Embed Size (px)
Citation preview

Review Article
A Primer on Image-guided Radiation Therapyfor the Interventional RadiologistNishita Kothary, MD, Sonja Dieterich, PhD, DABR, John D. Louie, MD, Albert C. Koong, MD,
Lawrence Vincent Hofmann, MD, and Daniel Y. Sze, MD, PhD
The use of image-guided radiation therapy in thoracic and abdominal tumors is increasing. Herein, the authors reviewthe process of image-guided radiation therapy and describe techniques useful for optimal implantation of fiducialmarkers.
J Vasc Interv Radiol 2009; 20:859–862
Abbreviation: DRR � digital deconstructed radiograph
IMAGE-GUIDED radiation therapy isan emerging field integrating a highlyfocused radiation therapy system withtwo- and three-dimensional imagingtechniques to produce frameless spa-tial registration, allowing for preciselocalization and targeting of tumors.Imaging guidance and the use of ra-diographic landmarks eliminate theneed for rigid, stereotactic frame fixa-tion. However, respiratory motion re-mains a major source of error and un-certainty for extracranial applicationsof image-guided radiation therapy (1–4). As image-guided radiation therapyevolves into exploiting hypofraction-ated courses of treatment by usinglarge doses of radiation per fraction,the issue of precision becomes increas-ingly more important to maximizeboth treatment efficacy and safety. A
From the Departments of Interventional Radiology(N.K., J.D.L., L.V.H., D.Y.S.) and Radiation Oncol-ogy (S.D., A.C.K.), Stanford University Medical Cen-ter, 300 Pasteur Dr, H3630, Stanford, CA 94305. Re-ceived February 3, 2009; final revision receivedMarch 24, 2009; accepted March 26, 2009. Addresscorrespondence to N.K.; E-mail: [email protected]
S.D. received an $8,000 research grant from Accuray,Inc.
None of the authors have identified a conflict ofinterest.
© SIR, 2009
DOI: 10.1016/j.jvir.2009.03.037
multitude of image-guided radiationtherapy systems are available, includ-ing CyberKnife (Accuray, Sunnyvale,California), Elekta XVI (Elekta, Stock-holm, Sweden), and Novalis Tx (Var-ian Medical Systems, Palo Alto, Cali-fornia) among others. The followingparagraphs describe our experiencewith one such system, the CyberKnife.The CyberKnife uses orthogonal digi-tal radiography (x-rays) and respirato-ry-triggered software to track im-planted fiducial markers in real time(5,6). As image-guided radiation ther-apy systems become more widelyavailable, interventionalists will in-creasingly participate in the care ofthese patients, placing fiducial mark-ers or combining image-guided radia-tion therapy with other conventional,percutaneous, or catheter-based thera-pies such as ablation and transhepaticarterial chemoembolization. A thor-ough understanding of the physicsand applications of image-guided ra-diation therapy is becoming essentialto providing appropriate patient care.
COMPONENTS OF THECYBERKNIFE SYSTEM
The CyberKnife is a commerciallyavailable image-guided radiation ther-apy system that combines image guid-ance, tracking technology, and roboticsto offer frameless precision stereotactic
radiation therapy. It consists of a light-weight, 6-MV, linear accelerator specifi-cally designed for radiation therapy thatis mounted on a highly maneuverablerobotic arm capable of precise position-ing and aiming of the linear acceleratorwith a total radial error of less than 0.6mm (7). Radiographic landmarks, ob-tained by two fixed x-ray sources ar-ranged orthogonal to the patient, elimi-nate the need for skeletal fixation bycorrecting for patient movement duringtreatment. In addition, to compensatefor respiratory motion, the CyberKnifeuses a continuous respiratory trackingsystem called the Synchrony (Accuray).Adjustments for respiratory variationsare made by correlating the motion ofradiopaque fiducial markers implantedin and around the tumor with chest orabdominal wall excursions. The fiducialmarkers act as internal radiographiclandmarks, ideally maintaining a fixedrelationship within the tumor and witheach other. The location of the fiducialmarkers on the orthogonal digital recon-structed radiographs (DRRs) obtainedduring the treatment indirectly specifiesthe spatial position of the tumor duringall phases of respiration. Differences inthe three translational directions andthree rotational angles (six-dimensional)are measured by using computer algo-rithms (8). On the basis of these calcu-lations, the robotic manipulator com-pensates for the differences andretargets the radiation beam, hence
maintaining targeting accuracy. This859

860 • Percutaneous Implantation of Fiducial Markers for Image-guided Radiation Therapy July 2009 JVIR
complete process of image acquisition,registration, and compensation is au-tomated and fast enough to providereal-time localization for extracranialapplications (5,9).
TECHNIQUE FORPERCUTANEOUS PLACEMENTOF FIDUCIAL MARKERS
At our institution, most percutane-ous fiducial marker implantations areperformed by using computed tomo-graphic (CT) guidance in a manner sim-ilar to that of percutaneous biopsies. Insome applications, fiduical markers canalso be placed under fluoroscopic, ultra-sonographic (US), bronchoscopic, or en-doscopic guidance. Procedures are per-formed with the patient under moderatesedation (intravenous midazolam andfentanyl) administered by a registeredradiology nurse. A preliminary unen-hanced CT scan is obtained and an ap-propriate needle trajectory determined.The skin entry site is prepared in a ster-ile fashion and local anesthesia (lido-caine 1%) administered. We routinelyuse a 19-gauge thin-wall coaxial intro-ducer needle (Allegiance; CardinalHealth, Dublin, Ohio) to implant the fi-ducial markers. The coaxial needle isadvanced into the lesion under CT flu-oroscopy guidance in a standard fash-ion. A vertical or semivertical trajectoryis preferred so that gravity can help“drop” the fiducial markers. We use cy-lindrical gold fiducial markers measur-ing 0.8 mm in diameter and 5 mm inlength (Alpha-Omega Services, Bell-flower, California) for tumors in solidorgans and 2 � 3-mm VortX 0.018-inchdiamond-shaped platinum microcoils(Boston Scientific, Natick, Massachu-setts) for tumors in lung, where solidgold fiducial markers have been foundto migrate (10) .
Sterile gold fiducial markers are bestpicked up from the tray by using asmall, curved hemostat and are placedin the hub of the 19-gauge coaxial intro-ducer needle. With use of the trocar ofthe 19-gauge introducer needle, the fi-ducial marker is advanced through theshaft of the introducer needle. Occasion-ally, the fiducial marker may get“stuck” in the hub of the needle, ob-scured by blood; hence, it is crucial toverify the deposition of each fiducialmarker with imaging. Fluoroscopy of-fers the ability to monitor advancement
and deposition of the fiducial marker inreal time and, hence, may offer an ad-vantage over CT for tumors that are eas-ily visible with fluoroscopy. When mi-crocoils are used as fiducial markers, thecasing that houses the coil is placedwithin the hub of the 19-gauge intro-ducer needle and the coil is initiallypushed through the shaft of the intro-ducer by using the coil pusher and thenthe trocar. Alternatively, a smaller-gauge needle, such as a 21-gauge coaxialneedle, can be used to allow for easydeposition of the microcoils. Typically,three to five fiducial markers are placed(see below) by tilting and repositioningthe introducer needle to deposit the fi-ducial markers in a non-collinear fash-ion.
After all the fiducial markers areplaced, limited unenhanced CT is per-formed to document the position ofthe fiducial markers and evaluate forimmediate complications. Patients areroutinely monitored for 4 hours afterplacement and then discharged home.Because previous studies have shownthat gold fiducial markers can migrateand settle for up to a week (11–13), weallow a 1-week interval between theplacement of fiducial markers andtreatment-planning CT. In our past ex-perience, migration of gold fiducialmarkers was the most problematic forthoracic tumors; since then we haveadopted the practice of placing micro-
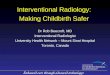
Figure 1. Schematic diagram of the Cybeoblique to the patient with the flat-panel demarks indicate collinear fiducial markers. Inindividual fiducial markers, they should noangulation.
coils because these appear to be rela-
tively more stable (14). To overcomethe problems of migration, alternativemethods of placement such as endo-scopic US, electromagnetically navi-gated bronchoscopy, and endovascu-lar placement of fiducial markers havebeen tried (15–17). In addition to goldfiducial markers and microcoils, alter-nate agents such as titanium clips (inbreast) have also been used; however,experience with this is limited andwarrants further studies.
OPTIMAL PLACEMENT OFFIDUCIAL MARKERS
To enable accurate detection of thefiducial markers, the importance ofcorrect geometric positioning of themarkers cannot be overstated (18). Theorthogonal x-ray sources are mountedon the ceiling while the imagers areplaced under the treatment table. Theorientation of the x-ray source is suchthat the DRRs are obtained in the 45°right and left posterior oblique views,as demonstrated in Figure 1. Hence,placement of the fiducial markersshould be such that no two markers liein the same line when viewed alongeither of the 45° angles used for imag-ing.
Typically, three to five fiducialmarkers are implanted. Fewer thenthree fiducial markers would result in
ife shows two x-ray sources angled at 45°ors placed under the patient table. The twoder for the CyberKnife system to recognizee collinear when viewed from 45° oblique
rKntect
ort b
translational tracking only. For a full

e sa lati
Kothary et al • 861Volume 20 Number 7
six-dimensional translational and rota-tional localization, at least three prop-erly placed fiducial markers are need.The fiducial markers should be placedin a way that their movement corre-sponds to the movement of the target.Preferably all fiducial markers shouldbe placed within the tumor. In tumorsthat are smaller than 2 cm, however,this may obscure the tumor margins;
Figure 3. (a,b) Axial unenhanced CT scmetachronous adenocarcinoma in the righfiducial markers (numbered 3 and 4) in th
hence, one fiducial marker should be
placed within the tumor and the restalong the perimeter of the tumor.
It is often inevitable that the final po-sition of one or more fiducial markers isnot optimal; in these instances, we sug-gest implanting additional fiducialmarkers. Because fiducial markers cancause artifacts and obscure adjacentmarkers, adjacent markers should bephysically at least 1.5 cm (preferably 2
and (c) DRR in the left posterior obliqd left lungs. Images demonstrate clusteredme line, making the six-dimensional trans
cm) apart and on the orthogonal views
should appear at least 1 cm apart. Giventhese requirements, one possible algo-rithm would be to imagine the tumor asa tetrahedron and to place fiducialmarkers in each corner. Another algo-rithm would be to imagine a cube andplace two fiducial markers in the cranio-caudal axes (one marker cranial and an-other caudal) and the other two fiducialmarkers in the anteroposterior axes (one
Figure 2. (a–d) Axial unenhanced CTscans in a 60-year-old patient with alarge caudate mass with implanted fidu-cial markers. (e) Corresponding DRR ob-tained in the right posterior oblique anglein the same patient at the time of treat-ment. The images demonstrate four dis-tinct well-placed fiducial markers (num-bered 1–4) that allow for a full six-di-mensional translational and rotationallocalization. A � anterior, Caud � caudal,Cran � cranial, P � posterior.
projection in a 55-year-old patient withducial markers (numbered 1–4), with twoonal and rotational localization difficult.
ans uet an fi
marker anterior and one marker poste-

862 • Percutaneous Implantation of Fiducial Markers for Image-guided Radiation Therapy July 2009 JVIR
rior). Another placement algorithmwould be two fiducial markers in theanterior-posterior axis (one marker an-terior and another posterior) and twofiducial markers to the left and right ofthe midline such that none of the fourfiducial markers are collinear on the 45°oblique views. If fluoroscopy is avail-able at implantation, a simple techniquewould be to rotate the C-arm 45° in bothright and left oblique views to visualizewhere the fiducial markers would bedeposited before actually depositingthem. Patients with metallic hardwareneed detailed planning because thehardware can completely obscure thefiducial markers. In such situations, notonly should the fiducial markers not bein the same axial plane as the bulk of thehardware (because the hardware willcause substantial artifacts at CT) butalso the fiducial markers should not becollinear with the hardware in theoblique views. All fiducial markersshould be within 10 cm of each other toaccommodate for the field of view of theimaging and targeting software.
Correlation of axial CT scans to DRRsobtained at the time of CyberKnife useis described in Figures 2 and 3. AxialCT scans in Figure 2 demonstrate alarge caudate mass with implanted fi-ducial markers. The DRR obtained inthe right posterior oblique in the samepatient a week later demonstrates fourdistinct well-placed fiducial markers.Conversely, the DRR in another pa-tient (Fig 3) demonstrates the fiducialmarkers clustered together. Two of thefiducial markers are superimposed onthe same line and are hence indistin-guishable.
In conclusion, the optimal placementof fiducial markers for successful image-guided radiation therapy can be chal-lenging. A proper understanding of the
physics behind image-guided radiationtherapy and the methodology em-ployed to visualize and target the tumoris crucial to place the least number offiducial markers in the most beneficialmanner.
References1. Ohara K, Okumura T, Akisada M, et al.
Irradiation synchronized with respira-tion gate. Int J Radiat Oncol Biol Phys1989; 17:853–857.
2. Ross CS, Hussey DH, Pennington EC,Stanford W, Doornbos JF. Analysis ofmovement of intrathoracic neoplasmsusing ultrafast computerized tomogra-phy. Int J Radiat Oncol Biol Phys 1990;18:671–677.
3. Davies SC, Hill AL, Holmes RB, Halli-well M, Jackson PC. Ultrasound quan-titation of respiratory organ motion inthe upper abdomen. Br J Radiol 1994;67:1096–1102.
4. Bryan PJ, Custar S, Haaga JR, BalsaraV. Respiratory movement of the pan-creas: an ultrasonic study. J UltrasoundMed 1984; 3:317–320.
5. Adler JR Jr, Murphy MJ, Chang SD,Hancock SL. Image-guided roboticradiosurgery. Neurosurgery 1999; 44:1299–1306, discussion 1306–1297.
6. Schweikard A, Shiomi H, Adler J.Respiration tracking in radiosurgery.Med Phys 2004; 31:2738–2741.
7. Muacevic A, Staehler M, Drexler C,Wowra B, Reiser M, Tonn JC. Technicaldescription, phantom accuracy, and clini-cal feasibility for fiducial-free frameless re-al-time image-guided spinal radiosurgery.J Neurosurg Spine 2006; 5:303–312.
8. Fu D, Kuduvalli G. A fast, accurate,and automatic 2D-3D image registra-tion for image-guided cranial radiosur-gery. Med Phys 2008; 35:2180–2194.
9. Chang SD, Adler JR. Robotics and ra-diosurgery: the cyberknife. StereotactFunct Neurosurg 2001; 76:204–208.
10. Kothary N, Heit JJ, Louie JD, et al.Safety and efficacy of percutaneous fi-ducial marker implantation for image-guided radiation therapy. J Vasc Interv
Radiol 2009; 20:235–239.11. Imura M, Yamazaki K, Shirato H, et al.Insertion and fixation of fiducial markersfor setup and tracking of lung tumors inradiotherapy. Int J Radiat Oncol BiolPhys 2005; 63:1442–1447.
12. Kitamura K, Shirato H, Shimizu S, et al.Registration accuracy and possible mi-gration of internal fiducial gold markerimplanted in prostate and liver treatedwith real-time tumor-tracking radia-tion therapy (RTRT). Radiother Oncol2002; 62:275–281.
13. Shirato H, Harada T, Harabayashi T,et al. Feasibility of insertion/implan-tation of 2.0-mm-diameter gold inter-nal fiducial markers for precise setupand real-time tumor tracking in radio-therapy. Int J Radiat Oncol Biol Phys2003; 56:240–247.
14. de Mey J, Van de Steene J, Vandenbro-ucke F, et al. Percutaneous placementof marking coils before stereotactic ra-diation therapy of malignant lung le-sions. J Vasc Interv Radiol 2005; 16:51–56.
15. Pishvaian AC, Collins B, Gagnon G,Ahlawat S, Haddad NG. EUS-guidedfiducial placement for CyberKnife ra-diotherapy of mediastinal and abdom-inal malignancies. Gastrointest Endosc2006; 64:412–417.
16. Anantham D, Feller-Kopman D, Shan-mugham LN, et al. Electromagneticnavigation bronchoscopy-guided fidu-cial placement for robotic stereotacticradiosurgery of lung tumors: a feasibil-ity study. Chest 2007; 132:930–935.
17. Prevost JB, Nuyttens JJ, HoogemanMS, Poll JJ, van Dijk LC, PattynamaPM. Endovascular coils as lung tu-mour markers in real-time tumourtracking stereotactic radiotherapy: pre-liminary results. Eur Radiol 2008; 18:1569–1576.
18. West JB, Fitzpatrick JM, Toms SA,Maurer CR Jr, Maciunas RJ. Fiducialpoint placement and the accuracy ofpoint-based, rigid body registration.Neurosurgery 2001; 48:810–816, dis-
cussion 816–817.