Embed Size (px)
Citation preview

A Predictive Risk Index for Nosocomial Pneumonia in the Intensive Care Unit NIRMAL JOSHI, M.D., A. RUSSELL LOCALIO, M.P.H., MS., BRUCE H. HAMORY, M.D., Hershey, Pennsylvania
PU~~POSB To develop a scoring system for stratifying patients in int4msive care units (ICUs) by risk of developing nosocomial pneu- monia (NP) and to identify the time period asso- ciated with the highest risk.
PATIENTS AND MJ!TEOD& Two hundred and three patients 18 years of age or older and resid- ing in the ICU for 72 hours or more were fol- lowed until development of NP or death or for 48 hours after discharge from the ICU. After the identification of independent risk factors for NP, a scoring system was developed to arrive at a predictive risk index for NP.
RESULFI’EIZ Twenty-six (12.3% ) patients devel- oped NP. The presence of a nasogastric (NG) tube [odds ratio (OR) = 6.43,95% confidence in- tervals (CI) = 2.11 to 19J2], upper abdominal/ thoracic surgery (OR = 434,95% CI = 1.43 to 13.14), and bronchoscopy (OR = 2.95,95% CI = 1.02 to 852), most commonly performed for res- piratory toilet, were identified as independent risk factors on multivariate analysis The risks associated with endotracheal intubation and al- tered consciousness, although not independently signifiicant, were highest when these factors were present for 1 to 4 days after the 72 hours required for study entry (endotracheal intuba- tion, OR = 2.2 to 23 altered consciousness, OR = 1.4 to 2.0). The risk then declined; ORs of less than 1 were observed at 7 day& The risk associ- ated with the NG tube was highest during the fmt 6 days (OR = 6.0 to 19.5). Although a subse- quent decrease in risk was observed, the OR was stillgreaterthan2at7dayuToobtainapredic- tive risk index for NP, a scoring system was de- veloped using a multivariate model. This system
From the Division of Infectious Diseases and Epidemiology (NJ, BHH), Department of Medicine, and Center for Biostatistics and Epidemiology (ARL). Milton S. Hershey Medical Center, Pennsylvania State University, Hershey, Pennsylvania.
Requests for reprints should be addressed to Nirmal Joshi, M.D., 630 Cardinal Drive, Harrisburg, Pennsylvania 17111.
Manuscript submitted September 19. 1991. and accepted in revised form April 7, 1992.
has a sensitivity of 35% and a specificity of 66% in predicting NP in this ICU population.
CONCLUSION: ICU patients can be stratified into high- and low-risk groups for NP using a bedside scoring system. Rndotracheal intubation, altered mental status, and NG tube are associ- ated with the highest risk of NP during the first 1 to 6 days of their presence after 72 hours of stay in the ICU. After this time period, the risk associated with these factors decreases. Bron- choscopy may be an independent risk factor for NP that has not been previously recognized. This procedure, often done in the ICU for respi- ratory toilet, may be an avoidable risk in this group of patients.
N osocomial pneumonia (NP) is the third most common nosocomial infection and the most
common cause of death from nosocomial infection in the United States [l]. A high proportion of NPs occur in intensive care units (ICUs). As many as 50% of all NPs occurring among patients on the medical service and 70% of NP among patients on the surgical service occur in ICUs [2]. Case fatality rates of 20% to 50% in some studies of NP [3-51, despite the availability of potent antibiotics, em- phasize the need for research directed at its prevention.
One potential approach to preventing NP is to stratify patients early in their ICU stay into high- and low-risk groups for the development of NP. Interventions can then be directed specifically at the high-risk patients. Although previous studies have identified risk factors for NP [5-S], prospec- tive cohort study designs and statistical methods were used to identify independent risk factors in only two studies [5,6]; both were limited to mechan- ically ventilated patients. An objective estimate of overall individual patient risk for NP cannot be derived from these studies.
To design effective strategies to prevent NP, it is important to identify not only the patients at high- est risk for NP, but also the period of stay in the
August 1992 The American Journal of Medicine Volume 93 135

NO6OCOMlAL PNEUMONIA IN THE ICU / JOSHI ET AL
ICU associated with such a risk. To our knowledge, no study has attempted to define systematically a relationship between the duration of exposure to one or more risk factors and the development of NP.
greater than or equal to 106 kg for men and greater than or equal to 80 kg for women, or if the records indicated that they were too heavy to be weighed.
The current study was designed to develop a sim- ple, easy-to-use predictive model to stratify pa- tients in the ICU into high- and low-risk groups for NP. In addition, we examined the relationship be- tween the duration of several risk factors and the development of NP to identify the period of highest risk.
PATIENTS AND METHODS Patient Population
The University Hospital of the Milton S. Hershey Medical Center is a 350-bed tertiary-care hospital with a 27-bed medical-surgical ICU. Of 762 patients admitted to this ICU during the 6 months between August 13,1999, and February 13,1991, all patients 18 years of age or older who resided in this ICU for 72 hours or more were entered into the study. One investigator (NJ) followed this cohort of 203 pa- tients prospectively until one of the following events occurred: development of NP, discharge from the ICU for more than 48 hours, or death. All ventilated patients had ventilator tubing changed and chest radiography performed three times per week (Monday, Wednesday, and Friday). Antipy- reties were not used routinely in any subset of patients.
A diagnosis of NP required the presence of all the following criteria: fever greater than 38”C, white blood cell count greater than 10,000/mm3, lung in- filtrate persisting more than 24 hours not attribut- able to another etiology (e.g., adult respiratory dis- tress syndrome, congestive heart failure, or pulmonary embolism), and purulent respiratory se- cretions (greater than 5 polymorphonuclear leuko- cytes per oil immersion field on Gram stain) yield- ing growth of microorganisms. A positive culture of blood, pleural fluid, or protected brush sample via bronchoscopy was regarded as additional proof of NP and as definitive for etiology but was not re- quired as a diagnostic criterion. Patients with pneu- monia diagnosed on admission to the ICU were not excluded from the study. A diagnosis of NP in this group of patients required, in addition to the above criteria, a worsening of the lung infiltrate and a change in the presumed causative microorganism.
Severity of illness was classified according to the method of McCabe and Jackson [lo]. This method was preferred over the recently described, more ac- curate methods to maintain simplicity and easy ap- plication at the bedside. Patient outcome (dead/ alive) was determined at discharge.
Statistical Analysis
Data Collection One of us (NJ) made all of the observations and
abstracted relevant data daily by review of the pa- tients’ medical records, bedside flow sheets, and radiographs. At the time of entry into the study, the following data were recorded by chart review: age, sex, admitting service, body weight, smoking histo- ry, serum albumin level, and a history of chronic obstructive lung disease (COPD). In addition, the presence or absence of each of the following poten- tial risk factors was recorded daily: endotracheal intubation, tracheostomy, administration of hista- mine type 2 receptor (Hz) blockers, nasogastric (NG) tube, tube feeding (instillation into the stom- ach of greater than 506 mL/d of enteral nutrition solution), altered level of consciousness (patient unable to respond to simple commands), upper abdominal/thoracic surgery, and bronchoscopy. The presence of any of these factors within 5 days prior to entry resulted in the classification of “present” on the day of entry. Bronchoscopy was considered a risk factor only if it had been per- formed 2 or more days prior to NP. Patients were classified as obese if their recorded body weight was
Univariate analysis of the association of outcome (pneumonia or death) with risk factors and patient demographics was done with generalized Mantel- Haenszel methods [ll]. The test for association was used when the risk factors were not ordinal; the test for differences in mean scores was used when one factor was ordinal. Fisher’s exact test and exact, non-parametric Wilcoxon and stratified trend tests [12] replaced x2 tests when sample sizes were too small to support asymptotic confidence intervals (CIs). Breslow-Day [13] and Zelen’s [14] exact tests were used to determine homogeneity of odds ratios (ORs) across strata.
Multivariate analysis proceeded only on models that were a priori judged sound clinically to avoid the pitfalls of producing spuriously significant re- sults with multiple comparisons. Using logistic re- gression with pneumonia as the outcome and risk factors as predictors, we fit several models to deter- mine the ORs of developing pneumonia while con- trolling for other factors [15]. Both SAS PROC LO- GISTIC and PROC CATMOD with the clogits option produced parameter estimates and model goodness-of-fit statistics [16,17]. Where interest centered on the effects of risk factors over time, we grouped risk factors according to length of patient
136 August 1992 The American Journal of Medicine Volume 93

exposure and then entered each group as a separate indicator in the model. This method allowed for nonlinear dose-response effects. We then fit a series of logistic regression models, each with a length of exposure only for the risk of interest, and with a dichotomous variable for the other factors.
Development of a Scoring System for Risk Stratification
Of several models tested, one model was used to develop a scoring system for risk stratification. Clinical considerations in model development were the desire to use predictors that remained relevant based on univariate analysis and on clinically plau- sible links to pneumonia, and the need to arrive at a parsimonious model for simple application at bed- side. Some factors thought to be of clinical rele- vance were left in the model regardless of statistical significance at p = 0.05. Statistical comparisons were based on model fit (proportion of deviance explained by the model), adjusted for the number of predictors used. Final model selection among sever- al alternatives with comparable fit and predictive ability was based on the need to limit the number of variables, especially those related to the length of exposure. From the selected model, fitted probabil- ities and odds for each patient were calculated from the parameter estimates. Receiver operating char- acteristic (ROC) curve analysis and sensitivity and specificity considerations determined the optimal threshold odds for classifying a patient as “high risk” [ 181. For field use of the model as a predictive tool, we chose to round the ORs for each patient risk factor so that a non-statistician with a hand calcula- tor (or even a pencil and paper) could predict out- come as above or below the odds threshold. The predictive model with rounded parameter esti- mates was tested against the data to determine the extent of misclassification between rounded and unrounded models.
RESULTS Table I summarizes the baseline characteristics
and the interventions performed on the 203 pa- tients who were entered in the study. A history of smoking and COPD was not recorded in the chart of 41% and 40% of patients, respectively. The most frequent admission diagnoses were related to the cardiopulmonary system (45%). Patients were al- most equally distributed between medical and sur- gical services. Fifty-eight percent of the patients were intubated.
Twenty-six (12.8%) patients met the study defi- nition for NP. The following risk factors were sta- tistically significant on univariate analysis: Hz blocker therapy (OR = 2.75,95% CI = 1.02 to 7.40),
TABLE I Characteristics of the Study Cohort*
Patients All With
Patients Pneumonia No. 96 No. %
Sex (M) 115 57 18 69
Obesity 17 8 4 15
Severity of illness Nonfatal 124 61 Ultimately fatal
!i 27 :A 3”:
Rapidly fatal 12 5 19
Smoking Present
Absent 2 ;:
9 35
Unknown 83 41 1: :i
COPD Present
1;: ki 3
Absent :i Unknown 80 40 ii 50
Admission service Medicine Surgery 1;; zi 2; 2
Admission diagnosis ~;arddcrlmonary
:: 45 16 ; :z Abdominal 19 9 4 15 Central nervous system Multisystem Cancer Others
Altered mental status 87 43 19 73
lntubation 117 58 23 88
Nasogastric tube 108 53 24 92
Tube feeding 47 23 0 0
Hz-blockers 128 63 21 81
Recent bronchoscopy 42 21 10 38
Tracheostomy 25 12 3 12
Upper abdominal/thoracic surgery 55 27 12 46
NOSOCOMIAL PNEUMONIA IN THE ICU / JOSHI ET AL
ke (mean ? SD) = 57.5 r 17.8 for all patients, and 62.7 t 16.9 for patients with pneumonia.
altered mental status (OR = 4.35,95% CI = 1.83 to 10.3), endotracheal intubation (OR = 6.77,95% CI = 2.25 to 20.4), NG tube (OR = 13.3,95% CI = 4.05 to 43.6), upper abdominal/thoracic surgery (OR = 2.67,95% CI = 1.17 to 6.09), recent bronchoscopy (OR = 2.83,95% CI = 1.21 to 6.65), and underlying diseases that were ultimately fatal (OR = 2.09,95% CI = 1.02 to 4.33) and rapidly fatal (OR = 2.89,95% CI = 1.04 to 8.26) as compared with those that were nonfatal (exact Wilcoxon, p = 0.035). The incidence of NP increased with patient age. NP occurred in 6% of patients 40 years old, 11% of patients 40 to 60 years of age, and 16% of patients older than 60 years. This trend, however, did not achieve statisti-
August 1992 The American Journal of Medicine Volume 93 137

TABLE II Importance of Risk Factors on Multivariate Analysis*
Odds 95% Confidence Risk Factor Ratio Intervals
1. Age >6Oy 1.93 0.70-5.32
2. Ultimately fatal disease 2.79 0.90-8.61
3. Rapidly fatal disease 3.89 0.92-16.40
4. Upper abdominal/ thoracic surgery 4.34 1.43-13.14
5. lntubation 2.09 0.49-9.04
6. Altered mental status 1.62 0.53-4.91
7. Nasogastric tube (l-6 d) 6.48 2.12-19.82
8. Hz-blockers 0.92 0.64-6.80
9. Recent bronchoscopy 2.95 1.02-8.52
Inconditional k&tic regression.
due
0.19
0.07
0.06
0.008
0.31
0.39
0.0008
0.21
0.04
cal significance (p = 0.25). The incidence of NP also increased among obese patients (24% in obese, 12% in nonobese) and smokers (17% in smokers, 8% in nonsmokers), but these differences also did not achieve statistical significance.
Selected risk factors were entered into a logistic regression model, and a multivariate analysis was performed. Only upper abdominal/thoracic sur- gery, presence of an NG tube, and recent bronchos- copy emerged as statistically significant, indepen- dent risk factors for NP (Table II). Of the 10 case-patients in whom bronchoscopy was recorded as a risk factor, two had three or more bronchoscop- ic procedures prior to NP. In addition to the above factors, the presence of ultimately fatal and rapidly fatal underlying illnesses approached statistical sig- nificance (p = 0.07 and 0.06, respectively).
The rate of NP also varied by admission diagno- sis. While 5.5% of patients with diagnoses involving the cardiopulmonary system developed NP, 23% of patients with diagnoses involving the abdominal system and 19% of patients with head trauma and central nervous system dysfunction developed NP. Although these differences were statistically signif- icant (Fisher’s exact p = 0.015) on univariate analy- sis, they did not achieve statistical significance on multivariate analysis.
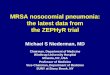
A relationship between the duration of exposure to each of three identified risk factors and the de- velopment of NP was sought. The odds of develop- ing NP during each period of exposure to a single risk factor while controlling for other risk factors are presented in Figure 1. The risks associated with endotracheal intubation and altered consciousness,
20
10
a
6
4
2
n I v NGTUBE INTUBATION ALTERED MENTAL
STATUS
Selected RI Faders
NO9OCOMlAL PNEUMONIA IN THE ICU / JOSH1 ET AL
Flgure 1. Duration of exposure to selected risks (Day 0 = 72- hour ICU stay) and the odds of nosocomial pneumonia rela- tive to patients with no exposure (other risk factors held con- stant). NG = nasogastric.
although not statistically significant, were highest when these factors were present for 1 to 4 days after the 72 hours required for study entry (endotracheal intubation, OR = 2.2 to 2.5; altered consciousness, OR = 1.4 to 2.0). The risk then declined; ORs of less than 1 were observed at 7 days. The risk associated with the NG tube was highest during the first 6 days (OR = 6.0 to 19.5). Although a subsequent decrease in risk was observed, the OR was still greater than 2 at 7 days.
The case-fatality rate for patients with NP was 46% compared with a crude mortality of 22% among non-cases (x2 = 7.01, df = 1, p = 0.008). Odds of death among the cases were 2.5 (95% CI = 0.946 to 6.57) times the odds among non-cases, when controlling for severity of illness (exact Mantel- Haenszel p = 0.054). Of 17 case-patients greater than 60 years of age, 11 (65%) died as compared with 1(14%) of 7 case-patients 40 to 60 years of age. Neither of two patients less than 40 years old died. These differences were statistically significant (x2 = 6.36, df = 1, p = 0.012). No other factor was associated with an increased risk of mortality.
The Scoring System and Its Use in the Study Cohort Table III presents the scoring system that was
derived from the selected logistic model. The score assigned to each risk factor represents the rounded OR for that risk factor from the logistic model. The scores for each risk factor present in a given patient are multiplied by one another and then multiplied by a constant factor or base odds [K = 0.00251 to yield the odds of developing NP. As an example, a 70-year-old intubated patient with an NG tube who has recently undergone abdominal surgery would
199 August 1992 The Amerlcen Journal of Medicine Volume 93

NOSOCOMIAL PNEUMONIA IN THE ICU / JOSHI ET AL
r TABLE III Scoring System to Stratify Patients by Risk of Developing Nosocomial Pneumonia*
L
Score [Sl if Risk Risk Factor Factor Present
1. Age>60y 2
2. Ultimately fatal disease 3
3. Rapidly fatal disease 4
4. Upper abdominal/thoracic surgery 4
5. lntubation 2
6. Altered consciousness 1.5
7. Nasogastric tube 6.5
8. Hz-blocker therapy 2
9. Recent bronchoscopy 3 *Calculated odds of ncsmxmlal pneumonia: odds = K x S1 x S2 x Sq, where S = 1 if factor absent and above score if present and where K = 0.0025 (e.g., patient with factors 3, 4, and 7 present: odds = 0.0025 x 4 x 4 x 6.5 = 0.26; “high risk” if odds >O.ll [sensitivity 85%, specificity 66961).
have calculated odds of developing NP of 0.13 [O&O25 X 2 X 6.5 X 41 or 13%:
Based on an analysis of the sensitivity and speci- ficity of the logistic model with different cut-points for the threshold odds of high risk (Figure 2, ROC curve, area under curve = 0.856), we chose odds of 0.11 (probability of 0.10) as a minimum level for classifying a patient as at high risk for NP. The patient in the above example would therefore be classified as being at high risk.
The scoring system, with this break-point, was then applied to estimate the odds of NP for any patient residing in the ICU for 72 hours or more. Using this bedside scoring system, predicted odds of NP were close to those of the logistic model. At the break-point value of 0.11,4 of 26 patients who eventually developed NP were classified as “low risk.” Using this break-point value, the model has a positive predictive value of 0.268 and a negative predictive value of 0.967.
COMMENTS We have developed a predictive model that may
be used to stratify adult patients admitted to the ICU into high- and low-risk groups for NP. Patients identified as being at high risk are potentially the most likely to benefit from preventive interven- tions. This model is simple to use at the bedside and has a high sensitivity. Eighty-five percent of NP cases were among the 82 patients identified as “high risk” by the model. The positive predictive value of the model (0.267) is more than twice the predictive
0.2 0.4 0.6 0.6 1.0
False-Positive Rate
Flgure 2. Receiver operating characteristic (ROC) curve for the logistic model.
value of admission to the ICU for 3 days or more (0.128). Thus, the model substantially improves one’s ability to segregate high-risk patients. At the same time, the high predictive negative value (0.967) ensures that few patients who will develop pneumonia are falsely classified as low risk. Given that the purpose of this model is to classify patients broadly into risk groups, the false-positive rate of 34% is reasonably low. When intervention studies are planned, however, an awareness of the false- positive rate is especially important. If, for exam- ple, a potentially toxic prophylactic drug regimen is planned for the high-risk patients, this false-posi- tive rate may be viewed as high. In contrast, if a relatively safe, but expensive prophylactic regimen is being considered, the false-positive rate is accept- ably low. Of note, the threshold that was used (odds = 0.11, probability of NP = 0.10) to stratify patients into high- and low-risk groups was arbitrary in that it was based on a nonstatistical evaluation of the relative clinical disadvantages of misclassifying pa- tients into high- or low-risk groups. Although it is appropriate for most purposes for which this model is designed, it could be changed to yield different sensitivities and specificities as is evident from the ROC curve (Figure 2). Choice of a higher threshold would reduce the false-positive rate but at a cost of increasing the false-negative rate (one true-positive rate) as reflected by movement down the ROC curve.
The ability of this model to “flag” certain ICU patients as being at high risk has an additional ad- vantage. In the high-risk patients, infection control precautions should be rigorously followed, and the
August 1992 The American Journal of Medlclne Volume 93 139

need for invasive interventions should be carefully assessed. In a previous study, the overall risk of nosocomial infection was significantly reduced when high-risk patients were identified early in the admission [ 191.
Three independent risk factors for NP were iden- tified using multivariate analysis. These included upper abdominal/thoracic surgery, the presence of an NG tube, and recent bronchoscopy. In addition, the presence of ultimately and rapidly fatal illness- es approached conventional statistical significance.
Although several of these risk factors have previ- ously been recognized, therapeutic bronchoscopy, performed for respiratory toilet, is a preventable risk factor not emphasized in earlier studies. The infectious complications of fiberoptic bronchosco- py have been reported by other workers. In a retro- spective, questionnaire survey, Credle et al [20] re- ported data on 24,521 bronchoscopies and identified only 2 pneumonias related to the proce- dure. Noting the obvious shortcomings of such a survey, Pereira and co-workers [21] did a prospec- tive study of 100 fiberoptic bronchoscopies. Fever occurred after the procedure in 16% of cases and parenchymal infiltrates followed in 6%. Although most infiltrates were transient, one patient died of a rapidly progressive pneumonia. Advanced age and the endoscopic finding of an abnormality were not- ed as possible predisposing factors. A case of a fatal pneumococcal bronchopneumonia with septicemia in an elderly man after bronchoscopy has been de- scribed [22]. In addition, two reports [23,24] have emphasized the propensity of elderly patients with underlying medical diseases to develop pneumonia after bronchoscopy. In most of these studies, bron- choscopy was performed for diagnostic purposes. To our knowledge, there are no data on the infec- tious complications of therapeutic bronchoscopy, a procedure frequently performed in the ICU. In the ICU setting, bronchoscopy is likely to be overlooked as a predisposing factor for NP since patients are perceived as being at high risk independent of the procedure.
The association between the use of therapeutic bronchoscopy and the development of NP must be viewed with caution. It is possible that the common indications for which bronchoscopy was performed, i.e., increased respiratory secretions or pulmonary atelectasis, placed this group of patients at a high risk of NP independent of the procedure. Further studies are needed to establish a clear causal rela- tionship between therapeutic bronchoscopy and NP.
Several risk factors identified in previous studies did not emerge as statistically significant in this
study. These include older age, smoking, COPD, obesity, malnutrition (low serum albumin level), and tracheostomy. While a trend towards increased risk of NP was noted in patients older than 60 years and the obese, information on the presence of smok- ing, COPD, and malnutrition was not available in many patients, restricting the ability to draw mean- ingful conclusions from these data. There were too few patients with a tracheostomy to make statisti- cal comparisons. Antacids such as Mylanta (alumi- na, magnesia, and simethicone), were never used alone in our ICU. They were always used with an Hz blocker. Therefore, we chose to combine these vari- ables. The measurement of gastric ph is not per- formed in our ICU.
This study also examined the relationship be- tween the duration of exposure to various risk fac- tors and the subsequent development of NP. An NG tube was associated with the highest risk of NP during the first 1 to 6 days of its presence after 72 hours in the ICU. The risks associated with endo- tracheal intubation and altered consciousness, al- though not statistically significant, were highest during the first 1 to 4 days. After this time, the risk associated with these factors decreased. The rela- tionship between the duration of endotracheal intu- bation and the development of NP has been exam- ined by several authors. Fagon et al [25] estimated an increased risk of lo/o/d of mechanical ventilation. Torres et al [5], using multivariate analysis, report- ed an increased incidence of NP among patients ventilated for greater than 5 days as compared with less than 5 days. However, only Langer et al [26] have carefully analyzed the effects of increasing lengths of endotracheal intubation on NP. Using life-table analysis, the authors demonstrated a high and constant rate of acquisition of NP in the first 8 to 10 days of endotracheal intubation, with a low rate thereafter. Our data suggest a similar trend for increasing lengths of endotracheal intubation, al- tered mental status, and the presence of an NG tube. Information on the “dose-response” effect of other risk factors upon NP has not been reported.
A unifying pathogenetic explanation for the high initial risk followed by a decline is not obvious. It is tempting to hypothesize that the initial period in the ICU involves the interaction of several risk fac- tors and that this is the cause of the high risk. How- ever, the trend was seen for each of the three risk factors when all other factors were held constant in the model. It is possible that there may be other environmental factors operating in the initial peri- od that were not studied. In addition, host factors may explain this pattern. Immunologic abnormali- ties have been identified in at least two groups of
NOSOCOMIAL PNEUMONIA IN THE ICU / JOSHI ET AL
140 August 1992 The American Journal of Medicine Volume 93

NOWCOMIAL PNEUMONIA IN THE ICU / JOSHI ET AL
patients, i.e., those undergoing abdominal surgery and those hospitalized after trauma [27,28]. These abnormalities, especially low immunoglobulin lev- els, are present during the first few days after the event and then spontaneously normalize. This may, at least in part, explain the increased susceptibility to infection during the early ICU stay. Alternative- ly, an “exhaustion” of the “susceptible” population of patients with time may account for the decline in the incidence of NP.
The crude mortality rate of patients with NP in this study was 46% and is comparable with the mor- tality rates of 20% to 50% reported in previous stud- ies [3,4]. When underlying severity of illness was controlled for, the risk of death continued to be significantly higher in patients with NP than among controls. A complete analysis of prognostic factors could not be done because of the small num- ber of case-patients. However, a significantly higher mortality rate was noted among patients older than 60 years. The mortality rates in this study empha- size the persisting high mortality associated with NP.
Three limitations of our study deserve mention: First, despite a large cohort, the total number of cases of NP meeting our relatively rigorous defini- tion was small. While this may have limited the power of the study to detect some risk factors, sev- eral others emerged as statistically significant and have been noted by previous authors as clinically relevant. Second, the first 72 hours of stay in the ICU were not studied. This “cut-off’ was chosen based on previous data indicating that a large pro- portion of patients admitted to this ICU are dis- charged within this time period and that this group of patients are at a very low risk of NP. Therefore, this predictive model cannot be applied to patients during their very early ICU stay. Finally, pathologic evidence or protected brush bronchoscopy speci- mens were not required for diagnosing NP. As a result, some cases with noninfectious etiologies for pulmonary infiltrates may have been misclassified as NP. Again, previous investigators have used sim- ilar definitions and have identified similar risk fac- tors [5,6]. Further, the study criteria were practical, yet fairly stringent. During the study period, two infection control nurses performing independent surveillance in the ICU, using criteria developed by the Centers for Disease Control [29], identified 55 cases of NP. These included all the cases identified in the study.
Caution is warranted when using this model at the bedside. It applies only to patients residing in the ICU for at least 72 hours and may not be useful in other settings. Also, while it has good predictive
ability in the cohort from which it was derived, it will need to be cross-validated on a separate cohort of ICU patients before its clinical utility is estab- lished. With continued use of this model, other fac- tors may be added to increase its sensitivity and specificity.
In conclusion, we have developed a clinically use- ful method to identify those patients in the ICU who are at greatest risk for NP. This study also identified a decline in the relative risk of NP with time associated with endotracheal intubation, al- tered consciousness, and use of an NG tube. A pre- viously unidentified factor, therapeutic bronchos- copy, was shown to have a significantly increased relative risk for the development of NP. If a causal association is confirmed by further study, the risks and benefits of this procedure in the ICU will need to be re-evaluated.
ACKNOWLEDGMENT We thank John Goldman, M.D., Michael Weitekamp, M.D., and Robert Aber, M.D., for useful suggestions and Joanne Hutton for secretarial support.
REFERENCES 1. Pennington JE. Hospital-acquired pneumonia. In: Wenzel RP. editor. Preven- tion and control of nosocomial infections. Baltimore: Williams & Wilkins, 1987: 321-34. 2. Hughes JM. Epidemiology and prevention of nosocomial pneumonia. Curr Clin Top Infect Dis 1988; 9: 241-59. 3. Gross PA, Neu HC, Aswapokee P. et al. Deaths from nosocomial infection: experience in a university hospital and a community hospital. Am J Med 1980; 68: 219-23. 4. Stevens RM. Teres D, Skillman JJ. Feingold DS. Pneumonia in an intensive care unit. Arch Intern Med 1974; 134: 106-11. 5. Torres A, Aznar R, Gatell JM. et a/. Incidence. risk and prognosis factors of nosocomial pneumonia in mechanically ventilated patients. Am Rev Respir Dis 1990; 142: 523-8. 6. Craven DE, Kuncher LM, Klinsky V, Lichtenberg DA, Make BJ. McCabe WR. Risk factors for pneumonia and fatality in patients receiving continuous mechan- ical ventilation. Am Rev Respir Dis 1986; 133: 792-6. 7. Garibald RA, Britt RM. Coleman ML, Reading JC, Pace NC. Risk factors for postoperative pneumonia. Am J Med 1981; 70: 677-80. 8. Celis R, Torres A, Gatell JM. et al. Nosocomial pneumonia. A multivariate analysis of risk and prognosis. Chest 1988; 93: 320-4. 9. Driks MR, Craven DE, Celli BR. et al. Nosocomial pneumonia in intubated patients given sucraifate as compared with antacids or histamine type 2 blockers. The role of gastric colonization. N Engi J Med 1987; 317: 1376-82. 10. McCabe WR. Jackson GG. Gram-negative bacteremia: I. Etiology and ecolo- gy. Arch Intern Med 1962; 110: 847-55. 11. Landis R. Heyman ER, Koch GG. Average partial association in three-way contingency tables: a review and discussion of alternative tests. Int Stat Rev 1978; 46: 237-54. 12. STATXACT. V2.0. Cambridge, MA; Software Corp., 1991. 13. Breslow NE, Day NE. The analysis of case-control studies. Lyon, France: IARC Scientific Publications, 1980. 14. Zelen M. The analysis of several 2 X 2 contingency tables. Biometrika 1971; 58: 129-37.
15. Hosmer DW, Lemeshow S. Applied logistic regression. New York: Wiley,
1989. 16. SAS Institute. SAS/STAT users guide: release 6.03. Cary, NC: SAS, 1988. 17. SAS Institute. SAS technical report p-200. Cary, NC: SAS, 1990.
August 1992 The American Journal of Medicine Volume 93 141

NOSOCOMIAL PNEUMONIA IN THE ICU / JOSHI ET AL
18. Weinstein M, Fineberg HV. Elstein AS, et al. Clinical decision analysis. Phila- delphia: Saunders, 1980. 19. Britt MR, Schkupner CJ. Matsumiya S. Severity of underlying disease as a predictor of nosocomial infection. Utility in the control of nosocomial infection. JAMA 1978; 239: 1047-51. 28. Credle WF. Smiddy JF. Elliott RC. Complications of fiberoptic bronchoscopy. Am Rev Respir Dis 1974: 109: 67-72. 21. Pereira W. Kovnat DM, Khan MA. Fever and pneumonia after flexible, fiber- optic bronchoscopy. Am Rev Respir Dis 1975; 112: 59-64. 22. Beyt BE Jr, King DK. Gfew RH. Fatal pneumonitis and septicemia after fiberoptic bronchoscopy. Chest 1977; 72: 105-7. 23. Timms RM. Harrell JH. Bacteremia related to fiberoptic bronchoscopy. A care report. Am Rev Respir Dis 1975; 111: 555-7. 24. Pereira W. Kovnat DM, Snider GL. A prospective co-operative study of com- plications foflowing fiberoptic bronchoscopy. Chest 1978; 73: 813-6.
25. Fagon JI, Chastre J. Domart Y, et al. Nosocomial pneumonia in patients receiving continuous mechanical ventilation. Prospective analysis of 52 epi- sodes with use of a protected specimen brush and quantitative culture tech- niques. Am Rev Respir Dis 1989; 139: 877-84. 28. Langer M, Mosconi P, Cigada M. Mandell M. Long-term respiratory support and risk of pneumonia in critically il l patients. Am Rev Respir Dis 1989; 140: 302-5. 27. Glinz W, Grob PJ, Nydesser VE, et a/. Polyvalent immunoglobulins for pro- phylaxis of bacterial infections in patients following trauma. A randomized, pla- cebocontrolled study. Intensive Care Med 1985; 11: 288-94. 28. Alexander JW. Stinnett JD. Dgfe CK, et a/. A comparison of immunologic profiles and their influence on bacteremia in surgical patients with a high risk of infection. Surgery 1979; 86: 94-104. 29. Site definitions. In: National Nosocomial Infections Surveillance (NNIS) man- ual. Atlanta, GA: US Department of Health and Human Services, 1987: Xl 11-3.
142 August 1992 The American JOUrn8l of Medicine Volume 93
![Neumonia nosocomial [Modo de compatibilidad] · Guia Neumonía nosocomial Separ. ... pneumonia. Title: Microsoft PowerPoint - Neumonia nosocomial [Modo de compatibilidad] Author:](https://img.pdfslide.net/doc/110x75/5c94920609d3f2c2238cacb0/neumonia-nosocomial-modo-de-compatibilidad-guia-neumonia-nosocomial-separ.jpg)