Embed Size (px)
Citation preview

COMPLIMENTARY ISSUE
Patient Safety Monitor Journal
At any given moment, the intensity level within the ICU at Beth Israel Deaconess Medical Center (BIDMC) in Boston can shift from relatively low to dangerously high. For clinicians, this shift is often instinctual, but difficult to grasp. A flurry of new patients may suddenly require more intensive care, causing the unit to buzz with activity. The intensity level spikes, and the providers naturally respond to the increase.
All ICUs in the country experience these same shifts, where everything from admissions and discharg-es to the experience level of nursing staff can impact the intensity level of the unit. Normally, clinicians are expected to roll with the punches and respond to high-er intensity levels as they emerge, but soon, BIDMC will be able to track, quantify, and even predict those changes using data compiled though a new project called “Risky States.”
Data analytics and systems engineering offer the keys to improved patient careMore hospitals are turning towards data collection and analysis, but experts say data must be trustworthy and actionable
State initiatives improve qualityWe look at collaborative efforts in Maryland and Pennsylvania to improve quality and patient safety.
After the fallTwo health systems share how they successfully reduced patient falls.
Post-fall huddle toolUse this tool to guide your actions after a patient fall occurs.
Q&AJohns Hopkins Hospital researcher Henry Michtalik discusses a recent study about real-time feedback.
P4
P7
P8
Risky States is a project BIDMC developed in partnership with the Massachusetts Institute of Technology (MIT) and Aptima, Inc., with funding from the Gordon and Betty Moore Foundation. The project utilizes previous ICU data to predict when the unit will enter high-intensity periods that could pose a risk to patients. This raw data, which includes admissions, dis-charges, transfers, staffing levels, time of day, and vulner-ability of ICU patients, was entered into an algorithm developed by MIT, which categorizes levels of risk and will eventually be able to predict when ICU patients will be more susceptible to harm.
“There are times when the intensity of the unit heats up and people are working as hard as they can to take care of the patients,” says Patricia Folcarelli, RN, PhD, senior director of patient safety at BIDMC. “All ICUs [within the hospital] will see each other’s
P11

2 HCPRO.COM © 2016 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Complimentary issue
intensity state. Even if you’re on a different floor, you’ll be able to see there are units with a higher level of intensity, and you can make decisions about re-source management or the flow of work for that par-ticular day. Some of the function will be to increase situational awareness about the state of the ICU in a complex system.”
Aptima is currently developing the electronic appli-cation that will be integrated into BIDMC’s ICUs this fall. The app will allow clinicians and patient safety leaders within the hospital to see how patient risk shifts throughout the day and how they can manipu-late staffing levels or environmental factors to reduce that risk.
“Some of the things we’ve learned are things that a lot of clinicians would say is intuitively obvious,” says Ken Sands, MD, chief quality officer at BID-MC. “So the important part is that we can quantify just how much increased risk there is through the
David M. Benjamin, PhDAdjunct Assistant ProfessorDepartment of Pharmacology & Experimental Therapeutics Tufts University School of Medicine Boston, Massachusetts
Steven W. BryantVice President and Managing DirectorAccreditation Services The Greeley Company Danvers, Massachusetts
Sue Dill Calloway, RN, JDDirector of Hospital Risk ManagementOHIC Insurance Company Columbus, Ohio
Wendy Fisher, RNPatient Education CoordinatorA.O. Fox Memorial Hospital Oneonta, New York
Patricia Gilroy, MSN, MBAClinical Patient Safety CoordinatorAlfred I. duPont Hospital for Children Wilmington, Delaware
Gayla J. Jackson, RN, BSNNurse ManagerMount Auburn Hospital Cambridge, Massachusetts
Tim O’KellyRisk ManagerDeaconess Hospital Oklahoma City, Oklahoma.
Patricia Pejakovich, RN, BSN, MPA, CPHQ, CSHASenior ConsultantThe Greeley Company Danvers, Massachusetts
Kenneth R. RohdeConsultantGranby, Connecticut
Mary J. Voutt-Goos, MSN, RN, CCRNDirector, Patient Safety Initiatives, Clinical Care DesignHenry Ford Health System Detroit, Michigan
This document contains privileged, copyrighted information. If you have not purchased it or are not otherwise entitled to it by agreement with HCPro, a division of BLR, any use, disclosure, forwarding, copying, or other communication of the contents is prohibited without permission.
EDITORIAL ADVISORY BOARD
Jay KumarAssociate Product [email protected]
Evan SweeneyContributing Editor
Follow UsFollow and chat with us about all things healthcare compliance, management, and reimbursement. @HCPro_Inc
Patient Safety Monitor Journal (ISSN: 2157-5630 [print]; 2157-5649 [online]) is published monthly by HCPro, a division of BLR®. Subscription rate: $399/year. • Patient Safety Monitor Journal, 100 Winners Circle, Suite 300, Brentwood, TN 37027. • Copyright © 2016 HCPro, a division of BLR. All rights reserved. Printed in the USA. Except where specifically encouraged, no part of this publication may be reproduced, in any form or by any means, without prior written consent of HCPro or the Copyright Clearance Center at 978-750-8400. Please notify us immediately if you have received an unauthorized copy. • For editorial comments or questions, call 781-639-1872 or fax 781-639-7857. For renewal or subscription information, call customer service at 800-650-6787, fax 800-639-8511, or email [email protected]. • Visit our website at www.hcpro.com. • Occasionally, we make our subscriber list available to selected companies/vendors. If you do not wish to be included on this mailing list, please write to the marketing department at the address above. • Opinions expressed are not necessarily those of PSMJ. Mention of products and services does not constitute endorsement. Advice given is general, and readers should consult professional counsel for specific legal, ethical, or clinical questions. PSMJ is not affiliated in any way with The Joint Commission, which owns the JCAHO and Joint Commission trademarks. MAGNET™, MAGNET RECOGNITION PROGRAM®, and ANCC MAGNET RECOGNITION® are trademarks of the American Nurses Credentialing Center (ANCC). The products and services of HCPro, a division of BLR, are neither sponsored nor endorsed by the ANCC. The acronym MRP is not a trademark of HCPro or its parent company.
model, and we can see how some of these things work together.”
Gravitating toward data analyticsBIDMC’s Risky States project represents one ex-
ample of a larger migration toward the use of patient and hospital data to improve quality care. As electronic health records (EHR) have become more prevalent, hospitals are collecting millions of data points with the potential to improve patient safety. With the help of sys-tems engineers, many of those hospitals are turning raw data into actionable changes.
For example, BIDMC is one of three medical sys-tems that make up the Libretto Consortium, founded in 2012 by the Gordon and Betty Moore Foundation. Together, BIDMC, Johns Hopkins Medical Center, and the University of California, San Francisco are looking at ways they can reduce harm, specifically in the ICU.

3HCPRO.COM© 2016 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Complimentary issue
In July, the National Quality Foundation (NQF) published a report, also funded by the Gordon and Betty Moore foundation, entitled Data Needed for Systemati-cally Improving Healthcare; it outlined ways to improve healthcare data usability. NQF indicated that although some pockets of the industry have begun using data to improve healthcare quality, opportunities still exist for widespread use.
Robert Saunders, a senior director at NQF in Wash-ington, D.C., says that many hospitals are using rudi-mentary data to shape process improvement, which can still make a big impact. He points specifically to Virginia Mason Medical Center in Seattle, which uncovered safety defects in sterile processing simply by tracking established defects on a whiteboard. (Editor’s note: Virginia Mason has done similar work with reducing bar code medication administration errors. See the Novem-ber 2014 issue of Patient Safety Monitor Journal.)
Saunders adds that healthcare providers can take advantage of a wealth of quality care data within EHRs, a source that some facilities have started tapping into only recently. “We are starting to see folks that are do-ing much more advanced work, such as looking at data through electronic health records or through data they have captured in some other data center within their hospital, to analyze things like how patients flow through the hospitals from the ED to the operating room to postop to a bed, and they are able to see the most ef-ficient way to do that.”
However, ICU data is particularly appealing for pro-viders because it offers a wealth of electronic informa-tion about patients who need the most intense levels of care.
“You can get a lot of information from moment to moment that you might not be able to get on a general unit right now,” Folcarelli says. “But it’s also a popula-tion of patients where their risks change. Some of them have really unpredictable patterns, so it’s appealing to think that when things are changing quickly on the unit, we could know that.”
Using data effectivelyOne of the key issues highlighted in the NQF report
was the fact that raw data alone is not enough to effect meaningful change. Instead, that data needs to be trans-lated into clear, actionable information.
“In a lot of places, we’re doing more and more things with the electronic health records system and health information technology systems, but those aren’t nec-essarily set up in a way that it’s providing meaningful, ac-tionable information that clinicians can use to improve,” Saunders says. “One of the big themes we came away with is that the data itself isn’t enough. It’s really about whether you can use the data.”
That’s where systems engineers come into play. Ac-cording to Sands, engineers at MIT have created algo-rithms and models that make healthcare data usable at BIDMC. He adds that BIDMC has already hired one systems engineer out of the MIT program and “would probably hire more if we were able to.” Although that engineer is focused more on wasted delays and man-aging capacity within the hospital, Sands notes that hospitals should look outside of their own organization to partner with other local entities with expertise in crunching large data sets.
“There is an increasing volume of data, some of which resides in different places,” he says. “For example, we were combining staffing data with clinical data, which is kind of unusual to look at that together, but we were able to look at signals that we otherwise wouldn’t have come up with by combining that data. Then there is sim-ply the knowledge of sophisticated statistical techniques that allow you to find meaning in that otherwise compli-cated data set.”
Saunders adds that part of making the data use-ful is making it trustworthy to physicians and nurses. Hospitals struggle to effectively use health data when clinicians don’t understand the data they are looking at, where it comes from, and how it impacts their day-to-day care for patients.
Part of building that trust is allowing clinicians to see the source of the data and how it can inform and im-prove the care they provide patients. This can involve the culture of the institution and how it approaches data collection, says Saunders, as well as the gradual familiar-ity that clinicians will gain as health data becomes more integral to quality improvement.
However, human intuition is equally important. In developing the Risky States project, clinician input has been and will continue to be integral to the process, Sands says. By soliciting feedback from staff regarding what they see as a safety risk, the model will become

4 HCPRO.COM © 2016 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Complimentary issue
smarter, more intuitive, and ultimately more reliable. That staff involvement can be crucial to the way clini-cians interact with improvement data.
“These aren’t things that are taught in clinical educa-tion programs, and yet they are really important in the day-to-day care of patients,” Saunders says. “We don’t need to turn everyone into a systems engineer, it’s just having even some level of familiarity and understanding of what these are and being able to start the process of these types of improvement methods can be very power-ful and lead to big results.”
Impacting patient safetyIn the end, the collection and dissemination of
healthcare data is most successful when it informs or drives patient safety initiatives or improves the way clinicians practice medicine. BIDMC’s Risky States project aims to do just that: Input multiple sources
of data into one model that spits out a straightfor-ward risk breakdown with the ability to shape clini-cal care.
Although BIDMC is still waiting to roll out a final app that will help clinicians predict when patients are entering periods of intense care, Folcarelli is op-timistic that the data analysis will ultimately reduce patient harm within the ICU and determine whether certain quality interventions are actually benefitting patient safety.
“What we will be able to do is manipulate the envi-ronment or manipulate the resources to reduce the intensity for those caregivers [when the risk is high], which I think gives people time to make decisions a little more slowly, and gives them time to think about how they want to order the activities for the day in order to mitigate risk,” she says. “What we’re hoping is a lot of those harm events will decrease over time.” H
State-based collaboratives lead to widespread quality care improvementsReports from Maryland and Pennsylvania show that a collective focus on patient safety has led to measurable improvement across the state
Quality improvement requires strength in numbers. At least that’s what hospitals in Maryland and Pennsyl-vania are finding as recent reports show that collabora-tion among local hospitals can lead to impressive patient safety improvements.
In March, the Maryland Hospital Association (MHA) released its annual report on quality, underscoring some of the statewide patient safety improvements through-out 2014. Last year, hospitals within the state improved hand hygiene rates from 71% in 2010 to 90% in 2014. Additionally, 90% of hospitals maintained zero central line–associated bloodstream infections (CLABSI) per month throughout the year, and 83% maintained zero catheter-associated urinary tract infections (CAUTI). Ventilator-associated complications decreased 55% from the previous year.
Meanwhile, in April, the Pennsylvania Patient Safety Authority (PPSA) released its 2014 Annual Report showing that high-harm events—events that result in
permanent harm to the patient, near death, or death—decreased 45% since 2005.
Finally, an Indiana report released in May by the Indiana Patient Safety Center shows improvements in a few specific areas of care. Early elective deliveries decreased 76% between 2012 and 2014, and hospitals prevented 1,254 readmissions and 110 blood clots, thanks to initiatives through the CMS Partnership for Patients campaign.
These statistics are indicative of an increasingly col-laborative approach to patient safety among state hos-pitals, patient safety groups, and hospital associations.
“Within Maryland there is very much the attitude and mindset that a rising tide raises all ships,” says Robert H. Imhoff III, president and CEO of the Maryland Patient Safety Center (MPSC) in Elkridge, Maryland. “Hospi-tals no longer say, ‘It’s just good for me, I just want to see my numbers and patient satisfaction and quality mea-sures go up.’ Everyone is working together to make sure

5HCPRO.COM© 2016 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Complimentary issue
all hospitals and all long-term care facilities are showing improvement in their quality measures.”
The collaborative environment in states like Maryland and Pennsylvania has allowed hospitals to feed off each other’s success and failure, learning from near misses and sharing best practices to improve patient safety. Although an element of competition still exists, quality improvement now relies on widespread collaboration.
“There is still competition, but [hospitals] realized what needs to be done to make sure that the population is getting the right care,” Imhoff says.
Maryland’s unique payment structureHealth experts believe the unique hospital payment
structure in Maryland has sparked collaboration among hospitals throughout the state. Last year, Maryland negotiated terms with the federal government that al-low that state to set hospital payment rates. In return, all hospitals must meet certain thresholds on specified
Leapfrog grades reveal disparities in quality care across state lines
In April, The Leapfrog Group updated its Hospital Safety
Score, which assigns letter grades to hospitals throughout the
country based on the facility’s prevention of errors, injuries,
accidents, and infections. The scores offer insight into quality
care at individual hospitals, but average statewide scoring
allows consumers, payers, and experts to see which states
are performing well.
According to Leapfrog scores, Maine was the safest
state to receive care, with 61% of hospitals receiving an A.
Massachusetts came in second with 50% of hospitals re-
ceiving an A, and Virginia, Florida, and New Jersey followed
close behind.
One of the reasons these states consistently provide high-
quality care has to do with strong payer initiatives that link
quality to hospital reimbursement, says Missy Danforth, vice
president of hospital ratings at The Leapfrog Group in Wash-
ington, D.C. In particular, payers in Maine, Massachusetts,
and New Jersey have made a strong push for value when it
comes to patient care, not unlike the federal agreement that
drives quality care in Maryland.
“I think hospitals are starting to understand that people
want to pay them based on the expectation that they can get
high quality at a reasonable cost,” Danforth says. “In order
to reach that high quality point, there needs to be some best
practice sharing.”
Alternatively, other areas of the country don’t fare as well
with Leapfrog grades. Washington, D.C., Arkansas, and North
Dakota did not have any hospitals with an A grade according
to the recent round of scoring. Part of this is due to the fact
that places like North Dakota have a high number of critical
access hospitals, which are not scored by Leapfrog. In
Washington, D.C., the high number of federal employees
has created a unique purchasing structure, Danforth says.
However, the number of states with a low percentage of
A hospitals—including Arkansas, Utah, Oklahoma, Nebraska,
West Virginia, and Connecticut—demonstrates that not all
states are making strides in quality improvement.
“It’s really difficult to pinpoint a single thing [in these
states],” Danforth says. “They just seem to have a lower
performance across a number of the measures.”
quality metrics surrounding hospital-acquired conditions and readmissions.
Specifically, the agreement requires hospitals to re-duce complications by 30% by the end of the five-year deal and bring readmission rates within the state down to the national average.
“Those are very aggressive, but I think we’re starting to see everyone is really focused on pulling in the same direc-tion,” says Nicole Stallings, vice president of policy and data analytics with the MHA in Elkridge, Maryland. “Collabo-ration has never been as high in Maryland as it is now.”
This unique structure has been particularly impact-ful on hand hygiene and readmissions. Hand hygiene compliance has been notoriously difficult for hospitals across the country, but knowing that it was one of the best ways to reduce infections, the MHA shifted its oversight approach by instituting a standard methodol-ogy using unknown observers. Using secret shoppers, they quickly found that compliance rates were much

6 HCPRO.COM © 2016 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Complimentary issue
about current trends within the state. Patient safety liai-sons go to hospitals to work with patient safety officers on specific quality concerns.
Hospitals are also required to report “non-harm” events. This might include a medication error caught by a nurse before it reached the patient. Doering says tracking those types of events can be just as valuable as serious events.
“You can take that event, and go back and say, ‘Why did that happen?’ ” Doering says. “It happened this time and someone caught it, but the next time it happens, there could be harm to the patient.”
State-run initiatives offer improvement opportunities Statewide collaboratives in Maryland, organized by
the MHA and the MPSC, have been the catalyst for change. Although hospitals have altered their ap-proach to competition when it comes to patient safety, the work done by these organizations drives focus areas for improvement.
“We convene focus groups, we talk to state health officials and look at public health data, and we look at the needs of the healthcare community and the provider community at large and what their requirements are,” Imhoff says. “[We find out] what cream is rising to the top and what issues are most important in the patient safety arena.”
Each year, Imhoff says the state looks at a list of approximately 20 new initiatives, but tries to focus its attention on those that will make the biggest im-pact. This year, MPSC has partnered with the MHA to address sepsis since it is associated with high rates of mortality.
Pennsylvania has a similar approach, using report-ing data to determine which areas could benefit from educational outreach. Doering says that although that collaborative attitude exists among hospitals, there is always going to be some undercurrent of competition. The PPSA exists as a third party that can assemble providers across the state to focus on certain areas of care.
“We’ll get together with patient safety officers and sit around and talk about what the issues are [in their facility],” he says. “We have networking sessions and they are happy to share what’s working for them or what’s not working for them.” H
lower than hospitals had previously reported. That data allowed hospitals to see where they could make improvements and how they measured up to other hospitals in the state.
Now, every hospital gets a report that also breaks down compliance according to physician group or employee type, so that hospitals can hone in on certain areas when necessary.
Readmissions in Maryland have seen a modest de-crease of 4%, but Imhoff says the collaborative approach is particularly important since it requires involvement from multiple community partners.
“The hospitals have done a really nice job in cooperat-ing with other healthcare providers, patients, and fami-lies to keep people out of the hospital and to keep them on their care plans to avoid continued hospital visits,” he says. “That population health model is very popular in Maryland. Hospitals work with community organi-zations, they work with outpatient facilities, and they work with long-term care postacute facilities, all toward providing a higher level of care which leads to a lower readmission rate.”
Benefits of data collectionIn Pennsylvania, state hospital reporting requirements
have been in effect since 2007, mandating that hospitals and nursing homes report healthcare-associated infec-tions (HAI) and serious events and incidents to the PPSA. Initially there was some concern among provid-ers about how the data would be used, but the eight-year-old database has proven to be vital to statewide quality improvement.
Part of that success relies on the way the system is structured, says Michael Doering, MBA, executive direc-tor of the PPSA in Harrisburg, Pennsylvania. The PPSA has become a trusted authority, using the data to help hospitals with system improvements, rather than punish those with low rates.
“We’re not going to come beat you over the head if you have a problem because we have no regulatory authority at all,” he says. “We’re an education, data col-lection, and training entity that is part of the state. The Department of Health is the regulator of this law and we’re not part of them.”
The PPSA has used the data to issue patient safety advisories and publish a quarterly peer-reviewed journal

7HCPRO.COM© 2016 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Complimentary issue
Reducing patient falls: Two healthcare systems, two different approachesAs patient falls continue to plague healthcare facilities of all shapes and sizes, health systems in Georgia and Nebraska share their success stories
Patient safety experts contend with a multitude of intricate health complications, from healthcare-associ-ated infections to medication management. However, amid these complex problems, one outwardly simple adverse event continues to pervade the industry: patient falls.
The Agency for Healthcare Research and Quality (AHRQ) estimates that as many as 1 million patients fall in the hospital each year. Falls may result in a few minor bumps and bruises, but in many cases, they can also lead to further health complications, including frac-tures, lacerations, or internal bleeding. AHRQ estimates that one-third of patient falls are preventable; however, what may seem like a straightforward problem is in fact very complicated. Falls can occur for any number of reasons, ranging from medication side effects to lower body weakness.
Healthcare facilities have found success in stopping patient falls by establishing an organized fall preven-tion program that identifies unique fall risk factors associated with each patient. Recently, two separate healthcare systems have been recognized for their ef-forts in this area.
In January, Grady Health Memorial Hospital in Atlan-ta was awarded the Quality and Patient Safety Award by the Partnership for Health and Accountability for a pro-gram that significantly reduced patient falls. Meanwhile, the University of Nebraska Medical Center (UNMC) in Omaha has received national attention for its “CAP-TURE Falls” program (Collaboration And Proactive Teamwork Used to Reduce Falls), which developed a multidisciplinary team approach to fall prevention in 19 Nebraska hospitals, many of which were critical access hospitals (CAH).
Although each provider took a different approach to fall prevention, both found that when they had leader-ship support and organizational awareness directed to-ward determining the risk factors associated with patient falls, their fall rates declined, sometimes significantly.
In the first quarter of 2014, following the rollout of a revamped fall prevention program, Grady Memorial reported a 75% decline compared to baseline measure-ments from 2011. Compared to the average fall rates in the three years before the program, the CAPTURE Falls program saw a 31% reduction in total falls during the first two years of the program, coupled with a 33% reduction in injurious falls.
These decreases occurred in the context of increased reporting, says Katherine J. Jones, PT, PhD, associate professor in the division of physical therapy education at the School of Allied Health Professions at UNMC and one of the leaders of the CAPTURE Falls program. Many hospitals did not report assisted falls that did not result in harm, nor did they include skin tears or bruises as injuries, both of which were emphasized during the rollout of the program.
Although some of the initial phases of the program were difficult to implement, hospitals ultimately saw the patient safety benefits to a team approach to fall prevention.
“We’re not talking about cardiac catheterization here, we’re talking about basic patient care,” Jones says. “If we can’t keep our patients safe from falls, then we really are not able to provide high-quality care.”
Identifying a problemsBoth fall prevention initiatives started with a few
simple questions: How frequently were patients falling, and why? For Grady Memorial, that question arose in 2011. During that year, the hospital reported 20 falls with injuries, which translated to a 15% fall rate. But in 2012, falls with injuries more than doubled to 46, jumping to a 28% fall rate.
“In that one year, we had more than twice as many falls than we had the previous year,” says Rosiland Harris, DNP, APRN, RNC, ACNS, BC, director of professional nursing education, practice, and research at Grady Memorial. “We did not want to see that rate continue to go upwards.”

8 HCPRO.COM © 2016 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Complimentary issue
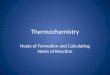
Post-fall huddle facilitation guide
Source: Developed by the University of Nebraska Medical Center CAPTURE Falls Program, under a federal grant from the Agency for Healthcare Research and Quality.

9HCPRO.COM© 2016 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Complimentary issue
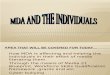
Post-fall huddle facilitation guide (cont.)
Source: Developed by the University of Nebraska Medical Center CAPTURE Falls Program, under a federal grant from the Agency for Healthcare Research and Quality.

10 HCPRO.COM © 2016 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Complimentary issue
Grady Memorial set out to identify the reasons behind patient falls, but it couldn’t pinpoint one particular risk factor. Instead, the hospital determined that its entire falls program was insufficient.
“We were not adhering to the best practices for fall prevention and didn’t have the best processes in place at that time to really accurately monitor falls or look at some of the debriefings that occurred after a patient fall to see if there was any opportunity for us to prevent those falls,” Harris says.
In Nebraska, the CAPTURE Falls program was born out of the desire to obtain a better understanding of fall rates specifically within CAHs. Sixteen of the hospitals that participated in the program are CAHs with 25 or fewer beds. Jones says there was very little research that looked specifically at small, rural hospitals, but research-ers at UNMC believed that the risks would be higher for the following reasons:• CAHs care for an older adult patient population
that is more at risk for falls.• CAHs often provide swing bed care that focuses on
physical therapy and improving independence.• CAHs have limited quality improvement resources and
frequently have one person performing multiple duties.• There are no valid benchmark rates for patient falls
in CAHs. Fall prevention is difficult to prioritize if hospital leaders don’t have the data to indicate it is problematic.
• CMS still pays CAHs for some healthcare-acquired conditions, including injuries from a fall. Larger hospi-tals are no longer reimbursed for those complications.
In 2011, Jones and others from UNMC conducted a baseline assessment of hospitals in Nebraska and found that fall rates were approximately 50% greater in CAHs compared to traditional hospitals (5.9 vs. 4.0 per 1,000 patient days), while injurious fall rates were 88% more likely (1.7 vs. 0.9 per 1,000 patient days). Their assess-ment was published in the Journal of Rural Health in 2014. Based on that assessment, researchers at UNMC determined that CAHs lacked organizational structures that addressed fall prevention.
“What we found was there wasn’t a lot of vari-ability between CAHs and larger hospitals in terms of interventions at the bedside. Where the variability occurred was in what was done organizationally,” says
Jones. “So what types of training programs did you have? Were you using a validated tool? Did you dedi-cate staff to your fall risk reduction program? Did you report assisted falls, and did you do a medication review prior to a fall?”
Risk reduction focus areasOnce each organization had evaluated baseline data,
both Grady Memorial and UNMC took a broad ap-proach to addressing patient falls. Recognizing that fall prevention varied at an organizational level, UNMC researchers sought to develop a comprehensive pro-gram that would involve physical therapy and pharmacy, as well as nursing. With a grant from AHRQ, UNMC developed the CAPTURE Falls program, emphasizing a team-based approach to care.
Through the AHRQ funding, UNMC developed a toolkit that would “plug a gap we saw in other tool-kits,” Jones says. Key focus areas included how to choose an appropriate fall risk assessment, determin-ing what patients may be at risk for falls, tracking assisted falls, and assessing a fall prevention program through the use of a scorecard. “Those hospitals that were the most successful understood the need for the change, and they recognized that what they were learning was a process they could apply to all safety and quality challenges,” she says.
In Atlanta, Grady Memorial used its baseline assess-ment to refocus fall prevention efforts. The hospital’s chief nursing officer took the lead on redesigning the program, assigning a nurse educator as the fall team leader and identifying fall champions for each unit.
After formalizing the goals and objectives of the program, Grady Memorial made tweaks by redefining what qualified as a fall, adding color-coded signs for at-risk patients, providing patient education, and con-ducting hourly rounding. She adds that Grady Memorial achieved a 75% decrease because the program evolved into a competition between units. Fall injury rates were included in unit director goal reports that were reported to senior leadership, which offered accountability for every unit. “When other units had done everything they were supposed to do and they were getting good compli-ance, it just got legs and started taking on a process,” Harris says. “Everybody really got engaged and began to really focus.” H

11HCPRO.COM© 2016 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Complimentary issue
A study published in the April edition of the Journal of Hospital Medicine combines the principles of real-time feedback and financial incentives to get frontline buy-in for quality improvement initiatives. Lead researcher Henry Michtalik, MD, MPH, MHS, assistant professor of medicine at John Hopkins Hospital in Baltimore, Mary-land, used real-time visual feedback of compliance rates for preventing venous thromboembolism (VTE), along with small monetary bonuses for improved care, to help reduce VTE among hospital patients.
In the first six months of the study, in which physicians were provided real-time feedback on a Web-based dis-play, VTE prophylaxis compliance rates improved 86% to 90%. Over the remaining 18 months, in which physi-cians were also paid for meeting quality improvement thresholds, compliance improved to 94%.
Patient Safety Monitor Journal spoke with Michtalik about the study and how this approach improved physi-cian involvement in quality improvement initiatives. (Editor’s note: The following transcript has been edited for clarity.)
Q What made you decide to focus on these two interventions: real-time feedback and
pay-for-performance?
A One of the easiest ways to frustrate frontline providers is to implement changes and bench-
marks without explaining them. The intervention here provides feedback and shares where there are potential opportunities for change and how those changes have an impact. So the dashboards and feedback really act di-rectly on that in terms of what the benchmarks are, what can be done to improve them, and how the providers are changing their practice.
This is all happening in the healthcare environment that’s really focused on pay-for-performance. This study has built on that and takes these concepts into account and applies them at the provider level.
Expert Q&A
Real-time feedback and monetary rewards pull physicians into quality careJohns Hopkins study ties together principles of real-time feedback and value-based purchasing to reduce blood clots
So the study was a way to combine both giving feedback to well-intentioned providers and affecting practice, as well as incorporating healthcare reform, which is focusing on pay-for-performance and value-based purchasing.
Q There have been other studies that looked at the impact of real-time feedback for physicians. How
was this approach different?
A Our approach is different in that it was timely. It was really real time. It wasn’t waiting until a
report was generated three months from now and you wouldn’t be sure which patient encounter it was associat-ed with and you would have to recall what you had been doing back then.
Another feature was that it was individualized and showed a comparison with local peers. It was individu-alized to providers themselves and showed how they compared to others in their own group. So it was a way to provide individual feedback in the setting of what was happening within their own practice.
I think the third aspect was that it showed change over time. So you were able to see what the practice was before, the current situation, and track it along in the future. It provided a chronological history as well, and that was all in a visual platform that was easy to access for the provider.
Q When you talk about that platform, is that something you had to build internally and work
with IT?
A EHRs really helped. It has both advantages and challenges. The advantage is you have lots of da-
ta and it’s easier to pull the data. The challenges are that there are attribution concerns and you have to validate the data.
So we took those metrics, but also had to put them in a physician-friendly dashboard. We know that provid-

12 HCPRO.COM © 2016 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Complimentary issue
ers are limited on their time and wanted to sum up as much information as we could in as simple a format as was possible.
We did visual displays and we tested those displays to see what was important to providers, what was easy to read, and what would quickly give a snapshot to the providers themselves of what was going on both within their own practice and in comparison to the others. Some of the feedback we got was that trends over time were important. There could always be fluc-tuations, but really seeing that there was a difference in a trend over time with a historical view was impor-tant to providers.
The other important aspect was comparison with the other physicians in the group. We know that with bench-marks in other institutions, there are various compound-ing factors like the services that are available to the providers and the patient populations. Physicians were more interested in what was going on in their own local group and how they compared with it. These were some things that we needed to incorporate into the displays and the dashboards.
Q How does that incorporate into a physician’s workflow? How often are they seeing that data?
A It’s within the provider’s workflow in a couple of aspects. One is that the dashboard is within the
same electronic system and same general login system that is used to access patient records, radiology, or put in orders; it’s all within the same system.
I think the other aspect is that when we present the metrics that we were including into the dashboard, we told providers how they were being calculated and what things were being measured. We pointed out that there is a VTE risk assessment built in to the order set and how recommendations were made. A lot of this was not trying to implement a system onto physicians, but really showing that it’s working in concert with other things that were going on and bringing their attention into a lot of the quality improvement interventions that were being pursued simultaneously.
Q Did it change the approach that physicians took in terms of providing care?
A What happened was physicians were more at-tentive to the risk assessments and ordering
appropriate prophylaxis. Whereas it would be the stan-dard to just really quickly go through the assessment and the order sheet, this was something that brought more attention to that specific metric and the rationale of why it was being measured and why these interventions were in place.
Q Why do you think the payments, even though they were small, served as a way to engage
physicians?
A The challenge that physicians have is they have many competing and often conflicting priori-
ties, so we really used the small financial incentive as a way to engage providers and bring attention to the dashboard.
As we mentioned in the study, there wasn’t a substan-tial portion of salary at risk for this; it was more bringing attention to the dashboard. Physicians themselves are lifetime learners and engaged in care. They are always seeking out additional information and seeing how they compare to their peers, and this is really building on those characteristics as well as healthcare reform incentives and the priorities of the institution and patient safety and quality care initiatives.
Q Do you think this approach is something more hospitals will consider?
A I think traditionally, a lot of the dashboards have been at the institutional level. So core metrics,
events, and hospital-acquired conditions, they have really been focused at the hospital level because that’s typical-ly where the financial risk is shared and the reporting is done. With healthcare reform and interventions, we’ve had a push to get frontline providers involved. Rather than things coming down from the administration as be-ing directives, instead, this shifted more toward frontline providers, which says this is what is going on in your in-dividual services and teams. What do you as a frontline provider see as going on? Where are our opportunities for improvement?
It’s a bottom-up approach taking into account front-line providers’ wisdom or the “hospital floor smarts” that they have of what is going on in the front line and coupling that with in reality the overall performance of the institution. So it’s taking a micro approach to a macro problem. H