Embed Size (px)
Citation preview
Autlsafiit
c
e
g
M
o
J Oral Maxillofac Surg63:449-456, 2005
A Qualitative Report of Patient Problemsand Postoperative Instructions
Kathryn A. Atchison, DDS, MPH,* Edward E. Black, DDS, MS,†
Richard Leathers, DDS,‡ Thomas R. Belin, PhD,§ Mirna Abrego, MBA,�Melanie W. Gironda, PhD, MSW,¶ Daniel Wong, BS,#
Vivek Shetty, BDS, DMD,** and Claudia DerMartirosian, PhD††
Purpose: While surgery related stress may interfere with the patient’s ability to concentrate oninstructions, language difficulty or low health literacy may also impede appropriate doctor/patientcommunication. The purpose of this study is to understand from a sample of minority patients the typesof problems encountered during healing and the level of information regarding elements of postoperativeinstructions they recalled receiving at an inner-city safety net hospital. We initiated a qualitative study tounderstand the care sequence process and provision of informed consent and postoperative instruction.
Methods: African American or Latino patients, 18 years of age or older, who had third molars removedunder general anesthesia or received treatment for a mandibular fracture were recruited to participate ina focus group to discuss their treatment. Patients described their problem and any informed consentgiven about treatment risks and benefits and postoperative information they recalled.
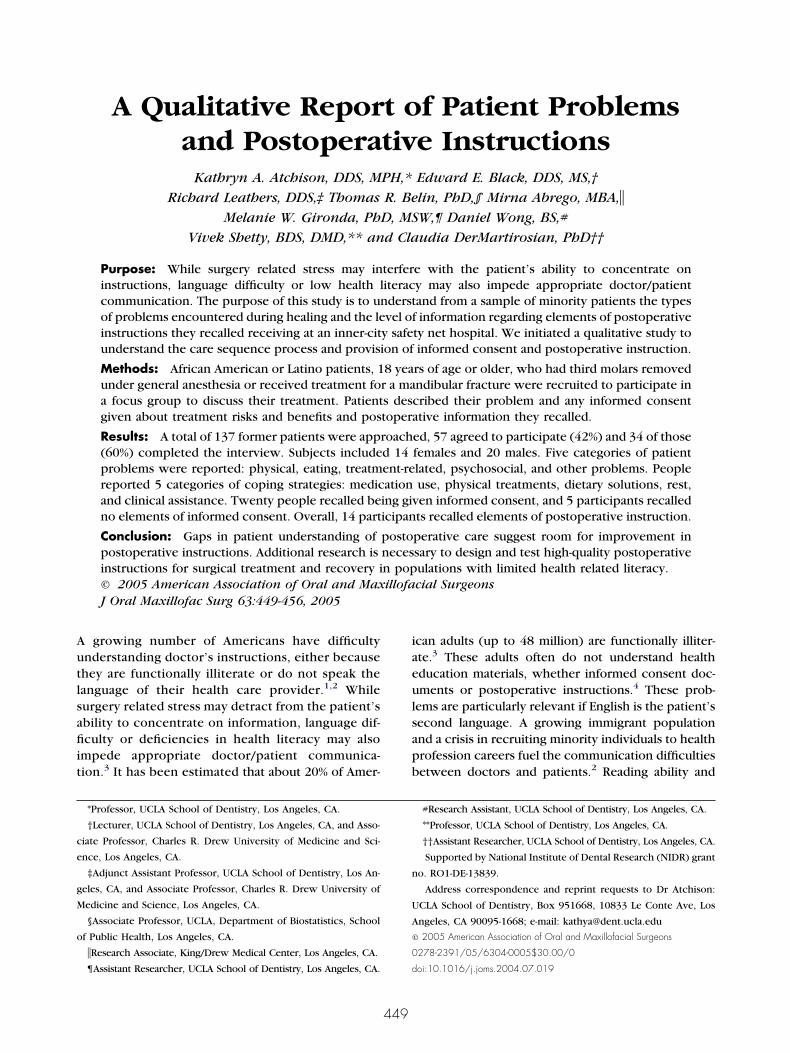
Results: A total of 137 former patients were approached, 57 agreed to participate (42%) and 34 of those(60%) completed the interview. Subjects included 14 females and 20 males. Five categories of patientproblems were reported: physical, eating, treatment-related, psychosocial, and other problems. Peoplereported 5 categories of coping strategies: medication use, physical treatments, dietary solutions, rest,and clinical assistance. Twenty people recalled being given informed consent, and 5 participants recalledno elements of informed consent. Overall, 14 participants recalled elements of postoperative instruction.
Conclusion: Gaps in patient understanding of postoperative care suggest room for improvement inpostoperative instructions. Additional research is necessary to design and test high-quality postoperativeinstructions for surgical treatment and recovery in populations with limited health related literacy.© 2005 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 63:449-456, 2005iaeulsapb
n
U
A
©
0
growing number of Americans have difficultynderstanding doctor’s instructions, either becausehey are functionally illiterate or do not speak theanguage of their health care provider.1,2 Whileurgery related stress may detract from the patient’sbility to concentrate on information, language dif-culty or deficiencies in health literacy may also
mpede appropriate doctor/patient communica-ion.3 It has been estimated that about 20% of Amer-
*Professor, UCLA School of Dentistry, Los Angeles, CA.
†Lecturer, UCLA School of Dentistry, Los Angeles, CA, and Asso-
iate Professor, Charles R. Drew University of Medicine and Sci-
nce, Los Angeles, CA.
‡Adjunct Assistant Professor, UCLA School of Dentistry, Los An-
eles, CA, and Associate Professor, Charles R. Drew University of
edicine and Science, Los Angeles, CA.
§Associate Professor, UCLA, Department of Biostatistics, School
f Public Health, Los Angeles, CA.
�Research Associate, King/Drew Medical Center, Los Angeles, CA.
¶Assistant Researcher, UCLA School of Dentistry, Los Angeles, CA. d
449
can adults (up to 48 million) are functionally illiter-te.3 These adults often do not understand healthducation materials, whether informed consent doc-ments or postoperative instructions.4 These prob-
ems are particularly relevant if English is the patient’second language. A growing immigrant populationnd a crisis in recruiting minority individuals to healthrofession careers fuel the communication difficultiesetween doctors and patients.2 Reading ability and
#Research Assistant, UCLA School of Dentistry, Los Angeles, CA.
**Professor, UCLA School of Dentistry, Los Angeles, CA.
††Assistant Researcher, UCLA School of Dentistry, Los Angeles, CA.
Supported by National Institute of Dental Research (NIDR) grant
o. RO1-DE-13839.
Address correspondence and reprint requests to Dr Atchison:
CLA School of Dentistry, Box 951668, 10833 Le Conte Ave, Los
ngeles, CA 90095-1668; e-mail: [email protected]
2005 American Association of Oral and Maxillofacial Surgeons
278-2391/05/6304-0005$30.00/0
oi:10.1016/j.joms.2004.07.019

cgrp
rsfmett
tmepttiapwrr
sttfcwaoaia
M
citosdLopRs
ulf
KcgtpAtcdprv((f
i(lecCma
pss
wswtfSitip.m
450 PATIENT PROBLEMS AND POSTOPERATIVE INSTRUCTIONS
omprehension of the spoken language, not intelli-ence or level of education, have been found to beelated to understanding of and compliance withostoperative instruction.The type and level of information that patients may
equire to make an informed decision in decidingpecific treatment types is not well understood. Pro-essional standards state that the health care providerust inform the patient about risks and benefits of
ach treatment. Nonetheless, the clinician struggleso succinctly and clearly present relevant informationo a patient.7
Good communication is also critical in assisting pa-ients to appropriately deal with postoperative manage-ent. Studies have shown that adequate postoperative
ducation can improve patient satisfaction and reduceostsurgical morbidity.8 Malins5 pointed out that pa-ients from ethnic minorities might need printed instruc-ions in their native language and the services of annterpreter. Moreover, verbal or a combination of verbalnd written instructions are preferred by most patients,articularly those with lower education.3,4,6 However,ithout written reinforcement the understanding and
etention of verbal instructions over a lengthy period ofecovery cannot be assured.
Alexander3,9 stated that it is time for dental profes-ionals, particularly those in the surgical specialties,o pay more attention to the phrasing, jargon, anderminology used in their postoperative instructionorms, as well as in their office brochures, informedonsent forms, and the like. The purpose of this studyas to elicit information from a minority sample
bout the types of problems encountered followingral surgery, the coping strategies they used to man-ge the problems, and the level of information regard-ng postoperative instructions they recalled receivingt an inner-city safety net hospital.
ethods
We initiated a qualitative study to understand theare sequence process and provision of postoperativenstruction. Qualitative research is defined as descrip-ive, inductive, or phenomenologic research used tobserve events, ask questions with open-ended an-wers, and interpret subject’s personal reactions toevelop emergent speculations or hypotheses.10,11
ittle is known about people’s process of care duringral and maxillofacial surgery and subsequent healinghase. The study was approved by the Institutionaleview Boards at UCLA and Charles R. Drew Univer-ity of Medicine and Science (Los Angeles, CA).
People who received either removal of third molarsnder general anesthesia or treatment for a mandibu-
ar fracture were recruited to participate in hour-long
ocus groups to discuss the treatment they received at .ing/Drew Medical Center. All participants signed 2onsent documents, one to participate in the focusroups and the second to allow video and audioaping of the focus group discussions. We recruitedeople 18 years of age or older who were eitherfrican American or Latino and had recently received
reatment. Lunch was served during the consent pro-ess in order for participants to get to know theoctor facilitators and other participants. Once peo-le had completed their lunch we asked if they wereeady to begin and commenced taping of the inter-iew. Interviews were conducted by the authorsK.A.A., E.B., R.L.). Another author who is bilingualM.A.) conducted the initial recruitment, the in-ormed consent process, and the videotaping.
Focus groups were organized by subject character-stics if sufficient numbers of subjects could be foundgender, race/ethnicity, and treatment type [third mo-ar removal or fracture]). This enabled the interview-rs to probe deeply during focus groups withoutoncern over possible gender or ethnic differences.omparisons of thematic differences by gender, treat-ent type, and race/ethnicity were made during the
nalysis.Using an open-ended interview style, we asked peo-
le to first describe the problem for which they hadought care. Once everyone had related his or hertory, we asked a series of questions regarding:
● Type of risk and benefit information presentedby the doctor during the informed consent pro-cess
● Postoperative instructions and any informationremembered
● Types of postoperative difficulties and their se-verity
● Coping strategies used for resolving problemsencountered
● Success of the coping strategies
After completion of the interview, participantsere thanked and given a $25 honorarium. Tran-
cripts were made from the audio tape. The videotapeas used to clarify specific responses on the audio
ape. We analyzed the recruitment rates of males andemales for patients with fractures and third molars.tatistically, there were no overall gender differencesn agreement to participate, but female fracture pa-ients were marginally statistically less likely to partic-pate (P � .05). In terms of group differences, fractureatients were more likely to agree to participate (P �
003). African American males with fracture wereore likely to agree to participate (63.2%) at P �
001. Table 1 shows the characteristics of the subjects.
R
oaspdpottlll
wmpimt
tbtwdtmtatpd
e(atieipr
A
L
A
L
T
A J Oral
PSNBLDSHTBCGT
A
ATCHISON ET AL 451
esults
PARTICIPANT REPORTED PROBLEMS
Participants were first asked to describe the typesf problems they encountered during the treatmentnd healing process. Our intent was not to determinepecific proportions of people who reported eachroblem, which is not a qualitative aim, but rather toetermine the range of problems with sufficient im-ortance to people that they would recall a problemnce treatment and healing had ended. We also askedhem to consider what bothered them the most, ashey relived their experience. Five categories of prob-ems were reported: physical problems, eating prob-ems, treatment-related problems, psychosocial prob-ems, and other problems.
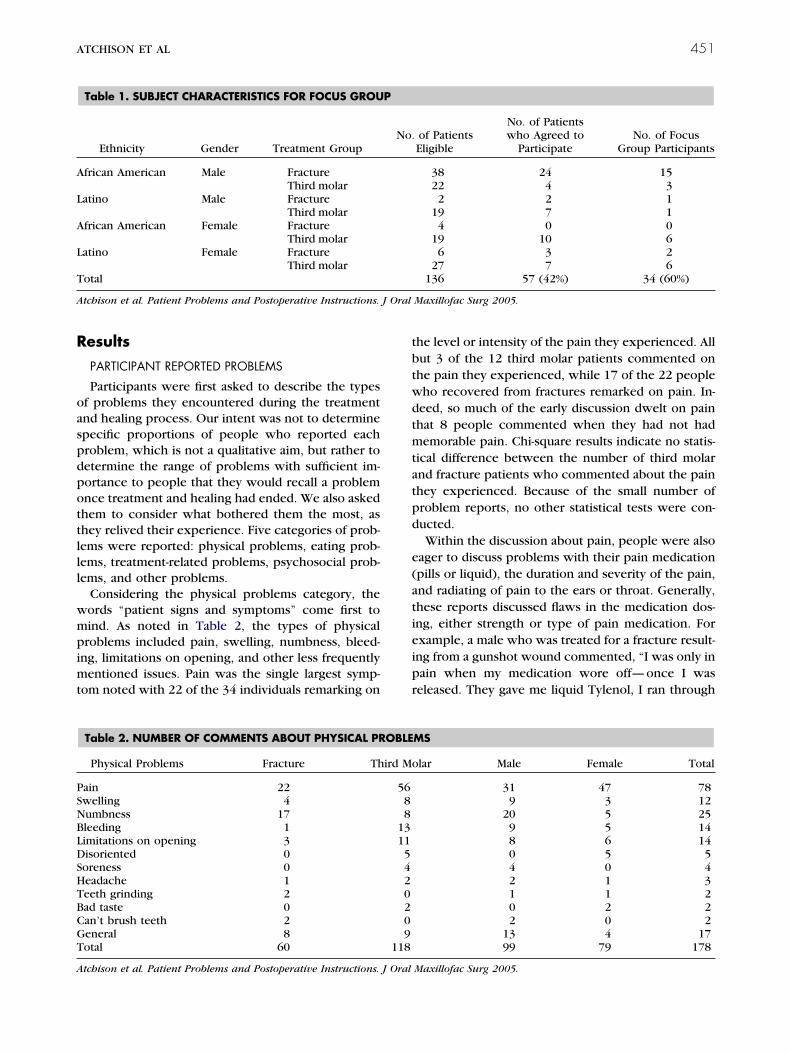
Considering the physical problems category, theords “patient signs and symptoms” come first toind. As noted in Table 2, the types of physicalroblems included pain, swelling, numbness, bleed-
ng, limitations on opening, and other less frequentlyentioned issues. Pain was the single largest symp-
om noted with 22 of the 34 individuals remarking on
Table 1. SUBJECT CHARACTERISTICS FOR FOCUS GROU
Ethnicity Gender Treatment Group
frican American Male FractureThird molar
atino Male FractureThird molar
frican American Female FractureThird molar
atino Female FractureThird molar
otal
tchison et al. Patient Problems and Postoperative Instructions.
Table 2. NUMBER OF COMMENTS ABOUT PHYSICAL PR
Physical Problems Fracture Th
ain 22welling 4umbness 17leeding 1imitations on opening 3isoriented 0oreness 0eadache 1eeth grinding 2ad taste 0an’t brush teeth 2eneral 8otal 60
tchison et al. Patient Problems and Postoperative Instructions. J Oral
he level or intensity of the pain they experienced. Allut 3 of the 12 third molar patients commented onhe pain they experienced, while 17 of the 22 peopleho recovered from fractures remarked on pain. In-eed, so much of the early discussion dwelt on painhat 8 people commented when they had not hademorable pain. Chi-square results indicate no statis-
ical difference between the number of third molarnd fracture patients who commented about the painhey experienced. Because of the small number ofroblem reports, no other statistical tests were con-ucted.Within the discussion about pain, people were also
ager to discuss problems with their pain medicationpills or liquid), the duration and severity of the pain,nd radiating of pain to the ears or throat. Generally,hese reports discussed flaws in the medication dos-ng, either strength or type of pain medication. Forxample, a male who was treated for a fracture result-ng from a gunshot wound commented, “I was only inain when my medication wore off—once I waseleased. They gave me liquid Tylenol, I ran through
of PatientsEligible
No. of Patientswho Agreed to
ParticipateNo. of Focus
Group Participants
38 24 1522 4 32 2 1
19 7 14 0 0
19 10 66 3 2
27 7 6136 57 (42%) 34 (60%)
Maxillofac Surg 2005.
MS
lar Male Female Total
31 47 789 3 12
20 5 259 5 148 6 140 5 54 0 42 1 31 1 20 2 22 0 2
13 4 1799 79 178
P
No.
OBLE
ird Mo
5688
13115420209
118
Maxillofac Surg 2005.

tcrempu
miwIwsteggbwfhpotIff
schclcehjr
wambps
hoccoYicm
dt
8sptfOdfcYfwcrtmwta
rflarmattecAiacth
ttaiicmTcbp
452 PATIENT PROBLEMS AND POSTOPERATIVE INSTRUCTIONS
hat in about 2 days. When I came back to the dentallinic they gave me pills which was OK because I hadubber bands in my mouth—I could open my mouthnough where I could get the pills in.” The liquid painedication, designed to be used for children, wasrescribed for a week’s worth of pain relief but wassed up in 2 days.When asked what the worst thing was about third-olar surgery, many participants reported pain and
ts juxtaposition with other problems. As one womanho had third molars removed said, “It took me likesaid 2 weeks for me to recuperate. I could not eat. Itas very hard for me to eat cause they took 4 at the
ame time. I was having severe. . . fevers and all so allhey gave me was Motrin for me to take, but it was notffective. I guess . . . I think that they know we areoing to have to deal with pain, they should haveiven something else than Motrin . . . 600. I cameack like 2 or 3 times because the pain was worse andorse, and I had to call the doctor.” A man with a
racture resulting from a gunshot wound describedow pain is related to daily physical functioning. “Theain only came when you eat or talk or when Ipened my mouth. My jaw is not even, when I eat oralk, I can feel the difference because of the fact thatwas shot on one side of my face.” People noted the
requency with which the mouth is used for commonunctions.
An African American man with a fracture demon-trated how even the presence of pain was insuffi-ient to assure compliance with doctor regimens. “Iave pain when they ask me to open my mouth. Youan’t open it too far because of the wires. And thatasts a long time. This happened April 7 and I stillan’t open my mouth too far. And I still be trying toat and all, I have to push it in my mouth.” This manad gone for over 7 months with wires closing his
aws. Despite doctor instructions to return for wireemoval, he had not returned to the clinic.
Eating problems were also common to both peopleho had fractures (13 patients made 22 comments)
nd third molar patients (12 patients made 17 com-ents). Types of eating difficulties included having a
ad bite, a dull or stinging taste, and even, for fractureatients who went longer periods on liquid diets, oftomach problems once food was reintroduced.
One aspect that participants clearly described isow the disruption of eating influences social aspectsf an individual’s life. As one man with a fractureaused by a gunshot injury reported when asked toompare having a broken bone in the face with a limbr another part of the body, “Oh no, not your face!ou see, that’s your vocal, that’s your mouth—when
ts time to eat, its time to eat. You can’t even eat porkhops, can’t open your mouth to eat chicken. I
issed Thanksgiving, Easter, and all the good holi- rays. I was stuffing food through this (missing)ooth.”
Treatment-related problems included irritating wires forfracture patients whose jaws were wired shut, and
utures for a third molar patient. Two people com-lained of broken teeth, 4 fracture patients notedheir jaws were now crooked, and 2 people who hadractures remarked on difficulties with swallowing.ne man who had maxillomandibular fixation clearlyescribed the difficulty people experience whenaced with wires breaking: “I had to get the wireutters and cut them. It was painful to lift your lip up.ou were bleeding from your lip. You’d be bleeding
rom your lip and the wires be sticking.” A Latinahose fracture was treated also noted the problem of
uts associated with broken wires. Her loose wiresesulted from tooth brushing. “When I brush myeeth, the brush moves the braces around and itakes me feel really uncomfortable . . . One of theires broke while I was brushing my teeth. Every
ime that I smile, the loose wire would scratch my lipnd would sometimes make my lip bleed.”
Finally, people who had suffered from a fractureeported psychosocial problems. These problems re-ected the uniqueness of the etiology of the injurynd included nightmares, breathing problems, embar-assment, reliving the experience, and facial disfigure-ent. To give an example, a man who complained
bout his appearance with maxillomandibular fixa-ion recounted that “My pride was killing me! Becausehe guy did this to me. It’s more about pride and whatveryone was saying. I would have killed him. Iouldn’t walk the streets because of what happened.”nother man whose fracture resulted from a gunshot
njury asserted, “I had nightmares and cold sweatsfter I got shot. After I got shot, I became moreonscious about my surroundings.” And he went ono discuss his worries about checking frequently thatis door was locked.
COPING MODALITIES USED TO MANAGEHEALING PROBLEMS
Participants were asked to describe the modalitieshey used to cope with problems encountered duringheir healing from the surgery. This question wassked before a discussion about the postoperativenstructions to not influence their memory of thenstructions. Participants reported 5 categories ofoping strategies: medication use, physical treat-ents, dietary solutions, rest, and clinical assistance.able 3 shows 21 of the 34 subjects discussed medi-ation use, including pain medication or drinkingrandy by 12 of 16 third molar patients and 7 of 17eople who had fracture repair. Four participants
eported antibiotic use as a coping strategy.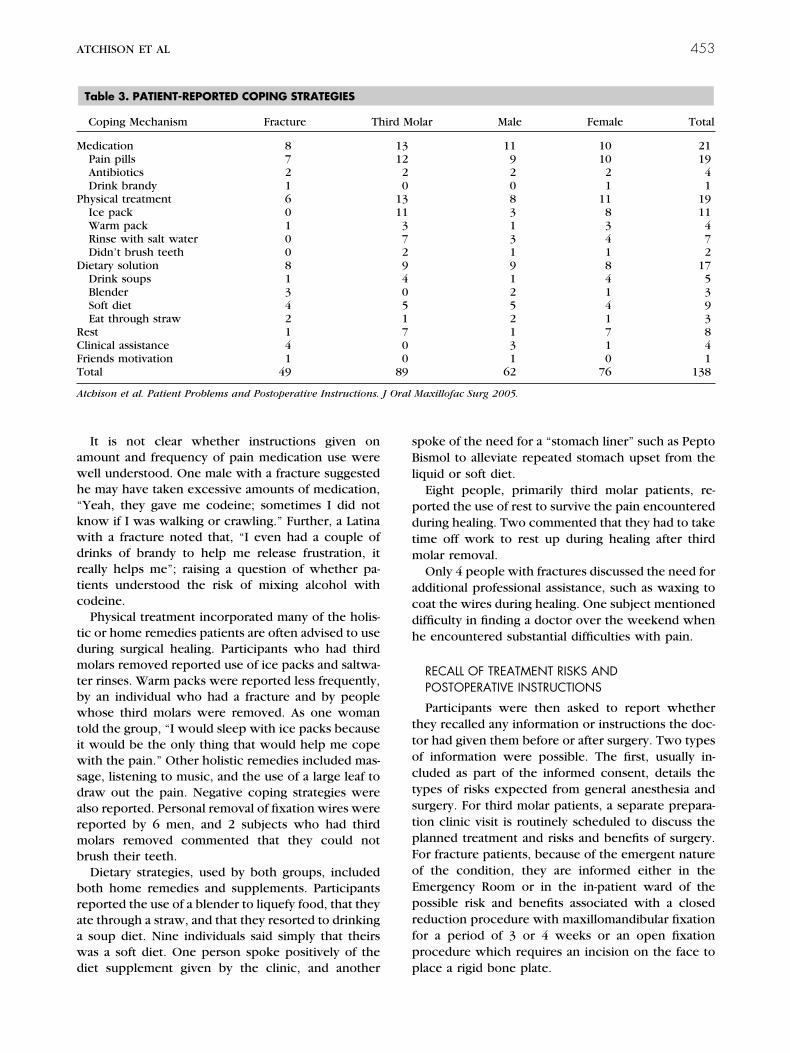
awh“kwdrtc
tdmtbwtiwsdarmb
braawd
sBl
pdtm
acdh
ttoctstpFoEprfp
M
P
D
RCFT
A J Oral
ATCHISON ET AL 453
It is not clear whether instructions given onmount and frequency of pain medication use wereell understood. One male with a fracture suggestede may have taken excessive amounts of medication,Yeah, they gave me codeine; sometimes I did notnow if I was walking or crawling.” Further, a Latinaith a fracture noted that, “I even had a couple ofrinks of brandy to help me release frustration, iteally helps me”; raising a question of whether pa-ients understood the risk of mixing alcohol withodeine.Physical treatment incorporated many of the holis-
ic or home remedies patients are often advised to useuring surgical healing. Participants who had thirdolars removed reported use of ice packs and saltwa-
er rinses. Warm packs were reported less frequently,y an individual who had a fracture and by peoplehose third molars were removed. As one woman
old the group, “I would sleep with ice packs becauset would be the only thing that would help me cope
ith the pain.” Other holistic remedies included mas-age, listening to music, and the use of a large leaf toraw out the pain. Negative coping strategies werelso reported. Personal removal of fixation wires wereeported by 6 men, and 2 subjects who had thirdolars removed commented that they could not
rush their teeth.Dietary strategies, used by both groups, included
oth home remedies and supplements. Participantseported the use of a blender to liquefy food, that theyte through a straw, and that they resorted to drinkingsoup diet. Nine individuals said simply that theirsas a soft diet. One person spoke positively of the
Table 3. PATIENT-REPORTED COPING STRATEGIES
Coping Mechanism Fracture Th
edication 8Pain pills 7Antibiotics 2Drink brandy 1
hysical treatment 6Ice pack 0Warm pack 1Rinse with salt water 0Didn’t brush teeth 0
ietary solution 8Drink soups 1Blender 3Soft diet 4Eat through straw 2
est 1linical assistance 4riends motivation 1otal 49
tchison et al. Patient Problems and Postoperative Instructions.
iet supplement given by the clinic, and another p
poke of the need for a “stomach liner” such as Peptoismol to alleviate repeated stomach upset from the
iquid or soft diet.Eight people, primarily third molar patients, re-
orted the use of rest to survive the pain encountereduring healing. Two commented that they had to takeime off work to rest up during healing after thirdolar removal.Only 4 people with fractures discussed the need for
dditional professional assistance, such as waxing tooat the wires during healing. One subject mentionedifficulty in finding a doctor over the weekend whene encountered substantial difficulties with pain.
RECALL OF TREATMENT RISKS ANDPOSTOPERATIVE INSTRUCTIONS
Participants were then asked to report whetherhey recalled any information or instructions the doc-or had given them before or after surgery. Two typesf information were possible. The first, usually in-luded as part of the informed consent, details theypes of risks expected from general anesthesia andurgery. For third molar patients, a separate prepara-ion clinic visit is routinely scheduled to discuss thelanned treatment and risks and benefits of surgery.or fracture patients, because of the emergent naturef the condition, they are informed either in themergency Room or in the in-patient ward of theossible risk and benefits associated with a closededuction procedure with maxillomandibular fixationor a period of 3 or 4 weeks or an open fixationrocedure which requires an incision on the face to
olar Male Female Total
11 10 219 10 192 2 40 1 18 11 193 8 111 3 43 4 71 1 29 8 171 4 52 1 35 4 92 1 31 7 83 1 41 0 1
62 76 138
Maxillofac Surg 2005.
ird M
1312
20
131137294051700
89
lace a rigid bone plate.

rtmpardnfacrtwjpnpsrmnstmaTht
mpmtfbhh
P
vlppnt“tamthg
rcirt
cswm
D
sscsr
g
P
GT
A J Oral
454 PATIENT PROBLEMS AND POSTOPERATIVE INSTRUCTIONS
A total of 20 people recalled being given treatmentisk information, and 5 participants stated firmly thathey had not been informed. Considering these com-ents were made by people with jaw fractures, theatient may have been not fully aware at the time ofdmission to the hospital. With respect to treatmentisk, people recalled discussion on anesthesia, nerveamage, opening to the nasal passage, pain and sore-ess, and limitations on opening. For some, the in-ormed consent was informative and reassuring anddequately prepared the patient for the experience toome. For example, a male who had third molarsemoved stated, “I remember them telling me somehings about the nasal sinus passage, the nerves thatere close to the bottom teeth. The doctor did a good
ob of telling me pre-surgery about what could hap-en. He told me I could have some tingly and numb-ess, some soreness and some teeth shifting when theressure was moved. Pretty much everything I amaying he told me. I did feel comfortable; he did notush me or anything like that. He took time to showe the x-ray.” On the other hand, 5 subjects recalled
o informed consent process. A man with a fractureaid “when I got here they sent me straight down tohe emergency room and the doctors came. They tolde my jaw was broken and he just got on moving it
nd moving it and I’m like, ‘Hold it man that hurts!’hen they did not explain anything. They said, ‘Giveim a bed.’ They didn’t explain anything until afterhe surgery.”
It was also clear from some statements that com-unication between the health professionals and theatient did not always reflect a well-calibrated assess-ent of risk. For example, one woman remembered
hat the informed consent included the risk of deathrom general anesthesia and the woman and herrother were so scared that the brother made her signer son over to him before he would permit her to
Table 4. SUBJECT RECALL OF POSTOPERATIVE INSTRUC
Patient Recalled Instructions Fracture
ostop instructions 7Allergic to codeine 0Change gauze regularly 0No spitting 0No smoking 0Rinse with salt water 0Go to emergency room 0Diabetic 0No dietician available 2Call dentist 2Given diet plan 2
eneral 5otal 18
tchison et al. Patient Problems and Postoperative Instructions.
ave her wisdom teeth extracted. n
ostoperative Instructions
It is routine at King/Drew Medical Center to pro-ide postoperative instructions to all patients beforeeaving the clinic or hospital. However, all partici-ants did not recall having received comprehensiveostoperative instructions. Nine participants defi-itely recalled being given verbal instructions. A pa-ient with maxillomandibular fixation commented,They gave me some Boost and stuff like that and theyold me that I had to be on a liquid diet. A lot of juicesnd things like that. I am not going to be able to eateat and stuff like that. They told me, ‘Don’t try to
ake the wires off yourself. Just deal with it!’ But I wasardheaded and tried to take them out, ’cause it wasetting on my nerves!”Overall, 14 participants recalled elements that rep-
esent postoperative instructions. The instructions in-luded changing gauze regularly, not spitting or smok-ng, when to call the doctor or go to the emergencyoom, and medical management instruction for a pa-ient who was a diabetic (Table 4).
Six participants stated that they received insuffi-ient information. For example, a male with a fracturetated, “I was given nothing. No paperwork thatould say how I was supposed to eat, all they gavee was Boost.”
iscussion
This study represents a qualitative study to under-tand, from a disadvantaged minority patient’s per-pective, how the process of surgery took place at aounty hospital. Clearly, given gaps in patient under-tanding of postoperative care, there is substantialoom for improvement in postoperative instructions.
Why did we select third molars as a comparisonroup for a study of patient preferences for surgery or
Molar Male Female Total
7 9 5 141 0 1 11 0 1 11 0 1 11 0 1 11 0 1 11 0 1 11 0 1 10 1 1 22 1 3 40 2 0 20 3 2 56 16 18 34
Maxillofac Surg 2005.
TIONS
Third
1
on-surgery for orofacial injury? We did so because

wupTpcpeetlmahsmomemdadi
WmlusDp2$affeAmSctElnptbppicnAt
obttmJpccerlwtm
oflrtsrciatitppiwpupgpttmippst
dwprltr
ATCHISON ET AL 455
e realized that there would be common aspects: these of general anesthesia and its related problems,ain, and the expected interruption to eating abilities.hese aspects were confirmed in the similarity of theatients’ descriptions of the physical problems en-ountered. The psychosocial impacts that patient ex-erience associated with treatment for a traumaticvent such as a fractured jaw emphasized the differ-nces between the elective third molar patient andhe non-elective fracture patient. It offered an excel-ent comparison of subjects with respect to decision-
aking. Third molar patients have time and choice,spects that non-elective patients do not have. Theyave the choice to decide whether or not to haveurgery after hearing about the possible risks of treat-ent. They have time to weigh the risks and benefits
f surgery, a perfect model for informed decision-aking. The communication misunderstandings, as
xemplified by the woman who reported her brotherade her sign her son to him in case of her death
uring third molar removal, showed that even withmple time to listen and the support of a close relativeuring the informed consent process, communication
s not assured.This analysis began with the recruitment process.e analyzed the characteristics of the subjects forultiple reasons. First, it is well documented in the
iterature that it is difficult to recruit minority individ-als to participate in research studies.12,13 All of theubjects were minority individuals, as befits Kingrew Medical Center’s catchment area. The high pro-ortion of people who did not elect to come to a-hour time commitment, despite a free lunch and a25 honorarium, confirms those difficulties. Further,ll people who agreed to participate were confirmedor the time and place of the meeting, and taxi or busare was offered to any who needed it. Despite thesefforts, it was difficult to successfully recruit patients.ll subjects were recruited by a bilingual Latina staffember in the Department of Oral and Maxillofacial
urgery. She was a familiar figure, not a hospital orounty administrator, and not a doctor, suggestinghat she was not apt to intimidate former patients.ven so, neither Latinos nor females appeared more
ikely to respond to her request to participate. Indeed,o African American females with fractures agreed toarticipate. In general, it appears that men with frac-ures are more willing to participate than females,ecause 2 of the 10 females with fractures ultimatelyarticipated. Because of possible worries about re-orting of domestic violence, future research involv-
ng females with orofacial injuries might be betteronducted away from the medical center at a safe,on-threatening location to encourage participation.dditionally, vulnerable women might respond better
o women of their own culture. a
We also worried that only subjects who had goodr successful experiences with their surgery woulde willing to return to tell us about their encoun-ers. This was certainly not the case. A review ofhe literature shows overall complication rates forandibular fractures ranging from 6% to 32%.14
udging from the high number of people who re-orted complications such as nerve damage,rooked jaws, broken wires, or insufficient painontrol, either sampling variability or a selectionffect may be the source of the higher complicationates in this sample than have been reported in theiterature. Indeed, with the inclusion of patients
hose fracture resulted from gunshot injury ratherhan a fall or motor vehicle accident, this sampleay represent a higher proportion of serious cases.Nonetheless, very interesting information came
ut of the focus group interviews for which theollowing clinical insights are presented. The prob-ems reported by these individuals confirm thoseeported by Conrad et al15 of third molar patientshat 63.5% of patients reported their worst pain asevere (score 5 to 7, 7 being severe). Patients alsoeported substantial interference in oral function;hewing, 85%; mouth opening, 78.5%; and speak-ng, 37.5%. Increasingly high amounts of surgeryre now performed in the ambulatory setting, yethe delivery of postoperative instructions remains,n some respects, an afterthought in the total pa-ient care process. Judging from the consistent re-orts of pain and insufficient pain control, it ap-ears that patients may need better postoperative
nstruction regarding ways to appropriately dealith pain following oral surgery. The design ofostoperative instructions for minority patient pop-lations should include a clear link between theatient’s immediate concerns and the clinician’soals for a successful recovery process. For exam-le, if pain reduction is the most salient problem tohe patient at time of discharge when a postopera-ive instruction form is presented, the clinicianust make it clear how following the postoperative
nstructions will, in fact, aid in the reduction ofain. The notion that good hygiene or eating a highrotein diet is ultimately linked to decreases ineverity or duration of pain may not be self evidento a patient with low health literacy.
Inadequate pain relief can prolong recovery andecrease patient satisfaction. Some of the problemsith inadequate pharmacologic pain management re-orts dealt directly with county mandated formularyestrictions at King Drew Medical Center. Other prob-ems associated with pain management, and many ofhem associated with other problems, such as wireemoval, certainly related to the patient’s memory
nd understanding of the postoperative instructions,
wgaibiastriavdoa
aomrhcsssmwcpsaea
R
1
1
1
1
1
1
456 PATIENT PROBLEMS AND POSTOPERATIVE INSTRUCTIONS
hich may have been impaired by after effects ofeneral anesthesia. One way to insure that postoper-tive instructions get used in the way they werentended is to provide a copy to a caregiver who maye available upon discharge. Then, not only are verbal
nstructions shared, but the written instructions arevailable when the patient is home and in a bettertate to review them. Another method of evaluatinghe influence that postoperative instructions have onecovery is to have the patient bring with them thenstructions and any left over medications such asntibiotics or pain medication to their follow-up clinicisit. This provides the clinician with tangible evi-ence that instructions were provided as well as anpportunity to go over each instruction and addressny questions or concerns.
Third molar patients reported a fair knowledge ofppropriate coping strategies, including use of antibi-tics, ice packs, over the counter and prescribed painedication, not smoking, use of soft diet, salt water
inses, return visits to the clinic, sleeping, and oralygiene. Problem responses were also reported, in-luding self-removal of sutures. Fracture patients de-cribed fewer instructions and coping strategies: mas-age, use of antibiotics and pain medication, use of aoft diet, use of wire wax, sleeping, and discourage-ent from self-removal of maxillomandibular fixationires. It was apparent that not all instructions were
lear, were remembered, or were sufficient to resolveatient’s problems. We conclude that additional re-earch on diverse populations with low health liter-cy is needed to design and test high quality postop-rative instructions necessary for surgical treatment
nd recovery.eferences1. Powers RD: Emergency department patient literacy and the
readability of patient-directed materials. Ann Emerg Med 17:124, 1988
2. Jackson RH, Davis TC, Bairnsfather LE, et al: Patient readingability: An overlooked problem in health care. South Med J84:1172, 1991
3. Alexander RE: Patient understanding of postsurgical instructionforms. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 87:153, 1999
4. Culbertson VL, Arthur TG, Rhodes PJ, et al: Consumer prefer-ences for verbal and written medication information. DrugIntel Clin Pharm 22:390, 1988
5. Malins AF: Do they do as they are instructed? A review ofout-patient anesthesia. Anaesthesia 33:832, 1978
6. Blinder D, Rotenberg L, Peleg M, et al: Patient compliance toinstructions after oral surgical procedures. Int J Oral MaxillofacSurg 30:216, 2001
7. Schouten BC, Eijkman MA, Hoogstraten J: Dentists’ and pa-tients’ communicative behaviour and their satisfaction with thedental encounter. Community Dent Health 20:11, 2003
8. Devine EC, Cook TD: Clinical and cost-saving effects of psy-choeducational interventions with surgical patients: A meta-analysis. Res Nurs Health 9:89, 1986
9. Alexander RE: Readability of published dental educational ma-terials. J Am Dent Assoc 131:937, 2000
0. Miles MB, Huberman AM: Qualitative Data Analysis: An Ex-panded Sourcebook. Thousand Oaks, CA, Sage Publications,1994
1. Atchison KA: Understanding and utilizing qualitative research.J Dent Educ 60:716, 1996
2. Corbie-Smith G, Thomas SB, Williams MV, et al: Attitudes andbeliefs of African Americans toward participation in medicalresearch. J Gen Intern Med 14:537, 1999
3. Shavers VL, Lynch CF, Burmeister LF: Factors that influenceAfrican-Americans’ willingness to participate in medical re-search studies. Cancer 91:233, 2001 (suppl 1)
4. Ellis E III: Treatment of mandibular angle fractures using twononcompression miniplates. J Oral Maxillofac Surg 52:1032,1994
5. Conrad SM, Blakey GH, Shugars DA, et al: Patients’ perceptionof recovery after third molar surgery. J Oral Maxillofac Surg
57:1288, 1999




























