Embed Size (px)
Citation preview

ORIGINAL ARTICLE
A novel germline SDHB mutation in a gastrointestinal stromaltumor patient without bona fide features of the Carney–Stratakisdyad
Ricardo Celestino • Jorge Lima • Alexandra Faustino •
Valdemar Maximo • Antonio Gouveia •
Joao Vinagre • Paula Soares • Jose Manuel Lopes
Published online: 10 December 2011
� Springer Science+Business Media B.V. 2011
Abstract Gastrointestinal stromal tumors (GISTs) are the
most common mesenchyme neoplasms of the gastrointes-
tinal tract. Gain-of-function somatic mutations of the KIT
or PDGFRA genes represent the most prevalent molecular
alterations in GISTs. In Carney–Stratakis dyad, patients
portray germline mutations of the succinate dehydrogenase
subunits B (SDHB), C (SDHC) and D (SDHD) and develop
multifocal GISTs and multicentric paragangliomas (PGLs).
We herein report a novel germline SDHB mutation
(c.T282A—Ile44Asn) occurring in a 26 years-old patient
diagnosed with a spindle cell intermediate risk GIST that
did not present KIT/PDGFRA/BRAF gene mutations. Fur-
ther analyses revealed loss of the wild-type SDHB allele
and complete loss of SDHB expression in the tumor tissue.
After genetic screening of other family members, we
detected in the patient0s mother a SDHB mutation without
any clinical/laboratorial evidence of GIST or PGL. Alto-
gether, our findings (germline SDHB mutation with
absence of PGL in the index case and of GIST and/or PGL
in his mother) raise the possibility that this familiar setting
corresponds to an incomplete phenotype of the Carney–
Stratakis dyad.
Keywords Gastrointestinal stromal tumor � SDH �Carney–Stratakis dyad
Introduction
Gastrointestinal stromal tumors (GISTs) are the most
common mesenchyme neoplasms of the gastrointestinal
tract [1]. The tumor cells of GISTs are morphologically
and immunohistochemically similar to the interstitial
cells of Cajal (ICCs) [2, 3], consistent with a common
origin from ICCs stem cells or a ICCs phenotype
differentiation.
While GISTs may display unique clinical and pathologic
features, they usually share genetic alterations. Somatic
gain-of-function mutations of v-kit Hardy–Zuckerman 4
feline sarcoma viral oncogene homolog (KIT) or of plate-
let-derived growth factor receptor, alpha polypeptide
(PDGFRA) genes are the most prevalent molecular alter-
ations occurring in GISTs [2, 4, 5]. So far, KIT and
PDGFRA mutations were reported to be mutually exclu-
sive [4]. KIT mutations occur in 41–92% of GISTs [6–11],
and albeit they do not induce KIT overexpression, they
cause constitutional activation of this receptor tyrosine
kinase pathway [12]. KIT expression is reported in [95%
of GISTs, including tumors with wild-type KIT and most of
PDGFRA-mutated GISTs [13].
R. Celestino � J. Lima � A. Faustino � V. Maximo � J. Vinagre �P. Soares (&) � J. M. Lopes
Institute of Molecular Pathology and Immunology
of the University of Porto (IPATIMUP), Rua Dr. Roberto Frias
s/n, 4200-465 Porto, Portugal
e-mail: [email protected]
R. Celestino � J. Vinagre
Institute of Biomedical Sciences Abel Salazar of the University
of Porto (ICBAS), 4099-003 Porto, Portugal
R. Celestino � J. Lima � V. Maximo � A. Gouveia � J. Vinagre �P. Soares � J. M. Lopes
Medical Faculty, University of Porto, 4200-319 Porto, Portugal
A. Gouveia
Department of Surgery, Hospital Sao Joao,
4200-319 Porto, Portugal
J. M. Lopes
Department of Pathology, Hospital Sao Joao,
4200-319 Porto, Portugal
123
Familial Cancer (2012) 11:189–194
DOI 10.1007/s10689-011-9499-x

GISTs occur as sporadically in 90% of the patients,
whereas in the remaining 10% they are familiar or part of
syndromes, including autosomal-dominant inheritance
pattern hereditary conditions. Germline mutations in KIT
and PDGFRA have been described in a few families pre-
senting multifocal GIST. GIST can also be part of the
tumor spectrum of the Carney triad (paragangliomas,
GISTs and pulmonary chondromas) [14], Carney–Stratakis
dyad (paragangliomas and GISTs) [15] and in the Neuro-
fibromatosis type I (neurofibromas, GIST and other lesions)
[16].
Concerning therapy, GISTs represents one of the most
successful examples of therapy with tyrosine kinase
inhibitors (TKI). The TKI Imatinib mesylate (STI571) is
a first line palliative therapy for advanced GIST, with
great efficiency in patients harboring KIT or PDGFRA
tumor somatic mutations [17]. Nevertheless, not all
GISTs harbor the same genetic status, and that a subset
of patients/tumors may not respond (primary resistance),
develop resistance (secondary resistance) or intolerance
to Imatinib mesylate therapy. Sunitinib was approved as
an alternative TKI, for the treatment of patients with
resistance or intolerance to Imatinib [18]. The patho-
genesis of resistance and/or intolerance reinforces the
concept that other molecular events, other than KIT
or PDGFRA mutations, may be implicated in GIST
tumorigenesis. Noteworthy, the BRAFV600E somatic
mutation was reported in 3–7% of KIT/PDGFRA wild-
type GISTs [19–21]. BRAFV600E mutations were reported
in KIT-mutated GISTs [22], as well as in one patient
with secondary Imatinib resistance without detectable
secondary mutations in KIT/PDGFRA [20]. Furthermore,
somatic mutations in the caspase-4 gene (CASP4) were
reported, with the CASP4L365V mutation being detected
in 18% of GISTs (wild-type and KIT/PDGFRA-mutated),
but without significant association with clinicopatholog-
ical features [23].
In the recently reported Carney–Stratakis dyad, where
patients develop multifocal GISTs and multicentric para-
gangliomas (PGL) [15, 24], molecular studies disclosed
the presence of germline mutations of the succinate
dehydrogenase subunits B (SDHB), C (SDHC) and D
(SDHD); GISTs occurring in these patients do not harbor
KIT or PDGFRA mutations [25]. Germline mutations of
the SDHB, SDHC and SDHD had been previously
reported in inherited PGL and pheochromocytoma (PCC)
[26–30], but not in familiar GISTs, until they were
described in patients with the Carney–Stratakis dyad [25,
31].
In this study we report a novel germline SDHB mutation
occurring in an otherwise unrecognized familial condition,
in which the index case presents a GIST without other
features of the Carney–Stratakis dyad.
Materials and methods
Case presentation
A 26 years-old man was admitted with a 3 days history of
melena, asthenia and no hematemesis. The patient had no
significant previous medical history, was on no regular
medication and did not report any familial history of gastric
malignancy. Clinical examination was unremarkable
except for paleness and a tachycardia of 110 bpm. Blood
tests showed an hemoglobin level of 5.6 g/dl with normal
urea and electrolytes, normal liver function and clotting
tests. An esophagogastroduodenoscopy revealed a polypoid
submucosal tumor in the lesser curvature of the distal
antrum, covered by normal mucosa with an ulcer on top of
the tumor. While he was stable, he received a total of 4
units of packed red blood cells. Endoscopic biopsy was
negative for tumoral cells and an endo-ultrasonography
(EUS) disclosed a hypoechoeic, homogeneous and well
circumscribed lesion, located in the 4th layer of gastric
wall. The staging work up (EUS; abdomino-pelvic con-
trast-enhanced computed tomography/CT; thoracic X-ray)
did not disclose any signs of distant disease.
A laparotomy on day 12 confirmed a large mass in the
pre-pyloric region, and a distal gastric resection with pri-
mary end-to-end gastro-duodenal anastomoses (Bilroth I)
was performed. The patient had an uneventful recovery
with no further bleeding.
The histopathology study depicted a spindle cell inter-
mediate risk GIST: 4.5 cm largest size, and a mitotic count
of 16/50 HPF. In the immunohistochemistry study, the
tumor cells displayed diffuse expression of CD117 and
CD34 in the absence of keratins, actin and S100 protein
expression. The resection margins were negative for tumor
cells (R0). The molecular analysis disclosed absence of
KIT/PDGFRA/BRAF gene mutations and the presence of a
SDHB germline mutation (see below). Then, a cervical-
thoracic-abdominal-pelvic CT scan (body CT) was per-
formed, and did not disclose any lesion suggestive of PGL.
Furthermore, 123I-metaiodobenzylguanidine (MIBG)
scintigraphy was also negative, as were the urine meta-
nephrines test (two measurements of 24 h urinary meta-
nephrine and normetanephrine). At last follow-up, 99
months after resection, the patient does not show any
evidence of recurrent disease.
Mutation screening
DNA was extracted from 10 lm paraffin-embedded sec-
tions of tumor tissue and corresponding adjacent no-tumor
tissue. Slides were microscopically examined, and tumor
areas were marked and carefully dissected under micro-
scopic observation. Dissected material was deparaffinized
190 R. Celestino et al.
123

in xylene, washed in ethanol, and rehydrated. DNA
extraction was performed using the Genomic DNA Puri-
fication Kit (Citomed, Lisbon, Portugal) according to the
manufacturer’s protocol. Germline DNA was extracted
from peripheral blood lymphocytes by the standard pro-
teinase K-SDS digestion and saline precipitation [32].
The presence of SDHB, SDHC and SDHD mutations
was evaluated by PCR and DNA sequencing was per-
formed as previously described by Lima et al. [33]. The
presence of mutations was validated by a second PCR
followed by direct sequencing.
Multiplex ligation-dependent probe amplification
(MLPA)
Germline and tumor DNA were analyzed for intragenic
deletions using multiplex-ligation dependent probe ampli-
fication (MLPA) assay (SALSA MLPA KIT, P226SDHD,
MRC-Holland b. v., Amsterdam, the Netherlands), accord-
ing to the manufacturer’s instructions. MLPA fragments
were discriminated in an ABI PRISM 310 Genetic Analyzer
(Applied Biosystem), and the resulting data was analyzed
using Coffalyser software (MRC Holland, Amsterdam, The
Netherlands). All MLPA results were reproduced at least
three times.
Immunohistochemistry for SDHA and SDHB proteins
Tissue sections with 2 lm thickness were deparaffinized,
rehydrated and pre-treated with 1xEpitope Retrieval Solu-
tion pH 9 (Tris/EDTA-based buffer containing surfactant)
(E7119; Leica Microsystems, Newcastle Upon Tyne,
United Kingdom) in a 98�C water bath during 20 min.
Immunohistochemical staining was performed with the
Envision G/2 System/AP (K5355; Dako, Glostrup, Den-
mark), according to the manufacturer’s instructions. The
tissue sections were incubated at 4�C overnight with SDHB
primary antibody (Complex II subunit 30 kDaIp mono-
clonal antibody, mouse, 1:600 dilution; MS203; Mito-
sciences, Eugene, Oregon, USA) and incubated 1 h with
SDHA primary antibody (Complex II subunit 70 kDaFp
monoclonal antibody, mouse, 1:1,250 dilution; MS204;
Mitosciences, Eugene, Ore, USA).
The APAP (alkaline phosphatase anti-phosphatase)
method was used for detection, and the samples were
developed with permanent red chromogen. The slides were
mounted using a water-miscible mounting medium, after
counterstaining with haematoxylin.
Negative and positive controls were used simultaneously to
ensure specificity and reliability of the staining process. Pre-
viously tested positive cases of oncocytic variant of papillary
thyroid carcinoma were used as positive controls. Omission
of the primary antibody was used as negative control.
Immunohistochemistry evaluation (positive/negative) was
performed independently by two observers (J.M.L. and V.M.).
Results
Our patient presented a KIT and PDGRFA wild-type GIST
without any known family history of GIST, PGL or PCC.
After sequencing the SDHB, SDHC and SDHD genes, we
identified a previously unreported germline point mutation
in the SDHB gene (c.T282A) in the genomic DNA of the
tumor, in non-tumor tissue as well as in the peripheral
blood of the patient. This mutation leads to the substitution
of an Isoleucine for an Asparagine at residue 44
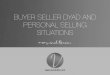
(p.Ile44Asn) (Fig. 1), which is a highly conserved residue
across eukaryotes. Analysis of 174 chromosomes from
healthy blood donors, revealed that the SDHB p.Ile44Asn
mutation was absent in the samples tested.
The sequencing electropherogram disclosed that the
mutation was heterozygous in the blood and in non-tumor
tissue, whereas only the mutant allele was present in the
GIST tumor cells (Fig. 1), suggesting loss of heterozy-
gosity (LOH) of the normal allele in the tumor. This result
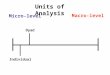
was further supported by MLPA analysis, which is con-
sistent with loss of the whole wild-type allele of SDHB
gene in tumor tissue (Fig. 2). MLPA analysis disclosed the
presence of both alleles in the non-tumor tissue and in the
peripheral blood of the patient.
Upon immunohistochemistry analysis, we observed
SDHA and SDHB protein expression in the patient’s nor-
mal gastric mucosa (Fig. 1); conversely, the SDHB-muta-
ted GIST showed complete loss of SDHB expression, while
retaining SDHA protein expression.
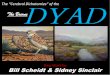
All patient’s first degree relatives (mother, 56 years-old;
father, 60 years-old; and the twin sisters, 31 years-old)
(Fig. 3) were tested for the SDHB p.Ile44Asn mutation in
DNA extracted from the peripheral blood. Only the patient’s
mother presented the p.Ile44Asn germline SDHB mutation,
but the subsequent clinical evaluation—a cervical-thoracic-
abdominal-pelvic CT scan and a 123I-metaiodobenzylgua-
nidine [MIBG] scintigraphy, as well as the 24 h urinary
metanephrines–showed no evidence of GIST and/or PGL, or
of any other lesion.
Discussion
In our study, we describe a novel germline SDHB mutation
occurring in a patient with an apparently sporadic GIST (no
known personal or family evidence of GIST, PGL or PCC)
without KIT or PDGFRA somatic mutations. Additionally,
the tumor tissue presented LOH of the wild-type SDHB
allele, consistent with the common two ‘‘hit’’ tumor-suppressor
A novel SDHB germline mutation in GIST 191
123

inactivation model. The SDHB p.Ile44Asn germline muta-
tion was also present in the patient’s mother, who, at last
follow-up is well and without evidence of disease. Our
results indicate that we are in face of a Carney–Stratakis dyad
with an incomplete penetrance as previously reported for
most SDHB germline mutations [33].
Carney–Stratakis dyad is a familial condition with an
autosomal dominant inheritance pattern with incomplete
penetrance, in which the development of GIST is associ-
ated with PGL [24, 25, 31]. Patients with Carney–Stratakis
dyad present germline mutations in SDHB, SDHC or
SDHD gene and do not harbor somatic or germline muta-
tions of KIT or PDGFR. The Carney triad is another con-
dition comprising GIST, PGL and pulmonary chondroma,
and without apparent familial history [14, 34]; the majority
of patients develop GIST and pulmonary chondromas [14]
Fig. 1 SDHA and SDHB immunoexpression and SDHB sequencing
results of the normal gastric mucosa (upper panel) and GIST tissue
(lower panel). Note the loss of SDHB immunoexpression in the GIST
tissue. Both electropherograms are evidencing the SDHB c.T282A
substitution in normal gastric mucosa and GIST, with loss of the wild-
type allele in the tumor. The mutated residue is indicated by an arrow.
Original magnification of images: 9200
Fig. 2 MLPA quantification of each SDHB exon in genomic DNA
extracted from the patient’s tumor tissue, normal gastric tissue and
peripheral blood; all SDHB exons show loss of DNA material in
tumor tissue when compared with normal tissue and peripheral blood.
Data was normalized using 5 genomic DNA control samples isolated
from normal human tissue. The bars represent the average of 3
experimental replicas
Fig. 3 Pedigree of the family with SDHB-mutated GIST
192 R. Celestino et al.
123

and so far no somatic or germline KIT/PDGFRA, SDHB,
SDHC and SDHD mutations have been detected in the
Carney triad [35, 36].
The case herein reported does not completely fit with a
Carney–Stratakis dyad, because there is neither evidence of
PGL in the patient nor in the mother who also carries the
mutation. It is possible that the absence of tumors in the
index patient mother may indicate an incomplete pene-
trance or a higher susceptibility of males to develop partial
(only GIST) features of the Carney–Stratakis dyad. Our
case fits with those recently described by Janeway et al.,
who identified germline mutations in SDHB and SDHC in
12% of patients with apparently sporadic GIST (no known
personal or family history of PGL) which also did not
disclosed KIT or PDGFRA somatic mutations [37]. Whe-
ther our case and those reported by Janeway et al. are cases
of the Carney–Stratakis dyad with reduced penetrance and/
or expressivity of the disease, or represent a new hereditary
GIST syndrome remains to be ascertained.
It was recently reported that the immunohistochemical
expression of SDHB strongly correlates with the genetic
status of SDH genes [38]: cases without germline SDH
mutations display SDHB expression, whereas cases har-
boring germline mutations in any SDH (B, C or D) gene are
consistently negative for SDHB expression [38, 39].
Accordingly, we observed that SDHB expression was
absent in the tumor cells, despite its expression in the
normal, non-tumor tissues of the patient. Ours results
reinforces the pathogenicity of the SDHB p.Ile44Asn
mutation and further supports the use of SDHB immuno-
expression as useful routine test for the identification of
GISTs with germline SDH mutations.
GISTs without KIT/PDGFRA somatic mutations repre-
sent a therapeutic challenge since it is known that they do
not respond well or may be resistant to treatment with
Imatinib [40, 41]. Considering the recent reports pointing
to SDH defects as an alternative molecular mechanism in
GIST tumorigenesis, therapies targeting SDH-induced
pathways might be considered in the medical decision of
Imatinib-resistant GISTs. Several promising drugs are
under trial evaluation, such as HIF1-a inhibitors and
derivatives of a-ketoglutarate or dichloroacetate (DCA).
In summary, we report a GIST patient without KIT/
PDGFR somatic mutations, who harbors a previously
unreported germline SDHB mutation. The absence of PGL
in the patient as well as the absence of GIST and/or PGL in
his mother (who carries the mutation) raises the possibility
that our case may represent an incomplete phenotype of the
Carney–Stratakis dyad or a distinct entity.
Acknowledgments This study was supported by Fundacao Calouste
Gulbenkian through a PhD grant to R.C.; by Fundacao para a Ciencia
e Tecnologia through the program Ciencia 2007 (V.M.) and 2008
(J.L.) and Novartis through a project grant. IPATIMUP is an Asso-
ciate Laboratory of the Portuguese Ministry of Science, Technology
and Higher Education that is partially supported by the FCT.
References
1. Fletcher CD, Berman JJ, Corless C et al (2002) Diagnosis of
gastrointestinal stromal tumors: a consensus approach. Hum
Pathol 33(5):459–465
2. Hirota S, Isozaki K, Moriyama Y et al (1998) Gain-of-function
mutations of c-kit in human gastrointestinal stromal tumors.
Science 279(5350):577–580
3. Kindblom LG, Remotti HE, Aldenborg F, Meis-Kindblom JM
(1998) Gastrointestinal pacemaker cell tumor (GIPACT): gas-
trointestinal stromal tumors show phenotypic characteristics of
the interstitial cells of Cajal. Am J Pathol 152(5):1259–1269
4. Heinrich MC, Corless CL, Duensing A et al (2003) PDGFRA
activating mutations in gastrointestinal stromal tumors. Science
299(5607):708–710
5. Lasota J, Miettinen M (2006) KIT and PDGFRA mutations in
gastrointestinal stromal tumors (GISTs). Semin Diagn Pathol
23(2):91–102
6. Choi YR, Kim H, Kang HJ et al (2003) Overexpression of high
mobility group box 1 in gastrointestinal stromal tumors with KIT
mutation. Cancer Res 63(9):2188–2193
7. Kim NG, Kim JJ, Ahn JY et al (2000) Putative chromosomal
deletions on 9P, 9Q and 22Q occur preferentially in malignant
gastrointestinal stromal tumors. Int J Cancer 85(5):633–638
8. Lasota J, Jasinski M, Sarlomo-Rikala M, Miettinen M (1999)
Mutations in exon 11 of c-kit occur preferentially in malignant
versus benign gastrointestinal stromal tumors and do not occur in
leiomyomas or leiomyosarcomas. Am J Pathol 154(1):53–60
9. Lux ML, Rubin BP, Biase TL et al (2000) KIT extracellular and
kinase domain mutations in gastrointestinal stromal tumors. Am J
Pathol 156(3):791–795
10. Rubin BP, Singer S, Tsao C et al (2001) KIT activation is a
ubiquitous feature of gastrointestinal stromal tumors. Cancer
61(22):8118–8121
11. Taniguchi M, Nishida T, Hirota S et al (1999) Effect of c-kit
mutation on prognosis of gastrointestinal stromal tumors. Cancer
Res 59(17):4297–4300
12. Miettinen M, Lasota J (2006) Gastrointestinal stromal tumors:
pathology and prognosis at different sites. Semin Diagn Pathol
23(2):70–83
13. Lasota J, Miettinen M (2008) Clinical significance of oncogenic
KIT and PDGFRA mutations in gastrointestinal stromal tumours.
Histopathology 53(3):245–266
14. Carney JA (1999) Gastric stromal sarcoma, pulmonary chon-
droma, and extra-adrenal paraganglioma (Carney triad): natural
history, adrenocortical component, and possible familial occur-
rence. Mayo Clin Proc 74(6):543–552
15. Daum O, Vanecek T, Sima R, Michal M (2006) Gastrointestinal
stromal tumor: update. Klin Onkol 19(4):203–211
16. Rubin BP (2006) Gastrointestinal stromal tumours: an update.
Histopathology 48(1):83–96
17. Demetri GD, von Mehren M, Blanke CD et al (2002) Efficacy
and safety of imatinib mesylate in advanced gastrointestinal
stromal tumors. N Engl J Med 347(7):472–480
18. Demetri GD, van Oosterom AT, Garrett CR et al (2006) Efficacy
and safety of sunitinib in patients with advanced gastrointestinal
stromal tumour after failure of imatinib: a randomised controlled
trial. Lancet 368(9544):1329–1338
19. Agaimy A, Terracciano LM, Dirnhofer S et al (2009) V600E
BRAF mutations are alternative early molecular events in a
A novel SDHB germline mutation in GIST 193
123

subset of KIT/PDGFRA wild-type gastrointestinal stromal
tumours. J Clin Pathol 62(7):613–616
20. Agaram NP, Wong GC, Guo T et al (2008) Novel V600E BRAF
mutations in imatinib-naive and imatinib-resistant gastrointestinal
stromal tumors. Genes Chromosomes Cancer 47(10):853–859
21. Martinho O, Gouveia A, Viana-Pereira M et al (2009) Low fre-
quency of MAP kinase pathway alterations in KIT and PDGFRA
wild-type GISTs. Histopathology 55(1):53–62
22. Agaimy A, Markl B, Arnholdt H et al (2009) Multiple sporadic
gastrointestinal stromal tumours arising at different gastrointestinal
sites: pattern of involvement of the muscularis propria as a clue to
independent primary GISTs. Virchows Arch 455(2):101–108
23. Kim YR, Kim KM, Yoo NJ, Lee SH (2009) Mutational analysis
of CASP1, 2, 3, 4, 5, 6, 7, 8, 9, 10, and 14 genes in gastroin-
testinal stromal tumors. Hum Pathol 40(6):868–871
24. Carney JA, Stratakis CA (2002) Familial paraganglioma and
gastric stromal sarcoma: a new syndrome distinct from the Car-
ney triad. Am J Med Genet 108(2):132–139
25. McWhinney SR, Pasini B, Stratakis CA (2007) Familial gastro-
intestinal stromal tumors and germ-line mutations. N Engl J Med
357(10):1054–1056
26. Amar L, Bertherat J, Baudin E et al (2005) Genetic testing in
pheochromocytoma or functional paraganglioma. J Clin Oncol
23(34):8812–8818
27. Bolland M, Benn D, Croxson M et al (2006) Gastrointestinal
stromal tumour in succinate dehydrogenase subunit B mutation-
associated familial phaeochromocytoma/paraganglioma. ANZ J
Surg 76(8):763–764
28. Brouwers FM, Eisenhofer G, Tao JJ et al (2006) High frequency
of SDHB germline mutations in patients with malignant cate-
cholamine-producing paragangliomas: implications for genetic
testing. J Clin Endocrinol Metab 91(11):4505–4509
29. Neumann HP, Pawlu C, Peczkowska M et al (2004) Distinct
clinical features of paraganglioma syndromes associated with
SDHB and SDHD gene mutations. JAMA 292(8):943–951
30. Schiavi F, Boedeker CC, Bausch B et al (2005) Predictors and
prevalence of paraganglioma syndrome associated with mutations
of the SDHC gene. JAMA 294(16):2057–2063
31. Pasini B, McWhinney SR, Bei T et al (2008) Clinical and
molecular genetics of patients with the Carney-Stratakis syn-
drome and germline mutations of the genes coding for the suc-
cinate dehydrogenase subunits SDHB, SDHC, and SDHD. Eur J
Hum Genet 16(1):79–88
32. Miller SA, Dykes DD, Polesky HF (1988) A simple salting out
procedure for extracting DNA from human nucleated cells.
Nucleic Acids Res 16(3):1215
33. Lima J, Feijao T, Ferreira da Silva A et al (2007) High frequency of
germline succinate dehydrogenase mutations in sporadic cervical
paragangliomas in northern Spain: mitochondrial succinate dehy-
drogenase structure-function relationships and clinical-pathologi-
cal correlations. J Clin Endocrinol Metab 92(12):4853–4864
34. Carney JA, Sheps SG, Go VL, Gordon H (1977) The triad of
gastric leiomyosarcoma, functioning extra-adrenal paraganglioma
and pulmonary chondroma. N Engl J Med 296(26):1517–1518
35. Matyakhina L, Bei TA, McWhinney SR et al (2007) Genetics of
carney triad: recurrent losses at chromosome 1 but lack of
germline mutations in genes associated with paragangliomas and
gastrointestinal stromal tumors. J Clin Endocrinol Metab 92(8):
2938–2943
36. Stratakis CA, Carney JA (2009) The triad of paragangliomas,
gastric stromal tumours and pulmonary chondromas (Carney
triad), and the dyad of paragangliomas and gastric stromal sar-
comas (Carney-Stratakis syndrome): molecular genetics and
clinical implications. J Intern Med 266(1):43–52
37. Janeway KA, Kim SY, Lodish M et al (2011) Defects in succinate
dehydrogenase in gastrointestinal stromal tumors lacking KIT and
PDGFRA mutations. Proc Natl Acad Sci USA 108(1):314–318
38. van Nederveen FH, Gaal J, Favier J et al (2009) An immuno-
histochemical procedure to detect patients with paraganglioma
and phaeochromocytoma with germline SDHB, SDHC, or SDHD
gene mutations: a retrospective and prospective analysis. Lancet
Oncol 10(8):764–771
39. Gill AJ, Benn DE, Chou A et al (2010) Immunohistochemistry for
SDHB triages genetic testing of SDHB, SDHC, and SDHD in
paraganglioma-pheochromocytoma syndromes. Hum Pathol 41(6):
805–814
40. Heinrich MC, Owzar K, Corless CL et al (2008) Correlation of
kinase genotype and clinical outcome in the North American
intergroup phase III trial of imatinib mesylate for treatment of
advanced gastrointestinal stromal tumor: CALGB 150105 study
by cancer and leukemia group B and Southwest oncology group.
J Clin Oncol 26(33):5360–5367
41. Janeway KA, Albritton KH, Van Den Abbeele AD et al (2009)
Sunitinib treatment in pediatric patients with advanced GIST
following failure of imatinib. Pediatr Blood Cancer 52(7):
767–771
194 R. Celestino et al.
123