Embed Size (px)
Citation preview

A Novel Approach to
AAC: Maximizing
Language Recovery for
People with Aphasia
Aimee Dietz, PhD, CCC-SLP
Associate Professor
Director of MA SLP Program
Director: Language Recovery Lab
Twitter: @Aimee.Dietz
13th Annual Northern Kentucky
Brain Injury Conference
Erlanger, KY
March 29, 2019

• American Speech-Language & Hearing Association-Sponsored this Talk
• NIH-NCRR 8KL2TR000078-05 & NIH-NCRR 8ULTR000077-05
• NIH-NIDCD: 1R15DC017280-01
• Collaborators
– Dr. Jennifer Vannest, Phd – Cincinnati Children’s Hospital Medical Center
– Dr. Jerzy Szaflarski, MD, PhD – University of Alabama at Birmingham
– Dr. Krista Wilkinson, PhD— Pennsylvania State University
– Dr. Weihong Yuan, PhD- Cincinnati Children’s Hospital Medical Center
• Research Assistants
– Jacqueline “Alyse” Watt, MS, CCC-SLLP– University of Cincinnati
– Thomas Maloney, MS - Cincinnati Children’s Hospital Medical Center
– Michelle Kryc, BS
– Mariah Emery
– Cassandra “Cassy” Stall
• Statistical Support
– Mekibib Altaye, PhD - Cincinnati Children’s Hospital and
Medical Center
Acknowledgements &
Disclosure Statement

Learner Outcomes Attendees will be able to:
• describe and differentiate what it means to support communication and to facilitate language recovery.
• describe how to apply principles of plasticity and intersystemic reorganization to promote language recovery in people with post-stroke aphasia.
• list the pros and cons of three common interface designs in terms of using augmentative and alternative communication for people with aphasia.
• identify at least 2 strategies to support the comprehension and expression of people with aphasia


What is Augmentative &
Alternative Communication? (ASHA, 2018)
• Augmentative and alternative communication (AAC) is an area of clinical
practice that addresses the needs of individuals with significant and complex
communication disorders characterized by impairments in speech-language
production and/or comprehension, including spoken and written modes of
communication.
• AAC uses a variety of techniques and tools, including picture communication
boards, line drawings, speech-generating devices (SGDs), tangible objects,
manual signs, gestures, and finger spelling, to help the individual express
thoughts, wants and needs, feelings, and ideas.
• AAC is augmentative when used to supplement existing speech,
and alternative when used in place of speech that is absent or not functional.
• AAC may be temporary, as when used by patients postoperatively in intensive
care, or permanent, as when used by an individual who will require the use of
some form of AAC throughout his or her lifetime.

Augmentative & Alternative
Communication (AAC): Challenges
for People with Aphasia
Example of AAC for People without Aphasia
• What are the pitfalls to this type of interface design for people with aphasia?
• What can we do to exploit the strengths of people with aphasia? – What are those strengths?

Muscle weakness, flaccidity, nor is it ataxic, spastic, hyper- or hypokinetic movement
dysarthria
Motor planning
apraxia
Cognitive Impairment
dementia
traumatic
brain injury (TBI)
Aphasia is NOT:

Aphasia Defined • An acquired language disorder
• Common causes include damage to LEFT
hemisphere:
– stroke, brain injury, tumor, degenerative diseases
Right Left Right Left
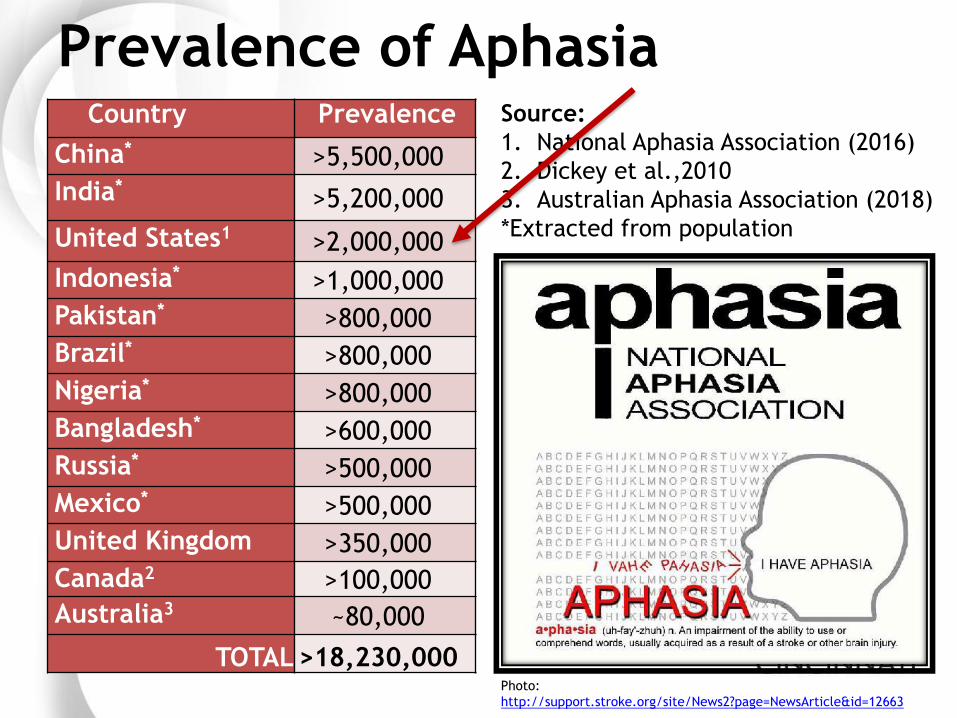
Prevalence of Aphasia Country Prevalence
China* >5,500,000
India* >5,200,000
United States1 >2,000,000
Indonesia* >1,000,000
Pakistan* >800,000
Brazil* >800,000
Nigeria* >800,000
Bangladesh* >600,000
Russia* >500,000
Mexico* >500,000
United Kingdom >350,000
Canada2 >100,000
Australia3 ~80,000
TOTAL >18,230,000
Source:
1. National Aphasia Association (2016)
2. Dickey et al.,2010
3. Australian Aphasia Association (2018)
*Extracted from population
Photo:
http://support.stroke.org/site/News2?page=NewsArticle&id=12663

Aphasia: Reality
• When you listen or read:
– unable to fully understand
all that is going on around
you
• When you speak or write
– Can only say/write a few
key words
– Jargon comes out Photo: https://www.writingforward.com/writing-
tips/read-and-write
Photo: https://abilitytools.org/blog/assistive-
technology-for-living-with-aphasia/
EXAMPLE: Fluent Aphasia
EXAMPLE: Nonfluent Aphasia

“…When I awoke and struggled to find words, I thought
for sure I had lost my tongue, but it was far worse than
that, as I was to find out… My tongue was fine but I
couldn’t come up with the right words or put them in the
right order. And then, when I tried to write or read, I had
the same trouble. And it sounded like everyone was
speaking a language I did not know. Talk about
terrifying!” –Betty LaPointe, L. L. (2005). Foundations: Adaptation, Accommodation, Aristos. In L. L. LaPointe, Aphasia and related neurogenic
language disorders (pp. 1-18). New York, NY, US: Thieme New York.
Perspective…
Photo:
https://sites.google.com/site/aphasiacdh/h
ome/what-area-of-the-brain-is-affected-by-
aphasia
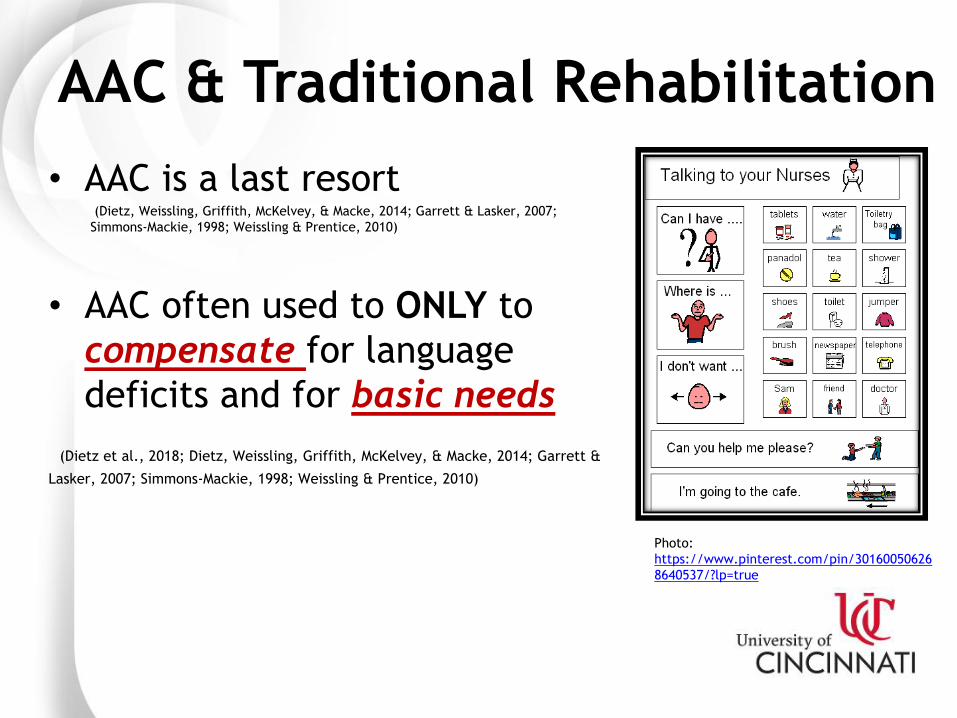
AAC & Traditional Rehabilitation
• AAC is a last resort (Dietz, Weissling, Griffith, McKelvey, & Macke, 2014; Garrett & Lasker, 2007;
Simmons-Mackie, 1998; Weissling & Prentice, 2010)
• AAC often used to ONLY to
compensate for language
deficits and for basic needs
(Dietz et al., 2018; Dietz, Weissling, Griffith, McKelvey, & Macke, 2014; Garrett &
Lasker, 2007; Simmons-Mackie, 1998; Weissling & Prentice, 2010)
Photo:
https://www.pinterest.com/pin/30160050626
8640537/?lp=true

Figure used with permission from Julie Griffith, PhD
Source: Griffith, J.D. (2014) Post-stroke Language Remediation through Constraint-induced Aphasia
Therapy. University of Cincinnati, Cincinnati, Ohio.
AAC is avoided due to fear of
“learned non-use”…
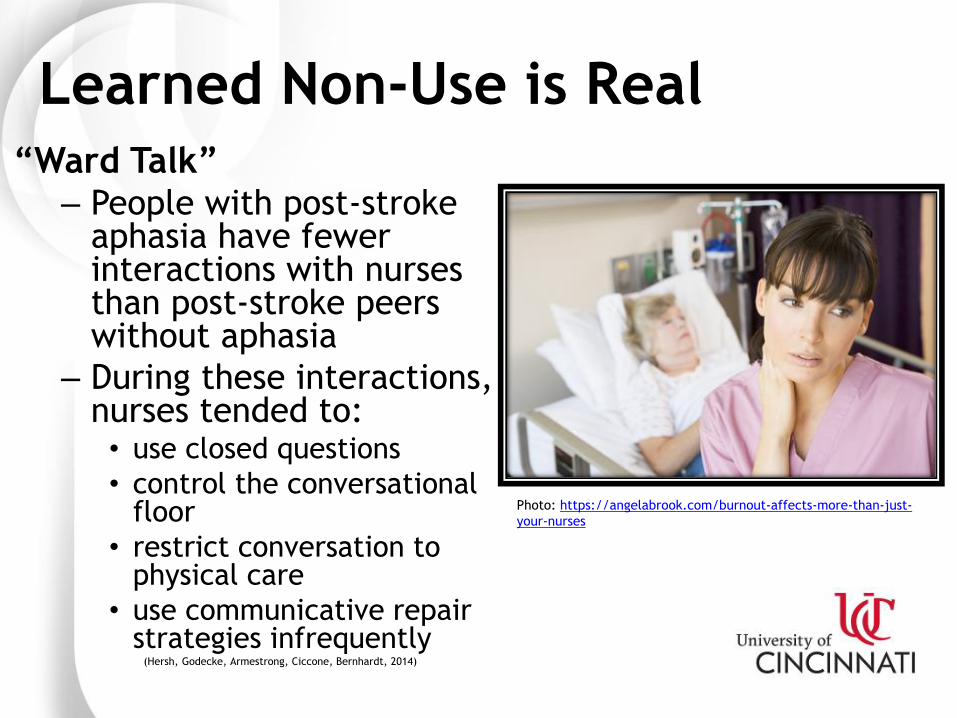
Learned Non-Use is Real “Ward Talk”
– People with post-stroke aphasia have fewer interactions with nurses than post-stroke peers without aphasia
– During these interactions, nurses tended to: • use closed questions
• control the conversational floor
• restrict conversation to physical care
• use communicative repair strategies infrequently
(Hersh, Godecke, Armestrong, Ciccone, Bernhardt, 2014)
Photo: https://angelabrook.com/burnout-affects-more-than-just-
your-nurses

So….how do we help?
We have to
rethink how we
interact with
people who
have aphasia –
including the
use of AAC! Photo: https://lowestoftcommunitychurch.co.uk/sermons/rethink-prayer-the-
legacy-of-prayer/

Google Image Search:
AAC Aphasia Stroke

Google Image Search:
Stroke Wheelchair

Photo Credit: Case Western Reserve:
https://www.laboratoryequipment.com/news/2017/05/stroke-ms-
patients-walk-significantly-better-neural-stimulation

So NOW let me tell you how…
• To avoid using AAC only to compensate for language deficits
• And how to harness the principles of neural plasticity and intersystemic reorganization to use as a language recovery tool
– Even if you are NOT an SLP!
Neural Plasticity (MedicineNet)
• Neuroplasticity allows the neurons (nerve
cells) in the brain to compensate for injury
and disease and to adjust their activities in
response to new situations or to changes
in their environment…”
© ML FACTS BY COLABERRY
FUZZY SYNAPSE
• “The brain's ability to
reorganize itself by
forming new neural
connections throughout
life.

Continued…(MedicineNet)
• Neuroplasticity sometimes may
also contribute to impairment. For
example, people who are deaf may
suffer from a continual ringing in
their ears (tinnitus), the result of
the rewiring of brain cells starved
for sound. For neurons to form
beneficial connections, they must
be correctly stimulated.
• Neuroplasticity is also called brain
plasticity or brain malleability.”

Continued…(MedicineNet)
• Neuroplasticity sometimes may
also contribute to impairment. For
example, people who are deaf may
suffer from a continual ringing in
their ears (tinnitus), the result of
the rewiring of brain cells starved
for sound. For neurons to form
beneficial connections, they must
be correctly stimulated.
• Neuroplasticity is also called brain
plasticity or brain malleability.”

So, how do principles of neuroplasticity translate to the use of AAC as a language recovery tool while avoiding learned non-use?

X
Photo: http://thebrain.mcgill.ca/flash/i/i_10/i_10_cr/i_10_cr_lan/i_10_cr_lan.html
“…Undamaged
axons can also
sprout nerve
endings and
connect with
other undamaged
nerve cells,
forming new
neural pathways
to accomplish a
needed
function…”
(MedicineNet)

Hebbian Learning Neurons that
– “fire together wire together” (Hebb, 1949)
– “fire out of sync lose their link…”
(Artola & Singer 1993; Hebb, 1949; Pulvermuller & Berthier, 2008)
• Recently, CIAT researchers have modified their view on how constraints should be applied during intervention – AAC techniques are
appropriate IF they are not used as a SUBSTITUTE for language. (Difrancesco, Pulvermuller, Mohr, 2012)
Photo: http://standoutpublishing.com/g/hebb,-
donald-o..html Photo: http://www.thecni.org/wp-content/uploads/2013/09/Multiple-Sclerosis.jpeg

Photo: Colleen Kelley University of Cincinnati

TIPz: Technology

TIPz: Personalization
Grids
• People with aphasia CAN learn to sequence iconic codes
• Generalization beyond learned sequences is fair to poor
• Typically employed in a manner that promotes learned non-use
VSDs
• Presence of AAC alone does not
create learned non-use
– Learned non-use is indeed learned!
– Instruction is critical
• Personalization of AAC
– is overwhelming preferred by people
with aphasia and communication
partners
– generates improved communicative
success
– facilitates improved spoken
language
• VSDs promote quicker
generalization and learned
navigation of AAC

Hybrid Displays
PROS
• Best of both worlds
CONS
• High levels of syntactic
and semantic demands
required
• High levels of working
memory and attention
required
• The picture/scene
changes when touched

Hybrid Displays:
What do the data reveal?
• What data?
• TBD…..
• THINK: TIPz
– Technology
– Instruction
– Personalization
Copyright : Marina Gloria Gallud Carbonell

TIPz: Instruction
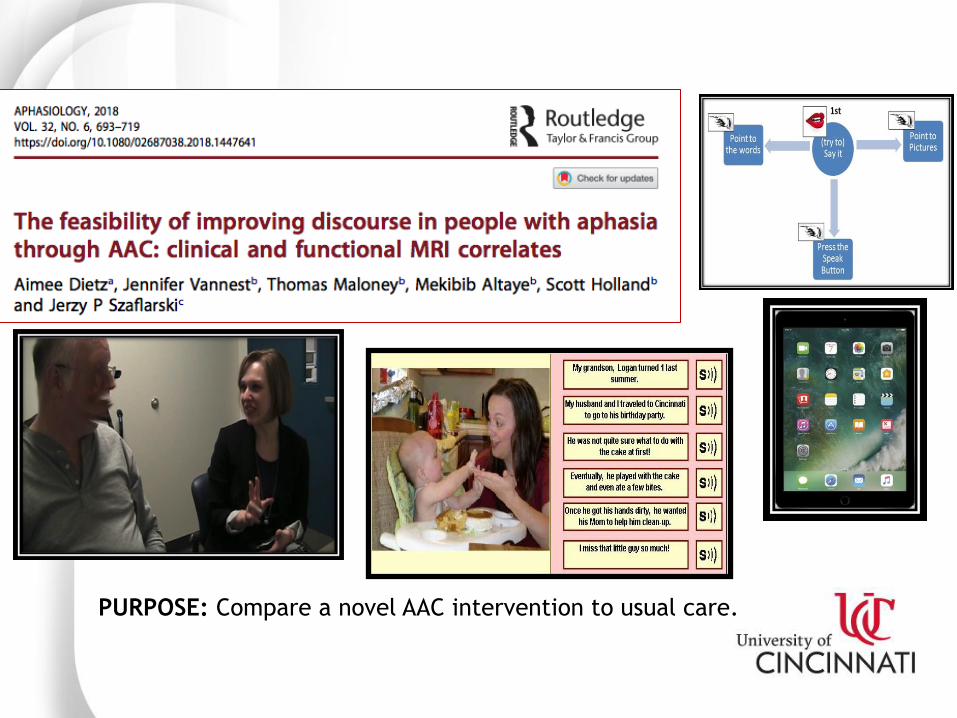
PURPOSE: Compare a novel AAC intervention to usual care.

TIPz: Instruction of Self-Cueing (1)
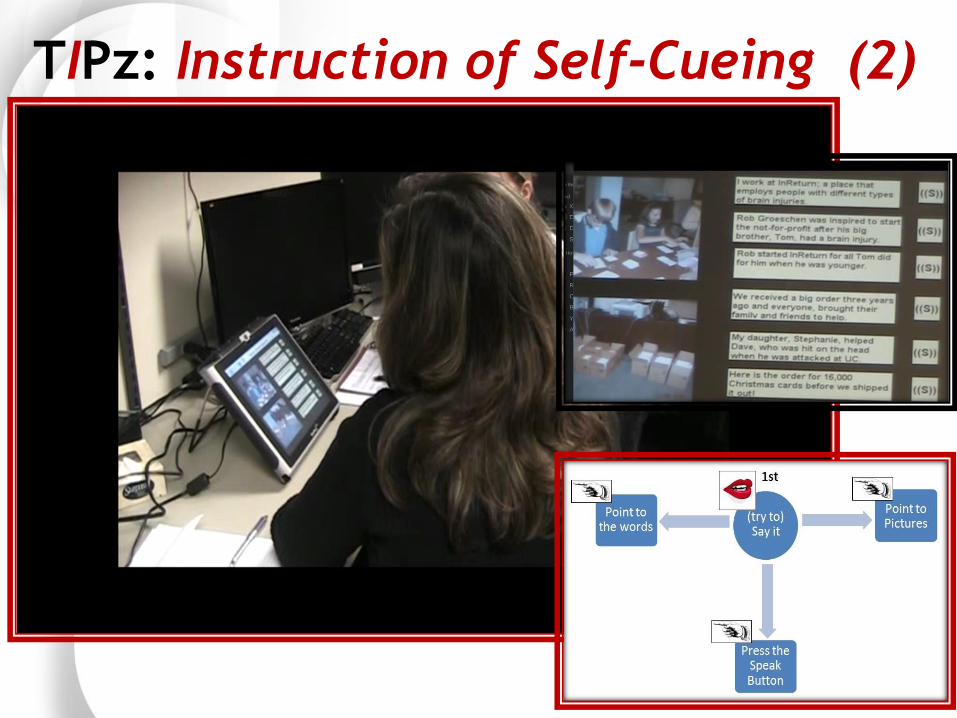
TIPz: Instruction of Self-Cueing (2)

What Happens to Language and
Communication Skills
• Aphasia severity decreased
• Spoke LESS but
– More content
– Longer sentences
• Used pictures and text to
convey thoughts
• No one used “speak
buttons”

Behavio
ral D
ata

What Happens in the Brain?
Photo: Colleen Kelley University of Cincinnati

1. The left-hemisphere
takes over language tasks!
– associated with better
recovery
2. Visual processing regions
help out!
– “backdoor” to language
© ML FACTS BY COLABERRY
FUZZY SYNAPSE
Unique Brain-Based Biomarkers
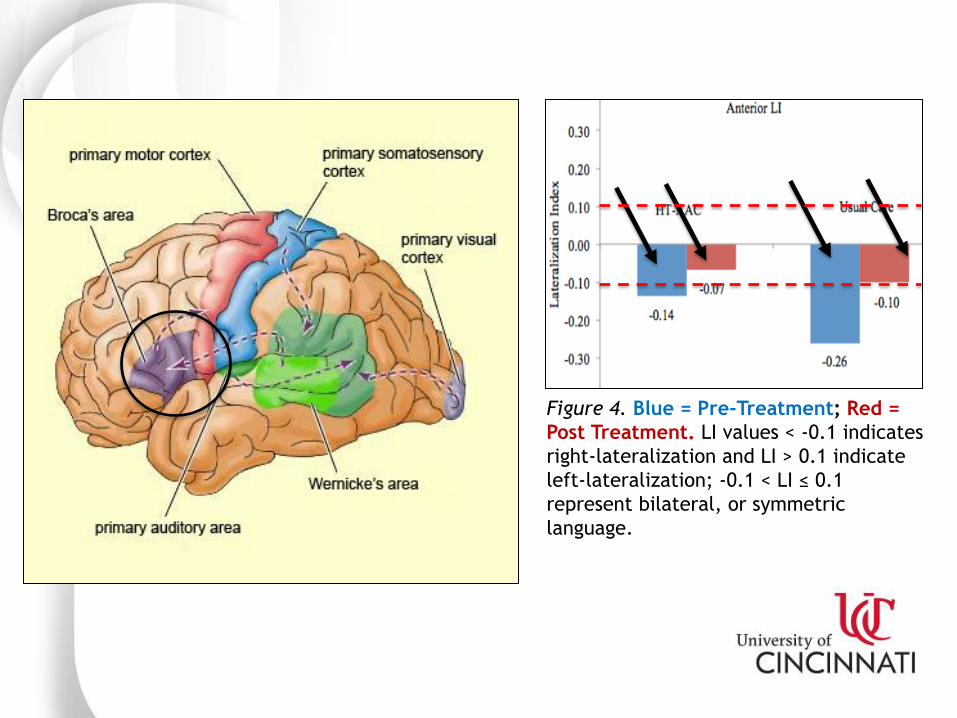
Figure 4. Blue = Pre-Treatment; Red =
Post Treatment. LI values < -0.1 indicates
right-lateralization and LI > 0.1 indicate
left-lateralization; -0.1 < LI ≤ 0.1
represent bilateral, or symmetric
language.

AAC-induced Language Recovery:
A Unique Neurobiological Mechanism? Left = Visual Word Form Area
Right = Object Recognition Object & Face Recognition • Likely alternative
bilateral,
extrasylvian
mechanisms to
help support
language
recovery
• Linking to
canonical
language regions
of interest

In Summary….
• Technology, or AAC, can
facilitate language
recovery
• Instruction is crucial
• Personalized interfaced
Photo: Colleen Kelley University of Cincinnati

PHOTO:
HTTPS://WWW.GOOGLE.COM/SEARCH?RLZ=1C5CHFA_ENUS729US729&BIW=1418&BIH=923&TBM=ISCH&SA=1&EI=ZQEVXI_
RBOAYJWTBPOOQBG&Q=WHAT+CAN+YOU+DO+IMAGE&OQ=WHAT+CAN+YOU+DO+IMAGE&GS_L=IMG.3..0J0I8I30.3244.3244
..3447...0.0..0.132.132.0J1......1....1..GWS-WIZ-IMG.L-NV9D2EUIA#IMGRC=KMERM1BQJPDIEM:

#1 Augmented Input
• Partner identifies that PWA has misunderstood
– blank expression, nodding ambiguously, looks away, answers incorrectly
• Partner then supplements the most difficult, or the most important concepts, by:
a. Writing key words on paper
b. Gesturing symbolically
c. Gesturing deictically (pointing)
d. Pantomiming
e. Referencing pictures
-communication book, communication device
(iPad?), Google ImageTM
• Recheck PWA’s comprehension: “Got it?”
(Garrett & Lasker, 2005; 2013; Wallace, Dietz, Hux, & Weissling 2012)

#2 Written Choice Method
• I have had a stroke. I would like to talk to you, but I cannot speak. We CAN converse if you ask me a question and offer me written choices to point to.
Here’s how:
• THINK OF A QUESTION YOU WOULD HAVE ASKED ME BEFORE MY STROKE.
• TRY TO FIND OUT MY OPINION, GET MY ADVICE, OR PREFERENCES.
(Garrett & Lasker, 2005;
2013)
(Garrett & Lasker, 2005; 2013)

Written Choice Strategy cont’d
• ONCE YOU’VE ASKED THE QUESTION, THINK OF POSSIBLE
ANSWERS OR CHOICES.
• WRITE THEM IN THIS NOTEBOOK. USE A DARK PEN OR
MARKER.
• USE LARGE CAPITAL LETTERS. PUT A DOT IN FRONT OF
EACH CHOICE.
• USE A SCALE FOR “HOW MUCH” QUESTIONS.
(Garrett & Lasker, 2005; 2013)

Where are you from:
• FLORIDA
• MICHIGAN
• NEBRASKA
• OTHER
Written Choice Examples
What do you want to talk about today?
• THERAPY
• MEDICINE
• ARM PAIN
• OTHER

#3 Graphic Rating Scales
The medicine helps…..
1 2 3 4 5 6 7 8 9 10
NONE SOME A LOT
The therapy is……
1 2 3 4 5 6 7 8 9 10
BAD OK GREAT
(Garrett & Lasker, 2005; 2013)

#4 Tagged Yes/No
• Ask questions using reliable response:
– Gesture
– Head nod
– Thumbs-up or -down
– Pointing
• Do you like perogies? Yes (pointing to YES) or No (pointing to NO)
YES
NO
(Garrett & Lasker, 2005; 2013)

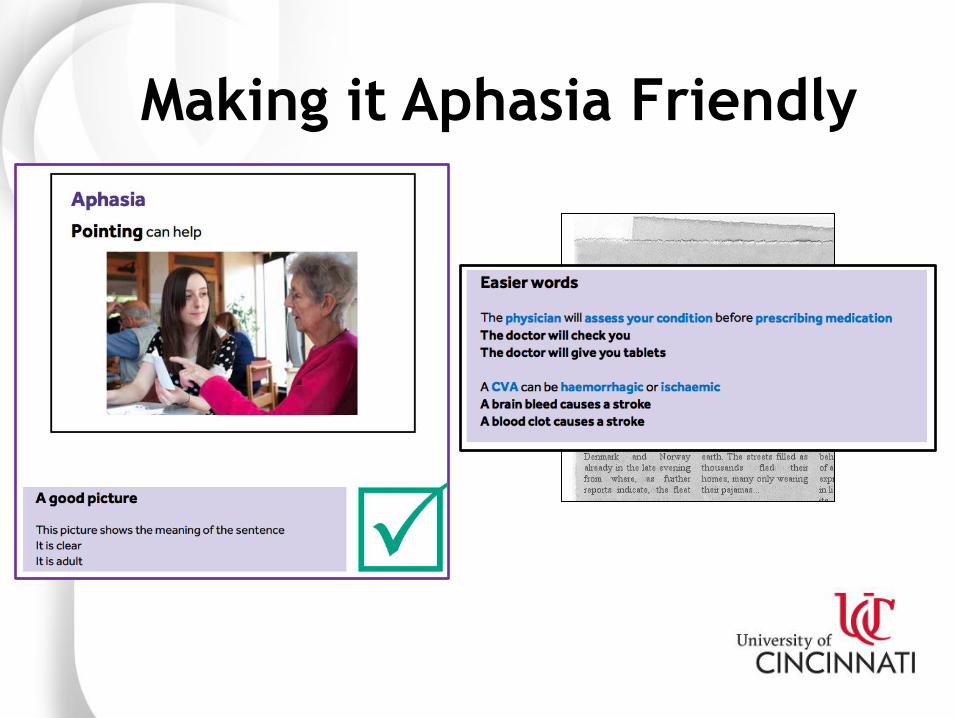
#5 Aphasia Friendly Principles
• White Space (written)
• Pause (spoken)
• Key words*
• Topic setters*
• 14-16 point font
• Simplified syntax &
vocabulary
• Pictures
(Brennan, et al., 2005; Dietz et al., 2009; 2014; Rose et al, 2003)
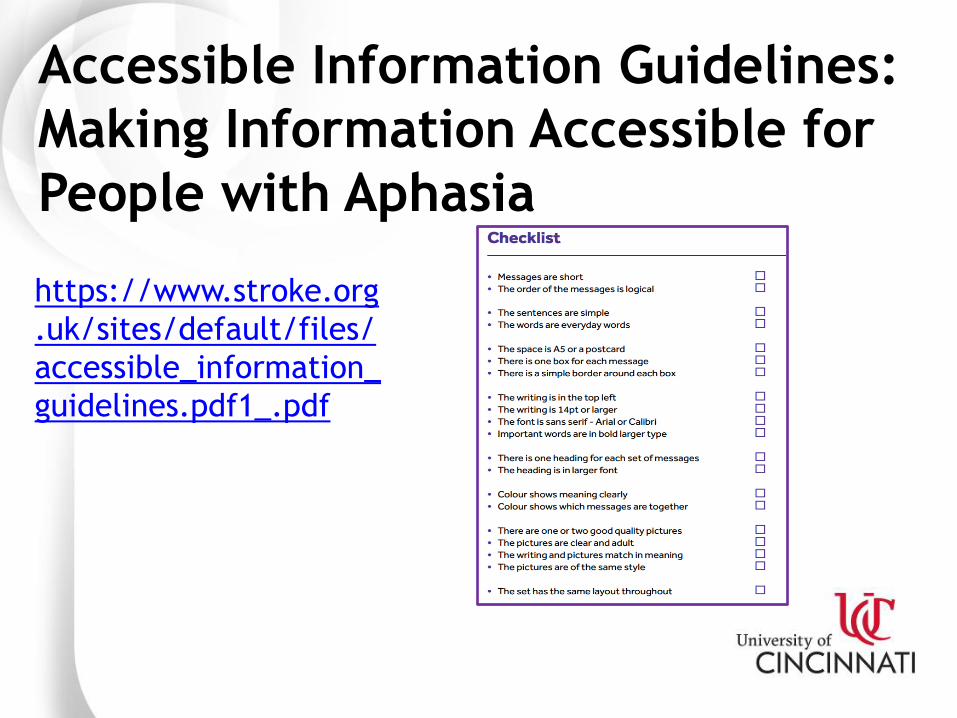
Accessible Information Guidelines:
Making Information Accessible for
People with Aphasia
https://www.stroke.org
.uk/sites/default/files/
accessible_information_
guidelines.pdf1_.pdf
Making it Aphasia Friendly

HERE’S A FEW MORE!

#6 Confirm Accuracy
• EXAMPLE: "You get it?”
• Let me see if I got it right….
– Any takers?
• Use Strategies 1-5, above.

#7 Encourage Circumlocution
GROUP – What kind of a
thing is it? USE
– What do you use
it for?
ACTION
– What does it
do?
(Boyle, 2010; Sutton, 2016)
PROPERTIES
– Describe it to
me. • Color, location,
shape, size
ASSOCATION
– What does it remind you of?

#8 Encourage Writing/Pointing to First Letter
• May not be able to write the
entire word
• Form of self-cueing
• “Air writing”
– Kusho in Japanese
(Dietz et al., 2014; Garrett & Huth, 2002; Wambaugh & Wright, 2007)

#9 Encourage Drawing
• Partner or Patient
• Stimulates word
retrieval
– Highlight semantic
features
• Communicative
Sweetene
r Iced Coffee Hot
Coffee
(Farias, Davis, & Harrington, 2006)
Photo Credits: 2nd Year MA SLP Students at UC!
Photo Credits: “Pat”

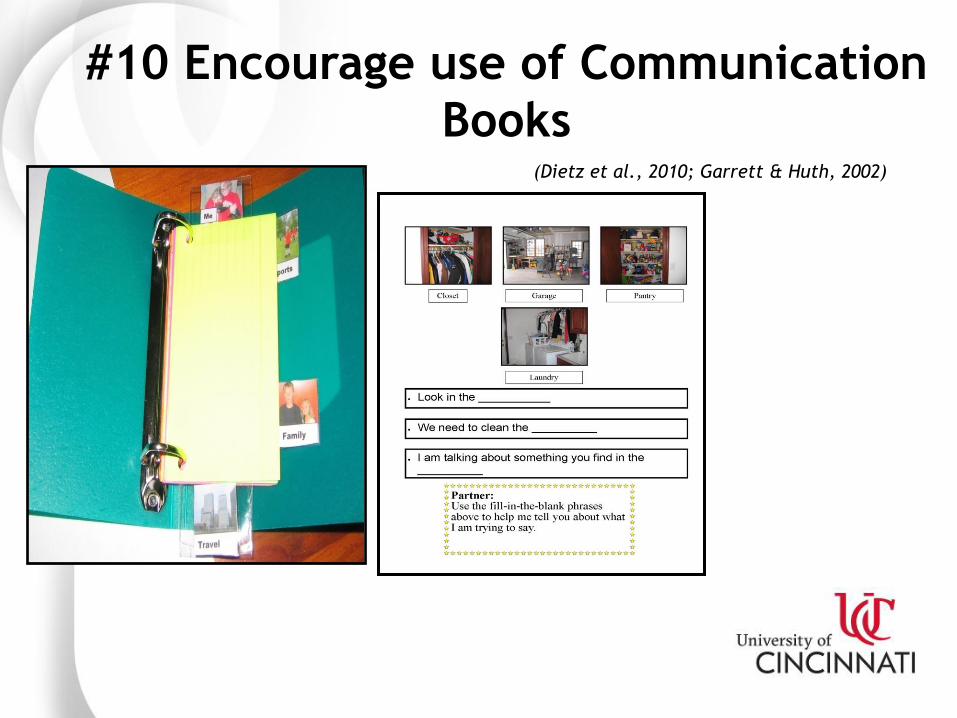
#10 Encourage use of Communication
Books (Dietz et al., 2010; Garrett & Huth, 2002)

NAIL: Neurobiology of AAC-Induced Language Recovery • Aim 1: Determine the therapeutic effect of providing AAC
treatment, designed to evoke language recovery, to people with chronic, post-stroke aphasia.
• Aim 2: Evaluate underlying changes in functional and structural neuroanatomy associated with AAC treatment.
• Exploratory Aim: Identify treatment responder subgroups based on data collected in Aim 1 and Aim 2.
NIH-NIDCD R15DC017280 - 01

Selected References 1. ASHA (2018). Augmentative and alternative communication. Retrieved from https://www.asha.org/Practice-
Portal/Professional-Issues/Augmentative-and-Alternative-Communication/
2. Allendorfer, J.B., Lindsell, C.J., Siegel, M., Banks, C.L., Vannest J., Holland S.K., Szaflarski J.P. (2012) Females
and males are highly similar in language performance and cortical activation patterns during verb generation.
Cortex, 48(9), 1218-33
3. Artola, A. & Singer, W. (1993). Long-term depression of excitatory synaptic transmission and its relationship to
long-term potentiation. Trends in Neurosciences, 16, 480 - 487.
4. Dietz, A., McKelvey, M., & Beukelman, D. (2006). Visual scene display: New AAC interface for persons with aphasia,
Perspectives on Augmentative and Alternative Communication, 15(1), 13-17. doi: 10.1044/aac15.1.13
5. Dietz, A., Weissling, K., Griffith, J.,* McKelvey, M., Macke, D.* (2014). The impact of interface design during an
initial high-technology AAC experience: A collective case study of people with aphasia. Augmentative and
Alternative Communication.
6. Dietz, A., Vannest, J., Maloney, T., Altaye, M., Holland, S., & Szaflarski, J.P. (2018). Pilot study of AAC for the
treatment of post-stroke aphasia: Clinical and fMRI correlates. Aphasiology.
7. Garrett, K., & Lasker, J. (2013). Adults with severe aphasia. In D. Beukelman & P. Mirenda (Eds.), Augmentative
and alternative communication (4th ed., pp. 405-446). Baltimore, MD: Paul H. Brooks.
8. Griffith, J., Dietz, A., & Weissling, K. (2014). Supporting Narrative Retells for People with Aphasia using AAC:
Photographs or Line Drawings? Text or No Text? American Journal of Speech Language Pathology. Supplement:
Select papers from the 43rd Clinical Aphasiology Conference, S1-S12. DOI: 10.1044/2014_ASLP-13-008.
9. Hebb, D. O. (1949). The Organization of Behavior. New York: Wiley & Sons.
10. Hunt K. W. (1970). Syntactic maturity of school children and adults. Monograph of the Society for Research in
Child Development, 35, 1 - 78.
11. Hunt, K. W. (1965). Grammatical structures written at three grade levels. (Research Rep. No 3). Champaign, IL:
National Council of Teachers of English.
12. McKelvey, M., Hux, K., Dietz, A., & Beukelman, D. R. (2010). Impact of Personal Relevance and Contextualization
on Comprehension by People with Chronic Aphasia. American Journal of Speech-Language Pathology, 19, 22-33.
13. Pulvermuller, F., & Berthier, M. L. (2008). Aphasia therapy on a neuroscience basis. Aphasiology, 22(6), 563 - 599
16. Rose, M.L., Releasing the Constraints on Aphasia Therapy: The Positive Impact of Gesture and Multimodality
Treatments. American Journal of Speech-Language Pathology, 2013. 22(2): p. S227-S239.
17. Weissling, K. & Prentice, C. (2010). The timing of remediation and compensation rehabilitation programs for
individuals with acquired brain injuries: Opening the conversation. Perspectives on Augmentative and Alternative
Communication, 19(3), 87-96.





























