508) (allages age-adjustedto US 2012population)
403630(387445ndash419833)
Abbreviations CI = confidence interval DMT = disease-modifying treatment ICD-9 = International Classification of Diseasesndash9 NR = not reported
472 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
family member reports of physician-diagnosed MS1012 risk-ing the inclusion of false-positive MS cases or provisionalcases that would not meet formal case definition criteria Onlyone national survey the Behavioral Risk Factor SurveillanceSurvey (BRFSS) which surveys more than 500000 individ-uals each year has a sample size that would potentially yieldprecise estimates of MS prevalence Feasibility work would beneeded to determine if this BRFSS could be used for thispurpose
Administrative health claims dataIn other countries with universally funded health care systemssuch as Canada and many European nations AHC databaseshave been used to provide a population-based alternative to thetraditional intensive methods of case ascertainment used inregional studies1 In the United States AHC data are main-tained by government (public) insurance programs includingMedicare andMedicaid and by private (commercial) insuranceproviders AHC databases are a tremendous resource forstudying neurologic disease incidence and prevalence becauseof their rich prospective data on patients from defined pop-ulations and their use of the standardized international disease-coding framework (using the ICD system)26 However AHCdatabases are not created for research purposes making it
necessary to demonstrate the validity and the accuracy of caseascertainment algorithm prior to using them for estimatingdisease prevalence These challenges exist for estimating prev-alence of all other common chronic neurologic conditions26
AHC data sources have potential strengths and limitationswhen applied for the purpose of estimating disease prevalence(table 5) The information from AHC databases begins withenrollment into health insurance plans and provides a stan-dardized source of longitudinal patient health care utilizationThese data contain near complete capture of demographic in-formation (sex date of birth raceethnicity zip code or state ofresidence) and health care utilization data including diagnosticcodes and pharmacy records They can be used for researchwithout specific consent because the databases are de-identified Identifying persons with MS through pharmacyrecords is an excellent case ascertainment strategy given thatmany of the DMTs are prescribed only for MS thus the per-sons withMS using suchmedications are highly likely to be trueMS cases However over 40 of persons withMS in theUnitedStates do not take DMTs necessitating additional case-findingmethods Because clinical details are often not available such aswhether a diagnostic code was entered by a neurologist phy-sician or nonphysicianmost claims database studies have reliedon case-finding algorithms that have not been judged against
Table 3 Strengths weaknesses opportunities and threats (SWOT) analysis using population-based multiple sclerosis(MS) registries to estimate national MS prevalence in the US
Strengths Weaknesses Opportunities Threats
Multiple overlapping caseascertainment methods areused to yield a high degree ofcase ascertainment
Organizational demands makea nationwide registry infeasible in theUnited States with rare exceptions(National Amyotrophic LateralSclerosis Registry2425)
A systematic approach could bedeveloped to extrapolate results frommultiple regional registries to nationalMS prevalence howevera geographically valid sample of selectstates would need to be selected torepresent the nation
If registry relies on patientvolunteers or requires consenta large degree of nonresponse canseriously affect the validity of theregistry
Data are rigorously collected forresearch purposes according tostandard protocols
Very high cost to implement inpopulation-based regions possiblyinfeasible for nationwideimplementation in the United States
For regions where registryparticipation is high can obtain validand precise estimates of MSprevalence
Confirming clinician diagnoses iscostly and impractical for largenumbers of patients
Some US registries rely in parton case ascertainment throughneurologists primary carephysicians and hospitals
In the United States registries oftenalso rely on MS diagnosis reported bypatient or family member whichmight be misreported medical chartsmay be requested for verification ofcase definition but may be difficult toobtain for all patients in a population-based registry
Need to collect patient identifiers toidentify duplicates identified bymore than one case ascertainmentmethod (risks HIPAAnoncompliance)
Data can be collected on raceethnicity and othersociodemographiccharacteristics
Registries often contain moreclinical details (eg initialsymptomatology clinicalcourse disability status) than doother sources
Abbreviation HIPAA = Health Insurance Portability and Accountability ActWith the exception of studies conducted by Mayo Clinic researchers in Rochester Minnesota17 population-based MS registries do not exist in the UnitedStates However there are several notable population-basedMS registries in Europe that enable ongoing estimation of nationalMS incidence andprevalenceincluding in Denmark1718 Sweden19 Norway20 and Poland21 Such studies often rely on case ascertainment through multiple data sources includingneurologists primary care physicians and hospitals
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 473
case definitions or even neurologist diagnoses for accuracyTwo studies used a case definition that required only a singlehealth care encounter for MS1215 which is likely to be highlynonspecific risking an unknown number of false-positives Thestudy by Dilokthornsakul et al16 that used private insuranceclaims data was strengthened by conducting sensitivity analysesthat examined the performance of 2 alternative algorithms oneof which produced estimates very similar to the primaryalgorithm
Developing a new approach forestimating MS prevalence in theUnited StatesBased on the SWOT analysis and through discussion andconsensus we concluded that AHC data would provide themost cost-effective method to develop a national prevalenceestimate for MS Collectively government and private healthclaims databases represent a very large proportion of the USpopulation (84 in 2010)28 which together enables preciseestimates of MS prevalence The data are sufficiently distrib-uted geographically and socioeconomically to be representa-tive of the entire US population Figure 1 illustrates a new4-step approach we devised for estimating the prevalence ofMS for the United States as a whole using a segmental
approach for each insurance source and then combining theminto a national estimate
Step 1 Identify datasets covering US publicly and privatelyinsured populations figure 2 illustrates the fragmented natureof insurance coverage of the US population which doesnot enable a single health care source for estimating MSprevalence as is often available in Scandinavian countries withnational unified health care systems Nevertheless AHC dataare available for almost all of the insurance segments of theUS population allowing the estimation of MS prevalenceseparately for each insurance segment which can then beaggregated into an overall national estimate ofMS prevalenceFigure 2 shows US Census Current Population Survey datafor 2008ndash2010 presented separately for individuals under age65 vs those ages 65 and older because the sources of insurancecoverage vary considerably for these 2 age groups In 2010 forindividuals below age 65 private insurance comprised thelargest segment of insurance coverage 65 when employer-purchased and self-purchased private insurance were consid-ered together The next largest segment of insurance coveragein 2010 for individuals under age 65 is Medicaid (17)a government insurance program that provides free medicalinsurance to low-income people Smaller percentages ofindividuals under age 65 in 2010 were covered by a militarysource such as Department of Defense (DOD) or Veterans
Table 4 Strengths weaknesses opportunities and threats (SWOT) analysis using national probability survey samples toestimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can be obtained from existinggovernment surveys
Dedicated MS-specific patientsurveys are costly to carry out andinfeasible for national scope
This method can be feasible ifmultiple years of survey data can beaggregated
Existing national probabilitysamples usually comprise onlysegments of the US population(ie noninstitutionalized)
Sampling designs are rigorous(probability samples) of the USpopulation rigorously collected forresearch purposes according tostandard protocols
Survey participation rates are athistorically low levels
Successful application would requireaccess to a very large survey samplesuch as the BRFSS conducted annuallyby the CDC however a geographicallyvalid sample of select states wouldneed to be selected to represent thenation
Survey questions for patients andfamily members have not beenvalidated for accuracy againsta gold standard (neurologistdiagnosis)
Data are accessible and either cost-free or low-cost
Surveys rely on MS diagnosisreported by patient or a familymember which are susceptible toboth underreporting and false-positive reports
If survey questions were validatedagainst a gold standard (neurologistdiagnosis) this method could befeasibly implemented in a subset ofUS states
Restrictions on number ofquestions limits collection ofclinical details (eg clinicalcourse disability status)
Data are available on age sex raceethnicity broad geographic locationand other sociodemographiccharacteristics
Count ofMS patients in single yearsof data are often too small forprecise estimation
Some surveys collect self-reporteddata that can inform other analyseseg prevalence of comorbidity healthcare utilization and cost DMT uselifestyle risk factors
Overall prevalence might beestimable but data are often toosparse for getting breakdowns bysex age race or geographic region
Abbreviations BRFSS = Behavioral Risk Factor Surveillance Survey CDC = Centers for Disease Control and Prevention DMT = disease-modifying treatmentIn the United States national probability survey samples include the National Health Interview Survey Medical Expenditure Panel Survey HouseholdComponent National Nursing Home Survey and the BRFSS (a probability survey completed by500000 Americans per year and for which disease-specificquestions can be added on a state-by-state basis)
474 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Health Administration (VHA) (4) or by anothergovernment-provided insurance plan (Medicare 3) In2010 18 of individuals under age 65 had no insurancecoverage In 2010 for individuals ages 65 and abovegovernment insurance provided by Medicare covered 93of the population and was often supplemented by privatecoinsurance (33 employer-provided 29 self-purchased)Medicaid either alone or in combination with Medicarecovered 9 of those age 65 and above In 2010 8 ofindividuals age 65 and above were covered by amilitary source(DOD or VHA) and only 2 of the elderly were uninsuredThus despite the fragmentation of the US health care systemAHC databases for all of the insured segments of the USpopulation are available and can be used to estimate MSprevalence in each dataset separately before combining theestimates into a whole (step 4)Step 2 Develop and validate a highly accurate MS case-finding algorithm that can be standardly applied in all AHCdatabases Our approach requires a highly accurate casedefinition to identify MS cases that performs consistently
across AHC databases with differing characteristics so thatit can be applied even in datasets where formal validationis not possible Notably no MS prevalence studies in theUnited States have used validated algorithms for identifyingpersons with MS yet having a validated algorithm for thispurpose is a necessary step for carrying out valid prevalenceestimation26 Culpepper et al27 recently conducted a multi-site validation study to develop a valid and reliable algorithmfor identifying MS cases using AHC data with excellentsensitivity specificity and positive predictive value For thefirst time ever this provides a high-performing algorithmthat performs consistently well across datasets and can beapplied across all AHC databases Similar methodologycould be employed for other chronic neurologic diseasesusing existing literature to provide a starting point for thedevelopment of such case definitions26
Step 3 Apply the case definition algorithm to estimate thenumber of MS cases and prevalence estimates separately foreach database The third step of this approach is simply touse the validated algorithm (step 2) within each of the
Table 5 Strengths weaknesses opportunities and threats (SWOT) analysis using administrative health claims databasesto estimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can develop systematic approachthat could be repeatedly utilizedover time to obtain estimates nowand in the future
Lack of universal health care in theUnited States therefore not allpatients are identifiable throughadministrative data
Can develop a systematic approachthat can be repeatedly utilized overtime to obtain estimates now and inthe future
Lack of certainty whether casedefinitions developed in one datasetwill have same performancecharacteristics in other datasets
Data are accessible and relativelylow-cost
Must accessmultiple administrativedatasets
A case definition can be validated in2 or 3 different administrativedatasets to show consistency offindings across datasets thenapplied even in datasets wherevalidation is not possible4
No easily accessible national sourceof data for uninsured or self-paypopulations
Consistent capture of sex and dateof birth supports calculation of age-and sex-specific prevalenceestimates
Data are collected for health systemmanagement therefore theirvalidity for research must becarefully assessed
If a careful analytic approach is usedcan minimize overlap betweendatasets and avoid duplicatecounting
No easily accessible data forincarcerated or aboriginalpopulations
Data often include zip code whichcan be geocoded to determinesocioeconomic status and establishregion of residence
Lack of identified data to enableidentification of duplicates createsdifficulty identifying the sameindividuals in overlapping datasets
Would ideally include collection ofpatient identifiers to identifyduplicates present inmore than onedatabase howevernongovernment researchers arenot allowed access to suchidentifiers
These databases often haveadditional information that couldinform other analyses egprevalence of comorbidity healthcare utilization and disease-modifying treatment use
Some datasets lack informationregarding raceethnicity or havepoor geographic resolution
Representativeness cannot accessall administrative health databasesin United States must select few toestimate MS prevalence andextrapolate to all
Issue of misdiagnosis as a source oferror lack of clinical detail makes itdifficult to distinguish inaccuratelycoded diagnoses from clinicianmisdiagnosis
In the United States administrative health claims databases include Medicare (a government insurance program covering 93 of US residents age 65 andabove) Medicaid (a government insurance program for low-income parents and children and disabled persons in the United States) the Minimum Data Set(administrative data onMedicare- or Medicaid-certified nursing facilities) the Veterans Health Administration (health care program for veterans of US wars)commercial health insurance claims data (for employer-paid or self-paid insurance) and health maintenance organization health records
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 475
databases (step 1) to obtain valid MS prevalence estimates(overall and specific with respect to age sex raceethnicityand geographic location)Step 4 CombineMSprevalence estimates into a single estimateof the prevalence of MS for the United States weightedaccording to the number of insured persons in each healthinsurance segment after obtaining MS prevalence estimatesseparately for each of the US health insurance segments theycan be combined into a single national prevalence estimateInformation from theCurrent Population Survey can be used toobtain the necessary weights by determining the number of USresidents with each type of insurance coverage stratified by sexage group race and geographic region The total estimatednumber of MS cases for each age sex race and geographicregionndashspecific category can then be summed to estimatethe total number ofMS cases in the United States For exampleMS prevalence for the private insurance segment can beestimated by accessing AHC data for Optum (Eden PrairieMN) and Truven Health (Ann Arbor MI) which in 2010together comprise approximately 68 million individuals or 35of the 2010 privately insured US population MS prevalence inthe government-insured segment of the population can bedirectly and completely estimated for 100 of people coveredby using administrative claims data for Medicaid and MedicareMS prevalence in the military population which is pre-dominantly male can be estimated used the Veterans HealthAdministration database A limitation of this method is that noclaims data exist for persons without health insurance estimatedat 163 in 201028 however for this uninsured group MSprevalence estimates from the Medicaid health care claims datacould be applied because the 2 groups have similar sociodemo-graphic characteristics
Our new approach cannot be applied to estimate the in-cidence of MS in the United States Incidencemdashthe number
of new MS cases per year in a populationmdashis an importantmeasure of disease frequency However it can only be derivedfor countries that have single uniform health care systemswhere longitudinal AHC records for each person enable rel-atively precise indicators of the onset of new MS diagnosisand the exclusion of existing prevalent cases The lack ofa single payer health care system or national tracking systemin the United States does not allow reliable estimates of MSincidence because some individuals may change health carecoverage over time and it is not possible to link patientrecords across insurance sources to provide a single longi-tudinal record within which newly diagnosed persons withMS may be ascertained This creates short periods of ob-servation which do not allow accurate estimates of incidencefor conditions such as MS and cancer due to the inability todefinitively determine which individuals are truly newlydiagnosed29
DiscussionWe have proposed a new approach for applying validatedcase-finding algorithms to AHC data from both governmentand private sources to produce robust estimates of MSprevalence in the United States In a companion article weapplied this approach to estimate the total number of MScases in the United States30 This approach could be appliedto estimate prevalence of other neurologic disorders andchronic conditions that face similar methodologic challengessuch as Parkinson disease dementia and epilepsy
There are several reasons why our new approach is a valuablemethodologic development to estimate the national MSprevalence First this paradigm offers the potential to useexisting AHC data for case ascertainment across the UnitedStates without requiring the cost and effort involved in re-gional MS prevalence studies which typically employ in-tensive case ascertainment methods The data are sufficientlydistributed both geographically and socioeconomically tobe representative of the entire US population and do notrequire consent because the databases are de-identifiedSecond our method is efficient and cost-effective and can beapplied repeatedly with datasets that represent a large pro-portion of the country enabling updates to population-based estimates of MS prevalence over time Third applyingthis approach with data that represent the entire UnitedStates allows us to obtain more stable and precise prevalenceestimates and to fill in knowledge gaps regarding the prev-alence of MS in many regions for which we have never hadestimates Once AHC data are able to accurately and com-pletely capture race and ethnicity this approach could beapplied to racial and ethnic minorities that have receivedlittle study in the past Fourth the use of a highly accuratecase-finding algorithm4 ensures that there will be greatercomparability between estimates derived from these sourcesin the future By adopting a standard paradigm for ascer-taining MS cases and applying validated case definition
Figure 1 Stepwise process for determining the prevalenceof multiple sclerosis (MS) in the United States
476 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
criteria we will be better able to monitor and comparespatial differences in MS prevalence and to examine changesin disease prevalence over time without the variation in-troduced by differing methodologic approaches
Despite many strengths our new approach is limited in thatthe case ascertainment methods do not cover all segments ofthe US population It excludes native American residents whochoose to receive care through the Indian Health Service
Figure 2 Source of health insurance by age (estimates from the current population survey 2008ndash2010)
(A) Population younger than 65 years (B) Population 65 years of age and older
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 477
(06 of the US population in 2010)31 and US residents whoare incarcerated (approximately 05 of the US population in2010)32 If health care databases existed for these populationswe could similarly apply an MS algorithm to estimate MSprevalence and incorporate them into the overall nationalestimate Our approach also cannot distinguish between dif-ferent racial and ethnic groups thus we cannot address towhat extent variations in prevalence by geography or otherfactors may be better explained by racialethnic differences inprevalence33
Our work has important implications for the new era of MSepidemiologic research that will be possible through the 21stCentury Cures Act legislation enacted in December 2016which authorized the establishment of a federally fundedneurologic disorders surveillance system34 A national registryfor MS could be implemented similar to the NationalAmyotrophic Lateral Sclerosis Registry with AHC data asa primary method for case ascertainment and a web portalavailable for all persons with MS to register242535 Withoutaccess to a national registry in the intermediate term wepropose that our approach will deliver the most current andscientifically sound US estimate of the number of personswith MS By addressing methodologic challenges and pro-posing a new paradigm for measuring the prevalence of MS inthe United States we hope that our work will benefit scientistswho study all chronic conditions for which national preva-lence estimates do not currently exist
AcknowledgmentThe authors thank the following members of the US MultipleSclerosis Prevalence Workgroup for their contributionsAlbert Lo Robert McBurney Oleg Muravov Bari Talenteand Leslie Ritter The authors also thank the following keystaff members at the National Multiple Sclerosis Society fortheir contributions to this project Cathy Carlson TimCoetzee Sherri Giger Weyman Johnson Eileen MadrayGraham McReynolds and Cyndi Zagieboylo
Study fundingThe study was funded by contracts from the National Mul-tiple Sclerosis Society to the principal investigators in the MSPrevalence Working Group (HC-1508-05693) The ArticleProcessing Charge was funded by the National MultipleSclerosis Society
DisclosureL Nelson receives grants from the Centers for DiseaseControl and Prevention NIH and National Multiple Scle-rosis Society and contracts from the Agency for Toxic Sub-stances and Diseases Registry She receives compensation forserving as a consultant to Acumen Inc and is on the DataMonitoring Committee of Neuropace M Wallin has servedon data safety monitoring boards for the National Institutes ofNeurological Disease and StrokendashNIH has been an associateeditor for the Encyclopedia of the Neurological Sciences andreceived funding support from the National Multiple Sclerosis
Society and the Department of Veterans Affairs Merit ReviewResearch Program R Marrie is supported by the WaughFamily Chair in Multiple Sclerosis receives research fundingfrom Canadian Institutes of Health Research ResearchManitoba Multiple Sclerosis Society of Canada MultipleSclerosis Scientific Foundation National Multiple SclerosisSociety and Rx amp D Health Research Foundation and hasconducted clinical trials funded by Sanofi-Aventis She alsoserves on the Editorial Board ofNeurologyregW Culpepper hasadditional research funding from the National MultipleSclerosis Society receives support from the VHA MS Centerof Excellence and is a member of the National MultipleSclerosis Society Health Care Delivery and Policy Researchstudy section A Langer-Gould is site principal investigatorfor 2 industry-sponsored phase 3 clinical trials (BiogenIdec Hoffman-LaRoche) and was site PI for one industry-sponsored observation study (Biogen Idec) She receivesgrant support from the NIH National Institute of Neuro-logical Disorders and Stroke Patient-Centered OutcomesResearch Institute and the National Multiple Sclerosis Soci-ety J Campbell has consultancy or research grants over thelast 5 years with Agency for Healthcare Research and QualityALSAM Foundation Amgen AstraZeneca Bayer BiogenIdec Boehringer Ingelheim Centers for Disease Control andPrevention Colorado Medicaid Enterprise CommunityPartners Inc Institute for Clinical and Economic ReviewMallinckrodt NIH National Multiple Sclerosis Society Kai-ser Permanente PhRMA Foundation Teva Research in RealLife Ltd Respiratory Effectiveness Group and Zogenix IncS Buka receives research funding from the NIH and theNational Multiple Sclerosis Society H Tremlett is theCanada Research Chair for Neuroepidemiology and MultipleSclerosis She receives research support from the NationalMultiple Sclerosis Society the Canadian Institutes of HealthResearch the Multiple Sclerosis Society of Canada and theMultiple Sclerosis Scientific Research Foundation In addi-tion in the last 5 years she has received research support fromthe Multiple Sclerosis Society of Canada the Michael SmithFoundation for Health Research and the UK MS Trust andspeaker honoraria andor travel expenses to attend confer-ences G Cutter is a member of Data and Safety MonitoringBoards for AMO Pharmaceuticals Apotek Horizon Phar-maceuticals ModigenetechProlor Merck MerckPfizerOpko Biologics Neurim Sanofi-Aventis Reata Pharmaceut-icals ReceptosCelgene Teva pharmaceuticals NHLBI(Protocol Review Committee) and NICHD (OPRU over-sight committee) and is on the Consulting or AdvisoryBoards for Atara Biotherapeutics Argenix Bioeq GmbHConsortium of MS Centers (grant) Genzyme GenentechInnate Therapeutics Klein-Buendel Incorporated Medi-mmune Medday Novartis Opexa Therapeutics RocheSavara Inc Somahlution Teva Pharmaceuticals Trans-parency Life Sciences and TGTherapeutics W Kaye receivesfunding from the Agency for Toxic Substances and DiseaseRegistry the National Multiple Sclerosis Society and theAssociation for the Accreditation of Human ResearchProtection Programs L Wagner receives funding from the
478 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Agency for Toxic Substances and Disease Registry and Na-tional Multiple Sclerosis Society N LaRocca is employed fulltime by the National Multiple Sclerosis Society and has noother disclosures to report Statistical analysis conducted byDr Gary Cutter PhD University of Alabama at BirminghamGo to NeurologyorgN for full disclosures
Publication historyReceived byNeurology July 17 2018 Accepted in final form October 222018
References1 Wallin MT Kurtzke JF Neuroepidemiology In Bradley WG Daroff RB Fenichel
GM Jankovic J editors Neurology in Clinical Practice Philadelphia Butterworth-Heinemann 2008762ndash780
2 Browne P Chandraratna D Angood C et al Atlas of multiple sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
3 Mayr WT Pittock SJ McClelland RL Jorgensen NW Noseworthy JH Rodriguez MIncidence and prevalence of multiple sclerosis in Olmsted County Minnesota 1985-2000 Neurology 2003611373ndash1377
4 Evans C Beland SG Kulaga S et al Incidence and prevalence of multiple sclerosis inthe Americas a systematic review Neuroepidemiology 201340195ndash210
5 Noonan CW Williamson DM Henry JP et al The prevalence of multiple sclerosis in3 US communities Prev Chronic Dis 20107A1
6 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
7 Baum HM Rothschild BB The incidence and prevalence of reported multiple scle-rosis Ann Neurol 198110420ndash428
8 Anderson DW Ellenberg JH Leventhal CM Reingold SC Rodriguez M SilberbergDH Revised estimate of the prevalence of multiple sclerosis in the United States AnnNeurol 199231333ndash336
9 Nelson LM Hamman RF Thompson DS et al Higher than expected prevalence ofmultiple sclerosis in Northern Colorado dependence on methodological issuesNeuroepidemiology 1986517ndash28
10 Collins JG Prevalence of selected chronic conditions United States 1990-1992 VitalHealth Stat 10 19971941ndash89
Appendix 1 Authors
Name Location Role Contribution
Lorene MNelsonMS PhD
Stanford UniversityCA
Author Study concept anddesign preparation ofdraft manuscriptrevision of themanuscript forcontent approval offinal manuscript
Mitchell TWallin MDMPH
Veterans HealthAdministrationGeorgetownUniversityWashington DC
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
Ruth AnnMarrieMD PhD
University ofManitoba WinnipegCanada
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
William JCulpepperPhD MA
Veterans HealthAdministrationWashington DCUniversity ofMaryland Baltimore
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
AnnetteLanger-GouldMD PhD
Kaiser PermanenteSouthern CaliforniaLos Angeles
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
JonathanCampbellPhD
University of DenverCO
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
StephenBuka PhD
Brown UniversityProvidence RI
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
HelenTremlettPhD
University of BritishColumbia VancouverCanada
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
GaryCutterPhD
University ofAlabamaBirmingham
Author Study concept anddesign critical reviewof the manuscript forcontent
Appendix 1 (continued)
Name Location Role Contribution
WendyKaye PhD
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
LaurieWagnerMPH
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Nicholas GLaRoccaPhD
National MultipleSclerosis Society NewYork NY
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Appendix 2 Coinvestigators and members of the USMultiple Sclerosis Prevalence Workgroup
Name Location Role Contribution
Albert LoMD PhD
Brown UniversityProvidence RI
Coinvestigator Studyconcept anddesign
RobertMcBurneyPhD
Accelerated CureProject Boston MA
Coinvestigator Studyconcept anddesign
OlegMuravovPhD
Agency for ToxicSubstances andDisease RegistryDivision of HealthStudies Atlanta GA
Coinvestigator Studyconcept anddesign
BariTalenteEsq
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
LeslieRitter
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 479
11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

disabled populations These estimates are not strictly com-parable due to the different age distributions and the expec-tation that MS prevalence would be much higher in theMedicaid disabled population In addition no algorithm wasdeveloped or used for MS cases Dilokthornsakul et al16 es-timatedMS prevalence for 2008ndash2012 in the privately insuredUS population by applying a case definition algorithm usingthe PharMetrics Plus Health Plan Claims data a large USprivate insurance claims database that contained claims datafor approximately 42 million enrollees in 2011 The casedefinition algorithm required at least 2 inpatient claims withICD-9 code 340 at least 3 ICD-9 code 340 outpatient claimsor at least one MS-specific disease-modifying treatment(DMT) claim The estimated MS prevalence for 2012 was149 per 100000 (95 CI 1476ndash1509) and when extrapo-lated to the United States as a whole yielded an estimate of403630 individual cases (95 CI 387445ndash419833)
Methods for conducting a nationalstudy of MS prevalence in thecurrent eraBefore designing our study to estimate the US prevalenceof MS the working group members carried out a strengthsweaknesses opportunities and threats (SWOT) analysis for 3approaches to estimate MS prevalence (1) population-basedMS registries (table 3) (2) national probability health surveys(table 4) and (3) analysis of AHC databases (table 5) Studiesof each type were evaluated as potential sources for estimatingthe national prevalence ofMS based on the populations studied
Population-based MS registriesLongstanding MS registries have been successfully used toestimate MS prevalence in 4 countries Denmark1718 Swe-den19 Norway20 and Poland21 However a similar USpopulation-based MS registry does not exist In the UnitedStates there are several voluntary MS registries for conduct-ing outcomes research however none of these registriesattempts the near-complete case ascertainment in a definedgeographic region that would enable the estimation of MSprevalence The benefits and pitfalls of population-baseddisease registries were recently reviewed22 and are summa-rized in table 3 A nationwide population-based registry wouldbe costly to implement however it is possible that a geo-graphically representative system of regional registries couldbe implemented similar to the approach used for cancersurveillance23 In the United States only one neurologic dis-ease registry has been implemented The National Amyo-trophic Lateral Sclerosis Registry was established bya Congressional mandate and began estimating nationalamyotrophic lateral sclerosis prevalence in 20102425
National probability health surveysThe primary method used to estimate national MS prevalencein the past has been probability health surveys Howeveralmost none of the national probability surveys conducted bythe US government are sufficiently large enough to containenough people with MS to enable precise estimation of MSprevalence much less prevalence within demographic or re-gional subgroups Moreover the national survey that onceallowed an overall estimate of MS prevalence (NHIS) nolonger includes questions about MS and other disablingconditions National probability survey data rely on patient or
Table 2 Epidemiologic studies of multiple sclerosis (MS) prevalence in large regions of the United States usingadministrative health claims databases
ReferenceAuthors (year)
Studyyears Case definition Population
National MSprevalence per100000 population(95 CI)
Number ofpersons with MSin the UnitedStates (95 CI)
Popeet al (2002)15 1994ndash1997 One ormore ICD-9 codes for MS(diagnosis code 340)
Nationally representative samplesof administrative claims from 6states (California ColoradoGeorgia Michigan MissouriTennessee)
Privately insured (MedstatMarketScan database)
240 per 100000(95 CI NR) (all ages)
NR
Medicare age 65 and above 180 per 100000(95 CI NR) (age ge65)
NR
Medicaid disabled population allages
710 per 10000 (95CI NR) (all ages)
NR
Dilokthornsakulet al (2016)16
2012 At least 2 inpatient claims withICD-9 code 340 at least 3 ICD-9code 340 outpatient claims orat least 1 MS-indicated DMT
Commercially insured population(Truven Market-Scan)
149 per 100000(1475ndash1508) (allages age-adjustedto US 2012population)
403630(387445ndash419833)
Abbreviations CI = confidence interval DMT = disease-modifying treatment ICD-9 = International Classification of Diseasesndash9 NR = not reported
472 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
family member reports of physician-diagnosed MS1012 risk-ing the inclusion of false-positive MS cases or provisionalcases that would not meet formal case definition criteria Onlyone national survey the Behavioral Risk Factor SurveillanceSurvey (BRFSS) which surveys more than 500000 individ-uals each year has a sample size that would potentially yieldprecise estimates of MS prevalence Feasibility work would beneeded to determine if this BRFSS could be used for thispurpose
Administrative health claims dataIn other countries with universally funded health care systemssuch as Canada and many European nations AHC databaseshave been used to provide a population-based alternative to thetraditional intensive methods of case ascertainment used inregional studies1 In the United States AHC data are main-tained by government (public) insurance programs includingMedicare andMedicaid and by private (commercial) insuranceproviders AHC databases are a tremendous resource forstudying neurologic disease incidence and prevalence becauseof their rich prospective data on patients from defined pop-ulations and their use of the standardized international disease-coding framework (using the ICD system)26 However AHCdatabases are not created for research purposes making it
necessary to demonstrate the validity and the accuracy of caseascertainment algorithm prior to using them for estimatingdisease prevalence These challenges exist for estimating prev-alence of all other common chronic neurologic conditions26
AHC data sources have potential strengths and limitationswhen applied for the purpose of estimating disease prevalence(table 5) The information from AHC databases begins withenrollment into health insurance plans and provides a stan-dardized source of longitudinal patient health care utilizationThese data contain near complete capture of demographic in-formation (sex date of birth raceethnicity zip code or state ofresidence) and health care utilization data including diagnosticcodes and pharmacy records They can be used for researchwithout specific consent because the databases are de-identified Identifying persons with MS through pharmacyrecords is an excellent case ascertainment strategy given thatmany of the DMTs are prescribed only for MS thus the per-sons withMS using suchmedications are highly likely to be trueMS cases However over 40 of persons withMS in theUnitedStates do not take DMTs necessitating additional case-findingmethods Because clinical details are often not available such aswhether a diagnostic code was entered by a neurologist phy-sician or nonphysicianmost claims database studies have reliedon case-finding algorithms that have not been judged against
Table 3 Strengths weaknesses opportunities and threats (SWOT) analysis using population-based multiple sclerosis(MS) registries to estimate national MS prevalence in the US
Strengths Weaknesses Opportunities Threats
Multiple overlapping caseascertainment methods areused to yield a high degree ofcase ascertainment
Organizational demands makea nationwide registry infeasible in theUnited States with rare exceptions(National Amyotrophic LateralSclerosis Registry2425)
A systematic approach could bedeveloped to extrapolate results frommultiple regional registries to nationalMS prevalence howevera geographically valid sample of selectstates would need to be selected torepresent the nation
If registry relies on patientvolunteers or requires consenta large degree of nonresponse canseriously affect the validity of theregistry
Data are rigorously collected forresearch purposes according tostandard protocols
Very high cost to implement inpopulation-based regions possiblyinfeasible for nationwideimplementation in the United States
For regions where registryparticipation is high can obtain validand precise estimates of MSprevalence
Confirming clinician diagnoses iscostly and impractical for largenumbers of patients
Some US registries rely in parton case ascertainment throughneurologists primary carephysicians and hospitals
In the United States registries oftenalso rely on MS diagnosis reported bypatient or family member whichmight be misreported medical chartsmay be requested for verification ofcase definition but may be difficult toobtain for all patients in a population-based registry
Need to collect patient identifiers toidentify duplicates identified bymore than one case ascertainmentmethod (risks HIPAAnoncompliance)
Data can be collected on raceethnicity and othersociodemographiccharacteristics
Registries often contain moreclinical details (eg initialsymptomatology clinicalcourse disability status) than doother sources
Abbreviation HIPAA = Health Insurance Portability and Accountability ActWith the exception of studies conducted by Mayo Clinic researchers in Rochester Minnesota17 population-based MS registries do not exist in the UnitedStates However there are several notable population-basedMS registries in Europe that enable ongoing estimation of nationalMS incidence andprevalenceincluding in Denmark1718 Sweden19 Norway20 and Poland21 Such studies often rely on case ascertainment through multiple data sources includingneurologists primary care physicians and hospitals
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 473
case definitions or even neurologist diagnoses for accuracyTwo studies used a case definition that required only a singlehealth care encounter for MS1215 which is likely to be highlynonspecific risking an unknown number of false-positives Thestudy by Dilokthornsakul et al16 that used private insuranceclaims data was strengthened by conducting sensitivity analysesthat examined the performance of 2 alternative algorithms oneof which produced estimates very similar to the primaryalgorithm
Developing a new approach forestimating MS prevalence in theUnited StatesBased on the SWOT analysis and through discussion andconsensus we concluded that AHC data would provide themost cost-effective method to develop a national prevalenceestimate for MS Collectively government and private healthclaims databases represent a very large proportion of the USpopulation (84 in 2010)28 which together enables preciseestimates of MS prevalence The data are sufficiently distrib-uted geographically and socioeconomically to be representa-tive of the entire US population Figure 1 illustrates a new4-step approach we devised for estimating the prevalence ofMS for the United States as a whole using a segmental
approach for each insurance source and then combining theminto a national estimate
Step 1 Identify datasets covering US publicly and privatelyinsured populations figure 2 illustrates the fragmented natureof insurance coverage of the US population which doesnot enable a single health care source for estimating MSprevalence as is often available in Scandinavian countries withnational unified health care systems Nevertheless AHC dataare available for almost all of the insurance segments of theUS population allowing the estimation of MS prevalenceseparately for each insurance segment which can then beaggregated into an overall national estimate ofMS prevalenceFigure 2 shows US Census Current Population Survey datafor 2008ndash2010 presented separately for individuals under age65 vs those ages 65 and older because the sources of insurancecoverage vary considerably for these 2 age groups In 2010 forindividuals below age 65 private insurance comprised thelargest segment of insurance coverage 65 when employer-purchased and self-purchased private insurance were consid-ered together The next largest segment of insurance coveragein 2010 for individuals under age 65 is Medicaid (17)a government insurance program that provides free medicalinsurance to low-income people Smaller percentages ofindividuals under age 65 in 2010 were covered by a militarysource such as Department of Defense (DOD) or Veterans
Table 4 Strengths weaknesses opportunities and threats (SWOT) analysis using national probability survey samples toestimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can be obtained from existinggovernment surveys
Dedicated MS-specific patientsurveys are costly to carry out andinfeasible for national scope
This method can be feasible ifmultiple years of survey data can beaggregated
Existing national probabilitysamples usually comprise onlysegments of the US population(ie noninstitutionalized)
Sampling designs are rigorous(probability samples) of the USpopulation rigorously collected forresearch purposes according tostandard protocols
Survey participation rates are athistorically low levels
Successful application would requireaccess to a very large survey samplesuch as the BRFSS conducted annuallyby the CDC however a geographicallyvalid sample of select states wouldneed to be selected to represent thenation
Survey questions for patients andfamily members have not beenvalidated for accuracy againsta gold standard (neurologistdiagnosis)
Data are accessible and either cost-free or low-cost
Surveys rely on MS diagnosisreported by patient or a familymember which are susceptible toboth underreporting and false-positive reports
If survey questions were validatedagainst a gold standard (neurologistdiagnosis) this method could befeasibly implemented in a subset ofUS states
Restrictions on number ofquestions limits collection ofclinical details (eg clinicalcourse disability status)
Data are available on age sex raceethnicity broad geographic locationand other sociodemographiccharacteristics
Count ofMS patients in single yearsof data are often too small forprecise estimation
Some surveys collect self-reporteddata that can inform other analyseseg prevalence of comorbidity healthcare utilization and cost DMT uselifestyle risk factors
Overall prevalence might beestimable but data are often toosparse for getting breakdowns bysex age race or geographic region
Abbreviations BRFSS = Behavioral Risk Factor Surveillance Survey CDC = Centers for Disease Control and Prevention DMT = disease-modifying treatmentIn the United States national probability survey samples include the National Health Interview Survey Medical Expenditure Panel Survey HouseholdComponent National Nursing Home Survey and the BRFSS (a probability survey completed by500000 Americans per year and for which disease-specificquestions can be added on a state-by-state basis)
474 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Health Administration (VHA) (4) or by anothergovernment-provided insurance plan (Medicare 3) In2010 18 of individuals under age 65 had no insurancecoverage In 2010 for individuals ages 65 and abovegovernment insurance provided by Medicare covered 93of the population and was often supplemented by privatecoinsurance (33 employer-provided 29 self-purchased)Medicaid either alone or in combination with Medicarecovered 9 of those age 65 and above In 2010 8 ofindividuals age 65 and above were covered by amilitary source(DOD or VHA) and only 2 of the elderly were uninsuredThus despite the fragmentation of the US health care systemAHC databases for all of the insured segments of the USpopulation are available and can be used to estimate MSprevalence in each dataset separately before combining theestimates into a whole (step 4)Step 2 Develop and validate a highly accurate MS case-finding algorithm that can be standardly applied in all AHCdatabases Our approach requires a highly accurate casedefinition to identify MS cases that performs consistently
across AHC databases with differing characteristics so thatit can be applied even in datasets where formal validationis not possible Notably no MS prevalence studies in theUnited States have used validated algorithms for identifyingpersons with MS yet having a validated algorithm for thispurpose is a necessary step for carrying out valid prevalenceestimation26 Culpepper et al27 recently conducted a multi-site validation study to develop a valid and reliable algorithmfor identifying MS cases using AHC data with excellentsensitivity specificity and positive predictive value For thefirst time ever this provides a high-performing algorithmthat performs consistently well across datasets and can beapplied across all AHC databases Similar methodologycould be employed for other chronic neurologic diseasesusing existing literature to provide a starting point for thedevelopment of such case definitions26
Step 3 Apply the case definition algorithm to estimate thenumber of MS cases and prevalence estimates separately foreach database The third step of this approach is simply touse the validated algorithm (step 2) within each of the
Table 5 Strengths weaknesses opportunities and threats (SWOT) analysis using administrative health claims databasesto estimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can develop systematic approachthat could be repeatedly utilizedover time to obtain estimates nowand in the future
Lack of universal health care in theUnited States therefore not allpatients are identifiable throughadministrative data
Can develop a systematic approachthat can be repeatedly utilized overtime to obtain estimates now and inthe future
Lack of certainty whether casedefinitions developed in one datasetwill have same performancecharacteristics in other datasets
Data are accessible and relativelylow-cost
Must accessmultiple administrativedatasets
A case definition can be validated in2 or 3 different administrativedatasets to show consistency offindings across datasets thenapplied even in datasets wherevalidation is not possible4
No easily accessible national sourceof data for uninsured or self-paypopulations
Consistent capture of sex and dateof birth supports calculation of age-and sex-specific prevalenceestimates
Data are collected for health systemmanagement therefore theirvalidity for research must becarefully assessed
If a careful analytic approach is usedcan minimize overlap betweendatasets and avoid duplicatecounting
No easily accessible data forincarcerated or aboriginalpopulations
Data often include zip code whichcan be geocoded to determinesocioeconomic status and establishregion of residence
Lack of identified data to enableidentification of duplicates createsdifficulty identifying the sameindividuals in overlapping datasets
Would ideally include collection ofpatient identifiers to identifyduplicates present inmore than onedatabase howevernongovernment researchers arenot allowed access to suchidentifiers
These databases often haveadditional information that couldinform other analyses egprevalence of comorbidity healthcare utilization and disease-modifying treatment use
Some datasets lack informationregarding raceethnicity or havepoor geographic resolution
Representativeness cannot accessall administrative health databasesin United States must select few toestimate MS prevalence andextrapolate to all
Issue of misdiagnosis as a source oferror lack of clinical detail makes itdifficult to distinguish inaccuratelycoded diagnoses from clinicianmisdiagnosis
In the United States administrative health claims databases include Medicare (a government insurance program covering 93 of US residents age 65 andabove) Medicaid (a government insurance program for low-income parents and children and disabled persons in the United States) the Minimum Data Set(administrative data onMedicare- or Medicaid-certified nursing facilities) the Veterans Health Administration (health care program for veterans of US wars)commercial health insurance claims data (for employer-paid or self-paid insurance) and health maintenance organization health records
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 475
databases (step 1) to obtain valid MS prevalence estimates(overall and specific with respect to age sex raceethnicityand geographic location)Step 4 CombineMSprevalence estimates into a single estimateof the prevalence of MS for the United States weightedaccording to the number of insured persons in each healthinsurance segment after obtaining MS prevalence estimatesseparately for each of the US health insurance segments theycan be combined into a single national prevalence estimateInformation from theCurrent Population Survey can be used toobtain the necessary weights by determining the number of USresidents with each type of insurance coverage stratified by sexage group race and geographic region The total estimatednumber of MS cases for each age sex race and geographicregionndashspecific category can then be summed to estimatethe total number ofMS cases in the United States For exampleMS prevalence for the private insurance segment can beestimated by accessing AHC data for Optum (Eden PrairieMN) and Truven Health (Ann Arbor MI) which in 2010together comprise approximately 68 million individuals or 35of the 2010 privately insured US population MS prevalence inthe government-insured segment of the population can bedirectly and completely estimated for 100 of people coveredby using administrative claims data for Medicaid and MedicareMS prevalence in the military population which is pre-dominantly male can be estimated used the Veterans HealthAdministration database A limitation of this method is that noclaims data exist for persons without health insurance estimatedat 163 in 201028 however for this uninsured group MSprevalence estimates from the Medicaid health care claims datacould be applied because the 2 groups have similar sociodemo-graphic characteristics
Our new approach cannot be applied to estimate the in-cidence of MS in the United States Incidencemdashthe number
of new MS cases per year in a populationmdashis an importantmeasure of disease frequency However it can only be derivedfor countries that have single uniform health care systemswhere longitudinal AHC records for each person enable rel-atively precise indicators of the onset of new MS diagnosisand the exclusion of existing prevalent cases The lack ofa single payer health care system or national tracking systemin the United States does not allow reliable estimates of MSincidence because some individuals may change health carecoverage over time and it is not possible to link patientrecords across insurance sources to provide a single longi-tudinal record within which newly diagnosed persons withMS may be ascertained This creates short periods of ob-servation which do not allow accurate estimates of incidencefor conditions such as MS and cancer due to the inability todefinitively determine which individuals are truly newlydiagnosed29
DiscussionWe have proposed a new approach for applying validatedcase-finding algorithms to AHC data from both governmentand private sources to produce robust estimates of MSprevalence in the United States In a companion article weapplied this approach to estimate the total number of MScases in the United States30 This approach could be appliedto estimate prevalence of other neurologic disorders andchronic conditions that face similar methodologic challengessuch as Parkinson disease dementia and epilepsy
There are several reasons why our new approach is a valuablemethodologic development to estimate the national MSprevalence First this paradigm offers the potential to useexisting AHC data for case ascertainment across the UnitedStates without requiring the cost and effort involved in re-gional MS prevalence studies which typically employ in-tensive case ascertainment methods The data are sufficientlydistributed both geographically and socioeconomically tobe representative of the entire US population and do notrequire consent because the databases are de-identifiedSecond our method is efficient and cost-effective and can beapplied repeatedly with datasets that represent a large pro-portion of the country enabling updates to population-based estimates of MS prevalence over time Third applyingthis approach with data that represent the entire UnitedStates allows us to obtain more stable and precise prevalenceestimates and to fill in knowledge gaps regarding the prev-alence of MS in many regions for which we have never hadestimates Once AHC data are able to accurately and com-pletely capture race and ethnicity this approach could beapplied to racial and ethnic minorities that have receivedlittle study in the past Fourth the use of a highly accuratecase-finding algorithm4 ensures that there will be greatercomparability between estimates derived from these sourcesin the future By adopting a standard paradigm for ascer-taining MS cases and applying validated case definition
Figure 1 Stepwise process for determining the prevalenceof multiple sclerosis (MS) in the United States
476 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
criteria we will be better able to monitor and comparespatial differences in MS prevalence and to examine changesin disease prevalence over time without the variation in-troduced by differing methodologic approaches
Despite many strengths our new approach is limited in thatthe case ascertainment methods do not cover all segments ofthe US population It excludes native American residents whochoose to receive care through the Indian Health Service
Figure 2 Source of health insurance by age (estimates from the current population survey 2008ndash2010)
(A) Population younger than 65 years (B) Population 65 years of age and older
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 477
(06 of the US population in 2010)31 and US residents whoare incarcerated (approximately 05 of the US population in2010)32 If health care databases existed for these populationswe could similarly apply an MS algorithm to estimate MSprevalence and incorporate them into the overall nationalestimate Our approach also cannot distinguish between dif-ferent racial and ethnic groups thus we cannot address towhat extent variations in prevalence by geography or otherfactors may be better explained by racialethnic differences inprevalence33
Our work has important implications for the new era of MSepidemiologic research that will be possible through the 21stCentury Cures Act legislation enacted in December 2016which authorized the establishment of a federally fundedneurologic disorders surveillance system34 A national registryfor MS could be implemented similar to the NationalAmyotrophic Lateral Sclerosis Registry with AHC data asa primary method for case ascertainment and a web portalavailable for all persons with MS to register242535 Withoutaccess to a national registry in the intermediate term wepropose that our approach will deliver the most current andscientifically sound US estimate of the number of personswith MS By addressing methodologic challenges and pro-posing a new paradigm for measuring the prevalence of MS inthe United States we hope that our work will benefit scientistswho study all chronic conditions for which national preva-lence estimates do not currently exist
AcknowledgmentThe authors thank the following members of the US MultipleSclerosis Prevalence Workgroup for their contributionsAlbert Lo Robert McBurney Oleg Muravov Bari Talenteand Leslie Ritter The authors also thank the following keystaff members at the National Multiple Sclerosis Society fortheir contributions to this project Cathy Carlson TimCoetzee Sherri Giger Weyman Johnson Eileen MadrayGraham McReynolds and Cyndi Zagieboylo
Study fundingThe study was funded by contracts from the National Mul-tiple Sclerosis Society to the principal investigators in the MSPrevalence Working Group (HC-1508-05693) The ArticleProcessing Charge was funded by the National MultipleSclerosis Society
DisclosureL Nelson receives grants from the Centers for DiseaseControl and Prevention NIH and National Multiple Scle-rosis Society and contracts from the Agency for Toxic Sub-stances and Diseases Registry She receives compensation forserving as a consultant to Acumen Inc and is on the DataMonitoring Committee of Neuropace M Wallin has servedon data safety monitoring boards for the National Institutes ofNeurological Disease and StrokendashNIH has been an associateeditor for the Encyclopedia of the Neurological Sciences andreceived funding support from the National Multiple Sclerosis
Society and the Department of Veterans Affairs Merit ReviewResearch Program R Marrie is supported by the WaughFamily Chair in Multiple Sclerosis receives research fundingfrom Canadian Institutes of Health Research ResearchManitoba Multiple Sclerosis Society of Canada MultipleSclerosis Scientific Foundation National Multiple SclerosisSociety and Rx amp D Health Research Foundation and hasconducted clinical trials funded by Sanofi-Aventis She alsoserves on the Editorial Board ofNeurologyregW Culpepper hasadditional research funding from the National MultipleSclerosis Society receives support from the VHA MS Centerof Excellence and is a member of the National MultipleSclerosis Society Health Care Delivery and Policy Researchstudy section A Langer-Gould is site principal investigatorfor 2 industry-sponsored phase 3 clinical trials (BiogenIdec Hoffman-LaRoche) and was site PI for one industry-sponsored observation study (Biogen Idec) She receivesgrant support from the NIH National Institute of Neuro-logical Disorders and Stroke Patient-Centered OutcomesResearch Institute and the National Multiple Sclerosis Soci-ety J Campbell has consultancy or research grants over thelast 5 years with Agency for Healthcare Research and QualityALSAM Foundation Amgen AstraZeneca Bayer BiogenIdec Boehringer Ingelheim Centers for Disease Control andPrevention Colorado Medicaid Enterprise CommunityPartners Inc Institute for Clinical and Economic ReviewMallinckrodt NIH National Multiple Sclerosis Society Kai-ser Permanente PhRMA Foundation Teva Research in RealLife Ltd Respiratory Effectiveness Group and Zogenix IncS Buka receives research funding from the NIH and theNational Multiple Sclerosis Society H Tremlett is theCanada Research Chair for Neuroepidemiology and MultipleSclerosis She receives research support from the NationalMultiple Sclerosis Society the Canadian Institutes of HealthResearch the Multiple Sclerosis Society of Canada and theMultiple Sclerosis Scientific Research Foundation In addi-tion in the last 5 years she has received research support fromthe Multiple Sclerosis Society of Canada the Michael SmithFoundation for Health Research and the UK MS Trust andspeaker honoraria andor travel expenses to attend confer-ences G Cutter is a member of Data and Safety MonitoringBoards for AMO Pharmaceuticals Apotek Horizon Phar-maceuticals ModigenetechProlor Merck MerckPfizerOpko Biologics Neurim Sanofi-Aventis Reata Pharmaceut-icals ReceptosCelgene Teva pharmaceuticals NHLBI(Protocol Review Committee) and NICHD (OPRU over-sight committee) and is on the Consulting or AdvisoryBoards for Atara Biotherapeutics Argenix Bioeq GmbHConsortium of MS Centers (grant) Genzyme GenentechInnate Therapeutics Klein-Buendel Incorporated Medi-mmune Medday Novartis Opexa Therapeutics RocheSavara Inc Somahlution Teva Pharmaceuticals Trans-parency Life Sciences and TGTherapeutics W Kaye receivesfunding from the Agency for Toxic Substances and DiseaseRegistry the National Multiple Sclerosis Society and theAssociation for the Accreditation of Human ResearchProtection Programs L Wagner receives funding from the
478 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Agency for Toxic Substances and Disease Registry and Na-tional Multiple Sclerosis Society N LaRocca is employed fulltime by the National Multiple Sclerosis Society and has noother disclosures to report Statistical analysis conducted byDr Gary Cutter PhD University of Alabama at BirminghamGo to NeurologyorgN for full disclosures
Publication historyReceived byNeurology July 17 2018 Accepted in final form October 222018
References1 Wallin MT Kurtzke JF Neuroepidemiology In Bradley WG Daroff RB Fenichel
GM Jankovic J editors Neurology in Clinical Practice Philadelphia Butterworth-Heinemann 2008762ndash780
2 Browne P Chandraratna D Angood C et al Atlas of multiple sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
3 Mayr WT Pittock SJ McClelland RL Jorgensen NW Noseworthy JH Rodriguez MIncidence and prevalence of multiple sclerosis in Olmsted County Minnesota 1985-2000 Neurology 2003611373ndash1377
4 Evans C Beland SG Kulaga S et al Incidence and prevalence of multiple sclerosis inthe Americas a systematic review Neuroepidemiology 201340195ndash210
5 Noonan CW Williamson DM Henry JP et al The prevalence of multiple sclerosis in3 US communities Prev Chronic Dis 20107A1
6 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
7 Baum HM Rothschild BB The incidence and prevalence of reported multiple scle-rosis Ann Neurol 198110420ndash428
8 Anderson DW Ellenberg JH Leventhal CM Reingold SC Rodriguez M SilberbergDH Revised estimate of the prevalence of multiple sclerosis in the United States AnnNeurol 199231333ndash336
9 Nelson LM Hamman RF Thompson DS et al Higher than expected prevalence ofmultiple sclerosis in Northern Colorado dependence on methodological issuesNeuroepidemiology 1986517ndash28
10 Collins JG Prevalence of selected chronic conditions United States 1990-1992 VitalHealth Stat 10 19971941ndash89
Appendix 1 Authors
Name Location Role Contribution
Lorene MNelsonMS PhD
Stanford UniversityCA
Author Study concept anddesign preparation ofdraft manuscriptrevision of themanuscript forcontent approval offinal manuscript
Mitchell TWallin MDMPH
Veterans HealthAdministrationGeorgetownUniversityWashington DC
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
Ruth AnnMarrieMD PhD
University ofManitoba WinnipegCanada
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
William JCulpepperPhD MA
Veterans HealthAdministrationWashington DCUniversity ofMaryland Baltimore
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
AnnetteLanger-GouldMD PhD
Kaiser PermanenteSouthern CaliforniaLos Angeles
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
JonathanCampbellPhD
University of DenverCO
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
StephenBuka PhD
Brown UniversityProvidence RI
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
HelenTremlettPhD
University of BritishColumbia VancouverCanada
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
GaryCutterPhD
University ofAlabamaBirmingham
Author Study concept anddesign critical reviewof the manuscript forcontent
Appendix 1 (continued)
Name Location Role Contribution
WendyKaye PhD
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
LaurieWagnerMPH
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Nicholas GLaRoccaPhD
National MultipleSclerosis Society NewYork NY
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Appendix 2 Coinvestigators and members of the USMultiple Sclerosis Prevalence Workgroup
Name Location Role Contribution
Albert LoMD PhD
Brown UniversityProvidence RI
Coinvestigator Studyconcept anddesign
RobertMcBurneyPhD
Accelerated CureProject Boston MA
Coinvestigator Studyconcept anddesign
OlegMuravovPhD
Agency for ToxicSubstances andDisease RegistryDivision of HealthStudies Atlanta GA
Coinvestigator Studyconcept anddesign
BariTalenteEsq
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
LeslieRitter
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 479
11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

family member reports of physician-diagnosed MS1012 risk-ing the inclusion of false-positive MS cases or provisionalcases that would not meet formal case definition criteria Onlyone national survey the Behavioral Risk Factor SurveillanceSurvey (BRFSS) which surveys more than 500000 individ-uals each year has a sample size that would potentially yieldprecise estimates of MS prevalence Feasibility work would beneeded to determine if this BRFSS could be used for thispurpose
Administrative health claims dataIn other countries with universally funded health care systemssuch as Canada and many European nations AHC databaseshave been used to provide a population-based alternative to thetraditional intensive methods of case ascertainment used inregional studies1 In the United States AHC data are main-tained by government (public) insurance programs includingMedicare andMedicaid and by private (commercial) insuranceproviders AHC databases are a tremendous resource forstudying neurologic disease incidence and prevalence becauseof their rich prospective data on patients from defined pop-ulations and their use of the standardized international disease-coding framework (using the ICD system)26 However AHCdatabases are not created for research purposes making it
necessary to demonstrate the validity and the accuracy of caseascertainment algorithm prior to using them for estimatingdisease prevalence These challenges exist for estimating prev-alence of all other common chronic neurologic conditions26
AHC data sources have potential strengths and limitationswhen applied for the purpose of estimating disease prevalence(table 5) The information from AHC databases begins withenrollment into health insurance plans and provides a stan-dardized source of longitudinal patient health care utilizationThese data contain near complete capture of demographic in-formation (sex date of birth raceethnicity zip code or state ofresidence) and health care utilization data including diagnosticcodes and pharmacy records They can be used for researchwithout specific consent because the databases are de-identified Identifying persons with MS through pharmacyrecords is an excellent case ascertainment strategy given thatmany of the DMTs are prescribed only for MS thus the per-sons withMS using suchmedications are highly likely to be trueMS cases However over 40 of persons withMS in theUnitedStates do not take DMTs necessitating additional case-findingmethods Because clinical details are often not available such aswhether a diagnostic code was entered by a neurologist phy-sician or nonphysicianmost claims database studies have reliedon case-finding algorithms that have not been judged against
Table 3 Strengths weaknesses opportunities and threats (SWOT) analysis using population-based multiple sclerosis(MS) registries to estimate national MS prevalence in the US
Strengths Weaknesses Opportunities Threats
Multiple overlapping caseascertainment methods areused to yield a high degree ofcase ascertainment
Organizational demands makea nationwide registry infeasible in theUnited States with rare exceptions(National Amyotrophic LateralSclerosis Registry2425)
A systematic approach could bedeveloped to extrapolate results frommultiple regional registries to nationalMS prevalence howevera geographically valid sample of selectstates would need to be selected torepresent the nation
If registry relies on patientvolunteers or requires consenta large degree of nonresponse canseriously affect the validity of theregistry
Data are rigorously collected forresearch purposes according tostandard protocols
Very high cost to implement inpopulation-based regions possiblyinfeasible for nationwideimplementation in the United States
For regions where registryparticipation is high can obtain validand precise estimates of MSprevalence
Confirming clinician diagnoses iscostly and impractical for largenumbers of patients
Some US registries rely in parton case ascertainment throughneurologists primary carephysicians and hospitals
In the United States registries oftenalso rely on MS diagnosis reported bypatient or family member whichmight be misreported medical chartsmay be requested for verification ofcase definition but may be difficult toobtain for all patients in a population-based registry
Need to collect patient identifiers toidentify duplicates identified bymore than one case ascertainmentmethod (risks HIPAAnoncompliance)
Data can be collected on raceethnicity and othersociodemographiccharacteristics
Registries often contain moreclinical details (eg initialsymptomatology clinicalcourse disability status) than doother sources
Abbreviation HIPAA = Health Insurance Portability and Accountability ActWith the exception of studies conducted by Mayo Clinic researchers in Rochester Minnesota17 population-based MS registries do not exist in the UnitedStates However there are several notable population-basedMS registries in Europe that enable ongoing estimation of nationalMS incidence andprevalenceincluding in Denmark1718 Sweden19 Norway20 and Poland21 Such studies often rely on case ascertainment through multiple data sources includingneurologists primary care physicians and hospitals
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 473
case definitions or even neurologist diagnoses for accuracyTwo studies used a case definition that required only a singlehealth care encounter for MS1215 which is likely to be highlynonspecific risking an unknown number of false-positives Thestudy by Dilokthornsakul et al16 that used private insuranceclaims data was strengthened by conducting sensitivity analysesthat examined the performance of 2 alternative algorithms oneof which produced estimates very similar to the primaryalgorithm
Developing a new approach forestimating MS prevalence in theUnited StatesBased on the SWOT analysis and through discussion andconsensus we concluded that AHC data would provide themost cost-effective method to develop a national prevalenceestimate for MS Collectively government and private healthclaims databases represent a very large proportion of the USpopulation (84 in 2010)28 which together enables preciseestimates of MS prevalence The data are sufficiently distrib-uted geographically and socioeconomically to be representa-tive of the entire US population Figure 1 illustrates a new4-step approach we devised for estimating the prevalence ofMS for the United States as a whole using a segmental
approach for each insurance source and then combining theminto a national estimate
Step 1 Identify datasets covering US publicly and privatelyinsured populations figure 2 illustrates the fragmented natureof insurance coverage of the US population which doesnot enable a single health care source for estimating MSprevalence as is often available in Scandinavian countries withnational unified health care systems Nevertheless AHC dataare available for almost all of the insurance segments of theUS population allowing the estimation of MS prevalenceseparately for each insurance segment which can then beaggregated into an overall national estimate ofMS prevalenceFigure 2 shows US Census Current Population Survey datafor 2008ndash2010 presented separately for individuals under age65 vs those ages 65 and older because the sources of insurancecoverage vary considerably for these 2 age groups In 2010 forindividuals below age 65 private insurance comprised thelargest segment of insurance coverage 65 when employer-purchased and self-purchased private insurance were consid-ered together The next largest segment of insurance coveragein 2010 for individuals under age 65 is Medicaid (17)a government insurance program that provides free medicalinsurance to low-income people Smaller percentages ofindividuals under age 65 in 2010 were covered by a militarysource such as Department of Defense (DOD) or Veterans
Table 4 Strengths weaknesses opportunities and threats (SWOT) analysis using national probability survey samples toestimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can be obtained from existinggovernment surveys
Dedicated MS-specific patientsurveys are costly to carry out andinfeasible for national scope
This method can be feasible ifmultiple years of survey data can beaggregated
Existing national probabilitysamples usually comprise onlysegments of the US population(ie noninstitutionalized)
Sampling designs are rigorous(probability samples) of the USpopulation rigorously collected forresearch purposes according tostandard protocols
Survey participation rates are athistorically low levels
Successful application would requireaccess to a very large survey samplesuch as the BRFSS conducted annuallyby the CDC however a geographicallyvalid sample of select states wouldneed to be selected to represent thenation
Survey questions for patients andfamily members have not beenvalidated for accuracy againsta gold standard (neurologistdiagnosis)
Data are accessible and either cost-free or low-cost
Surveys rely on MS diagnosisreported by patient or a familymember which are susceptible toboth underreporting and false-positive reports
If survey questions were validatedagainst a gold standard (neurologistdiagnosis) this method could befeasibly implemented in a subset ofUS states
Restrictions on number ofquestions limits collection ofclinical details (eg clinicalcourse disability status)
Data are available on age sex raceethnicity broad geographic locationand other sociodemographiccharacteristics
Count ofMS patients in single yearsof data are often too small forprecise estimation
Some surveys collect self-reporteddata that can inform other analyseseg prevalence of comorbidity healthcare utilization and cost DMT uselifestyle risk factors
Overall prevalence might beestimable but data are often toosparse for getting breakdowns bysex age race or geographic region
Abbreviations BRFSS = Behavioral Risk Factor Surveillance Survey CDC = Centers for Disease Control and Prevention DMT = disease-modifying treatmentIn the United States national probability survey samples include the National Health Interview Survey Medical Expenditure Panel Survey HouseholdComponent National Nursing Home Survey and the BRFSS (a probability survey completed by500000 Americans per year and for which disease-specificquestions can be added on a state-by-state basis)
474 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Health Administration (VHA) (4) or by anothergovernment-provided insurance plan (Medicare 3) In2010 18 of individuals under age 65 had no insurancecoverage In 2010 for individuals ages 65 and abovegovernment insurance provided by Medicare covered 93of the population and was often supplemented by privatecoinsurance (33 employer-provided 29 self-purchased)Medicaid either alone or in combination with Medicarecovered 9 of those age 65 and above In 2010 8 ofindividuals age 65 and above were covered by amilitary source(DOD or VHA) and only 2 of the elderly were uninsuredThus despite the fragmentation of the US health care systemAHC databases for all of the insured segments of the USpopulation are available and can be used to estimate MSprevalence in each dataset separately before combining theestimates into a whole (step 4)Step 2 Develop and validate a highly accurate MS case-finding algorithm that can be standardly applied in all AHCdatabases Our approach requires a highly accurate casedefinition to identify MS cases that performs consistently
across AHC databases with differing characteristics so thatit can be applied even in datasets where formal validationis not possible Notably no MS prevalence studies in theUnited States have used validated algorithms for identifyingpersons with MS yet having a validated algorithm for thispurpose is a necessary step for carrying out valid prevalenceestimation26 Culpepper et al27 recently conducted a multi-site validation study to develop a valid and reliable algorithmfor identifying MS cases using AHC data with excellentsensitivity specificity and positive predictive value For thefirst time ever this provides a high-performing algorithmthat performs consistently well across datasets and can beapplied across all AHC databases Similar methodologycould be employed for other chronic neurologic diseasesusing existing literature to provide a starting point for thedevelopment of such case definitions26
Step 3 Apply the case definition algorithm to estimate thenumber of MS cases and prevalence estimates separately foreach database The third step of this approach is simply touse the validated algorithm (step 2) within each of the
Table 5 Strengths weaknesses opportunities and threats (SWOT) analysis using administrative health claims databasesto estimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can develop systematic approachthat could be repeatedly utilizedover time to obtain estimates nowand in the future
Lack of universal health care in theUnited States therefore not allpatients are identifiable throughadministrative data
Can develop a systematic approachthat can be repeatedly utilized overtime to obtain estimates now and inthe future
Lack of certainty whether casedefinitions developed in one datasetwill have same performancecharacteristics in other datasets
Data are accessible and relativelylow-cost
Must accessmultiple administrativedatasets
A case definition can be validated in2 or 3 different administrativedatasets to show consistency offindings across datasets thenapplied even in datasets wherevalidation is not possible4
No easily accessible national sourceof data for uninsured or self-paypopulations
Consistent capture of sex and dateof birth supports calculation of age-and sex-specific prevalenceestimates
Data are collected for health systemmanagement therefore theirvalidity for research must becarefully assessed
If a careful analytic approach is usedcan minimize overlap betweendatasets and avoid duplicatecounting
No easily accessible data forincarcerated or aboriginalpopulations
Data often include zip code whichcan be geocoded to determinesocioeconomic status and establishregion of residence
Lack of identified data to enableidentification of duplicates createsdifficulty identifying the sameindividuals in overlapping datasets
Would ideally include collection ofpatient identifiers to identifyduplicates present inmore than onedatabase howevernongovernment researchers arenot allowed access to suchidentifiers
These databases often haveadditional information that couldinform other analyses egprevalence of comorbidity healthcare utilization and disease-modifying treatment use
Some datasets lack informationregarding raceethnicity or havepoor geographic resolution
Representativeness cannot accessall administrative health databasesin United States must select few toestimate MS prevalence andextrapolate to all
Issue of misdiagnosis as a source oferror lack of clinical detail makes itdifficult to distinguish inaccuratelycoded diagnoses from clinicianmisdiagnosis
In the United States administrative health claims databases include Medicare (a government insurance program covering 93 of US residents age 65 andabove) Medicaid (a government insurance program for low-income parents and children and disabled persons in the United States) the Minimum Data Set(administrative data onMedicare- or Medicaid-certified nursing facilities) the Veterans Health Administration (health care program for veterans of US wars)commercial health insurance claims data (for employer-paid or self-paid insurance) and health maintenance organization health records
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 475
databases (step 1) to obtain valid MS prevalence estimates(overall and specific with respect to age sex raceethnicityand geographic location)Step 4 CombineMSprevalence estimates into a single estimateof the prevalence of MS for the United States weightedaccording to the number of insured persons in each healthinsurance segment after obtaining MS prevalence estimatesseparately for each of the US health insurance segments theycan be combined into a single national prevalence estimateInformation from theCurrent Population Survey can be used toobtain the necessary weights by determining the number of USresidents with each type of insurance coverage stratified by sexage group race and geographic region The total estimatednumber of MS cases for each age sex race and geographicregionndashspecific category can then be summed to estimatethe total number ofMS cases in the United States For exampleMS prevalence for the private insurance segment can beestimated by accessing AHC data for Optum (Eden PrairieMN) and Truven Health (Ann Arbor MI) which in 2010together comprise approximately 68 million individuals or 35of the 2010 privately insured US population MS prevalence inthe government-insured segment of the population can bedirectly and completely estimated for 100 of people coveredby using administrative claims data for Medicaid and MedicareMS prevalence in the military population which is pre-dominantly male can be estimated used the Veterans HealthAdministration database A limitation of this method is that noclaims data exist for persons without health insurance estimatedat 163 in 201028 however for this uninsured group MSprevalence estimates from the Medicaid health care claims datacould be applied because the 2 groups have similar sociodemo-graphic characteristics
Our new approach cannot be applied to estimate the in-cidence of MS in the United States Incidencemdashthe number
of new MS cases per year in a populationmdashis an importantmeasure of disease frequency However it can only be derivedfor countries that have single uniform health care systemswhere longitudinal AHC records for each person enable rel-atively precise indicators of the onset of new MS diagnosisand the exclusion of existing prevalent cases The lack ofa single payer health care system or national tracking systemin the United States does not allow reliable estimates of MSincidence because some individuals may change health carecoverage over time and it is not possible to link patientrecords across insurance sources to provide a single longi-tudinal record within which newly diagnosed persons withMS may be ascertained This creates short periods of ob-servation which do not allow accurate estimates of incidencefor conditions such as MS and cancer due to the inability todefinitively determine which individuals are truly newlydiagnosed29
DiscussionWe have proposed a new approach for applying validatedcase-finding algorithms to AHC data from both governmentand private sources to produce robust estimates of MSprevalence in the United States In a companion article weapplied this approach to estimate the total number of MScases in the United States30 This approach could be appliedto estimate prevalence of other neurologic disorders andchronic conditions that face similar methodologic challengessuch as Parkinson disease dementia and epilepsy
There are several reasons why our new approach is a valuablemethodologic development to estimate the national MSprevalence First this paradigm offers the potential to useexisting AHC data for case ascertainment across the UnitedStates without requiring the cost and effort involved in re-gional MS prevalence studies which typically employ in-tensive case ascertainment methods The data are sufficientlydistributed both geographically and socioeconomically tobe representative of the entire US population and do notrequire consent because the databases are de-identifiedSecond our method is efficient and cost-effective and can beapplied repeatedly with datasets that represent a large pro-portion of the country enabling updates to population-based estimates of MS prevalence over time Third applyingthis approach with data that represent the entire UnitedStates allows us to obtain more stable and precise prevalenceestimates and to fill in knowledge gaps regarding the prev-alence of MS in many regions for which we have never hadestimates Once AHC data are able to accurately and com-pletely capture race and ethnicity this approach could beapplied to racial and ethnic minorities that have receivedlittle study in the past Fourth the use of a highly accuratecase-finding algorithm4 ensures that there will be greatercomparability between estimates derived from these sourcesin the future By adopting a standard paradigm for ascer-taining MS cases and applying validated case definition
Figure 1 Stepwise process for determining the prevalenceof multiple sclerosis (MS) in the United States
476 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
criteria we will be better able to monitor and comparespatial differences in MS prevalence and to examine changesin disease prevalence over time without the variation in-troduced by differing methodologic approaches
Despite many strengths our new approach is limited in thatthe case ascertainment methods do not cover all segments ofthe US population It excludes native American residents whochoose to receive care through the Indian Health Service
Figure 2 Source of health insurance by age (estimates from the current population survey 2008ndash2010)
(A) Population younger than 65 years (B) Population 65 years of age and older
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 477
(06 of the US population in 2010)31 and US residents whoare incarcerated (approximately 05 of the US population in2010)32 If health care databases existed for these populationswe could similarly apply an MS algorithm to estimate MSprevalence and incorporate them into the overall nationalestimate Our approach also cannot distinguish between dif-ferent racial and ethnic groups thus we cannot address towhat extent variations in prevalence by geography or otherfactors may be better explained by racialethnic differences inprevalence33
Our work has important implications for the new era of MSepidemiologic research that will be possible through the 21stCentury Cures Act legislation enacted in December 2016which authorized the establishment of a federally fundedneurologic disorders surveillance system34 A national registryfor MS could be implemented similar to the NationalAmyotrophic Lateral Sclerosis Registry with AHC data asa primary method for case ascertainment and a web portalavailable for all persons with MS to register242535 Withoutaccess to a national registry in the intermediate term wepropose that our approach will deliver the most current andscientifically sound US estimate of the number of personswith MS By addressing methodologic challenges and pro-posing a new paradigm for measuring the prevalence of MS inthe United States we hope that our work will benefit scientistswho study all chronic conditions for which national preva-lence estimates do not currently exist
AcknowledgmentThe authors thank the following members of the US MultipleSclerosis Prevalence Workgroup for their contributionsAlbert Lo Robert McBurney Oleg Muravov Bari Talenteand Leslie Ritter The authors also thank the following keystaff members at the National Multiple Sclerosis Society fortheir contributions to this project Cathy Carlson TimCoetzee Sherri Giger Weyman Johnson Eileen MadrayGraham McReynolds and Cyndi Zagieboylo
Study fundingThe study was funded by contracts from the National Mul-tiple Sclerosis Society to the principal investigators in the MSPrevalence Working Group (HC-1508-05693) The ArticleProcessing Charge was funded by the National MultipleSclerosis Society
DisclosureL Nelson receives grants from the Centers for DiseaseControl and Prevention NIH and National Multiple Scle-rosis Society and contracts from the Agency for Toxic Sub-stances and Diseases Registry She receives compensation forserving as a consultant to Acumen Inc and is on the DataMonitoring Committee of Neuropace M Wallin has servedon data safety monitoring boards for the National Institutes ofNeurological Disease and StrokendashNIH has been an associateeditor for the Encyclopedia of the Neurological Sciences andreceived funding support from the National Multiple Sclerosis
Society and the Department of Veterans Affairs Merit ReviewResearch Program R Marrie is supported by the WaughFamily Chair in Multiple Sclerosis receives research fundingfrom Canadian Institutes of Health Research ResearchManitoba Multiple Sclerosis Society of Canada MultipleSclerosis Scientific Foundation National Multiple SclerosisSociety and Rx amp D Health Research Foundation and hasconducted clinical trials funded by Sanofi-Aventis She alsoserves on the Editorial Board ofNeurologyregW Culpepper hasadditional research funding from the National MultipleSclerosis Society receives support from the VHA MS Centerof Excellence and is a member of the National MultipleSclerosis Society Health Care Delivery and Policy Researchstudy section A Langer-Gould is site principal investigatorfor 2 industry-sponsored phase 3 clinical trials (BiogenIdec Hoffman-LaRoche) and was site PI for one industry-sponsored observation study (Biogen Idec) She receivesgrant support from the NIH National Institute of Neuro-logical Disorders and Stroke Patient-Centered OutcomesResearch Institute and the National Multiple Sclerosis Soci-ety J Campbell has consultancy or research grants over thelast 5 years with Agency for Healthcare Research and QualityALSAM Foundation Amgen AstraZeneca Bayer BiogenIdec Boehringer Ingelheim Centers for Disease Control andPrevention Colorado Medicaid Enterprise CommunityPartners Inc Institute for Clinical and Economic ReviewMallinckrodt NIH National Multiple Sclerosis Society Kai-ser Permanente PhRMA Foundation Teva Research in RealLife Ltd Respiratory Effectiveness Group and Zogenix IncS Buka receives research funding from the NIH and theNational Multiple Sclerosis Society H Tremlett is theCanada Research Chair for Neuroepidemiology and MultipleSclerosis She receives research support from the NationalMultiple Sclerosis Society the Canadian Institutes of HealthResearch the Multiple Sclerosis Society of Canada and theMultiple Sclerosis Scientific Research Foundation In addi-tion in the last 5 years she has received research support fromthe Multiple Sclerosis Society of Canada the Michael SmithFoundation for Health Research and the UK MS Trust andspeaker honoraria andor travel expenses to attend confer-ences G Cutter is a member of Data and Safety MonitoringBoards for AMO Pharmaceuticals Apotek Horizon Phar-maceuticals ModigenetechProlor Merck MerckPfizerOpko Biologics Neurim Sanofi-Aventis Reata Pharmaceut-icals ReceptosCelgene Teva pharmaceuticals NHLBI(Protocol Review Committee) and NICHD (OPRU over-sight committee) and is on the Consulting or AdvisoryBoards for Atara Biotherapeutics Argenix Bioeq GmbHConsortium of MS Centers (grant) Genzyme GenentechInnate Therapeutics Klein-Buendel Incorporated Medi-mmune Medday Novartis Opexa Therapeutics RocheSavara Inc Somahlution Teva Pharmaceuticals Trans-parency Life Sciences and TGTherapeutics W Kaye receivesfunding from the Agency for Toxic Substances and DiseaseRegistry the National Multiple Sclerosis Society and theAssociation for the Accreditation of Human ResearchProtection Programs L Wagner receives funding from the
478 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Agency for Toxic Substances and Disease Registry and Na-tional Multiple Sclerosis Society N LaRocca is employed fulltime by the National Multiple Sclerosis Society and has noother disclosures to report Statistical analysis conducted byDr Gary Cutter PhD University of Alabama at BirminghamGo to NeurologyorgN for full disclosures
Publication historyReceived byNeurology July 17 2018 Accepted in final form October 222018
References1 Wallin MT Kurtzke JF Neuroepidemiology In Bradley WG Daroff RB Fenichel
GM Jankovic J editors Neurology in Clinical Practice Philadelphia Butterworth-Heinemann 2008762ndash780
2 Browne P Chandraratna D Angood C et al Atlas of multiple sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
3 Mayr WT Pittock SJ McClelland RL Jorgensen NW Noseworthy JH Rodriguez MIncidence and prevalence of multiple sclerosis in Olmsted County Minnesota 1985-2000 Neurology 2003611373ndash1377
4 Evans C Beland SG Kulaga S et al Incidence and prevalence of multiple sclerosis inthe Americas a systematic review Neuroepidemiology 201340195ndash210
5 Noonan CW Williamson DM Henry JP et al The prevalence of multiple sclerosis in3 US communities Prev Chronic Dis 20107A1
6 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
7 Baum HM Rothschild BB The incidence and prevalence of reported multiple scle-rosis Ann Neurol 198110420ndash428
8 Anderson DW Ellenberg JH Leventhal CM Reingold SC Rodriguez M SilberbergDH Revised estimate of the prevalence of multiple sclerosis in the United States AnnNeurol 199231333ndash336
9 Nelson LM Hamman RF Thompson DS et al Higher than expected prevalence ofmultiple sclerosis in Northern Colorado dependence on methodological issuesNeuroepidemiology 1986517ndash28
10 Collins JG Prevalence of selected chronic conditions United States 1990-1992 VitalHealth Stat 10 19971941ndash89
Appendix 1 Authors
Name Location Role Contribution
Lorene MNelsonMS PhD
Stanford UniversityCA
Author Study concept anddesign preparation ofdraft manuscriptrevision of themanuscript forcontent approval offinal manuscript
Mitchell TWallin MDMPH
Veterans HealthAdministrationGeorgetownUniversityWashington DC
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
Ruth AnnMarrieMD PhD
University ofManitoba WinnipegCanada
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
William JCulpepperPhD MA
Veterans HealthAdministrationWashington DCUniversity ofMaryland Baltimore
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
AnnetteLanger-GouldMD PhD
Kaiser PermanenteSouthern CaliforniaLos Angeles
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
JonathanCampbellPhD
University of DenverCO
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
StephenBuka PhD
Brown UniversityProvidence RI
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
HelenTremlettPhD
University of BritishColumbia VancouverCanada
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
GaryCutterPhD
University ofAlabamaBirmingham
Author Study concept anddesign critical reviewof the manuscript forcontent
Appendix 1 (continued)
Name Location Role Contribution
WendyKaye PhD
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
LaurieWagnerMPH
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Nicholas GLaRoccaPhD
National MultipleSclerosis Society NewYork NY
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Appendix 2 Coinvestigators and members of the USMultiple Sclerosis Prevalence Workgroup
Name Location Role Contribution
Albert LoMD PhD
Brown UniversityProvidence RI
Coinvestigator Studyconcept anddesign
RobertMcBurneyPhD
Accelerated CureProject Boston MA
Coinvestigator Studyconcept anddesign
OlegMuravovPhD
Agency for ToxicSubstances andDisease RegistryDivision of HealthStudies Atlanta GA
Coinvestigator Studyconcept anddesign
BariTalenteEsq
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
LeslieRitter
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 479
11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

case definitions or even neurologist diagnoses for accuracyTwo studies used a case definition that required only a singlehealth care encounter for MS1215 which is likely to be highlynonspecific risking an unknown number of false-positives Thestudy by Dilokthornsakul et al16 that used private insuranceclaims data was strengthened by conducting sensitivity analysesthat examined the performance of 2 alternative algorithms oneof which produced estimates very similar to the primaryalgorithm
Developing a new approach forestimating MS prevalence in theUnited StatesBased on the SWOT analysis and through discussion andconsensus we concluded that AHC data would provide themost cost-effective method to develop a national prevalenceestimate for MS Collectively government and private healthclaims databases represent a very large proportion of the USpopulation (84 in 2010)28 which together enables preciseestimates of MS prevalence The data are sufficiently distrib-uted geographically and socioeconomically to be representa-tive of the entire US population Figure 1 illustrates a new4-step approach we devised for estimating the prevalence ofMS for the United States as a whole using a segmental
approach for each insurance source and then combining theminto a national estimate
Step 1 Identify datasets covering US publicly and privatelyinsured populations figure 2 illustrates the fragmented natureof insurance coverage of the US population which doesnot enable a single health care source for estimating MSprevalence as is often available in Scandinavian countries withnational unified health care systems Nevertheless AHC dataare available for almost all of the insurance segments of theUS population allowing the estimation of MS prevalenceseparately for each insurance segment which can then beaggregated into an overall national estimate ofMS prevalenceFigure 2 shows US Census Current Population Survey datafor 2008ndash2010 presented separately for individuals under age65 vs those ages 65 and older because the sources of insurancecoverage vary considerably for these 2 age groups In 2010 forindividuals below age 65 private insurance comprised thelargest segment of insurance coverage 65 when employer-purchased and self-purchased private insurance were consid-ered together The next largest segment of insurance coveragein 2010 for individuals under age 65 is Medicaid (17)a government insurance program that provides free medicalinsurance to low-income people Smaller percentages ofindividuals under age 65 in 2010 were covered by a militarysource such as Department of Defense (DOD) or Veterans
Table 4 Strengths weaknesses opportunities and threats (SWOT) analysis using national probability survey samples toestimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can be obtained from existinggovernment surveys
Dedicated MS-specific patientsurveys are costly to carry out andinfeasible for national scope
This method can be feasible ifmultiple years of survey data can beaggregated
Existing national probabilitysamples usually comprise onlysegments of the US population(ie noninstitutionalized)
Sampling designs are rigorous(probability samples) of the USpopulation rigorously collected forresearch purposes according tostandard protocols
Survey participation rates are athistorically low levels
Successful application would requireaccess to a very large survey samplesuch as the BRFSS conducted annuallyby the CDC however a geographicallyvalid sample of select states wouldneed to be selected to represent thenation
Survey questions for patients andfamily members have not beenvalidated for accuracy againsta gold standard (neurologistdiagnosis)
Data are accessible and either cost-free or low-cost
Surveys rely on MS diagnosisreported by patient or a familymember which are susceptible toboth underreporting and false-positive reports
If survey questions were validatedagainst a gold standard (neurologistdiagnosis) this method could befeasibly implemented in a subset ofUS states
Restrictions on number ofquestions limits collection ofclinical details (eg clinicalcourse disability status)
Data are available on age sex raceethnicity broad geographic locationand other sociodemographiccharacteristics
Count ofMS patients in single yearsof data are often too small forprecise estimation
Some surveys collect self-reporteddata that can inform other analyseseg prevalence of comorbidity healthcare utilization and cost DMT uselifestyle risk factors
Overall prevalence might beestimable but data are often toosparse for getting breakdowns bysex age race or geographic region
Abbreviations BRFSS = Behavioral Risk Factor Surveillance Survey CDC = Centers for Disease Control and Prevention DMT = disease-modifying treatmentIn the United States national probability survey samples include the National Health Interview Survey Medical Expenditure Panel Survey HouseholdComponent National Nursing Home Survey and the BRFSS (a probability survey completed by500000 Americans per year and for which disease-specificquestions can be added on a state-by-state basis)
474 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Health Administration (VHA) (4) or by anothergovernment-provided insurance plan (Medicare 3) In2010 18 of individuals under age 65 had no insurancecoverage In 2010 for individuals ages 65 and abovegovernment insurance provided by Medicare covered 93of the population and was often supplemented by privatecoinsurance (33 employer-provided 29 self-purchased)Medicaid either alone or in combination with Medicarecovered 9 of those age 65 and above In 2010 8 ofindividuals age 65 and above were covered by amilitary source(DOD or VHA) and only 2 of the elderly were uninsuredThus despite the fragmentation of the US health care systemAHC databases for all of the insured segments of the USpopulation are available and can be used to estimate MSprevalence in each dataset separately before combining theestimates into a whole (step 4)Step 2 Develop and validate a highly accurate MS case-finding algorithm that can be standardly applied in all AHCdatabases Our approach requires a highly accurate casedefinition to identify MS cases that performs consistently
across AHC databases with differing characteristics so thatit can be applied even in datasets where formal validationis not possible Notably no MS prevalence studies in theUnited States have used validated algorithms for identifyingpersons with MS yet having a validated algorithm for thispurpose is a necessary step for carrying out valid prevalenceestimation26 Culpepper et al27 recently conducted a multi-site validation study to develop a valid and reliable algorithmfor identifying MS cases using AHC data with excellentsensitivity specificity and positive predictive value For thefirst time ever this provides a high-performing algorithmthat performs consistently well across datasets and can beapplied across all AHC databases Similar methodologycould be employed for other chronic neurologic diseasesusing existing literature to provide a starting point for thedevelopment of such case definitions26
Step 3 Apply the case definition algorithm to estimate thenumber of MS cases and prevalence estimates separately foreach database The third step of this approach is simply touse the validated algorithm (step 2) within each of the
Table 5 Strengths weaknesses opportunities and threats (SWOT) analysis using administrative health claims databasesto estimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can develop systematic approachthat could be repeatedly utilizedover time to obtain estimates nowand in the future
Lack of universal health care in theUnited States therefore not allpatients are identifiable throughadministrative data
Can develop a systematic approachthat can be repeatedly utilized overtime to obtain estimates now and inthe future
Lack of certainty whether casedefinitions developed in one datasetwill have same performancecharacteristics in other datasets
Data are accessible and relativelylow-cost
Must accessmultiple administrativedatasets
A case definition can be validated in2 or 3 different administrativedatasets to show consistency offindings across datasets thenapplied even in datasets wherevalidation is not possible4
No easily accessible national sourceof data for uninsured or self-paypopulations
Consistent capture of sex and dateof birth supports calculation of age-and sex-specific prevalenceestimates
Data are collected for health systemmanagement therefore theirvalidity for research must becarefully assessed
If a careful analytic approach is usedcan minimize overlap betweendatasets and avoid duplicatecounting
No easily accessible data forincarcerated or aboriginalpopulations
Data often include zip code whichcan be geocoded to determinesocioeconomic status and establishregion of residence
Lack of identified data to enableidentification of duplicates createsdifficulty identifying the sameindividuals in overlapping datasets
Would ideally include collection ofpatient identifiers to identifyduplicates present inmore than onedatabase howevernongovernment researchers arenot allowed access to suchidentifiers
These databases often haveadditional information that couldinform other analyses egprevalence of comorbidity healthcare utilization and disease-modifying treatment use
Some datasets lack informationregarding raceethnicity or havepoor geographic resolution
Representativeness cannot accessall administrative health databasesin United States must select few toestimate MS prevalence andextrapolate to all
Issue of misdiagnosis as a source oferror lack of clinical detail makes itdifficult to distinguish inaccuratelycoded diagnoses from clinicianmisdiagnosis
In the United States administrative health claims databases include Medicare (a government insurance program covering 93 of US residents age 65 andabove) Medicaid (a government insurance program for low-income parents and children and disabled persons in the United States) the Minimum Data Set(administrative data onMedicare- or Medicaid-certified nursing facilities) the Veterans Health Administration (health care program for veterans of US wars)commercial health insurance claims data (for employer-paid or self-paid insurance) and health maintenance organization health records
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 475
databases (step 1) to obtain valid MS prevalence estimates(overall and specific with respect to age sex raceethnicityand geographic location)Step 4 CombineMSprevalence estimates into a single estimateof the prevalence of MS for the United States weightedaccording to the number of insured persons in each healthinsurance segment after obtaining MS prevalence estimatesseparately for each of the US health insurance segments theycan be combined into a single national prevalence estimateInformation from theCurrent Population Survey can be used toobtain the necessary weights by determining the number of USresidents with each type of insurance coverage stratified by sexage group race and geographic region The total estimatednumber of MS cases for each age sex race and geographicregionndashspecific category can then be summed to estimatethe total number ofMS cases in the United States For exampleMS prevalence for the private insurance segment can beestimated by accessing AHC data for Optum (Eden PrairieMN) and Truven Health (Ann Arbor MI) which in 2010together comprise approximately 68 million individuals or 35of the 2010 privately insured US population MS prevalence inthe government-insured segment of the population can bedirectly and completely estimated for 100 of people coveredby using administrative claims data for Medicaid and MedicareMS prevalence in the military population which is pre-dominantly male can be estimated used the Veterans HealthAdministration database A limitation of this method is that noclaims data exist for persons without health insurance estimatedat 163 in 201028 however for this uninsured group MSprevalence estimates from the Medicaid health care claims datacould be applied because the 2 groups have similar sociodemo-graphic characteristics
Our new approach cannot be applied to estimate the in-cidence of MS in the United States Incidencemdashthe number
of new MS cases per year in a populationmdashis an importantmeasure of disease frequency However it can only be derivedfor countries that have single uniform health care systemswhere longitudinal AHC records for each person enable rel-atively precise indicators of the onset of new MS diagnosisand the exclusion of existing prevalent cases The lack ofa single payer health care system or national tracking systemin the United States does not allow reliable estimates of MSincidence because some individuals may change health carecoverage over time and it is not possible to link patientrecords across insurance sources to provide a single longi-tudinal record within which newly diagnosed persons withMS may be ascertained This creates short periods of ob-servation which do not allow accurate estimates of incidencefor conditions such as MS and cancer due to the inability todefinitively determine which individuals are truly newlydiagnosed29
DiscussionWe have proposed a new approach for applying validatedcase-finding algorithms to AHC data from both governmentand private sources to produce robust estimates of MSprevalence in the United States In a companion article weapplied this approach to estimate the total number of MScases in the United States30 This approach could be appliedto estimate prevalence of other neurologic disorders andchronic conditions that face similar methodologic challengessuch as Parkinson disease dementia and epilepsy
There are several reasons why our new approach is a valuablemethodologic development to estimate the national MSprevalence First this paradigm offers the potential to useexisting AHC data for case ascertainment across the UnitedStates without requiring the cost and effort involved in re-gional MS prevalence studies which typically employ in-tensive case ascertainment methods The data are sufficientlydistributed both geographically and socioeconomically tobe representative of the entire US population and do notrequire consent because the databases are de-identifiedSecond our method is efficient and cost-effective and can beapplied repeatedly with datasets that represent a large pro-portion of the country enabling updates to population-based estimates of MS prevalence over time Third applyingthis approach with data that represent the entire UnitedStates allows us to obtain more stable and precise prevalenceestimates and to fill in knowledge gaps regarding the prev-alence of MS in many regions for which we have never hadestimates Once AHC data are able to accurately and com-pletely capture race and ethnicity this approach could beapplied to racial and ethnic minorities that have receivedlittle study in the past Fourth the use of a highly accuratecase-finding algorithm4 ensures that there will be greatercomparability between estimates derived from these sourcesin the future By adopting a standard paradigm for ascer-taining MS cases and applying validated case definition
Figure 1 Stepwise process for determining the prevalenceof multiple sclerosis (MS) in the United States
476 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
criteria we will be better able to monitor and comparespatial differences in MS prevalence and to examine changesin disease prevalence over time without the variation in-troduced by differing methodologic approaches
Despite many strengths our new approach is limited in thatthe case ascertainment methods do not cover all segments ofthe US population It excludes native American residents whochoose to receive care through the Indian Health Service
Figure 2 Source of health insurance by age (estimates from the current population survey 2008ndash2010)
(A) Population younger than 65 years (B) Population 65 years of age and older
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 477
(06 of the US population in 2010)31 and US residents whoare incarcerated (approximately 05 of the US population in2010)32 If health care databases existed for these populationswe could similarly apply an MS algorithm to estimate MSprevalence and incorporate them into the overall nationalestimate Our approach also cannot distinguish between dif-ferent racial and ethnic groups thus we cannot address towhat extent variations in prevalence by geography or otherfactors may be better explained by racialethnic differences inprevalence33
Our work has important implications for the new era of MSepidemiologic research that will be possible through the 21stCentury Cures Act legislation enacted in December 2016which authorized the establishment of a federally fundedneurologic disorders surveillance system34 A national registryfor MS could be implemented similar to the NationalAmyotrophic Lateral Sclerosis Registry with AHC data asa primary method for case ascertainment and a web portalavailable for all persons with MS to register242535 Withoutaccess to a national registry in the intermediate term wepropose that our approach will deliver the most current andscientifically sound US estimate of the number of personswith MS By addressing methodologic challenges and pro-posing a new paradigm for measuring the prevalence of MS inthe United States we hope that our work will benefit scientistswho study all chronic conditions for which national preva-lence estimates do not currently exist
AcknowledgmentThe authors thank the following members of the US MultipleSclerosis Prevalence Workgroup for their contributionsAlbert Lo Robert McBurney Oleg Muravov Bari Talenteand Leslie Ritter The authors also thank the following keystaff members at the National Multiple Sclerosis Society fortheir contributions to this project Cathy Carlson TimCoetzee Sherri Giger Weyman Johnson Eileen MadrayGraham McReynolds and Cyndi Zagieboylo
Study fundingThe study was funded by contracts from the National Mul-tiple Sclerosis Society to the principal investigators in the MSPrevalence Working Group (HC-1508-05693) The ArticleProcessing Charge was funded by the National MultipleSclerosis Society
DisclosureL Nelson receives grants from the Centers for DiseaseControl and Prevention NIH and National Multiple Scle-rosis Society and contracts from the Agency for Toxic Sub-stances and Diseases Registry She receives compensation forserving as a consultant to Acumen Inc and is on the DataMonitoring Committee of Neuropace M Wallin has servedon data safety monitoring boards for the National Institutes ofNeurological Disease and StrokendashNIH has been an associateeditor for the Encyclopedia of the Neurological Sciences andreceived funding support from the National Multiple Sclerosis
Society and the Department of Veterans Affairs Merit ReviewResearch Program R Marrie is supported by the WaughFamily Chair in Multiple Sclerosis receives research fundingfrom Canadian Institutes of Health Research ResearchManitoba Multiple Sclerosis Society of Canada MultipleSclerosis Scientific Foundation National Multiple SclerosisSociety and Rx amp D Health Research Foundation and hasconducted clinical trials funded by Sanofi-Aventis She alsoserves on the Editorial Board ofNeurologyregW Culpepper hasadditional research funding from the National MultipleSclerosis Society receives support from the VHA MS Centerof Excellence and is a member of the National MultipleSclerosis Society Health Care Delivery and Policy Researchstudy section A Langer-Gould is site principal investigatorfor 2 industry-sponsored phase 3 clinical trials (BiogenIdec Hoffman-LaRoche) and was site PI for one industry-sponsored observation study (Biogen Idec) She receivesgrant support from the NIH National Institute of Neuro-logical Disorders and Stroke Patient-Centered OutcomesResearch Institute and the National Multiple Sclerosis Soci-ety J Campbell has consultancy or research grants over thelast 5 years with Agency for Healthcare Research and QualityALSAM Foundation Amgen AstraZeneca Bayer BiogenIdec Boehringer Ingelheim Centers for Disease Control andPrevention Colorado Medicaid Enterprise CommunityPartners Inc Institute for Clinical and Economic ReviewMallinckrodt NIH National Multiple Sclerosis Society Kai-ser Permanente PhRMA Foundation Teva Research in RealLife Ltd Respiratory Effectiveness Group and Zogenix IncS Buka receives research funding from the NIH and theNational Multiple Sclerosis Society H Tremlett is theCanada Research Chair for Neuroepidemiology and MultipleSclerosis She receives research support from the NationalMultiple Sclerosis Society the Canadian Institutes of HealthResearch the Multiple Sclerosis Society of Canada and theMultiple Sclerosis Scientific Research Foundation In addi-tion in the last 5 years she has received research support fromthe Multiple Sclerosis Society of Canada the Michael SmithFoundation for Health Research and the UK MS Trust andspeaker honoraria andor travel expenses to attend confer-ences G Cutter is a member of Data and Safety MonitoringBoards for AMO Pharmaceuticals Apotek Horizon Phar-maceuticals ModigenetechProlor Merck MerckPfizerOpko Biologics Neurim Sanofi-Aventis Reata Pharmaceut-icals ReceptosCelgene Teva pharmaceuticals NHLBI(Protocol Review Committee) and NICHD (OPRU over-sight committee) and is on the Consulting or AdvisoryBoards for Atara Biotherapeutics Argenix Bioeq GmbHConsortium of MS Centers (grant) Genzyme GenentechInnate Therapeutics Klein-Buendel Incorporated Medi-mmune Medday Novartis Opexa Therapeutics RocheSavara Inc Somahlution Teva Pharmaceuticals Trans-parency Life Sciences and TGTherapeutics W Kaye receivesfunding from the Agency for Toxic Substances and DiseaseRegistry the National Multiple Sclerosis Society and theAssociation for the Accreditation of Human ResearchProtection Programs L Wagner receives funding from the
478 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Agency for Toxic Substances and Disease Registry and Na-tional Multiple Sclerosis Society N LaRocca is employed fulltime by the National Multiple Sclerosis Society and has noother disclosures to report Statistical analysis conducted byDr Gary Cutter PhD University of Alabama at BirminghamGo to NeurologyorgN for full disclosures
Publication historyReceived byNeurology July 17 2018 Accepted in final form October 222018
References1 Wallin MT Kurtzke JF Neuroepidemiology In Bradley WG Daroff RB Fenichel
GM Jankovic J editors Neurology in Clinical Practice Philadelphia Butterworth-Heinemann 2008762ndash780
2 Browne P Chandraratna D Angood C et al Atlas of multiple sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
3 Mayr WT Pittock SJ McClelland RL Jorgensen NW Noseworthy JH Rodriguez MIncidence and prevalence of multiple sclerosis in Olmsted County Minnesota 1985-2000 Neurology 2003611373ndash1377
4 Evans C Beland SG Kulaga S et al Incidence and prevalence of multiple sclerosis inthe Americas a systematic review Neuroepidemiology 201340195ndash210
5 Noonan CW Williamson DM Henry JP et al The prevalence of multiple sclerosis in3 US communities Prev Chronic Dis 20107A1
6 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
7 Baum HM Rothschild BB The incidence and prevalence of reported multiple scle-rosis Ann Neurol 198110420ndash428
8 Anderson DW Ellenberg JH Leventhal CM Reingold SC Rodriguez M SilberbergDH Revised estimate of the prevalence of multiple sclerosis in the United States AnnNeurol 199231333ndash336
9 Nelson LM Hamman RF Thompson DS et al Higher than expected prevalence ofmultiple sclerosis in Northern Colorado dependence on methodological issuesNeuroepidemiology 1986517ndash28
10 Collins JG Prevalence of selected chronic conditions United States 1990-1992 VitalHealth Stat 10 19971941ndash89
Appendix 1 Authors
Name Location Role Contribution
Lorene MNelsonMS PhD
Stanford UniversityCA
Author Study concept anddesign preparation ofdraft manuscriptrevision of themanuscript forcontent approval offinal manuscript
Mitchell TWallin MDMPH
Veterans HealthAdministrationGeorgetownUniversityWashington DC
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
Ruth AnnMarrieMD PhD
University ofManitoba WinnipegCanada
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
William JCulpepperPhD MA
Veterans HealthAdministrationWashington DCUniversity ofMaryland Baltimore
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
AnnetteLanger-GouldMD PhD
Kaiser PermanenteSouthern CaliforniaLos Angeles
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
JonathanCampbellPhD
University of DenverCO
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
StephenBuka PhD
Brown UniversityProvidence RI
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
HelenTremlettPhD
University of BritishColumbia VancouverCanada
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
GaryCutterPhD
University ofAlabamaBirmingham
Author Study concept anddesign critical reviewof the manuscript forcontent
Appendix 1 (continued)
Name Location Role Contribution
WendyKaye PhD
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
LaurieWagnerMPH
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Nicholas GLaRoccaPhD
National MultipleSclerosis Society NewYork NY
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Appendix 2 Coinvestigators and members of the USMultiple Sclerosis Prevalence Workgroup
Name Location Role Contribution
Albert LoMD PhD
Brown UniversityProvidence RI
Coinvestigator Studyconcept anddesign
RobertMcBurneyPhD
Accelerated CureProject Boston MA
Coinvestigator Studyconcept anddesign
OlegMuravovPhD
Agency for ToxicSubstances andDisease RegistryDivision of HealthStudies Atlanta GA
Coinvestigator Studyconcept anddesign
BariTalenteEsq
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
LeslieRitter
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 479
11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Health Administration (VHA) (4) or by anothergovernment-provided insurance plan (Medicare 3) In2010 18 of individuals under age 65 had no insurancecoverage In 2010 for individuals ages 65 and abovegovernment insurance provided by Medicare covered 93of the population and was often supplemented by privatecoinsurance (33 employer-provided 29 self-purchased)Medicaid either alone or in combination with Medicarecovered 9 of those age 65 and above In 2010 8 ofindividuals age 65 and above were covered by amilitary source(DOD or VHA) and only 2 of the elderly were uninsuredThus despite the fragmentation of the US health care systemAHC databases for all of the insured segments of the USpopulation are available and can be used to estimate MSprevalence in each dataset separately before combining theestimates into a whole (step 4)Step 2 Develop and validate a highly accurate MS case-finding algorithm that can be standardly applied in all AHCdatabases Our approach requires a highly accurate casedefinition to identify MS cases that performs consistently
across AHC databases with differing characteristics so thatit can be applied even in datasets where formal validationis not possible Notably no MS prevalence studies in theUnited States have used validated algorithms for identifyingpersons with MS yet having a validated algorithm for thispurpose is a necessary step for carrying out valid prevalenceestimation26 Culpepper et al27 recently conducted a multi-site validation study to develop a valid and reliable algorithmfor identifying MS cases using AHC data with excellentsensitivity specificity and positive predictive value For thefirst time ever this provides a high-performing algorithmthat performs consistently well across datasets and can beapplied across all AHC databases Similar methodologycould be employed for other chronic neurologic diseasesusing existing literature to provide a starting point for thedevelopment of such case definitions26
Step 3 Apply the case definition algorithm to estimate thenumber of MS cases and prevalence estimates separately foreach database The third step of this approach is simply touse the validated algorithm (step 2) within each of the
Table 5 Strengths weaknesses opportunities and threats (SWOT) analysis using administrative health claims databasesto estimate national multiple sclerosis (MS) prevalence in the US
Strengths Weaknesses Opportunities Threats
Can develop systematic approachthat could be repeatedly utilizedover time to obtain estimates nowand in the future
Lack of universal health care in theUnited States therefore not allpatients are identifiable throughadministrative data
Can develop a systematic approachthat can be repeatedly utilized overtime to obtain estimates now and inthe future
Lack of certainty whether casedefinitions developed in one datasetwill have same performancecharacteristics in other datasets
Data are accessible and relativelylow-cost
Must accessmultiple administrativedatasets
A case definition can be validated in2 or 3 different administrativedatasets to show consistency offindings across datasets thenapplied even in datasets wherevalidation is not possible4
No easily accessible national sourceof data for uninsured or self-paypopulations
Consistent capture of sex and dateof birth supports calculation of age-and sex-specific prevalenceestimates
Data are collected for health systemmanagement therefore theirvalidity for research must becarefully assessed
If a careful analytic approach is usedcan minimize overlap betweendatasets and avoid duplicatecounting
No easily accessible data forincarcerated or aboriginalpopulations
Data often include zip code whichcan be geocoded to determinesocioeconomic status and establishregion of residence
Lack of identified data to enableidentification of duplicates createsdifficulty identifying the sameindividuals in overlapping datasets
Would ideally include collection ofpatient identifiers to identifyduplicates present inmore than onedatabase howevernongovernment researchers arenot allowed access to suchidentifiers
These databases often haveadditional information that couldinform other analyses egprevalence of comorbidity healthcare utilization and disease-modifying treatment use
Some datasets lack informationregarding raceethnicity or havepoor geographic resolution
Representativeness cannot accessall administrative health databasesin United States must select few toestimate MS prevalence andextrapolate to all
Issue of misdiagnosis as a source oferror lack of clinical detail makes itdifficult to distinguish inaccuratelycoded diagnoses from clinicianmisdiagnosis
In the United States administrative health claims databases include Medicare (a government insurance program covering 93 of US residents age 65 andabove) Medicaid (a government insurance program for low-income parents and children and disabled persons in the United States) the Minimum Data Set(administrative data onMedicare- or Medicaid-certified nursing facilities) the Veterans Health Administration (health care program for veterans of US wars)commercial health insurance claims data (for employer-paid or self-paid insurance) and health maintenance organization health records
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 475
databases (step 1) to obtain valid MS prevalence estimates(overall and specific with respect to age sex raceethnicityand geographic location)Step 4 CombineMSprevalence estimates into a single estimateof the prevalence of MS for the United States weightedaccording to the number of insured persons in each healthinsurance segment after obtaining MS prevalence estimatesseparately for each of the US health insurance segments theycan be combined into a single national prevalence estimateInformation from theCurrent Population Survey can be used toobtain the necessary weights by determining the number of USresidents with each type of insurance coverage stratified by sexage group race and geographic region The total estimatednumber of MS cases for each age sex race and geographicregionndashspecific category can then be summed to estimatethe total number ofMS cases in the United States For exampleMS prevalence for the private insurance segment can beestimated by accessing AHC data for Optum (Eden PrairieMN) and Truven Health (Ann Arbor MI) which in 2010together comprise approximately 68 million individuals or 35of the 2010 privately insured US population MS prevalence inthe government-insured segment of the population can bedirectly and completely estimated for 100 of people coveredby using administrative claims data for Medicaid and MedicareMS prevalence in the military population which is pre-dominantly male can be estimated used the Veterans HealthAdministration database A limitation of this method is that noclaims data exist for persons without health insurance estimatedat 163 in 201028 however for this uninsured group MSprevalence estimates from the Medicaid health care claims datacould be applied because the 2 groups have similar sociodemo-graphic characteristics
Our new approach cannot be applied to estimate the in-cidence of MS in the United States Incidencemdashthe number
of new MS cases per year in a populationmdashis an importantmeasure of disease frequency However it can only be derivedfor countries that have single uniform health care systemswhere longitudinal AHC records for each person enable rel-atively precise indicators of the onset of new MS diagnosisand the exclusion of existing prevalent cases The lack ofa single payer health care system or national tracking systemin the United States does not allow reliable estimates of MSincidence because some individuals may change health carecoverage over time and it is not possible to link patientrecords across insurance sources to provide a single longi-tudinal record within which newly diagnosed persons withMS may be ascertained This creates short periods of ob-servation which do not allow accurate estimates of incidencefor conditions such as MS and cancer due to the inability todefinitively determine which individuals are truly newlydiagnosed29
DiscussionWe have proposed a new approach for applying validatedcase-finding algorithms to AHC data from both governmentand private sources to produce robust estimates of MSprevalence in the United States In a companion article weapplied this approach to estimate the total number of MScases in the United States30 This approach could be appliedto estimate prevalence of other neurologic disorders andchronic conditions that face similar methodologic challengessuch as Parkinson disease dementia and epilepsy
There are several reasons why our new approach is a valuablemethodologic development to estimate the national MSprevalence First this paradigm offers the potential to useexisting AHC data for case ascertainment across the UnitedStates without requiring the cost and effort involved in re-gional MS prevalence studies which typically employ in-tensive case ascertainment methods The data are sufficientlydistributed both geographically and socioeconomically tobe representative of the entire US population and do notrequire consent because the databases are de-identifiedSecond our method is efficient and cost-effective and can beapplied repeatedly with datasets that represent a large pro-portion of the country enabling updates to population-based estimates of MS prevalence over time Third applyingthis approach with data that represent the entire UnitedStates allows us to obtain more stable and precise prevalenceestimates and to fill in knowledge gaps regarding the prev-alence of MS in many regions for which we have never hadestimates Once AHC data are able to accurately and com-pletely capture race and ethnicity this approach could beapplied to racial and ethnic minorities that have receivedlittle study in the past Fourth the use of a highly accuratecase-finding algorithm4 ensures that there will be greatercomparability between estimates derived from these sourcesin the future By adopting a standard paradigm for ascer-taining MS cases and applying validated case definition
Figure 1 Stepwise process for determining the prevalenceof multiple sclerosis (MS) in the United States
476 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
criteria we will be better able to monitor and comparespatial differences in MS prevalence and to examine changesin disease prevalence over time without the variation in-troduced by differing methodologic approaches
Despite many strengths our new approach is limited in thatthe case ascertainment methods do not cover all segments ofthe US population It excludes native American residents whochoose to receive care through the Indian Health Service
Figure 2 Source of health insurance by age (estimates from the current population survey 2008ndash2010)
(A) Population younger than 65 years (B) Population 65 years of age and older
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 477
(06 of the US population in 2010)31 and US residents whoare incarcerated (approximately 05 of the US population in2010)32 If health care databases existed for these populationswe could similarly apply an MS algorithm to estimate MSprevalence and incorporate them into the overall nationalestimate Our approach also cannot distinguish between dif-ferent racial and ethnic groups thus we cannot address towhat extent variations in prevalence by geography or otherfactors may be better explained by racialethnic differences inprevalence33
Our work has important implications for the new era of MSepidemiologic research that will be possible through the 21stCentury Cures Act legislation enacted in December 2016which authorized the establishment of a federally fundedneurologic disorders surveillance system34 A national registryfor MS could be implemented similar to the NationalAmyotrophic Lateral Sclerosis Registry with AHC data asa primary method for case ascertainment and a web portalavailable for all persons with MS to register242535 Withoutaccess to a national registry in the intermediate term wepropose that our approach will deliver the most current andscientifically sound US estimate of the number of personswith MS By addressing methodologic challenges and pro-posing a new paradigm for measuring the prevalence of MS inthe United States we hope that our work will benefit scientistswho study all chronic conditions for which national preva-lence estimates do not currently exist
AcknowledgmentThe authors thank the following members of the US MultipleSclerosis Prevalence Workgroup for their contributionsAlbert Lo Robert McBurney Oleg Muravov Bari Talenteand Leslie Ritter The authors also thank the following keystaff members at the National Multiple Sclerosis Society fortheir contributions to this project Cathy Carlson TimCoetzee Sherri Giger Weyman Johnson Eileen MadrayGraham McReynolds and Cyndi Zagieboylo
Study fundingThe study was funded by contracts from the National Mul-tiple Sclerosis Society to the principal investigators in the MSPrevalence Working Group (HC-1508-05693) The ArticleProcessing Charge was funded by the National MultipleSclerosis Society
DisclosureL Nelson receives grants from the Centers for DiseaseControl and Prevention NIH and National Multiple Scle-rosis Society and contracts from the Agency for Toxic Sub-stances and Diseases Registry She receives compensation forserving as a consultant to Acumen Inc and is on the DataMonitoring Committee of Neuropace M Wallin has servedon data safety monitoring boards for the National Institutes ofNeurological Disease and StrokendashNIH has been an associateeditor for the Encyclopedia of the Neurological Sciences andreceived funding support from the National Multiple Sclerosis
Society and the Department of Veterans Affairs Merit ReviewResearch Program R Marrie is supported by the WaughFamily Chair in Multiple Sclerosis receives research fundingfrom Canadian Institutes of Health Research ResearchManitoba Multiple Sclerosis Society of Canada MultipleSclerosis Scientific Foundation National Multiple SclerosisSociety and Rx amp D Health Research Foundation and hasconducted clinical trials funded by Sanofi-Aventis She alsoserves on the Editorial Board ofNeurologyregW Culpepper hasadditional research funding from the National MultipleSclerosis Society receives support from the VHA MS Centerof Excellence and is a member of the National MultipleSclerosis Society Health Care Delivery and Policy Researchstudy section A Langer-Gould is site principal investigatorfor 2 industry-sponsored phase 3 clinical trials (BiogenIdec Hoffman-LaRoche) and was site PI for one industry-sponsored observation study (Biogen Idec) She receivesgrant support from the NIH National Institute of Neuro-logical Disorders and Stroke Patient-Centered OutcomesResearch Institute and the National Multiple Sclerosis Soci-ety J Campbell has consultancy or research grants over thelast 5 years with Agency for Healthcare Research and QualityALSAM Foundation Amgen AstraZeneca Bayer BiogenIdec Boehringer Ingelheim Centers for Disease Control andPrevention Colorado Medicaid Enterprise CommunityPartners Inc Institute for Clinical and Economic ReviewMallinckrodt NIH National Multiple Sclerosis Society Kai-ser Permanente PhRMA Foundation Teva Research in RealLife Ltd Respiratory Effectiveness Group and Zogenix IncS Buka receives research funding from the NIH and theNational Multiple Sclerosis Society H Tremlett is theCanada Research Chair for Neuroepidemiology and MultipleSclerosis She receives research support from the NationalMultiple Sclerosis Society the Canadian Institutes of HealthResearch the Multiple Sclerosis Society of Canada and theMultiple Sclerosis Scientific Research Foundation In addi-tion in the last 5 years she has received research support fromthe Multiple Sclerosis Society of Canada the Michael SmithFoundation for Health Research and the UK MS Trust andspeaker honoraria andor travel expenses to attend confer-ences G Cutter is a member of Data and Safety MonitoringBoards for AMO Pharmaceuticals Apotek Horizon Phar-maceuticals ModigenetechProlor Merck MerckPfizerOpko Biologics Neurim Sanofi-Aventis Reata Pharmaceut-icals ReceptosCelgene Teva pharmaceuticals NHLBI(Protocol Review Committee) and NICHD (OPRU over-sight committee) and is on the Consulting or AdvisoryBoards for Atara Biotherapeutics Argenix Bioeq GmbHConsortium of MS Centers (grant) Genzyme GenentechInnate Therapeutics Klein-Buendel Incorporated Medi-mmune Medday Novartis Opexa Therapeutics RocheSavara Inc Somahlution Teva Pharmaceuticals Trans-parency Life Sciences and TGTherapeutics W Kaye receivesfunding from the Agency for Toxic Substances and DiseaseRegistry the National Multiple Sclerosis Society and theAssociation for the Accreditation of Human ResearchProtection Programs L Wagner receives funding from the
478 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Agency for Toxic Substances and Disease Registry and Na-tional Multiple Sclerosis Society N LaRocca is employed fulltime by the National Multiple Sclerosis Society and has noother disclosures to report Statistical analysis conducted byDr Gary Cutter PhD University of Alabama at BirminghamGo to NeurologyorgN for full disclosures
Publication historyReceived byNeurology July 17 2018 Accepted in final form October 222018
References1 Wallin MT Kurtzke JF Neuroepidemiology In Bradley WG Daroff RB Fenichel
GM Jankovic J editors Neurology in Clinical Practice Philadelphia Butterworth-Heinemann 2008762ndash780
2 Browne P Chandraratna D Angood C et al Atlas of multiple sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
3 Mayr WT Pittock SJ McClelland RL Jorgensen NW Noseworthy JH Rodriguez MIncidence and prevalence of multiple sclerosis in Olmsted County Minnesota 1985-2000 Neurology 2003611373ndash1377
4 Evans C Beland SG Kulaga S et al Incidence and prevalence of multiple sclerosis inthe Americas a systematic review Neuroepidemiology 201340195ndash210
5 Noonan CW Williamson DM Henry JP et al The prevalence of multiple sclerosis in3 US communities Prev Chronic Dis 20107A1
6 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
7 Baum HM Rothschild BB The incidence and prevalence of reported multiple scle-rosis Ann Neurol 198110420ndash428
8 Anderson DW Ellenberg JH Leventhal CM Reingold SC Rodriguez M SilberbergDH Revised estimate of the prevalence of multiple sclerosis in the United States AnnNeurol 199231333ndash336
9 Nelson LM Hamman RF Thompson DS et al Higher than expected prevalence ofmultiple sclerosis in Northern Colorado dependence on methodological issuesNeuroepidemiology 1986517ndash28
10 Collins JG Prevalence of selected chronic conditions United States 1990-1992 VitalHealth Stat 10 19971941ndash89
Appendix 1 Authors
Name Location Role Contribution
Lorene MNelsonMS PhD
Stanford UniversityCA
Author Study concept anddesign preparation ofdraft manuscriptrevision of themanuscript forcontent approval offinal manuscript
Mitchell TWallin MDMPH
Veterans HealthAdministrationGeorgetownUniversityWashington DC
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
Ruth AnnMarrieMD PhD
University ofManitoba WinnipegCanada
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
William JCulpepperPhD MA
Veterans HealthAdministrationWashington DCUniversity ofMaryland Baltimore
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
AnnetteLanger-GouldMD PhD
Kaiser PermanenteSouthern CaliforniaLos Angeles
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
JonathanCampbellPhD
University of DenverCO
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
StephenBuka PhD
Brown UniversityProvidence RI
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
HelenTremlettPhD
University of BritishColumbia VancouverCanada
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
GaryCutterPhD
University ofAlabamaBirmingham
Author Study concept anddesign critical reviewof the manuscript forcontent
Appendix 1 (continued)
Name Location Role Contribution
WendyKaye PhD
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
LaurieWagnerMPH
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Nicholas GLaRoccaPhD
National MultipleSclerosis Society NewYork NY
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Appendix 2 Coinvestigators and members of the USMultiple Sclerosis Prevalence Workgroup
Name Location Role Contribution
Albert LoMD PhD
Brown UniversityProvidence RI
Coinvestigator Studyconcept anddesign
RobertMcBurneyPhD
Accelerated CureProject Boston MA
Coinvestigator Studyconcept anddesign
OlegMuravovPhD
Agency for ToxicSubstances andDisease RegistryDivision of HealthStudies Atlanta GA
Coinvestigator Studyconcept anddesign
BariTalenteEsq
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
LeslieRitter
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 479
11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

databases (step 1) to obtain valid MS prevalence estimates(overall and specific with respect to age sex raceethnicityand geographic location)Step 4 CombineMSprevalence estimates into a single estimateof the prevalence of MS for the United States weightedaccording to the number of insured persons in each healthinsurance segment after obtaining MS prevalence estimatesseparately for each of the US health insurance segments theycan be combined into a single national prevalence estimateInformation from theCurrent Population Survey can be used toobtain the necessary weights by determining the number of USresidents with each type of insurance coverage stratified by sexage group race and geographic region The total estimatednumber of MS cases for each age sex race and geographicregionndashspecific category can then be summed to estimatethe total number ofMS cases in the United States For exampleMS prevalence for the private insurance segment can beestimated by accessing AHC data for Optum (Eden PrairieMN) and Truven Health (Ann Arbor MI) which in 2010together comprise approximately 68 million individuals or 35of the 2010 privately insured US population MS prevalence inthe government-insured segment of the population can bedirectly and completely estimated for 100 of people coveredby using administrative claims data for Medicaid and MedicareMS prevalence in the military population which is pre-dominantly male can be estimated used the Veterans HealthAdministration database A limitation of this method is that noclaims data exist for persons without health insurance estimatedat 163 in 201028 however for this uninsured group MSprevalence estimates from the Medicaid health care claims datacould be applied because the 2 groups have similar sociodemo-graphic characteristics
Our new approach cannot be applied to estimate the in-cidence of MS in the United States Incidencemdashthe number
of new MS cases per year in a populationmdashis an importantmeasure of disease frequency However it can only be derivedfor countries that have single uniform health care systemswhere longitudinal AHC records for each person enable rel-atively precise indicators of the onset of new MS diagnosisand the exclusion of existing prevalent cases The lack ofa single payer health care system or national tracking systemin the United States does not allow reliable estimates of MSincidence because some individuals may change health carecoverage over time and it is not possible to link patientrecords across insurance sources to provide a single longi-tudinal record within which newly diagnosed persons withMS may be ascertained This creates short periods of ob-servation which do not allow accurate estimates of incidencefor conditions such as MS and cancer due to the inability todefinitively determine which individuals are truly newlydiagnosed29
DiscussionWe have proposed a new approach for applying validatedcase-finding algorithms to AHC data from both governmentand private sources to produce robust estimates of MSprevalence in the United States In a companion article weapplied this approach to estimate the total number of MScases in the United States30 This approach could be appliedto estimate prevalence of other neurologic disorders andchronic conditions that face similar methodologic challengessuch as Parkinson disease dementia and epilepsy
There are several reasons why our new approach is a valuablemethodologic development to estimate the national MSprevalence First this paradigm offers the potential to useexisting AHC data for case ascertainment across the UnitedStates without requiring the cost and effort involved in re-gional MS prevalence studies which typically employ in-tensive case ascertainment methods The data are sufficientlydistributed both geographically and socioeconomically tobe representative of the entire US population and do notrequire consent because the databases are de-identifiedSecond our method is efficient and cost-effective and can beapplied repeatedly with datasets that represent a large pro-portion of the country enabling updates to population-based estimates of MS prevalence over time Third applyingthis approach with data that represent the entire UnitedStates allows us to obtain more stable and precise prevalenceestimates and to fill in knowledge gaps regarding the prev-alence of MS in many regions for which we have never hadestimates Once AHC data are able to accurately and com-pletely capture race and ethnicity this approach could beapplied to racial and ethnic minorities that have receivedlittle study in the past Fourth the use of a highly accuratecase-finding algorithm4 ensures that there will be greatercomparability between estimates derived from these sourcesin the future By adopting a standard paradigm for ascer-taining MS cases and applying validated case definition
Figure 1 Stepwise process for determining the prevalenceof multiple sclerosis (MS) in the United States
476 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
criteria we will be better able to monitor and comparespatial differences in MS prevalence and to examine changesin disease prevalence over time without the variation in-troduced by differing methodologic approaches
Despite many strengths our new approach is limited in thatthe case ascertainment methods do not cover all segments ofthe US population It excludes native American residents whochoose to receive care through the Indian Health Service
Figure 2 Source of health insurance by age (estimates from the current population survey 2008ndash2010)
(A) Population younger than 65 years (B) Population 65 years of age and older
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 477
(06 of the US population in 2010)31 and US residents whoare incarcerated (approximately 05 of the US population in2010)32 If health care databases existed for these populationswe could similarly apply an MS algorithm to estimate MSprevalence and incorporate them into the overall nationalestimate Our approach also cannot distinguish between dif-ferent racial and ethnic groups thus we cannot address towhat extent variations in prevalence by geography or otherfactors may be better explained by racialethnic differences inprevalence33
Our work has important implications for the new era of MSepidemiologic research that will be possible through the 21stCentury Cures Act legislation enacted in December 2016which authorized the establishment of a federally fundedneurologic disorders surveillance system34 A national registryfor MS could be implemented similar to the NationalAmyotrophic Lateral Sclerosis Registry with AHC data asa primary method for case ascertainment and a web portalavailable for all persons with MS to register242535 Withoutaccess to a national registry in the intermediate term wepropose that our approach will deliver the most current andscientifically sound US estimate of the number of personswith MS By addressing methodologic challenges and pro-posing a new paradigm for measuring the prevalence of MS inthe United States we hope that our work will benefit scientistswho study all chronic conditions for which national preva-lence estimates do not currently exist
AcknowledgmentThe authors thank the following members of the US MultipleSclerosis Prevalence Workgroup for their contributionsAlbert Lo Robert McBurney Oleg Muravov Bari Talenteand Leslie Ritter The authors also thank the following keystaff members at the National Multiple Sclerosis Society fortheir contributions to this project Cathy Carlson TimCoetzee Sherri Giger Weyman Johnson Eileen MadrayGraham McReynolds and Cyndi Zagieboylo
Study fundingThe study was funded by contracts from the National Mul-tiple Sclerosis Society to the principal investigators in the MSPrevalence Working Group (HC-1508-05693) The ArticleProcessing Charge was funded by the National MultipleSclerosis Society
DisclosureL Nelson receives grants from the Centers for DiseaseControl and Prevention NIH and National Multiple Scle-rosis Society and contracts from the Agency for Toxic Sub-stances and Diseases Registry She receives compensation forserving as a consultant to Acumen Inc and is on the DataMonitoring Committee of Neuropace M Wallin has servedon data safety monitoring boards for the National Institutes ofNeurological Disease and StrokendashNIH has been an associateeditor for the Encyclopedia of the Neurological Sciences andreceived funding support from the National Multiple Sclerosis
Society and the Department of Veterans Affairs Merit ReviewResearch Program R Marrie is supported by the WaughFamily Chair in Multiple Sclerosis receives research fundingfrom Canadian Institutes of Health Research ResearchManitoba Multiple Sclerosis Society of Canada MultipleSclerosis Scientific Foundation National Multiple SclerosisSociety and Rx amp D Health Research Foundation and hasconducted clinical trials funded by Sanofi-Aventis She alsoserves on the Editorial Board ofNeurologyregW Culpepper hasadditional research funding from the National MultipleSclerosis Society receives support from the VHA MS Centerof Excellence and is a member of the National MultipleSclerosis Society Health Care Delivery and Policy Researchstudy section A Langer-Gould is site principal investigatorfor 2 industry-sponsored phase 3 clinical trials (BiogenIdec Hoffman-LaRoche) and was site PI for one industry-sponsored observation study (Biogen Idec) She receivesgrant support from the NIH National Institute of Neuro-logical Disorders and Stroke Patient-Centered OutcomesResearch Institute and the National Multiple Sclerosis Soci-ety J Campbell has consultancy or research grants over thelast 5 years with Agency for Healthcare Research and QualityALSAM Foundation Amgen AstraZeneca Bayer BiogenIdec Boehringer Ingelheim Centers for Disease Control andPrevention Colorado Medicaid Enterprise CommunityPartners Inc Institute for Clinical and Economic ReviewMallinckrodt NIH National Multiple Sclerosis Society Kai-ser Permanente PhRMA Foundation Teva Research in RealLife Ltd Respiratory Effectiveness Group and Zogenix IncS Buka receives research funding from the NIH and theNational Multiple Sclerosis Society H Tremlett is theCanada Research Chair for Neuroepidemiology and MultipleSclerosis She receives research support from the NationalMultiple Sclerosis Society the Canadian Institutes of HealthResearch the Multiple Sclerosis Society of Canada and theMultiple Sclerosis Scientific Research Foundation In addi-tion in the last 5 years she has received research support fromthe Multiple Sclerosis Society of Canada the Michael SmithFoundation for Health Research and the UK MS Trust andspeaker honoraria andor travel expenses to attend confer-ences G Cutter is a member of Data and Safety MonitoringBoards for AMO Pharmaceuticals Apotek Horizon Phar-maceuticals ModigenetechProlor Merck MerckPfizerOpko Biologics Neurim Sanofi-Aventis Reata Pharmaceut-icals ReceptosCelgene Teva pharmaceuticals NHLBI(Protocol Review Committee) and NICHD (OPRU over-sight committee) and is on the Consulting or AdvisoryBoards for Atara Biotherapeutics Argenix Bioeq GmbHConsortium of MS Centers (grant) Genzyme GenentechInnate Therapeutics Klein-Buendel Incorporated Medi-mmune Medday Novartis Opexa Therapeutics RocheSavara Inc Somahlution Teva Pharmaceuticals Trans-parency Life Sciences and TGTherapeutics W Kaye receivesfunding from the Agency for Toxic Substances and DiseaseRegistry the National Multiple Sclerosis Society and theAssociation for the Accreditation of Human ResearchProtection Programs L Wagner receives funding from the
478 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Agency for Toxic Substances and Disease Registry and Na-tional Multiple Sclerosis Society N LaRocca is employed fulltime by the National Multiple Sclerosis Society and has noother disclosures to report Statistical analysis conducted byDr Gary Cutter PhD University of Alabama at BirminghamGo to NeurologyorgN for full disclosures
Publication historyReceived byNeurology July 17 2018 Accepted in final form October 222018
References1 Wallin MT Kurtzke JF Neuroepidemiology In Bradley WG Daroff RB Fenichel
GM Jankovic J editors Neurology in Clinical Practice Philadelphia Butterworth-Heinemann 2008762ndash780
2 Browne P Chandraratna D Angood C et al Atlas of multiple sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
3 Mayr WT Pittock SJ McClelland RL Jorgensen NW Noseworthy JH Rodriguez MIncidence and prevalence of multiple sclerosis in Olmsted County Minnesota 1985-2000 Neurology 2003611373ndash1377
4 Evans C Beland SG Kulaga S et al Incidence and prevalence of multiple sclerosis inthe Americas a systematic review Neuroepidemiology 201340195ndash210
5 Noonan CW Williamson DM Henry JP et al The prevalence of multiple sclerosis in3 US communities Prev Chronic Dis 20107A1
6 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
7 Baum HM Rothschild BB The incidence and prevalence of reported multiple scle-rosis Ann Neurol 198110420ndash428
8 Anderson DW Ellenberg JH Leventhal CM Reingold SC Rodriguez M SilberbergDH Revised estimate of the prevalence of multiple sclerosis in the United States AnnNeurol 199231333ndash336
9 Nelson LM Hamman RF Thompson DS et al Higher than expected prevalence ofmultiple sclerosis in Northern Colorado dependence on methodological issuesNeuroepidemiology 1986517ndash28
10 Collins JG Prevalence of selected chronic conditions United States 1990-1992 VitalHealth Stat 10 19971941ndash89
Appendix 1 Authors
Name Location Role Contribution
Lorene MNelsonMS PhD
Stanford UniversityCA
Author Study concept anddesign preparation ofdraft manuscriptrevision of themanuscript forcontent approval offinal manuscript
Mitchell TWallin MDMPH
Veterans HealthAdministrationGeorgetownUniversityWashington DC
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
Ruth AnnMarrieMD PhD
University ofManitoba WinnipegCanada
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
William JCulpepperPhD MA
Veterans HealthAdministrationWashington DCUniversity ofMaryland Baltimore
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
AnnetteLanger-GouldMD PhD
Kaiser PermanenteSouthern CaliforniaLos Angeles
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
JonathanCampbellPhD
University of DenverCO
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
StephenBuka PhD
Brown UniversityProvidence RI
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
HelenTremlettPhD
University of BritishColumbia VancouverCanada
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
GaryCutterPhD
University ofAlabamaBirmingham
Author Study concept anddesign critical reviewof the manuscript forcontent
Appendix 1 (continued)
Name Location Role Contribution
WendyKaye PhD
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
LaurieWagnerMPH
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Nicholas GLaRoccaPhD
National MultipleSclerosis Society NewYork NY
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Appendix 2 Coinvestigators and members of the USMultiple Sclerosis Prevalence Workgroup
Name Location Role Contribution
Albert LoMD PhD
Brown UniversityProvidence RI
Coinvestigator Studyconcept anddesign
RobertMcBurneyPhD
Accelerated CureProject Boston MA
Coinvestigator Studyconcept anddesign
OlegMuravovPhD
Agency for ToxicSubstances andDisease RegistryDivision of HealthStudies Atlanta GA
Coinvestigator Studyconcept anddesign
BariTalenteEsq
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
LeslieRitter
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 479
11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

criteria we will be better able to monitor and comparespatial differences in MS prevalence and to examine changesin disease prevalence over time without the variation in-troduced by differing methodologic approaches
Despite many strengths our new approach is limited in thatthe case ascertainment methods do not cover all segments ofthe US population It excludes native American residents whochoose to receive care through the Indian Health Service
Figure 2 Source of health insurance by age (estimates from the current population survey 2008ndash2010)
(A) Population younger than 65 years (B) Population 65 years of age and older
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 477
(06 of the US population in 2010)31 and US residents whoare incarcerated (approximately 05 of the US population in2010)32 If health care databases existed for these populationswe could similarly apply an MS algorithm to estimate MSprevalence and incorporate them into the overall nationalestimate Our approach also cannot distinguish between dif-ferent racial and ethnic groups thus we cannot address towhat extent variations in prevalence by geography or otherfactors may be better explained by racialethnic differences inprevalence33
Our work has important implications for the new era of MSepidemiologic research that will be possible through the 21stCentury Cures Act legislation enacted in December 2016which authorized the establishment of a federally fundedneurologic disorders surveillance system34 A national registryfor MS could be implemented similar to the NationalAmyotrophic Lateral Sclerosis Registry with AHC data asa primary method for case ascertainment and a web portalavailable for all persons with MS to register242535 Withoutaccess to a national registry in the intermediate term wepropose that our approach will deliver the most current andscientifically sound US estimate of the number of personswith MS By addressing methodologic challenges and pro-posing a new paradigm for measuring the prevalence of MS inthe United States we hope that our work will benefit scientistswho study all chronic conditions for which national preva-lence estimates do not currently exist
AcknowledgmentThe authors thank the following members of the US MultipleSclerosis Prevalence Workgroup for their contributionsAlbert Lo Robert McBurney Oleg Muravov Bari Talenteand Leslie Ritter The authors also thank the following keystaff members at the National Multiple Sclerosis Society fortheir contributions to this project Cathy Carlson TimCoetzee Sherri Giger Weyman Johnson Eileen MadrayGraham McReynolds and Cyndi Zagieboylo
Study fundingThe study was funded by contracts from the National Mul-tiple Sclerosis Society to the principal investigators in the MSPrevalence Working Group (HC-1508-05693) The ArticleProcessing Charge was funded by the National MultipleSclerosis Society
DisclosureL Nelson receives grants from the Centers for DiseaseControl and Prevention NIH and National Multiple Scle-rosis Society and contracts from the Agency for Toxic Sub-stances and Diseases Registry She receives compensation forserving as a consultant to Acumen Inc and is on the DataMonitoring Committee of Neuropace M Wallin has servedon data safety monitoring boards for the National Institutes ofNeurological Disease and StrokendashNIH has been an associateeditor for the Encyclopedia of the Neurological Sciences andreceived funding support from the National Multiple Sclerosis
Society and the Department of Veterans Affairs Merit ReviewResearch Program R Marrie is supported by the WaughFamily Chair in Multiple Sclerosis receives research fundingfrom Canadian Institutes of Health Research ResearchManitoba Multiple Sclerosis Society of Canada MultipleSclerosis Scientific Foundation National Multiple SclerosisSociety and Rx amp D Health Research Foundation and hasconducted clinical trials funded by Sanofi-Aventis She alsoserves on the Editorial Board ofNeurologyregW Culpepper hasadditional research funding from the National MultipleSclerosis Society receives support from the VHA MS Centerof Excellence and is a member of the National MultipleSclerosis Society Health Care Delivery and Policy Researchstudy section A Langer-Gould is site principal investigatorfor 2 industry-sponsored phase 3 clinical trials (BiogenIdec Hoffman-LaRoche) and was site PI for one industry-sponsored observation study (Biogen Idec) She receivesgrant support from the NIH National Institute of Neuro-logical Disorders and Stroke Patient-Centered OutcomesResearch Institute and the National Multiple Sclerosis Soci-ety J Campbell has consultancy or research grants over thelast 5 years with Agency for Healthcare Research and QualityALSAM Foundation Amgen AstraZeneca Bayer BiogenIdec Boehringer Ingelheim Centers for Disease Control andPrevention Colorado Medicaid Enterprise CommunityPartners Inc Institute for Clinical and Economic ReviewMallinckrodt NIH National Multiple Sclerosis Society Kai-ser Permanente PhRMA Foundation Teva Research in RealLife Ltd Respiratory Effectiveness Group and Zogenix IncS Buka receives research funding from the NIH and theNational Multiple Sclerosis Society H Tremlett is theCanada Research Chair for Neuroepidemiology and MultipleSclerosis She receives research support from the NationalMultiple Sclerosis Society the Canadian Institutes of HealthResearch the Multiple Sclerosis Society of Canada and theMultiple Sclerosis Scientific Research Foundation In addi-tion in the last 5 years she has received research support fromthe Multiple Sclerosis Society of Canada the Michael SmithFoundation for Health Research and the UK MS Trust andspeaker honoraria andor travel expenses to attend confer-ences G Cutter is a member of Data and Safety MonitoringBoards for AMO Pharmaceuticals Apotek Horizon Phar-maceuticals ModigenetechProlor Merck MerckPfizerOpko Biologics Neurim Sanofi-Aventis Reata Pharmaceut-icals ReceptosCelgene Teva pharmaceuticals NHLBI(Protocol Review Committee) and NICHD (OPRU over-sight committee) and is on the Consulting or AdvisoryBoards for Atara Biotherapeutics Argenix Bioeq GmbHConsortium of MS Centers (grant) Genzyme GenentechInnate Therapeutics Klein-Buendel Incorporated Medi-mmune Medday Novartis Opexa Therapeutics RocheSavara Inc Somahlution Teva Pharmaceuticals Trans-parency Life Sciences and TGTherapeutics W Kaye receivesfunding from the Agency for Toxic Substances and DiseaseRegistry the National Multiple Sclerosis Society and theAssociation for the Accreditation of Human ResearchProtection Programs L Wagner receives funding from the
478 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Agency for Toxic Substances and Disease Registry and Na-tional Multiple Sclerosis Society N LaRocca is employed fulltime by the National Multiple Sclerosis Society and has noother disclosures to report Statistical analysis conducted byDr Gary Cutter PhD University of Alabama at BirminghamGo to NeurologyorgN for full disclosures
Publication historyReceived byNeurology July 17 2018 Accepted in final form October 222018
References1 Wallin MT Kurtzke JF Neuroepidemiology In Bradley WG Daroff RB Fenichel
GM Jankovic J editors Neurology in Clinical Practice Philadelphia Butterworth-Heinemann 2008762ndash780
2 Browne P Chandraratna D Angood C et al Atlas of multiple sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
3 Mayr WT Pittock SJ McClelland RL Jorgensen NW Noseworthy JH Rodriguez MIncidence and prevalence of multiple sclerosis in Olmsted County Minnesota 1985-2000 Neurology 2003611373ndash1377
4 Evans C Beland SG Kulaga S et al Incidence and prevalence of multiple sclerosis inthe Americas a systematic review Neuroepidemiology 201340195ndash210
5 Noonan CW Williamson DM Henry JP et al The prevalence of multiple sclerosis in3 US communities Prev Chronic Dis 20107A1
6 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
7 Baum HM Rothschild BB The incidence and prevalence of reported multiple scle-rosis Ann Neurol 198110420ndash428
8 Anderson DW Ellenberg JH Leventhal CM Reingold SC Rodriguez M SilberbergDH Revised estimate of the prevalence of multiple sclerosis in the United States AnnNeurol 199231333ndash336
9 Nelson LM Hamman RF Thompson DS et al Higher than expected prevalence ofmultiple sclerosis in Northern Colorado dependence on methodological issuesNeuroepidemiology 1986517ndash28
10 Collins JG Prevalence of selected chronic conditions United States 1990-1992 VitalHealth Stat 10 19971941ndash89
Appendix 1 Authors
Name Location Role Contribution
Lorene MNelsonMS PhD
Stanford UniversityCA
Author Study concept anddesign preparation ofdraft manuscriptrevision of themanuscript forcontent approval offinal manuscript
Mitchell TWallin MDMPH
Veterans HealthAdministrationGeorgetownUniversityWashington DC
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
Ruth AnnMarrieMD PhD
University ofManitoba WinnipegCanada
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
William JCulpepperPhD MA
Veterans HealthAdministrationWashington DCUniversity ofMaryland Baltimore
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
AnnetteLanger-GouldMD PhD
Kaiser PermanenteSouthern CaliforniaLos Angeles
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
JonathanCampbellPhD
University of DenverCO
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
StephenBuka PhD
Brown UniversityProvidence RI
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
HelenTremlettPhD
University of BritishColumbia VancouverCanada
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
GaryCutterPhD
University ofAlabamaBirmingham
Author Study concept anddesign critical reviewof the manuscript forcontent
Appendix 1 (continued)
Name Location Role Contribution
WendyKaye PhD
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
LaurieWagnerMPH
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Nicholas GLaRoccaPhD
National MultipleSclerosis Society NewYork NY
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Appendix 2 Coinvestigators and members of the USMultiple Sclerosis Prevalence Workgroup
Name Location Role Contribution
Albert LoMD PhD
Brown UniversityProvidence RI
Coinvestigator Studyconcept anddesign
RobertMcBurneyPhD
Accelerated CureProject Boston MA
Coinvestigator Studyconcept anddesign
OlegMuravovPhD
Agency for ToxicSubstances andDisease RegistryDivision of HealthStudies Atlanta GA
Coinvestigator Studyconcept anddesign
BariTalenteEsq
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
LeslieRitter
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 479
11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

(06 of the US population in 2010)31 and US residents whoare incarcerated (approximately 05 of the US population in2010)32 If health care databases existed for these populationswe could similarly apply an MS algorithm to estimate MSprevalence and incorporate them into the overall nationalestimate Our approach also cannot distinguish between dif-ferent racial and ethnic groups thus we cannot address towhat extent variations in prevalence by geography or otherfactors may be better explained by racialethnic differences inprevalence33
Our work has important implications for the new era of MSepidemiologic research that will be possible through the 21stCentury Cures Act legislation enacted in December 2016which authorized the establishment of a federally fundedneurologic disorders surveillance system34 A national registryfor MS could be implemented similar to the NationalAmyotrophic Lateral Sclerosis Registry with AHC data asa primary method for case ascertainment and a web portalavailable for all persons with MS to register242535 Withoutaccess to a national registry in the intermediate term wepropose that our approach will deliver the most current andscientifically sound US estimate of the number of personswith MS By addressing methodologic challenges and pro-posing a new paradigm for measuring the prevalence of MS inthe United States we hope that our work will benefit scientistswho study all chronic conditions for which national preva-lence estimates do not currently exist
AcknowledgmentThe authors thank the following members of the US MultipleSclerosis Prevalence Workgroup for their contributionsAlbert Lo Robert McBurney Oleg Muravov Bari Talenteand Leslie Ritter The authors also thank the following keystaff members at the National Multiple Sclerosis Society fortheir contributions to this project Cathy Carlson TimCoetzee Sherri Giger Weyman Johnson Eileen MadrayGraham McReynolds and Cyndi Zagieboylo
Study fundingThe study was funded by contracts from the National Mul-tiple Sclerosis Society to the principal investigators in the MSPrevalence Working Group (HC-1508-05693) The ArticleProcessing Charge was funded by the National MultipleSclerosis Society
DisclosureL Nelson receives grants from the Centers for DiseaseControl and Prevention NIH and National Multiple Scle-rosis Society and contracts from the Agency for Toxic Sub-stances and Diseases Registry She receives compensation forserving as a consultant to Acumen Inc and is on the DataMonitoring Committee of Neuropace M Wallin has servedon data safety monitoring boards for the National Institutes ofNeurological Disease and StrokendashNIH has been an associateeditor for the Encyclopedia of the Neurological Sciences andreceived funding support from the National Multiple Sclerosis
Society and the Department of Veterans Affairs Merit ReviewResearch Program R Marrie is supported by the WaughFamily Chair in Multiple Sclerosis receives research fundingfrom Canadian Institutes of Health Research ResearchManitoba Multiple Sclerosis Society of Canada MultipleSclerosis Scientific Foundation National Multiple SclerosisSociety and Rx amp D Health Research Foundation and hasconducted clinical trials funded by Sanofi-Aventis She alsoserves on the Editorial Board ofNeurologyregW Culpepper hasadditional research funding from the National MultipleSclerosis Society receives support from the VHA MS Centerof Excellence and is a member of the National MultipleSclerosis Society Health Care Delivery and Policy Researchstudy section A Langer-Gould is site principal investigatorfor 2 industry-sponsored phase 3 clinical trials (BiogenIdec Hoffman-LaRoche) and was site PI for one industry-sponsored observation study (Biogen Idec) She receivesgrant support from the NIH National Institute of Neuro-logical Disorders and Stroke Patient-Centered OutcomesResearch Institute and the National Multiple Sclerosis Soci-ety J Campbell has consultancy or research grants over thelast 5 years with Agency for Healthcare Research and QualityALSAM Foundation Amgen AstraZeneca Bayer BiogenIdec Boehringer Ingelheim Centers for Disease Control andPrevention Colorado Medicaid Enterprise CommunityPartners Inc Institute for Clinical and Economic ReviewMallinckrodt NIH National Multiple Sclerosis Society Kai-ser Permanente PhRMA Foundation Teva Research in RealLife Ltd Respiratory Effectiveness Group and Zogenix IncS Buka receives research funding from the NIH and theNational Multiple Sclerosis Society H Tremlett is theCanada Research Chair for Neuroepidemiology and MultipleSclerosis She receives research support from the NationalMultiple Sclerosis Society the Canadian Institutes of HealthResearch the Multiple Sclerosis Society of Canada and theMultiple Sclerosis Scientific Research Foundation In addi-tion in the last 5 years she has received research support fromthe Multiple Sclerosis Society of Canada the Michael SmithFoundation for Health Research and the UK MS Trust andspeaker honoraria andor travel expenses to attend confer-ences G Cutter is a member of Data and Safety MonitoringBoards for AMO Pharmaceuticals Apotek Horizon Phar-maceuticals ModigenetechProlor Merck MerckPfizerOpko Biologics Neurim Sanofi-Aventis Reata Pharmaceut-icals ReceptosCelgene Teva pharmaceuticals NHLBI(Protocol Review Committee) and NICHD (OPRU over-sight committee) and is on the Consulting or AdvisoryBoards for Atara Biotherapeutics Argenix Bioeq GmbHConsortium of MS Centers (grant) Genzyme GenentechInnate Therapeutics Klein-Buendel Incorporated Medi-mmune Medday Novartis Opexa Therapeutics RocheSavara Inc Somahlution Teva Pharmaceuticals Trans-parency Life Sciences and TGTherapeutics W Kaye receivesfunding from the Agency for Toxic Substances and DiseaseRegistry the National Multiple Sclerosis Society and theAssociation for the Accreditation of Human ResearchProtection Programs L Wagner receives funding from the
478 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
Agency for Toxic Substances and Disease Registry and Na-tional Multiple Sclerosis Society N LaRocca is employed fulltime by the National Multiple Sclerosis Society and has noother disclosures to report Statistical analysis conducted byDr Gary Cutter PhD University of Alabama at BirminghamGo to NeurologyorgN for full disclosures
Publication historyReceived byNeurology July 17 2018 Accepted in final form October 222018
References1 Wallin MT Kurtzke JF Neuroepidemiology In Bradley WG Daroff RB Fenichel
GM Jankovic J editors Neurology in Clinical Practice Philadelphia Butterworth-Heinemann 2008762ndash780
2 Browne P Chandraratna D Angood C et al Atlas of multiple sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
3 Mayr WT Pittock SJ McClelland RL Jorgensen NW Noseworthy JH Rodriguez MIncidence and prevalence of multiple sclerosis in Olmsted County Minnesota 1985-2000 Neurology 2003611373ndash1377
4 Evans C Beland SG Kulaga S et al Incidence and prevalence of multiple sclerosis inthe Americas a systematic review Neuroepidemiology 201340195ndash210
5 Noonan CW Williamson DM Henry JP et al The prevalence of multiple sclerosis in3 US communities Prev Chronic Dis 20107A1
6 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
7 Baum HM Rothschild BB The incidence and prevalence of reported multiple scle-rosis Ann Neurol 198110420ndash428
8 Anderson DW Ellenberg JH Leventhal CM Reingold SC Rodriguez M SilberbergDH Revised estimate of the prevalence of multiple sclerosis in the United States AnnNeurol 199231333ndash336
9 Nelson LM Hamman RF Thompson DS et al Higher than expected prevalence ofmultiple sclerosis in Northern Colorado dependence on methodological issuesNeuroepidemiology 1986517ndash28
10 Collins JG Prevalence of selected chronic conditions United States 1990-1992 VitalHealth Stat 10 19971941ndash89
Appendix 1 Authors
Name Location Role Contribution
Lorene MNelsonMS PhD
Stanford UniversityCA
Author Study concept anddesign preparation ofdraft manuscriptrevision of themanuscript forcontent approval offinal manuscript
Mitchell TWallin MDMPH
Veterans HealthAdministrationGeorgetownUniversityWashington DC
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
Ruth AnnMarrieMD PhD
University ofManitoba WinnipegCanada
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
William JCulpepperPhD MA
Veterans HealthAdministrationWashington DCUniversity ofMaryland Baltimore
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
AnnetteLanger-GouldMD PhD
Kaiser PermanenteSouthern CaliforniaLos Angeles
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
JonathanCampbellPhD
University of DenverCO
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
StephenBuka PhD
Brown UniversityProvidence RI
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
HelenTremlettPhD
University of BritishColumbia VancouverCanada
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
GaryCutterPhD
University ofAlabamaBirmingham
Author Study concept anddesign critical reviewof the manuscript forcontent
Appendix 1 (continued)
Name Location Role Contribution
WendyKaye PhD
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
LaurieWagnerMPH
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Nicholas GLaRoccaPhD
National MultipleSclerosis Society NewYork NY
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Appendix 2 Coinvestigators and members of the USMultiple Sclerosis Prevalence Workgroup
Name Location Role Contribution
Albert LoMD PhD
Brown UniversityProvidence RI
Coinvestigator Studyconcept anddesign
RobertMcBurneyPhD
Accelerated CureProject Boston MA
Coinvestigator Studyconcept anddesign
OlegMuravovPhD
Agency for ToxicSubstances andDisease RegistryDivision of HealthStudies Atlanta GA
Coinvestigator Studyconcept anddesign
BariTalenteEsq
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
LeslieRitter
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 479
11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Agency for Toxic Substances and Disease Registry and Na-tional Multiple Sclerosis Society N LaRocca is employed fulltime by the National Multiple Sclerosis Society and has noother disclosures to report Statistical analysis conducted byDr Gary Cutter PhD University of Alabama at BirminghamGo to NeurologyorgN for full disclosures
Publication historyReceived byNeurology July 17 2018 Accepted in final form October 222018
References1 Wallin MT Kurtzke JF Neuroepidemiology In Bradley WG Daroff RB Fenichel
GM Jankovic J editors Neurology in Clinical Practice Philadelphia Butterworth-Heinemann 2008762ndash780
2 Browne P Chandraratna D Angood C et al Atlas of multiple sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
3 Mayr WT Pittock SJ McClelland RL Jorgensen NW Noseworthy JH Rodriguez MIncidence and prevalence of multiple sclerosis in Olmsted County Minnesota 1985-2000 Neurology 2003611373ndash1377
4 Evans C Beland SG Kulaga S et al Incidence and prevalence of multiple sclerosis inthe Americas a systematic review Neuroepidemiology 201340195ndash210
5 Noonan CW Williamson DM Henry JP et al The prevalence of multiple sclerosis in3 US communities Prev Chronic Dis 20107A1
6 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
7 Baum HM Rothschild BB The incidence and prevalence of reported multiple scle-rosis Ann Neurol 198110420ndash428
8 Anderson DW Ellenberg JH Leventhal CM Reingold SC Rodriguez M SilberbergDH Revised estimate of the prevalence of multiple sclerosis in the United States AnnNeurol 199231333ndash336
9 Nelson LM Hamman RF Thompson DS et al Higher than expected prevalence ofmultiple sclerosis in Northern Colorado dependence on methodological issuesNeuroepidemiology 1986517ndash28
10 Collins JG Prevalence of selected chronic conditions United States 1990-1992 VitalHealth Stat 10 19971941ndash89
Appendix 1 Authors
Name Location Role Contribution
Lorene MNelsonMS PhD
Stanford UniversityCA
Author Study concept anddesign preparation ofdraft manuscriptrevision of themanuscript forcontent approval offinal manuscript
Mitchell TWallin MDMPH
Veterans HealthAdministrationGeorgetownUniversityWashington DC
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
Ruth AnnMarrieMD PhD
University ofManitoba WinnipegCanada
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
William JCulpepperPhD MA
Veterans HealthAdministrationWashington DCUniversity ofMaryland Baltimore
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
AnnetteLanger-GouldMD PhD
Kaiser PermanenteSouthern CaliforniaLos Angeles
Author Study concept anddesign critical reviewrevision of themanuscript forcontent approval offinal manuscript
JonathanCampbellPhD
University of DenverCO
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
StephenBuka PhD
Brown UniversityProvidence RI
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
HelenTremlettPhD
University of BritishColumbia VancouverCanada
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
GaryCutterPhD
University ofAlabamaBirmingham
Author Study concept anddesign critical reviewof the manuscript forcontent
Appendix 1 (continued)
Name Location Role Contribution
WendyKaye PhD
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
LaurieWagnerMPH
McKing ConsultingCorp Atlanta GA
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Nicholas GLaRoccaPhD
National MultipleSclerosis Society NewYork NY
Author Study concept anddesign critical reviewof the manuscript forcontent approval offinal manuscript
Appendix 2 Coinvestigators and members of the USMultiple Sclerosis Prevalence Workgroup
Name Location Role Contribution
Albert LoMD PhD
Brown UniversityProvidence RI
Coinvestigator Studyconcept anddesign
RobertMcBurneyPhD
Accelerated CureProject Boston MA
Coinvestigator Studyconcept anddesign
OlegMuravovPhD
Agency for ToxicSubstances andDisease RegistryDivision of HealthStudies Atlanta GA
Coinvestigator Studyconcept anddesign
BariTalenteEsq
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
LeslieRitter
National MultipleSclerosis SocietyWashington DC
Coinvestigator Studyconcept anddesign
NeurologyorgN Neurology | Volume 92 Number 10 | March 5 2019 479
11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

11 Noonan CW Kathman SJ White MC Prevalence estimates for MS in the US andevidence of an increasing trend in women Neurology 200258136ndash138
12 Campbell JD Ghushchyan V Brett McQueen R et al Burden of multiple sclerosis ondirect indirect costs and quality of life national US estimates Mult Scler Relat Disord20143227ndash236
13 Buchanan RJ Radin D Huang C Zhu L Caregiver perceptions associated with risk ofnursing home admission for people with multiple sclerosis Disabil Health J 20103117ndash124
14 Northrop DE Frankel D editors Nursing Home Care of Individuals with MultipleSclerosis Guidelines and Recommendations for Quality Care Monograph NewYork National Multiple Sclerosis Society Professional Resource Center Available atnationalmssocietyorgNationalMSSocietymediaMSNationalFilesBrochuresBrochure-Nursing-Home-Care-of-Individuals-with-MSpdf Accessed July 1 2018
15 Pope GC Urato CJ Kulas ED Kronick R Gilmer T Prevalence expendituresutilization and payment for persons with MS in insured populations Neurology20025837ndash43
16 Dilokthornsakul P Valuck RJ Nair KV Corboy JR Allen RR Campbell JD Multiplesclerosis prevalence in the United States commercially insured population Neurology2016861014ndash1021
17 Koch-Henriksen N Magyari M Laursen B Registers of multiple sclerosis in Den-mark Acta Neurol Scand 20151324ndash10
18 Koch-Henriksen N Sorensen PS The changing demographic pattern of multiplesclerosis epidemiology Lancet Neurol 20109520ndash532
19 Hillert J Stawiarz L The Swedish MS registry clinical support tool and scientificresource Acta Neurol Scand 201513211ndash19
20 Myhr KM Grytten N Aarseth JH Nyland H The Norwegian multiple sclerosisNational Competence Centre and National Multiple Sclerosis Registry a resource forclinical practice and research Acta Neurol Scand Suppl 200618337ndash40
21 Brola W Sobolewski P Fudala M et al Self-reported quality of life in multiplesclerosis patients preliminary results based on the Polish MS Registry Patient PreferAdherence 2016101647ndash1656
22 Rooney JPK Brayne C Tobin K Logroscino G Glymour MM Hardiman O Ben-efits pitfalls and future design of population-based registers in neurodegenerativedisease Neurology 2017882321ndash2329
23 National Cancer Institute (NCI) National Institutes of Health US Department ofHealth and Human Services Surveillance Epidemiology and End Results (SEER)Program Available at seercancergovregistries Accessed July 1 2018
24 Mehta P Kaye W Bryan L et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2012-2013 MMWR Surveill Summ 2016651ndash12
25 Mehta P Antao V Kaye W et al Prevalence of amyotrophic lateral sclerosis UnitedStates 2010-2011 MMWR Suppl 2014631ndash14
26 StGermaine-SmithCMetcalfe A PringsheimT et al Recommendations for optimal ICDcodes to study neurologic conditions a systematic reviewNeurology 2012791049ndash1055
27 Culpepper JW Marrie RA Langer-Gould A et al Validation of an algorithm for iden-tifyingMS cases across administrative health claims datasets Neurology (in press 2019)
28 US Census Bureau Income Poverty and Health Insurance Coverage in the UnitedStates 2010 Washington DC US Department of Commerce Economics and Sta-tistics Administration 2011
29 Griffiths RI OrsquoMalley CD Herbert RJ Danese MD Misclassification of incidentconditions using claims data impact of varying the period used to exclude pre-existingdisease BMC Med Res Methodol 20131332
30 WallinMT Culpepper JW Campbell J et al The prevalence ofMS in the United Statesa population-based estimate using health claims data Neurology (in press 2019)
31 US Department of Health and Human Services Indian Health Service Trends inIndian Health 2014 edition Office of Public Health Support Division of ProgramStatistics Available at ihsgovdpsincludesthemesnewihsthemedisplay_objectsdocumentsTrends2014Book508pdf Accessed July 1 2018
32 US Department of Justice Bureau of Justice Statistics Prisoners in 2010 2011Available at bjsgovcontentpubpdfp10pdf Accessed July 1 2018
33 Langer-Gould A Brara SM Beaber BE Zhang JL Incidence of multiple sclerosis inmultiple racial and ethnic groups Neurology 2013801734ndash1739
34 21st Century Cures Act Enacted by the 114th United States Congress in December2016 An Act to Accelerate the Discovery Development and Delivery of 21st CenturyCures and for Other Purposes Public Law 114ndash255 Available at congressgovbill114th-congresshouse-bill6 Accessed July 1 2018
35 Horton DK Mehta P Antao VC Quantifying a nonnotifiable disease in the UnitedStates the National Amyotrophic Lateral Sclerosis Registry model JAMA 20143121097ndash1098
New AAN Practice Management Webinar Format Digs Deeper
The new format offers a live 30- to 45-minute webinar with expert faculty followed by several shorter recorded online lecturesthat explore the topic in greater depth Each topic concludes with a 30-minute live webchat for further participant QampAPurchase a single webinar series for $99 or purchase a 2019 Practice Management Webinar subscription for only $189mdashthatrsquosless than $32 per webinar
2019 Webinar Series
bull January 15 ndash Boss MD Managing a Better Practicebull March 12 ndash Understanding How You Get Paidbull May 21 ndash Everything You Wanted to Know About Your Patients but Were Afraid to Ask HavingDifficult Conversations with Patients from Vulnerable Populations
bull August 13 ndash Increasing Revenue in Your Practice Care Models Ancillary Services and Other Strategiesbull October 1 ndash Using Technology for Better Practice Management of Strokebull November 19 ndash Seeing the Future Clearly How to Succeed in 2020
Learn more and register at AANcomviewwebinar
480 Neurology | Volume 92 Number 10 | March 5 2019 NeurologyorgN
DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

DOI 101212WNL0000000000007044201992469-480 Published Online before print February 15 2019Neurology
Lorene M Nelson Mitchell T Wallin Ruth Ann Marrie et al with MS
A new way to estimate neurologic disease prevalence in the United States Illustrated
This information is current as of February 15 2019
ServicesUpdated Information amp
httpnneurologyorgcontent9210469fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9210469fullref-list-1
This article cites 26 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9210469fullotherarticles
This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionprevalence_studiesPrevalence studies
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectionall_health_services_researchAll Health Services Research
httpnneurologyorgcgicollectionall_epidemiologyAll epidemiologyfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology