Embed Size (px)
Citation preview

ARTICLE IN PRESS
Ann Anat 191 (2009) 280—287
0940-9602/$ - sdoi:10.1016/j.
�CorrespondE-mail addr
(M. Laskarin).
www.elsevier.de/aanat
RESEARCH ARTICLE
A quantitative analysis of splint therapy ofdisplaced temporomandibular joint disc
Tomislav Badela,�, Miljenko Marottib, Josipa Kernc, Mirko Laskarind
aDepartment of Prosthodontics, School of Dental Medicine, University of Zagreb, Gunduliceva 5,HR-10000 Zagreb, CroatiabDepartment of Diagnostic and Interventional Radiology, Clinical Hospital ‘‘Sestre milosrdnice’’,University of Zagreb, Vinogradska cesta 29, HR-10000 Zagreb, CroatiacDepartment of Medical Statistics, Epidemiology and Medical Informatics, School of Public Health ‘‘Andrija Stampar’’,School of Medicine, University of Zagreb, Rockefellerova 4, HR-10000 Zagreb, CroatiadHealth Center Sibenik, Stjepana Radica 83, HR-22000 Sibenik, Croatia
Received 5 September 2008; received in revised form 6 December 2008; accepted 16 December 2008
KEYWORDSTemporomandibulardisorder;Temporomandibularjoint;Disc displacement;Magnetic resonanceimaging;Michigan splint
ee front matter & 2009aanat.2008.12.004
ing author. Tel.: +385 14esses: [email protected] (T
SummaryObjectives: The effects of the Michigan splint on the change in disc displacement(DD) as well as the position of the condyles were determined by metrical analysisusing magnetic resonance imaging (MRI).Methods: Twenty-five patients with clinical DD symptoms were treated by means ofthe Michigan splint, and an assessment of the effects of the splint was conducted orverified by MRI before and during the period of therapy, 5 months follow-up. Thepositions of the condyles and the disc were calculated from the MRI in theparasagittal plane.Results: There were no changes in the positions of the disc and condyles in thephysiological joints of the patients (n ¼ 23) prior to and during the time the splintwas in place (p40.05). The splint achieved a DD decrease (po0.05), and pain waseliminated in 69.2% of the DD joints with reduction (n ¼ 13). As far as the DD jointswithout reduction (n ¼ 13) are concerned, pain was eliminated in 74.9% of thejoints, that is, without any change in the positions of the disc and condyles(p40.05).Conclusions: The evaluation of the Michigan splint therapy showed that it has noinfluence in the repositioning of the DD joints without reduction, but the DD jointswith reduction have a limited positive effect. In both forms of these displacements,conditions for the elimination of the clinical symptoms are created.& 2009 Elsevier GmbH. All rights reserved.
Elsevier GmbH. All rights reserved.
8 021 25.. Badel), [email protected] (M. Marotti), [email protected] (J. Kern), [email protected]

ARTICLE IN PRESS
Figure 1. MRI of the physiological disc positions with themouth closed (left) and open (right).
Figure 2. MRI of DD with reduction with the mouthclosed (left) and open (right).
Analysis of displaced TMJ disc 281
Introduction
The term temporomandibular disorder (TMD)designates a cluster of descriptive diagnoses ofthe temporomandibular joint (TMJ) and/or masti-catory muscle disorders of the musculoskeletaldisorders group. As far as the diagnosticallyimportant clinical signs and symptoms of TMDs areconcerned, the most uncomfortable for the patientis temporomandibular pain, followed by limitationof mandibular movement (Turp et al., 2006; Palla,2003; Dworkin and LeResche, 1992).
The anterior disc displacement (DD) is the mostfrequent form of disc malpositioning of TMJ. DD canonly occur in the intercuspal occlusional position(DD with reduction) or during condylar movementswhen opening the mouth (DD without reduction).Magnetic resonance imaging (MRI) is a noninvasivediagnostic method for the analysis of arthrogenicTMDs that enables a qualitative as well as aquantitative analysis of the structures within thejoint, as well as the soft tissues, especially those ofthe disc (Hugger, 2002; Larheim, 2005).
Occlusal splint therapy is the most frequent formof initial TMD treatment, despite the fact that all ofthe effects of the different types of splints on thetreatment of TMD symptoms are controversial (Daoand Lavigne, 1998; Dylina, 2001; Clark and Minaku-chi, 2006). The most frequently used permissivesplint in TMD and bruxism therapy is the Michigansplint (Ash Jr. and Ramfjord, 1998; Ekberg et al.,1998; Baldissara et al., 1998; Ekberg and Nilner,1999, 2002; Jokstad et al., 2005; Fayed et al., 2004;Babadag et al., 2004; Ohnuki et al., 2006). Of thenonpermissive types, the anterior repositioning splintis also much in use. It is exclusively indicated for DDconditions, with the goal of achieving physiologicalrelationships between the disc and the condyles bypositioning the mandible into the therapeutic ante-rior position (Kurita et al., 1998a, 1998b; Dylina,2001; Eberhard et al., 2002).
The purpose of this study is to determine theeffects of Michigan splint therapy on change in discposition as well as the position of the condylesthrough use of metrical analysis in MRI-confirmedclinical diagnosis of DD. The hypothesis was thatduring initial Michigan splint therapy there were nodifferences between the position of an anterior DDand the position of the condyles.
Materials and methods
Subjects
The subjects of this study, 25 patients, agedbetween 18 and 71 years (mean: 38 years; 1:5 ratio
men to women), were selected from the totalnumber of 40 patients with DD (between 15 and 82years of age, mean 37; 23.3% men and 76.7%women) seeking treatment for TMD at the Depart-ment of Prosthodontics at the School of DentalMedicine in Zagreb in the period from 2001 to 2004.The selected patients included in this studyvoluntarily agreed to an additional MRI assessmentwhen the splint was applied (Figures 1 and 2).
The clinical parameters were pain and/or click-ing in the TMJ region, and limited mouth opening.The DD diagnoses were set based on MRI-confirmedclinical diagnostics. All patients were informed ofthe type and purpose of diagnostic procedures andgave their written consent for participation, andthe execution of the study was approved by theEthics Committee of the School of Dental Medicinein Zagreb.
Clinical method
The patients were diagnosed with a DD with orwithout reduction in congruence with the Researchdiagnostic criteria (RDC)/temporomandibular dis-orders diagnostics system (Axis I) (Dworkin and

ARTICLE IN PRESS
T. Badel et al.282
LeResche, 1992). In the clinical examinationBumann and Groot Landeweer’s techniques ofmanual functional analysis were also used (Bumannand Lotzmann, 2002). The Michigan splint therapywas indicated for these patients, which was thenperformed. In this study, the Michigan splint wasmade as an occlusal bite plane stabilization splintwith cuspid rise and freedom in centric in anarticulator SAM 2P (Prazisiontechnik, Gauting beiMunchen, Germany). A face bow was used (SAMAxioquick, Prazisiontechnik, Gauting bei Munchen,Germany) and all splints were fabricated by onedental technician (Witt, 1998).
Patients were instructed to wear the splintduring the night. During the period of wearing thesplint the patients were regularly checked so that itcould be seen that the splint was successfullyaccepted and the subjective and objective condi-tions of the patient were improving. The effects ofthe splint treatment on the positions of the disc andthe condyles were checked in addition to clinicalcondition, also by TMJ analysis during the initialtreatment, by repeating the MRI with the splintapplied. Because all patients had an arthrogenicdisorder, it was expected that a relatively longperiod of splint wearing to improve functional oralstatus would be necessary. In this study, a 5-monthinterval for MR evaluation was chosen, because 6months of treatment were considered an optimalperiod for evaluation, and, if necessary, thetreatment modality could have been changed(Conti et al., 2006; Ottl, 1997). The clinical stateof the patient’s individual joints was monitored sothat the subjective result of the splint therapy wasevaluated as: a state without discomfort, a statewithout pain, but with clicking present, a state ofreduced pain, and a state of still significant pain.
MRI protocol
The bilateral MRI of TMJs was performed using asuper-conductive device, the ‘‘Harmony’’ magnetby Siemens AG (Erlangen, Germany), magnetic fieldstrength of 1 T. Gradient magnets of 20mT/ms withquick system reboot time and radio frequentsystem for the head coil. The coil includeddigitalized transmitters and antennae with fre-quency signals of 42MHz; the resultant resolutionwas 100 ns.
The angle of the parasagittal imaging is indivi-dually determined by the angle shown on theindividual angulated layers of the axial and coronalslice. TMJs of the patients were scanned inintercuspal occlusion with their mouths closed.The open mouth position was fixated with an
interincisal individual fixator (Optosils P plus,Heraeus Kulzer, Hanau, Germany). The layers inthe position of an open or closed mouth could becompared well. In all, seven slices of 3mm thickwere scanned, with a 256� 192 matrix, and field ofview of 160� 160. Scanning sequences included aT1 weighted image with a repetition time of450ms, and an echo time of 12ms.
Metric evaluation
The patient’s joint with asymptomatic DD with-out reduction was excluded. The rest of thepatients’ joints were distributed according to thedisc position. Only one patient had a bilateral DD,with reduction in one joint and no reduction inthe other. The disc’s physiological position in theparasagittal plane was defined according tothe placement of its intermedial zone betweenthe articular eminence and the shortest distance ofthe bone contours of the condyles’ ventrocranialpart. The pars posterior of the disc was located onthe condylar head (Orsini et al., 1998; Bumann andLotzmann, 2002).
The quantitative analysis of the position andrelationship between the disc and the condyles wasdescribed using Kurita et al.’s method of measuringthe relative and absolute distances of referencepoints (Kurita et al., 1998b). A tangent was drawnbetween the lowest part of the articular eminence(T) and the highest edge of the external auditorycanal (P). A line was drawn perpendicular to thetangent, touching the back edge of the disc, andtheir intersection was marked as point D. Anotherperpendicular, touching the back edge of thecondyle was also drawn, and point C marked theintersection of this line and the tangent. Thedistances between points T and P were taken asmeasurement reference values and individual dis-tances on the tangent-distances between points Tand C, and points T and D (Figure 3) were alsomeasured. Absolute values (TP, TC and TD) weremeasured in millimeters to one decimal place usingAdobes Photoshops 7.0. Millimeter values werecalculated based on the measurement scale shownin the MRI. The disc and condyle positions werecalculated as TC/TP and TD/TP and expressed inone-hundredths of the distance between points Tand P. A lower value indicates a more anteriorcondyle, or disc position.
Statistical analysis
The statistical analysis was performed by usingSTATISTICA and SAS programs. The measured values

ARTICLE IN PRESS
Figure 3. The disc and condyles position measuring inthe parasagittal plane using Kurita et al.’s (1998b)method. The TP, TC and TD distances are measured inmillimeters.
Table 1. Measurement of the method error (ME) byDahlberg, and the average difference of two measure-ments.
Variable (in mm) ME Mean SD min. max.
Distance T–P 0.100 0.108 0.093 0 0.3Distance T–C 0.076 0.100 0.042 0 0.2Distance T–D 0.095 0.096 0.095 0 0.3
SD – standard deviation, min. – minimum, max. – maximum.
Analysis of displaced TMJ disc 283
of the metric evaluation are displayed as box-and-whisker plots. The box with the marked medianencompassed the values between the 25%- to the75%-quantile, and all the measured values wereshown in the limits of the whisker, except theoutliers (therefore, all the values are in the non-outlier range).
The left and the right TMJs of each person werepresented as two separate entities within the dataanalysis. The properties of joints with DD (DD withreduction and DD without reduction) were observedseparately. A control group consisted of joints ofthe same patients without clinical signs andsymptoms of TMD. In this case, the physiologicalposition of the disc is confirmed by MRI. TheWilcoxon pair test was used to compare databefore the insertion of the Michigan splint andafter it was applied. The significant difference forstatistical testing was 5% and 1%.
The reliability of MRI assessment was evaluatedon the basis of two researchers’ (a radiologist’s anda dentist’s) inspection, which was conductedindependently of the patient’s clinical signs onMRI images prior to the insertion of the Michigansplint. The Kappa index of reliability was between0.8 and 1.0 for all variables. The MRI assessmentwas judged to be extremely reliable.
The reliability of results for the metrical vari-ables was tested by calculating the error accordingto Dahlberg (Houston, 1983). When no measure-ment error exists then the Dahlberg error equals 0.To calculate the method error (ME) according toDahlberg, the following formula was used:
ME ¼ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiðP
d2Þ=2n
q, where d is the difference
between two measurements, and n is the numberof measured MRI images.
For the purpose of determining the reliability ofthe measurements, a metrical analysis was con-ducted on 12 patients twice on the same MRIs ofboth joints (24 measurements in all). The compar-ison results for the two measurements of metricalvariables are shown in Table 1. There is a greatpossibility of reproduction of the metrical analysisreference points.
Results
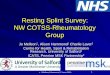
The physiological position of the disc was estab-lished in 23 patients’ joints. The quantitativerelationship of the patients’ joints was comparedwith the physiological disc position during theperiod when the occlusal splint was worn. Therewas no statistically significant change in the relativedisc position (Wilcoxon’s pair test z ¼ 0.821 withp ¼ 0.412; Figure 4A), or to the relative condyleposition (Wilcoxon’s pair test z ¼ 0.568 withp ¼ 0.570; Figure 4B) before the insertion of theMichigan splint and after it was applied.
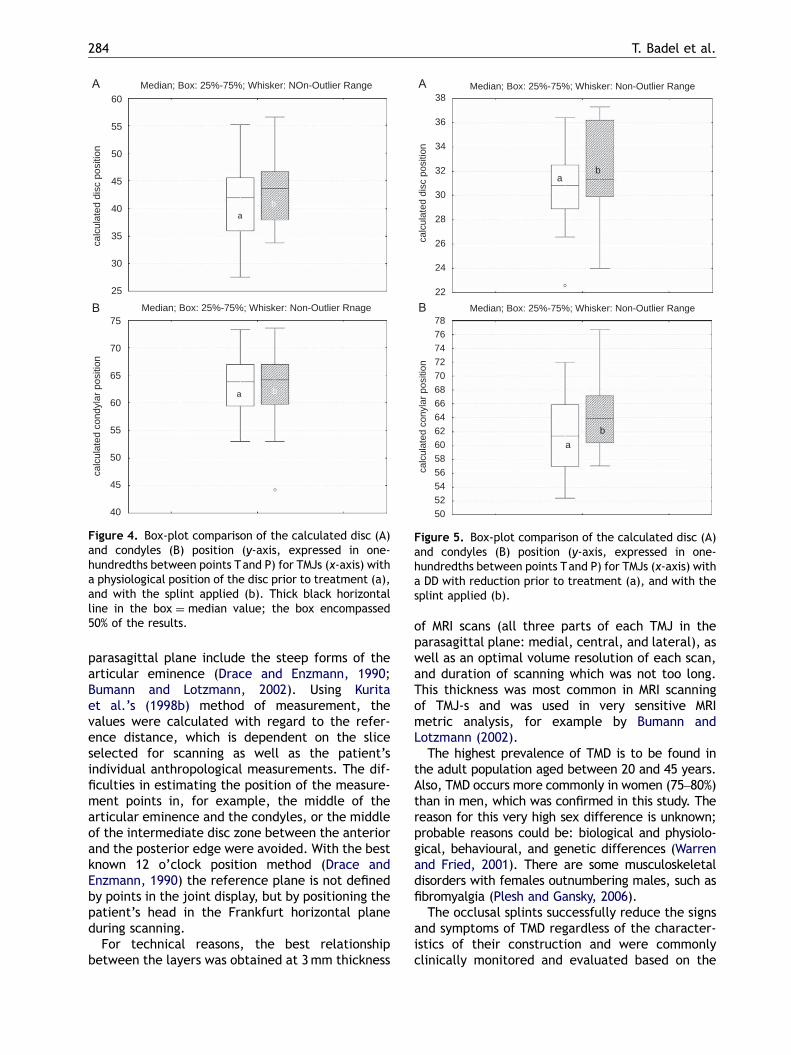
In 13 joints a DD with reduction was noted. Themetrical analysis showed a statistically significantdecrease in anterior DD during splint therapy whenthe relative disc position in the mouth (Wilcoxon’spair test z ¼ 2.795 with po0.005) was comparedwith the dorsal relative condyle positioning (Wil-coxon’s pair test z ¼ 2.510 with p ¼ 0.012) beforeand after splint application (Figure 5).
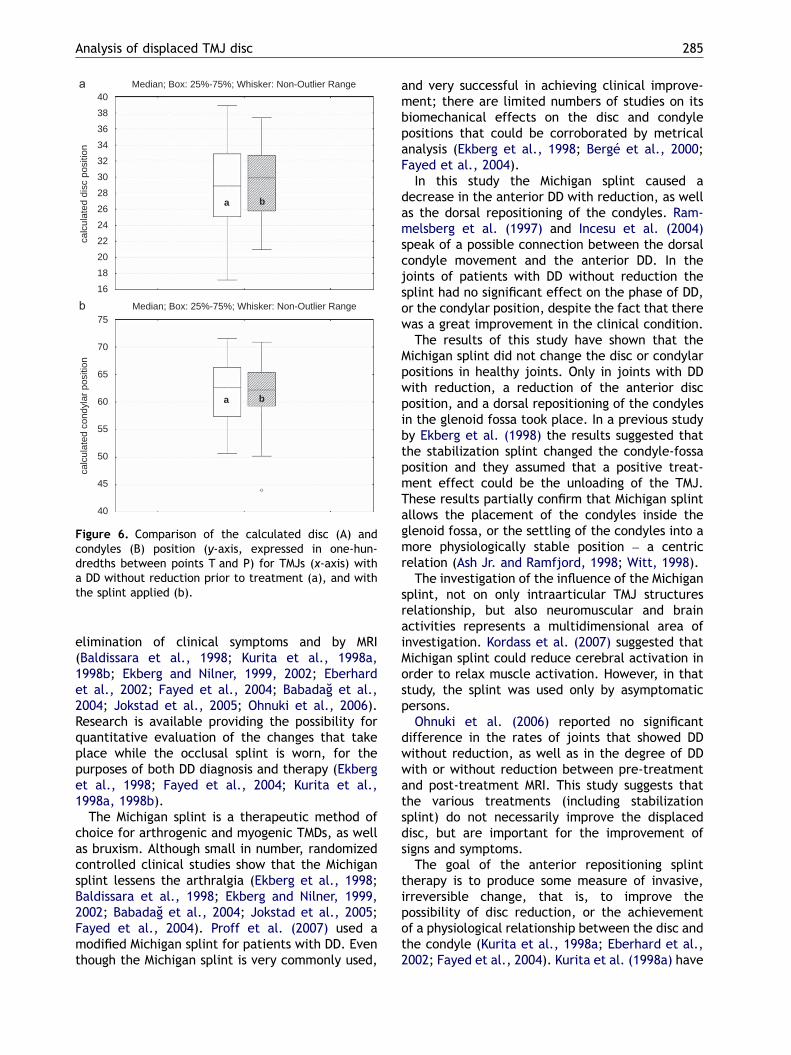
The DD without reduction was diagnosed in 13joints. Based on the Wilcoxon pair test, there wasno decrease in the anterior DD during splinttherapy, when the relative disc position(z ¼ 0.489) at p ¼ 0.625 and the relative positionof condyles (z ¼ 0.384) at p ¼ 0.701 were com-pared before and after splint application (Figure 6).
Discussion
In this study the criteria applied for determiningthe physiological position of the disc in the
ARTICLE IN PRESS
Median; Box: 25%-75%; Whisker: NOn-Outlier Range60
55
50
45
40
35
30
25
calc
ulat
ed d
isc
posi
tion
Median; Box: 25%-75%; Whisker: Non-Outlier Rnage75
70
65
60
55
50
45
40
calc
ulat
ed c
ondy
lar p
ositi
on
ab
a b
Figure 4. Box-plot comparison of the calculated disc (A)and condyles (B) position (y-axis, expressed in one-hundredths between points Tand P) for TMJs (x-axis) witha physiological position of the disc prior to treatment (a),and with the splint applied (b). Thick black horizontalline in the box ¼ median value; the box encompassed50% of the results.
Median; Box: 25%-75%; Whisker: Non-Outlier Range
Median; Box: 25%-75%; Whisker: Non-Outlier Range
ab
ab
38
36
34
32
30
28
26
24
22
calc
ulat
ed d
isc
posi
tion
787674727068666462605856545250
calc
ulat
ed c
onyl
ar p
ositi
on
Figure 5. Box-plot comparison of the calculated disc (A)and condyles (B) position (y-axis, expressed in one-hundredths between points Tand P) for TMJs (x-axis) witha DD with reduction prior to treatment (a), and with thesplint applied (b).
T. Badel et al.284
parasagittal plane include the steep forms of thearticular eminence (Drace and Enzmann, 1990;Bumann and Lotzmann, 2002). Using Kuritaet al.’s (1998b) method of measurement, thevalues were calculated with regard to the refer-ence distance, which is dependent on the sliceselected for scanning as well as the patient’sindividual anthropological measurements. The dif-ficulties in estimating the position of the measure-ment points in, for example, the middle of thearticular eminence and the condyles, or the middleof the intermediate disc zone between the anteriorand the posterior edge were avoided. With the bestknown 12 o’clock position method (Drace andEnzmann, 1990) the reference plane is not definedby points in the joint display, but by positioning thepatient’s head in the Frankfurt horizontal planeduring scanning.
For technical reasons, the best relationshipbetween the layers was obtained at 3mm thickness
of MRI scans (all three parts of each TMJ in theparasagittal plane: medial, central, and lateral), aswell as an optimal volume resolution of each scan,and duration of scanning which was not too long.This thickness was most common in MRI scanningof TMJ-s and was used in very sensitive MRImetric analysis, for example by Bumann andLotzmann (2002).
The highest prevalence of TMD is to be found inthe adult population aged between 20 and 45 years.Also, TMD occurs more commonly in women (75–80%)than in men, which was confirmed in this study. Thereason for this very high sex difference is unknown;probable reasons could be: biological and physiolo-gical, behavioural, and genetic differences (Warrenand Fried, 2001). There are some musculoskeletaldisorders with females outnumbering males, such asfibromyalgia (Plesh and Gansky, 2006).
The occlusal splints successfully reduce the signsand symptoms of TMD regardless of the character-istics of their construction and were commonlyclinically monitored and evaluated based on the
ARTICLE IN PRESS
Median; Box: 25%-75%; Whisker: Non-Outlier Range
Median; Box: 25%-75%; Whisker: Non-Outlier Range
40
38
36
34
32
30
28
26
24
22
20
18
16
calc
ulat
ed d
isc
posi
tion
75
70
65
60
55
50
45
40
calc
ulat
ed c
ondy
lar p
ositi
on
a b
a b
Figure 6. Comparison of the calculated disc (A) andcondyles (B) position (y-axis, expressed in one-hun-dredths between points T and P) for TMJs (x-axis) witha DD without reduction prior to treatment (a), and withthe splint applied (b).
Analysis of displaced TMJ disc 285
elimination of clinical symptoms and by MRI(Baldissara et al., 1998; Kurita et al., 1998a,1998b; Ekberg and Nilner, 1999, 2002; Eberhardet al., 2002; Fayed et al., 2004; Babadag et al.,2004; Jokstad et al., 2005; Ohnuki et al., 2006).Research is available providing the possibility forquantitative evaluation of the changes that takeplace while the occlusal splint is worn, for thepurposes of both DD diagnosis and therapy (Ekberget al., 1998; Fayed et al., 2004; Kurita et al.,1998a, 1998b).
The Michigan splint is a therapeutic method ofchoice for arthrogenic and myogenic TMDs, as wellas bruxism. Although small in number, randomizedcontrolled clinical studies show that the Michigansplint lessens the arthralgia (Ekberg et al., 1998;Baldissara et al., 1998; Ekberg and Nilner, 1999,2002; Babadag et al., 2004; Jokstad et al., 2005;Fayed et al., 2004). Proff et al. (2007) used amodified Michigan splint for patients with DD. Eventhough the Michigan splint is very commonly used,
and very successful in achieving clinical improve-ment; there are limited numbers of studies on itsbiomechanical effects on the disc and condylepositions that could be corroborated by metricalanalysis (Ekberg et al., 1998; Berge et al., 2000;Fayed et al., 2004).
In this study the Michigan splint caused adecrease in the anterior DD with reduction, as wellas the dorsal repositioning of the condyles. Ram-melsberg et al. (1997) and Incesu et al. (2004)speak of a possible connection between the dorsalcondyle movement and the anterior DD. In thejoints of patients with DD without reduction thesplint had no significant effect on the phase of DD,or the condylar position, despite the fact that therewas a great improvement in the clinical condition.
The results of this study have shown that theMichigan splint did not change the disc or condylarpositions in healthy joints. Only in joints with DDwith reduction, a reduction of the anterior discposition, and a dorsal repositioning of the condylesin the glenoid fossa took place. In a previous studyby Ekberg et al. (1998) the results suggested thatthe stabilization splint changed the condyle-fossaposition and they assumed that a positive treat-ment effect could be the unloading of the TMJ.These results partially confirm that Michigan splintallows the placement of the condyles inside theglenoid fossa, or the settling of the condyles into amore physiologically stable position – a centricrelation (Ash Jr. and Ramfjord, 1998; Witt, 1998).
The investigation of the influence of the Michigansplint, not on only intraarticular TMJ structuresrelationship, but also neuromuscular and brainactivities represents a multidimensional area ofinvestigation. Kordass et al. (2007) suggested thatMichigan splint could reduce cerebral activation inorder to relax muscle activation. However, in thatstudy, the splint was used only by asymptomaticpersons.
Ohnuki et al. (2006) reported no significantdifference in the rates of joints that showed DDwithout reduction, as well as in the degree of DDwith or without reduction between pre-treatmentand post-treatment MRI. This study suggests thatthe various treatments (including stabilizationsplint) do not necessarily improve the displaceddisc, but are important for the improvement ofsigns and symptoms.
The goal of the anterior repositioning splinttherapy is to produce some measure of invasive,irreversible change, that is, to improve thepossibility of disc reduction, or the achievementof a physiological relationship between the disc andthe condyle (Kurita et al., 1998a; Eberhard et al.,2002; Fayed et al., 2004). Kurita et al. (1998a) have
ARTICLE IN PRESS
T. Badel et al.286
by an identical metric method showed a successfulrepositioning of the disc to the physiologicalposition to the condyle. The metrical analysis withMRI on the basis of the small sample size by Fayedet al. (2004) showed that disc recapture was betterby stabilization splint than anterior repositioningsplint, but appliances were effective in eliminatingpain and clicking.
It is important to emphasize the differences inthe biomechanical effects of these two types ofsplint therapy, because joint analyses of asympto-matic subjects re-evaluate the clinical importanceof the position or displacement of the disc in TMDpatients. Because of the significant prevalence(20–33%) of asymptomatic DD, the anterior ana-tomic disc position cannot be said to be anexclusive cause of TMJ pain (Haiter-Neto et al.,2002; Larheim et al., 2001).
Conclusions
This study shows, regardless of its limits, that theMichigan splint has no effect on the changing of thedisc or condylar positions in healthy joints. Jointswith DD without reduction also have a smallerpossibility of reduction, and the splint was aneffective therapeutic means, even though nochanges occurred in that group of joints either. Injoints with DD with reduction, a reduction of theanterior DD, and a dorsal repositioning of thecondyles in the glenoid fossa took place.
Acknowledgements
This study was performed with the support of theCroatian Ministry of Science, Education and Sports,numbers 065-0650448-0438 and 134-1080232-1494.
References
Ash Jr., B.M., Ramfjord, S.P., 1998. Reflections on theMichigan splint and other intraocclusal devices.J. Mich. Dent. Assoc. 80, 32–46.
Baldissara, S., Mascellani, S.C., Catapano, S., Baldissara,P., 1998. Efffetti a breve termine della placca diMichigan sul dolore muscolare ed articolare. MinervaStomatol. 47, 235–238.
Babadag, M., S-ahin, M., Gorgun, S., 2004. Pre- and post-treatment analysis of clinical symptoms of patientswith temporomandibular disorders. Quintessence Int.35, 811–814.
Berge, S., Conrad, R., von Lindern, J.-J., Niederhagen,B., Appel, T., Reich, R.H., 2000. Funktionelle
MR-Aufnahmen des Kiefergelenkes. Vergleich mitund ohne Aufbissbehelfe. Dtsch. Zahnarztl. Z. 55,285–287.
Bumann, A., Lotzmann, U., 2002. TMJ Disorders andOrofacial Pain – The Role of Dentistry in a Multi-disciplinary Diagnostic Approach. Thieme, Stuttgart,New York.
Clark, G.T., Minakuchi, H., 2006. Oral appliances. In:Laskin, D.M., Green, C.S., Hylander, W.L. (Eds.),Temporomandibular Disorders. An Evidence-BasedApproach to Diagnosis and Treatment. Quintessence,Chicago, pp. 377–390.
Conti, P.C., dos Santos, C.N., Kogawa, E.M., de CastroFerreira Conti, A.C., de Araujo, C., dos, R., 2006. Thetreatment of painful temporomandibular joint clickingwith oral splints: a randomized clinical trial. J. Am.Dent. Assoc. 137, 1108–1114.
Dao, T.T.T., Lavigne, G.J., 1998. Oral splints: thecrutches for temporomandibular disorders and brux-ism? Crit. Rev. Oral Biol. Med. 9, 345–361.
Drace, J.E., Enzmann, D.R., 1990. Defining the normaltemporomandibular joint: closed-, partially open-,and open-mouth MR imaging of asymptomatic sub-jects. Radiology 177, 67–71.
Dylina, T.J., 2001. A common-sense approach to splinttherapy. J. Prosthet. Dent. 86, 539–645.
Dworkin, S.F., LeResche, L. (Eds.), 1992. Researchdiagnostic criteria for temporomandibular disorders:review, criteria, examinations and specifications,critique. J. Craniomandibular Disord. Fac. Pain 6,301–355.
Eberhard, D., Bantleon, H.-P., Steiger, W., 2002. Theefficacy of anterior repositioning splint therapystudied by magnetic resonance imaging. Eur. J.Orthodont. 24, 343–352.
Ekberg, E., Sabet, M.E., Petersson, A., Nilner, M., 1998.Occlusal appliance therapy in a short-term perspec-tive in patients with temporomandibular disorderscorrelated to condyle position. Int. J. Prosthodont. 11,236–268.
Ekberg, E., Nilner, M., 1999. The influence of stabilisationappliance therapy and other factors on the treatmentoutcome in patients with temporomandibular disor-ders of arthrogeneous origin. Swed. Dent. J. 23,39–47.
Ekberg, E., Nilner, M., 2002. A 6- and 12-month follow-upof appliance therapy in TMD patients: a follow-up of acontrolled trial. Int. J. Prosthodont. 15, 564–570.
Fayed, M.M.S., El-Mangoury, N.H., El-Bokle, D.N., Belal,A.I., 2004. Occlusal splint therapy and magneticresonance imaging. World J. Orthodont. 5, 133–140.
Haiter-Neto, F., Hollender, L., Barclay, P., Maravilla, K.R.,2002. Disk position and the bilaminar zone of thetemporomandibular joint in asymptomatic youngindividuals by magnetic resonance imaging. Oral Surg.Oral Med. Oral Pathol. Oral Radiol. Endodont. 94,372–378.
Hugger, A., 2002. Bildgebende Diagnostik bei Schmerz-symptomatik im Kiefergelenkbereich. Der Schmerz 16,355–364.
ARTICLE IN PRESS
Analysis of displaced TMJ disc 287
Houston, W.J.B., 1983. The analysis of errors in ortho-dontic measurements. Am. J. Orthodont. 83, 382–390.
Incesu, L., Tas-kaya Yılmaz, N., Ogutcen-Toller, M., Uzun,E., 2004. Relationship of condylar position to discposition and morphology. Eur. J. Radiol. 51, 269–273.
Jokstad, A., Mo, A., Krogstad, B.S., 2005. Clinicalcomparison between two different splint designs fortemporomandibular disorder therapy. Acta Odontol.Scand. 63, 218–226.
Kordass, B., Lucas, C., Huetzen, D., Zimmermann, C.,Gedrange, T., Langner, S., Domin, M., Hosten, N.,2007. Ann. Anat. 189, 371–376.
Kurita, H., Kurashina, K., Baba, H., Ohtsuka, A., Kotani,A., Kopp, S., 1998a. Evaluation of disk capture with asplint repositioning appliance. Oral Surg. Oral Med.Oral Pathol. Oral Radiol. Endodont. 85, 377–380.
Kurita, H., Kurashina, K., Ohtsuka, A., Kotani, A., 1998b.Change of position of the temporomandibular jointdisk with insertion of a disk-repositioning appliance.Oral Surg. Oral Med. Oral Pathol. Oral Radiol.Endodont. 85, 142–145.
Larheim, T.A., Westesson, P.-L., Sano, T., 2001. Tempor-omandibular joint disk displacement: comparison inasymptomatic volunteers and patients. Radiology 218,428–432.
Larheim, T.A., 2005. Role of magnetic resonance imagingin the clinical diagnosis of the temporomandibularjoint. Cells Tissues Organs 180, 6–21.
Ohnuki, T., Fukuda, M., Nakata, A., Nagai, H., Takahashi,T., Sasano, T., Miyamoto, Y., 2006. Evaluation of theposition, mobility, and morphology of the disc by MRIbefore and after four different treatments fortemporomandibular joint disorders. Dentomaxillofac.Radiol. 35, 103–109.
Orsini, M.G., Kuboki, T., Terada, S., Matsuka, Y.,Yamashita, A., Clark, G.T., 1998. Diagnostic value of
4 criteria to interpret temporomandibular jointnormal disk position on magnetic resonance images.Oral Surg. Oral Med. Oral Pathol. Oral Radiol.Endodont. 86, 489–497.
Ottl, P., 1997. Okklusionsschienentherapie. Dtsch. Zah-narztl. Kalender. 122–144.
Palla, S., 2003. Myoarthropatischer Schmerz: oft ver-kannt. Der Schmerz. 17, 425–431.
Plesh, O., Gansky, S.A., 2006. In: Laskin, D.M., Green,C.S., Hylander, W.L. (Eds.), Temporomandibular Dis-orders. An Evidence-Based Approach to Diagnosis andTreatment. Quintessence, Chicago, pp. 335–345.
Proff, P., Richter, E.J., Blens, T., Fanghanel, J., Hutzen,D., Kordass, B., Gedrange, T., Rottner, K., 2007. AMichigan-type occlusal splint with spring-loaded man-dibular protrusion functionality for treatment ofanterior disk dislocation with reduction. Ann. Anat.189, 362–366.
Rammelsberg, P., Pospiech, P.R., Jager, L., Pho Duc, J.-M.,Bohm, A.O., Gernet, W., 1997. Variability of diskposition in asymptomatic volunteers and patientswith internal derangement of the TMJ. Oral Surg.Oral Med. Oral Pathol. Oral Radiol. Endodont. 83,393–399.
Turp, J.C., Hugger, A., Nilges, P., Hugger, S., Siegert, J.,Busche, E., et al., 2006. Aktualisierung der Empfelun-gen zur standardisierten Diagnostik und Klassifikationvon Muskel und Kiefergelenkschmerzen. Der Schmerz.20, 481–489.
Warren, M.P., Fried, J.L., 2001. Temporomandibulardisorders and hormones in women. Cells TissuesOrgans 169, 187–192.
Witt, E., 1998. Die Michiganschiene. In: Palla, S. (Ed.),Myoarthropathien des Kausystems und orofazialeSchmerzen. ZZMK der Universitat Zurich, Zurich,pp. 181–194.