Embed Size (px)
Citation preview

A Plan of Action for Improvingthe Oral Health Statusof Michigan Residents

Table of Contents
Introduction ..................................................................................................2
Oral Health & Systemic Health...................................................................6
Oral Health Status of Michigan Residents..................................................7
Access to Care...............................................................................................10
References and Sources for Literature Review...........................................14
Summary of Recommendations ...................................................................16
Action Plan Matrix for the Oral Health Plan of Action ............................17
Data Workgroup...........................................................................17Prevention, Education and Awareness Workgroup ..................22Funding Workgroup ....................................................................29Workforce Workgroup ................................................................32

Introduction
"I can see clearly now the rain is gone. I can see all obstacles in my way."~ from the song I Can See Clearly Now by Johnny Nash
T his simple phrase summarizes the status of oral health in Michigan. While we know there areobstacles, we can see them and, as a result, plan for how to overcome them. The recent creationand continuous expansion of the Michigan Oral Health Coalition has brought with it momentum
to move oral health to the forefront of policy discussions. The connection between oral health andsystemic health is beginning to be recognized by not only policymakers but also the public at large. Thecoalition, as well as multiple trade associations and advocates, has identified that oral health is integral toprimary health care and has been actively communicating this statewide. As a statewide community, wenow know where we are going and are preparing for how to get there.
The Michigan Department of Community Health (MDCH) recognized the need for Michigan to developa coordinated effort around improving the oral health status of residents and submitted a proposal to theCenters for Disease Control and Prevention (CDC) to improve the oral health infrastructure in Michiganand develop a state oral health plan. Michigan is now in the second year of this infrastructure project.
The Michigan Oral Health Coalition kicked off on December 11, 2003, with a full membership meeting.At this meeting, participants were welcomed by Janet Olszewski, Director of the Michigan Department ofCommunity Health. Director Olszewski stressed to the participants the important role of the coalitionand the commitment of MDCH to adopt the five-year plan of action developed by the Oral HealthCoalition. At the kick off participants also identified a mission, outlined important issues, and describedoral health assets in Michigan.
The actions outlined in this paper are designed to improve the oral health status of Michigan’s residents.Such a challenging task would not be possible without the work of many motivated organizations andindividuals. This paper represents the work of an interagency coalition known as the Michigan OralHealth Coalition. Members of the coalition include:
Advantage Health Centers / DetroitAlcona Health Center / LincolnBaker College / Port HuronBaldwin Family Health Care / BaldwinBlue Cross Blue Shield of Michigan / SouthfieldBranch, Hillsdale, and St. Joseph County Health Department / ColdwaterCalhoun County Health Department / Battle CreekCapital Area Community Services, Inc. / LansingCapital Area Health Alliance / LansingCenter for Family Health / JacksonCherry Street Health Services / Grand RapidsChildren’s Hospital of Michigan / DetroitDelta Dental Plan of Michigan / LansingDental Clinics North / CharlevoixDetroit Community Health Connection / DetroitDetroit Department of Health & Wellness Promotion / Detroit
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 2

Family Health Center of Battle Creek / Battle CreekFamily Independence Agency / LansingHackley Community Care Center / Muskegon HeightsHackley Hospital / MuskegonHamilton Community Health Network / FlintHead Start-State Collaborative Program / LansingHealth Delivery, Inc. / SaginawHenry Ford Health System, School Health Initiative / DetroitHillsdale County Human Services Network / HillsdaleIngham County Health Department / LansingIngham Oral Health Coalition / LansingIntercare Community Health Network / BangorInterTribal Council / Sault Ste. MarieIonia County Health Department / IoniaKalamazoo County Dental Clinic / KalamazooLansing Community College Dental Hygienist Program / LansingLifeways / JacksonMarquette County Health Department / MarquetteMedical Services Administration / LansingMichigan Academy of Pediatric Dentistry / FlintMichigan Council for Maternal and Child Health / LansingMichigan Dental Association / LansingMichigan Dental Assistants Association / LansingMichigan Dental Hygienists Association / East LansingMichigan Department of Community Health / LansingMichigan Department of Education / LansingMichigan Department of Environmental Quality / LansingMichigan Department of Environmental Quality-Water Division / LansingMichigan Family Resources, Inc. / WalkerMichigan Health & Hospital Association / LansingMichigan Health Council / OkemosMichigan Primary Care Association / OkemosMichigan Public Health Institute / OkemosMichigan Spit Tobacco Education Program / LansingMid-Michigan District Health Department / StantonMobile Dentists/Children’s Dental Health Foundation / Farmington HillsMonroe County Health Department / MonroeMott Children’s Health Center / FlintMuskegon Community Health Project / MuskegonMuskegon County Health Department / MuskegonMuskegon Family Care / MuskegonNorthwest Michigan Community Health Agency / Traverse CityNorthwest Michigan Health Services, Inc. / Traverse CityOakland/Livingston Human Service Agency, Child Development Division / PontiacOmni Oral Pharmaceuticals / KentwoodOttawa County Health Department / HollandPublic Sector Consultants / LansingSaginaw County Department of Public Health / SaginawSault Tribe of Chippewa Indians / Sault Ste. Marie
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 3

School-Community Health Alliance of Michigan / OkemosSt. Clair County Health Department / Port HuronSterling Area Health Center / SterlingTelamon Corporation / LansingTri-County Dental Health Council / SouthfieldUniversity of Detroit Mercy School of Dentistry / DetroitUniversity of Michigan Health System / Ann ArborUniversity of Michigan School of Dentistry / Ann ArborUniversity of Michigan School of Public Health / Ann ArborUpper Peninsula Association of Rural Health Services / MarquetteVan Buren/Cass County Health Department / HartfordWashtenaw Children’s Dental Clinic / Ann ArborWayne County Health Department / DetroitWolverine Dental Society / Detroit
MissionTo improve oral health in Michigan by focusing on prevention, health promotion,surveillance, access and the link between oral health and total health.
Key oral health assets and issues were identified at the kick off meeting of the Michigan Oral HealthCoalition and were identified as follows:
Assets
CDC grant for preventionA good supply of dentists, dental auxiliary,physicians, and nurses (albeit maldistributed)Major universities with expertise to work with community partnersFluoridated water in many communitiesGrassroots coalitions in local communitiesSafety-net dental programs, including those at Federally Qualified Health Centers, local health departments, and school-based health centersProtection of oral health services for children through Early Periodic Screening, Diagnosis, and TestingEducation and business partnershipsHealth education in schools - Michigan Model(K-12) includes oral healthGovernor Granholm and her administration interested in oral healthMedia interested in health issuesStrong third-party payor structureHealth professional studentsPassionate leaders and vision
Key Issues
Lack of providers willing to serve low-incomepeople and those with special needsLack of a State Oral Health OfficerLack of public awareness of importance of oral healthLack of utilization of all dental professionalsLack of pediatric dental resourcesProvider maldistributionScope of practice limitationsLack of statewide dataLack of affordable services for uninsured Lack of Medicaid adult dental coverageLack of oral health funding in generalLack of public/private funding for prevention strategies Insufficient payment rates
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 4

Participants then voted, as a way to guide deliberations, for those issues they felt were the mostsignificant facing oral health in Michigan. The issues were divided among key topics and workgroupsformed: Data, Prevention, Education and Awareness, Funding, Leadership, and Workforce. Theworkgroups were asked to begin by addressing those issues of highest concern. Workgroup chairs werenominated and meeting participants identified workgroups in which they wished to participate. MichiganPrimary Care Association (MPCA) staff provided support to all workgroups in order to coordinate effortsbetween groups and provide documentation of their activities.
After the kick-off meeting, a Steering Committee of key stakeholders representing broad oral healthinterests and backgrounds was selected to guide the work of the coalition. The 10 member SteeringCommittee was comprised of the workgroup chairs and other leaders within the oral health community.The committee met throughout the development of the plan to review preliminary work plans andmeeting summaries from the workgroups to avoid overlap among workgroups and ensure that all grantobjectives were being met. As the Steering Committee noted areas that could be strengthened, additionalmembers were asked to join based on their expertise.
The Oral Health Coalition has nearly 160 members who are involved in various workgroups. Fiveworkgroups met on a regular basis and were led by volunteer workgroup chairs. Workgroup sizes rangedbetween 10 and 22 members. The meetings focused on the development of goals and objectives relatedto their specific area of focus. After four months of meetings, it was determined that the objectives of the Leadership Workgroup could easily be folded into the activities of other workgroups and, as aresult, discontinued. The final work plan includes the goals and objectives outlined by the remainingfour workgroups.
In May and November 2004, the entire Michigan Oral Health Coalition reconvened to review each of theworkgroups’ draft work plans and oral health surveillance findings. Membership then worked together toestablish the next steps for the coalition. The work plans were then incorporated into the Plan of Actionand presented to the Steering Committee, the workgroups, and the full coalition for review and approval.After the coalition approved the draft plan, it was presented at five community meetings across the statein order to gain feedback. The forums occurred in Grand Rapids, Detroit, Gaylord, Saginaw, andMarquette via video conference. Approximately 100 participants attended a community meeting to givefeedback on the plan. These comments were summarized in a report prepared by Public SectorConsultants and presented to the coalition for review. Workgroups adapted the plan as a result of forumcomments. These changes were presented to the Steering Committee and then the full coalition. Theplan was submitted for approval by the Michigan Department of Community Health in May 2005. InAugust 2005, the Plan was officially approved by the Director of MDCH, Janet Olszewski.
Strategies to Identify Best PracticesWorkgroups will continue to convene as necessary to implement each of the activities outlined in thePlan of Action. They will also continue to identify best practices that can be replicated in Michigan andshare practices that may be helpful to other states through continued collaboration with the Association ofState and Territorial Dental Directors (ASTDD) and the CDC. Workgroups have identified best practicesthat they will implement in their work plans. For example, the Workforce work plan has proposed toresearch approaches used by other states to address access issues with the current workforce.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 5

Implementation Strategies, Leveragingof Resources, Partnerships, and Plan MaintenanceThe Michigan Oral Health Coalition is fortunate enough to have nearly 160 individual partners with abroad range of experience who are eager to begin implementation of the plan. Responsible individuals ororganizations have been identified in the plan as the lead to ensure that action steps are accomplished.Workgroups will continue to meet as necessary to monitor their progress and if appropriate identify andincorporate new research initiatives. The MDCH Oral Health Program Coordinator will act as a liaisonbetween the coalition and MDCH. Progress on the implementation of the plan will be reported at theannual conference and coalition meeting hosted by MDCH and MPCA.
Many of the coalition partners have committed local resources to implement various components of theaction plan. For example, the Michigan Dental Association has volunteered to spearhead the statewideoral health campaign each February. Many other activities can be accomplished utilizing existingresources. The Oral Health Coalition will continue to examine resources at the state and local level thatmay be leveraged in order to complete the outlined objectives.
Healthy People 2010 Objectives & Evaluation Strategies for Monitoringthe Outcomes and Impacts of Plan ImplementationAn evaluation committee convened by the Michigan Department of Community Health willperiodically evaluate the effectiveness of the coalition. The surveillance provided by the Data Workgroupand the monitoring mechanisms identified in the action plan will serve as key evaluation tools inmonitoring the effectiveness of coalition activities. The coalition Steering Committee will serve asmembers of the evaluation committee. The Oral Health Coalition Workgroups will work with MDCH toprovide continuous reporting on the oral health status of Michigan residents and present this informationas well as reporting progress on the impact of prevention interventions annually during the annual OralHealth Coalition meeting each June. The surveillance plan includes each of the Healthy People 2010Oral Health Objectives, which will be continuously monitored for improvement. Status on meeting eachof the Healthy People 2010 objectives will be provided annually the Michigan Department ofCommunity Health evaluation committee.
Oral Health & Systemic Health
O ne of the primary areas of focus of the Michigan Oral Health Coalition is recognition of theconnection between systemic health and oral health. Inattention to oral health has importantimplications for our ability to reach current and future health outcome goals. Poor oral health
has effects on pre-term births/low birth weight babies, diabetes control, heart disease, and respiratorydisease.
National Institute of Health funded studies estimate that as many as 18% of the 250,000 prematurebabies born weighing less than 5.5 pounds in the United States each year are due to periodontal infection(NIDCR, 2004). Pregnant women with periodontal disease may be seven times more likely to have ababy who is born too early or too small (AAP, 2004).
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 6

Recent studies point to an increased risk of heart disease and stroke in people with periodontal disease.The risk increases with the severity of infection. Heart disease is the leading cause of death in Michigan(MDCH, 2003).
Numerous studies have shown the impact periodontal disease can have on diabetes. People withdiabetes are twice as likely to have periodontal disease (ADHA, 2003). Periodontal disease makes itmore difficult to control blood sugar levels, and badly managed blood sugar levels can make periodontalproblems worse. The Michigan BRFSS found that 41.8% of individuals with diabetes had lost six ormore teeth in 2002 compared to 15.2% for those without diabetes (MDCH BRFSS, 2003). Many systemic diseases have oral manifestations and can inform clinicians of the need for furtherevaluation. The oral cavity can also be adversely affected by many pharmaceuticals and other therapiescommonly used in treating systemic conditions. Finally, individuals such as immunocompromised andhospitalized patients are at greater risk for morbidity due to oral infections.
Oral Health Status of Michigan Residents
Oral Health InfrastructureThe Michigan Department of Community Health recognized the need for Michigan to develop acoordinated effort around improving the oral health status of residents and submitted a proposal to theCenters for Disease Control and Prevention. Michigan is now in the second year of this infrastructureproject. The previous two-year planning grant focused on the development of a baseline oral healthassessment and assessing Michigan’s current oral health surveillance tools. Another area of focus duringthe first two years was providing training, consultation, and technical assistance to communities onconducting an oral health capacity/staffing assessment, conducting a validation survey of services forchildren less than 20 years of age, and utilizing data in program planning.
The first year of the current five-year (Fiscal Year ‘04 to Fiscal Year ‘08) proposal focused on theformation of a coalition. The coalition is responsible for the development of a five-year plan to improveoral health and compilation and analysis of data available to implement a statewide oral healthsurveillance system. These activities began in July 2003. A part-time oral health epidemiologist washired at MDCH to begin working on the surveillance system and MDCH contracted with MichiganPrimary Care Association (MPCA) to develop and facilitate the activities of the Oral Health Coalition.
Michigan had been without an Oral Health Program Coordinator at the Michigan Department ofCommunity Health for two years, until September 2004. The lack of a statewide coordinator tospearhead statewide efforts had left a considerable gap in the state. An oral health coordinator was hiredin September 2004, who has aided in the coordination of services in the state.
In 1991, the Michigan Department of Community Health, with the assistance of an interagencyworkgroup, developed the Michigan Oral Data (MOD) System as a tool to provide a dental disease
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 7

profile of the population served in the participating publicly funded dental clinics. The system involvesthe collection of caries, untreated decay, and several other oral health indicators. Currently 11 dentalclinics in Michigan collect oral health data using this system. The MOD System is not population basedor statewide; but, data from the system can provide some insight on the status of oral disease and may bea useful component of the statewide oral health surveillance system. Efforts continue in order to expandthe number of clinics in Michigan who collect oral health data using the MOD system.
In the future, the Michigan Oral Health Coalition is examining the use of an additional source of oralhealth data. The Basic Screening Survey (BSS) is a statewide and population based oral data collectiontool. The BSS is a standardized set of forms developed to collect information on the observed oral healthof participants of all ages. The survey notes the presence of untreated decay and the urgency fortreatment of all ages and edentulism in adults.
There is concern that the oral health infrastructure for underserved individuals in Michigan and the healthstatus of residents is at risk. Oral health services for adults on Medicaid, beyond emergency care, wereeliminated as of October 2003. With the elimination of the benefit more than 600,000 adults in Michiganlost access to oral health care. This benefit elimination has forced dental clinics to reduce hours andcaused at least one clinic to cease operation.
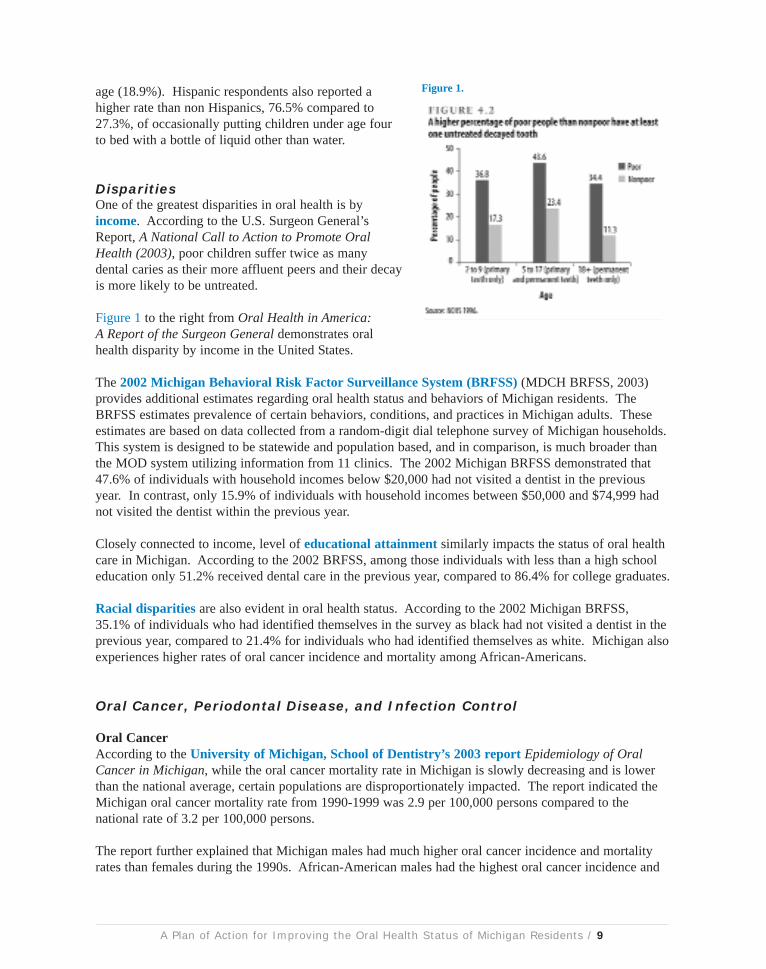
Description of Priority Populations, Burden of Disease & CariesDental caries (tooth decay) have been considered the single most common chronic childhood disease.According to the MOD System findings, approximately one in six underserved children had evidence ofearly childhood caries. Among 6- to 12-year-old children, 46.3% had caries experience in theirpermanent teeth and 30.8% had untreated permanent tooth decay. An average of 2.9 permanent teeth haddecay among children with caries experience. The rate of caries experience in permanent teeth isdramatically higher among underserved adolescents at 82%, with 54.6% having untreated decay (MDCH,2004). It is difficult to make direct comparisons to national caries data for these age breakdowns;however, national numbers can be found in Figure 1.
The MOD System also indicated poor oral health status for underserved adults. Two-thirds ofunderserved adults in Michigan aged 20-64 had untreated permanent tooth decay and 55.6% had lost atleast one tooth due to caries experience or periodontal disease (MDCH, 2004). In comparison, the CDCestimates that nationally approximately one-third of poor adults 18 and over have untreated decay in apermanent tooth (CDC, 2004). The Michigan system also found that nearly one in six of the adults hadroot caries experience.
The coalition proposes ongoing surveillance of caries experience in both children and adults. Otheractivities geared at reducing the incidence of caries include providing education on oral health throughoutthe lifespan, supporting efforts of MDCH to implement a school-rinse program and school-based sealantprogram, and improving access to preventive care for underserved populations.
Early Childhood Caries (ECC)The 2003 Michigan Child Dental Coverage Validation Survey reported that among all children underage four, 29.3% had been put to bed at least occasionally with a bottle of juice, formula, milk, or otherliquid besides water (Eklund, 2003). The validation survey found there were significant differencesbased on the age and ethnicity of the respondent. Respondents under age 30 were much more likely toreport this having been done at least occasionally (41.4%) compared to those respondents 30-39 years of
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 8
age (18.9%). Hispanic respondents also reported ahigher rate than non Hispanics, 76.5% compared to27.3%, of occasionally putting children under age fourto bed with a bottle of liquid other than water.
DisparitiesOne of the greatest disparities in oral health is byincome. According to the U.S. Surgeon General’sReport, A National Call to Action to Promote OralHealth (2003), poor children suffer twice as many dental caries as their more affluent peers and their decayis more likely to be untreated.
Figure 1 to the right from Oral Health in America:A Report of the Surgeon General demonstrates oralhealth disparity by income in the United States.
The 2002 Michigan Behavioral Risk Factor Surveillance System (BRFSS) (MDCH BRFSS, 2003)provides additional estimates regarding oral health status and behaviors of Michigan residents. TheBRFSS estimates prevalence of certain behaviors, conditions, and practices in Michigan adults. Theseestimates are based on data collected from a random-digit dial telephone survey of Michigan households.This system is designed to be statewide and population based, and in comparison, is much broader thanthe MOD system utilizing information from 11 clinics. The 2002 Michigan BRFSS demonstrated that47.6% of individuals with household incomes below $20,000 had not visited a dentist in the previousyear. In contrast, only 15.9% of individuals with household incomes between $50,000 and $74,999 hadnot visited the dentist within the previous year.
Closely connected to income, level of educational attainment similarly impacts the status of oral healthcare in Michigan. According to the 2002 BRFSS, among those individuals with less than a high schooleducation only 51.2% received dental care in the previous year, compared to 86.4% for college graduates.
Racial disparities are also evident in oral health status. According to the 2002 Michigan BRFSS,35.1% of individuals who had identified themselves in the survey as black had not visited a dentist in theprevious year, compared to 21.4% for individuals who had identified themselves as white. Michigan alsoexperiences higher rates of oral cancer incidence and mortality among African-Americans.
Oral Cancer, Periodontal Disease, and Infection Control
Oral CancerAccording to the University of Michigan, School of Dentistry’s 2003 report Epidemiology of OralCancer in Michigan, while the oral cancer mortality rate in Michigan is slowly decreasing and is lowerthan the national average, certain populations are disproportionately impacted. The report indicated theMichigan oral cancer mortality rate from 1990-1999 was 2.9 per 100,000 persons compared to thenational rate of 3.2 per 100,000 persons.
The report further explained that Michigan males had much higher oral cancer incidence and mortalityrates than females during the 1990s. African-American males had the highest oral cancer incidence and
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 9
Figure 1.
mortality rates among all races and gender groups. The incidence rate of oral cancer in African-American males of 25 per 100,000 individuals was 1.5 times higher than the rates of the white males and3.6 times higher than the rates of the African-American females. The attached Plan of Action outlinesactivities aimed at improving the oral cancer mortality rate and the disparities that exist.
The Data Workgroup and the MDCH Oral Health Epidemiologist will investigate options to measureperiodontal disease in Michigan. Measures to improve oral health status and reduce periodontal diseaseare identified throughout the Plan of Action, including education on the importance of oral heath care andimproving access to care for un-served populations.
All individuals involved in clinical activities related to the work of the coalition will be educated on theCDC's Guidelines for Infection Control in Dental Health-Care Settings (2003). Information on statewidetrainings on infection control in the dental setting will be widely distributed to coalition partners. MPCAwill also propose hosting a session on Infection Control at the annual Michigan Oral Health Conferencein which continuing education credits are made available.
DiabetesStudies have shown several relationships between oral health and diabetes. In Michigan, the 2002BRFSS found that persons with diabetes were much more likely to have lost six or more teeth than thosewithout diabetes (MDCH Diabetes 2004). Nearly forty-two percent of those with diabetes lost six ormore teeth compared to just over 15% for those without the disease.
Access to Care
W hile certain populations in Michigan are able to access dental care easily in their community,there are many for whom access to dental care is extremely limited. The oral health disparitiesin the United States due to these access barriers are vast. The 2003 Michigan Child Dental
Coverage Validation Survey reported that for children three years of age and older, 83.8% of them hadseen a dentist within the past 12 months. The survey demonstrated that those without dentalinsurance are twice as likely to have never visited a dentist as were those with insurance. Of the childrenwithout dental insurance, 11.2% had never visited the dentist compared to 5.2% for those with dentalinsurance (Eklund, 2003).
Michigan established a State Children's Health Insurance Program (SCHIP), MIChild, which offersinsurance for children who are uninsured and not eligible for Medicaid. The MIChild dental program hashad great success in provider participation and in the number of children utilizing dental care. Theincreased provider participation has been attributed to increased reimbursement levels and decreasedadministrative burden.
Michigan also has a dental demonstration project in 37 of Michigan’s 83 counties called Healthy KidsDental. The program has moved the children who were in the traditional Medicaid dental program intothis state-private dental partnership. This was accomplished by purchasing the use of a private dentalhealth plan that results in increased Medicaid reimbursement levels and reduced administrative
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 10
difficulties. It has proven to be effective in increasing the number of children who receive dental care inthe rural counties where it has been implemented by increasing the number of providers willing to carefor the patients.
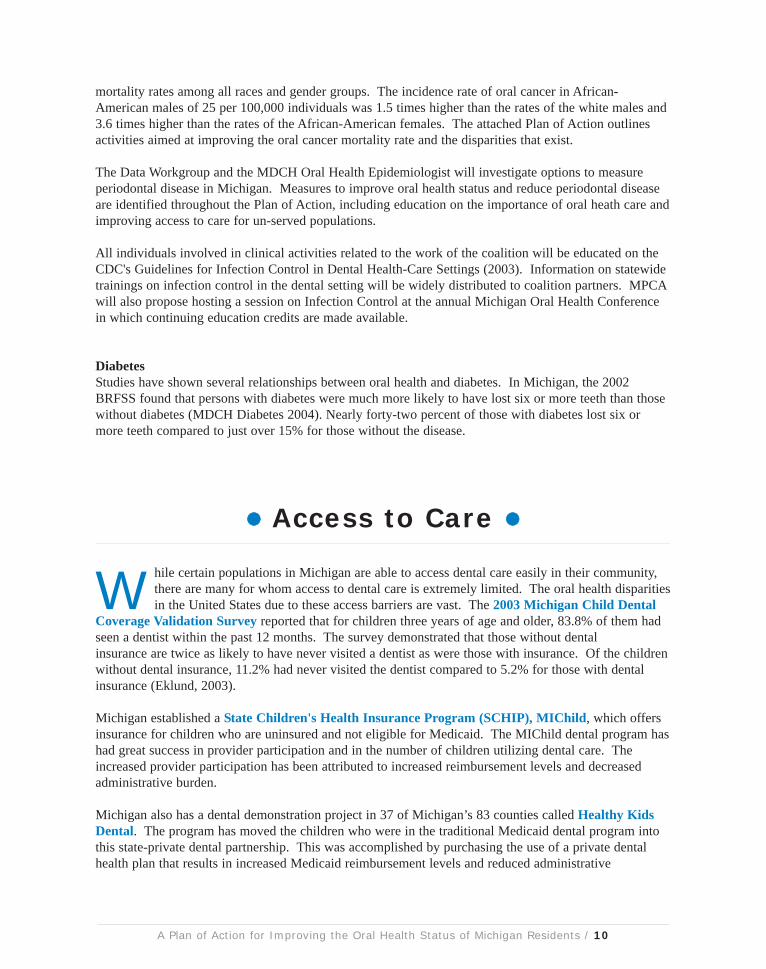
Thirty percent of Michigan’s children were enrolled in Medicaid in 2002. Only 23% of Medicaidenrolled children aged 0-19 received a dental visit during that same time period. Of all Michiganchildren, including those on Medicaid, 51% had a dental visit during that same year. Figure 2 depicts theproportion of Medicaid enrolled children who had at least one dental visit in 2002. Figure 3 depicts theproportion of all Michigan children who had at least one dental visit in 2002 (Eklund, 2003).
Figure 2. Figure 3.
Despite efforts of a few existing dental programs for persons with special needs (e.g. those who aremedically compromised or who are mentally impaired), access barriers continue to plague theseindividuals. One issue is the availability of medical facilities for the provision of dental services undersedation or with medical support. Provider training programs also continue to be limited, which in turnhas restricted access in many parts of the state.
Strategies to Address Oral Health Promotion Across the LifespanThe Michigan Oral Health Coalition is focused on improving oral health throughout the lifespanbeginning with proper prenatal oral health care and continuing through care in nursing homes and athome health facilities. Comprehensive oral health education resources will be developed for all ages andnon-dental health care providers will be provided with information on the importance of oral health. Thecoalition will continue to build networks throughout the state to improve education on the importance oforal health for individuals throughout the lifespan and will aim to increase access to evidence basedpreventive practices that maintain optimal health for all ages.
Water FluoridationHealthy People 2010-Oral Health proposes to increase the proportion of the U.S. population served bycommunity water systems with optimally fluoridated water in order to reduce dental caries. As noted inOral Health in America: A Report of the Surgeon General, community water fluoridation continues to bethe most cost-effective, equitable, and safe means to provide protection from tooth decay in a community.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 11

In Michigan, 73% of the state’s population isserved by a community water system. Of theindividuals served by community water, 89.4%are being provided with adequately fluoridatedwater. This equates to 65.3% of Michiganresidents who are being served by a communitywater supply with adequately fluoridated water(MDEQ 2003). Nationally, 67% of thepopulation served by public water supplies isprovided with optimal fluoride levels forpreventing decay (CDC, 2004).
Figure 4 shows the proportion of persons servedby community water supplies who receiveadequate fluoridation levels by county. Fluoridelevels in Michigan will continue to be monitoredand reported by the Michigan Department ofEnvironmental Quality and, through coordinationwith the MDCH, Oral Health Program, the Water Fluoridation Reporting System (WFRS) will beencouraged. This system monitors the extent and consistency of water fluoridation.
School-Based or School-Linked Sealant ProgramsThe Michigan Oral Health Coalition recognizes that sealants are an effective method to prevent toothdecay. The coalition supports efforts by the Michigan Department of Community Health to implement aschool-based and school-linked sealant program in conjunction with coalition partners, including theSchool Community Health Alliance of Michigan.
Publicly Supported Dental ClinicsMichigan currently has 75 community based, publicly supported dental clinics. The number of clinicsgrew in Fiscal Year 2000 when the legislature appropriated $10.9 million for a one-time oral healthexpansion grant. This grant allowed for the uninsured and Medicaid beneficiaries in many communities
to access oral health services that had beendesperately needed. However, with theelimination of the adult oral health benefits forMedicaid enrollees in 2003, and the increased numberof persons without dental insurance, the infrastructuredeveloped in 2000 is in jeopardy. Clinics arereducing hours eliminating services, and laying offdedicated staff. Some clinics have recently beenforced to close.
The map to the left (Figure 5) shows each of thepublicly supported dental sites in Michigan today.The services provided at each site vary fromcleanings to restorations. Some provide services toonly children or adults, while others provide a full-range of oral health services to the community.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 12
Figure 4.
Figure 5.

Dental ProvidersAccording to 2004 MDCH dental licensing information, Michigan has 6,366 licensed dentists for anoverall population to dentist ratio of 1,561 to 1 (MDCH Licensing, 2004). The overall population todentist ratio is based on dentists licensed to practice in Michigan and is not adjusted for those who are notcurrently practicing in the state or who are working part-time.
There is a shortage of providers willing to serve low-income populations. According to the MichiganDepartment of Community Health, 8% of Michigan counties (7 out of 83 counties) have no enrolledMedicaid dentists (MDCH CDC, 2004). According to the same report, only 43% (36 out of 83) of thecounties have only one enrolled Medicaid dentist with paid claims above $10,000 per year. Sixty-fiveout of 83 Michigan counties are designated as a full or partial Health Professional Shortage Area (HPSA)for low income and Medicaid populations. A map showing the Dental Health Professional ShortageAreas (HPSAs) by county can be found below (HHS 2004).
Figure 6.
Nationally, specific racial and ethnic groups are underrepresented in dentistry compared to theirrepresentation in the population. According to the document, A National Call to Action to Promote OralHealth, African Americans comprise 2.2% of active dentists versus 12% of the population; Hispanicscomprise 2.8% of active dentists versus 10.7% of the population; Native Americans comprise 0.2% ofactive dentists versus 0.7% of the population (HHS, 2003). We believe a similar disparity exists inMichigan. The Workforce Workgroup is interested in exploring this further.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 13
Figure 7.
References & Sourcesfor Literature Review
American Academy of Periodontology (AAP). “Baby Steps to a Healthy Pregnancy and On-TimeDelivery,” June 2004. http://www.perio.org/consumer/pregnancy.htm
American Dental Hygienists' Association (ADHA). “Healthy Mouth, Healthy Body,” 2003.
Centers for Disease Control and Prevention. “Oral Health Resources,” 2004. http://www.cdc.gov/oralhealth/
Centers for Disease Control and Prevention. “Guidelines for Infection Control in Dental Health-CareSettings”, 2003. http://www.cdc.gov/OralHealth/infectioncontrol/guidelines/index.htm
Centers for Disease Control and Prevention. National Oral Health Surveillance System.http://www.cdc.gov/nohss/
Centers for Disease Control and Prevention. “Synopsis of State and Territorial Dental Health Programs.”http://www2a.cdc.gov/nccdphp/doh/synopses/index.asp
Eklund, Stephen. “Michigan Child Dental Coverage Validation Survey, 2003: Methodological Report.”
Michigan Department of Community Health (MDCH): Bureau of Health Professions, Dental Licensure,2004.
Michigan Department of Community Health (MDCH). “CDC Synopsis Questionnaire 2004.”
Michigan Department of Community Health (MDCH): Diabetes, Kidney and Other Chronic DiseaseSection, “Diabetes in Michigan.” June 2004.
Michigan Department of Community Health (MDCH). “Michigan Oral Health Surveillance,” EPIInsight, Spring 2004.
Michigan Department of Community Health (MDCH). “Oral Health 2002 Michigan Behavioral RiskFactor Surveillance Survey,” May 2003.
Michigan Department of Community Health (MDCH): Vital Statistics, 2003.
Michigan Department of Environmental Quality (MDEQ). “Community Water Supply Listings,” 2003.www.michigan.gov/deq
National Institute of Dental and Craniofacial Research (NIDCR), National Institutes of Health. “TheOral-Systemic Health Connection.”http://www.nidcr.nih.gov/HealthInformation/OralHealthInformationIndex/SpectrumSeries/OralSystemic.htm
University of Michigan School of Dentistry (U of M), Department of Cardiology, Restorative Sciencesand Endodontics. “Epidemiology of Oral Cancer in Michigan,” May 2003.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 14
U.S. Department of Health and Human Services. National Call to Action to Promote Oral Health, PublicHealth Services, National Institute of Health, National Institute of Dental and Craniofacial Research.NIH Publication No. 03-5303, Spring 2003.
U.S. Department of Health and Human Services, Health Resources & Services Administration, Bureau ofHealth Professions, Shortage Designation Branch. Health Professional Shortage Area Database, 2004.http://belize.hrsa.gov/newhpsa/newhpsa.cfm
US Department of Health and Human Services. “Oral Health in America: A Report of the SurgeonGeneral-- Executive Summary.” Rockville, MD: US Department of Health and Human Services, NationalInstitute of Dental and Craniofacial Research, National Institutes of Health, 2000.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 15
Summary of Recommendations
Data Workgroup Develop a statewide oral health surveillance system to provide a routine source of actionable data.Increase the sustainability of the statewide oral health surveillance system.Provide assistance in the collection and analysis of oral health data related to major policy changes and prevention and intervention initiatives.
Prevention,Education &AwarenessWorkgroup
Increase access to evidence-based prevention practices that maintain optimal oral health.Develop a statewide education program aimed at increasing knowledge about therelationship between oral health and systemic health.Assure the availability of comprehensive, culturally competent, oral health education resources for all ages as well as those designed to enhance patient involvement throughself management.Increase the education of non-dental health care providers on the importance of oral health. Encourage health care providers to discuss with patients the oral effects of tobacco use (cigarettes, cigars, pipes, and spit tobacco).
FundingWorkgroup
Create a Medicaid adult oral health benefit that ensures access to and is consistent with high quality of care standards.Support efforts to roll out Healthy Kids Dental as the preferred model for optimal oral health care in children with the gradual expansion to additional counties based on thosecounties with greatest need and funding availability.Develop a system of care that ensures access to oral health services for low-income uninsured populations. Support efforts of the other coalition work groups to assess resources needed to implement their initiatives.Ensure the successful implementation of the oral health plan through the acquisition ofneeded resources.
WorkforceWorkgroup
Increase access to oral health services in medically underserved communities and for medically underserved populations by allowing the provision of high-quality dental care through qualified health care providers.Develop and support incentive programs to attract oral health professionals tounderserved areas and to serve medically underserved populations. Create and maintain a process for assessing and responding to the supply of and demand for oral health professionals.Develop a dental director leadership position in state government or at the Michigan Department of Community Health to serve as the focal point of oral health activity for the state.Facilitate provider education and medical care facility access to improve oral health care for persons with special needs.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 16
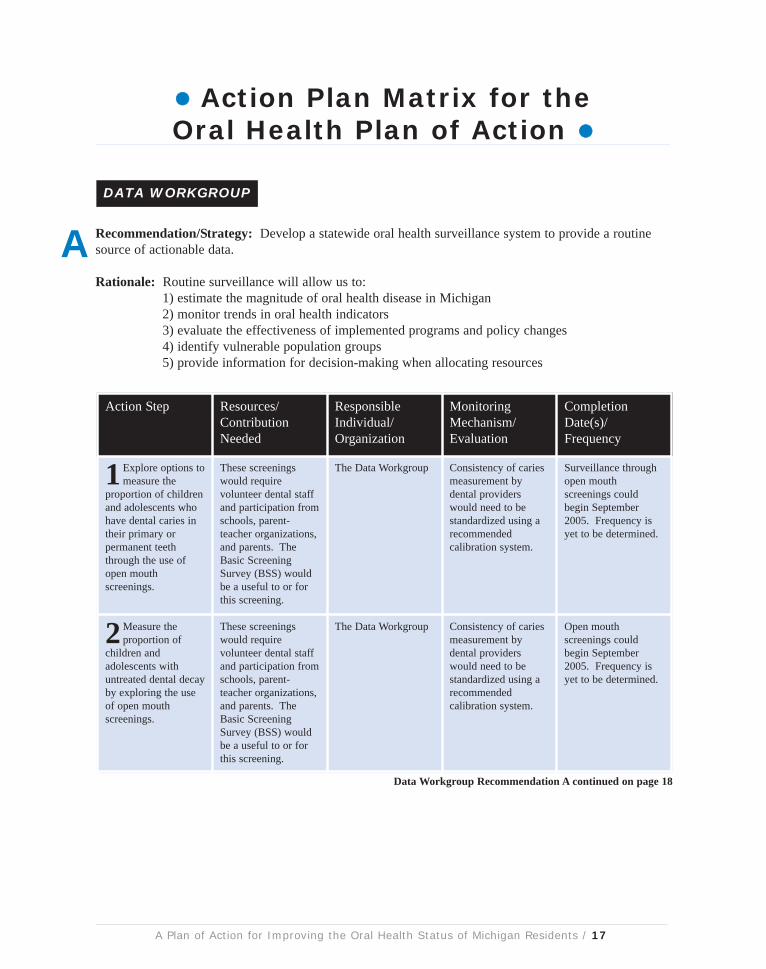
Action Plan Matrix for theOral Health Plan of Action
Recommendation/Strategy: Develop a statewide oral health surveillance system to provide a routinesource of actionable data.
Rationale: Routine surveillance will allow us to: 1) estimate the magnitude of oral health disease in Michigan2) monitor trends in oral health indicators3) evaluate the effectiveness of implemented programs and policy changes4) identify vulnerable population groups5) provide information for decision-making when allocating resources
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Explore options tomeasure the
proportion of childrenand adolescents whohave dental caries intheir primary orpermanent teeththrough the use ofopen mouthscreenings.
These screeningswould requirevolunteer dental staffand participation fromschools, parent-teacher organizations,and parents. TheBasic ScreeningSurvey (BSS) wouldbe a useful to or forthis screening.
The Data Workgroup Consistency of cariesmeasurement bydental providerswould need to bestandardized using arecommendedcalibration system.
Surveillance throughopen mouthscreenings couldbegin September2005. Frequency isyet to be determined.
2Measure theproportion of
children andadolescents withuntreated dental decayby exploring the useof open mouthscreenings.
These screeningswould requirevolunteer dental staffand participation fromschools, parent-teacher organizations,and parents. TheBasic ScreeningSurvey (BSS) wouldbe a useful to or forthis screening.
The Data Workgroup Consistency of cariesmeasurement bydental providerswould need to bestandardized using arecommendedcalibration system.
Open mouthscreenings couldbegin September2005. Frequency isyet to be determined.
DATA WORKGROUP
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 17
A
Data Workgroup Recommendation A continued on page 18
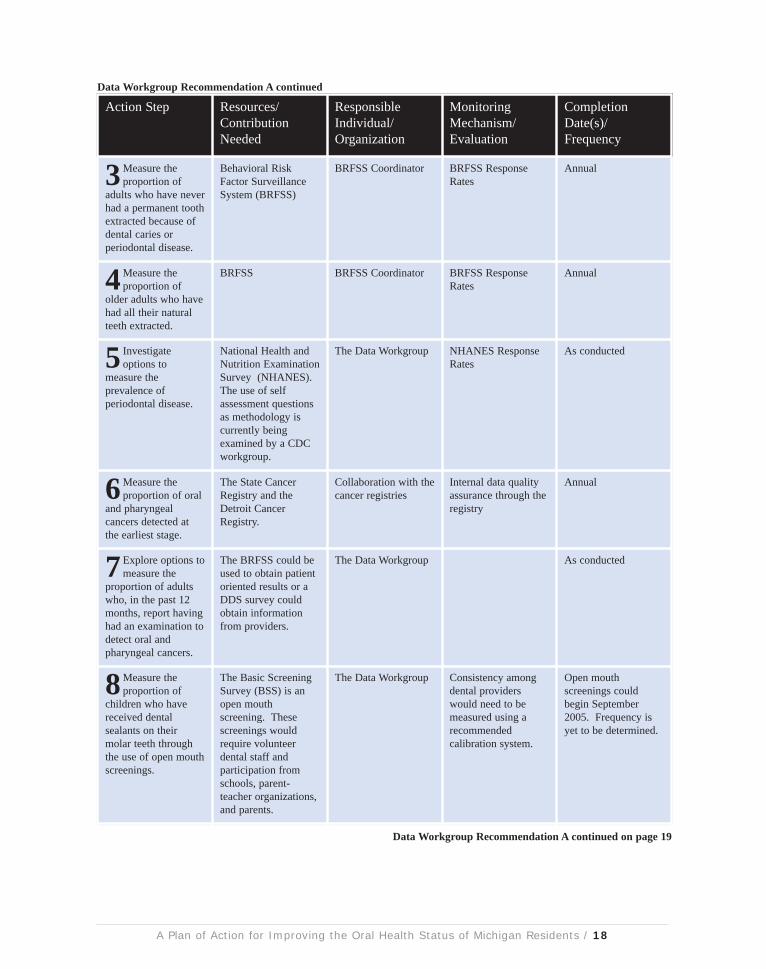
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
3Measure theproportion of
adults who have neverhad a permanent toothextracted because ofdental caries orperiodontal disease.
Behavioral RiskFactor SurveillanceSystem (BRFSS)
BRFSS Coordinator BRFSS ResponseRates
Annual
4Measure theproportion of
older adults who havehad all their naturalteeth extracted.
BRFSS BRFSS Coordinator BRFSS ResponseRates
Annual
5 Investigateoptions to
measure theprevalence ofperiodontal disease.
National Health andNutrition ExaminationSurvey (NHANES). The use of selfassessment questionsas methodology iscurrently beingexamined by a CDCworkgroup.
The Data Workgroup NHANES ResponseRates
As conducted
6Measure theproportion of oral
and pharyngealcancers detected atthe earliest stage.
The State CancerRegistry and theDetroit CancerRegistry.
Collaboration with thecancer registries
Internal data qualityassurance through theregistry
Annual
7 Explore options tomeasure the
proportion of adultswho, in the past 12months, report havinghad an examination todetect oral andpharyngeal cancers.
The BRFSS could beused to obtain patientoriented results or aDDS survey couldobtain informationfrom providers.
The Data Workgroup As conducted
8Measure theproportion of
children who havereceived dentalsealants on theirmolar teeth throughthe use of open mouthscreenings.
The Basic ScreeningSurvey (BSS) is anopen mouthscreening. Thesescreenings wouldrequire volunteerdental staff andparticipation fromschools, parent-teacher organizations,and parents.
The Data Workgroup Consistency amongdental providerswould need to bemeasured using arecommendedcalibration system.
Open mouthscreenings couldbegin September2005. Frequency isyet to be determined.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 18
Data Workgroup Recommendation A continued
Data Workgroup Recommendation A continued on page 19

Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
9Measure theproportion of the
Michigan populationserved by communitywater systems withoptimally fluoridatedwater.
The MichiganDepartment ofEnvironmentalQuality (DEQ) canprovide informationon community watersupplies, includingthose artificiallyfluoridated, and theEnvironmentalProtection Agency(EPA) providesinformation onnaturally fluoridatedcommunity watersupplies.
DEQ and EPA Internal monitoringmechanisms
Annual
10Measure theproportion of
children and adultswho use the oralhealth care systemeach year throughreview of claims data.
Claims data fromprivate insurers andMedicaid. Adultinformation can bethrough the BRFSSfor adults. Care pro-vided to the uninsuredthrough safety netdental programs willalso be examined.
The Data Workgroupand the BRFSSCoordinator
Annual
11Measure theproportion of
long-term careresidents who use theoral health caresystem each year.
Minimum Data Setfor Home CareSurvey. The work-group might alsoexamine additionalresources to identifyoral disease amonglong-term careresidents, as the MDSis not an accurate toolfor this assessment.
Collaborationbetween theCommunity andHome-Based WaiverProgram and the DataWorkgroup
This survey has beenpreviously validatedas a measurement foruse of the oral healthcare system
Annual
12Measure theproportion of
low-income childrenand adolescents whoreceived any preven-tive dental serviceduring the past year.
Medicaid claims data MDCH Annual
13Measure theproportion of
school-based healthcenters with an oralhealth component.
Survey of school-based health centers
School HealthAlliance
As conducted (every2 years)
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 19
Data Workgroup Recommendation A continued
Data Workgroup Recommendation A continued on page 20
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
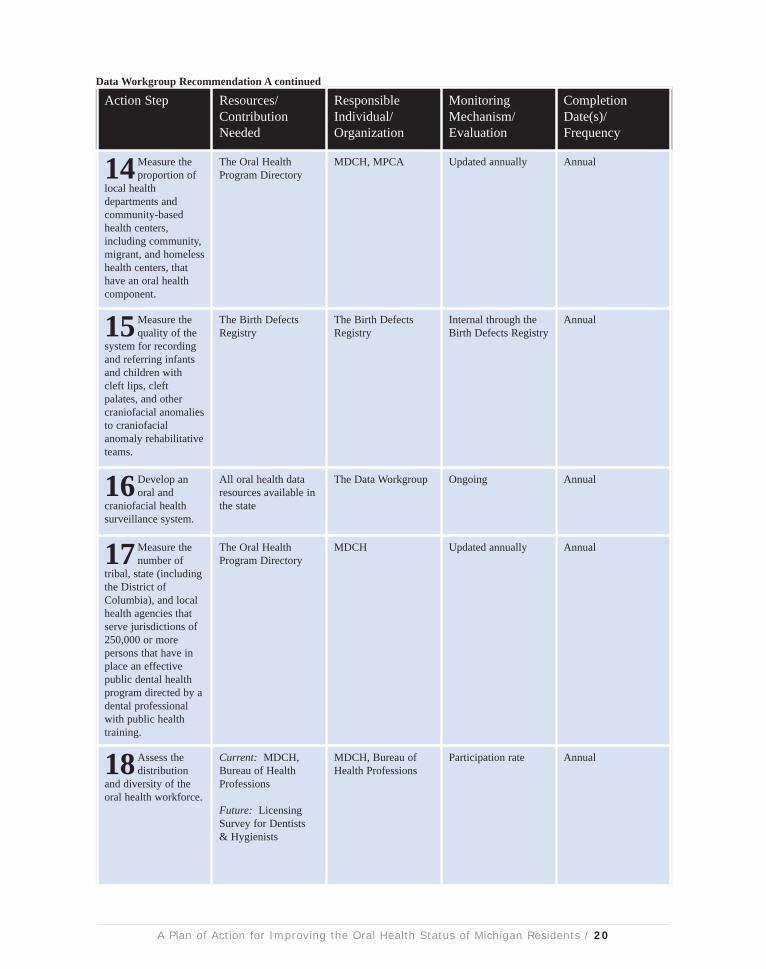
14Measure theproportion of
local healthdepartments andcommunity-basedhealth centers,including community,migrant, and homelesshealth centers, thathave an oral healthcomponent.
The Oral HealthProgram Directory
MDCH, MPCA Updated annually Annual
15Measure thequality of the
system for recordingand referring infantsand children withcleft lips, cleftpalates, and othercraniofacial anomaliesto craniofacialanomaly rehabilitativeteams.
The Birth DefectsRegistry
The Birth DefectsRegistry
Internal through theBirth Defects Registry
Annual
16Develop anoral and
craniofacial healthsurveillance system.
All oral health dataresources available inthe state
The Data Workgroup Ongoing Annual
17Measure thenumber of
tribal, state (includingthe District ofColumbia), and localhealth agencies thatserve jurisdictions of250,000 or morepersons that have inplace an effectivepublic dental healthprogram directed by adental professionalwith public healthtraining.
The Oral HealthProgram Directory
MDCH Updated annually Annual
18Assess thedistribution
and diversity of theoral health workforce.
Current: MDCH,Bureau of HealthProfessions
Future: LicensingSurvey for Dentists& Hygienists
MDCH, Bureau ofHealth Professions
Participation rate Annual
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 20
Data Workgroup Recommendation A continued

Recommendation/Strategy: Increase the sustainability of the statewide oral health surveillance system.
Rationale: A surveillance system should be feasible, adaptable, representative, and acceptable.A passive surveillance system should work towards minimizing resource costs while maximizing dataquality and stability yet remain adaptable to changing needs.
Recommendation/Strategy: Provide assistance in the collection and analysis of oral health data relatedto major policy changes and prevention and intervention initiatives.
Rationale: Policy changes related to oral health can have both positive and negative implications for theoral health status of Michigan residents. Measuring the effect of these changes is necessary in order todevelop sound oral health policy. The impact of these changes cannot always be identified by theproposed surveillance system.
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Enlist thecooperation of
dental insuranceproviders in obtaininginformation regardingutilization of dentalservices.
Dental insuranceproviders, MDCH
MDCH Participation byinsurers and quality ofinformation provided
November 2005
2 Exploreintegration of
technologicalalternatives to oralhealth screenings forfuture statewidesurveillance measures(e.g. the use ofElectronic MedicalRecords).
Data Workgroup Data Workgroup Methodology isdeveloped for majorpolicy changes and/orstatewide initiatives
Ongoing
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Coordinate withthe MDCH Oral
Health ProgramCoordinator tomonitor policychanges and newprevention and inter-vention initiatives.
MDCH Oral HealthProgram Coordinator
MDCH Oral HealthEpidemiologist
Policy changes andinitiatives are broughtto the DataWorkgroup fordiscussion.
Ongoing
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 21
B
C
Data Workgroup Recommendation C continued on page 22

Recommendation/Strategy: Increase access to evidence-based preventive practices that maintainoptimal oral health.
Rationale: There are a number of safe, evidence-based methods to prevent dental caries, includingnutrition education, sealants, water fluoridation, and fluoride varnishes.
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
2 Collect andanalyze
information related tothe changes.
Varied byintervention/policychange. The MDCHData Warehouse.
Data Workgroup Analysis is completedfor major policychanges and/orstatewide initiatives
Ongoing
PREVENTION, EDUCATION, & AWARENESS WORKGROUP
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Supportcommunities in
efforts to maintainand implementoptimal levels ofwater fluoridation.
MDA, DEQ, MDCH MDCH Percent ofcommunities withoptimally fluoridatedwater is maintained orincreased
Ongoing
2 Support efforts byMDCH to
implement a schoolrinse program innon-fluoridatedcommunities.
Funding, coordinator MDCH Oral HealthLead
School rinse programis implemented
Ongoing
3 Support efforts byMDCH to
implement a school-based school-linkedsealant program.
Funding, coordinator,equipment, localhealth departments,and school-basedhealth centers
MDCH Oral HealthLead
School-based school-linked sealantprogram isimplemented
June 2007
4 Support efforts byMDCH to
implement theapplication of fluoridevarnishes during thewell child visits.
Ensure this isallowable under thescope of practice forphysicians and nursesand check withinsurance companiesto insure that theywill accept dentalcodes from medicalproviders.
MDCH Fluoride varnishes areincorporated into wellchild visits accordingto annual query ofinsurance claims byMDCH
June 2006
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 22
A
Data Workgroup Recommendation C continued
Prevention, Education, & Awareness Workgroup Recommendation A continued on page 23

Recommendation/Strategy: Develop a statewide education program aimed at increasing knowledgeabout the relationship between oral health and systemic health.
Rationale: Oral health is essential to systemic health. When developing health policy, oral health mustbe considered primary care.
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
5 Evaluate theeffectiveness for
improving oral healthby mandating an oralhealth exam prior toentrance intokindergarten.
Research on otherareas that this hasbeen done for and itseffectiveness
Delta Dental, MDCH Study of effectivenessis completed
August 2007
6 Explorepreventive
practices for prenataland postpartum oralhealth care.
Research of bestpractices
MDCH Oral HealthProgram Coordinator
Research completedand recommendationsmade to the coalition
June 2007
7 Provide trainingon the CDC’s
Guidelines forInfection Control inDental HealthSettings.
The CDC guidelinesas a model, the oralhealth conference as atraining venue
MDCH Oral HealthProgram Coordinator
Training provided June 2007
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Coordinate astatewide public
education andawareness campaign.
MDCH, Delta Dental,Blue Cross BlueShield, privateindustry partners,local broadcasting andother media
MDCH Oral HealthProgram Coordinatorand partnership withinsurers and privateindustry
Public relations planand campaigndeveloped
CY 2005 and thenannually
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 23
B
Prevention, Education, & Awareness Workgroup Recommendation A continued
Prevention, Education, & Awareness Workgroup Recommendation B continued on page 24
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
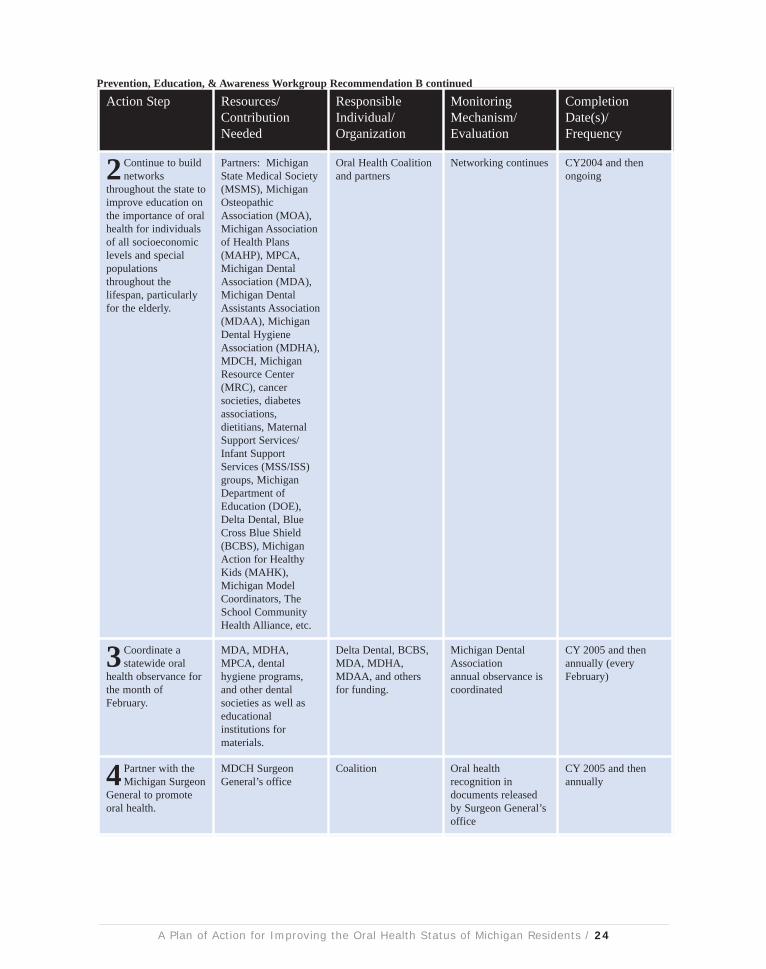
2 Continue to buildnetworks
throughout the state toimprove education onthe importance of oralhealth for individualsof all socioeconomiclevels and specialpopulationsthroughout thelifespan, particularlyfor the elderly.
Partners: MichiganState Medical Society(MSMS), MichiganOsteopathicAssociation (MOA),Michigan Associationof Health Plans(MAHP), MPCA,Michigan DentalAssociation (MDA),Michigan DentalAssistants Association(MDAA), MichiganDental HygieneAssociation (MDHA),MDCH, MichiganResource Center(MRC), cancersocieties, diabetesassociations,dietitians, MaternalSupport Services/Infant SupportServices (MSS/ISS)groups, MichiganDepartment ofEducation (DOE),Delta Dental, BlueCross Blue Shield(BCBS), MichiganAction for HealthyKids (MAHK),Michigan ModelCoordinators, TheSchool CommunityHealth Alliance, etc.
Oral Health Coalitionand partners
Networking continues CY2004 and thenongoing
3 Coordinate astatewide oral
health observance forthe month ofFebruary.
MDA, MDHA,MPCA, dentalhygiene programs,and other dentalsocieties as well aseducationalinstitutions formaterials.
Delta Dental, BCBS,MDA, MDHA,MDAA, and othersfor funding.
Michigan DentalAssociationannual observance iscoordinated
CY 2005 and thenannually (everyFebruary)
4 Partner with theMichigan Surgeon
General to promoteoral health.
MDCH SurgeonGeneral’s office
Coalition Oral healthrecognition indocuments releasedby Surgeon General’soffice
CY 2005 and thenannually
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 24
Prevention, Education, & Awareness Workgroup Recommendation B continued

Recommendation/Strategy: Assure the availability of comprehensive, culturally competent, oral healtheducation resources for all ages as well as those designed to enhance patient involvement through selfmanagement.
Rationale: In order to increase awareness about the importance of oral health, age appropriateinformation should be provided to health professionals, parents, teachers, etc.
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Partner with HeadStart agencies in
their project to ensureoral health educationand preventionactivities areavailable.
Curriculadevelopment, staffcoordination
Michigan Head StartAssociation
Materials areavailable
December 2005
2 Identify existinghealth resource
clearinghouses fordissemination ofelectronic informationand written materials,particularly for oralhealth. (e.g., thePrevention ResourceCenter).
Coalition Existing resourcesidentified
September 2005
3 Identify fundingfor a clearing-
house of oral healthmaterials that woulddirect people toappropriate resources.
Funding for staffingand technology,distribution ofmaterials, etc.
Coalition Funding is obtained March 2006
4 Establish theclearinghouse for
oral health.
Funding for staffingand technology,distribution ofmaterials, etc.
Coalition The clearinghouse isestablished
September 2006
5 Provideinformation on
the availability of theclearinghouse as aresource to healthproviders, educators,etc.
Brochures, web linksto other commonlyvisited websites
MPCA, MDCH, TheMichigan EducationAssociation (MEA),Michigan’s SurgeonGeneral, Oral HealthCoalition members
Increase in the use ofthe clearinghouse
September 2006and ongoing
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 25
C
Prevention, Education, & Awareness Workgroup Recommendation C continued on page 26

Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
6Work with theDepartment of
Education to continueoral health modules inschool curriculum.
The Michigan Model Department ofEducation, MDCH,and Education &Awareness Workgroup
Oral health modulesare continued
Ongoing
7 Provide a selfmanagement
curriculum focused onoral health to Women,Infant and Children(WIC) providers;Maternal SupportServices/InfantSupport Services(MSS/ISS) providers;Children’s SpecialHealth Care Services(CSHCS); School-based health centers;after school day carecenters; and summercare programs.
Department ofEducation and MDCH
Curriculum isprovided
Ongoing
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 26
Prevention, Education, & Awareness Workgroup Recommendation C continued
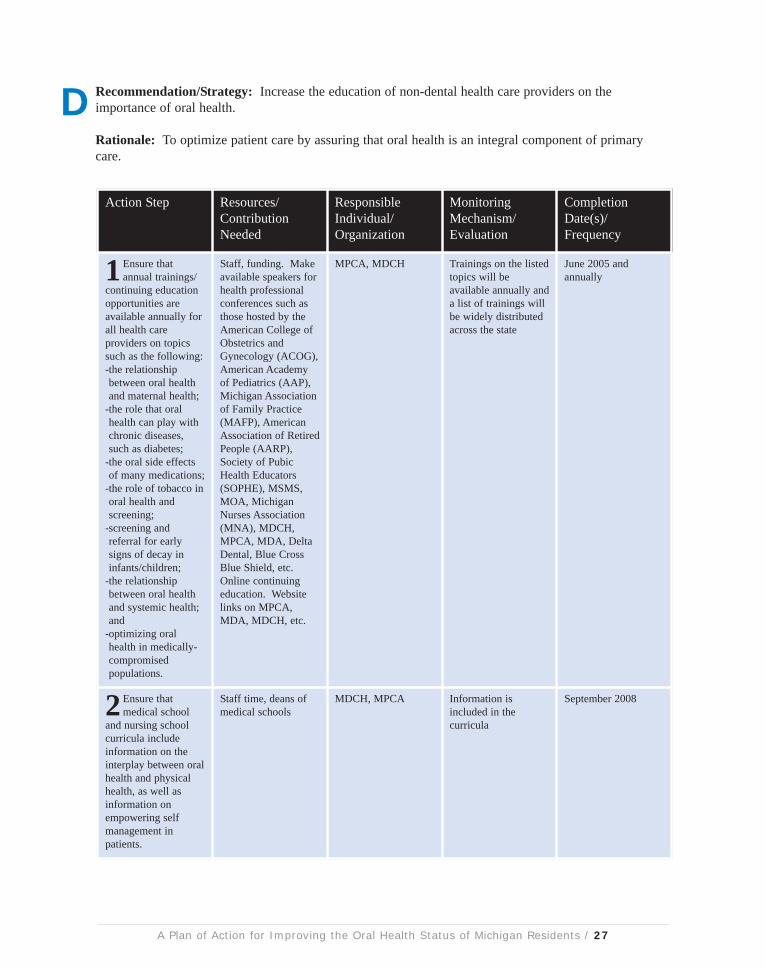
Recommendation/Strategy: Increase the education of non-dental health care providers on theimportance of oral health.
Rationale: To optimize patient care by assuring that oral health is an integral component of primarycare.
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Ensure thatannual trainings/
continuing educationopportunities areavailable annually forall health careproviders on topicssuch as the following:-the relationshipbetween oral healthand maternal health;
-the role that oralhealth can play withchronic diseases,such as diabetes;
-the oral side effectsof many medications;
-the role of tobacco inoral health andscreening;
-screening andreferral for earlysigns of decay ininfants/children;
-the relationshipbetween oral healthand systemic health;and
-optimizing oralhealth in medically-compromisedpopulations.
Staff, funding. Makeavailable speakers forhealth professionalconferences such asthose hosted by theAmerican College ofObstetrics andGynecology (ACOG),American Academyof Pediatrics (AAP),Michigan Associationof Family Practice(MAFP), AmericanAssociation of RetiredPeople (AARP),Society of PubicHealth Educators(SOPHE), MSMS,MOA, MichiganNurses Association(MNA), MDCH,MPCA, MDA, DeltaDental, Blue CrossBlue Shield, etc.Online continuingeducation. Websitelinks on MPCA,MDA, MDCH, etc.
MPCA, MDCH Trainings on the listedtopics will beavailable annually anda list of trainings willbe widely distributedacross the state
June 2005 andannually
2 Ensure thatmedical school
and nursing schoolcurricula includeinformation on theinterplay between oralhealth and physicalhealth, as well asinformation onempowering selfmanagement inpatients.
Staff time, deans ofmedical schools
MDCH, MPCA Information isincluded in thecurricula
September 2008
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 27
D
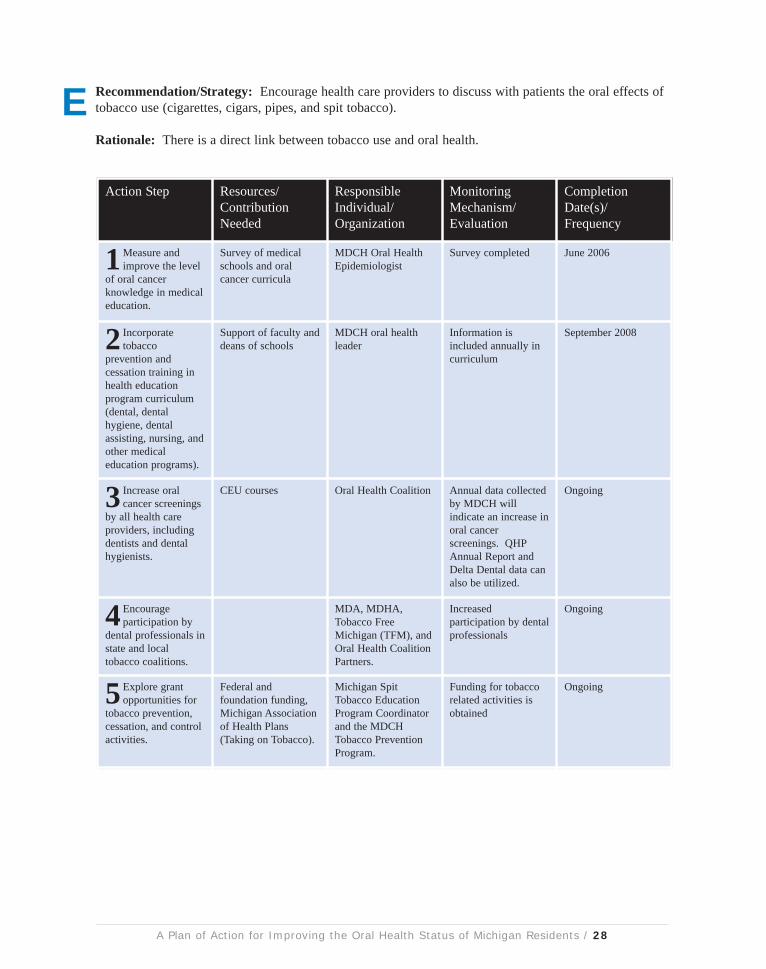
Recommendation/Strategy: Encourage health care providers to discuss with patients the oral effects oftobacco use (cigarettes, cigars, pipes, and spit tobacco).
Rationale: There is a direct link between tobacco use and oral health.
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1Measure andimprove the level
of oral cancerknowledge in medicaleducation.
Survey of medicalschools and oralcancer curricula
MDCH Oral HealthEpidemiologist
Survey completed June 2006
2 Incorporatetobacco
prevention andcessation training inhealth educationprogram curriculum(dental, dentalhygiene, dentalassisting, nursing, andother medicaleducation programs).
Support of faculty anddeans of schools
MDCH oral healthleader
Information isincluded annually incurriculum
September 2008
3 Increase oralcancer screenings
by all health careproviders, includingdentists and dentalhygienists.
CEU courses Oral Health Coalition Annual data collectedby MDCH willindicate an increase inoral cancerscreenings. QHPAnnual Report andDelta Dental data canalso be utilized.
Ongoing
4 Encourageparticipation by
dental professionals instate and localtobacco coalitions.
MDA, MDHA,Tobacco FreeMichigan (TFM), andOral Health CoalitionPartners.
Increasedparticipation by dentalprofessionals
Ongoing
5 Explore grantopportunities for
tobacco prevention,cessation, and controlactivities.
Federal andfoundation funding,Michigan Associationof Health Plans(Taking on Tobacco).
Michigan SpitTobacco EducationProgram Coordinatorand the MDCHTobacco PreventionProgram.
Funding for tobaccorelated activities isobtained
Ongoing
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 28
E

Recommendation/Strategy: Create a Medicaid adult oral health benefit that ensures access to and isconsistent with high quality of care standards.
Rationale: Research has shown that poor oral health has a tremendous impact on an individual’s overallhealth. Poor oral health has been linked to health problems such as pre-term births, uncontrolleddiabetes, and heart disease. The elimination of the adult dental benefit will result in increased Medicaidmedical costs since the services sought by individuals unable to get appropriate dental services are stillcovered by the Medicaid program.
FUNDING WORKGROUP
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Reinstate aMedicaid adult
dental benefit.
$10 million in generalfund dollars
MDCH, Coalition Benefit is reinstated Fiscal Year 2007
2 Implement aneffective and
efficient adultMedicaid dentalbenefit that providesmeaningful access byincreasing providerreimbursement andencouraging providerparticipation.
Will be determinedbased on plans
MDCH, MDA,MALPH, MPCA,Coalition
Primary: Utilization,provider participation
Secondary: Bi-annualreview of paymentrates compared toUCR
Phase-in completedby Fiscal Year 2009
3 EncourageMDCH to provide
the local matchrequired for localhealth departments toaccess Title V dollars.
$1.2 million Dental Clinics North,MALPH
State funds providedfor local match
Fiscal Year 2006
4Work with theMDCH to modify
the Medicaid oralhealth benefits toreflect the currentstandards of practice.
Staff time Michigan DentalAssociation
Benefit reflectscurrent standards ofpractice
Fiscal Year 2007
5 Support efforts tomandate oral
health as part of theMedicaid package.
Commitment and stafftime
MPCA will work withNACHC and theASTDD; MDA willwork with ADA;MDHA will workwith the ADHA
Dental services are amandatory benefit forMedicaid
Fiscal Year 2007
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 29
A
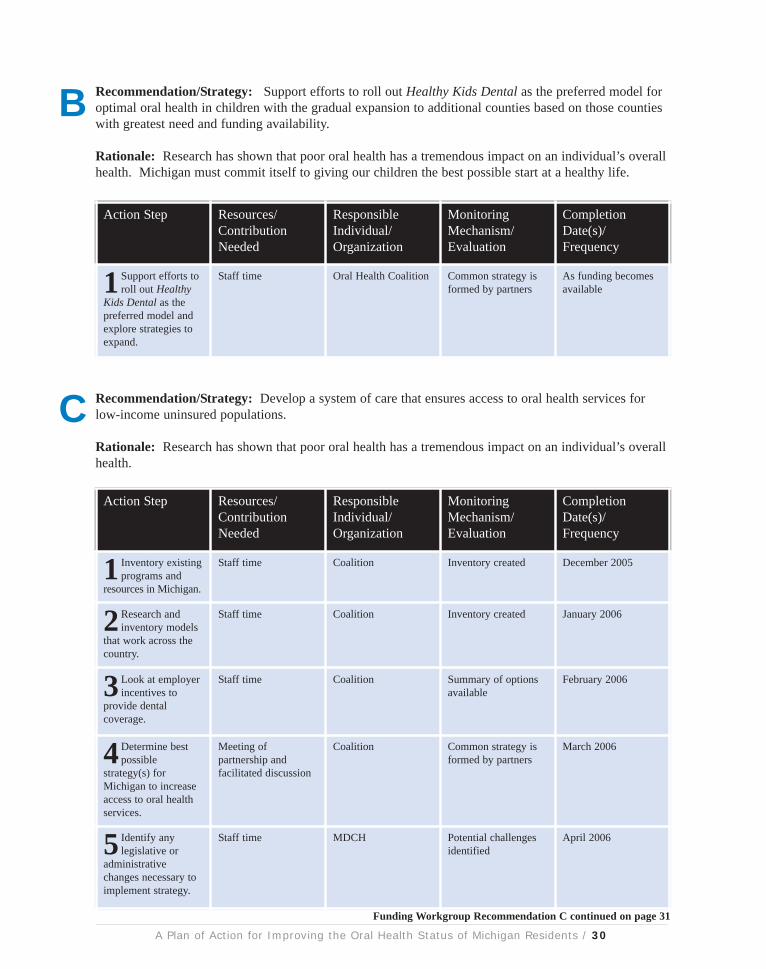
Recommendation/Strategy: Support efforts to roll out Healthy Kids Dental as the preferred model foroptimal oral health in children with the gradual expansion to additional counties based on those countieswith greatest need and funding availability.
Rationale: Research has shown that poor oral health has a tremendous impact on an individual’s overallhealth. Michigan must commit itself to giving our children the best possible start at a healthy life.
Recommendation/Strategy: Develop a system of care that ensures access to oral health services forlow-income uninsured populations.
Rationale: Research has shown that poor oral health has a tremendous impact on an individual’s overallhealth.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 30
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Support efforts toroll out Healthy
Kids Dental as thepreferred model andexplore strategies toexpand.
Staff time Oral Health Coalition Common strategy isformed by partners
As funding becomesavailable
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Inventory existingprograms and
resources in Michigan.
Staff time Coalition Inventory created December 2005
2 Research andinventory models
that work across thecountry.
Staff time Coalition Inventory created January 2006
3 Look at employerincentives to
provide dentalcoverage.
Staff time Coalition Summary of optionsavailable
February 2006
4Determine bestpossible
strategy(s) forMichigan to increaseaccess to oral healthservices.
Meeting ofpartnership andfacilitated discussion
Coalition Common strategy isformed by partners
March 2006
5 Identify anylegislative or
administrativechanges necessary toimplement strategy.
Staff time MDCH Potential challengesidentified
April 2006
B
C
Funding Workgroup Recommendation C continued on page 31
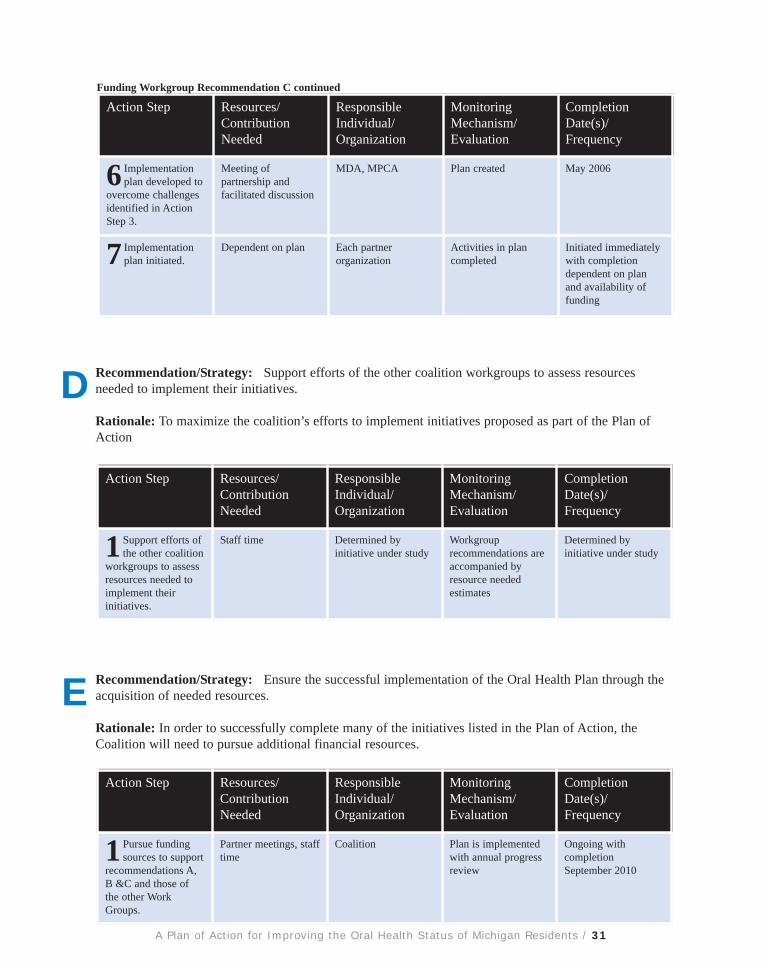
Recommendation/Strategy: Support efforts of the other coalition workgroups to assess resourcesneeded to implement their initiatives.
Rationale: To maximize the coalition’s efforts to implement initiatives proposed as part of the Plan ofAction
Recommendation/Strategy: Ensure the successful implementation of the Oral Health Plan through theacquisition of needed resources.
Rationale: In order to successfully complete many of the initiatives listed in the Plan of Action, theCoalition will need to pursue additional financial resources.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 31
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
6 Implementationplan developed to
overcome challengesidentified in ActionStep 3.
Meeting ofpartnership andfacilitated discussion
MDA, MPCA Plan created May 2006
7 Implementationplan initiated.
Dependent on plan Each partnerorganization
Activities in plancompleted
Initiated immediatelywith completiondependent on planand availability offunding
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Support efforts ofthe other coalition
workgroups to assessresources needed toimplement theirinitiatives.
Staff time Determined byinitiative under study
Workgrouprecommendations areaccompanied byresource neededestimates
Determined byinitiative under study
D
Funding Workgroup Recommendation C continued
E
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Pursue fundingsources to support
recommendations A,B &C and those ofthe other WorkGroups.
Partner meetings, stafftime
Coalition Plan is implementedwith annual progressreview
Ongoing withcompletionSeptember 2010

Recommendation/Strategy: Increase access to oral health services in medically underservedcommunities and for underserved populations by allowing the provision of high quality dental carethrough qualified health care providers.
Rationale: There is a serious shortage of dentists willing to care for the uninsured and publicly insuredpopulations. In addition, a number of communities lack enough dentists to care for even thecommercially insured population. This strategy will allow us to increase the number of people whoreceive regular, high quality oral health care from qualified professionals.
WORKFORCE WORKGROUP
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Inquire withpotential partners
to identify willingnessto participate.
Staff time Coalition Partnership formed Ongoing
2 Researchapproaches used
by other states toaddress access issueswith currentworkforce.
Staff time Coalition Assessmentcompleted
September 2006
3Develop a plan toaddress issues
identified in surveycompleted by DataWorkgroup.
MDA, MDHA,MDAA, MPCA
Coalition Plan is developed July 2007
4 Identify anylegislative or
administrativechanges necessary toimplement strategy.
Staff time Coalition Potential challengesidentified
July 2007
5 Implement plan. MDA, MDHA,MDAA, MPCA
Coalition Plan implemented,annual review
July 2008
6 Periodicevaluation of
progress andmodification ofstrategies and/orimplementation planmade as appropriate.
MDA, MDHA,MDAA, MPCA
Coalition Quarterly meetings ofthe partnership
Ongoing
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 32
A

Recommendation/Strategy: Develop and support incentive programs to attract oral health careprofessionals to underserved areas and to serve the medically underserved populations.
Rationale: There is a serious shortage of dentists willing to care for the uninsured and publicly insuredpopulations. In addition, a number of communities lack the dentists to care for even the commerciallyinsured population. This strategy will allow us to increase the number of people who receive regular,high quality oral health care from qualified professionals.
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Inventory existingstate and federal
incentive programsand include benefits/limitations and impactinformation.
Staff time Coalition Inventory created August 2006
2 Researchapproaches used
by other states toaddress access issueswith incentiveprograms.
Staff time MPCA Summary of creativeapproaches
October 2006
3Determination ofbest possible
strategy(s) forMichigan.
Meeting ofworkgroup andfacilitated discussion
Coalition Common strategy isidentified
November 2006
4 Identify andsupport legislative
or administrativechanges necessary toimplement changes toexisting programs orcreate new ones.
Staff time Coalition Potential challengesidentified
January 2006
5 Implement plan. MDA, MDHA,MDAA, MPCA
Coalition Plan created March 2007
6 Periodicevaluation of
progress andmodification ofstrategies and/orimplementation planmade as appropriate.
Meeting ofpartnership andfacilitated discussion
MPCA Quarterly meetings ofthe partnership
Ongoing
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 33
B

Recommendation/Strategy: Create and maintain a process for assessing and responding to the supplyof and demand for oral health professionals.
Rationale: Very little quantifiable information is gathered and analyzed on the amount of oral healthresources currently available. Until we can determine what we already have, it will be difficult to gatherenough momentum to change the system to better meet our needs.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 34
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Inventory otherstates’ approaches
for monitoringworkforce supplyand/or demand.
Staff time Michigan HealthCouncil
Inventory created July 2006
2 Estimateresources required
to implement mostpromising processesidentified in ActionStep 1.
Staff time MDCH, MichiganHealth Council
Resources estimatedfor most promisingprocesses
August 2006
3Determination ofbest possible
process(s) forMichigan.
Meeting ofwork group andfacilitated discussion
Coalition Best process forMichigan is identified
September 2006
4 Identify anylegislative or
administrativechanges necessary toimplement identifiedstrategy.
Staff time Coalition Potential challengesidentified
November 2006
5Develop plan. Staff time MDCH Plan created March 2007
6 Implement plan. Dependent on plan Each partnerorganization
Activities in plancompleted
Annually
C

Recommendation/Strategy: Develop a dental director leadership position in state government or at theMichigan Department of Community Health to serve as the focal point of oral health activity for thestate.
Rationale: There is a lack of leadership in oral health within the State of Michigan administration thatcan effectively work with all components of the health care system and professional training programs.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 35
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Initiateconversations
with MDCHadministrationregarding coalition’ssupport for a dentaldirector.
Staff time Michigan PublicHealth Association -Oral Health Section
Conversations began January 2006
2Develop thecoalition’s
qualifications for thedental directorposition.
Staff time Michigan PublicHealth Association -Oral Health Section
Wish list created January 2006
3 Support a dentaldirector
leadership position instate governmentwhich has the powerand authority forpolicy developmentand implementation.
Meetings MPHA, MDA,Coalition
Position establishedand filled withqualified candidate
October 2007
D
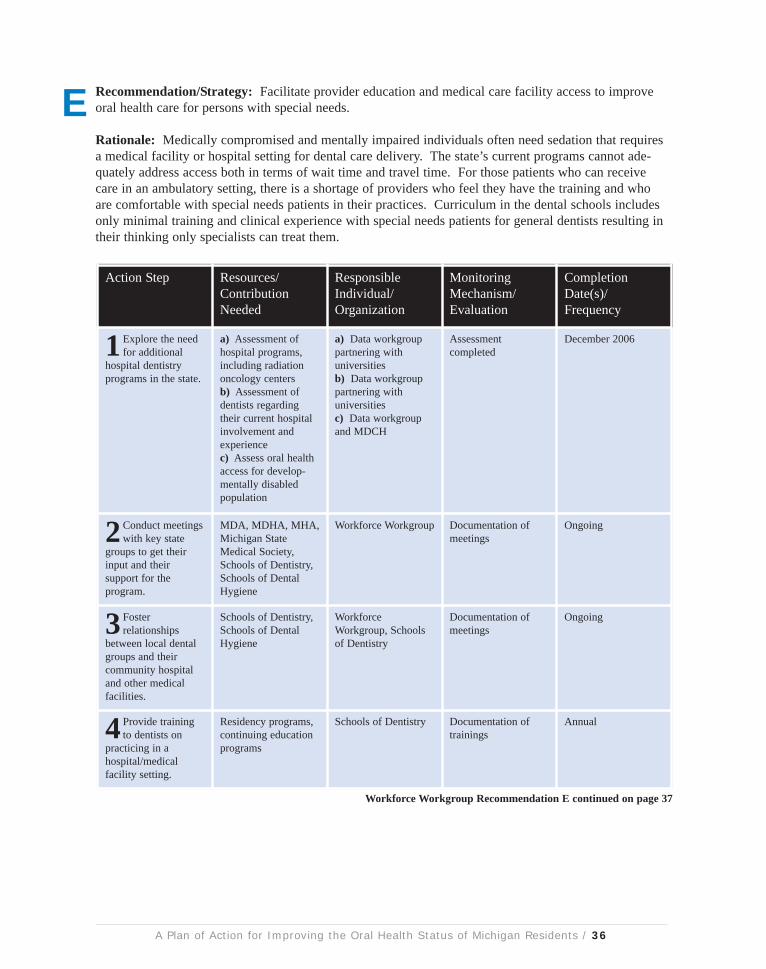
Recommendation/Strategy: Facilitate provider education and medical care facility access to improveoral health care for persons with special needs.
Rationale: Medically compromised and mentally impaired individuals often need sedation that requiresa medical facility or hospital setting for dental care delivery. The state’s current programs cannot ade-quately address access both in terms of wait time and travel time. For those patients who can receivecare in an ambulatory setting, there is a shortage of providers who feel they have the training and whoare comfortable with special needs patients in their practices. Curriculum in the dental schools includesonly minimal training and clinical experience with special needs patients for general dentists resulting intheir thinking only specialists can treat them.
A Plan of Action for Improving the Oral Health Status of Michigan Residents / 36
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
1 Explore the needfor additional
hospital dentistryprograms in the state.
a) Assessment ofhospital programs,including radiationoncology centersb) Assessment ofdentists regardingtheir current hospitalinvolvement andexperiencec) Assess oral healthaccess for develop-mentally disabledpopulation
a) Data workgrouppartnering withuniversitiesb) Data workgrouppartnering withuniversitiesc) Data workgroupand MDCH
Assessmentcompleted
December 2006
2 Conduct meetingswith key state
groups to get theirinput and theirsupport for theprogram.
MDA, MDHA, MHA,Michigan StateMedical Society,Schools of Dentistry,Schools of DentalHygiene
Workforce Workgroup Documentation ofmeetings
Ongoing
3 Fosterrelationships
between local dentalgroups and theircommunity hospitaland other medicalfacilities.
Schools of Dentistry,Schools of DentalHygiene
WorkforceWorkgroup, Schoolsof Dentistry
Documentation ofmeetings
Ongoing
4 Provide trainingto dentists on
practicing in ahospital/medicalfacility setting.
Residency programs,continuing educationprograms
Schools of Dentistry Documentation oftrainings
Annual
E
Workforce Workgroup Recommendation E continued on page 37

A Plan of Action for Improving the Oral Health Status of Michigan Residents / 37
Action Step Resources/ContributionNeeded
ResponsibleIndividual/Organization
MonitoringMechanism/Evaluation
CompletionDate(s)/Frequency
5 Provideinformation to
dentists in areas ofhospital protocol,credentialing, billingmedically-relatedcare, etc. that willencourage theirinvolvement.
a) Residencyprograms, continuingeducation programsb) Handbook toprovide informationto others on how it'sdone
Schools of Dentistry Documentation oftraining materialdevelopment anddistribution
Ongoing
6 Provide trainingand education
programs for dentalhygienists and dentalassistants practicingin public health andhospital/medicalfacility settings.
Continuing education,curriculumdevelopment,off-campus placement
Schools of DentalHygiene and DentalAssisting TrainingPrograms
Documentation oftrainings
Annual
7 Seek financial andlegislative support
for the developmentof additionalgeographicallydiverse medicalfacilities.
Meetings with MDA,MHA, Michigan StateMedical Society, andSchools of Dentistry;staff time
Schools of Dentistry Documentation ofmeetings
December 2006
8 Provide trainingto providers on
treating special needspatients in anambulatory settingthrough onlinecourses and othercontinuing education.
Staff time Schools of Dentistry,MDA, Schools ofDental Hygiene
Documentation ofmaterials andtrainings completed
December 2006
9 Identify networkof providers who
will accept specialneeds patients in theirpractice.
Meetings with MDAto discuss surveydevelopment andimplementation. Stafftime.
WorkforceWorkgroup, Schoolsof Dentistry, Schoolsof Dental Hygiene
Development of thenetwork
December 2007
10Meet with theSchools of
Dentistry to discusschanges in thecurriculum andincreased clinicalexperience for dentalstudents to improvetheir aptitude fortreating special needspatients.
Staff time Workforce Workgroup Documentation ofmeetings
December 2006
Workforce Workgroup Recommendation E continued





























