Embed Size (px)
Citation preview

NUTRITION AND CANCER, 59(2), 217–227Copyright C© 2007, Lawrence Erlbaum Associates, Inc.
A Novel Dietary-Related Model of Esophagitis and Barrett’sEsophagus, a Premalignant Lesion
Naihsuan C. Guy, Harinder Garewal, Hana Holubec, Harris Bernstein, Claire M. Payne,Carol Bernstein, Achyut K. Bhattacharyya, and Katerina Dvorak
Abstract: Barrett’s esophagus (BE) is a premalignant le-sion in which columnar epithelium (containing goblet cells)replaces esophageal squamous cells. Previous evidence sug-gested that hydrophobic bile acids and zinc deficiency eachplay a role in BE development. We fed wild-type C57BL/6mice a zinc-deficient diet containing the hydrophobic bileacid, deoxycholic acid for various times up to 152 days. Allmice fed this diet developed esophagitis by 69 days on the dietand 63% of the mice on this diet for 88 to 152 days also devel-oped a BE-like lesion. Esophageal tissues showed thickenedmucosa, increased proliferation, and increased expression ofmarkers associated with oxidative and nitrosative stress. Thenewly formed BE-like lesions expressed Mucin-2, a markerof columnar differentiation. They also showed translocationof the p65 subunit of nuclear factor-κB and β-catenin to thenucleus and typical histological changes associated with BElesions. This mouse model of esophagitis and BE is expectedto contribute to a deeper understanding of BE pathogenesisand to strategies for prevention of BE progression to cancer.
Introduction
Barrett’s esophagus (BE) is a premalignant lesion at thedistal part of the esophagus that arises as a consequenceof chronic gastroesophageal reflux. Heartburn and gastroe-sophageal reflux disease (GERD) are common medical con-ditions in Western countries. Approximately 40% of adultscomplain of heartburn at least monthly (1). BE is estimatedto be present in approximately 10 to 12% of patients un-dergoing endoscopic examination for symptomatic GERD(2). This represents at least 2 million people in the UnitedStates (1). Patients with BE have an increased risk of de-veloping esophageal adenocarcinoma (EAC) (3). Multiple
N. C. Guy is affiliated with the Department of Immunobiology, College of Medicine, University of Arizona, Tucson, AZ 85724. H. Garewal is affiliatedwith the Arizona Cancer Center and the Department of Internal Medicine, College of Medicine, University of Arizona, Tucson, AZ 85724 and with the Sectionof Hematology/Oncology, Southern Arizona VA Health Care System, Tucson, AZ 85723. H. Holubec, H. Bernstein, C. M. Payne, C. Bernstein, and K. Dvorakare affiliated with the Department of Cell Biology and Anatomy, College of Medicine, University of Arizona, Tucson, AZ 85724. H. Bernstein, C. M. Payne,and K. Dvorak are also affiliated with the Arizona Cancer Center, College of Medicine, University of Arizona, Tucson, AZ 85724. H. Garewal, C. M. Payne, andC. Bernstein are also affiliated with the Section of Hematology/Oncology, Southern Arizona VA Health Care System, Tucson, AZ 85723. A. K. Bhattacharyyais affiliated with the Department of Pathology, College of Medicine, University of Arizona, Tucson, AZ 85724.
epidemiological studies have shown that the incidence ofesophageal adenocarcinoma in the United States and West-ern Europe is rapidly rising (4). EAC has a poor prognosis,with a median survival of less than 1 yr (1).
Histologically, BE is characterized by intestinal metapla-sia (IM), a condition where squamous epithelial cells arereplaced by metaplastic intestinal-like columnar epitheliumcontaining goblet cells. However, the mechanism of devel-opment of BE is poorly understood. Obesity and chronicirritation of the esophageal mucosa by gastric acids, pro-teases, and bile acids are considered 2 major risk factors forBE development (5–7).
Current animal models used for studying BE and EACinclude canine, rabbit, rat, and mouse models, which all re-quire a surgical procedure. The most common rat model usesesophagogastroduodenal anastomosis without concomitantchemical carcinogen treatment, leading to development ofcolumnar-lined esophagus (CLE) including metaplasia, dys-plasia, and EAC (8). However, these surgical animal mod-els have significant limitations. They are expensive, tech-nically challenging, time consuming, nonphysiological, andnot very efficient. Therefore, it is important to develop ananimal model that can acquire CLE by a nonartificial andless invasive method.
Epidemiological studies have indicated the associationof zinc deficiency with increased risk of cancer develop-ment (9). The total body zinc content in humans is 2 to4 g, and there is no specialized zinc storage system inthe body. Therefore, regular supplementation is essential(10). Approximately 10% of the U.S. population consumesless than half the recommended daily allowance for zinc(10). Interestingly, tumors and glandular metaplasia resem-bling BE developed in nearly 20% of p53−/− mice af-ter 3 wk on a zinc-deficient diet and a single treatmentwith N -nitrosomethylbenzylamine (NMBA) and in 14% of

transgenic mice overexpressing cyclin D1 after 4 wk ona zinc-deficient diet and a single treatment with NMBA(11,12).
Clinical studies have shown that obesity, 1 of the riskfactors for developing BE, is associated with hypozincemiaand defective antioxidant status (5). Also, certain commonlyused drugs that lower gastric secretion, such as proton pumpinhibitors (PPI) and H2 receptor inhibitors, diuretics, ACEinhibitors, and oral contraceptives decrease zinc absorption(13–16).
Bile is a component of gastroduodenal refluxate (17). Pri-mary bile acids, such as glycocholic acid, taurocholic acid,glycodeoxycholic acid, and glycochenodeoxycholic acid, arethe bile acids predominantly present in the esophagus of pa-tients with GERD. It has been shown that PPI therapy causesan overgrowth of gastric bacteria in patients with GERD (18).Such bacteria may deconjugate the primary bile acids to formthe more toxic unconjugated bile acids such as deoxycholicacid (DOC) (18). DOC is also present in the refluxate of BEpatients (19).
We hypothesized that a diet deficient in zinc and sup-plemented with a bile acid, such as DOC, can lead to thedevelopment of BE-like lesions in mice. Such a novel ex-perimental animal model for studying esophagitis and BEmay give insight into the induction of columnar differen-tiation, proliferation, DNA damage, and oxidative stress inthe esophagus. Experimental animal models should provideuseful insights into possible molecular mechanisms underly-ing development of esophagitis and consequently to possiblestrategies for preventing progression to BE.
Materials and Methods
Animal Model
Forty-eight male C57BL/6 mice were obtained from Jack-son Laboratory (Bar Harbor, ME) and maintained in the Uni-versity of Arizona’s Animal Care facility. The animals werehoused 2 in a cage and raised under nonsterile microiso-lator conditions in compliance with the National Institutesof Health’s regulations and guidelines for care and use oflaboratory animals. The mice were maintained on a 12-hlight–dark cycle with free access to deionized drinking wa-ter. The mice were randomized into 4 dietary groups with 12mice per group. They were fed customized diets prepared byHarlan Teklad (Madison, WI). The diets were fed starting at5 wk of age until completion of the dietary treatment. The 4diet groups were a control diet, a zinc-deficient diet (Zn−), adiet supplemented with 0.2% DOC (Sigma D6750) (DOC+),and a zinc-deficient diet supplemented with 0.2% DOC(DOC+Zn−). The vitamin mix used in each of the diets isgiven in Table 1, and all components of the 4 diets are shownin Table 2. The mice were monitored for clinical signs of illhealth. One mouse on the DOC+Zn− diet died after 137 dayson the diet, before sacrifice, and was not included in the study.
Table 1. Vitamin Mix From Teklad (CA.40060) in g/kg
p-Aminobenzoic acid 11.0132Vitamin C, ascorbic acid, coated (97.5%) 101.6604Biotin 0.0441Vitamin B12 (0.1% in mannitol) 2.9736Calcium pantothenate 6.6079Choline dihydrogen citrate 349.6916Folic acid 0.1982Inositol 11.0132Vitamin K3, menadione 4.9559Niacin 9.9119Pyridoxine HCl 2.2026Riboflavin 2.2026Thiamin HCl 2.2026Vitamin A palmitate (500,000 IU/g) 3.9648Vitamin D3, cholecalciferol (500,000 IU/g) 0.4405Vitamin E, DL-alpha tocopheryl acetate (500 IU/g) 24.2291Corn starch 466.6878
Mice were kept on their diets and then sacrificed at inter-vals up to 152 days on diet, except for 3 mice on the DOC+diet and 4 mice on the control diet, which were terminatedafter a longer period (225 days) to determine if a lengthiertime on the DOC+ diet would give rise to BE (there was noBE in these longer-treated mice). Mice were sacrificed usingCO2 asphyxiation.
Animal Tissue Preparation
Tissues from the esophagus and stomach were taken andimmediately fixed in 10% buffered formalin for 24 h at 4◦Cand then transferred to 70% ethanol. The tissue samples werethen processed for paraffin embedding and sectioned.
Histopathological Analysis
For histological evaluation, the formalin-fixed, paraffin-embedded mouse tissues were sectioned and stained withhematoxylin and eosin (H&E). Diagnosis of BE was madeby the presence of columnar metaplasia containing gobletcells surrounded by squamous epithelium. The pathologistevaluating the tissues was blinded as to the identity of thediets of the mice prior to his histological evaluation andanalysis for the presence of BE lesions.
Immunohistochemistry
Tissues were evaluated for expression of individualbiomarkers by employing standard indirect immunohisto-chemical techniques using different antibodies. In brief, thetissue sections were deparaffinized and hydrated. Antigen re-trieval was performed by immersing the sections in 0.01Mcitrate buffer (pH 6.1) and heating in a microwave at highpower for 2 min and 45 s and then at the defrost settingfor 6 min. 8-hydroxy-deoxyguanosine monoclonal antibody
218 Nutrition and Cancer 2007

Table 2. Composition of the Mouse Diets in g/kga
Control Zn(−) DOC(+) Zn(–)DOC(+)
Egg white solids, spray dried 200.0000 200.0000 200.0000 200.0000Dextrose, monohydrate 632.2658 632.2658 632.2658 632.2658Corn oil 100.0000 100.0000 100.0000 100.0000Cellulose 29.9107 30.0000 29.9107 30.0000Vitamin mix (see Table 1) 10.0000 10.0000 10.0000 10.0000Biotin 0.0040 0.0040 0.0040 0.0040Ethoxyquin (antioxidant) 0.0200 0.0200 0.0200 0.0200Calcium phosphate, dibasic 19.7670 19.7670 19.7670 19.7670Magnesium sulfate 2.4752 2.4752 2.4752 2.4752Potassium chloride 2.2882 2.2882 2.2882 2.2882Sodium chloride 0.7781 0.7781 0.7781 0.7781Ferrous sulfate 0.2000 0.2000 0.2000 0.2000Manganese sulfate 0.1662 0.1662 0.1662 0.1662Cupric sulfate 0.0151 0.0151 0.0151 0.0151Potassium iodate 0.0004 0.0004 0.0004 0.0004Chromium potassium sulfate 0.0200 0.0200 0.0200 0.0200Zinc carbonate 0.0893 — 0.0893 —Sodium deoxycholate — — 2.0000 2.0000
a: Abbreviations are as follows: Zn, zinc; DOC, deoxycholic acid.
(2 µg/ml; QED Bioscience Inc., San Diego, CA) was usedfor detecting oxidative DNA damage. For this special stain-ing, the slides were immersed in 4N HCl for 20 min andthen rinsed in 4 changes of nanopure water and placed in0.1M Borax for 5 min followed by 2 rinses in nanopurewater to open up the chromatin. Endogenous peroxidase ac-tivity was blocked with 3% hydrogen peroxide for 20 min,and then the slides were incubated with 1.5% normal serum(of either goat, mouse, horse, or rabbit, corresponding to theorganism in which the secondary antibody was created) for45 min. The primary antibodies included polyclonal anti-bodies against Mucin-2 (MUC2; Santa Cruz Biotechnology,Santa Cruz, CA; 1:50 dilution), proliferating cell nuclearantigen (PCNA; Santa Cruz Biotechnology, Santa Cruz, CA;1:100 dilution), nitrotyrosine (Upstate Cell Signaling Solu-tions, Lake Placid, NY; 1:60 dilution), and nuclear factor-κB (NF-κB) p65 (Santa Cruz Biotechnology, Santa Cruz,CA; 1:400 dilution) and monoclonal antibodies against 8-hydroxy-deoxyguanosine (8-OH-dG; QED Bioscience, SanDiego, CA; 1:400 dilution) and β-catenin (BD TransductionLaboratories, Franklin Lakes, NJ; 1:300 dilution). For de-velopment and detection of antibody staining, sections wereincubated with appropriate secondary biotinylated antibodyand treated with avidin-biotin complex followed by a chro-mogen, 3,3′-diaminobenzidine tetrahydrochloride. The sec-tions were counterstained with hematoxylin, dehydrated, andmounted with CytosealTM 60 mounting medium (Richard-Allan Scientific, Kalmazoo, MI).
Statistical Evaluations
Histological changes in gastroesophageal morphologywere determined in hematoxylin and eosin stained sectionsfrom esophageal tissue obtained from each of the terminatedmice in each experimental group. A morphologic grading
score was established by evaluating degrees of proliferation,keratinization, and esophagitis on a scale of 0 to 4 for eachof these categories (with 0 being no significant change fromthose mice on the control diet, 1 being a small detectablechange, 2 being a moderate change, 3 being a substantialchange, and 4 being a maximal change) and presence or ab-sence of BE-like lesions evaluated as 0 or 4 for absenceor presence of BE, respectively. A composite score wasdetermined as the sum of the scores for the 4 categories. Themorphologic score for each dietary group was expressed as amean ± SD. An unpaired Student t-test was performed, anda P value of <0.05 was considered statistically significant.
To determine whether the frequency of BE occurring dur-ing a dietary treatment was significantly different from that incontrol-fed mice, the 2-sample Wilcoxon rank sum (Mann–Whitney) test was used.
Results
Histopathology
Mice were terminated at intervals after starting on the 4test diets (control, Zn−, DOC+ and DOC+Zn− diets) toevaluate at what point histological changes began to occurin their esophagus and to determine when, if at all, BE oc-curred. By 152 days on the diets, mice on the DOC+Zn−and Zn− diets showed a decline in their general health sothat the majority of mice were terminated by this point. The2 mice terminated at the early time of only 41 days on thediets (1 on a DOC+ diet and 1 on a DOC+Zn− diet) had nohistopathological changes. At longer times of 69 to 152 dayson the diets, the DOC+Zn− diet induced gastroesophagealchanges resembling typical histological findings associatedwith reflux esophagitis and BE in patients (Fig. 1D, 1E,1F). Of the mice fed the DOC+Zn− diet for times between
Vol. 59, No. 2 219

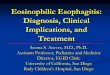
Figure 1. Histological appearance of the esophagus of mice fed different diets. A: Control diet. B: DOC+ diet. Note thickened epithelium and hyperkeratiniza-tion compared to the control. C: Zn− diet. Note some hypertrophy of papillae and hyperkaritization. D: DOC+Zn− diet. Note development of esophagitis. E:DOC+Zn− diet. Note the presence of metaplastic epithelium with goblet cells of BE-like lesion. [hematoxylin and eosin (H&E); original magnification A toE: ×100). F: DOC+Zn− diet. Note papillae hypertrophy (green arrow), increased angiogenesis (black arrow), and inflammation (red arrow) (H&E; originalmagnification: ×200).
88 days and 152 days (Fig. 2A), 63% (5 out of 8) devel-oped BE-like lesions in which normal squamous epitheliumwas replaced by specialized intestinal metaplastic epitheliumcontaining goblet cells (Fig. 1E). One mouse on the Zn− dietdeveloped BE by 152 days on the diet as indicated in Fig.2A. All mice fed for between 69 days and 152 days with theDOC+ diet (Fig. 1B), Zn− diet (Fig. 1C), or Zn−DOC+diet (Fig. 1D) developed basal cell hyperproliferation and/orhyperkeratinization in esophageal tissues. The Zn−DOC+
diet, fed for between 69 and 152 days, induced esophagitischaracterized by the development of papillae hypertrophy(Fig. 1F, green arrow), angiogenesis (Fig. 1F, black arrow),and an increased infiltration of inflammatory cells (Fig. 1F,red arrow). We performed immunohistochemical staining ofthe newly formed BE-like lesions to examine the expressionof biomarkers of columnar differentiation, proliferation, ox-idative and nitrosative stresses, NF-κB p65, and β-catenin(see following).
220 Nutrition and Cancer 2007

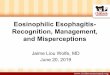
Figure 2. A: The mean weights of the mice on each diet between the time they were entered onto the diets (at 5 wk of age) until 152 days on the diets isshown. Arrows below the weight curves indicate the times at which the indicated number of mice on the deoxycholic acid (DOC)+zinc(Zn)− diet (shownin the Fig. as D+Z− ) were terminated. The text below these lower arrows also indicates how many of the mice had Barrett’s esophagus (BE) at the time oftermination. Arrows above the weight curves indicate the times at which the given number of mice on the control diet (shown by C), the DOC+ diet (shownby D+), and the Zn− diet (shown by Z−) were terminated. Only 1 of these latter mice (on the Zn− diet) had a small BE lesion, as indicated. B: Effect of dietsshown on the abscissa on gastroesophgeal morphology. The mean morphology composite score based on degree of proliferation, keratinization, esophagitis,and the presence of BE-like lesions was determined for each group of mice. Asterisks indicate a statistically significant difference compared to the controlgroup (P<0.05).
Dietary Effects on Body Weight and GastroesophagealMorphology
Mean body weight for each group of mice, measured dur-ing days 0 to 152 of the dietary treatments, is shown in Fig.2A. Fig. 2A also shows the numbers and times at which mice
were terminated, between 42 and 152 days on the diets, byvertical arrows. Fig. 2B shows the mean morphologic com-posite scores for mice terminated between 69 and 152 dayson the diet for mice fed the control diet, the DOC+ diet,the Zn− diet and the DOC+Zn− diet based on the degree
Vol. 59, No. 2 221

Figure 3. Immunohistochemical analysis of Mucin2 (MUC2) in the esophagus of mice fed different diets. (A–C) A: Control diet. B: deoxycholic acid(DOC)+zinc(Zn)− diet. Note that this tissue section shows esophagitis but no Barrett’s esophagus (BE)-like lesion. C: DOC+Zn− diet. Note that this tissueshows strong MUC2-positive expression in the goblet cells at the base of crypts in a BE-like lesion (original magnification: ×400). Immunohistochemicalanalysis for proliferating cell nuclear antigen (PCNA) in the esophagus of mice fed different diets. (D–F) D: Control diet. Note that there are relatively fewPCNA stained cells, thus indicating the normal baseline of proliferating cells in the esophageal tissue. E: DOC+Zn− diet. Note that this tissue has developedesophagitis and increased PCNA-positive cells throughout the hypertrophied papillae. F: DOC+Zn− diet. Note that this tissue has developed a BE-like lesion.Strong nuclear staining and a significant increase of positive PCNA expression is observed in the metaplastic epithelium of this BE-like lesion (originalmagnification: ×200).
of proliferation, keratinization, incidence of esophagitis, andpresence of BE-like lesions in the esophageal tissues. Spec-imens taken from mice fed the DOC+ diet (P = 0.005),the Zn− (P = 0.0004), and the DOC+Zn− (P = 0.00002)all showed significant increases in morphological changesin gastroesophageal morphology in comparison to mousetissues from mice fed the control diet. The combination ofzinc-deficient diet plus supplementation with DOC showed asynergistic effect in increased alteration of gastroesophagealmorphology and induction of the development of BE-likelesions.
We did continue 3 mice on the DOC+ diet and 4 mice onthe control diet for 225 days (until 32 wk of age or 8.5 moof age) to see if the extended time on the DOC+ diet wouldresult in BE. There was no evidence of BE in these olderDOC+ mice, although they did gain much more weight thanthe mice on the control diet, with older mice on the DOC+diet weighing an average of 44.7 g and older mice on thecontrol diet weighing an average of 23.0 g at the time oftermination.
We compared the incidence of BE in mice fed for 88 daysor more on the DOC+Zn− diet (5 out of 8 developed BE)with the incidence of BE in mice fed the control diet for 88days or more (0 out of 11 developed BE) using the 2-sampleWilcoxon rank-sum (Mann–Whitney) test and found that thedifference in incidence was significant (P >|z| = 0.003). Bythis test, the single incidence of BE in the mice fed the
Zn− diet for more than 88 days did not reflect a significantdifference from the mice fed the control diet.
Columnar Differentiation Markers
As shown in Fig. 1E, there was goblet cell-type metaplasiain BE-like lesions in tissues from mice fed with a DOC+Zn−diet. The lesions were characterized by the appearance ofcolumnar-like epithelium with expression of MUC2 in thegoblet cells (Fig. 3C). MUC2-positive cells were not ob-served in the mice fed the control diet (Fig. 3A) or in themice fed a DOC+Zn− diet that only developed esophagitis(Fig. 3B).
PCNA
PCNA is an accessory protein for DNA polymeraseδ and an indicator of cell cycle progression at the G1/Stransition (20). There was minimal PCNA staining withincells of mice fed the control diet (Fig. 3D). In contrast, inmice fed a DOC+Zn− diet, numerous PCNA-positive cellsoccurred throughout the mucosal tissue displaying esophagi-tis, especially in the enlarged papillae in the basal layer (Fig.3E). Strong abundant positive expression of PCNA was alsoobserved in the metaplastic epithelium of BE-like lesions
222 Nutrition and Cancer 2007

Figure 4. Immunohistochemical analysis of 8-hydroxy-deoxyguanosine (8-OH-dG) in the esophagus of mice fed different diets. (A–C) A: Control diet. Notethat there are relatively few 8-OH-dG stained cells, indicating normal minimal oxidative stress in the esophageal tissue. B: deoxycholic acid (DOC)+zinc(Zn)−diet. Note that this tissue has developed esophagitis and increased 8-OH-dG immunoreactivity indicating increased oxidative stress. C: DOC+Zn− diet.Note the Barrett’s esophagus (BE)-like lesion with increased immunoreactivity of 8-OH-dG (original magnification: ×400). Immunohistochemical analysis ofnitrotyrosine in the esophagus of mice fed different diets. (D–F) D: Control diet. Note that nitrotyrosine immunoreactivity is absent. E: DOC+Zn− diet. Notethat this tissue has developed esophagitis, but nitrotyrosine immunoreactivity is absent. F: DOC+Zn− diet. Note the BE-like lesion with intense nitrotyrosinestaining in the epithelial cells, especially in the upper portion of the epithelial mucosa (original magnification: ×400).
in the esophageal tissue of mice fed the DOC+Zn− diet(Fig. 3F).
Oxidative Stress and DNA Damage
8-OH-dG is a modified DNA base that is formed due toattack by hydroxyl radicals that are formed as byproducts andintermediates of aerobic metabolism and during oxidativestress (21). As shown in Fig. 4A, there was minimal 8-OH-dG signal in cells of mice fed the control diet. However, thetissues from mice fed a DOC+Zn− diet resulted in elevatedlevels of 8-OH-dG in inflamed esophageal tissue (Fig. 4B)and in BE-like lesions (Fig. 4C).
Nitrosative Stress
Antinitrotyrosine antibody was used to detect 3-nitrotyrosine, providing good evidence for the formation ofperoxynitrite and other reactive nitrogen species in vivo. Asshown in Fig. 4D and 4E, nitrotyrosine was absent or weakin esophageal tissues taken from mice fed the control dietand from mice that were fed the DOC+Zn− diet but thatonly developed esophagitis. In contrast, nitrotyrosine im-munoreactivity was intense in the epithelial cells in BE-likelesions from mice that were fed the DOC+Zn− diet (Fig. 4F).
Positive nuclear nitrotyrosine expression is also present insome cells in the BE-like lesions (Fig. 4F).
Transcription Factor NF-κB p65)
As illustrated in Fig. 5A, esophageal epithelium from micefed the control diet showed only cytoplasmic immunoreactiv-ity of the p65 subunit of NF-κB. However, nuclear translo-cation of the p65 was observed in regions of esophagitis(Fig. 5B) and BE-like lesion tissues (Fig. 5C) of mice fed theDOC+Zn− diet.
β-Catenin
β-catenin is a key regulator in the E-cadherin-mediatedcell adhesion system and acts as an oncoprotein whentransported to the nucleus. Fig. 5D shows that β-cateninexpression is localized at the cell membrane in the esophagealsquamous epithelium of mice fed the control diet and for mostcells in mice fed the DOC+Zn− diet and showing esophagitis(Fig. 5E). Loss of membranous β-catenin immunoreactivitywith diffuse cytoplasmic staining and nuclear staining wereobserved in some cells of tissues showing esophagitis (Fig.5E) and BE-like lesions (Fig. 5F) in tissues of mice fed theDOC+Zn− diet. Focal nuclear staining for β-catenin was
Vol. 59, No. 2 223

Figure 5. Immunohistochemical analysis for the p65 subunit of nuclear factor-κB (NF-κB) in the esophagus of mice fed different diets. (A–C) A: Controldiet. Note the cytoplasmic immunoreactivity of the esophageal epithelial cells. B: deoxycholic acid (DOC)+zinc(Zn)− diet. Note the tissue has developedesophagitis and a marked increase in p65 subunit immunoreactivity. C: DOC+Zn− diet. Note the increase in nuclear translocation of NF-κB in metaplasticcolumnar epithelial cells in BE-like lesions. This image is shown at higher magnification than the other images to better demonstrate translocation of thep65 subunit into the nuclei. Immunohistochemical analysis of β-catenin in the esophagus of mice fed different diets. (D–F) D: Control diet. Note that thenormal esophageal squamous epithelial cells show homogeneous membrane staining for β-catenin. E: DOC+Zn− diet. Note that there is generally no changein expression of β-catenin in the esophagitis tissue compared to the expression in normal esophageal epithelium, although there is some loss of membraneβ-catenin immunoreactivity with diffuse cytoplasmic staining in some cells in this tissue showing esophagitis. F: DOC+Zn− diet. Note the BE-like lesionwith loss of membranous β-catenin immunoreactivity with diffuse cytoplasmic staining in some cells. Also, some cells show nuclear localization of β-catenin(original magnification: ×400).
also observed in some scattered cells in the BE-like lesions(Fig. 5F).
Discussion
EAC is one of the most deadly forms of cancer, with amortality rate exceeding 90%, and an incidence that is in-creasing rapidly in the United States and many regions ofWestern Europe. The major risk factor for the developmentof EAC is BE (22). Patients with BE are at 30 to 40 timesgreater risk of developing EAC than individuals in the generalpopulation (23). BE is a premalignant lesion of the distal partof the esophagus that arises as a consequence of chronic gas-troesophageal reflux. The classic endoscopic feature of BEis the presence of salmon pink mucosa at the distal region ofthe esophagus. Histologically, BE is defined as the metaplas-tic conversion of normal esophageal squamous epitheliuminto columnar intestinalized epithelium with the presenceof goblet cells. The molecular mechanisms underlying thedevelopment of BE are unclear. However, BE appears to re-sult from chronic irritation by bile acids and gastric acid(7).
Importantly, bile acids have been linked to the develop-ment of gastrointestinal (GI) cancers (24). Clinical studieshave shown an increased concentration of bile acids in pa-
tients with reflux disease and BE (17). Bile acids cause ox-idative stress, DNA damage, perturbed mitochondrial res-piration, and induction of apoptosis (24–28). In addition,gastric acid and bile acids may alter cell signaling pathways(29–31). Bile acids are implicated in promoting GI cancersby modulating cell signaling pathways, causing epigeneticchanges, increasing proliferation, and promoting develop-ment of apoptosis resistance on long-term exposure (24).Both human studies and animal models of GI reflux esophagi-tis have implicated hydrophobic bile acids in the developmentof the BE lesion and EAC (24).
Zinc is an essential mineral that is found in almost ev-ery cell. Zinc is an important component of over 1,000 pro-teins, including DNA-binding proteins with zinc fingers, cop-per/zinc superoxide dismutase, and several proteins involvedin DNA-damage repair such as p53, which is mutated in halfof human tumors (32). Zinc directly stimulates the activ-ity of more than 100 enzymes (33). Therefore, insufficientzinc intake can impair antioxidant defenses and compromiseDNA-repair mechanisms, making the cell highly susceptibleto oxidative DNA damage. In humans, there is a significantinverse association between dietary intake of zinc and in-cidence of EAC (34). Furthermore, BE lesions develop inabout 20% of p53−/− mice or transgenic mice overexpress-ing cyclin D1 that were on a zinc deficient diet and treatedonce with the carcinogen NMBA (11).
224 Nutrition and Cancer 2007

Mucins are secretory proteins of the GI mucosa expressedin a cell-specific manner in normal GI tissues. MUC2 is aprincipal secretory mucin abundantly found in the colorec-tum (35). MUC2 is associated predominantly with normalintestinal goblet cells and is highly expressed in colon andgastric tumors (36). MUC2 is also a specific marker for IM inBE (35,37,38). We observed MUC2 positive cells in BE-likelesions but not in normal appearing tissue or in tissue dis-playing esophagitis. Because MUC2 expression is a markerfor goblet cells in human BE (35,37,38), our study indicatesthat a DOC+Zn− diet induces the development of intestinal-like columnar epithelium containing goblet cells, a BE-likelesion in mice.
We assessed the proliferative responses of mouse tissuesby evaluating PCNA immunoreactivity. PCNA is a proteinsynthesized in early G1 and S phases of the cell cycle. Itplays an essential role in cell cycle progression, DNA repli-cation, and DNA repair (20). PCNA staining was increasedin mice fed a DOC+Zn− diet, indicating that cell prolifera-tion increased during progression from normal squamous toesophagitis to the BE-like lesion. These results are consistentwith findings in surgical animal models (21). Also, PCNA ex-pression in BE-like lesions in our mouse model was similar tothe expression pattern in patient BE tissues that we evaluatedby Ki-67 immunoreactivity, another marker of proliferation(39).
Accumulating evidence indicates that oxidative stressplays a key role in the pathogenesis of reflux esophagitis,BE, and EAC (40). Oxidative injury is increased, and an-tioxidant capacity is suppressed in the esophageal mucosaduring chronic gastroesophageal reflux (41). Formation of8-OH-dG is an indicator of oxidative DNA damage. Our di-etary model showed increased 8-OH-dG immunoreactivityin BE-like lesions. This result is consistent with our find-ings in patients with BE that levels of 8-OH-dG are in-creased in BE tissue compared to normal squamous tissue(42).
The powerful oxidant peroxynitrite anion is formedwhen the superoxide anion is scavenged by nitric oxide.Peroxynitrite can amplify the inflammatory process (43).Nitrotyrosine, resulting from the reaction of peroxynitritewith tyrosine, serves as a footprint of peroxynitrite (44,45).Nitrotyrosine staining can be used as an indirect measureof peroxynitrite formation in vivo (46). In a surgical ratmodel for EAC, increased nitrotyrosine staining was found,suggesting that peroxynitrite generation may contribute toesophageal carcinogenesis (44). We investigated nitrotyro-sine formation in our dietary model and found intense nitroty-rosine staining in BE-like lesions in mice fed the DOC+Zn−diet. Our findings are consistent with those reported in anexperimental model of esophagitis where peroxynitrite for-mation was a common event in the presence of excess ofsuperoxide anion radicals (43).
NF-κB is a ubiquitous transcription factor that is acti-vated in response to a variety of pathogenic stimuli includingendotoxins, oxidative and nitrosative stresses, and proinflam-matory cytokines (47). NF-κB is a dimer, which consists of
p50 and p65 subunits. NF-κB is normally sequestered inthe cytoplasm by the inhibitory molecule IkB (48). Phos-phorylation of the p65 subunit, or phosphorylation of IkBand its subsequent degradation, leads to translocation of NF-κB from the cytoplasm to the nucleus and activation of theDNA binding activity of NF-κB (48). NF-κB subsequentlyupregulates the transcription of proinflammatory genes andgenes involved in cell growth, proliferation, apoptosis, an-giogenesis, and metastasis (49). Increased levels of NF-κBactivation have been found in a number of tumors includingEAC (49). NF-κB is translocated to the nucleus in Barrett’smucosa, probably as a consequence of the inflammation ofthis mucosa resulting from GERD. We found infiltration ofinflammatory cells in esophagitis tissue and BE-like lesionsfrom mice that were fed the DOC+Zn− diet. Nuclear translo-cation of NF-κB occurred in esophagitis tissue and BE-likelesions from mice fed the zinc-deficient diet supplementedwith DOC. Our study demonstrates that zinc deficiency incombination with DOC may play a role in activating NF-κBDNA-binding activity, which may, in turn, contribute to thedevelopment of BE.
β-Catenin is an important regulator in the cadherin-mediated cell adhesion system. Nuclear β-catenin expres-sion has been associated with cellular transformation and tu-mor invasion and metastasis in many cancers including EAC(50–52). β-catenin contributes to carcinogenesis when thereis a disruption in the adenomatous polyposis coli (APC)/β-catenin/T-cell factor signal transduction pathway (53,54). Inour study, all normal squamous epithelium from the con-trol diet group showed uniform membranous β-catenin im-munoreactivity, and no nuclear staining was detected. Nor-mally, β-catenin nuclear translocation is prevented by bind-ing to E-cadherin on the cellular membrane or by the destruc-tion of β-catenin by APC-GSK3 complex formation (53).We found decreased or absent expression of β-catenin in thecellular membrane and an increase in diffuse cytoplasmicstaining in esophagitis tissue and BE-like lesions from micefed the DOC+Zn− diet compared to normal control epithe-lium. Focal nuclear staining for β-catenin was observed insome cells in BE-like lesions.
In conclusion, our mouse model, employing a diet thatmimics inadequate zinc intake and a component associatedwith a high fat diet, DOC, has led to the development ofmurine esophagitis and BE-like lesions. Our dietary animalmodel has many advantages over current surgical animalmodels. Feeding the mice a diet that mimics inadequate in-take of micronutrients, such as zinc, and DOC is a much sim-pler, noninvasive, cost-effective, and less time-consumingmethod than surgical alteration. The striking finding in thisstudy is that these dietary modifications induced gastroe-sophageal changes resembling BE in 5 out of 8 mice (63%)within the period from 88 to 152 days on a DOC+Zn− diet,a significant difference from mice fed a control diet. In ad-dition, in 100% of animals fed with the DOC+Zn− diet,we observed histopathologic changes in areas of the squa-mous epithelium, which included basal cell hyperprolifera-tion, hyperkeratinization, papillae hypertrophy, metaplasia of
Vol. 59, No. 2 225

the esophagus, increased infiltration of inflammatory cells,and increased angiogenesis. The altered tissues expressedbiomarkers for columnar differentiation (MUC2), oxidativestress (8-OH-dG), nitrosative stress (nitrotyrosine), prolifer-ation (PCNA), and activation of the NF-κB p65 subunit andβ-catenin. Proliferation and oxidative stress, along with nu-clear translocation of NF-κB and β-catenin, all appeared tobe enhanced in a manner comparable to the expression patternseen in patient biopsies taken from BE lesions (47,49,53–56).Accordingly, the animal model developed here may prove ad-vantageous for the study of the molecular mechanisms under-lying development of esophagitis and consequently possiblestrategies for preventing progression to BE.
The studies shown herein emphasize the deleteriouseffects of increased hydrophobic bile acids and zincdeficiency, 2 components associated with a Western-style,high-fat, low-micronutrient diet on the esophagus. Theobserved histopathologic lesions of esophagitis, hyperprolif-eration, papillae hypertrophy, angiogenesis, and metaplasticcolumnar epithelium are cellular events on the pathway toneoplasia.
Acknowledgments and Notes
This work was supported by grants from the Arizona Biomedical Re-search Commission Contract ID#0012 and from National Institute of Healthand National Cancer Institute Grant 1 P50 CA95060 Specialized Program ofResearch Excellence (SPORE). Address correspondence to Katerina Dvo-rak, Department of Cell Biology and Anatomy, College of Medicine, Uni-versity of Arizona, Tucson, AZ 85724. Phone: 520-626-3934. FAX: 520-626-2097. E-mail: [email protected].
Submitted 18 January 2007; accepted in final form 31 May 2007.
References
1. Jankowski JA, Harrison RF, Perry I, Balkwill F, and Tselepis, C: Bar-rett’s metaplasia. Lancet 356, 2079–2085, 2000.
2. Falk GW: Barrett’s esophagus. Gastroenterology 122, 1569–1591,2002.
3. Bonino JA and Sharma P: Barrett’s esophagus. Curr Opin Gastroenterol21, 461–465, 2005.
4. Devesa SS, Blot WJ, and Fraumeni JF Jr.: Changing patterns in theincidence of esophageal and gastric carcinoma in the United States.Cancer 83, 2049–2053, 1998.
5. Ozata M, Mergen M, Oktenli C, Aydin A, Sanisoglu SY, et al.: Increasedoxidative stress and hypozincemia in male obesity. Clin Biochem 35,627–631, 2002.
6. Pandolfino JE, El-Serag HB, Zhang Q, Shah N, Ghosh SK, et al.: Obe-sity: a challenge to esophagogastric junction integrity. Gastroenterology130, 639–649, 2006.
7. Oh DS, Hagen JA, Fein M, Bremner CG, Dunst CM, et al.: The im-pact of reflux composition on mucosal injury and esophageal function.J Gastrointest Surg 10, 787–796, 796–797, 2006.
8. Su Y, Chen X, Klein M, Fang M, Wang S, et al.: Phenotype of columnar-lined esophagus in rats with esophagogastroduodenal anastomosis: sim-ilarity to human Barrett’s esophagus. Lab Invest 84, 753–765, 2004.
9. Prasad AS and Kucuk O: Zinc in cancer prevention. Cancer MetastasisRev 21, 291–295, 2002.
10. Maret W and Sandstead HH: Zinc requirements and the risks andbenefits of zinc supplementation. J Trace Elem Med Biol 20, 3–18,2006.
11. Fong LY, Ishii H, Nguyen VT, Vecchione A, Farber JL, et al.: p53deficiency accelerates induction and progression of esophageal andforestomach tumors in zinc-deficient mice. Cancer Res 63, 186–195,2003.
12. Fong LY, Mancini R, Nakagawa H, Rustgi AK, and Huebner K: Com-bined cyclin D1 overexpression and zinc deficiency disrupts cell cycleand accelerates mouse forestomach carcinogenesis. Cancer Res 63,4244–4252, 2003.
13. Webb JL: Nutritional effects of oral contraceptive use: a review.J Reprod Med 25, 150–156, 1980.
14. Golik A, Zaidenstein R, Dishi V, Blatt A, Cohen N, et al.: Effects ofcaptopril and enalapril on zinc metabolism in hypertensive patients.J Am Coll Nutr 17, 75–78, 1998.
15. Ozutemiz AO, Aydin HH, Isler M, Celik HA, and Batur Y: Effect ofomeprazole on plasma zinc levels after oral zinc administration. IndianJ Gastroenterol 21, 216–218, 2002.
16. Reyes AJ, Olhaberry JV, Leary WP, Lockett CJ, and van der Byl K:Urinary zinc excretion, diuretics, zinc deficiency and some side-effectsof diuretics. S Afr Med J 64, 936–941, 1983.
17. Kauer WK, Peters JH, DeMeester TR, Feussner H, Ireland AP, et al.:Composition and concentration of bile acid reflux into the esophagus ofpatients with gastroesophageal reflux disease. Surgery 122, 874–878,1997.
18. Theisen J, Nehra D, Citron D, Johansson J, Hagen JA, et al.: Suppres-sion of gastric acid secretion in patients with gastroesophageal refluxdisease results in gastric bacterial overgrowth and deconjugation of bileacids. J Gastrointest Surg 4, 50–54, 2000.
19. Nehra D, Howell P, Williams CP, Pye JK, and Beynon J: Toxic bileacids in gastro-oesophageal reflux disease: influence of gastric acidity.Gut 44, 598–602, 1999.
20. Kelman Z: PCNA: structure, functions and interactions. Oncogene 14,629–640, 1997.
21. Li Y, Wo JM, Su RR, Ray MB, Jones W, et al.: Esophageal injury withexternal esophageal perfusion. J Surg Res 129, 107–113, 2005.
22. Lagergren J, Bergstrom R, Lindgren A, and Nyren O: Symptomaticgastroesophageal reflux as a risk factor for esophageal adenocarcinoma.N Engl J Med 340, 825–831, 1999.
23. Cameron AJ: Epidemiology of columnar-lined esophagus and adeno-carcinoma. Gastroenterol Clin North Am 26, 487–494, 1997.
24. Bernstein H, Bernstein C, Payne CM, Dvorakova K, and Garewal H:Bile acids as carcinogens in human gastrointestinal cancers. Mutat Res589, 47–65, 2005.
25. Bernstein C, Bernstein H, Garewal H, Dinning P, Jabi R, et al.: Abile acid-induced apoptosis assay for colon cancer risk and associatedquality control studies. Cancer Res 59, 2353–2357, 1999.
26. Dixon MF, Neville PM, Mapstone NP, Moayyedi P, and Axon AT: Bilereflux gastritis and Barrett’s oesophagus: further evidence of a role forduodenogastro-oesophageal reflux? Gut 49, 359–363, 2001.
27. Olliver JR, Hardie LJ, Gong Y, Dexter S, Chalmers D, et al.: Riskfactors, DNA damage, and disease progression in Barrett’s esophagus.Cancer Epidemiol Biomarkers Prev 14, 620–625, 2005.
28. Payne CM, Crowley-Weber CL, Dvorak K, Bernstein C, Bernstein H,et al.: Mitochondrial perturbation attenuates bile acid-induced cytotox-icity. Cell Biol Toxicol 21, 215–231, 2005.
29. Souza RF, Shewmake K, Terada LS, and Spechler SJ: Acid exposureactivates the mitogen-activated protein kinase pathways in Barrett’sesophagus. Gastroenterology 122, 299–307, 2002.
30. Kaur BS and Triadafilopoulos G: Acid- and bile-induced PGE(2) re-lease and hyperproliferation in Barrett’s esophagus are COX-2 andPKC-epsilon dependent. Am J Physiol Gastrointest Liver Physiol 283,G327–334, 2002.
31. Duggan SP, Gallagher WM, Fox EJ, Abdel-Latif MM, Reynolds JV,et al.: Low pH induces co-ordinate regulation of gene expression inoesophageal cells. Carcinogenesis 27, 319–327, 2006.
32. Ho E and Ames BN: Low intracellular zinc induces oxidative DNAdamage, disrupts p53, NFkappa B, and AP1 DNA binding, and affectsDNA repair in a rat glioma cell line. Proc Natl Acad Sci USA 99,16770–16775, 2002.
226 Nutrition and Cancer 2007

33. Sandstead HH: Understanding zinc: recent observations and interpre-tations. J Lab Clin Med 124, 322–327, 1994.
34. Chen H, Tucker KL, Graubard BI, Heineman EF, Markin RS, et al.: Nu-trient intakes and adenocarcinoma of the esophagus and distal stomach.Nutr Cancer 42, 33–40, 2002.
35. Steininger H, Pfofe DA, Muller H, Haag-Sunjic G, and Fratianu V:Expression of CDX2 and MUC2 in Barrett’s mucosa. Pathol Res Pract201, 573–577, 2005.
36. Carrato C, Balague C, de Bolos C, Gonzalez E, Gambus G, et al.:Differential apomucin expression in normal and neoplastic human gas-trointestinal tissues. Gastroenterology 107, 160–172, 1994.
37. Van De Bovenkamp JH, Korteland-Van Male AM, Warson C, BullerHA, Einerhand AW, et al.: Gastric-type mucin and TFF-peptide expres-sion in Barrett’s oesophagus is disturbed during increased expressionof MUC2. Histopathology 42, 555–565, 2003.
38. Ishizuka I, Andoh A, Koyama S, Moritani S, Kushima R, et al.: Im-munohistochemical analysis of short-segment Barrett’s esophagus. JGastroenterol Hepatol 19, 1410–1416, 2004.
39. Dvorak K, Ramsey L, Payne CM, Sampliner R, Fass R, et al.: Abnormalexpression of biomarkers in incompletely ablated Barrett’s esophagus.Ann Surg 244, 1031–1036, 2006.
40. Farhadi A, Fields J, Banan A, and Keshavarzian A: Reactive oxy-gen species: are they involved in the pathogenesis of GERD, Barrett’sesophagus, and the latter’s progression toward esophageal cancer? AmJ Gastroenterol 97, 22–26, 2002.
41. Oh TY, Lee JS, Ahn BO, Cho H, Kim WB, et al.: Oxidative dam-ages are critical in pathogenesis of reflux esophagitis: implication ofantioxidants in its treatment. Free Radic Biol Med 30, 905–915, 2001.
42. Dvorak K, Payne CM, Chavarria M, Ramsey L, Dvorakova B, et al.: Bileacids in combination with low pH induce oxidative stress and oxidativeDNA damage: relevance to the pathogenesis of Barrett’s oesophagus.Gut 5, 763–771, 2006.
43. Beckman JS: Oxidative damage and tyrosine nitration from peroxyni-trite. Chem Res Toxicol 9, 836–844, 1996.
44. Bae JD, Jung KH, Ahn WS, Bae SH, and Jang TJ: Expression ofinducible nitric oxide synthase is increased in rat Barrett’s esophagusinduced by duodenal contents reflux. J Korean Med Sci 20, 56–60,2005.
45. Jimenez P, Piazuelo E, Sanchez MT, Ortego J, Soteras F, et al.: Freeradicals and antioxidant systems in reflux esophagitis and Barrett’sesophagus. World J Gastroenterol 11, 2697–2703, 2005.
46. Lanas A, Soteras F, Jimenez P, Fiteni I, Piazuelo E, et al.: Superoxideanion and nitric oxide in high-grade esophagitis induced by acid andpepsin in rabbits. Dig Dis Sci 46, 2733–2743, 2001.
47. Konturek PC, Nikiforuk A, Kania J, Raithel M, Hahn EG, et al.: Ac-tivation of NFkappaB represents the central event in the neoplasticprogression associated with Barrett’s esophagus: a possible link to theinflammation and overexpression of COX-2, PPARgamma and growthfactors. Dig Dis Sci 49, 1075–1083, 2004.
48. Baldwin AS Jr.: The NF-kappa B and I kappa B proteins: new discov-eries and insights. Annu Rev Immunol 14, 649–683, 1996.
49. Abdel-Latif MM, O’Riordan J, Windle HJ, Carton E, Ravi N, et al.:NF-kappaB activation in esophageal adenocarcinoma: relationship toBarrett’s metaplasia, survival, and response to neoadjuvant chemora-diotherapy. Ann Surg 239, 491–500, 2004.
50. Takayama T, Shiozaki H, Shibamoto S, Oka H, Kimura Y, et al.:Beta-catenin expression in human cancers. Am J Pathol 148, 39–46,1996.
51. Bailey T, Biddlestone L, Shepherd N, Barr H, Warner P, et al.: Alteredcadherin and catenin complexes in the Barrett’s esophagus-dysplasia-adenocarcinoma sequence: correlation with disease progression anddedifferentiation. Am J Pathol 152, 135–144, 1998.
52. Kimura Y, Shiozaki H, Doki Y, Yamamoto M, Utsunomiya T, et al.:Cytoplasmic beta-catenin in esophageal cancers. Int J Cancer 84, 174–178, 1999.
53. Bian YS, Osterheld MC, Bosman FT, Fontolliet C, and Benhattar J:Nuclear accumulation of beta-catenin is a common and early eventduring neoplastic progression of Barrett esophagus. Am J Clin Pathol114, 583–590, 2000.
54. Osterheld MC, Bian YS, Bosman FT, Benhattar J, and Fontolliet C:Beta-catenin expression and its association with prognostic factors inadenocarcinoma developed in Barrett esophagus. Am J Clin Pathol 117,451–456, 2002.
55. Jenkins GJ, Harries K, Doak SH, Wilmes A, Griffiths AP, et al.: The bileacid deoxycholic acid (DCA) at neutral pH activates NF-{kappa}B andinduces IL-8 expression in oesophageal cells in vitro. Carcinogenesis25, 317–323, 2004.
56. O’Riordan JM, Abdel-latif MM, Ravi N, McNamara D, Byrne PJ,et al.: Proinflammatory cytokine and nuclear factor kappa-B expres-sion along the inflammation-metaplasia-dysplasia-adenocarcinoma se-quence in the esophagus. Am J Gastroenterol 100, 1257–1264,2005.
Vol. 59, No. 2 227