Embed Size (px)
Citation preview

1
A Practical Approach to Managing Metabolic Complications in Children
Treated with Second Generation Antipsychotics
Dina Panagiotopoulos, MD, FRCPCClinical Professor of Pediatrics, UBC
Endocrinologist, BC Children’s HospitalMedical Director, Provincial Mental Health Metabolic Program
Disclosures
None
Learning Objectives
• Participants will become familiar with the Canadian Alliance for Monitoring Effectiveness and Safety of Antipsychotics in Children (CAMESA) Management Guidelines*
• Participants will utilize and apply the CAMESA Management Guidelines in the clinical setting
*Ho, J., Panagiotopoulos, C., McCrindle, B., Grisaru, S. & Pringsheim, T. (2011). Management Recommendations for Metabolic Complications Associated with Second Generation Antipsychotic Use in Children and Youth. Journal of the Canadian Acadamy of Child and Adolescent Psychiatry, 20(3), 234-241.

2
Background
Second generation antipsychotic (SGA) prescriptions are on the rise
• RCT-supported evidence for SGA use in kids is limited
Olfson et al. (2006) 63: 679-685
Ronsley R et al. (2013). Canadian Journal of Psychiatry
RCT-supported evidence for SGA use in kids is LIMITED
Indication Target Symptoms
Autism† and Pervasive Developmental Disorders
Irritability, Aggression
Bipolar I Disorder † Manic or mixed episodes
Conduct Disorder Aggression
Developmental Disabilities Aggression, Self-injurious behaviour
Disruptive Behaviour DisorderConduct problems, Irritability, Hyperactivity,
Aggression
Tourette Syndrome Tics
Schizophrenia † Positive and negative symptoms
Panagiotopoulos et al. (2010), J Can Acad Child Adolesc Psychiatry. 19(2):124-37.
www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm094303.htm
- All SGA use in children in Canada is off-label*
*except for Aripiprazole for youth aged 15-17 with schizophrenia and 13-17 yo with manic/mixed episodes of BP I
† = FDA approvals
Background (Cont’d)-Increasing body of literature that SGAs are associated with metabolic complications in both adults and children
JAMA Psychiatry 2013 Oct;70(10):1067-75.

3
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
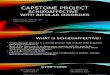
Elevated waistcircumference
Elevatedtriglycerides
Impaired fastingglucose
Low HDL-cholesterol Hypertension Metabolic Syndrome
Pe
rce
nta
ge
(%
)
SGA-treated (N=117)SGA-naïve (N=217)
*
§
†
*
*
Increased Prevalence of the Metabolic Syndrome and its Components
* P<0.001 †P=0.005 § P=0.01 vs. SGA-naïve subjects
Panagiotopoulos et al. (2012). Can J Psychiatry
Metabolic Assessment, Screening and Monitoring Tool

4
CAMESA Guidelines Process• No industry sponsorship
• Recommendations created by:– Incorporating results of systematic review of the
literature on metabolic complications
– Nominal group process
• External review by Can Acad Child & AdolescPsychiatry AND Can Pediatric Society
CAMESA Guidelines: Assumptions
• Appropriate diagnostic assessment has been completed
• SGA-treatment is indicated
• Guidelines are intended to assist with management of complications where the decision to treat with an SGA has already been made (risk/benefit ratio assessment already completed)
www.bcmhsus.ca

5
Case 1• 17 year old boy• Dx: Schizoaffective Disorder (dx at age 12) and
Asperger Syndrome• Referred for: 28 lb weight gain since starting
Clozapine (3 months ago)• Current Medications: Clozapine (200mg), Valproic
Acid (1000mg)• Meds Failed: olanzapine and risperidone (return of
psychosis)• Anthropometrics at 1st visit: weight 121.1 kg
(>97%ile); height 177.8 cm (50-75%ile); BMI 38.3 (>97%ile); waist circumference 118 cm (>90%ile)
How to measure waist circumference
Waist Circumference (WC)
Adult cut-offs: ≥ 94cm for Europid men and ≥ 80cm for Europid women, with ethnicity specific values for other groups*
Source: International Diabetes Federation

6
Treatment Recommendations: Abnormal BMI
1. Normal BMI (5th – 85th percentile):• Repeat measurement at next scheduled screen
2. Overweight (85th ≤ BMI < 95th percentile)• Re-evaluate use of SGA (Grade 3)
• Consider Cognitive/Behavioural lifestyle intervention aimed at weight loss (Grade 1B)
3. Obese (≥ 95th percentile)• As per overweight (same level of evidence (LOE))
AND
• Consider metformin in consultation with specialist (Grade 2B)
Treatment Recommendations: Abnormal WC
1. Normal WC (5th – 75th percentile):
• Repeat measurement at next scheduled screen
2. Abdominally Overweight (75th ≤ WC < 90th percentile)
• Re-evaluate use of SGA (Grade 3)
• Consider Cognitive/Behavioural lifestyle intervention aimed at weight loss (Grade 1B)
3. Abdominally Obese (≥ 90th percentile or > adult cut-off)
• As per overweight (same LOE) AND
• Consider metformin in consultation with specialist (Grade 2B)
Minimizing Metabolic Complications: Minimizing Weight Gain
1. Re-evaluate the use of SGA (Grade 3)– Can medication be stopped?
– Lowest effective dose?
– Switch to different antipsychotic with lower weight gain potential?
– Assess for other medications causing weight gain that could be stopped, changed, reduced
2. Lifestyle Intervention (Grade 3)– Counselling (nutrition, exercise, lifestyle) for all
children at SGA-initiation
– Esp. important if BMI elevated at initiation

7
Cognitive/behavioural lifestyle intervention
Strategies that work:– Self-monitoring of behaviour (food/exercise
diaries)– Weight monitoring– Assessment of motivation and motivational
counselling– Stimulus control– Education on nutrition and physical activity
principles– Goal setting (i.e. SMART goals)
SMART Goal Setting
• SMART goal setting has been found to help children maintain focus and provides structure in changing behaviour
Setting S.M.A.R.T. Goals:
S: Specific (What do you want to do?)
M: Measurable (How much and how often?)
A: Action Plan (How will you do it?)
R: Realistic (Can you do it? 1-10 Scale)
T: Timely (When will you do it/review it?)
Cognitive/Behavioural Lifestyle - Nutrition
Nutrition SMART Goal Setting: Two SMART Goals were made after this patient’s first visit:
S: More vegetables
M: 1 serving/day
A: Mom to add veggie to lunch
R: 6/10
T: Review at next f/u appt
S: Less sugar-sweetened drinks
M: 1 drink/day
A: Fruit instead of juice; diet pop instead of regular pop
R: 7/10
T: Review at next f/u appt

8
Cognitive/Behavioural Lifestyle – PA
• PA SMART Goal Setting: Two SMART Goals were made after this patient’s first visit:
S: short bursts of fast walking
M: work at 7/10 for 1 minute every 5 minutes
A: during walk
R: 9/10
T: Review at next f/u appt
S: decrease screen time
M: by ten minutes each hour
A: getting up from sitting at the computer –activity break
R: 7/10
T: Review at next f/u appt
MetforminStudies limited by short duration of follow-up, small subject numbers, and variability in SGA-treatmentKlein et al. (2006); double blind randomized study:
– improvement in weight, BMI z-score, insulin sensitivity in patients (on olanzapine, risperidone or quetiapine) treated with metformin over 16 weeks
Arman et al. (2008); double blind, randomized study:– mean weight and BMI improved in risperidone treated patients over
first 4 weeks compared with placebo but no difference by 12 weeks
Morrison et al. (2002); open label, prospective cohort study– 15/19 patients lost weight on metformin over 12 weeks
Shin et al. (2009); open label, prospective cohort study– no weight loss while treated with metformin but no further weight
gain
Other medicationsSystematic review (Maayan, Vakhrusheva & Correll 2010) of 32 studies and 15 different medications used in the management of weight gain
• Total number of patients was small, and only 5 medications demonstrated small weight loss when compared to placebo:
– Metformin (n=334)
– D-fenfluramine (n=16)
– Sibutramine (n=55)
– Topiramate (n=133)
– Reboxetine (n=79)
• Insufficient evidence to support routine clinical usage of these agents

9
Case 1: Labwork
Labwork came back after the first visit. The abnormal results were:
Fasting Blood Glucose: 6.1 mmol/L
(110 mg/dl) (Normal: <6.1 mmol/L (<110 mg/dl))
Fasting Insulin: 239 pmol/L
(Normal: <100 pmol/L)
Treatment Recommendations: Abnormal FPG and fasting insulin
1. Normal FPG (< 6.1 mmol/L (<110 mg/dl)):
• Repeat measurement at next scheduled screen
• If fasting insulin > upper limit of normal for assay, consider OGTT (Grade 3)
• For FPG 5.6 – 6.0 mmol/L (100-108 mg/dl), consider OGTT
2. Impaired FPG ( 6.1 – 6.9 mmol/L (110-124 mg/dl))
• Consider OGTT and specialist consultation if abnormal
• Consider metformin in consultation with specialist
3. Abnormal FPG – Diabetes: ( ≥ 7.0 mmol/L (≥126 mg/dl))
• Consult with specialist for management of diabetes
Case 1: Results of more labwork
• More labwork showed:Fasting Blood Glucose: 6.2 mmol/L
OGTT 2hr BG: 8.2 mmol/L(Normal: <7.8mmol/L)
Dx: Impaired glucose tolerance

10
Case 1: Metformin Initiation
Breakfast Supper
Week 1 - 500 mgWeek 2 500 mg 500 mgWeek 3 500 mg 1000 mgWeek 4 1000 mg 1000 mg
Cognitive/Behavioural Lifestyle –PA Follow Up Visit
S: Add weight training
M: 2 times/ week (advised re: intensity and repetitions)
A: Clinic to provide gym pass and Dad will accompany to gym
R: 8/10
T: Review at next appt.
Case 1: Changes in BMI and WC?
1st visit
4 months
7 months
BMI 38.3 37.4 38.2
WC 118 116 115
Last visit at 19.5 years: BMI 36; WC: 110
Most recent fasting BG is 4.8 mmol/L

11
Case 2:
• 11 year old boy
• Dx: Reactive Attachment Disorder, Disruptive Behaviour Disorder NOS, ADHD, Post Traumatic Stress Disorder, Mixed Expressive and Receptive Language Disorder, Mild MR
• Referred for: elevated LDL; Atorvastatin 40 mg once daily had been already initiated by family physician
• Other Medications: Topiramate (75mg), Divalproex (1000mg), Seroquel XR (400mg), Docusate Sodium (100mg)
Case 2: continued
• Anthropometrics at 1st visit: – weight 55.9 kg (>97%ile)
– height 147 cm (50-75%ile)
– BMI 25.8 (>97%ile)
– waist circumference 89 cm (>90%ile)
• Labwork on referral: FBG 5.3 mmol/L, insulin 78 pmol/L, TSH 4.16 mU/L, cholesterol 6.57 mmol/L, HDL 1.26 mmol/L, LDL 4.3 mmol/L, TG 1.06 mmol/L (41 mg/dl)
Treatment Recommendations: Low Density Lipoprotein (LDL)
1. Normal LDL (< 3.35 mmol/L (<130 mg/dl))
• Repeat measurement at next scheduled screen
2. Abnormal LDL (≥ 3.35 mmol/L (≥130mg/dl))
• Re-evaluate use of SGA to minimize weight (Grade 3)
• Consider cognitive/behavioural lifestyle intervention aimed at weight loss (Grade 1B)
3. Elevated LDL: (≥ 4.15 mmol/L (≥160mg/dl) despite aggressive lifestyle / diet/ exercise modification as above for 3 - 6 months)
• Consider consultation with specialist for possible medical therapy

12
Cognitive/Behavioural Lifestyle
- Patient recently moved into group home and dietician was able to work with the home to implement a healthy meal plan (this was very different from home environment)
- As patient was meeting PA guidelines, continued with activity/exercise; continue to add variety to activity.
Cardiovascular Health Integrated Lifestyle Diet: (CHILD) 1 Diet
- Total fat: 25-30% pf daily kcal/EER
- Saturated fat 8-10% of daily kcal/EER
- Avoid trans fat as much as possible
- Monounsaturated and polyunsaturated fat up to 20% of daily kcal
- Cholesterol <300 mg/day
- Other: Promote water; limit SSB, encourage high dietary fibre (F&V, whole grains)
Elevated LDL-c: CHILD 2 Diet
- Total fat: 25-30% pf daily kcal/EER
- Saturated fat ≤7% of daily kcal/EER
- Avoid trans fat as much as possible
- ~10% from monounsaturated fat
- Cholesterol <200 mg/day
- Additional Supportive actions:- Plant sterol esters and/or plant stanol esters up
to 2g/day can be used in FH kids ≥2years
- Psyllium 6g/day (age 2-12); 12 g/day (≥12 years)
Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents, NIH, October 2012

13
Case 2: BMI Chart and Cholesterol Results
Cholesterol Results:Initial Visit
6 months later*
1 year later#
Total Cholesterol (<4.4mmol/L)
6.57(254)
4.83(187)
4.28(165)
LDL(<3.35 mmol/L)
4.3(166)
3.08(119)
2.83(109)
HDL(>1.05 mmol/L)
1.26(49)
1.37(53)
1.35(52)
TG (<1.5 mmol/L
1.06(94)
0.84(74)
0.85(75)
Lipitor was halved* and then discontinued#.
Case 3:
• 13 year old girl• Dx: Bipolar with psychotic features• Referred for: Dyslipidemia• Current Medications: Paliperidone (6 mg),
Lithium (1200 mg)• Previous Meds: Seroquel XR (250 mg)• Lab Results: Cholesterol 5.19 mmol/L,
LDL 2.93 mmol/L, HDL 1.2 mmol/L, TG 2.98 mmol/L
Treatment Recommendations: Triglycerides (TG)
1. Normal TG (< 1.5 mmol/L (<133 mg/dl))
• Repeat measurement at next scheduled screen
2. Abnormal TG (≥ 1.5 mmol/L (≥133 mg/dl))
• Re-evaluate use of SGA to minimize weight (Grade 3)
• Consider cognitive/behavioural lifestyle intervention aimed at weight loss (Grade 1B)
• Consider consultation with a specialist if TG ≥ 5 mmol/L (≥443 mg/dl) for possible medical therapy

14
Elevated TG or nonHDL-c: CHILD 2
CHILD 2 as per previous
Other supportive actions:
• Decrease sugar intake (Grade B):– Replace simple with complex CHO
– No SSB
• Increase dietary fish to increase omega-3 fatty acids (Grade D)
Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents, NIH, October 2012
Case 3: Repeat bloodwork
• Following elimination of 7 cans of pop per week, replaced with diet pop/water: :
Initial Visit 3 months
Total Cholesterol (<4.4 mmol/L)
5.19 4.12
TG (<1.5 mmol/L) 2.98 0.89
Typically a drop in TG also shows a concurrent increase in HDL.
Prolactin
• Elevations in prolactin may be associated with– Gynecomastia
– Galactorrhea
– Infertility
– Menstrual irregularities
– Sexual dysfunction, decreased libido
– Acne and hirsutism (females)
• Hyperprolactinemia may be asymptomatic in some individuals, particularly pre-pubertal children
• Olanzapine, clozapine, risperidone – worst increases
Due to a lack of evidence, the following recommendations are based on expert consensus opinion

15
Treatment Recommendations: Abnormal Prolactin
1. Normal prolactin• Repeat measurement at next scheduled screen
2. Elevated prolactin• Re-evaluate use of SGA (Grade 3)
• Lowest dose?
• Switch to prolactin-sparing agent
• If continued treatment with current SGA essential for psychiatric illness, consult with specialist regarding further management of increased prolactin
• If clinical concerns, consider specialist consult for further investigation regarding other underlying causes
Case 3: More Results
• Prolactin measured at 46.6 ug/L (Normal: <25 ug/L)
• No menstrual period since starting Paliperidone
• No galactorrhea• Recommend d/c paliperidone and try a
different SGA
Case 3: More results
• Paliperidone was stopped with no issues. No further SGA initiated. Patient doing well solely on Lithium.
• Prolactin result 2 weeks after Paliperidone stopped: 9.6 ug/L (Normal: <25 ug/L)

16
Case 4:
• 6 year old boy• Dx: Prenatal substance exposure,
developmental delay, autistic features, difficulties with behaviour and aggression
• Referred for: Prolactin 175.6 ug/L (Normal: <20ug/L) – (Note: no prolactin had been done at baseline)
• Current Medications: Risperidone (1.25 mg)• No symptoms of hyperprolactinemia
Case 4: Recommendations and Results
• Recommendations: removal of risperidone to r/o prolactinoma or other pituitary tumour
• Patient was taken off risperidone for 2 weeks and labs rechecked
– Prolactin level: 2.9 ug/L (<20 ug/L)
• Risperidone reintroduced. Next labs show prolactin of 66.1 ug/L. Counselled on Calcium/Vitamin D for bone health. Recheck prolactin every 6 months.
Prolactin Lowering with Aripiprazole: (Pringsheim T et al. Drug Saf 2011)

17
Provincial Mental Health Metabolic Program
• The Mental Health Metabolic Program is located at BC Children’s Hospital and opened in April 2010
• The multi-disciplinary team includes a:– Pediatric Endocrinologist– Nurse Practitioner– Child & Adolescent Psychiatrist– Dietitian– Physiotherapist
Provincial Mental Health Metabolic Program
We assess:
• Weight Gain (including central adiposity)• Dyslipidemia (low HDL-C, high LDL-C, high TG,
high total cholesterol)• Type 2 diabetes or impaired glucose metabolism
or hyperinsulinemia (NOT type 1 diabetes)• TSH abnormalities associated with lithium or
quetiapine• Hyperprolactinemia • PCOS/Menstrual irregularities/pubertal issues
Kelty Mental Health Resource Centre Website:http://keltymentalhealth.ca

18
Healthy Living Toolkit for Professionals
• The Healthy Living Toolkit for Professionals addresses how to help families make changes to eating, physical activity, sleep and stress management.
• Modules include:– Getting Started (a suggested approach to using the
toolkit)
– Healthy eating
– Physical activity
– Sleep
– Stress management
Healthy Living Toolkit for Families
• Developed by The F.O.R.C.E. Society for Kids’ Mental Health
• The F.O.R.C.E. (Families Organized for Recognition and Care Equality) is a non-profit, BC-based organization that aims to support and empower families and work collaboratively with professionals and systems in understanding and meeting the mental health needs of families.
• Information is consistent with the Healthy Living Toolkit for Professionals
Translation: FA FR KO PA SC TC
Patient & Family Guide to Second-Generation Antipsychotics

19
Specific Patient Handouts
www.bcmhsus.ca
Online Metabolic Monitoring Training Module (coming soon…)

20
Summary: Clinical Relevance
• A large number of children and youth you see in your practice will experience the metabolic side effects of SGAs
• Guidelines have been developed for monitoring these side effects –baseline measures are critical!
• The CAMESA guidelines will assist practitioners with the management of these metabolic complications
• Being proactive about implementing healthy active living at the time of SGA initiation can help mitigate some side-effects
Questions or Comments?
Thank You!
Dr. Dina Panagiotopoulos: [email protected]

CAMESA TREATMENT RECOMMENDATIONS
Management Recommendations for Metabolic ComplicationsAssociated with Second Generation Antipsychotic Usein Children and Youth
Josephine Ho, Constadina Panagiotopoulos, Brian McCrindle, Silviu Grisaru and Tamara
Pringsheim for the CAMESA guideline group
The Canadian Alliance for Monitoring Effectiveness and Safety of Antipsychotics in Children (CAMESA) Guideline Project
Abstract
Background: Second generation antipsychotics (SGAs) are commonly associated with metabolic complications. Thesemedications are being used more frequently for the treatment of mental health disorders in children, which has stimulated the needfor creating formal guidelines on monitoring their safety and effectiveness. Previous guidelines have been developed for monitoringfor metabolic and neurological complications. In order to assist practitioners who perform these monitoring procedures, we havecreated a complementary set of treatment recommendations if abnormal measurements or results are encountered. Objective: Tocreate evidence-based recommendations to assist in managing metabolic complications in children being treated with secondgeneration antipsychotics. Methods: A systematic review of the literature on metabolic complications of second generationantipsychotic medications in children was conducted. Members of the consensus group evaluated the information gathered from thesystematic review of the literature and used a nominal group process to come to consensus on treatment recommendations.Wherever possible, references were made to existing guidelines on the evaluation and treatment of metabolic abnormalities inchildren. Results: Evidence-based recommendations are presented to assist in managing metabolic complications, including weightgain, increased waist circumference, elevation in cholesterol, triglycerides and glucose, liver function tests, abnormal thyroid studies,and elevation in prolactin. Conclusion: The use of SGAs requires proper monitoring procedures. This treatment guideline providesguidance to clinicians on clinical management of metabolic complications if they occur.
Background
Metabolic complications of second generation antipsychotics
are a common and unfortunate consequence of therapy. The
rising use of these medications in Canada and internationally
for the treatment of mental health disorders in children has
stimulated the creation of formal guidelines on monitoringtheir safety and effectiveness. The CAMESA guideline grouphas made evidence-based recommendations on monitoring formetabolic and neurological complications. In order to assistpractitioners who perform these monitoring procedures, wehave created a complementary set of treatment
J Can Acad Child Adolesc Psychiatry, 20:3, August 2011234
The CAMESA guideline group includes:
Stacey Belanger, Neurologist, University of Montreal
Lisa Casselman, Consultant, Mental Health Commission of Canada
Jana Davidson, Child Psychiatrist, University of British Columbia
Asif Doja, Pediatric Neurologist, University of Ottawa
Silviu Grisaru, Pediatric Nephrologist, University of Calgary
Josephine Ho, Pediatric Endocrinologist, University of Calgary
Rekha Jabbal, Pharmacist, Alberta Children’s Hospital MentalHealth Program
Gail MacKean, Consultant, Mental Health Commission of Canada
Brian McCrindle, Pediatric Cardiologist, University of Toronto
John McLennan, Child Psychiatrist, University of Calgary
Valerie Palda, General Internist and Clinical Epidemiologist,University of Toronto
Constadina Panagiotopoulos, Pediatric Endocrinologist, Universityof British Columbia
Scott Patten, Psychiatrist and Clinical Epidemiologist, University ofCalgary
Michelle Pearce, Child Psychiatrist, University of Toronto
Jonathan Ponesse, Developmental Pediatric Neurologist, Universityof Ottawa
Tamara Pringsheim, Neurologist and Clinical Epidemiologist,University of Calgary
Roger Thomas, Family Physician, University of Calgary
Waqar Waheed, Child Psychiatrist, University of Calgary
Chris Wilkes, Child Psychiatrist, University of Calgary
Correspondence to: Tamara Pringsheim, [email protected]
CAMESA Treatment Recommendations

recommendations if abnormal measurements or results areencountered.
The purpose of this article is to provide guidance to clinicianson the appropriate course of action to follow when abnormalmetabolic results are detected over the course of screeningexaminations. Abnormal values for each parameter are speci-fied, and recommendations on further investigations, repeattesting, and management are listed. The target users of theseguidelines are prescribers of antipsychotic medications forchildren and adolescents, which include psychiatrists, pedia-tricians, neurologists, and family physicians.
MethodsThe following metabolic complication treatment recommen-dations are based on the assumption that the clinician hascompleted an appropriate diagnostic assessment and thattreatment with a second generation antipsychotic medicationis indicated. This guideline is intended to assist in managingmetabolic complications in situations where the decision totreat with a second generation antipsychotic has already beenmade by the clinician based on an assessment of the potentialrisks and benefits for the patient. It is beyond the scope of thearticle to provide guidance as to whether a second generationantipsychotic should be used as a treatment method.
The CAMESA guideline group did not receive any industrysponsorship and were able to independently develop thismanuscript with no restrictions of any kind. Recommenda-tions were created by incorporating the results of a systematicreview of the literature on metabolic complications of secondgeneration antipsychotic medications in children (see moni-toring guideline for detailed discussion of search methodsand knowledge synthesis) with a consensus group processinvolving experts in the fields of endocrinology, cardiology,nephrology, psychiatry, neurology and paediatrics. Membersof the consensus group evaluated the information gatheredfrom the systematic review of the literature and used a nomi-nal group process to come to consensus on treatment recom-mendations. A nominal group process is a method of smallgroup discussion in which information is gathered by askingindividuals to respond to questions posed by a moderator, andthen having participants prioritize the suggestions of allgroup members. This process allows all group participants tocontribute to the prioritization of recommendations. Wher-ever possible, we have made references to existing guidelineson the evaluation and treatment of metabolic abnormalities inchildren. Prior to the consensus group process, individualinterviews were conducted with community paediatricians,psychiatrists, and family practitioners as a needs assessment.The need for formal treatment recommendations was identi-fied, and preferences on format were sought. This informa-tion was incorporated into the development of these
guidelines. Upon completion, this guideline was externallyreviewed by the Canadian Academy of Child and AdolescentPsychiatry and the Canadian Pediatric Society.
The level of evidence (LOE) associated with treatment rec-ommendations is provided. Randomized controlled trials areconsidered “high” levels of evidence, observational studiesare “low”, and any other evidence (retrospective study, caseseries, or case report) are “very low”. Recommendations havebeen graded using a classification scheme based on theGRADE system (Brozek, Akl, Alonso-Coello, & al., 2009;Brozek, Akl, Alonso-Coello, Lang, et al., 2009) (Table 1). Aswith many other paediatric conditions, there is often a lack oflarge randomized, controlled trials on which to make evi-dence-based recommendations. Therefore, expert consensusrecommendations can still be important even in the absenceof strong evidence. Recommendations are listed in the orderby which prescribers should pursue them.
Recommendations
MINIMIZING METABOLIC COMPLICATIONS
Treatment recommendations for minimizingweight gain:
1. Lifestyle intervention
Since second generation antipsychotic medication use in chil-dren and youth is associated with weight gain and resultantmetabolic complications, it is strongly recommended thatpatients receive counselling (nutrition, lifestyle and exercise)at the initiation of therapy regardless of baseline body massindex. This is particularly important in a child who is over-weight or obese prior to treatment with a second generationantipsychotic medication (Grade 3).
2. Re-evaluate use of antipsychotic medication to
minimize weight gain (Grade 3):
a. Can the medication be stopped?
Strong consideration should be made to stopping themedication if severe metabolic side effects areencountered. In placebo discontinuation studies,discontinuation of the antipsychotic medication canresult in improvement of weight (Lindsay, Leone, &Aman, 2004; Reyes, Buitelaar, Toren, Augustyns, &Eerdekens, 2006).
b. Is the lowest effective dose of medication being used?
Higher doses of both risperidone (LOE high) (Haas etal., 2009) and olanzapine (LOE low) (Correll et al.,2009) have been associated with greater weight gainand an increased likelihood of metabolic abnormalitiesin children.
Management Recommendations for Metabolic Complications Associated with Second Generation Antipsychotic Use in Children and Youth
J Can Acad Child Adolesc Psychiatry, 20:3, August 2011 235

c. Can the antipsychotic medication be switched to adifferent antipsychotic?
Weight gain is the highest with olanzapine (LOE high)(Correll et al., 2009) and clozapine (LOE high)(Kumra et al., 2008), and the risk of high cholesterol,triglycerides and fasting blood sugar is greatest witholanzapine (LOE low) (Correll et al., 2009). Could thepatient be switched to risperidone or aripiprazole,which are associated with lower amounts of weightgain and lipid abnormality (LOE low) (Correll et al.,2009)? Ziprasidone has been associated withcomparatively less weight gain than other atypicalantipsychotics in adult patients (LOE high) (Komossaet al., 2009); however, data is lacking in youngchildren. Switching to ziprasidone may be aconsideration in older adolescent patients.
d. Is the patient taking any other medications in additionto the antipsychotic which also causes weight gain?If yes, can these medications be stopped, changed, orreduced?
BODY MASS INDEX (BMI)
BMI is determined using a height and weight measurement.For proper technique in measuring, please see the CanadianPediatric Society position statement regarding the use ofgrowth charts (“A health professional’s guide to using growthcharts,” 2004). Age and sex-adjusted growth charts and BMIcharts are available at http://www.cdc.gov/growthcharts/clinical_charts.htm#Set1 (Source: Centers for Disease Con-trol and Prevention).
The Canadian clinical practice guidelines on the managementand prevention of obesity in adults and children recommendscomprehensive healthy lifestyle intervention as the first linetherapy for obese children (Lau et al., 2007). Behaviourallifestyle intervention in children has been shown to be effec-tive in managing obesity (Oude Luttikhuis et al., 2009). Sin-gle blind, randomized controlled trials have been done inadults being treated with antipsychotic medication and haveshown that cognitive behavioural therapy aimed at healthylifestyles improves weight loss compared to no cognitive
J Can Acad Child Adolesc Psychiatry, 20:3, August 2011236
CAMESA Treatment Recommendations
Table 1. Summary of strength of recommendations using the GRADE approach (Brozek, Akl,Alonso-Coello, Lang, et al., 2009)
Grade of recommendation Benefit vs risk and burdensMethodological quality of
supporting evidenceImplications
1A/ strong recommendation,high quality evidence
Benefits clearly outweigh riskand burdens, or vice versa
RCTs without importantlimitations or overwhelmingevidence from observationalstudies
Strong recommendation
Can apply to most patients inmost circumstances withoutreservation
1B/ strong recommendation,moderate quality evidence
Benefits clearly outweigh riskand burdens, or vice versa
RCTs with important limitations,or exceptionally strong evidencefrom observational studies
Strong recommendation
Can apply to most patients inmost circumstances withoutreservation
1C/ strong recommendation,low quality or very low qualityevidence
Benefits clearly outweigh riskand burdens, or vice versa
Observational studies or caseseries
Strong recommendation but maychange when higher qualityevidence becomes available
2A/ weak recommendation,high quality evidence
Benefits closely balanced withrisks and burden
RCTs without importantlimitations, or overwhelmingevidence from observationalstudies
Weak recommendation, bestaction may differ depending oncircumstances or patients orsocietal values
2B/ weak recommendation,moderate quality evidence
Benefits closely balanced withrisks and burden
RCTs with important limitations,or exceptionally strong evidencefrom observational studies
Weak recommendation, bestaction may differ depending oncircumstances or patients orsocietal values
2C/ weak recommendation,low quality or very low qualityevidence
Uncertainty in the estimates ofbenefits, risks, and burden;benefits, risk, and burden maybe closely balanced
Observational studies or caseseries
Very weak recommendations;other alternatives may beequally reasonable
3/ weak recommendation, noevidence, consensus based
Uncertainty in the estimates ofbenefits, risks, and burden
No data from RCTs orobservational studies.Recommended on the basis ofexpert opinion
Weak recommendation, bestaction may differ depending oncircumstances

behavioural therapy (Alvarez-Jimenez et al., 2006; Khazaalet al., 2007; Weber & Wyne, 2006).
Metformin has been used in some small trials of children onantipsychotic medication (Arman, Sadramely, Nadi, &Koleini, 2008; Klein, Cottingham, Sorter, Barton, & Morri-son, 2006; Morrison, Cottingham, & Barton, 2002; Shin,Bregman, Breeze, Noyes, & Frazier, 2009). In a double blind,randomized, placebo controlled study, Arman et al. (2008)found that mean weight and BMI improved in patients onrisperidone treated with metformin for the first four weekscompared to placebo, but by 12 weeks there was no signifi-cant difference. However, Klein et al. (2006) noted animprovement in weight, BMI z-score and insulin sensitivityin patients treated with metformin compared to placebo in a16 week double blind, randomized controlled study of chil-dren on olanzapine, risperidone or quetiapine. In an openlabel, prospective cohort study of 12 weeks duration, Morri-son et al. (2002) found that 15 of 19 patients on variousantipsychotic medications lost weight while on metformin.Another open label, prospective cohort study by Shin et al.(2009) of 12 weeks duration did not show weight loss in thoseon antipsychotic medication treated with metformin, but diddemonstrate that overall, the patients did not continue to gainweight. To date, study findings are discordant and are limitedby the short duration of follow-up, small subject numbers,and variability in the antipsychotic medication with which thepatients were being treated.
Other medications have been used in the management ofweight gain associated with antipsychotic use. Maayan(Maayan, Vakhrusheva, & Correll, 2010) conducted a sys-tematic review which included 32 studies and 15 differentmedicat ions: amantadine, dextroamphetamine,d-fenfluramine, famotidine, fluoxetine, fluvoxamine,metformin, nizatidine, orlistat, phenypropanolamine,reboxetine, rosiglitazone, sibutramine, topiramate andmetformin plus sibutramine. The total number of patients wassmall and only five of these demonstrated small weight losswhen compared to placebo: metformin (n=334),d-fenfluramine (n=16), sibutramine (n=55), topiramate(n=133) and reboxetine (n=79). This systematic review dem-onstrated that there is insufficient evidence to support routineclinical usage of these agents.
Treatment recommendations for abnormalBMI:
1. Normal BMI = 5th
percentile to 85th
percentile
Recommend: Repeat BMI measurement at next scheduledscreen (refer to screening document).
2. Overweight BMI = � 85th
percentile and < 95th
percentile
Recommend: Re-evaluate use of antipsychotic medication tominimize weight (Grade 3).
Consider cognitive/behavioral lifestyle intervention aimed atweight loss (Grade 1B).
3. Obese BMI = BMI � 95th
percentile
Recommend: Re-evaluate use of antipsychotic medication tominimize weight (Grade 3).
Consider cognitive/behavioral lifestyle intervention aimed atweight loss (Grade 1B).
Considermetformin inconsultationwithaspecialist (Grade2B).
WAIST CIRCUMFERENCE
Waist circumference percentiles are sex and age-adjusted andvary for different ethnicities. Technique for waist circumfer-ence measurement is described by Douketis et al. (Douketis,Paradis, Keller, & Martineau, 2005). Age and sex-adjustedwaist circumference percenti les are available athttp://www.idf.org/webdata/docs/Mets_definition_chil-dren.pdf (Source: International Diabetes Federation).
Treatment recommendations for abnormalwaist circumference:
1. Normal waist circumference = 5th
percentile to 75th
percentile
Recommend: Repeat waist circumference measurement atnext scheduled screen (refer to screening document).
2. Elevated waist circumference (abdominally over-
weight) = �75th
percentile and <90th
percentile
Recommend: Re-evaluate use of antipsychotic medication tominimize weight (Grade 3).
Consider cognitive/behavioral lifestyle intervention aimed atweight loss (Grade 1B).
3. Elevated waist circumference (abdominally obese) =
�90th
percentile or exceeding the adult cut-off
Recommend: Re-evaluate use of antipsychotic medication tominimize weight (Grade 3).
Consider cognitive/behavioral lifestyle intervention aimed atweight loss (Grade 1B).
Considermetformin inconsultationwithaspecialist (Grade2B).
BLOOD PRESSURE (BP)
Systolic blood pressure (SBP) and diastolic blood pressure(DBP) percentiles are sex, age and height percentile-adjusted.Proper technique for blood pressure measurement in childrenhas been published by the National High Blood Pressure Edu-cation Program Working Group on High Blood Pressure inChildren and Adolescents (“The fourth report on the
Management Recommendations for Metabolic Complications Associated with Second Generation Antipsychotic Use in Children and Youth
J Can Acad Child Adolesc Psychiatry, 20:3, August 2011 237

diagnosis, evaluation, and treatment of high blood pressure inchildren and adolescents,” 2004). Specific BP percentiles areavailable at http://pediatrics.aappublications.org/cgi/con-tent/full/114/2/S2/555. The following recommendations arebased on the Fourth Report on the Diagnosis, Evaluation, andTreatment of High Blood Pressure in Children and Adoles-cents (“The fourth report on the diagnosis, evaluation, andtreatment of high blood pressure in children and adolescents,”2004).
Treatment recommendations for abnormal BP:
1. Normal BP = SBP and DBP <90th
percentile
Recommend: Repeat BP check at next scheduled screen (referto screening document).
2. Pre-hypertension = SBP or DBP �90th
percentile and
<95th
percentile or BP exceeds 120/80 mmHg
Recommend: Recheck BP reading in six months (“The fourthreport on the diagnosis, evaluation, and treatment of highblood pressure in children and adolescents,” 2004).
If still elevated, consider specialist consultation (“The fourthreport on the diagnosis, evaluation, and treatment of highblood pressure in children and adolescents,” 2004).
3. Stage 1 Hypertension = SBP and/or DBP 95th
to 99th
percentile plus 5mmHg
Recommend: Recheck BP reading in one to two weeks orsooner if symptomatic (“The fourth report on the diagnosis,evaluation, and treatment of high blood pressure in childrenand adolescents,” 2004).
If persistently elevated on two additional occasions, considerspecialist consultation for evaluation and treatment withinone month (“The fourth report on the diagnosis, evaluation,and treatment of high blood pressure in children and adoles-cents,” 2004).
Example: For a three year old girl with a height at the 95th per-centile, a BP of 110/69 would be at the 95th percentile (fromtable provided in the Fourth Report (“The fourth report on thediagnosis, evaluation, and treatment of high blood pressure inchildren and adolescents,” 2004)). She would be at stage 1hypertension with a BP of 115/74 (5 mmHg above the 95th
percentile).
4. Stage 2 Hypertension = SBP and/or DBP >99th
per-
centile plus 5mmHg
Recommend: Consult specialist within one week or immedi-ately if patient is symptomatic (“The fourth report on the diag-nosis, evaluation, and treatment of high blood pressure inchildren and adolescents,” 2004).
Example: For a 12 year old boy with a height at the 95th per-centile, a BP of 135/91 would be at the 99th percentile (from
table provided in the Fourth Report (“The fourth report on thediagnosis, evaluation, and treatment of high blood pressure inchildren and adolescents,” 2004)). He would be at stage 2hypertension with a BP of 140/96 (5 mmHg above the 99th
percentile).
5. Severe hypertension = SBP or DBP >95th
percentile
plus > 20 mmHg and above or symptomatic
Recommend: Immediate assessment by specialist for investi-gation and management (“The fourth report on the diagnosis,evaluation, and treatment of high blood pressure in childrenand adolescents,” 2004).
Patients with symptomatic malignant hypertension (sudden,severe hypertension with threat of organ damage) should bereferred to the nearest emergency room (“The fourth report onthe diagnosis, evaluation, and treatment of high blood pres-sure in children and adolescents,” 2004).
Example: For a 10 year old girl with a height at the 95th per-centile, a BP of 122/80 would be at the 95th percentile (fromtable provided in the Fourth Report (“The fourth report on thediagnosis, evaluation, and treatment of high blood pressure inchildren and adolescents,” 2004)). She would have severehypertension with a BP of >142/100 (>20 mmHg above the95th percentile).
FASTING PLASMA GLUCOSE (FPG) & INSULIN
The following recommendations are based on the CanadianDiabetes Association 2008 Clinical Practice Guidelines forthe Prevention and Management of Diabetes in Canada(Canadian Diabetes Association Clinical Practice GuidelinesExpert Committee, 2008).
Treatment recommendations for abnormal
FPG & fasting insulin:
1. Normal FPG = FPG < 6.1 mmol/L
Recommend:Repeat FPG at next scheduled screen (refer toscreening document).
If the fasting insulin is above the upper limit of normal for theassay being used, consider oral glucose tolerance test(OGTT) and specialist consultation (Grade 3).
For those individuals with a FPG value of 5.6 - 6.0 mmol/L,consideration should be given to performing an OGTT(Canadian Diabetes Association Clinical Practice GuidelinesExpert Committee, 2008).
2. Impaired FPG = FPG 6.1 - 6.9 mmol/L
Recommend: Consider OGTT and specialist consultation ifabnormal (Canadian Diabetes Association Clinical PracticeGuidelines Expert Committee, 2008).
J Can Acad Child Adolesc Psychiatry, 20:3, August 2011238
CAMESA Treatment Recommendations

Consider metformin in consultation with a specialist (Cana-dian Diabetes Association Clinical Practice GuidelinesExpert Committee, 2008).
3. Abnormal FPG (Diabetes) = FPG � 7 mmol/L
Recommend: Consult with specialist for the management ofdiabetes (Canadian Diabetes Association Clinical PracticeGuidelines Expert Committee, 2008).
FASTING LIPID PROFILE
Normal lipid levels vary by sex and age (Daniels & Greer,2008) and several clinical management guidelines have beenpublished on the management of dyslipidemia in children(Daniels & Greer, 2008; Kavey et al., 2006; McCrindle et al.,2007). The following recommendations are based on theguidelines by McCrindle (McCrindle, in press).
Treatment recommendations for abnormal
fasting lipid profile:
Low Density Lipoprotein (LDL)
1. Normal LDL < 3.35 mmol/L (McCrindle, in press).
Recommend: Repeat LDL measurement at next scheduledscreen (refer to screening document).
2. Abnormal LDL � 3.35 mmol/L or a non-HDL choles-
terol (total cholesterol minus HDL) � 3.75 mmol/L
(McCrindle, in press).
Recommend: Re-evaluate use of antipsychotic medication tominimize weight (Grade 3).
Consider cognitive/behavioral lifestyle intervention aimed atweight loss (Grade 1B).
3. Elevated LDL � 4.15 mmol/L despite aggressive life-
style/diet/exercise modification as above for 3-6 months
(McCrindle, in press).
Recommend: Consider consultation with specialist for possi-ble medical therapy (McCrindle, in press).
High Density Lipoprotein (HDL)
1. Normal HDL � 1.05 mmol/L (McCrindle, in press).
Recommend: Repeat HDL measurement at next scheduledscreen (refer to screening document).
2. Abnormal HDL <1.05 mmol/L (McCrindle, in press).
Recommend: Re-evaluate use of antipsychotic medication tominimize weight (Grade 3).
Consider cognitive behavioural lifestyle intervention aimedat weight loss (Grade 1B).
Triglycerides (TG)
1. Normal TG < 1.5 mmol/L (McCrindle, in press).
Recommend: Repeat TG measurement at next scheduledscreen (refer to screening document).
2. Abnormal TG � 1.5 mmol/L (McCrindle, in press).
Recommend: Re-evaluate use of antipsychotic medication tominimize weight (Grade 3).
Consider cognitive behavioural lifestyle intervention aimedat weight loss (Grade 1B).
Consider consultation with specialist if TG � 5 mmol/L forpossible medical therapy (McCrindle, in press).
LIVER FUNCTION
Due to the lack of evidence, the following recommendationsare based on expert consensus opinion.
Treatment recommendations for abnormalliver function tests:
1. Normal AST/ALT
Recommend: Repeat AST/ALT measurement at next sched-uled screen (refer to screening document).
2. Abnormal AST/ALT
Recommend: Consider repeating AST/ALT (Grade 3).
Consider specialist consultation for further investigation andmanagement (Grade 3).
THYROID STIMULATING HORMONE
Thyroid stimulating hormone measurements have been rec-ommended for children and youth taking quetiapine. Due tothe lack of evidence, the following recommendations arebased on expert consensus opinion.
Treatment recommendations for abnormalTSH:
1. Normal TSH
Recommend: Repeat TSH measurement at next scheduledscreen (refer to screening document).
2. Abnormal TSH
Recommend: Consider assessment of free thyroxine level(Grade 3).
Consider specialist consultation for further investigation andmanagement (Grade 3).
PROLACTIN
Elevations in prolactin may be associated with signs andsymptoms such as gynecomastia, galactorrhea, infertility,
Management Recommendations for Metabolic Complications Associated with Second Generation Antipsychotic Use in Children and Youth
J Can Acad Child Adolesc Psychiatry, 20:3, August 2011 239

menstrual irregularities, oligomenorrhea, amenorrhea, sexualdysfunction, decreased libido, acne and hirsutism in females.However, hyperprolactinemia may be asymptomatic in someindividuals, and in particular, in pre-pubertal children. Due tothe lack of evidence, the following recommendations arebased on expert consensus opinion.
Treatment recommendations for abnormalprolactin:
1. Normal prolactin
Recommend: Repeat prolactin measurement at next sched-uled screen (refer to screening document).
2. Elevated prolactin
Recommend: Re-evaluate use of antipsychotic medication(Grade 3):
a. Is the lowest effective dose of the antipsychotic beingused? There is evidence to support that higher doses ofboth risperidone (LOE high) (Kleinberg, Davis, deCoster, Van Baelen, & Brecher, 1999) and olanzapine(LOE low) (Alfaro et al., 2002) cause more prolactinelevation and prolactin-related side effects incomparison to lower doses.
b. Can the antipsychotic medication be switched to aprolactin-sparing agent? Risperidone is the secondgeneration antipsychotic with the greatest effect onprolactin (LOE high), while aripiprazole, quetiapineand clozapine do not elevate prolactin (LOE high)(Haddad & Wieck, 2004; Roke, van Harten, Boot, &Buitelaar, 2009). Switching to a prolactin-sparingagent results in return to normal levels of prolactinwithin weeks (LOE low) (Lee, Kim, & Park, 2006).
c. If continued treatment with the current antipsychoticmedication is essential for the patient’s psychiatricillness, consult with a specialist regarding furthermanagement of the hyperprolactinemia.
d. If clinical concerns, consider specialist consultation forfurther investigation regarding other causes ofhyperprolactinemia and/or amenorrhea.
ConclusionThese treatment recommendations have been formulated toadvise practitioners of an appropriate course of action if meta-bolic or other laboratory abnormalities are encountered overthe course of screening activities related to second generationantipsychotic use. Practitioners should incorporate these rec-ommendations with their clinical judgement, as the individ-ual and unique nature of patient and drug relatedcomplications cannot be ignored. As further long term databecomes available, revisions to these recommendations maybe required. It is our hope that the recommendations made
will allow practitioners to feel more confident about theirmonitoring procedures, and more prepared to act if adverseevents occur.
There are potential organizational barriers in applying theserecommendations, particularly in the area of allied healthsupport. One large potential barrier is the lack of access toappropriate cognitive behavioral therapy for weight loss inobese children, as well as support from registered dieticiansand exercise therapists. Given that the main first line interven-tion recommended for many of the metabolic complicationsis lifestyle intervention, it is important to ensure that appropri-ate resources are available for patients to access. The screen-ing and interventions recommended are anticipated to becost-effective, since early detection and treatment of meta-bolic side effects would prevent progression to more severedisease states and long term complications.
Acknowledgements / Conflicts of InterestThe CAMESA Guideline Project was funded by the Canadian Institute forHealth Research. Dr. Panagiotopoulos receives Clinician Scientist salarysupport from the Child & Family Research Institute and CanadianDiabetes Association. We wish to acknowledge the Canadian Academy ofChild and Adolescent Psychiatry and the Canadian Pediatric Society fortheir external review of the manuscript. The CAMESA guideline groupauthors have no conflicts of interest to declare.
ReferencesAlfaro, C. L., Wudarsky, M., Nicolson, R., Gochman, P., Sporn, A.,
Lenane, M., & Rapoport, J. (2002). Correlation of antipsychotic andprolactin concentrations in children and adolescents acutely treatedwith haloperidol, clozapine, or olanzapine. Journal of Child and
Adolescent Psychopharmacology, 12(2), 83-91.Alvarez-Jimenez, M., Gonzalez-Blanch, C., Vazquez-Barquero, J. L.,
Perez-Iglesias, R., Martinez-Garcia, O., Perez-Pardal,T.,…Crespo-Facorro, B. (2006). Attenuation of antipsychotic-inducedweight gain with early behavioral intervention in drug-naivefirst-episode psychosis patients: A randomized controlled trial.Journal of Clinical Psychiatry, 67(8), 1253-1260.
Arman, S., Sadramely, M. R., Nadi, M., & Koleini, N. (2008). Arandomized, double-blind, placebo-controlled trial of metformintreatment for weight gain associated with initiation of risperidone inchildren and adolescents. Saudi Medical Journal, 29(8), 1130-1134.
Brozek, J. L., Akl, E. A., Alonso-Coello, P., & al., e. (2009). Gradingquality of evidence and strength of recommendations in clinicalpractice guidelines. Part 1 of 3. An overview of the GRADE approachand grading quality of evidence about interventions. Allergy, 64(5),669-677.
Brozek, J. L., Akl, E. A., Alonso-Coello, P., Lang, D., Jaeschke, R.,Williams, J. W.,…GRADE Working Group. (2009). Grading qualityof evidence and strength of recommendations in clinical practiceguidelines. Part 1 of 3. An overview of the GRADE approach andgrading quality of evidence about interventions. Allergy, 64(5),669-677.
Canadian Diabetes Association Clinical Practice Guidelines ExpertCommittee (2008). Canadian Diabetes Association 2008 clinicalpractice guidelines for the prevention and management of diabetes inCanada. Canadian Journal of Diabetes, 32(Suppl 1), S1-S201.
Correll, C. U., Manu, P., Olshanskiy, V., Napolitano, B., Kane, J. M., &Malhotra, A. K. (2009). Cardiometabolic risk of second-generationantipsychotic medications during first-time use in children andadolescents. Journal of the American Medical Association, 302(16),1765-1773.
J Can Acad Child Adolesc Psychiatry, 20:3, August 2011240
CAMESA Treatment Recommendations

Daniels, S. R., & Greer, F. R. (2008). Lipid screening and cardiovascularhealth in childhood. Pediatrics, 122(1), 198-208.
Douketis, J. D., Paradis, G., Keller, H., & Martineau, C. (2005). Canadianguidelines for body weight classification in adults: Application inclinical practice to screen for overweight and obesity and to assessdisease risk. Canadian Medical Association Journal, 172(8), 995-998.
The fourth report on the diagnosis, evaluation, and treatment of highblood pressure in children and adolescents (2004). Pediatrics, 114(2Suppl 4th Report), 555-576.
Haas, M., Eerdekens, M., Kushner, S., Singer, J., Augustyns, I., Quiroz,J.,…Kusumakar, V. (2009). Efficacy, safety and tolerability of twodosing regimens in adolescent schizophrenia: Double-blind study.British Journal of Psychiatry, 194(2), 158-164.
Haddad, P. M., & Wieck, A. (2004). Antipsychotic-inducedhyperprolactinaemia: Mechanisms, clinical features and management.Drugs, 64(20), 2291-2314.
A health professional’s guide to using growth charts (2004). Paediatrics
and Child Health, 9(3), 174-188.Kavey, R. E., Allada, V., Daniels, S. R., Hayman, L. L., McCrindle, B.
W., Newburger, J. W.,… Steinberger, J. (2006). Cardiovascular riskreduction in high-risk pediatric patients: A scientific statement fromthe American Heart Association Expert Panel on Population andPrevention Science; the Councils on Cardiovascular Disease in theYoung, Epidemiology and Prevention, Nutrition, Physical Activityand Metabolism, High Blood Pressure Research, CardiovascularNursing, and the Kidney in Heart Disease; and the InterdisciplinaryWorking Group on Quality of Care and Outcomes Research: Endorsedby the American Academy of Pediatrics. Circulation, 114(24),2710-2738.
Khazaal, Y., Fresard, E., Rabia, S., Chatton, A., Rothen, S., Pomini,V.,…Zullino, D. (2007). Cognitive behavioural therapy for weightgain associated with antipsychotic drugs. Schizophrenia Research,
91(1-3), 169-177.Klein, D. J., Cottingham, E. M., Sorter, M., Barton, B. A., & Morrison, J.
A. (2006). A randomized, double-blind, placebo-controlled trial ofmetformin treatment of weight gain associated with initiation ofatypical antipsychotic therapy in children and adolescents. American
Journal of Psychiatry, 163(12), 2072-2079.Kleinberg, D. L., Davis, J. M., de Coster, R., Van Baelen, B., & Brecher,
M. (1999). Prolactin levels and adverse events in patients treated withrisperidone. Journal of Clinical Psychopharmacology, 19(1), 57-61.
Komossa, K., Rummel-Kluge, C., Hunger, H., Schwarz, S., Bhoopathi, P.S., Kissling, W., & Leucht, S. (2009). Ziprasidone versus otheratypical antipsychotics for schizophrenia. Cochrane Database
Systemic Review, (4), CD006627.Kumra, S., Kranzler, H., Gerbino-Rosen, G., Kester, H. M., De Thomas,
C., Kafantaris, V.,…Kane J. (2008). Clozapine and “high-dose”olanzapine in refractory early-onset schizophrenia: A 12-weekrandomized and double-blind comparison. Biological Psychiatry,
63(5), 524-529.
Lau, D. C., Douketis, J. D., Morrison, K. M., Hramiak, I. M., Sharma, A.M., & Ur, E. (2007). 2006 Canadian clinical practice guidelines on themanagement and prevention of obesity in adults and children[summary]. Canadian Medical Association Journal, 176(8), S1-13.
Lee, B. H., Kim, Y. K., & Park, S. H. (2006). Using aripiprazole toresolve antipsychotic-induced symptomatic hyperprolactinemia: Apilot study. Progress in Neuropsychopharmacology & Biological
Psychiatry, 30(4), 714-717.
Lindsay, R. L., Leone, S., & Aman, M. G. (2004). Discontinuation ofrisperidone and reversibility of weight gain in children with disruptivebehavior disorders. Clinical Pediatrics (Philadelphia), 43(5), 437-444.
Maayan, L., Vakhrusheva, J., & Correll, C. (2010). Effectiveness ofmedications used to attenuate antipsychotic-related weight gain andmetabolic abnormalities: A systematic review and meta-analysis.Neuropsychopharmacology, 35(7), 1520-1530.
McCrindle, B. W. (in press). Pathogenesis and management ofobesity-related dyslipidemia. New York, NY: Humana Press.
McCrindle, B. W., Urbina, E. M., Dennison, B. A., Jacobson, M. S.,Steinberger, J., Rocchini, A. P.,… Daniels, S. (2007). Drug therapy ofhigh-risk lipid abnormalities in children and adolescents: A scientificstatement from the American Heart Association Atherosclerosis,Hypertension, and Obesity in Youth Committee, Council ofCardiovascular Disease in the Young, with the Council onCardiovascular Nursing. Circulation, 115(14), 1948-1967.
Morrison, J. A., Cottingham, E. M., & Barton, B. A. (2002). Metforminfor weight loss in pediatric patients taking psychotropic drugs.American Journal of Psychiatry, 159(4), 655-657.
Oude Luttikhuis, H., Baur, L., Jansen, H., Shrewsbury, V. A., O’Malley,C., Stolk, R. P., & Summerbell, C. (2009). Interventions for treatingobesity in children. Cochrane Database Systemic Review, (1),CD001872.
Reyes, M., Buitelaar, J., Toren, P., Augustyns, I., & Eerdekens, M.(2006). A randomized, double-blind, placebo-controlled study ofrisperidone maintenance treatment in children and adolescents withdisruptive behavior disorders. American Journal of Psychiatry,
163(3), 402-410.
Roke, Y., van Harten, P. N., Boot, A. M., & Buitelaar, J. K. (2009).Antipsychotic medication in children and adolescents: A descriptivereview of the effects on prolactin level and associated side effects.Journal of Child and Adolescent Psychopharmacology, 19(4),403-414.
Shin, L., Bregman, H., Breeze, J. L., Noyes, N., & Frazier, J. A. (2009).Metformin for weight control in pediatric patients on atypicalantipsychotic medication. Journal of Child and Adolescent
Psychopharmacology, 19(3), 275-279.
Weber, M., & Wyne, K. (2006). A cognitive/behavioral groupintervention for weight loss in patients treated with atypicalantipsychotics. Schizophrenia Research, 83(1), 95-101.
Management Recommendations for Metabolic Complications Associated with Second Generation Antipsychotic Use in Children and Youth
J Can Acad Child Adolesc Psychiatry, 20:3, August 2011 241

Copyright January 2014 Drs C Panagiotopoulos and J DavidsonJanuary 2014 MMT Revised for Use in BC Based on Provincial Consensus Workshop
Client Name (last, first):
PHN: DOB: (dd/mm/yyyy)
Hospital/Clinic ID:
Gender:□ Male□ Female > □ Menstrual □ Pre-menstrual
Assessment Date: (dd/mm/yyyy)
(Check all that apply with respect to starting Second Generation Antipsychotic (SGA))
□ Mania□ Mood/affect lability□ Mood stabilization (Bipolar Disorder)□ Oppositionality□ Psychosis□ Self-injurious behaviour
□ Motor/vocal tic□ Sedation/sleep□ Aggression □ Augmentation of (i.e. Antidepressant, anti-anxiety, mood stabilizer, psychostimulant) □ Other (list)
Primary Diagnosis:
Other Diagnoses:
□ Aboriginal*□ Mexican/Hispanic* □ Caucasian
□ South Asian* (i.e. Indian/Pakistani/Bangladesh)□ African/Caribbean*□ Arab (i.e. Saudi Arabian/Egyptian/Iraqi)
□ Asian* (i.e. Japanese/Chinese)
* = high risk ethnicity
Family History
No Yes Unknown 1st degree relative*
2nd degree relative*
Diabetes □ Type 1 □ Type 2 □ Gestational
Hyperlipidemia
Cardiovascular Disease
Schizophrenia
Schizoaffective Disorder
Psychosis Not Otherwise Specified
Bipolar Disorder
*1st degree relative (mother/father/sibling), 2nd degree relative (grandmother/grandfather/cousin/aunt/uncle)
Individual Risk Factors
Smoking □ No □ Yes, ______ cigarettes/day
Physical Activity eg. Exercise (walking) □ No □ Yes, ______ min/day
Screen Time eg. computers, tv, video games □ No □ Yes, ______ min/day
Sugar-sweetened beverages □ No □ Yes, ______ cans of pop/day □ Yes, ______ juice boxes/day
Clie
nt D
etai
lsTa
rget
Sy
mpt
oms
Dia
gnos
esEt
hnic
ity
Risk
Fac
tor
Eval
uati
onMETaboliC aSSESSMEnT, SCREEning anD MoniToRing Tool
P1

Copyright January 2014 Drs C Panagiotopoulos and J DavidsonJanuary 2014 MMT Revised for Use in BC Based on Provincial Consensus Workshop
Parameter Pre-treatment Baseline
1 month 2 month 3 month 6 month 9 month 12 month
Assessment Date (dd/mm/yy): >
Height (cm)
Height percentile(1)
Weight (kg)
Weight percentile(1)
BMI: (Wt (kg) / Ht (cm2) x10,000)
BMI percentile(1)
Waist Circumference (At the level of the umbilicus)
Waist Circumference percentile(2)
Blood Pressure (systolic/diastolic) / / / / / / /
Blood Pressure percentile(3) (systolic/diastolic) / / / / / / /
Neurological Examination(4) □ completed □ completed □ completed □ completed
laboratory Evaluations: Normal Values
Fasting Plasma Glucose ≤ 6.1 mmol/L(5)
Fasting Insulin(6) ≤ 100 pmol/L(7)
Fasting Total Cholesterol < 5.2 mmol/L
Fasting LDL-C < 3.35 mmol/L
Fasting HDL-C ≥ 1.05 mmol/L
Fasting Triglycerides < 1.5 mmol/L
AST
ALT
TSH(8)
Prolactin(9)
Other_______________ (eg. Amylase, A1C, OGTT)(10)
Physician Initials: >
Interventions(continue checking as conducted throughout the year)
Pre-treatment□ Discuss metabolic risks□ Discuss diet□ Discuss physical activity□ Risk/benefit assessment□ Discuss smoking cessation
Post-treatment□ Discuss diet□ Refer to dietitian□ Discuss signs and symptoms
of diabetes/DKA□ Discuss physical activity□ Refer to rehab/groups for
lifestyle
□ Switch antipsychotic medication□ Refer to specialized services
(via GP) e.g. lipid clinic, diabetes clinic
□ Liaise with GP re: abnormal labs□ Other ____________________
Comments
Frequency of follow up after 12 month assessment recommended as yearly or sooner if clinically indicated
Mon
itor
ing
gui
delin
es f
or p
atie
nts
trea
ted
wit
h Se
cond
gen
erat
ion
ant
ipsy
chot
ics
(Sg
as)
P2
= not recommended = highly recommended, but not required
= highly recommended, but not required unless issues identified at month 3, or other clinical indications.
= required only for Risperidone & olanzapine= required
1 To determine height, weight and BMI percentiles, use age and sex-specific growth charts at: http://www.cdc.gov/growthcharts/ 2 To determine age and sex-specific percentiles, go to: http://www.idf.org/webdata/docs/Mets_definition_children.pdf (pages 18-19); Use Adult cut-off (page 10) if lower.3 To determine age and sex-specific percentiles, go to: http://pediatrics.aappublications.org/cgi/content/full/114/2/S2/555. Note that height percentile is required for the
calculation of BP percentile.4 Tools available for monitoring extrapyramidal symptoms that may be used: AIMS (Abnormal Involuntary Movement Scale), SAS (Simpson-Angus Scale), ESRS (Extrapyramidal
Symptom Rating Scale), BARS (Barnes Akathisia Rating Scale).5 For FPG values of 5.6 – 6.0 mmol/L, consideration should be given to performing an oral glucose tolerance test (OGTT).6 Note that this assessment is NOT recommended for Aripiprazole or Ziprasidone, but IS appropriate for all other SGAs. Only recommended at baseline if other risk factors exist.7 For fasting insulin levels > 100 pmol/L, consideration should be given to performing an OGTT.8 Only for Quetiapine. Check yearly if clinical indications exist.9 Note that assessment of prolactin levels should be completed according to protocol EXCEPT when the patient is displaying clinical symptoms of hyperprolactinemia (ie: menstrual
irregularity, gynecomastia, or galactorrhea), in which case more frequent monitoring may be warranted. Please also note that Risperidone is the SGA with the greatest effect on prolactin.
10 It is recommended that Amylase levels be monitored in cases where the patient presents with clinical symptoms of pancreatitis (ie: abdominal pain, nausea, vomiting).
METaboliC aSSESSMEnT, SCREEning anD MoniToRing Tool (continued)
▲ t
§
§
▲
▲
t
t
t
t
t
t
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲

Copyright January 2014 Drs C Panagiotopoulos and J DavidsonJanuary 2014 MMT Revised for Use in BC Based on Provincial Consensus Workshop
Med
icat
ion
s
DrugInitiation
1 month 2 month 3 month 6 month 9 month 12 month
SGAsAssessment Date (dd/mm/yyyy): >
Risperidone (Risperdal)Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Quetiapine (Seroquel)Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Olanzapine (Zyprexa)Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Paliperidone (Invega)Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Clozapine (Clozaril)Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Ziprasidone (Zeldox)Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Aripiprazole (Abilify)Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Other MedicationsAssessment Date (dd/mm/yyyy): >
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Dose _____ Freq _____
Physician Initials: >
Comments and description of changes made to medication dose at other time interval
Additional Comments
METaboliC aSSESSMEnT, SCREEning anD MoniToRing Tool (continued)
P3

Normal BmI(5th to 85th percentile)
overweIght BmI (≥85th and <95th percentile)
oBese BmI (≥95th percentile)
Repeat BMI measurement at next scheduled screen.
Re-evaluate use of SGAs to minimize weight.
Consider lifestyle intervention aimed at weight loss.
Re-evaluate use of SGAs to minimize weight.
Consider lifestyle intervention aimed at weight loss.
Consider metformin in consultation with a specialist.
Normal(5th to 75th percentile)
aBdomINally overweIght (≥75th and <90th percentile)
aBdomINally oBese (≥90th percentile)
Repeat waist circumference measurement at next scheduled screen.
Re-evaluate use of SGAs to minimize weight.
Consider lifestyle intervention aimed at weight loss.
Re-evaluate use of SGAs to minimize weight.
Consider lifestyle intervention aimed at weight loss.
Consider metformin in consultation with a specialist.
Normal (FPG <6.1 mmol/L)
ImpaIred (FPG 6.1 – 6.9 mmol/L)
aBNormal (FPG ≥ 7 mmol/L)
Repeat FBP at next scheduled screen.
If fasting insulin is above the upper limit of normal for the assay being used, consider OGTT and specialist consultation.
For an FPG value of 5.6 – 6.0 mmol/L consideration should be given to an OGTT.
Consider OGTT and specialist consultation if abnormal.
Consider metformin in consultation with a specialist.
Consult with specialist for the management of diabetes.
Normal(SPB and DPB <90th percentile)
pre-hyperteNsIoN (SBP or DPB ≥90th and <95th percentile OR BP exceeds 120/80 mmHg)
stage 1 hyperteNsIoN(SBP and/or DPB 95th to 99th percentile + 5 mmHg)
Repeat BP check at next scheduled screen. Recheck BP reading in 6 months; if still elevated, consider specialist consultation.
Recheck BP reading in 1-2 weeks or sooner if symptomatic.
If persistently elevated on 2 additional occasions, consider specialist consultation for evaluation and treatment within 1 month.
stage 2 hyperteNsIoN (SBP and/or DBP >99th percentile + 5 mmHg)
severe hyperteNsIoN (SBP or DBP >95th percentile + >20 mmHg or symptomatic)
Consult specialist within 1 week, or immediately if patient is symptomatic.
Immediate assessment by specialist for investigation and management.
Patients with symptomatic malignant hypertension should be referred to the nearest emergency room.
Body Mass Index (BMI)
Waist Circumference (WC)
Fasting Plasma Glucose (FPG) & Insulin
Blood Pressure (BP)
Treatment Recommendations for Metabolic Complications Associated with Second Generation Antipsychotic (SGA) Use in Children:
A Quick Reference Guide
P1

Normal ldl(LDL < 3.35 mmol/L)
aBNormal ldl(LDL ≥ 3.35 mmol/L or a non-HDL cholesterol (total cholesterol – HDL) ≥3.75 mmol/L)
elevated ldl(LDL ≥ 4.15 mmol/L despite aggressive lifestyle/diet/exercise modification for 3-6 months)
Repeat LDL measurement at next scheduled screen.
Re-evaluate use of SGAs to minimize weight.
Consider cognitive/behavioural lifestyle intervention aimed at weight loss.
Consider consultation with specialist for possible medical therapy.
Normal hdl(HDL ≥1.05 mmol/L)
aBNormal hdl(HDL <1.05 mmol/L)
Repeat HDL measurement at next scheduled screen. Re-evaluate use of SGAs to minimize weight.
Consider cognitive behavioral lifestyle intervention aimed at weight loss.
Normal tg(TG <1.5 mmol/L)
aBNormal tg (TG ≥1.5 mmol/L)
Repeat TG measurement at next scheduled screen. Re-evaluate use of SGAs to minimize weight.
Consider cognitive behavioural lifestyle intervention aimed at weight loss.
Consider consultation with specialist if TG ≥5 mmol/L for possible medical therapy.
Normal ast/alt aBNormal ast/alt
Repeat AST/ALT measurement at next scheduled screen. Consider repeating AST/ALT.
Consider specialist consultation for further investigation and management.
Normal tsh aBNormal tsh
Repeat TSH measurement at next scheduled screen. Consider assessment of free thyroxine level.
Consider specialist consultation for further investigation and management.
Low Density Lipoprotein (LDL)
High Density Lipoprotein (HDL)
Triglycerides (TG)
Liver Function (AST/ALT)
Thyroid Stimulating Hormone (TSH)
P2
Normal prolactIN elevated prolactIN
Repeat prolactin measurement at next scheduled screen.
Re-evaluate use of SGAs:
a) Is the lowest effective dose of the SGA being used? There is evidence to suggest that higher doses of both risperidone and olanzapine cause more prolactin elevation and prolactin-related side effects in comparison to lower doses.
b) Can the SGA be switched to a prolactin-sparing agent? Risperidone is the second generation antipsychotic with the greatest effect on prolactin. Switching to a prolactin-sparing agent results in return to normal levels of prolactin within weeks.
c) If continued treatment with the current SGA is essential for the patient’s psychiatric illness, consult with a specialist regarding further management of the hyperprolactinemia
d) If clinical concerns, consider specialist consultation for further investigation regarding other causes of hyperprolactinemia and/or amenorrhea.
Prolactin
Treatment Recommendations for Metabolic Complications Associated with Second Generation Antipsychotic (SGA) Use in Children: A Quick Reference Guide