Embed Size (px)
Citation preview

A novel non-estrogenic HRT in postmenopausal women with diabetes:
DHEA supplementation
Bharti Kalra, Sanjay Kalra

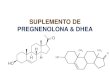
ADRENAL ANDROGEN PHYSIOLOGY cholesterol
zona glomerulosa pregnenolone aldosterone 100 mg/d
zona fasciculata 17-OH pregnenolone cortisol 10mg/d
zona reticularis DHEA androstened- >20mg/d
4mg 1.5mg
DHEAS
7-15mg
estradiolDHT

ACTH cortical androgen stimulating hormone (CASH)
POMC derivatives
joining peptide
prolactin
IGF- 1cortisol DHEA
androstenedione age & gender
related changes
DHEA S
no diurnal variation

AGE RELATED CHANGES
Foetus birth
Puberty peak old ageAdrenarche 20-30gadrenopause
250 to 500 μ g/dl
25 μ g/dl

AIMS AND OBJECTIVES
To assess the incidence of DHEAS deficiency amongst
postmenopausal diabetic women with asthenia
To assess the clinical correlates of DHEAS deficiency .
To assess the effects of DHEA supplementation on
asthenic symptoms in postmenopausal diabetic women.

STUDY DESIGN
Prospective,open-label randomized study over 6 months
Single centre study conducted from Oct 2005 to June
2006.
354 consecutive postmenopausal diabetic women
complaining of asthenia were administered the Energy
Fatigue Scale (Stanford).
Women with positive score ( ≥ 2.20) underwent DHEAS
estimation.

STUDY DESIGN
Women with DHEAS levels below normal or in the lower
quartile of normal range were randomized to either of 2
groups.
Study group given DHEA supplementation
25 mg /day x 6 months along with routine medication;
control given only antidiabetic drugs.

STUDY DESIGN
Clinical and biochemical assessment was
carried out at 3 months and 6 months.
Dose of DHEA was adjusted at 3 months and 6
months according to DHEAS values.
Aim to keep DHEAS values in upper half of
normal range according to age

RESULTS
354 postmenopausal women with diabetes with asthenia.
(diabetes 1-35 years; asthenia 1-24 months)
women with AADS (42.4%)
STUDY GROUP: 75
DHEA Supplementation
CONTROL GROUP: 75
No DHEA Supplementation

AGE DISTRIBUTION OF PATIENTS
Age Yrs. 31-40 41-50 51-60 61-70 71-80 81-90
Study group
1
(1.3%)
27
(35.52)
32
(42.10%)
6
(7.89%)
5
(6.57%)
5
(6.57%)
Control group
0
(0%)
32
(42.10%)
26
()
10
()
4
(%)
3
()

AVERAGE DOSE/LEVELS OF DHEA
• The average dose of DHEA required to correct DHEAS
levels was 24.31 ± 10.75 mg at 3 months and 30.40 ±
13.67 mg at 6 months.
• The average level at baseline was 40.86 ± 23.40
μg/ml in the AADS cohort. It rose to 81.39 ± 51.71 μg/ml
at 3 months and 89.53 ± 51.50 μg/ml at 6 months

IMPROVEMENT IN ENERGY SCORE: Study group
0
2
4
6
8
10
12
changein score
3 monthsfollow up
6 monthsfollow up
No. ofsubjects
Drop-out
zero 0.2-0.8
≥ 1.0

CLINICAL CORRELATES OF ASTHENIC PATIENTS
Frequency in Asthenic Patients
(Total=354)
DHEA-S deficient (AADS) patients
(Total =150)
Age > 60 Years* 75
(21.18%)
79
(52.67%)
Sensory neuropathy* 186
(52.54%)
142
(94.66%)
Motor neuropathy* 79
(22.31%)
63
(42.00%)
Albuminuria * 19
(5.4%)
47
(31.33%)
Chronic renal failure*
(se creat >1.5)
14
(3.9%)
24
(16.00%)
Hypothyroidism* 75
(21.18%)
71
(47.33%)
Poor glycemic control *
(HB A1c >8.0%)
158
(44.64%)
95
(63.33%)

SIGNIFICANT CORRELATES
0
10
20
30
40
50
60
70
80
90
100
age senN motN alb CRF thyr poorcontr
asthenia
AADS

CLINICAL CORRELATES OF ASTHENIC PATIENTS
Frequency in Asthenic Patients
(Total=354)
DHEA-S deficient (AADS) patients
(Total =150)
Hypertension 288
(81.35%)
134
(89.33%)
Coronary Heart disease 5
(1.41%)
0
(0%)
Stroke 27
(7.62%)
15
(10. 00%)
Foot Ulcer 9
(2.54%)
0
(0%)
Anemia 130
(36.72%)
71
(47.33%)
Hypoproteinemia 18
(5.08%)
8
(5.33%)
Hepatic Dysfunction 28
(7.91%)
0
(0%)

EFFECTS
• DHEA-S levels rose significantly after supplementation with
oral DHEA .
• Most patients felt the maximum benefit of therapy within 4-6
weeks.
• 16.00% study patients and 4.00% controls reported a
subjective improvement in libido.

SIDE EFFECTS
• One patient each complained of excessive perspiration,
itching, and ‘increased anger’, but there was no drop out.
Symptoms were self-limiting in all patients.
• DHEA-S therapy is not associated with the side effects
of estrogen therapy.

CONCLUSION
Adrenal androgen deficiency
(dehydroepiandrosterone sulfate [DHEAS]
deficiency) is a common cause of asthenia
(42 %) in postmenopausal women with
diabetes

CONCLUSION
DHEA supplementation is effective in
89.33%; and very effective in 76% of
women with documented low or below
average DHEAS.

CONCLUSION
DHEA supplementation is well tolerated by
postmenopausal women with diabetes. It
is not associated with the side effects of
estrogen therapy.

Sunsets are beautiful: our postmenopausal patients need not suffer unnecessarily

Thank you