Embed Size (px)
Citation preview

Guest Presenter: Professor Anthony Shakeshaft
31/01/17
Today’s webinar:A practical guide to community-based approaches to reducing alcohol harm
An Australian Indigenous Alcohol and Other Drugs Knowledge Centre webinar

A practical guide to community-based approaches for
reducing alcohol harm
Professor Anthony Shakeshaft, Deputy Director, NDARC

3
Define the problem
Define the program and why it should work
Check the literature: what do we already know?
Define evaluation design and measures
How will program be sustained beyond evaluation phase
Partner with other services/LHDs/communities
Principles

4
• What we’ve learned so far in our initial attempts:
– Clear role delineation (researchers know research; practitioners know practice)
– Be clear (and precise) about what outcomes you are trying to achieve and how
those outcomes will be measured
– Design ‘good’ interventions:
o Clear line of sight (alignment) from the intervention activities to the outcomes
o Practitioner and researcher input to avoid reinventing the wheel (literature reviews)
and access local/clinical knowledge (actual definition of evidence-based practice!)
o Ideas (and models) flow both ways between practitioners and researchers
o Standardised interventions and flexible/tailored
o Practical to implement and sustain if effective
o Service delivery is never stagnant: core stability + tweaking (CQI?)
– Design evaluations that are rigorous but practical (good enough idea)
Solution: integrated models

5
Example 1:BackTrack program for high-risk young people
• Communities:
• Armidale
• Gunnedah, Tenterfield, Glen Innes
• PhD candidate: Alice Knight (NDARC)
• BackTrack based in Armidale, managed
by Bernie Shakeshaft
• BackTrack staff: “It just works…”
• Literature review: no economic
evaluations, no use of routine data, no
crime outcomes (all self-report psych +
D&A)

6
1. Define BackTrack: standardisation and flexibility.
2. Evaluate BackTrack program: How?
Aims of the BackTrack evaluation

7
Have worked together to define 4 core components of BackTrack:
i. Effective engagement process between staff and young people
(e.g. non-threatening activities; young people come and go)
ii. Skills training (e.g. school or TAFE certificates done at shed;
farmers/trades provide opportunities for work experience)
iii. Case management (e.g. getting a tax file number, court
appearances)
iv. Personal development (essentially CBT & MI; community
engagement – e.g. volunteer to assist rural fire brigade; mentoring by
staff)
What is BackTrack?

8
What is BT and why should it ‘work’?

9
Hawkins, Sanson-Fisher, Shakeshaft, et al. Am J Prev Medicine, 2007
• Does BackTrack reduce harms? Alice Knight’s talk…
BackTrack evaluation design (cf AARC RCT)

10
• Communities:
• Griffith
• Narrandera
• Lake Cargelligo/Murrin Bridge
• PhD candidate: Mieke Snijder (NDARC)
Example 2: a community approach to alcohol harm

11
• Principles to design the intervention:
– Multiple intervention components (multiple risk factors/harms)
– Core components standardised (generalisable across communities)
– Community representatives design the intervention activities within core
components based on their interests, available resources, etc. (tailoring)
– Target most prevalent harms/risk factors based on analysis of routinely
collected hospital/police data (most likely to achieve change – ‘low hanging
fruit’)
– Target high-risk individuals (associated with majority of harm)
– Incorporate into existing roles (sustainability)
Example 2: alcohol harm

12
• Intervention core components:
– Improved service engagement (case co-ordination) – more targeted delivery
of the most relevant services to different clients with alcohol harms
o Reduce the likelihood of re-engaging in alcohol harms
– Improved empowerment (family well being) – better understanding of the
nature and causes of alcohol harms
o Increase resilience and empowerment
– Community activities (non-drinking)
o Provide opportunities to do things other then drinking
Example 2: alcohol harm

13
What is Maldahnalanga?
Core Components Griffith Lake Cargelligo/Murrin Bridge Narrandera
Activity Activity Activity
Improved service engagement
♦ Case Coordination
♦ Skills training
♦ Engagement Officers
♦ Case Coordination
♦ Engagement Officers
♦ Engagement Officers
Community activities
♦ Midnight Basketball 1
♦ Midnight Basketball 2
♦ Midnight Basketball 3
♦ Midnight Basketball 4
♦ Cultural activities
♦ Pool/Dart competition
♦ Skate Slam
♦ Cultural and sports day
♦ BBQ in the park
♦ Family Bingo event
♦ Movie night
♦ Fitness Beyond Barriers
♦ At risk boys group
♦ At risk girls group
♦ Touch football nights
♦ Movie night
♦ Cultural Activities
♦ Boxing classes
♦ BT – School Holidays
♦ Music event
♦ Youth Centre Jam Sessions
♦ Indoor Basketball
♦ Beauty classes
♦ Movie night
♦ Country music night
♦ Community meeting
♦ Cultural Activities
♦ Night Basketball*
♦ Hip hop dancing*
♦ Indoor soccer
♦ Talent quest
♦ Outdoor movie
♦ Touch football day
Improved empowerment
♦ Family Wellbeing*
♦ Family Wellbeing*
♦ Men group FWB*
♦ School group FWB*
♦ Family Wellbeing* ♦ Family Wellbeing *
♦ Self-esteem program
Total 21 12 13

14
• Measures
– Outcomes: community survey (self-report); program participants’ survey;
police incidents; A&E attendances; inpatient hospital admissions.
– Process: community perceptions of change; researcher/community
partnership; professionals’ perceptions of the interventions; rates of
attendance at intervention programs
– Economic: Costs (cost to implement interventions) and benefits (monetary
value of reduced harms/risk factors + the value of the intervention program
to the community measured using DCEs).
• More detail? See Mieke’s poster!
Example 2: alcohol harm
15
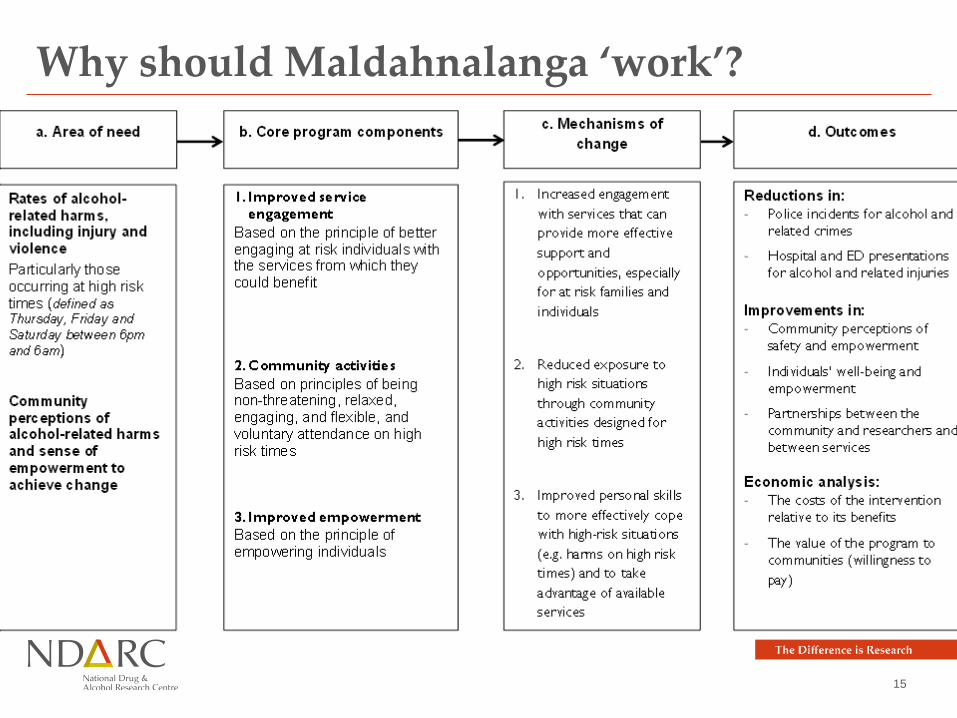
Why should Maldahnalanga ‘work’?

16
• Some implications:
i. Both researchers and practitioners have input, and benefits for both
Staff benefits
– Greater control over the process of service delivery
– Develop academic pathways for professional development
– Increased relevance of research
– Engagement in ground-breaking research
Researcher benefits
– Engage in real world research that makes a difference in short-term
– Publications, more competitive grant applications
i. Researchers can no longer only do what they want to do
ii. Communities/clinicians have to agree to trial new ways of doing things and to work in
partnership with agencies (and other researchers) – organisational culture
Implications of integrated models

17
• Some implications (continued):
iii. Opportunity to reduce the evidence/practice gap
iv. Better use of routinely collected service data
v. Over time deliver better quality programs, and services become dynamic, adapting
organisms. Promising but challenging.
Implications of integrated models

18www.aodknowledgecentre.net.au©2014 Australian Indigenous Alcohol
and Other Drugs Knowledge Centre
Contact detailsProfessor Anthony Shakeshaft
Email: [email protected]
Australian Indigenous Alcohol and Other Drugs
Knowledge Centre
Ph: (08) 9370 6336
Avinna: [email protected]
Millie: [email protected]
Email: [email protected]